Zealand Pharma holds Capital Markets Day in London, and unveils a “Metabolic Frontiers 2030” strategy –
Zealand plans to build a multi-hormone metabolic franchise plus survodutide and petrelintide; up to $2.5 billion partnership with OTR Therapeutics will study novel therapies for metabolic diseases
Denmark-based Zealand Pharma announced today its new long-term strategic growth roadmap, “Metabolic Frontiers 2030,” at its Capital Markets Day in London. Over a half day of presentations, Zealand emphasized a focus on obesity and metabolic disease, positioning both areas as “civilization-scale” healthcare challenges that will define the coming decades.
Zealand CEO Dr. Adam Steensberg, CFO Ms. Henriette Wennicke, CMO Dr. David Kendall, CCO Mr. Eric Cox, and CSO Dr. Utpal Singh explored Zealand’s opportunity, strategy, and pipeline, offering compelling perspectives on how the company plans to execute on its ambition to build “the most valuable pipeline in metabolic health.” See the webcast and presentation slides.
Table of Contents
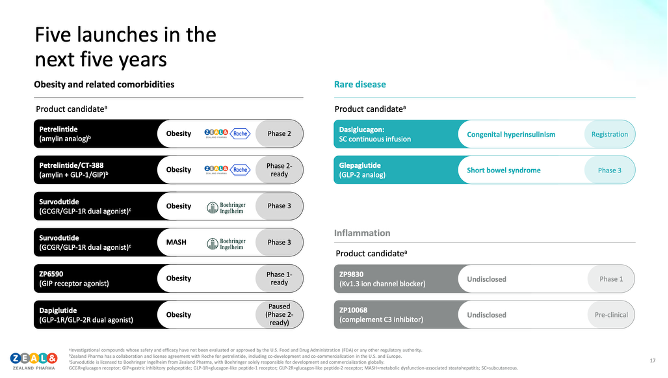
- Zealand’s long-term strategic ambitions include five product launches over the next five years
- Beyond the “Weight Loss Olympics”: Zealand’s focus on new mechanisms and next-gen incretins
- Survodutide for obesity, T2D, and MASH
- Petrelintide, a long-acting amylin analog
- R&D engine and early-stage assets
- Capital allocation will heavily favor obesity and inflammation
- Zealand and OTR Therapeutics partner to develop novel therapeutics for metabolic disease in an up to $2.5 billion deal
- Analyst Q&A
- Close Concerns’ Questions
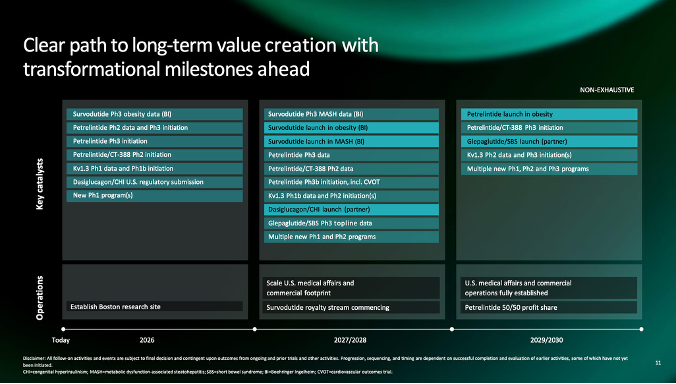
Zealand’s long-term strategic ambitions include five product launches over the next five years
In this compelling session, management outlined Zealand’s long-term strategic goals for its “Metabolic Frontier 2030 Strategy,” including:
- Five product launches over five years;
- Advancing over 10 active clinical programs in metabolic health; and
- An industry-leading development cycle time for these therapies, spanning idea generation to clinical entry by 2030.
Excitingly, Zealand hopes to build a “generational biotech company,” as described by Dr. Steensberg, by establishing a scalable obesity medicines platform supported by a broad, multi-product pipeline. “We are not going to be the one hit wonder,” Dr. Steensberg reiterated.
We do note that all the indications are for obesity and MASH, and not type 2 diabetes, even though some would likely “work on” T2D. We are wondering, could Zealand be the first company with an indication to delay or prevent T2D?
CSO Dr. Uptal Singh said, “We commit to, by 2030, if not earlier, be the fastest discovery engine in the industry by benchmark be the fastest discovery engine in the industry by benchmark number one… After 25 years of working in the space, we have unique insights. These insights are feeding into our discovery engine that are driving our engine today. But what really makes us special is not just that. Not only do we have 25 years of data that we're now going to see that we are going to – we're going to start partnering with people to build machine learning models and AI/ML models to accelerate our idea to data cycle times. But our close integration with medical and this, I think, is a unique secret sauce, having worked across multiple pharma companies, is that integration across research and medical.”
He continued, “Number one, we're going to focus on what we are really good at. And that's one, the cross-tuning access that's on a peptide heritage historically around metabolic health. We will commit to focusing on what is best, what we are the best at. At the same time, we also commit to partnering with experts externally to augment our capabilities. And third speed is our currency. We commit to actually, by 2030, if not earlier, be the fastest discovery engine in the industry by benchmark be the fastest discovery engine in the industry by benchmark number one. And number two, we deliver at least 10 molecules into the clinic before the end of the decade.”
Beyond the “Weight Loss Olympics”: Zealand’s focus on new mechanisms and next-gen incretins
Zealand framed obesity as a large, institutional global health challenge. By 2030, roughly half of the global adult population is expected to be overweight or have obesity, according to the company. In the US, an estimated 35% of children and adolescents aged 2-19 years already fall into these BMI categories.
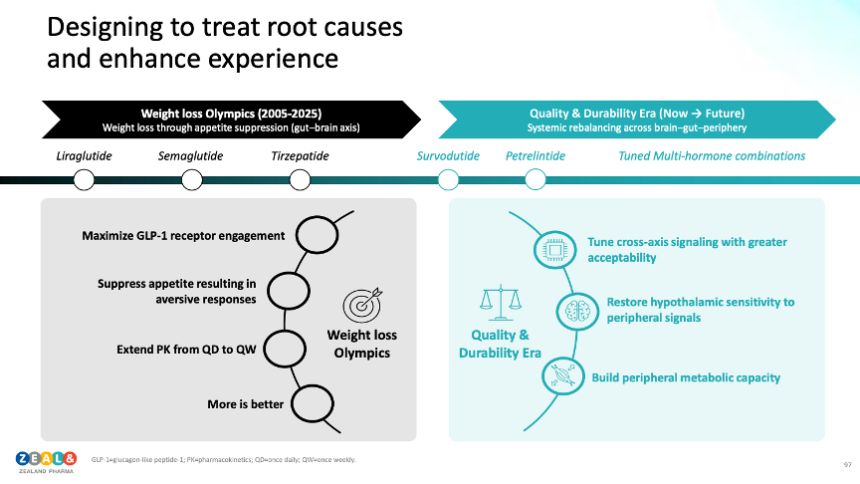
Management contrasted its approach with what it described as the ongoing “Weight Loss Olympics,” where leading pharmaceutical companies are competing to develop a candidate that leads across both speed and magnitude of weight reduction. Approximately 80% of current GLP-1 RA users report a target of up to 20% body weight loss, rather than higher weight loss outcomes often emphasized in randomized controlled trials.
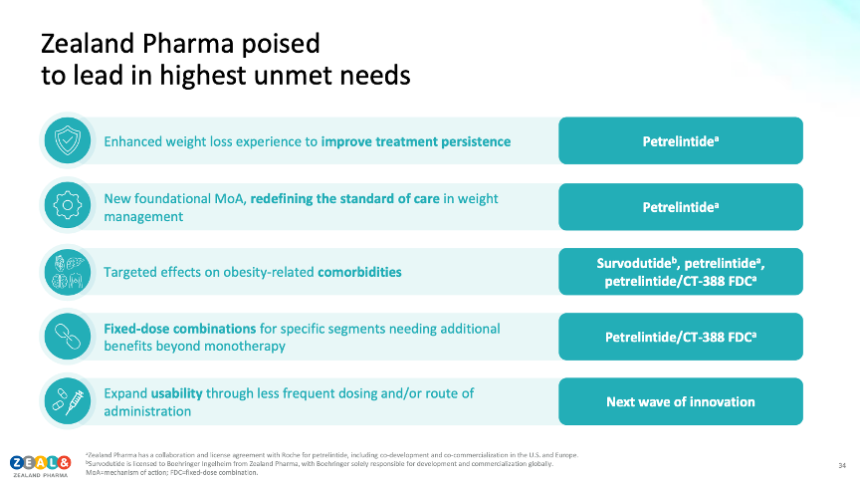
Accordingly, management argued that the obesity treatment narrative has become overly focused on rapid, maximal weight loss, leaving key patient and physician needs underserved. These needs include: (i) durable weight maintenance; (ii) improved (ideally placebo-like) tolerability profiles; and (iii) the management of obesity-related comorbidities. Given that GLP-1-based therapies represent the leading major drug class currently approved for obesity, management emphasized a clear need for additional, differentiated therapeutic classes to broaden treatment options and improve long-term outcomes. Thereby, the team began its Capital Markets Day by defining Zealand’s targeted therapeutic niche. As termed by Dr. Steensberg, “that is what Zealand is about… addressing the healthcare crisis that follows longstanding obesity and not just being part of a Weight Loss Olympics that has excited many for some period.”
Survodutide for obesity, T2D, and MASH
Survodutide, the company’s GLP-1/glucagon dual agonist, was highlighted as the cornerstone of the company’s disease-modifying metabolic strategy with MASH as a core indication, rather than an exclusive obesity competitor. Recall that survodutide is licensed to Boehringer Ingelheim (BI); BI is responsible for global development and commercialization of survodutide while Zealand is eligible to receive royalties on global sales, as well as up to £315 million in remaining development, regulatory, and commercial milestones.
For T2D, a 16-week phase 2 study evaluating multiple survodutide doses compared to placebo and semaglutide demonstrated up to a 1.9% reduction in A1c, from a baseline of 7.97% and 9.0% body-weight loss at the highest, bi-weekly dose (1.8 mg). In patients with obesity and without diabetes, a 46-week phase 2 study conferred clear dose-dependent weight loss, ranging from 6.8% (0.6 mg QW) to 19% (4.8 mg QW), compared to just 2.0% on placebo. Higher doses (2.4 mg; 3.6 mg; 4.8 mg) were also associated with clinically significant reductions in blood pressure. Gastrointestinal adverse events drove the majority of treatment discontinuations, supporting a slower, four-week dose-escalation schedule for phase 3.
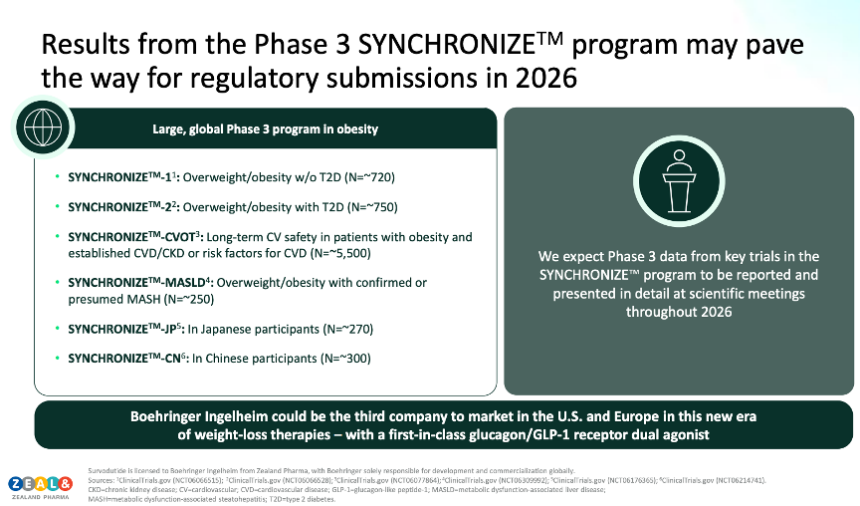
- Building on phase 2 findings, the phase 3 obesity program (SYNCHRONIZE) began in 2024. For people with overweight or obesity without T2D, topline results from SYNCHRONIZE-1 (n=725) are expected in the first half of 2026.
- The broader SYNCHRONIZE program also comprises five additional Phase 3 studies, including trials in obesity with T2D, a cardiovascular outcomes study, a MASLD/MASH-focused study, and dedicated programs for patients in Japan and China. Management expects multiple phase 3 readouts for the program to be presented at scientific meetings in 2026, which may support subsequent regulatory submissions next year.
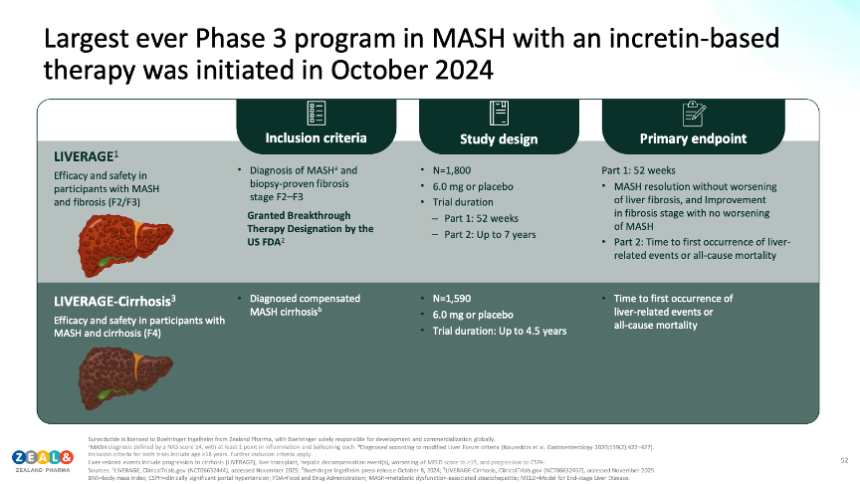
Both management and Prof. Carel le Roux (Ulster University, UK) emphasized the therapy’s direct hepatic benefit, potentially enabling fibrosis regression beyond weight-loss mediated benefits, challenging the historical view that fibrosis is irreversible. In patients with F2/F3 fibrosis, post-hoc analyses of phase 2 findings demonstrated MASH resolution without the worsening of fibrosis in roughly two-thirds of participants across higher-dose survodutide arms (compared to 13% of the placebo group). While noting the absence of head-to-head trials and differences in study designs, management highlighted that such fibrosis improvement rates are numerically greater than those reported for FDA approved agents (Madrigal’s resmetirom and Novo Nordisk’s semaglutide)! Notably, survodutide has received Breakthrough Therapy Designation from the FDA for MASH.
- The phase 3 LIVERAGE program is also evaluating the safety and efficacy of survodutide. The LIVERAGE trial (n=1,590) in patients with F2/F3 fibrosis will assess MASH resolution without worsening of fibrosis and fibrosis improvement without worsening of MASH at 52-weeks, followed by long-term outcomes including liver-related events and all-cause mortality. Notably, the LIVERAGE trial was also discussed to address tolerability issues in earlier studies with slower, more flexible titration schemes. Separately, the LIVERAGE-Cirrhosis study (n=1,800) is actively enrolling patients with compensated cirrhosis (F4), with time to liver-related events or death as the primary endpoint. In forward-looking, commercial discussions, management expressed optimism that healthcare systems were more likely to reimburse treatments for obesity-related complications, compared to those indicated for weight loss alone.
Prof. le Roux said, “These are not weight loss drugs. These are drugs for the treatment of obesity. These are disease modifying drugs. So when I was in med school, we were taught that fibrosis is a one-way ticket. The best that we could do is slow it down. Now, what this shows is anything in biology that goes in that direction can also go in the opposite direction if you change the metabolic milieu. And that is what these drugs are doing.”
Petrelintide, a long-acting amylin analog
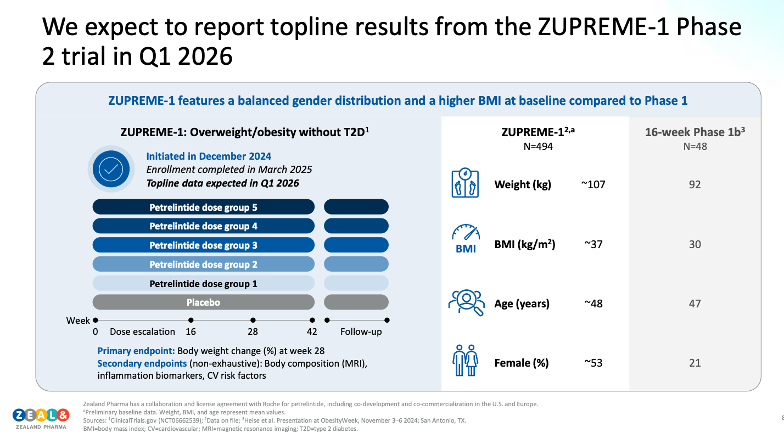
On petrelintide, Mr. Steensberg said, “It's a product that has been designed for doable and high quality weight loss, and it's a product which we believe as a standalone medicine has potential to form the future foundational and first choice medicine for people who wants to lose weight and importantly, want to maintain that weight loss. When you sit with what we consider a crown jewel, like petrelintide, you don't want to do shortcuts in development. That's why we designed the Phase 2 study the way we did with a 50-50 balance of males to females and not an 80% female, 20% males, where we don't learn a lot about a molecule in males.”
Echoing these remarks, in Q&A, Dr. Louis Aronne (Weill Cornell University), shared, “Like, I don't know about you, but I know what I would do. I think combining Amylin with the other incretin-based therapies is going to be a very good way to go to get the kind of greater weight losses that will treat patients who are in that surgical range. I mean, personally, I see surgery. I don't want to say it's going to vanish, but it's going to be a last line therapy, a very last line therapy compared to even where it is now. And I think that the strategy a very last line therapy compared to even where it is now. And I think that the strategy, my personal belief is that the strategy moving forward is going to be to maximize the Amylin based compound and then add GLP-1s on top of that. I personally think, you know, based on our experience and some of the animal data, that that will be the best strategy for the greatest weight loss and the greatest tolerability.”
Petrelintide, Zealand’s lead long-acting amylin analog, was framed as a foundational, first-choice “crown jewel” monotherapy for chronic weight management. Currently, the therapy is in development to address key limitations of current obesity therapies: (i) tolerability; (ii) durability; and (iii) chronic usability. By promoting earlier and prolonged fullness, Zealand views petrelintide as a solution to a structural adherence problem of weight-loss therapy. As background, Zealand and Roche have partnered to co-develop and co-commercialize petrelintide and petrelintide-based combinations in the US and Europe. In other markets, Roche will commercialize the therapy, with Zealand eligible to receive up to $2.4 billion in sales-based milestones and $1.2 billion in development milestones. Roche will be responsible for commercial manufacturing and supply.
- In single-ascending-dose studies in healthy participants and participants who are overweight, single doses up to 12 mg conferred placebo-adjusted weight loss of up to 4.8% at seven days post-dose, with no reported nausea or vomiting at effective dose levels. In multiple-ascending-dose (MAD) studies, 1.2 mg over six rounds of weekly dosing demonstrated ~5% weight loss compared to 0.4% weight loss in the placebo group. Strikingly, there were fewer gastrointestinal adverse events in the petrelintide group than placebo. In a subsequent 16-week MAD study in adults with overweight and obesity (baseline weight ~92 kg; BMI ~30), petrelintide demonstrated dose-dependent efficacy, with weight loss of 4.8%, 8.6%, and 8.3%, at 2.4 mg, 4.8 mg, and 9.0 mg, respectively, compared to 1.7% on placebo.
- ZUPREME-1 (n=494) is a phase 2 study in adults with obesity and without T2D (see below). The study was initiated in December 2024, completed enrollment in March 2025, and topline 28-week and 42-week data are expected in the first quarter of 2026.
- In parallel, ZUPREME-2 (n=216) is a phase 2 study evaluating petrelintide in individuals with obesity and T2D. 28-week topline data expected in the second half of 2026.
- Moving beyond phase 2, management offered a look at Zealand’s phase 3 staged development strategy. Phase 3a monotherapy trials are planned to support an accelerated launch in obesity, while phase 3b will explore petrelintide for other comorbidities and indications, including a potential cardiovascular outcomes trial. In parallel, a phase 2 combination trial of petrelintide with CT-388, Roche’s GLP-1/GIP dual agonist, is expected to begin in the first half of 2026. The combination study will include active comparator arms of petrelintide monotherapy and CT-388 monotherapy with an objective of identifying dose combinations which maximize weight loss and optimizing tolerability.
R&D engine and early-stage assets
Throughout the Capital Market Day, management emphasized Zealand’s over 25-year track record in peptide research and development. This competitive advantage is expected to support the company’s ambitious goals. Strategically, management described a focus on “tuned multi-hormone” approaches, including amylin, GLP-1, glucagon, and GIP, to achieve systemic metabolic “rebalancing” rather than single-pathway appetite suppression.
- Management also highlighted two emerging pipeline assets:
- ZP9830 is a Kv1.3 inhibitor described as having “pipeline in a product potential.” A phase 1, first-in-human single-ascending-dose study is currently underway, with pharmacokinetic and safety data expected in the first quarter of 2026. Phase 1b and phase 2a multi-indication studies are already planned pending phase 1 results.
- ZP6590 is a GIP analog described to improve tolerability and adipose insulin sensitivity, reduce ectopic fat accumulation, and enhance metabolic flexibility. A phase 1 trial is planned for 2026.
Capital allocation will heavily favor obesity and inflammation
Ms. Henriette Wennicke (EVP + CFO) described upcoming asset allocation priorities, saying, “Number one. We will invest to establish a leading multi-asset amylin-based franchise. Both in terms of on the investments, but also commercial investments, as you heard Eric talk about today. And these investments were of course, mainly go into [indiscernible] and monotherapy. But have you also heard evolve, pursue combination and we will pursue new emerging opportunities. We'll also invest to accelerate and strengthen our research engine. Utpal have just talked us through the step change will do in research over the coming years. And lastly, number three, to pursue inorganic investments to enhance our R&D capabilities and our pipeline, as Utpal mentioned today, we announced a first exciting new partnership with OTR. And this will give us more capabilities and strength in order to build out our pipeline.”
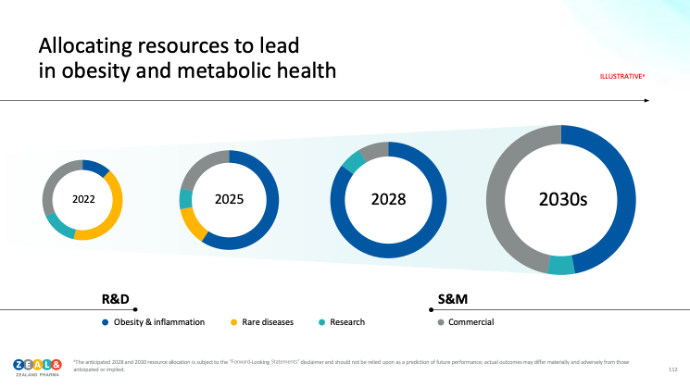
Management outlined plans for an increase in research investments. Over the past five years, Zealand has invested approximately DKK 1 billion (just over $150 million) in research activities. Over the next five years, the company expects this figure to soar to roughly DKK 5 billion (over $785 million), with the majority of spending directed toward obesity and inflammation.
Further, management outlined Zealand’s capital allocation priorities, most notably to establish a leading, multi-asset amylin franchise that includes: (i) petrelintide monotherapy; (ii) combination regimens; and (iii) next-generation amylin-based candidates. The company also plans to further accelerate and strengthen its research engine through continued investment in artificial intelligence, machine learning capabilities, and its discovery infrastructure. Lastly, management shared a desire to pursue selective partnerships or acquisitions that enhance R&D capabilities and add pipeline assets for obesity and inflammation. In closing, management characterized its goal as building a “pharma pipeline with biotech financial discipline,” balancing the scale typically associated with larger pharmaceutical companies with the efficiency, focus, and execution rigor of a biotechnology organization.
Zealand and OTR Therapeutics partner to develop novel therapeutics for metabolic disease in an up to $2.5 billion deal
Though not mentioned in its Capital Markets Day presentation, Zealand also announced today that it has entered a multi-program strategic collaboration and license agreement with Shanghai, China-based biotech OTR Therapeutics. The companies intend to discover and develop novel therapeutics for metabolic diseases. The collaboration will combine Zealand’s obesity and metabolic health expertise with OTR Therapeutics’ proprietary oral small-molecule platform and drug discovery capabilities.
Under the agreement, OTR Therapeutics will receive a $20 million upfront payment and is eligible for up to $2.5 billion in preclinical, development, regulatory, commercial milestone payments, and tiered royalties.
Analyst Q&A
On survodutide
Q (Mr. Thomas Bowers, SEB): How should we think about optimal positioning for survodutide? Is there a sort of critical path here for both the program to evolve more into a premium-priced MASH therapy rather than targeting obesity?
A (Dr. Adam Steensberg, CEO): Yeah. So, of course, this is a program that is being developed and commercialized by Boehringer. We will just receive high singles to low double-digit royalties. And it's for them to comment on the specifics around the pricing strategies and go to market. But as both Carel and David alluded to, it's quite clear that where we see this opportunity is, of course, not only in for a weight loss agent, but also to really make a breakthrough therapy for people with MASH, which speaks a little bit perhaps into the segments that Eric talks about, the prescriber-driven segments where you have a key understanding of the need from a co-morbidity perspective, and thus that may also for some pricing considerations, but we cannot comment on their pricing considerations.
A (Dr. David Kendall, CMO): I think the success of resmetirom in the US, which obviously does not compare at least in terms of magnitude of effect, show the desire for treatment in this space which our BI colleagues clearly recognize. Not to forget, too, that mazdutide is approved in Asia, in China, and all indications are this is something that that population is turning to. So I think from a former clinician now a pharma guy perspective, clearly an unmet need. And maybe, Carel, comment on what you're seeing in terms of the need or the desire to fill this position in your clinic.
A (Prof. Carel Le Roux): And I think the problem is that people are not being diagnosed with liver disease. So when you actually come into a system, be it primary care and primary care doctor, really the ones driving the system, when they now suddenly make a diagnosis and say to you, turns out, now with a non-invasive test, you also have liver disease, which I never thought about. It's highly motivating for patients. And it also really comes in to that metabolic health gain that people will actually continue with treatment for. So I think this is a real opportunity.
Q (Ms. Kirsty Ross-Stewart, BNP Paribas SA): Your slide mentioned the potency was sort of 8 to 1 on GLP-1 to glucagon. We've obviously seen GLP-1 only in receptor agonists has a benefit on fibrosis, but without the glucagon mechanism. So, can you elaborate on the benefit of also hitting the glucagon receptor, but also whether you believe that 8 to 1 ratio is optimal, and whether that will confer a meaningfully differentiated effect on the liver disease versus a pure GLP-1 RA?
A (Prof. Le Roux): I think this ratio does appear to be optimal because what you have is you've got many of the upsides of GLP-1, you have the upsides of glucagon, but we do not see any of the downsides of glucagon, right? So that's why I think the ratios are important. But what we do see, if we actually look at data only driven by GLP-1 based therapies, that is fibrosis appears to be weight loss dependent. That means you reduce the adipocyte mass in the liver and therefore it allows the liver to recover, right?
What you now see when you actually have a treatment such as survodutide, you have all the benefits of the weight loss. So you have the reduction in adipocyte mass, but you have benefits on fibrosis that goes beyond what you would expect and that's why we see those graphs being substantially different. So the glucagon receptor really makes a difference. Right. But it's not pulling the wagon on its own because it has the benefit of GLP-1 and I think this ratio, which is specifically designed appears to be an optimal ratio.
Q (Mr. Xian Deng, UBS): You also have the fixed rate ongoing for F4. So just wondering, given previously this is really a hard bar and some of the jobs haven't been successful. Just wondering what you know, what gives you the confidence there.
A (Prof. Le Roux): So maybe if I take the last one, so the F4 fibrosis, patients who have cirrhosis, compensated cirrhosis, I'm not the clinical investigator in that study. I'm the clinical investigator for the SYNCHRONIZE-1. So I give you an opinion, somebody in the field rather than an investigator in that study. I think it is ambitious. Right? But I think the data that they have so far supports that ambition. And that is something that is also one of these halo effects. Right? If you can actually take patients who previously have been thought of almost now entering into a palette of emotion, and you can show that you can actually not only slow it down, but you can reverse it, that would be very, very impressive. You saw that the primary outcome there was not only liver death, but also all-cause mortality.
And remember that what we see with a lot of these treatments now, we see that all-cause mortality is really one of the most intriguing things because then all-cause mortality is not only driven by reduction in cardiovascular events, it's also driven by reduction in infectious states. And that's something that, again, is we learning how these compounds are reducing inflammation and allowing patients to actually deal with infection much better.
Now, again, if you think about that cohort of patients who have F4 cirrhosis, why do people die? What's written on the death certificate? It's not a very often liver failure. It's – they died from infection. They died from cardiovascular events. And I think that is part of that ambition. So, I think that that is the right way to go. And these are one of these things that actually really changes the space. And if it turns out that that study is neutral, then, that would be a massive disappointment for many people in the room. I get that. But for us as clinicians, we go, wow, we have so little to help those patients. And now we actually have something that not only is going to be safe, but those patients are going to come back and say, for the first time in my life, I can play with my – well, first of again, I can play with my children, I can pick things up from the floor. My functionality is so much better. And that's what we see is quality of life with these, and I would expect the same to come out with the survodutide study, it's the quality of life is not driven by the mental component.
We do not make people thin and we do not make them happy, right? But what we do, do is we make them healthier and we make them more functional. And that's what drives quality of life. So I think those are – well I think it's a good program and that's what I would expect to see.
A (Dr. Kendall): A quick comment on the glucagon component. I started my ill-fated metabolism career studying the sort of forgotten hormone glucagon, low dose glucagon infusion, low exposure has effects on energy expenditure. Obviously, these effects on lipolysis and fat deposition and clearance when high dose glucagon exposure obviously can raise plasma glucose and increase the likelihood of GI side effects. So, getting that balance right, having given emergency doses of glucagon, giving high dose glucagon infusion, you sort of see what happens with too much, just enough for getting this just right. A bit of Goldilocks, I guess is a tough needle to thread, but I think a long history that low dose glucagon exposure as these salutary effects.
Q (Mr. Xian Deng, UBS): You have extra liver benefit on top of the normal GLP-1. So just wondering what other sort of data supporting, let's say, per percentage or weight loss, having the glucagon component has extra liver benefit versus your OP one, because we do also see this correlation generally with weight loss as well. So that's the first question.
A (Dr. David Kendall, CMO): A quick comment on the glucagon component, I started my ill fated metabolism career studying the sort of forgotten hormone glucagon, low dose glucagon infusion, Low exposure has effects on energy expenditure. Obviously, these effects on lipolysis and fat deposition and clearance when high dose glucagon exposure obviously can raise plasma glucose and increase the likelihood of GI side effects. So, getting that balance right, having given emergency doses of glucagon, giving high dose glucagon infusion, you sort of see what happens with too much, just enough for getting this just right. A bit of Goldilocks, I guess is a tough needle to thread, but I think a long history that low dose glucagon exposure as these salutary effects.
Q (Jacob Mekhael, KBC Securities): I have a bit of a technical question, if I may, since we have the scientific here. And survodutide and the fibrosis data that you shared, 38.6% looks really good, but this was post hoc data. So I'm curious, how would you expect that to evolve, or looking at intention to treat in Phase 3? And given that this is what FDA will look at for the approval? And do you think this level can be maintained or should we factor in a drop? And if so, what's the magnitude, if you can give us any indication?
A (Prof. Le Roux): So certainly from my side and remember, because this is some biopsy data. So biopsies before and biopsies afterwards. And so therefore the data has been collected prospectively. But then of course, you analyzed and it's almost like now when I speak to colleagues at Zealand and others, I say to them, almost like the regulator is the easiest path to get across, right, because people don't actually think this was possible. So, actually getting it over the regulatory body is pretty easy. Now it's like, how do you actually turn this into value for the provider like me or for the patient, but specifically for the payer? So I think those numbers, I think, if we see anything above 50%, that would be very impressive. So but I think we are in that ballpark even on an intention to treat analysis.
On petrelintide
Q (Ms. Sushila Hernandez, Kempen): So you've mentioned in the past it's not only about weight loss, so how do you expect petrelintide to do body composition or quality of weight versus the other eminence?
A (Dr. Kendall): So I think for us, obviously, the consistent preclinical readouts from most Amylin-based therapy programs have shown this difference in preserving lean mass targeting fat mass. Jon Roth in his discussion, showed some of the early data with Pramlintide and rat Amylin achieving the same thing. I think for us, given what's been observed with Cagri, we're doing much more careful our assessments in ZUPREME-1. This would be a value add a nice to have and certainly hope that it could add to the benefits of an Amylin based therapy. But obviously effective weight loss, tolerability and that experience come first for us. Certainly if we see improvements in or at least maintenance in muscle mass, that would be a clear value add. I would say even with inhibin e-activin the myostatin inhibitors, the best muscle to have is the muscle you started with. In my personal opinion, Lou, I'd love to hear your comments as a clinician.
A (Prof. Louis Aronne): I agree that preventing the loss of lean mass is really going to turn out to be the way to go. And leptin sensitization, I think, could turn out to be a very good way to do this. You know, in early studies from back in the old days, leptin is one of the key modulators of skeletal muscle mass. And, you know, part of losing muscle has to do with low leptin levels so we can keep leptin sensitivity up. So that leptin activity is higher. Whether the levels are low or high should preserve lean mass and metabolic mass. So, I'm enthusiastic about that.
Q (Mr. Yi Han Li, Barclays): I guess my question is really on amylin market potential. To me, I feel like the key differentiations for amylin versus GLP-1. The first one will be the [indiscernible] but as Dr. [indiscernible] said earlier, so if it's like the tolerability issue should be very minimal as long as the procreation is slow enough, always dosing reduction.
The amylin cause the satiety enhancement, as you emphasized in the presentation, versus the appetite suppression, just like the GLP-1, but again in the [indiscernible] one study lacked that appendix. It seems like kind of being tight showed that generally similar incidences of decreased appetite, rising tide. So I think I'm just curious, first of all, like how clinically meaningful or relevant do you expect this regulating mail size to be in the real world positioning for this coming business [indiscernible] and what his you know, how should we size the true commercial potential by amylin costs over the next decade? Thank you.
A (Prof. Aronne): So, you know, the only way to know is to do the study, right? And so when I think that right now, when you look at how we're treating patients with GLP-1, we're kind of over-suppressing their appetite and their interest in eating food. And you've all heard about examples of that where people lose interest in, and we have people who are, and we have people who are – they're food critics put it that way, and we have to back off on the dose because they feel they can't be a food critic. They’re not that interested in food with the currently available compound. So I think that it'll be very interesting to see if we can change that. I have a belief that we will, but I'm not certain that we will until we do it.
A (Dr. Kendall): And I'll add that, I mean, decreased appetite can be measured a number of ways. I've eaten, and I eat enough; my appetite is decreased, or I don't wish to consume food, both can be reported as medical terms for decreased appetite. I think both will work. But as Adam alluded to, that could be a very different experience for those who look to eat but eat less.
A (Dr. Steensberg): Eric has also alluded to some of these observations. One thing is what you can do and what you can achieve by careful titration. But it is a little bit if you think about a category that is probably going to be the largest health category in the world. It's a strange conversation to have about you can tolerate it? And how can I titrate you to be able to tolerate this therapy? And we argue that once you have alternatives, radically different alternatives that we believe eminent will be, then you will not talk about can you tolerate it? Then the conversation will be, will you accept it? Will you, as a patient, accept that you have to go through all that struggle to achieve your weight loss? That's number one. So alternative therapies will change the conversation. It is not a natural conversation to have when you think about chronic therapy. Can you tolerate it in my mind?
And number two is the weight loss in my mind? And number two is the weight loss experience. I think we underestimate how motivated people are to lose weight. And that's why we see this sick use of GLP-1s today, where people use them to lose weight. And then once you get you have achieve your weight loss, you are less motivated. You will accept this. We know that from any other weight loss program in history. Once you let go of the patient, they will regain weight, most of them, and they are back to square. And that weight cycling is not healthy. And if so, if we don't manage to get therapies that people stay on, then we will not achieve the health benefits. So we need to move beyond what we see today. And better to envision a different future which is more suited to the lives of patients want to live and not the ones that we think they should. And we believe that is what Amylin can provide.
Q (Ms. Lucy Codrington, Jefferies): You showed the data at the beginning, where you showed the discontinuation rates due to ease. And I just wondered, do you have a split for that between patients who are being seen by a prescriber that segment and the patients who are DTC or consumer based? And is it higher when in the latter, where you are being patient with the tolerability? Or is that primarily the consumer base? And then the second question, you talked about the best-in-class profile, and I understand your argument for it, but I just guess, what are the chances that it's going to be differentiated enough that you would choose one Amylin over the other when there are two on the market and one of them is being marketed by Lilly?
A (Dr. Steensberg): Some other data available, but I would say I'm not sure we have those days that bring down that experience between a very skilled prescriber versus a phasing that achieved this product from a less prescribed, less skilled prescriber base. But I have no doubt that if you are treated by a very skilled prescriber, you can have a much better experience. And these guys also know how to encourage patients to stay in therapy they as compared to if you just seek these wait clinics. But today, the majority of patients are receiving treatment from these Waycross clinics. And that segment will grow in the future, as we heard Eric talk about. And it's coming back to not all patients. Actually, very few patients have the luxury of seeing people who are as good as the guys you hear from today. So we need to focus on those people. That is where the peak commercial opportunity is. And it's also a big opportunity to actually, truly have a global scale health impact.
A (Prof. Aronne): I think that when we're using these more tolerable medicines, they have fewer side effects. I think it's going to be easier for everybody to prescribe. But the question about, which one are you going to pick? I mean, in hypertension, there are over 100 drugs available. Are you aware of that? How many how many lipid-lowering drugs are there? And when you look at the weight-regulating pathways, there are a lot more complicated than those pathways. So my guess is that if there are two or three drugs in that category now, I'm sure that the sales team at Roche is itching to get at this problem, you know, and at other companies as well. I'm guessing they can figure out how to help doctors decide which one to prescribe.
I mean, I just saw in New York, we have Pfizer, Pfizer's there. I've been advising Pfizer for 15 years and the people, I see a number of people on the marketing team who take care of them, and people like that are losing their minds because they don't have a horse in the race. So I'm guessing that when you look at the size of the market, it's going to be DKK 200 billion or something, or who knows what it is, but it's going to be massive, and right now it's like this. So I think everybody would like an opportunity to convince doctors that their medicine is the best one.
A (Dr. Kendall): Lucy, you point out an opportunity we have, which is that these differentiating factors may not be huge, but they could be critically important. How simple is dose escalation? How likely is it that you will stay on the maximum dose? I think for all the positives that came out of the eloralintide data, the rush to high dose clearly sort of blew up in our face, meaning going on 6 or 9 milligrams, if you go beyond GLP-1 like tolerability concerns, whereas their titration scheme, which may have sacrificed a few percentage points. But I know, our development teams at Roche and at Zealand are excited to look at these opportunities. Back to the previous question, doing exit interviews to talk about the experience and then building that into mechanistic studies and Phase 3b studies, where we can bring it forth and say, here's the value. I think of one other example, which is the thiazolidinedione. On rosiglitazone, pioglitazone weren't that different. But there were small pieces to that, the lipid profile, some of the experiences using lower doses of one that ultimately helped differentiate both were widely utilized, but there were opportunities that I think we on the development medical commercial side are excited to leverage going forward.
Q (Mr. Rajan Sharma, Goldman Sachs): Just thinking about if this does become more of a consumer market, will that influence how you think about a Phase 3 trial? I'm just thinking, would it be worth it at some point, or would you consider running a head-to-head versus GLP-1 to really hone in on that differentiation, or maybe even a reference arm, even if it's not necessarily a regulatory requirement?
A (Dr. Steensberg): I think you're absolutely right that the profile of Petrelintide, which has this ability to make hopefully people feel full faster, have a better way, those experiences speak directly into that consumer segment, which Eric also showed that 60% of all scripts today are patient initiated. So what do you need to differentiate out there, considering that a lot of patients will have conversations around their weight loss experiences once these molecules get to market. That can be a very, very strong sentiment. If you hear somebody having had a completely different weight loss experience on an amylin versus on a GLP-1. So that sentiment on an amylin versus on a GLP-1. So that sentiment around conversations among patients we think will be a major driver for success and early uptake. And since it's really consumers, patients that are initiating most of the conversations, this is probably the area where you could see the fastest swing from one category to another because it doesn't necessarily go through the normal channels, starting with a key opinion leader data and then down until the guideline. But actually you start with patients and they have a tendency to talk on social media. So we think we could actually have a very fast swing if we can ultimately in the real world provide those experiences that David have talked about today.
A (Dr. Kendall): And I think to your comment about head-to-head in the other set is part of that Phase 3b excitement that we share. But again, we're going to focus on three and get this to patients and providers.
A (Prof. Aronne): So when you're doing clinical trials, patients are on a forced titration regimen. And, you know, we've seen this where people are eating nothing literally because they're sensitive to it, but they're on a dose that's higher than they probably need. And so, you know, what are they eating? Yogurt for breakfast and three ounces of chicken, and three string beans for dinner. And they're exhausted. They come in the next time they're exhausted. Of course they are, because they're getting no nutrition. So in my opinion, there are a number of people like that who are going to be mixed in, and they should be on a lower dose. As time goes on and we're able, we understand what's happening better. And when I say we understand, we know what's happening. We just need a more adaptive trial design so that we can focus on the side effect profile rather than maximum efficacy, because that's what the trials are really focused on now.
A (Dr. Kendall): And I think it's important that the weight loss lets me explore both speed and magnitude, and that's, you know, helpful in clinical trials, it's helpful for you to try to make judgments of the efficacy. Clinical reality and clinical trials are often not terribly well-aligned.
Q (Rajan Sharma, Goldman Sachs): In phase 2, I know there was a fatigue signal that seems to emerge. Do you think that there is a risk that that's a class effect? And specifically, could that be an effect with Petrelintide as well?
A (Dr. Kendall): And on the second part of the question on fatigue, I guess, it's also fair to say that, of course, we saw that in some of the treatment arms in the LRM ZUPREME-2 trial, where relatively high rates of fatigue with petrelintide, we haven't seen that signal or that imbalance relative to placebo. And I'm quite confident that's the same [indiscernible] on site in the we define one trial around two standard clinical data from. I think we have time for one last question before we need to move on.
Q (Kirsty Ross-Stewart, BNP Paribas SA): Just on the timelines, it showed that you're expecting Phase 3 data for the petrelintide program in 2027 and 2028. So can you confirm that you'll be able to launch in 2029 at the earlier end of your 2029- 2030 estimation? And can you also just provide a quick comment on, I think the ZUPREME-2 timelines have shifted to 2H next year from midyear. Just what has driven that change?
A (Dr. Steensberg): So we can confirm that we are hydrophobic together with our colleagues at Roche to accelerate the program towards market. And we will do our utmost to get it as soon as possible to patients. But we are not committing to a specific year right now, but 2029 is of course a possibility.
A (Dr. Kendall): Yeah. I think partly the challenges of recruiting a fairly challenging population who were essentially treatment naive in the setting of Type 2 diabetes were something that we obviously succeeded with. We announced recently that we've fully enrolled in that trial, but it gave us more precision as to when patients last, as if the data readout would be. So I don't see it as, but it gave us more precision as to when the last patient patients last as if the data readout would be. So I don't see it as a seismic shift, but just a dose of honesty from us to you. But again, our efforts to initiate Phase 3 are only tied back to ZUPREME-1 that's what we're using as our guide forward, as our ZUPREME-2 is a value-add at this point, and so it does not change the other timelines.
Q (Mr. Jacob Mekhael, KBC): I had a question maybe on your commercial plans for petrelintide in the US, now that the Roche partnership has evolved quite a bit and it's been a few months since you've had it, how has your thinking evolved there and what kind of commercial model do you think would be suitable for Zealand and yeah, what would be a good fit in that sense? And how do you take into account DTP and also the rise of telehealth into all of those plans?
A (Mr. Eric Cox, CCO): Yes. So it's a little bit early. It's kind of some of these conversations. I mean, the market's evolving at a speed that we have we're trying to keep up with. We've just we've just gone through the discussions with Roche, and we're in those early discussions. So I think probably over the next several months and next several quarters will start to kind of materialize how we're thinking about this. But I think to your question on the DTP side of it, I think you'll start to see, and we've seen DTP be an extremely important role. We know it's a consumerized category, and we still think it's going to be consumerized as we go forward. So it is about unlocking that opportunity. I don't think it's direct-to-consumer. I think it's more around DTP.
Q (Mr. Håkon Hemme Bro Jorgenson, Danske Bank): On the next era, treatment beyond set aside, how should we think of the innovation in the metabolic field? I mean, have we reached a point where we should expect only incremental improvements for the next generation innovations?
A (Dr. Steensberg): I think if we start by recognizing that obesity is the driving the biggest health crisis across I think if we start by recognizing that obesity is the driving the biggest health crisis across the globe, and we also look at the curves for how many patients have been exposed to it yet the one and how many patients are [indiscernible] one today. I think we will all realize that we are in the very early days of treatment and getting our hands around this health crisis that is needed in order not to break for the breakdown of our healthcare system. So you ask, can we only expect slight innovations in the next crisis that comes out? And that, of course, depends on the eyes that you look with.
If you talk about weight loss, the weight loss Olympics, I think you can only expect slight improvements because we have already seen very, very deep and very fast weight loss but where you can see significant breakthrough innovation is in how you address metabolic health and when it comes to weight loss, as we have argued today, it's not about speed or depth of the weight loss it's about the ability and the quality of that weight loss and we think that way of a step change is a breakthrough change in management of obesity that is what amylin brings along, in particular with the petrelintide.
If you then think further into the future, we need to keep a firm eye on what has also been shared by some of the experts who will need different tools. Also some patience, of course, there will be patients who don't respond as well as others to the amylin category because it's such a heterogeneous disease that doesn't remove the – what we believe that petrelintide will form the foundation for the most patients and the first choice but as we move into what would [ph] people talk about it's really about metabolic health and beyond on weight loss.
A (Dr. Utpal Singh, CSO): Yeah, absolutely. And I will point you to my comments around weight-independent insulin sensitivity. If you really think about the therapies that are out there for truly weight-independent and insulin sensitization, there really aren't many, if any, in that space. And I come back to that analogy of the engine, and I come back to that analogy of the engine and the parts like the fuel injection system will shrink the engine with the current therapeutics. But the system itself is still clogged. Right. And I think we need to get to the point where we have improved insulin sensitivity and metabolic flexibility such that you can switch from different fuels force-fed in fasted conditions. So I think the opportunity that's left with current therapeutics is significant. The question now is really going to be for the scientists, which of that biology actually translates in a meaningful way to have that impact?
A (Dr. Kendall): And I'll add one example with type 2 diabetes, where we see with GLP-1-based therapies, you clearly lower the curve, meaning glycemic control improves, but the progressive deterioration and beta cell function is still evident in longer-term follow-up. So we've moved the curve, but we haven't changed the shape. So disease-modifying therapies in both Type 1 and Type 2 diabetes are essentially unheard of today. If that can be brought to bear, that will be a seismic change in metabolic health. And I think similarly, survodutide, instead of just winning the numbers game to leverage that potential impact on liver disease, is transformational. If this becomes the drug of choice or an approach of choice for that population, to me, that would be transformative.
Q (Mr. Xian Deng, UBS): I'm very intrigued by one of your comments, Utpal, saying there are many people who actually have a BMI that's smaller than 25, but actually have metabolic dysfunction. And also as you alluded to, you know, for example, the BMI definition for overweight is also different ethnicities as well, right. So if I may take a step back, actually, how do we know how to define metabolic health? What exactly are you measuring? So why are some people who are, for example, who eat a lot but never really get much weight, whereas others can cycle a lot, but there's not much happening. So how can you actually -- do we actually know what the difference?
Second one is particularly amylin, you know, particularly tied in terms of the comments throughout the day in terms of maintenance and also the consumer driver. So just wondering, in terms of actual maintenance therapy, again, just wondering what exactly you would consider as maintenance therapy? Because in the real world, we already see, you know, on social media, people doing microdosing or whatnot every three months or whatnot. So, what exactly constitutes maintenance, and what you will actually measure in a study, would it actually be a very long-term study? What would you actually be measuring?
A (Dr. Singh): First of all, thank you for asking that. On metabolic health, from a very fundamental standpoint, as I said, it's about energy intake, energy storage, energy metabolism on a fundamental sense. Now, as you think about in the pre-clinical way, the way I'm thinking about this is really going to be around certainly weight loss to one component will have that. There's also around insulin sensitisation and particular weight-independent insulin sensitization as well as around some of the insulin left in sensitization centrally. That's how we think about it preclinical.
Now, as you go into the clinic, certainly those measures change significantly. Ultimately, the advance in the clinic, your insulin sensitization is still going to be a significant measure for that. But what we believe, if you focus on these elements preclinically, they'll translate into much better outcomes. You will actually see improvement in the absolute risk ratio for CKD, CVOT cardiovascular, et cetera. So I think it really metabolic health needs different things, but from a clinical standpoint, from a patient standpoint, it means improved outcomes around cardiovascular, renal, et cetera.
A (Dr. Steensberg): I think the dilemma today is that we have already seen from the GLP-1s the value of maintenance, at least for a few years in a clinical setting. The problem is in the real world, very few patients get to that benefit because, as Eric showed us, 80% will be off therapy within a year. And we know that cycling your weight is actually unhealthy. You often would consider, will you just get back to square one? You will actually very often be worse off once you are back because you put on a few more pounds. So we don't want to be in that situation. And as David also alluded to, GLP-1s and we heard from some of the speakers, stimulus insulin, amylin potentially will not do -- it's not stimulating insulin and exhausting beta cells if you think about treatment 5 to 10 years and may not be the smartest thing to do if you want to achieve metabolic health.
And this is why if you think about it, exhausting beta cells if you think about treatment 5 years to 10 years and may not be the smartest thing to do if you want to achieve metabolic health. And this is why, if you think about it, if we -- within the eminent category deliver what we have set out to deliver in a clinical setting, we think it will translate directly into real-world experiences because people will actually manage to stay in therapy and gain those health benefits that we think we can achieve on amylin.
A (Dr. Kendall): And to add to that, I think what Paul alluded to it, but expanding and improving health span and lose comment about why should I wait till I've had a stroke and my hypertension dyslipidemia type 2 diabetes if we can get on the front end of that and many of you know the famous Nike curve of deterioration in glycemic control that occurs in type 2 diabetes, you get on the front end and you maintain all of these measures at a stable level, almost independent of the weight number you achieve. To me, that's part of our desire with metabolic health, which is to expand health span, not simply get the number possible.
A (Dr. Steensberg): And actually just want to build on this and also refer back to some of the presentations before as an industry and those of you who have been around for a long time know that we have been talking about preventive medicine when it comes to chronic diseases and many other diseases. It's an incredibly difficult thing to approach because society find it difficult to pay for it and patients often find it difficult to engage in it because the benefits are so far. Now we are looking at a category where patients, they receive immediate benefit in the weight loss, which we've also heard from Eric is what they see. So we are actually now in a situation for the first time where we can think about preventive early intervention and not just have it as an intellectual conversation, but a practical conversation because patients are ready to engage in those efforts as long as they fit into the aspirations of their life.
And that is why it's such an exciting moment right now and why we talk about this metabolic moment where for the first time, we actually have a practical solution to achieve what Utpal is talking about metabolic health, increasing metabolic lifespan.
Q (Mr. Callum, Barenberg): My question is around the petrelintide Phase 3 and you mentioned earlier, obviously, you need sort of 68 to 72 weeks to reach that nadir of weight loss. But given, I guess petrelintide weight loss and you're not trying to get to that 20 plus category is a more mild weight loss and probability of you guys being third to market. Is there a possibility of or maybe a shorter interim data readout in the face that you might be able to go to regulators with? And then the second question is probably quite early, so about pricing, but given your messaging around tolerability and the ability for patients to stay on drug. Do you think this gives you more flexibility around pricing compared to the GLP1 assets?
A (Dr. Steensberg): When you sit with what we consider a crown jewel, like petrelintide, you don't want to do shortcuts in development. That's why we designed the Phase 2 study the way we did with a 50-50 balance of males to females and not an 80% female, 20% males, where we don't learn a lot about a molecule in males. So this is about doing it right. If you truly have a crown jewel that can form the future foundation of weight management and be it kind of first choice, you have to do it right and that also means we should not do shortcuts in Phase 3. Having said that, we are, of course, hyper-focused on accelerating anything possible to get to market as early as possible, to provide this new potential solution for patients transformative solution. So -- and this is how we will continue to push this forward with maximum focus and acceleration, but also, life has taught most people, I think that shortcuts may feel nice short term, but long term they don't.
A (Dr. Kendall): And I'll add to that, I mean, it's sort of the think fast, think slow, meaning do as much as you can to bring these forward and do this as thoughtfully as possible of some of the happiest days of my current life are when Steve, Jonathon and Utpal joined. And I can share some of the interest. But I think the regulatory requirements for Phase 3 in obesity and the critical importance of demonstrating both safety and efficacy, not just tolerability and that's why I mentioned all three are part of the benefits of these extended programs, not solely the way they do year. Again, clinical trials represent clinical trials, not clinical reality. We hope to gather as much as possible. Then use Phase 3b once the Phase 3a submission is expedited as much as possible.
On OTR partnership
Q (Mr. Thomas Bowers, SEB): Just a question on the partnership you just announced this morning as well. So that platform very early-stage company. No, we'll disclose partnerships so far. So, how did you validate that platform going into small molecules? And then the second question is just on the whole talk about Lipton synthesizing. So I'm just wondering if there's any evidence for potentially types that maybe both a stronger Lipton synthesized fix than what you see in with the other amylins potentially?
A (Dr. Singh): I think on the OTR Therapeutics, we're really excited about the collaboration. I think if you look at their leadership expertise and the capabilities that they've built in very short order, as well as take a look at some of the support that they've had from the venture fund to raise their Series A. We're very confident that this is the right team to deliver on our ambitions in the small molecule space. You also take a look at what we have learned about converting peptides into small molecules. There are ways that the industry has now learned how to do that, and I think there are mechanisms now in place, and certainly OTR is going to be building on that.
On the pipeline
Q (Mr. Håkon Hemme Bro Jorgenson): You've previously shown financial discipline on the policy that grew tight and focused on the most promising assets. So, how do you navigate aiming for plus 10 clinical trial programs, which is quite an ambitious target? Why also keep critically assessing your pipeline assets? I just want your reflections on that?
A (Dr. Steensberg): I mean, of course, you need to take risks in the early phases. So I should take that risk. But we also clearly perceive the commercial opportunity. There was a clear differentiation in the market. And I think there's this approach, both looking at the science and the clinical data or the preclinical data, and then, of course, positioning your target up against a potential market opportunity. And there you need to constantly evaluate that opportunity because the market opportunity or the market as such also evolves. And then of course, we need to watch also competition and what is coming out to see if we have the right positioning.
Close Concerns’ Questions
- What explicit criteria will determine the multi-hormone combination pathways that are prioritized for future programs?
- How might the partnership with OTR Therapeutics align with the Metabolic Frontiers 2030 plan?
- Does Zealand intend to position its long-term weight maintenance medications as treatments to start on and use instead of Lilly and Novo Nordisk’s rapid and maximal weight loss medications?
- Will Zealand, as the company with “the most valuable pipeline in metabolic health,” look to address public health by helping people address people with T2D as well as people with obesity? What might be possible on preventing or delaying T2D?
- Even given that there is not a T2D indication, was CGM used in any part of the trial? If so, what did the CGM metrics show?
--by Elizabeth Rose, Nour Khachemoune, Monica Oxenreiter, and Kelly Close