EASD 2025 Day #5 Highlights –
Executive Highlights
- The conclusion of EASD 2025 was filled with no less enthusiasm and insight than any of the previous days. On Day #5, we were so inspired by Dr. Viswanathan Mohan, who received the EASD Diabetes Global Impact Prize for his “outstanding contribution to diabetes research and prevention and his transformation of medical practice, not only in India but worldwide.” His impressive career has spanned work in digital diabetes delivery, epidemiology, education, rural practice, and charity. At Close Concerns, we’ve had the privilege of visiting Dr. Mohan in India and have been incredibly impressed by how his team of health workers has achieved A1cs similar to the United States in remote, disadvantaged areas.
- In therapy, a multitude of exciting T1D data were presented, along with work towards innovative combination therapies.
- Prof. Chantal Mathieu (KU Leuven, Belgium) presented full results of the phase 2 MELD-ATG trial (n=117), which evaluated anti-thymocyte globulin (ATG) on beta cell preservation in young people (5-25 years) newly diagnosed with stage 1 T1D. The study confirmed the efficacy of ATG on beta cell function preservation and established an effective minimum low dose (0.5 mg/kg) in a pediatric and young adult European cohort.
- In combination therapy, Dr. Hertzel Gerstein (McMaster University & Hamilton Health Sciences, Canada) reviewed meta-analyses of cardiovascular (CV) outcome trials. SGLT-2 inhibitors and GLP-1 RAs confer substantial CV and kidney benefits. Work to decode the precise mechanisms behind this remains ongoing. “Explanations are evanescent. Observations are robust,” he said, encouraging the use of combination therapy even as work continues to uncover precise mechanisms.
- In tech, we continued to learn about insightful clinical suggestions for AID and CGM use, from missed meal announcements to GDM.
- Dr. Salvatore Scirè Calabrisotto (University of Catania, Italy) presented a randomized crossover study (n=20) evaluating the response of hybrid closed-loop AID systems to unannounced meals. He said that PID-based algorithms (MiniMed 780G) appear to handle unannounced meals slightly better than MPC-based algorithms (Control-IQ), regardless of meal type.
- Gestational diabetes mellitus (GDM) was a huge focus in a highly-discussed symposium on CGM and pregnancy. Prof. Tina Linder (Medical University of Vienna, Austria), Prof. Christian Göbl (Medical University of Vienna, Austria), and Prof. Helen Murphy (University of East Anglia, the UK) explored recent data on CGM use in gestational diabetes, comparing findings from the GRACE and DipGluMo studies to explore the potential for CGM to improve both maternal glycemic management and neonatal outcomes. The sky is the limit, here, dear readers, both for recognizing gestational diabetes earlier and for treating it better.
Resource Hub | Day-by-Day Preview | Conference Website | Registration
In case you missed it, see our previous coverage of EASD 2025.
- EASD 2025 Day #1 Highlights - Nine industry symposia highlight dual glucose-ketone monitoring, new CGM features, cardiometabolic comorbidities, incretin-based therapies, and SGLT-2 inhibitors.
- EASD 2025 Day #2 Highlights - Presidential Address by Prof. Chantal Mathieu; AID outcomes with three-year RWE from MiniMed 780G and Tandem’s INRANGE results; Rybelsus in T2D, ASCVD, and CKD; incretins in T1D
- EASD 2025 Day #3 Highlights - CGM regulation in the EU and a new tech competencyframework; orforglipron, CagriSema, tirzepatide, amycretin, and NA-931 trial readouts; Albert Renold and Camillo Golgi Prize lectures
- EASD 2025 Day #4 Highlights - Full phase 3 SURPASS-CVOT results; REACH real world data; smart MDI systems by the numbers; Dr. Steven Kahn and Prof. Roy Taylor on T2D remission
Table of Contents
-
Big Picture
- 1. EASD Diabetes Global Impact Prize Lecture
- 2. Rethinking A1c: Genetics, aging, and CGM differences challenge the “one-size-fits-all”
- 3. C-peptide measurements to improve classifications of diabetes in routine clinical practice
- 4. Significant increases in dementia-related mortality in people with diabetes compared to those without
- 5. New insights into persistent and increasing burdens of diabetes morbidity
-
Therapy
- 6. Prespecified analysis of phase 2 CONFIDENCE trial: simultaneous use of finerenone (Bayer’s Karendia) and empagliflozin (BI/Lilly’s Jardiance) prompted far better outcomes while addition of GLP-1 yielded nothing additional
- 7. New paths for old friends: Potential new roles for GLP-1 RAs and SGLT-2 inhibitors
- 8. INNODIA’s phase 2 MELD-ATG trial finds low-dose ATG significantly preserves C-peptide levels in young individuals with new-onset T1D
- 9. In Ver-A-T1D trial, verapamil confers non-statistically significant preservation in C-peptide in new-onset T1D
- 10. “There's no insulin like your own”: Two-year outcomes of the BANDIT trial demonstrate JAK inhibitor baricitinib preserves C-peptide
- 11. Do we need really need a large outcome trial to prove the cardiorenal benefits of SGLT-2 inhibitor and GLP-1 RA combination use?
- 12. Benefits and challenges of AI-assisted screening for diabetic retinopathy and an overview of the eye health treatment landscape
-
Tech
- 13. GRACE and DipGluMo show the huge power of CGM’s role in GDM management
- 14. MiniMed 780G vs. Control-IQ: Handling unannounced meal in adolescents with T1D
- 15. New insights in glycemic management: Sleep duration, pregnancy, and a head-to-head comparison of three CGMs during exercise
- 16. *NEW* CGM as a routine for T2D: Evidence from RCTs, real-world data, and case studies
- 17. *NEW* Nationwide French data highlight durability and glycemic gains associated with AID use
- 18. *NEW* CamAPS FX and Control-IQ improve glycemia and neonatal outcomes vs. MiniMed 780G in pregnant women with T1D; strong outcomes across all systems
Big Picture
1. EASD Diabetes Global Impact Prize Lecture
The EASD Diabetes Global Impact Prize was today awarded to Dr. Viswanathan Mohan or “Mohan” for his “outstanding contribution to diabetes research and prevention, and his transformation of medical practice, not only in India but worldwide.” It is awarded to individuals who have made contributions to clinical or translational work on a global scale, impacting the lives of people with diabetes in resource constrained settings. There could hardly be a more fitting first recipient than Dr. Mohan, who was specifically cited for his efforts to “gain more knowledge on the etiology of diabetes that occur in populations worldwide.” The prize is supported by Lilly.
It was a great privilege to attend the award lecture by Dr. Mohan, who is a visionary and entrepreneur who has helped thousands of clinicians and millions of people with diabetes, starting in his home country of India. Dr. Mohan has published over 1,700 papers and has nearly 250,000 citations – one of the most cited diabetes researchers ever. He also has well over a million followers on social media. And, he will always slow down to be in touch with those who want to understand diabetes btter.
At Close Concerns, we’ve had the privilege of visiting Dr. Mohan in India multiple times over the last 20 years and have been incredibly impressed by how his team of health workers has achieved A1cs similar to the United States at scale in remote rural villages that possess minimal resources. While Time in Range is not measured for poor patients, we suspect they are doing far better than many people in the US, one of the highest-resourced countries.
Standing ovation! Dr. Mohan spoke for nearly an hour and only had time to begin to touch on some the highlights of his life’s work. At the conclusion of his lecture, there was not a single person seated in the large Paris Halle that we could see.
- Dr. Mohan started by describing how, as a young man, he followed in his father’s footsteps as a doctor, beginning to research diabetes in the garage of his father’s practice, while still a medical student. Between 1971 and 1991, he helped his father build the first diabetes hospital and diabetes research center in India.
- In 1991, with his late wife, Dr. Rema Mohan, he established a specialist diabetes hospital, ‘Dr. Mohan’s Diabetes Specialities Centre” (DMDSC) which was the foundation of his enormous impact and legacy. Today, DMDSC has 50 branches in 32 cities, a staff of >1,400 with over 130 diabetes doctors and serves 700,000 registered people with diabetes. The concept is ‘total diabetes care’ – every test or treatment that might be needed is available in the building and all check-ups can be completed within six hours.

Today, his current group of diabetes institutions can be described into four key parts – clinical care, research, education and training and charity. Each have had tremendous impact in India (and abroad), and he described them all during the course of this inspirational lecture, which we recommend reviewing in full.
Here are some of the (many) highlights:
- Digital Diabetes Delivery: Dr. Mohan’s team have created three applications: (i) “DIA”, an AI chatbot to help patients with diabetes questions; (ii) “DiaLA”, a super-useful mobile app to help with appointments, health tracking, prescriptions, medical records, CGM data; and (iii) “DiaNA”, a precision medicine tool to predict risk, classify T2D subgroups and recommend treatments.
- Epidemiology: Starting in Chennai with a urban population study (CUPS, n=1,399), Dr. Mohan and his team expanded to an urban/rural study (n=26,000) and then to a pan-India study (n=121,081), which was painstakingly sampled to be totally representative of the country. These incredible studies screened for diabetes, developed risk scores, published the first data on prevalence of complications, obtained data on metabolic markers, profiled diet and physical activity, and developed numerous interventions and recommendations. One important insight was the development of the “South Asian Phenotype,” which describes a person with propensity to develop T2D at a much younger age and lower BMI than White Europeans. Although genetic differences are important, a high carb diet (>65% of calories) was associated with risk. Dr. Mohan stated “[A high carb intake] is why we have a diabetes epidemic in India.”
- Education: Dr. Mohan’s Diabetes Education Academy has trained over 500 doctors in diabetes, that have collectively treated over 1.5 million people with diabetes. To scale faster, he created a distance learning program that has now trained over 19,000 doctors, who have benefitted 18.8 million people with diabetes. The program is now being offered free to neighboring countries. There is a similar program for diabetes educators, with nearly 29,000 trained to date.
- Rural Practices: 65% of India’s population lives in poor rural areas, whereas 74% of doctors practice in urban areas. In addition to poverty, rural areas have low literacy rates, low awareness of diabetes, and problems with access. Starting in one village, Chunampet, in 2006, Dr. Mohan created a model for rural care. He trained local villagers as health workers who could screen the entire population. Those with diabetes were treated in a mobile ‘telediabetology’ van (with a huge satellite dish bolted to the roof!). In three years, they screened 23,380 people, treated 1,138 people with diabetes, and achieved good control with low-cost drugs. This served as a model for expansion. Dr. Mohan cited the ‘snowball effect’ for his success: “Start small, never start big, expand whatever works well.”
- Charity: In India, only people below the poverty line receive any government healthcare funding. 70% of Indians therefore pay out of pocket for medical care. Often they can’t even afford insulin. Dr. Mohan’s charity, DIRECT, currently provides lifelong free treatment for >15,000 patients. The charity also supports free diabetes clinics and mobile hospitals, free diabetes camps (25,000 to date), free screening for diabetes (5m screened to date) and large public awareness programs.
Dr. Mohan closed by quoting an Indian scientist, Prof. J. C. Bose, who said, “When one dedicates himself (herself) wholly for a great object (cause), the closed doors shall open and the seemingly impossible will become possible for him (her).” He thanked his doctors, saying, “While I am standing here giving my talk, these people are doing the work, seeing patients six days a week .. it’s not easy…so this is for them.” Bravo.
2. Rethinking A1c: Genetics, aging, and CGM differences challenge the “one-size-fits-all”
Prof. Inês Barroso (University of Exeter Medical School, UK), Prof. Astrid Petersmann (University Medicine Oldenburg, Germany), and Prof. Guido Freckmann (Institute of Diabetes Technology GmbH, Germany) explored why the field should move beyond A1c levels alone. Their talks highlighted the influence of genetics, age, and emerging CGM metrics, which in conjunction warrant the refinement of current A1c thresholds for more equitable and accurate diagnosis that is applicable to diverse populations.
- Genetic variation can bias A1c readings, delaying diagnosis in high-risk groups. Prof. Barroso showed how non-glycemic factors, including ancestry, sex, and genetic variants, can substantially alter A1c values for a given glucose level. She pointed to G6PD deficiency (prevalent in one-in-seven Black men and 1-in-63 Asian men in the UK), which results in shorter red blood cell lifespan and produces A1c values approximately 10 mmol (~3.1%) lower than expected. Notably, this generates a four-year average delay in diabetes diagnosis in these groups, compounding already elevated risks for T2D and complications. PIEZO1 variants seen in South Asians also modestly lower A1c levels without improving glycemic management, though their impact on diagnosis and complications is less well defined. Prof. Barroso cautioned that reliance on A1c metrics alone risks systematic underdiagnosis and undertreatment in these affected populations, with downstream increases in the prevalence of microvascular complications like retinopathy. She proposed that genotype-adjusted A1c thresholds could be considered for variants with large effects, such as G6PD deficiency, though broader implementation would remain challenging.
- Age-related increases in A1c may also require revised diagnostic cut-offs. Prof. Petersmann presented evidence from large population studies, including the Framingham Offspring Study (n=2,473), SIGT (n=1,573), and German SHIP cohorts (n=2,973). These showed consistent age-related A1c increases in people without diabetes by approximately 0.07-0.09% per decade. While the analytic precision of A1c measurement has improved significantly in recent decades, she emphasized that the “one-size-fits-all” diagnostic limits fail to account for physiologic age effects. Prof. Petersmann called for robust population-based reference data, stratified by age, that could refine diagnostic cut-offs.
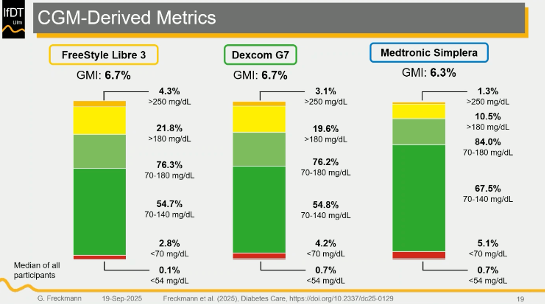
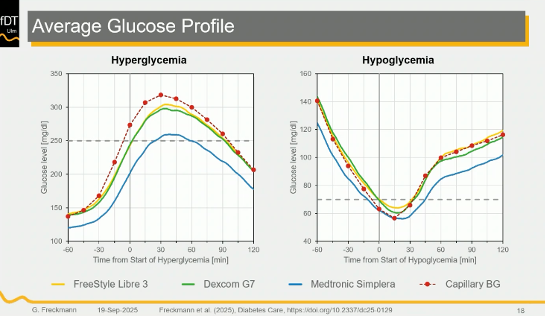
- CGM integration could complement A1c measures but requires standardization. Prof. Freckmann argued that while A1c remains a valuable standardized tool, it fails to determine short-term variability and transient hyperglycemia. With over 80% of people with T1D and a growing number of T2D patients now using CGM, real-world data offer opportunities to complement A1c with metrics such as TIR and GMI. However, he cautioned that CGM is currently designed for therapy, rather than diagnosis, and lacks international standardization, with different devices yielding systematically different results, as shown below. Early consensus efforts by IFCC and EASD working groups are currently underway to establish uniform CGM-derived metrics for potential diagnostic use. Prof. Freckmann concluded that while A1c will remain irreplaceable, pairing it with standardized CGM outputs could potentially provide a more individualized and accurate diagnostic framework.
3. C-peptide measurements to improve classifications of diabetes in routine clinical practice
Closing out one of the last sessions of EASD, Prof. Andy Jones (University of Exeter, UK) and Prof. Mark Strachan (Western General Hospital, UK) spoke on classifications of diabetes in adults in routine clinical practice. Both panelists highlighted the challenges of diabetes classification and the risks that come with misdiagnosis. They emphasized the importance of integrating better criteria for diagnosis, including C-peptide levels.
- Prof. Jones on overcoming diagnostic challenges of T1D and T2D. Differences in glycemic treatment requirements depend on endogenous insulin production, as T1D refers to absolute insulin deficiency and T2D relates to relative insulin deficiency. However, clinical features like onset of diabetes, ketone levels, and BMI do not clearly discriminate between T1D and T2D at diagnosis. Among many characteristics, the age of diagnosis serves as the strongest clinical indicator of diabetes subtype. Prof. Jones explained that the strong association between age and T2D risk indicates that the vast majority of new-onset diabetes in older adults is T2D. T1D diagnosis in older adults remains challenging because 95% of T1D cases include an onset at the age of 15, with any associated features and predictive value >96%. On the other hand, 1% of T1D cases have an onset at the age of 65 with no single feature that makes T1D diagnosis likely, along with a predictive value >7%.
- Prof. Jones reminded that islet autoantibodies provide the most utility to diabetes diagnosis and serve as a reliable predictor of future progress or decline in endogenous insulin. In comparison, C-peptide levels show most utility in longstanding diabetes but remain a poor predictor of future diagnosis. Therefore, islet autoantibodies have a weak relationship to current treatment requirements, while C-peptide levels are better for clinical use in diabetes management and intervention.
- Due to challenges in diabetes diagnosis, patients face misclassification of diabetes in older adults. In a study, 58% of adults in the UK with T1D who tested negative for autoantibodies were confirmed to have T2D through C-peptide and genetic testing. Furthermore, studies have shown that the presence of positive islet autoantibodies does not always confirm a diabetes diagnosis. Therefore, Prof. Jones encouraged the implementation of international guidelines that advise routine testing, especially among adults with suspected T1D. Furthermore, he urged the audience to consider other diagnostic criteria, as negative islet autoantibodies do not exclude T1D.
- Prof. Strachan on routine biomarker assessments in diabetes management. Prof. Strachan and his team have implemented a diagnostic algorithm to help increase the classification and diagnosis of T1D. The algorithm included three components, including: (i) C-peptide levels; (ii) autoantibody testing; and (iii) genetic testing. By integrating the structured algorithm into clinical care, the study detected 114 patients with C-peptide levels >200 pmol/L, among 859 participants tested. Additionally, 54 patients met the criteria for T1D diagnosis. Furthermore, 58 people were reclassified, including 44 people as T2D and 14 with monogenic diabetes. Prof. Strachan commented that a 7% reclassification rate reflects the challenges of diagnostic criteria and encouraged the use of C-peptide levels for better diagnosis and cost efficiency.
- Prof. Strachan highlighted the national program of diagnostic biomarker testing in T1D in Scotland. In 2021, Scotland became the first country to offer C-peptide blood tests to improve diagnostic accuracy. Scotland currently has 37,124 people with T1D diagnosis, and about 45% of this population has had a C-peptide measurement. However, Prof. Strachan commented that the implementation of this biomarker testing has significant geographic variation, especially as it depends on individual decision of HCPs. Therefore, he encouraged HCPs to increase awareness and uptake of C-peptide measurements.
4. Significant increases in dementia-related mortality in people with diabetes compared to those without
In a session focused on the intersection of cognitive dysfunction and diabetes, Prof. Kanika Mehta (Baker Heart and Diabetes Institute, Australia) presented findings from a population-based analysis on age-specific trends in mortality from dementia among people with and without diabetes. Alongside the increasing prevalence of diabetes and related complications, there has also been the emergence of dementia and mortality rates. In fact, some countries with high dementia rates among people with diabetes compared to those without have reported an increase in diabetes-associated mortality rates. To further investigate the relationship between dementia and diabetes, a study focused on whether mortality rates from diabetes-associated dementia differ by age and sex. Overall findings showed that dementia has generally increased at older ages, with a more significant rise among people with diabetes.
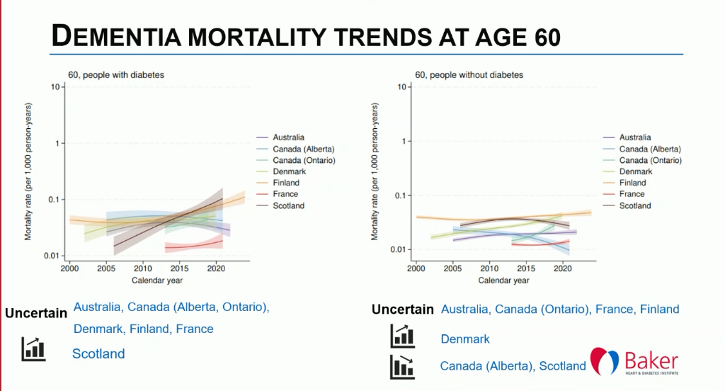
- Methods. The study used mortality data from registries from seven jurisdictions, including Australia, Denmark, Finland, France, Scotland, and Alberta and Ontario from Canada. The follow-up period was approximately 20 years. Data included mortality rates and ratios for women and men aged 60-90 years, with dementia as the underlying cause of death.
- Results. The study analyzed a total of 114,559 and 589,706 deaths related to dementia for people with and without diabetes, respectively. The trends in mortality from dementia varied across age groups but were relatively consistent for both men and women. Among ages 60 and 70, up to three jurisdictions showed increasing rates of mortality related to dementia, while others demonstrated unclear trends. At ages 80 and 90, up to six jurisdictions showed an increase in mortality rates for both people with and without diabetes, but the rates were more pronounced in those with diabetes. In Scotland, particularly, dementia in people with diabetes consistently increased, from 36% to 51% for women and 38% to 46% for men.
5. New insights into persistent and increasing burdens of diabetes morbidity
In the final session of EASD 2025, Prof. Edward Gregg (RCSI University of Medicine and Health Sciences, Ireland) outlined the changing landscape of diabetes complications, showing how multimorbidity persists and highlighting the need to move beyond single-complication research. Professor Gregg was previously at CDC in the US and we were absolutely thrilled that attendees could hear him speak.
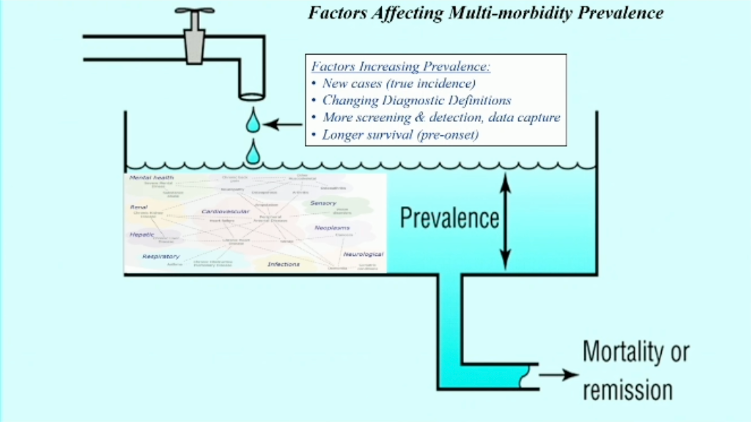
- Prof. Gregg began that diabetes confers a two-to-three times higher risks of multiple long-term conditions.These include traditional high-risk complications including chronic kidney disease and coronary heart disease (and also easier to manage ones, like hypertension), as well as more common lower-risk conditions that involve metabolic, vascular, respiratory, aging or fragility, and mental health. While CVD mortality has sharply fallen through the decades, mortality rates from other causes have not. He also pointed out that older adults have experienced disproportionately high mortality reductions, while younger individuals have face sharper increases in rising obesity, earlier onset T2D, and increasing complications – contributing to the persistence or increase of multimorbidity. Dr. Gregg’s analysis underscores the need for new metrics which account for multimorbidity, rather than considering complications as an isolated incident.
Therapy
6. Prespecified analysis of phase 2 CONFIDENCE trial: simultaneous use of finerenone (Bayer’s Karendia) and empagliflozin (BI/Lilly’s Jardiance) prompted far better outcomes while addition of GLP-1 yielded nothing additional
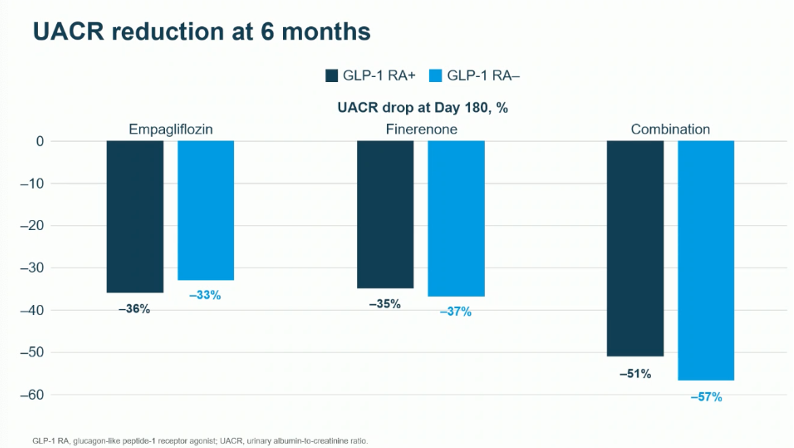
In this morning session, Dr. Rajiv Agarwal (Indiana University) presented results from a post-hoc analysis (n=182) of the CONFIDENCE trial, on the (n=800). The results were simultaneously published today in Diabetes Care. As a reminder, the trial found that simultaneous use of finerenone and empagliflozin reduced urinary albumin-to-creatinine ratio (UACR) by 52% at Day 180, conferring 29% and 32% greater relative reductions in UACR, compared to finerenone or empagliflozin alone, respectively – this is fantastic!. This prespecified analysis investigated whether the efficacy and safety of the combination therapy were affected by baseline GLP-1 RA use. We were a bit surprised about this – yet and still, we certainly think there is at least a bit of complexity with the better-known classes, specifically incretins. Titration, for example, continues to be extremely challenging for GLP-1 and for some (but at least they know it right away!) So perhaps it is better that better outcomes were not seen, since adding a third agent may have been very complicated. On a positive note, while SGLT-2 inhibitors are a bit hard to take due to emergence of UTIs, patients taking them understand very well where things are headed. By contrast, the side effect profile for Kerendia appears positively benign – so, getting to combination therapy with BI/Lilly’s Jardiance shouldn’t be hard at all and it yields a far better results. We love that this is an “oral combo” as well – yet another reason to prove to people how positive it is to be very proactive to look out for kidneys. Ultimately, we hear so many positives about how easy it is to both prescribe and take and we feel that the more people with diabetes at high risk of kidney disease will be over the moon at how easy it is to be proactive. Ultimately, we will say that so many negatives often pop up with titration with GLP-1 that we wouldn’t mind seeing clear assessment of how easy titration actually was. All this is our understanding seeing only a bit of the data and we look very forward to learning more from the scholars.
- Baseline characteristics. The analysis included 182 participants who were on a GLP-1 RAs at baseline. Dr. Agarwal highlighted the differences across baseline characteristics, with GLP-1 RA users having higher BMI compared to nonusers (32 kg versus 27 kg), higher insulin use (59% versus 34%), higher statin use (87% versus 71%), and lower DPP-4 inhibitor use (4% versus 41%).
- Results. At Day 180, in the combination therapy group, UACR in patients on GLP-1 RAs was reduced by 51% compared to 57% in those not using GLP-1 RAs. For participants receiving finerenone monotherapy, there was a 35 % reduction in GLP-1 RAs users versus 37% in nonusers. For participants using empagliflozin alone, GLP-1 RA users had 36% reduction in UACR versus 33% in nonusers. eGFR changes were consistent across groups, as well. In safety results, the incidence rate of hyperkalemia was 9% in GLP-1 RA users and 9.5% in nonusers. Overall, the analysis found that GLP-1 RA use at baseline does not compromise efficacy or safety, supporting the use of triple therapy in appropriate patients. Ultimately, this was a fairly small trial and we do wonder what might be seen in a far bigger group – we know, of course, from Novo Nordisk’s very exciting FLOW trial that GLP-1 solo did very well in this trial! That said, given tolerability and ease of use – while we imagine most patients would go with two orals any day compared to an incretin, Richard Wood’s dQ&A group is really the one to answer that! dQ&A has thousands of paitents in the US, Canada, and in seven European countries and they sure can give you their opinions – some of them have answered every single quarterly survey sent to them since 2009!
7. New paths for old friends: Potential new roles for GLP-1 RAs and SGLT-2 inhibitors
The final day of EASD 2025 featured an innovative, forward-looking symposium on potential new uses for GLP-1 RAs and SGLT-2 inhibitors. Prof. Martin Heni (University Hospital Ulm, Germany) offered evidence for the complex neurological benefits of these therapies. We heard more about some of the most exciting possibilities we could imagine, such as the fact that SGLT-2 inhibitors have demonstrated promise for restoring insulin sensitivity specifically to the brain, while GLP-1 RAs may be the next frontier for the treatment of alcohol use disorder (AUD).
- Prof. Heni began by encouraging the audience to dive deeper into the idea of “mind over metabolism” and its relevance for SGLT-2 inhibitors. It is known that these therapies function by interfering with the sodium-glucose transport process in the kidneys, resulting in glucose being excreted from the body in urine. With this caloric loss comes weight loss. He cited a number of studies that have demonstrated weight loss with the use of SGLT-2 inhibitors until approximately 28 weeks of treatment, when weight plateaus.
- Prof. Heni raised the question of why this occurs and explored the hypothesis that the brain may be involved in this process. As demonstrated by Sawada et al., the effect of SGLT-2 inhibition on weight loss is partly mediated by liver-brain-adipose neurocircuitry, and 2022 studies by Ruiten et al. were the first to show that dapagliflozin specifically causes an increase in activity in the right amygdala and right caudate nucleus, areas of the brain that are important for metabolism, eating behaviors, and cognitive function. These areas are also insulin sensitive. Prof. Heni then explored if SGLT-2 inhibitors may act on these areas of the brain to improve insulin sensitivity.
- While SGLT-2 inhibitors did not have an effect on whole-body insulin sensitivity, the therapeutic class has demonstrated improvements to insulin responsiveness in the brain. A 2022 study demonstrated no difference in whole body insulin sensitivity between patients taking empagliflozin versus placebo (p=0.8). However, in a study using intranasal insulin to affect the brain directly (n=40), empagliflozin has been found to restore hypothalamic insulin responsiveness in prediabetes with eight weeks of treatment (absolute change in CBF mL/100 g/min, p=0.04 for empagliflozin before and after treatment versus 0.2 for placebo). As this budding area of research continues to develop, Prof. Heni posits that SGLT-2 inhibitors may be used in the future to restore brain hypothalamic insulin sensitivity and improve systemic metabolism. Future work will continue to explore this therapeutic area, as well as promising work suggesting benefits of SGLT-2 inhibitors for protection against dementia.
8. INNODIA’s phase 2 MELD-ATG trial finds low-dose ATG significantly preserves C-peptide levels in young individuals with new-onset T1D
In this early morning session, Prof. Chantal Mathieu (KU Leuven, Belgium) presented full results of the phase 2 MELD-ATG trial (n=117), which evaluated anti-thymocyte globulin (ATG) on beta cell preservation in young people (5-25 years) newly diagnosed with stage 1 T1D. The results were simultaneously published in The Lancet. As background, ATG suppress immune T cells and are a potent immunosuppressant used for organ transplantation since the 1960s. TrialNet’s previous phase 2 study(n=89) found that low dose of ATG (~2.5 mg/kg vs. 9-12 mg/kg used for transplantation) may slow beta cell loss in new-onset T1D but also produced cytokine release syndrome (CRS; 48% vs. none) and serum sickness (72% vs. none) in participants. The MELT-ATG study aimed to answer if an even lower dose (0.5 mg/kg) may retain efficacy with an improved safety profile. Ultimately, the study confirmed the efficacy of ATG on beta cell function preservation and established an effective minimum low dose (0.5 mg/kg) in a pediatric and young adult European cohort.
For context, the MELD-ATG trial is one of four studies (Ver-A-T1D, MELD-ATG, Impact, and CFZ533) by Innodia, the largest European Network led by Prof. Mathieu. These studies have aligned trial design, such as inclusion criteria and biomarker analysis, to accelerate development of T1D prevention therapies and cures.
- Trial design. The MELD-ATG study recruited young individuals between 5-25 years newly diagnosed with T1D within six weeks. Participants were randomized to receive intravenous ATG (0.1, 0.5, 1.5, and 2.5 mg/kg) or placebo over two consecutive days. The trial adopted an adaptive dosing scheme; an independent unblinded Dose-Determining Committee regularly reviewed immune, metabolic, and safety data and adjusted doses as deemed necessary. The primary endpoint was change in stimulated C-peptide area under curve (AUC) at 12 months. Secondary endpoints included A1c, insulin dose, and CGM metrics, and immune biomarkers.
- At baseline, participants consisted of 18% children (5-9 years), 65% adolescents (10-17 years), and 17% young adults (18-25 years). Clinically, mean A1c was 7.8% and median of mixed-meal stimulated C-peptide level was 0.8 nmol/L/min.
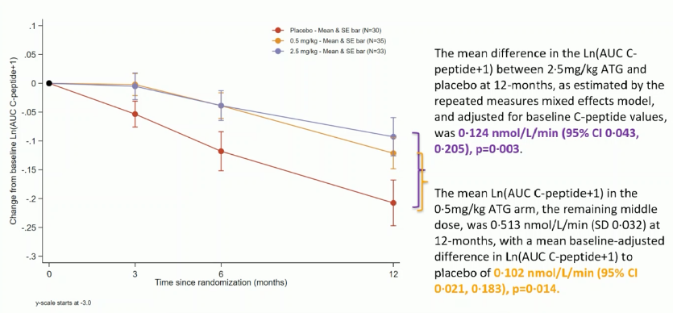
- Results. The trial met its primary endpoint, with ATG 2.5 mg/kg conferring significant C-peptide preservation over placebo by 0.124 nmol/L/min (p=0.003). Moreover, investigators identified 0.5 mg/kg as the minimum effective low dose, which significant preserved C-peptide AUC by 0.102 nmol/L/min (p=0.014). The efficacy was more pronounced in ages 5-17 and less in ages 18-25 (p-interaction=0.42). A1c remained low in both treatment groups (0.5 and 2.5 mg/kg), with the low dose achieving significant reduction compared to placebo group (0.5 percentage points; p=0.024). Insulin dose transiently increased in first month, which Prof. Mathieu attributed to serum sickness rescued by steroid therapy. Excitingly, ATG improved CGM metrics, measured at Months 3, 6, and 12 with blinded Dexcom G6. As shown in the figure below, Time in Range (TIR; 70-180 mg/dL) and Time in Tight Range (TITR; 70-140 mg/dL) remained stable in the 2.5 mg/kg arm at 63% and 38%, respectively, while placebo group experienced a decline from 65% to 58% and 41% to 34%, respectively.

Safety. Low-dose ATG was generally well-tolerated even in young children. Two Grade 4, life-threatening events (severe hypoglycemia) occurred, one in placebo and another in the 0.5 mg/kg arm. Expected adverse events included cytokine release syndrome (CRS) during infusion and serum sickness approximately 10-15 days later. In the trial, CRS occurred in 33% of 2.5 mg/kg arm (n=11) and 24% of 0.5 mg/kg arm (n=8), compared to none in placebo. Nonsteroidal anti-inflammatory drugs (e.g., ibuprofen or aspirin), antiemetics, and one-time steroid mitigated the symptoms. Serum sickness was more prevalent, with 81.8% in 2.5 mg/kg and 33% in 0.5 mg/kg experiencing for 3-5 days, compared to none in placebo.
9. In Ver-A-T1D trial, verapamil confers non-statistically significant preservation in C-peptide in new-onset T1D
- In an early morning session, Prof. Thomas Pieber (Medical University Graz, Austria) delivered full results of the year-long Ver-A-T1D trial (n=136), evaluating verapamil on beta cell function preservation in adults with new-onset stage 3 T1D. As background, verapamil is a calcium channel blocker used as an antihypertensive agent for over 40 years. Verapamil also lowers beta cell TXNIP (thioredoxin-interacting molecule), a stress molecule that promotes beta cell apoptosis. Human studies in 2018 and 2023 have also suggested preserved C-peptide in individuals newly diagnosed with T1D. Hence, this RCT aimed to assess the effect of verapamil 360 mg vs. placebo on the preservation of beta cell function in people with new-onset stage 3 T1D.
- Study design and baseline characteristics. 136 participants recently diagnosed with T1D were randomized 2:1 to once-daily oral verapamil or placebo treatment for 12 months. At baseline, participants were an average of 29 years old, with 68% being male. Clinically, participants had A1c of 7.9%, BMI of 24 kg/m2, total daily insulin dose of 0.32 U/day, and C-peptide AUC of 0.86 mmol/L.
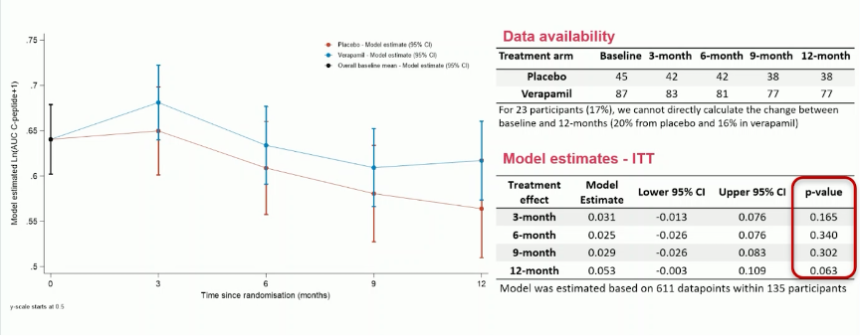
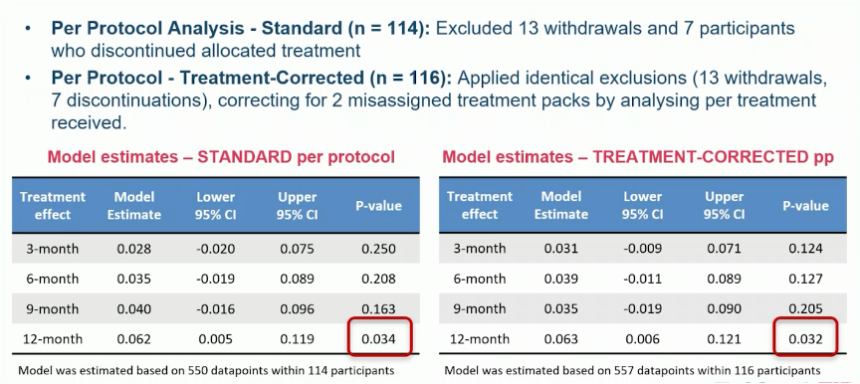
- Results. The trial did not meet the primary endpoint, as the change in C-peptide AUC from baseline did not differ significantly between verapamil and placebo (p=0.063). Nonetheless, as shown in the figure below, the intention-to-treat analysis showed verapamil numerically maintained C-peptide, while placebo declined modestly. Prof. Pieber explained that C-peptide decline in the placebo group was smaller than anticipated (experiencing ~10% loss) compared to prior studies, which likely made the threshold for clinically meaningful difference of 0.18 nmol/L/min “not appropriate” for the study. Per-protocol analysis,excluding withdrawals (n=13), discontinuations (n=7), and administrative or dispensing errors (n=2), found that verapamil significantly reduced C-peptide AUC (p=0.034).
- Secondary endpoints. Verapamil consistently lowered A1c by 0.3 to 0.5 percentage points compared to placebo – the difference of which was statistically significant for the first six months (p=0.001) but not at the numerically by 12 months (p=0.128). There was no significant difference in the insulin dose. Similarly, there were no significant differences in CGM metrics (TIR and TITR) at 1, 3, 6, 9, and 12 months between verapamil and placebo groups.
- Safety. Overall, verapamil was safe and generally well-tolerated in adults with no unexpected adverse events. Adverse events occurred at similar rates (97% vs. 94% in placebo), and serious adverse events were more prevalent in the placebo group (11%) than verapamil (7%). Two life-threatening events happened in the verapamil group — one severe hypoglycemia from accidental insulin overdose and one suicide attempt — which were deemed unrelated to the drug. Verapamil also caused expected side effects, including constipation (14% vs. 2%) and diarrhea (7% vs. 2%), mild first-degree atrioventricular (AV) block (20% vs. none), bradycardia (14% vs. 4%), and palpitations (4% vs. 4%). Neither second- or third-degree AV blocks nor hypotension occurred. All CV events were mild and reversible with dose reduction and did not lead to drug discontinuation.
- Verapamil may be an ideal candidate for combination therapies with other immune-modulating agents, given the favorable safety profile and the direct beta cell protection, Prof. Pieber said. Going forward, longer-term effects of verapamil (over three years of treatment) continue to be assessed in the open-label extension Ver-A-Long trial. Investigators also hope to conduct the T1DPlus to test possible drug combinations with verapamil.
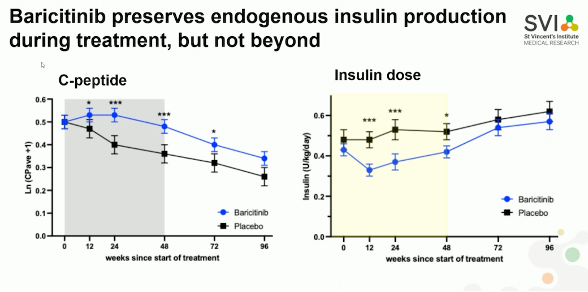
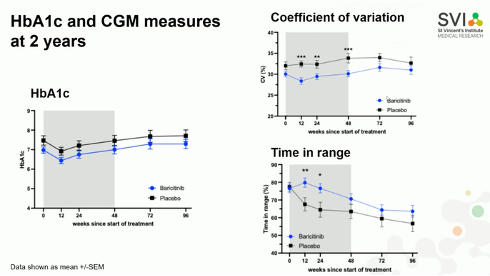
10. “There's no insulin like your own”: Two-year outcomes of the BANDIT trial demonstrate JAK inhibitor baricitinib preserves C-peptide
Dr. Michaela Waibel (St. Vincent’s Institute of Medical Research, Australia) delivered two-year outcomes of the phase 2 BANDIT trial (n=91), which evaluates JAK 1/2 inhibitor baricitinib in individuals with new-onset T1D. As background,certain immune cells require JAK-associated intracellular signaling molecules, so JAK1 and JAK2 inhibitors may be able to impair immune function to prevent the death of beta cells. This drug class is indicated for autoimmune diseases, such as rheumatoid arthritis and alopecia areata. In 2023, the BANDIT trial showed that baricitinib significantly preserved mixed-meal-stimulated mean C-peptide level compared to the placebo group (p=0.001) at Week 48. The presentation shared results of the two-year follow up of this study.
In addition to baricitinib, several JAK inhibitors are being assessed in T1D, such as JAK1 inhibitor abrocitinib and JAK3/TEC inhibitor ritlecitinib in the JAKPOT T1D trial.
- Trial design and baseline characteristics. 91 participants diagnosed with T1D within the past 100 days aged 10-30 years were randomized 2:1 to baricitinib (4 mg per day) or placebo. 89 participants were followed for 96 weeks. At baseline, the mean age was 18 years old, with vast majority being white. A1c across both treatment arms ranged from 7% to 7.5%, and the baseline median of the mixed-meal–stimulated mean C-peptide level at screening ranged from 0.6 to 0.67 nmol/L/min. See more details about baseline characteristics here.
- Results. Baricitinib significantly preserved C-peptide during the treatment but not beyond, as the difference lost the statistical significance at Week 96. Insulin requirement was similarly reduced during the treatment period but did not last beyond Week 48 (see figure below). A1c was not significantly different across all time points. While TIR was significantly improved for baricitinib group early treatment period, the effect diminished over time. Subgroup analysis further suggested that the benefits of baricitinib on C-peptide preservation and A1c reduction may be greater among adults (18-30 years) than children (10-17), though the study was not powered to detect differences. The treatment is well-tolerated and safe.
- Additional analyses. Pharmacological studies confirmed that the JAK-STAT pathway inhibition with baricitinib is reversible, as there is no difference in STAT3 phosphorylation 24 hours after a dose. By age groups, there was no difference in STAT3 phosphorylation or inhibition from baricitinib. These results were consistent with STAT1 and STAT5 phosphorylation. In another analysis evaluating potential effects on alpha cell function, baricitinib group seemed to experience slight decline in glucose response across the study. Further analysis by responders (n=48) and non-responders (n=12) to baricitinib had statistically significant differences in C-peptide preservation (p<0.001), A1c (p=0.004), and insulin dose (p=0.001). Dr. Waibel reported that BMI ≥30 kg/m2 and adherence rate ≥80% numerically predicts the response. As we do, she looks forward to larger phase 3 trials.
11. Do we need really need a large outcome trial to prove the cardiorenal benefits of SGLT-2 inhibitor and GLP-1 RA combination use?
In this morning session, the highly-admired Dr. Hertzel Gerstein (McMaster University & Hamilton Health Sciences, Canada) reviewed meta-analyses of cardiovascular (CV) outcome trials to make a compelling case for SLGT-2 inhibitors and GLP-1 RA combination therapy. SGLT-2 inhibitors and GLP-1 RAs confer substantial CV and kidney benefits, but no outcomes trial has directly investigated the benefit of using both therapies in combination, in comparison to either therapy alone. Rather than proposing an additional large outcomes trial, Dr. Gerstein leveraged background SGLT-2 inhibitor use in GLP-1 RA trials in existing CV meta-analyses, and vice versa, to support the combination use in high-risk patients.
- Dr. Gerstein advocated for filling in clinical context with existing evidence. GLP-1 RAs and SGLT-2 inhibitors are examples where randomized outcomes trials revealed clinical benefits beyond the trial’s original focus. These therapies, developed initially for diabetes management, demonstrated substantial and unexpected CV benefits. Therefore, Dr. Gerstein highlighted that such large studies not only confirm safety and efficacy of the trials’ focus but may also offer findings that confer unexpected advantages. Existing outcomes trials, which include the use of background GLP-1 RA use in SGLT-2 inhibitor outcomes trials (and vice versa), can help inform clinical decisions on whether combination therapy is appropriate for high-risk patients.
- Although the exact mechanisms of GLP-1 RAs and SGLT-2 inhibitors are debated, their benefits are well established. Both drug classes reduce CV and kidney 0utcomes in people with and without T2D, with no evidence suggesting differential effects base on diabetes status. Similarly, on intermediate measures including weight, A1c, blood pressure (BP), eGFR, and albuminuria, the effect of these drugs appears to be independent. Moreover, according to Dr. Gerstein’s analysis of recent outcomes trials, no meaningful interaction between the two occurred – indicating that combination therapy offers the additive benefits of both.
- “Explanations are evanescent. Observations are robust.” Debates on the mechanism of these therapies might go on forever, Dr. Gerstein added. However, individual benefits of GLP-1 RAs and SGLT-2 inhibitors are clear. Given the evidence of non-interaction between the two, Dr. Gerstein advocated for high-risk patients to receive the benefits of both and urged clinicians to apply existing data to their practice, rather than awaiting a designated SGLT-2 inhibitor/GLP-1 RA combination outcomes trial.
- Furthermore, Dr. Gerstein questioned if we need a large outcome trial to prove the added benefits of SGLT-2 inhibitor and GLP-1 RA combination use. Depriving high-risk patients of the “profound” potential additive benefits (decreased NNTs, MACE, HF, and kidney decline) would be hard to ethically justify, he argued.
12. Benefits and challenges of AI-assisted screening for diabetic retinopathy and an overview of the eye health treatment landscape
In a morning session dedicated to diabetic retinopathy, Dr. Maria Cicinelli (IRCCS San Raffaele Scientific Institute, Italy), Prof. Alicia Jenkins (Baker Heart and Diabetes Institute, Australia), and Dr. Inês Pereira Marques (AIBILI, Portugal) discussed screening and the therapeutic landscape.
- Dr. Cicinelli highlighted the benefits and challenges of AI-assisted screening. As background, screening for diabetic retinopathy is typically performed via a dilated fundus exam, which can cause temporary light sensitivity and blurred vision for hours afterwards. In contrast, non-mydriatic fundus photography is now available and eliminated the need for dilation. Additionally, these pictures can be analyzed using platforms such as ARIAS (Automated Retinal Image Analysis Software), which is AI-powered and offers high sensitivity and specificity for detecting diabetic retinopathy. In addition to accuracy, Dr. Cicinelli emphasized that AI-assisted screening can positively impact screening uptake by improving patient satisfaction, such as in children. Challenges that remain include image quality issues, generalizability across populations and devices, reimbursement, and implementation into clinic workflows.
- Prof. Jenkins gave an overview of clinical trials for the lipid-lowering drug fenofibrate, which is currently under further investigation for diabetic retinopathy. In diabetes, leaky retinal vasculature can cause lipids to accumulate in the retina. Crystalline cholesterol deposits have also been observed in the retinas of people with diabetes. These conditions lead to inflammation and oxidative damage due to altered metabolism. Fenofibrate, an oral medication used to treat high cholesterol and triglyceride levels, has been investigated in the LENS trial (n=1,151), which found that fenofibrate can reduce the progression of diabetic retinopathy in people with both T1D and T2D. Currently, the Breakthrough T1D-funded FAME-1 Eye trial is underway for adults with T1D and expected to complete in 2026. There is also the Protocol AF (Fenofibrate for Prevention of DR Worsening) trial for people with T1D and T2D, which is sponsored by the Jaeb Center for Health Research.
- Dr. Pereira Marques reviewed the landscape of treatments for diabetic macular edema (DME) and diabetic retinopathy. For DME, recent treatment options include long-acting steroids such as the intravitreal implant ILUVIEN (see NEW DAY study), as well as newly approved anti-VEGF therapies like Vaybysmo (faricimab) (see YOSEMITE/RHINE and RHONE-X studies) and Eylea (aflibercept) (see PHOTON study). However, these options are limited by factors such as variable response rates, side effects (e.g., increased intraocular pressure, cataracts), high costs, adherence challenges, and the need for frequent intravitreal injections (which are invasive, painful, and must be administered by a specialist). Specific therapies under investigation include anti-inflammatory drugs (e.g., anti-IL6 agents) and gene therapies (such as 4D-150 or RGX-314). For proliferative diabetic retinopathy, current treatment options include pan-retinal photocoagulation and approved intravitreal anti-VEGF therapies. Other delivery devices are being studied, such as the port delivery system (see PAVILION trial), as well as oral medications and topical eye drops, which may be effective in milder forms of diabetic retinopathy before the development of complications (e.g., APX3330, OCS-01, and DPP-4 inhibitor sitagliptin). Anti-diabetic drugs such as SGLT-2 inhibitors and GLP-1 RAs, along with lipid-lowering agents like fenofibrate, have shown protective effects against retinopathy progression and warrant further investigation in RCTs. The future of diabetic retinopathy management may involve personalized treatment, utilizing biomarkers of disease progression (including imaging and inflammatory biomarkers) to better define therapeutic strategies.
Tech
13. GRACE and DipGluMo show the huge power of CGM’s role in GDM management
Gestational diabetes mellitus (GDM) was a major focus on the final day of EASD 2025 in this Dexcom-sponsored symposium. Prof. Tina Linder (Medical University of Vienna, Austria), Prof. Christian Göbl (Medical University of Vienna, Austria), and Prof. Helen Murphy (University of East Anglia, the UK) explored recent data on CGM use in gestational diabetes, comparing findings from the GRACE and DipGluMo studies to explore the potential for CGM to improve both maternal glycemic management and neonatal outcomes. All over the floor today, we kept hearing, “did you see the GOBL data?” … which initially sounded like a trial, but really reflects the name Göbl, for Professor Göbl, of course!
- As a reminder, the GRACE study results were first presented on Tuesday by Prof. Linder (Medical University of Vienna, Austria). The open-label trial enrolled women with GDM (n=375) across four sites in Austria, Germany, and Switzerland. Participants were randomized 1:1 to either Dexcom G6 CGM (n=190) or BGM (n=185). Women in the BGM group also wore a blinded CGM for 10 days after randomization and again at 36-38 weeks’ gestation. LGA occurred in 3.5% of infants in the CGM group versus 10.3% with BGM. Mean newborn weight percentiles were also lower in the CGM group. As expected, women using CGM demonstrated more Time in Pregnancy Range (TIPR, 65-140 mg/dL) between 36-38 weeks of gestation compared to baseline. Prof. Linder added that it is clear that there is high patient acceptance for CGM, with glycemic benefits from continuous monitoring seen even among those who traditionally don’t adhere to regular BGM testing. However, she identified the ongoing need to identify optimal TIR and glucose ranges for patients with GDM, as well as if there is a need for variable TIR by GDM phenotype.
- Prof. Göbl then reviewed findings from the Swiss DipGluMo study (n=299), which closely mirrored GRACE in design but yielded strikingly different results: LGA rates were identical between CGM and BGM groups (10% each). He suggested several possible explanations, including slightly younger age (33 vs. 34 years) and lower BMI (26 vs. 27 kg/m²) in DipGluMo suggesting a better-managed study population, as well as looser treatment targets, fewer recommended BGM checks, and more conservative insulin algorithms. As a result, rapid-acting insulin use was far lower in DipGluMo (4-5%) than in GRACE (30-41%). Prof. Murphy seized on these differences, warning against unrealistic expectations for LGA outcomes in GDM. She argued that since ~10% of infants in the general population are above the 90th percentile, this should remain the threshold for GDM care, rather than aiming for even lower rates. “We shouldn’t expect women with GDM to have smaller babies than they would if they didn’t have diabetes,” she concluded, stressing that focus should instead be on minimizing excess postnatal growth.
- Looking ahead. Prof. Murphy also pointed to CGM’s promise for detecting dysglycemia and GDM early in pregnancy, enabling earlier interventions and potentially lowering LGA risk. She expressed optimism about forthcoming results from the MAGiC study and its collaboration with GLAM, which she hopes will show that abnormal glucose patterns are already detectable in the first trimester.
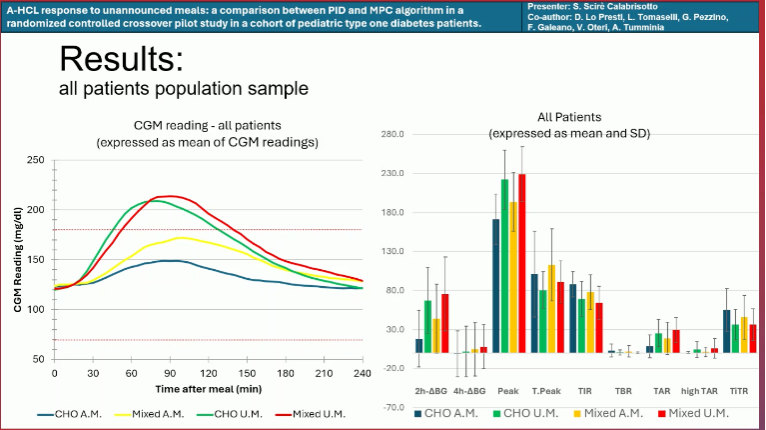
14. MiniMed 780G vs. Control-IQ: Handling unannounced meal in adolescents with T1D
Dr. Salvatore Scirè Calabrisotto (University of Catania, Italy) presented a randomized crossover study (n=20) evaluating the response of two hybrid closed-loop AID systems – Medtronic MiniMed 780G and Tandem Control-IQ – to unannounced meals. Unannounced meals remain a major challenge for AID systems, especially in adolescents, where missed or delayed boluses are common. MiniMed 780G’s Auto Correction bolus and Control-IQ’s (and Control-IQ+’s) AutoBolus features work to correct the associated rapid glucose excursions with unannounced meals, and both have been shown in separate studies to maintain positive glycemic outcomes even in those who frequently forget to bolus.
- Study design. The researchers employed a randomized crossover design. Participants consumed either a carbohydrate-only (CHO) breakfast (bread and jam, 31 g carbohydrates) or a mixed breakfast (30 g carbohydrates + 15 g protein). Group A (n=10) began with six meals (three CHO, three mixed) with meal announcements, followed by a seven-day washout and then six unannounced meals. Group B followed the opposite order. All participants were instructed to bolus 10 minutes before the announced meals.
- Baseline characteristics. Participants were adolescents with T1D (ages 11–18 years) who had been using AID for at least three months and had a diabetes duration at least one year. Mean age was 15 years, 35% were female, mean A1c was 6.9%, and mean TIR was 76%. Half the cohort used MiniMed 780G, which runs on a proportional-integral-derivative (PID) algorithm, while the other half used Control-IQ, which employs a model predictive control (MPC) algorithm.
- Results. Across both systems and meal types, glucose profiles converged within four hours. As expected, mixed meals produced a slightly delayed and higher peak due to protein metabolism. Unannounced meals led to earlier, sharper glucose excursions compared to announced meals (see figure below).
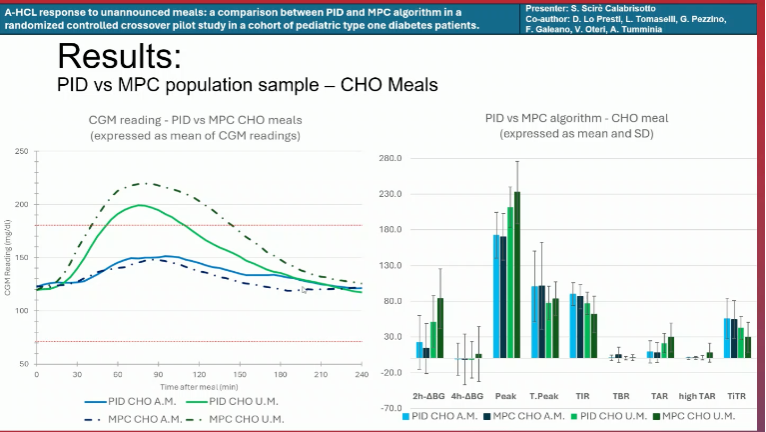
- MiniMed 780G vs. Control-IQ responding to CHO meals. With announced CHO meals, both systems produced nearly identical profiles, rising from ~120 mg/dL to ~150 mg/dL at ~90 minutes (see figure below). With unannounced meals, peaks were higher, but MiniMed 780G users had a lower mean peak (~200 mg/dL) than Control-IQ users (~220 mg/dL). Both systems achieved comparable TIR and Time in Tight Range (TITR; 70-140 mg/dL) with announced meals, though MiniMed 780G maintained slightly higher values with unannounced meals.
- MiniMed 780G vs. Control-IQ responding to mixed meals. With announced mixed meals, MiniMed 780G peaked at ~160 mg/dL and Control-IQ at ~180 mg/dL, both at ~90 minutes. With unannounced mixed meals, differences widened: MiniMed 780G peaked earlier and lower (~200 mg/dL) than Control-IQ (~230 mg/dL). Unlike with CHO meals, MiniMed 780G users achieved higher mean TIR with announced meals than Control-IQ users, which achieved a similar TIR to MiniMed 780G use with unannounced meals.
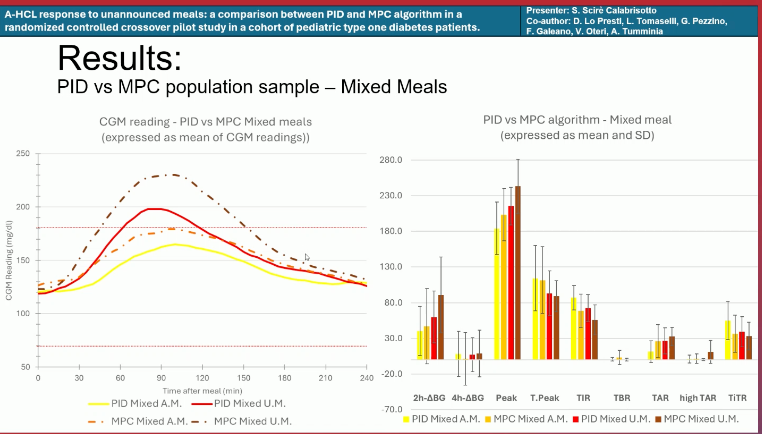
- Dr. Calabrisotto concluded that PID-based algorithms (MiniMed 780G) appear to handle unannounced meals slightly better than MPC-based algorithms (Control-IQ), regardless of meal type. However, both systems perform best when meals are announced, underscoring the importance of bolusing and meal disclosure even with advanced AID.
15. New insights in glycemic management: Sleep duration, pregnancy, and a head-to-head comparison of three CGMs during exercise
Prof. Anna Duda-Sobczak (Poznan University of Medical Sciences, Poland), Dr. Shristi Rawal (Rutgers University), and Sabrina Sanfilippo (University of Bayreuth, Germany) explored the role of sleep in T1D and pregnancy as well as head-to-head comparisons of different CGM systems during exercise. Collectively, the findings underscored how both lifestyle factors and device performance shape outcomes in T1D and pregnancy.
- Adequate sleep is independently associated with better glycemic stability in adults with T1D. Prof. Duda-Sobczak presented an analysis of CGM data from adults with T1D (n=155), which found that those meeting National Sleep Foundation (NSF) recommendations (between seven and nine hours of sleep) had: (i) significantly lower mean glucose (161 vs. 172-175 mg/dL); (ii) reduced glycemic variability; and (iii) higher TIR (64% vs. 57%) compared to both short (<7 hours) and long sleepers (>9 hours). Logistic regression analysis confirmed that recommended sleep duration predicted lower glycemic variability, highlighting sleep as an overlooked lifestyle factor in T1D management.
- Longer sleep improved glucose profiles in pregnant women with GDM or impaired glucose tolerance (IGT). Dr. Rawal presented a preliminary analysis of CGM data in women with GDM or IGT (n=48) across sites in the US and Nepal. Results showed that while sleep quality was not predictive of glycemic outcomes, longer sleep duration correlated with more favorable CGM-derived glycemic profiles. In the US subgroup, sleeping 6.1-7.9 hours was associated with significantly lower: (i) 24-hour mean glucose; (ii) fasting glucose; and (iii) nocturnal glucose. She said that the absence of these associations in the Nepal subgroup suggested contextual factors such as diet, lifestyle, and healthcare access may shape the sleep-glycemia relationship.
- Turning to exercise, Dexcom G7 and Abbott’s FreeStyle Libre 3 were found to outperform Medtronic’s Simplera during exercise and at-home settings. Sanfilippo reviewed a prospective head-to-head comparison of the three CGM systems (n=20 adults with T1D) over seven days. Participants simultaneously wore Dexcom G7, Libre 3, and Simplera across a structured three-day exercise protocol and a four-day at-home phase. Median absolute relative difference (MedARD) was 7.5% for Libre 3, 8.4% for Dexcom G7, and 13.8% for Simplera. While no significant differences were observed between Dexcom G7 and Libre 3 across the two study phases, Sanfilippo remarked that Simplera demonstrated significantly lower accuracy.
16. *NEW* CGM as a routine for T2D: Evidence from RCTs, real-world data, and case studies
In an Abbott-sponsored symposium chaired by Prof. Stefano Del Prato (University of Pisa School, Italy), Prof. Emma Wilmot (University of Nottingham, UK) and Prof. Virginia Bellido (Hospital Universitario Virgen del Rocío, Spain) discussed why CGM should be considered part of a routine for people with T2D. Across RCTs, real-world data, and case studies, the session highlighted the consistent glycemic and behavioral benefits of CGM and called for policy alignment with existing evidence.
- RCTs and systematic reviews confirm that CGM improves outcomes in both insulin and non-insulin-treated T2D. Building on presentations at ADA 2025, speakers suggested using CGM for diabetes management for insulin-treated individuals. Data from FreeStyle Libre trials demonstrated 0.5% A1c reductions with improved treatment satisfaction. Furthermore, the MOBILE study (n=175) demonstrated a 0.4% A1c reduction in basal insulin users with CGM, and the IMMEDIATE study (n=116) confirmed benefits in those on non-insulin therapy. Another umbrella review further reinforced consistent A1c reductions, as well as TIR and TAR improvements, with findings invariant across CGM modality, study funding, and prior insulin use.
- Pairing CGM with structured education enhances engagement and behavior change. Prof. Wilmot highlighted that CGM is most impactful when paired with simple, tailored education. The PDF study, a 12-week RCT (n=126), showed that adding intermittently scanned CGM (isCGM) to lifestyle counseling significantly improved glycemic outcomes in adults with T2D. Prof. Bellido further detailed several case studies illustrating how CGM revealed post-meal hyperglycemia and nocturnal lows, driving adjustments in diet, insulin timing, and lifestyle. Notably, through both RCTs and case studies, FreeStyle Libre 3 use was associated with improved patient confidence, awareness, and adherence, suggesting that behavior modification is another benefit of CGM use.
- Policy and access remain misaligned with evidence despite consistent benefits across populations. The symposium closed with a call for healthcare systems to align reimbursement with evidence showing the benefits of CGM use in people with T2D, both with and without insulin treatment. Both Prof. Wilmot and Prof. Bellido stressed that CGM provides fundamental insights empowering both patients and HCPs to act earlier and more effectively. They also noted that impactful data should be leveraged to expand access, as every individual with diabetes has the potential to benefit from CGMs across diverse settings.
17. *NEW* Nationwide French data highlight durability and glycemic gains associated with AID use
Dr. Chloe Amouyal (Sorbonne Université, Paris, France) presented results from a real-world French nationwide observatory study evaluating two years of AID use in children and adults who initiated the technology in 2022. All participants had T1D; 28% were children and 56% were female. The mean age was 38 years. Nearly all used either Tandem t:slim X2 with Control-IQ (50%) or MiniMed 780G (49%), the two systems reimbursed nationally at the time of the study.
- Dr. Amouyal described adherence as “excellent,” with 98% still using AID after two years. Most pump discontinuations were temporary, often due to system burden or timing (e.g., summer months might see more pump “vacations” than other seasons). Participants spent a mean 95% of time in automated mode.
- Glycemic outcomes. Mean A1c of 7.7% fell 0.5 percentage points to 7.2% after 24 months. TIR improved from 58% to 69%, up 11 percentage points, driven mainly by a reduction in Time above Range (>180 mg/dL), which fell substantially from 39% to 29%. The proportion of people achieving target TIR >70% more than doubled to 49% from 22%, and those meeting both targets (TIR >70% and <4% Time below Range [<70 mg/dL]) tripled to 42% from 14%. Still, Dr. Amouyal emphasized that fewer than half of participants reached both targets, underscoring the need for greater education on carbohydrate counting and ideally more regular follow-up.
- Complications. Severe hypoglycemic events were also significantly reduced by 24 months, falling from 4% of patients reporting one within the last 12 months to just 1%. DKA incidence remained stable, improving to 0.9% to 1.2% incidence in the previous 12 months.
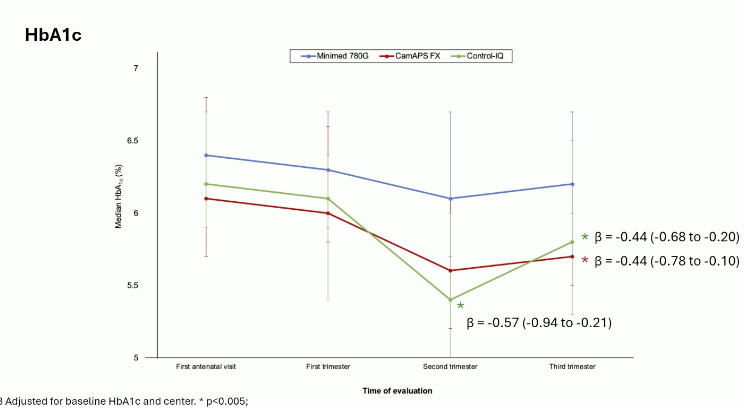
18. *NEW* CamAPS FX and Control-IQ improve glycemia and neonatal outcomes vs. MiniMed 780G in pregnant women with T1D; strong outcomes across all systems
Dr. Carmen Quiros (Hospital Universitari Mútua Terrassa, Spain) presented results from a multicenter observational trial comparing Tandem’s Control-IQ algorithm, Medtronic’s MiniMed 780G system, and CamDiab’s CamAPS FX hybrid closed-loop system in pregnant women with T1D. CamAPS FX had the edge in some glycemic measures and in neonatal outcomes. But the good news is that all three systems delivered A1c <6.5% and TIR above 65% in the third trimester. It seems clear that AID should be the logical choice for pregnancy.
- The trial spanned 27 hospitals in Spain, with AID use starting before 20 weeks of gestation. Participants (n=137) had a mean age of 34 years and diabetes duration of 19 years. Prior to pregnancy, most MiniMed 780G (80%) and Control-IQ (64%) users were already on their respective systems, compared to 37% of CamAPS FX users. In the cohort, n=14 were on Control-IQ systems, n=85 on MiniMed 780G, and n=38 on CamAPS FX.
- Glycemic targets: CamAPS FX users employed lower glucose targets during pregnancy (96 mg/dL, 91 mg/dL, and 87 mg/dL across trimesters) than MiniMed 780G users (103 mg/dL in the first trimester, 100 mg/dL thereafter).
- Control-IQ and CamAPS FX both achieved lower A1c levels than MiniMed 780G in later trimesters; In the second trimester, Control-IQ users had lower median A1c than MiniMed 780G users (~5.4% vs. ~6.2%), while both Control-IQ and CamAPS FX held significantly lower median A1c than MiniMed 780G by the third trimester. Notably, median A1c was <6.5% across all systems and trimesters. Turning to time in range (TIR), the only statistically significant TIR difference between systems occurred in the second trimester, when CamAPS FX users achieved higher TIR than MiniMed 780G (70% vs. 65%). By the third trimester, all systems reached mean TIR ≥70%.
- Maternal and neonatal outcomes: Rates of gestational weight gain, cesarean section, and preeclampsia did not differ by system. Neonatal outcomes, however, favored CamAPS FX: mean birthweight was lower, as were rates of large-for-gestational-age infants (38% vs. 63%), macrosomia (3% vs. 29% and 23% [Control-IQ]), and NICU admission (3% for CamAPS FX and MiniMed 780G vs. 15% with Control-IQ). Adjusted models showed both CamAPS FX and Control-IQ reduced the risk of large-for-gestational-age compared to MiniMed 780G.
--by Riya Chatterjee, Kayla Mathieu, Elizabeth Rose, Jeremy Alkire, Nour Khachemoune, Katherine Moon, Esther Min, Elaine Young, Monica Oxenreiter, and Kelly Close