ECO 2026 Day #4 Highlights –
Executive Highlights
- The 33rd European Congress on Obesity (ECO) continued in Istanbul on Friday – 4,500 attendees strong! Sessions spanned from new insights on therapeutic interventions CagriSema and semaglutide in adults aged 65 or older, obesity as a tool for cardiovascular risk reduction, and the neurobiology of hunger. See the conference website, agenda, and our day-by-day preview.
- Dr. Timothy Garvey (University of Alabama) discussed a post-hoc analysis of the REDEFINE 1 trial (n=3,417) that found no statistically significant difference in percent weight loss across different doses of CagriSema (Novo Nordisk’s combination medication). Of note, Dr. Garvey said that most CagriSema dose reductions were unlikely to be related to adverse events.
- Prof. Luca Busetto (University of Padua, Italy) presented a pooled analysis of the STEP trials to evaluate Novo Nordisk’s semaglutide vs. placebo in adults aged 65 years or older (older adults) with a BMI ≥30 kg/m2 or ≥27 kg/m2 with weight-related comorbidity, excluding T2D. Critically, there was no substantial difference in weight loss between older adults and the overall trial populations. However, improvements in BMI was more pronounced among older adults: 50% achieved normal or overweight status (up from a baseline of 10%), compared with 20% of the overall population (up from a baseline of 14%).
- Prof. Konstantinos Koskinas (Bern University Hospital, Switzerland) asked a practical clinical question: should obesity be part of cardiovascular risk calculators? He argued in favor of inclusion, emphasizing that obesity has broader cardiovascular effects than previously appreciated. Several newly published models that now incorporate obesity into heart failure risk prediction, including for individuals without known CVD, SMART2-HF for patients with established atherosclerotic disease, and LIFE-Preserved for patients with diagnosed HFpEF. The field has made meaningful progress, but more work is needed to refine risk prediction, extend assessment beyond 10-year projections, and develop more nuanced understanding of obesity-related phenotypes.
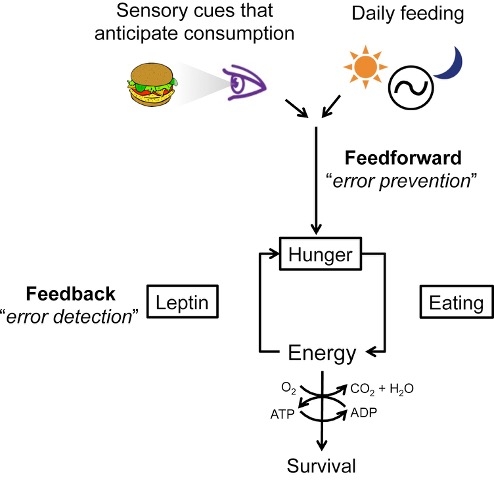
- Prof. Turgay Dalkara (Bilkent University, Ankara, Türkiye) delivered a neurobiological perspective on the translation of metabolic signals into motivation and behavior. He offered a mechanistic explanation for how modern environments can drive the emergence of obesity: appetite regulation is a product of cooperation between homeostatic signals, reward circuits, and cognitive control.
- In a grand closing ceremony, Dr. Jennifer Baker (Copenhagen University Hospital, Denmark), President-Elect of EASO, and Dr. Volkan Yumuk (Istanbul University, Türkiye), the organization’s current president, brought together representatives from partner organizations, including the European Coalition for People living with Obesity (ECPO) and national obesity associations.
- Prof. Dilek Yazici (Marmara University, Türkiye) said that nearly 5,000 in-person attendees from 100+ countries joined together this week in Istanbul to participate in ECO 2026. Next year’s Congress will be held in Munich, Germany, from May 18-21, 2027.
Table of Contents
- 1. Post-hoc analysis of the REDEFINE 1 trial shows no clear relationship between Novo Nordisk’s CagriSema dose and weight loss
- 2. Pooled analysis of STEP trials: Older adults aged 65+ years on Novo Nordisk’s semaglutide faced higher age-related adverse events, largely attributed to age rather than treatment
- 3. “Liking” and “wanting:” The neurobiology behind eating
- 4. Should obesity be included in cardiovascular risk factors? – Prof. Konstantinos Koskinas on obesity and CVD
- 5. Closing plenary: Awards given for research communication, reframing weight stigma as a modifiable risk factor
- 6. The 2025 Obesity Excellence Prize – more from the 2025 winner
1. Post-hoc analysis of the REDEFINE 1 trial shows no clear relationship between Novo Nordisk’s CagriSema dose and weight loss
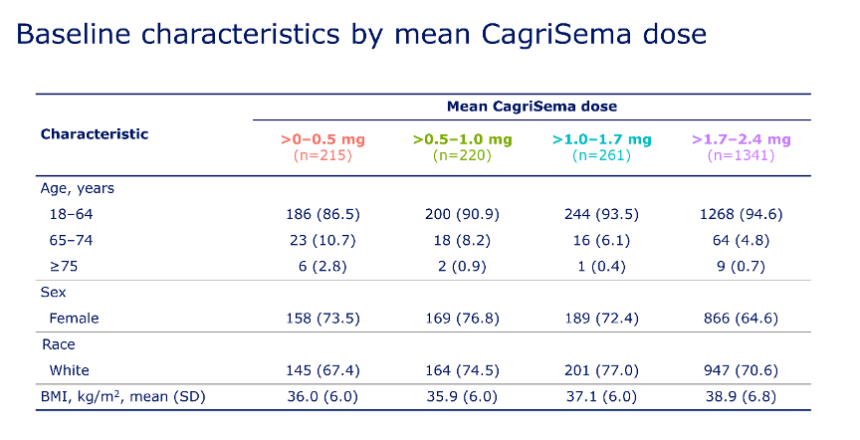
In this presentation, Dr. Timothy Garvey (University of Alabama) presented post-hoc analysis of the REDEFINE 1 trial (n=3,417) that examined the association between CagriSema dose and weight loss. In the trial, CagriSema (fixed combination of cagrilintide 2.4 mg and semaglutide 2.4 mg) conferred 23% weight loss at 68 weeks, compared with 16% with semaglutide, 12% with cagrilintide, and 2% with placebo. The trial employed flexible dose escalation, allowing patients to reduce doses and remain on a sub-maximal dose if they did not need further weight reduction or could not tolerate the medication. At the end of the study, 57% of participants on CagriSema were on the maximal dose of 2.4 mg, while the remaining were on unspecified sub-maximal doses. The post-hoc analysis aimed to further understand how the mean CagriSema maintenance dose (0-0.5 mg, 0.5-1.0 mg, 1.0-1.7 mg, and 1.7-2.4 mg) related to baseline characteristics, weight loss, and adverse events.
- At baseline, participants who were on submaximal doses tended to be older, female, and have lower BMI than those who reached higher maintenance doses (see figure below).
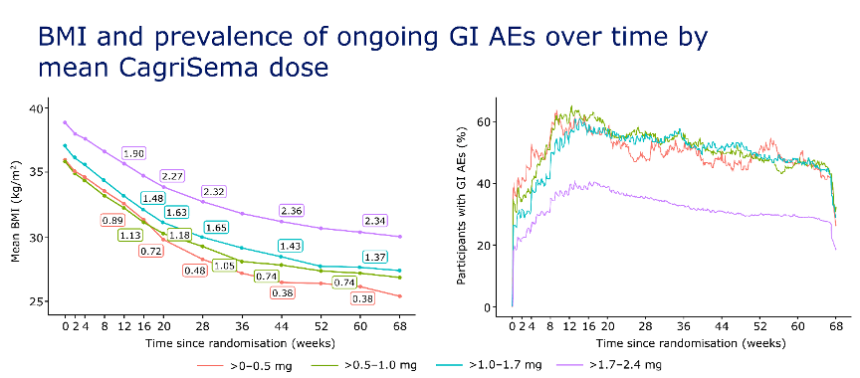
- There was no statistically significant difference in percent weight loss across mean CagriSema doses. At Week 68, participants who took 0-0.5 mg achieved 24% weight loss, those on 0.5-1.0 mg achieved 24%, those on 1.0-1.7 mg achieved 25%, and those on 1.7-2.4 mg achieved 23% weight loss. Consistent with baseline characteristics, BMI at Week 68 was higher for people on higher maintenance doses compared to those on lower doses; however, Dr. Garvey emphasized that percent weight reduction was the same across all groups. In terms of safety and tolerability, those on higher doses experienced fewer GI-related side effects (see figure below).
- Dr. Garvey argued that most CagriSema dose reductions were unlikely to be related to adverse events. When patients reduced their doses for the first time, they had already achieved significant weight loss: approximately one-third had achieved ≥10% weight loss, and one-fourth had achieved ≥20% weight loss. Moreover, most had no adverse events (24%) or experienced mild (46%) or moderate (26%) GI-related side effects. Hence, Dr. Garvey concluded that 24% of dose reductions were not related to GI tolerability, 31% were unlikely to be related, while 44% were possibly or probably related. Ultimately, these results show heterogeneity in people’s clinical needs and responses to treatments and support individual titration schemes.
2. Pooled analysis of STEP trials: Older adults aged 65+ years on Novo Nordisk’s semaglutide faced higher age-related adverse events, largely attributed to age rather than treatment
In this morning session, Prof. Luca Busetto (University of Padua, Italy) presented a pooled analysis of the STEP trials, which evaluated the efficacy and safety of Novo Nordisk’s semaglutide in people aged 65 years or older. Older people are more likely to have obesity-related complications, be frailer, and be more sensitive to adverse events. Given the limited evidence about GLP-1 RA use in older adults, investigators conducted a pooled analysis (n=358) of STEP 1, 3, 4, 5, 8, and 9 trials[1] to evaluate semaglutide vs. placebo in adults aged 65 years or older with a BMI ≥30 kg/m2 or ≥27 kg/m2 with weight-related comorbidity, excluding T2D.
- At baseline, participants were, on average, 69 years old, with 10% aged 75 or older. They were mostly female (72%) and white (86%). Clinically, participants had a mean body weight of 99 kg (218 lbs) and a BMI of 37 kg/m2, which were slightly lower than the overall STEP 1 population. However, older adults had greater clinical burdens, such as higher blood pressure of 134/79 mmHg (vs. 126/80 mmHg), hsCRP of 4.6 mg/L (vs. 3.9 mg/L), A1c of 5.8% (vs. 5.7%), and a higher proportion of those with prediabetes (48% vs. 44%).
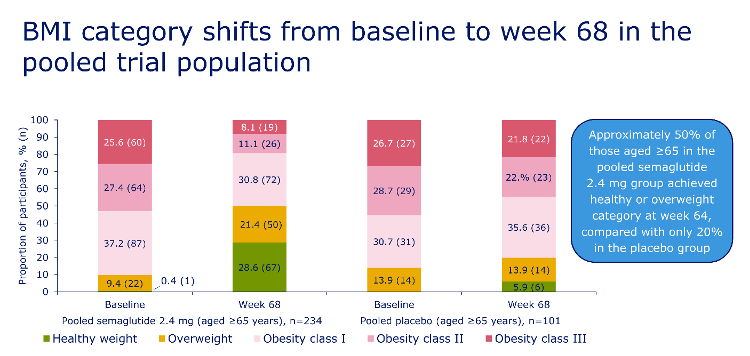
- There was no substantial difference in weight loss between older adults and the overall trial population. Both groups achieved 16% weight loss at Week 68, compared to 5.2% with placebo. The proportions of participants achieving ≥10%, ≥15%, and ≥20% weight loss were slightly lower among older adults but similar to those in the overall population (67% vs. 69%, 47% vs. 51%, and 29% vs. 32%, respectively). As shown in the figure below, the improvement in BMI was more pronounced among older adults: 50% achieved normal or overweight status (up from a baseline of 10%), compared with 20% of the overall population (up from a baseline of 14%). Semaglutide led to significant improvements in waist circumference, waist-to-height ratio, and cardiometabolic risk factors compared with placebo, consistent with the benefits seen in the overall population.
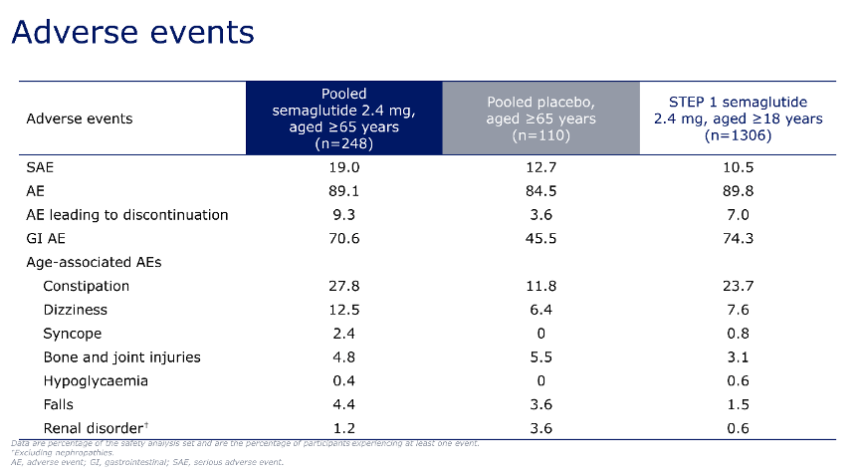
- On safety and tolerability, Prof. Busetto said that there was no statistically significant difference in the rates of adverse events (89% vs. 90%) between older adults and the overall population taking semaglutide. However, older adults were more likely to experience severe adverse events (19% vs. 11%). The most common adverse events were GI-related and did not differ between older adults and the overall population.
- Older adults were more likely to experience age-associated adverse events. For example, bone and joint injuries (4.8% vs. 3.1%), falls (4.4% vs. 1.5%), and hypoglycemia (0.4% vs. 0.6%) were more frequent in older adults than in the overall population taking semaglutide. However, Prof. Busetto noted that the rates of age-associated adverse events did not differ significantly between elderly patients treated with semaglutide or placebo. Hence, he said these adverse events may be more related to age rather than treatment.
3. “Liking” and “wanting:” The neurobiology behind eating
In an engaging morning session on the final day of ECO 2026, Prof. Turgay Dalkara (Bilkent University, Türkiye) delivered a neurobiological perspective on the translation of metabolic signals into motivation and behavior. He offered a mechanistic explanation for how modern environments can drive the emergence of obesity: appetite regulation is a product of cooperation between homeostatic signals, reward circuits, and cognitive control.
- Prof. Dalkara introduced the hypothalamus and brainstem as the foundation of homeostatic control, describing them as the signaling hub for multiple sensory systems. Specifically, the nucleus tractus solitarius (NTS) of the brainstem receives gut signals via the vagus nerve, while the arcuate nucleus (ARC) in the hypothalamus integrates hormonal cues, such as ghrelin, to stimulate hunger and leptin or insulin to signal satiety in regulating energy balance. Prof. Dalkara expanded on the ARC, noting that it lacks a blood-brain barrier, and therefore, it is better exposed to blood-borne hormones – like leptin, ghrelin, and insulin – or their agonists.
- Next, Prof. Dalkara introduced the concept of a core biological system in the hypothalamus, governed by two functionally opposing neuronal populations. AgRP/NPY neurons are activated during energy deficit and promote hunger and food-seeking behavior, whereas POMC neurons are generally associated with satiety and reduced food intake under conditions of sufficient energy availability. The relative concentrations of these populations act as a switch-like regulatory system, shifting the brain between hunger and satiety states.
- This circuit also operates through both fast synaptic and slower neuromodulatory signaling mechanisms. Fast amino acid neurotransmitters, like GABA, mediate rapid signaling inhibition and incur immediate changes in hunger-related circuit activity. Neuropeptides, including AgRP, NPY, and α-MSH, act more slowly as peptides linger in the extracellular space and confer sustained activity over extended periods. This hormonal architecture equips the system to flexibly coordinate acute food-related behaviors with metabolic state regulation.
- Prof. Dalkara turned from homeostatic hunger circuits to the brain’s reward architecture, explaining how metabolic signals are translated into motivation, reinforcement, and pleasure. Within the limbic system, distinct but interacting systems mediate “liking” and “wanting,” allowing food-related behavior to become uncoupled from actual energy needs. Hedonic pleasure, or “liking,” is generated through localized hotspots within structures such as the nucleus accumbens and ventral pallidum. “Hot” and “cold” hedonic spots within these structures drive “liking” and “disliking” responses, respectively. At the same time, dopamine projections from the ventral tegmental area encode “wanting,” the motivational drive to seek and consume rewarding stimuli. “Wanting” and “liking,” though interrelated, are mediated by independent systems. Stress, Prof. Dalkara noted, is one of the main drivers of this dopaminergic activation, which helps explain stress-related overeating.
- Lastly, Prof. Dalkara referenced a review published in Neuron, led by Dr. Mark Andermann (Harvard University), to demonstrate the way non-biological factors influence eating behaviors. The study found that, compared to rodents, humans showed greater cortical influence and a stronger susceptibility to external cues. Structured mealtimes were shown to replace physiological signals of hunger. Interestingly, even advertisements, culture, and social eating patterns independently amplified food intake. Further, neural plasticity embeds long-term vulnerability into biological feeding circuits. Prolonged fasting or dieting can induce synaptic and gene-expression changes in hypothalamic circuits, increasing hunger sensitivity and contributing to rebound eating and weight gain.
Source: Andermann and Lowel, Neuron (2017)
- Prof. Dalkara closed the session by describing the obesity epidemic as a mismatch between biological circuits, born from evolution, and the influences of modern environments. Homeostatic and reward systems are continuously engaged by abundant, highly palatable food and persistent external cues, which result in a compounding process: (i) dopamine-driven craving overrides satiety signals; (ii) learned and cultural behavioral patterns decouple intake from energy need; and (iii) plasticity stabilizes higher weight states over time.
4. Should obesity be included in cardiovascular risk factors? – Prof. Konstantinos Koskinas on obesity and CVD
In this Friday afternoon address, Prof. Konstantinos Koskinas (Bern University Hospital, Switzerland) discussed a practical clinical question: should obesity be part of cardiovascular risk calculators? Throughout his presentation, he argued that it should, emphasizing that obesity affects the cardiovascular system in more ways than previously appreciated. While obesity is often assumed to exert its effects primarily through atherosclerosis, Prof. Koskinas noted that its association may be even stronger with other cardiovascular conditions, particularly heart failure (HF). Specifically, he highlighted the close relationship between obesity and HF with preserved ejection fraction (HFpEF), noting that patients with HFpEF and obesity tend to face higher all-cause and cardiovascular mortality.
- Prof. Koskinas began by reviewing the European Society of Cardiology’s updated dyslipidemia guidelines, which use SCORE2 and SCORE2-OP algorithms to estimate 10-year risk of cardiovascular events based on age, sex, non-HDL cholesterol, and systolic blood pressure. While obesity is not directly included in the SCORE2 formula, he suggested that the updated guidelines recommend considering additional “risk modifiers” – particularly for primary prevention in patients at moderate risk or near treatment thresholds. Among these modifiers, Prof. Koskinas presented obesity as a particularly important factor that can support a patient’s risk reclassification.
- Clinically, Prof. Koskinas described two patients with identical SCORE2 profiles, one of whom had a normal BMI, while the other had obesity (BMI 31 kg/m2). Although both patients would fall into the same moderate-risk category with the SCORE2 and SCORE2-OP algorithms, he asserted that they should not be managed identically. Reclassifying the patient with obesity into a higher-risk category would strengthen recommendations for lipid-lowering therapy. Specifically, this intervention would lower their LDL-cholesterol target to below 1.8 mmol/L (from 2.6 mmol/L). In this way, Prof. Koskinas demonstrated how recognition of obesity could directly affect treatment decisions.
- Later, Prof. Koskinas shifted his focus to HF, arguing that obesity’s role is especially impactful and historically underrecognized in the cardiovascular complication. He highlighted several newly published models that now incorporate obesity into heart failure risk prediction, including SCORE2-HF for individuals without known CVD, SMART2-HF for patients with established atherosclerotic disease, and LIFE-Preserved for patients with diagnosed HFpEF. Across these algorithms, BMI was included among the predictors of future HF risk or HF-related outcomes, reinforcing Prof. Koskinas’s key argument that obesity should be more integrated into cardiovascular risk assessment.
- Prof. Koskinas emphasized that obesity is strongly associated with arrhythmias, particularly atrial fibrillation. He noted that obesity increases the risk of incident atrial fibrillation and is also associated with progression from acute, temporary episodes to chronic disease. He concluded that while the field has made meaningful progress, more work is needed to refine risk prediction, extend assessment beyond 10-year projections, and develop more nuanced understanding of obesity-based phenotypes.
5. Closing plenary: Awards given for research communication, reframing weight stigma as a modifiable risk factor
Led by Dr. Jennifer Baker (Copenhagen University Hospital, Copenhagen, Denmark), President-Elect of EASO, and Dr. Volkan Yumuk (Istanbul University, Türkiye), the organization’s current president, the closing ceremony brought together representatives from partner organizations, including the European Coalition for People Living with Obesity and national obesity associations. The speakers emphasized the importance of interdisciplinary collaboration, professional networks, and patient partnerships in advancing obesity prevention, treatment, and long-term management. The organizers also reflected on the congress’s global reach, noting participation from nearly 5,000 delegates representing approximately 100 countries, underscoring the increasingly international scope of obesity science and policy engagement.
- The closing ceremony recognized several early-career researchers whose work extended beyond conventional academic dissemination to include public engagement, advocacy, and science communication. The ECO 2026 Prize for Engagement and Science Communication was awarded to Dr. Pablo Jiménez López (University of Almeria, Spain) for his efforts to communicate research on nanoplastic exposure, impaired glucose tolerance, and adiposity in mice to broader public audiences. Meanwhile, the ECO 2026 Prize for Advocacy, Impact, and Innovation was presented to Dr. Nour Baratli (Luxembourg Institute of Health, Luxembourg), whose research examined the physical health consequences of weight bias and stigma among adults living with obesity. Her project was recognized for reframing weight stigma as a modifiable social determinant of health and for its potential implications for policy, clinical care pathways, and respectful communication practices.
6. The 2025 Obesity Excellence Prize – more from the 2025 winner
In a session that paralleled the opening ceremony, Prof. Antje Korner (Helmholtz Institute, Germany), recipient of last year’s Obesity Excellence Prize awarded by the Novo Nordisk Foundation (NNF), was introduced as a leading pediatrician-scientist whose work integrates metabolic research with clinical innovation in childhood obesity. Her recent work, which she said was made possible by the grant from NNF, concerns the identification of rare variants in the ASIP gene and their contribution to severe early-onset obesity. Her team’s findings suggest that dysregulation of melanocortin signaling pathways may extend beyond previously established genetic mechanisms. By implicating ASIP in pediatric obesity phenotypes, Prof. Korner provided evidence that obesity is a biologically heterogeneous and genetically mediated disease rather than solely a consequence of environmental or behavioral factors. Importantly, the work carries translational significance because it may help refine molecular classifications of obesity and identify patients who could benefit from targeted therapies acting on the melanocortin system.
-- Milenka Men, Elizabeth Rose, Kat Moon, Esther Min, Monica Oxenreiter, and Kelly Close
[1] As background, STEP 1 trial (n=1,961) tested semaglutide 2.4 mg with lifestyle intervention in adults with obesity or overweight but not diabetes. STEP 3 (n=611) evaluated semaglutide with intensive behavioral therapy in adults with obesity or overweight but not diabetes. STEP 4 (n=902) assessed the effects of discontinuing semaglutide. STEP 5 (n=304) examined two-year efficacy and safety in the same population. STEP 8 (n=338) compared semaglutide to liraglutide. STEP 9 (n=407) evaluated semaglutide in adults with obesity, knee osteoarthritis, and knee pain.