WCIRDC 2025 Day #1 Highlights –
Executive Highlights
- The 23rd annual World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease (WCIRDC) conference kicked off today at the Hilton Universal Hotel in LA. Surrounded by the festivity of Christmas decor, the first day comprised basic science discussions on insulin resistance and dysglycemia, as well as clinical insights into diabetes and comorbidities.
- On insulin resistance, Dr. Ralph DeFronzo illustrated an octet for insulin resistance – the earliest and central dysfunction that underlies T2D, prediabetes, obesity, MASH, and cardiovascular disease. He explained that insulin resistance is a two‑part disorder: (i) impaired insulin receptor signaling; and (ii) defective intracellular glucose metabolism. The latter metabolic disturbance begins long before dysglycemia and quietly incurs damage on blood vessels and organs. Thus, he pointed out that T2D “starts in the pre‑prediabetic state” with decline in insulin sensitivity and glucose tolerance before glycemic levels rise. Clinically, Dr. DeFronzo urged a return to treating insulin resistance itself, not just hyperglycemia, and advocated earlier use of insulin‑sensitizing therapies, TZDs and GLP‑1 RAs. For lean people with T2D, Dr. DeFronzo suggested combining insulin sensitizers with lifestyle change to restore normoglycemia.
- Continuing the discussion on “pre- prediabetes,” Dr. John Armato (Providence Medical Associates) highlighted the association between insulin resistance and cardiometabolic risk in people without obesity. Early detection and interventions remain crucial, as the pathophysiology characterized by insulin resistance and progressive loss of beta cell function typically appears decades before the onset of T2D. Focusing on prevention could significantly help mitigate complications and comorbidities. Further emphasizing this point, the STOP DIABETES trial (n=1,860) showed that 27% of people without prediabetes had abnormal oral glucose tolerance test measurements. Therefore, Dr. Armato spotlighted a subset of study populations – those with “pre-prediabetes” – who are not considered to have prediabetes based on fasting glucose levels or A1c levels but demonstrate insulin resistance.
- Several talks focused on preventing cardiorenal complications, including heart failure (HF), cardiovascular disease (CVD), and chronic kidney disease (CKD).
- On HF, Dr. Stephen Greene (Duke University) emphasized the role of metabolic dysfunction and visceral adiposity in its pathogenesis. Dr. Greene endorsed a tripartite therapeutic approach, including SGLT2 inhibitors, nonsteroidal MRAs, and incretin-based therapies for those with obesity.
- On CVD, Dr. Nathan Wong (UCLA, UCI) highlighted CV risk assessment in people with diabetes and CKM syndrome discussing newer risk scores followed by the role of coronary calcium and opportunistic testing.
- On CKD, Dr. Jennifer Green (Duke University) highlighted findings from the phase 2 CONFIDENCE trial (n=784) to advocate for simultaneous initiation of SGLT-2 inhibitors and finerenone.
- On hypercortisolism, Dr. Vivian Fonseca (Tulane University) said that excessive cortisol levels contribute to insulin resistance and difficult-to-control diabetes.
Table of Contents
- 1. Back to basics: Insulin resistance as a foundational defect in T2D pathogenesis
- 2. “Pre-prediabetes”: The association between insulin resistance and cardiometabolic risk in people without obesity
- 3. Beyond glycemic management: Visceral adiposity as a therapeutic target for HFpEF
- 4. Cardiovascular prevention: Dr. Nathan Wong discusses the role of risk scores, coronary calcium and opportunistic testing for cardiometabolic disease
- 5. Combination therapies for CKD and T2D: Dr. Jennifer Green spotlights clinical insights from the phase 2 CONFIDENCE trial
- 6. The impact of hypercortisolism on insulin resistance in people with diabetes
1. Back to basics: Insulin resistance as a foundational defect in T2D pathogenesis
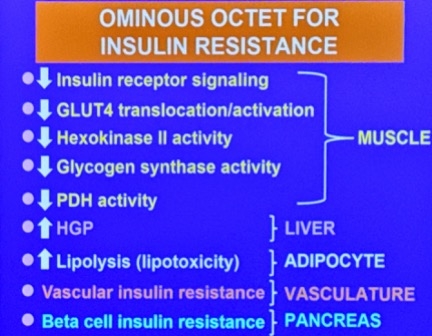
In a standing‑room‑only opening session, Dr. Ralph DeFronzo (UT Health San Antonio) returned to one of his signature themes: the Ominous Octet. Rather than referring to hyperglycemia, however, Dr. DeFronzo illustrated an octet for insulin resistance – the earliest and central dysfunction that underlies T2D, prediabetes, obesity, MASH, and cardiovascular disease. He explained that insulin resistance is a two‑part disorder: (i) impaired insulin receptor signaling; and (ii) defective intracellular glucose metabolism. The latter metabolic disturbance begins long before the onset of overt glucose intolerance and quietly incurs damage on blood vessels and organs.
- In normal post‑meal physiology, insulin coordinates a response among multiple organs: (i) skeletal muscle, the primary site of glucose disposal, increases GLUT4 translocation (the insulin-response glucose transporter responsible for moving glucose into cells) and intracellular glucose metabolism; (ii) the liver suppresses hepatic glucose production; (iii) adipocytes suppress lipolysis, lowering free fatty acids (FFA); and (iv) the vasculature dilates to deliver glucose and insulin to tissues. In insulin resistance, such responses are diminished: (i) muscle fails to take up glucose effectively; (ii) hepatic glucose production remains inappropriately high; (iii) adipose tissue continues to release FFAs and inflammatory adipokines; and (iv) impaired vasodilation limits muscle glucose uptake.
- Dr. DeFronzo summarized decades of clamp studies, muscle biopsies, and molecular work to summarize these defects as an “Ominous Octet” of insulin resistance affecting the muscle, liver (increased hepatic glucose production), adipose tissue (enhanced lipolysis and lipotoxicity), vasculature (loss of insulin‑mediated vasodilation), and pancreas (beta‑cell insulin resistance), and then extended the concept to kidney podocytes as well. Further, ß cell-specific insulin receptor knockout models show that intact insulin signaling within the beta cell itself is required for normal insulin secretion.
- Dr. DeFronzo stressed that insulin resistance appears well before dysglycemia. One of Dr. DeFronzo’s prior clamp studies conferred a 15-20% decline in insulin sensitivity even within the “normal” fasting glucose range, with far more severe defects in impaired glucose tolerance and T2D. Accordingly, he pointed out that T2D “starts in the pre‑prediabetic state.” Chronic hyperinsulinemia in the face of insulin resistance activates MAP kinase signaling, which promotes inflammation and atherosclerosis while PI3K‑mediated metabolic signaling is diminished. Such a combination positions chronic hyperinsulinemia as an immense risk factor for cardiovascular disease.
- Clinically, Dr. DeFronzo urged a return to treating insulin resistance itself, not just hyperglycemia. With microvascular and macrovascular complications beginning within the longer insulin‑resistant phase of normoglycemia, Dr. DeFronzo advocated earlier use of insulin‑sensitizing therapies – particularly TZDs (e.g. pioglitazone as an inhibitor to the MAP kinase pathway and activation of the insulin signaling IRS-1/PI3K/Akt pathway) and GLP‑1 RAs, which he argued “should be first‑line therapies in our diabetic patients.” For lean people with T2D, Dr. DeFronzo suggested combining insulin sensitizers with lifestyle change to potentially restore normoglycemia.
2. “Pre-prediabetes”: The association between insulin resistance and cardiometabolic risk in people without obesity
Terming “pre-prediabetes,” Dr. John Armato (Providence Medical Associates) highlighted the association between insulin resistance and cardiometabolic risk in people without obesity. As a physician practicing internal medicine and endocrinology, Dr. Armato focuses on opportunities for prevention, particularly from prediabetes to T2D, by characterizing physiology using oral glucose tolerance tests, insulin sensitivity (i.e., Matsuda Index), and beta cell response (i.e., Disposition Index). Dr. Armato and collaborators have introduced physiologic testing including a "Glucose-Insulin Stress Test" (GIST) which identifies the 30% patients who are prediabetic based upon A1c/Fasting Plasma Glucose levels, but have normal physiologic studies and require no intervention or treatment, which will become available nationwide in the coming weeks. Early detection and interventions remain crucial, as the pathophysiology characterized by insulin resistance and progressive loss of beta cell function typically appears decades before the onset of T2D. Focusing on prevention could significantly help mitigate microvascular and macrovascular complications, as well as prevent further comorbidities. Further emphasizing this point, the STOP DIABETES trial (n=1,860) showed that 27% of people without prediabetes had abnormal oral glucose tolerance test measurements. Therefore, Dr. Armato elaborated on a subset of populations in the STOP DIABETES, specifically those with “pre-prediabetes,” who are not considered to have prediabetes based on fasting glucose levels or A1c levels but demonstrate insulin resistance.
- The subset of the STOP DIABETES trial differentiated insulin resistance and the insulin sensitive group. The STOP DIABETES trial included 624 people who didn’t have obesity (BMI <30 kg/m²) and prediabetes (fasting plasma glucose <100 mg/dL and A1c <5.7%). Of this population, 151 individuals were defined as insulin resistant (Matsuda Index <25th percentile) and compared to a subset of populations with insulin sensitivity (n=151), matched for age, sex, and BMI.
- The insulin resistance group exhibited significant differences in cardiometabolic measures compared to the insulin sensitive group. Compared to the group with insulin sensitivity, the group with insulin resistance without obesity and prediabetes demonstrated significant differences in the following measurements: (i) 60-minute plasma glucose (147 vs. 123 mg/dL; p<0.0001); (ii) 120-minute plasma glucose (112 vs. 90 mg/dL; p<0.001); (iii) mean plasma glucose area under the curve from zero to 120 minutes (134 vs. 116 mg/dL/min; p<0.0001); (iv) unrecognized impaired glucose tolerance (15% vs. 5%; p=0.005); and (v) unrecognized T2D (3% vs. 0%; p=0.04). Furthermore, the insulin resistance group had significantly higher mean systolic blood pressure (124 vs. 119 mmHg; p=0.006) and diastolic blood pressure (75 vs. 72 mmHg; p<0.001), as well as significantly higher lipid levels. The insulin resistance group also had higher inflammatory levels, marked by hs-CRP (2.1 vs. 1.3 mg/L; p=0.005).
- Dr. Armato highlighted the importance of focusing on populations with “pre-prediabetes.” Overall findings from the subset of the STOP DIABETES trial showed the association between insulin resistance and abnormalities in glycemic levels, insulin secretion, cardiometabolic risk factors, and increased carotid plaque in those identified to have “pre-prediabetes.” Given that these findings were prevalent, regardless of the BMI cutoffs of <25 kg/m², <27.5 kg/m², and <30 kg/m², Dr. Armato encouraged a focus on populations with insulin resistance, in the absence of obesity and prediabetes. He said, “Insulin resistance doesn’t wait for glucose to go up. And you [physicians] shouldn’t wait either [to provide interventions].”
3. Beyond glycemic management: Visceral adiposity as a therapeutic target for HFpEF
In this lively presentation, Dr. Stephen Greene (Duke University) reframed traditional thinking around heart failure (HF) pathogenesis, emphasizing the critical role of metabolic dysfunction. Dr. Greene reviewed population attributable risk data across racial and ethnic groups, which found hypertension, obesity, and diabetes as the leading contributors to HF with preserved (HFpEF) and reduced ejection fraction (HFrEF). While obesity is often underscored as the main contributor in HFpEF, Dr. Greene spotlighted that diabetes is a dominant and underrecognized driver. One study showed a stepwise increase in HF risk with each additional uncontrolled CV risk factor, such as A1c ≥7.0, BP ≥140/80 mmgHg, albuminuria, active smoking, and LDL-c ≥2.5 mmol/L. Even patients with no risk factors had a 45% higher HF risk compared to controls, suggesting that diabetes confers unique downstream cardiomyopathic effects.
- Dr. Greene then turned to the active debate on HFpEF pathogenesis. Dr. Greene highlighted a novel framework published in August 2025 that proposed visceral adiposity, not dysglycemia, as the proximal cause of HFpEF, T2D, and hypertension. Supporting this, Dr. Greene highlighted the PARAGON-HF trial (n=4,796), which found that 96% of HFpEF patients had central adiposity. Dr. Greene reviewed the adipokine hypothesis, which links excess visceral fat to systemic inflammation, cardiac fibrosis, and sodium retention. He emphasized that therapies targeting adiposity, such as GLP-1 RAs, have shown efficacy in HFpEF, while spironolactone may worsen glycemic control despite its benefits on HF. Indeed, across three studies, spironolactone was associated with significant increases in A1c in people with T2D.
- Dr. Greene concluded with a pragmatic framework for clinical care and future innovation. He emphasized that CV outcomes trials now support therapies targeting adiposity, highlighting the SELECT trial (n=17,604), where semaglutide reduced the risk of incident heart failure by 18%, and the SUMMIT trial (n=731), where tirzepatide lowered the risk of worsening HF events in established HFpEF by 38%. While disentangling the independent effects of obesity, insulin resistance, and diabetes remains complex, the totality of evidence favors adiposity as the more proximal driver of HFpEF. For patients with EF >40%, Dr. Greene endorsed a tripartite therapeutic approach, including SGLT2 inhibitors, nonsteroidal MRAs, and incretin-based therapies for those with obesity. These three pillars have been shown to improve clinical outcomes and patient-reported quality of life. Greene urged clinicians to “keep it simple” by following outcome trial evidence in CKM populations, while researchers continue probing the mechanistic roots of HFpEF to guide next-generation therapies.
4. Cardiovascular prevention: Dr. Nathan Wong discusses the role of risk scores, coronary calcium and opportunistic testing for cardiometabolic disease
In this evening talk, Dr. Nathan Wong (UCLA, UCI) highlighted cardiovascular (CV) risk assessment in people with diabetes and CV-kidney-metabolic (CKM) syndrome. He traced how diabetes has long been linked to elevated cardiovascular risk, but reviewed emerging evidence that challenges older assumptions of it as a cardiovascular risk equivalent, and the role of newer risk calculators designed to capture both traditional and diabetes‑specific predictors. He also connected these tools to the AHA’s Presidential Advisory on CKM, which emphasizes staged prevention and early, personalized risk stratification.
- Dr. Wong explored the evolving landscape of cardiovascular risk assessment in individuals with diabetes and cardiometabolic disease. He highlighted a meta-analysis (n=45,108) showing that diabetes alone confers a 44% lower coronary risk than prior myocardial infarction (MI), challenging the notion of diabetes as a risk for coronary heart disease. He reviewed several modern risk calculators, including SCORE2-Diabetes, which estimates 10-year cardiovascular risk in T2D by incorporating diabetes-specific variables like age at diagnosis, A1c, and eGFR, alongside traditional predictors like age, sex, smoking, systolic blood pressure (SBP), and lipid profile. He also discussed the development of the Diabetes Mellitus Risk Score (DMRS), derived from a pooled US cohort study (n=2,174) and validated in ARIC and ACCORDION, with key predictors including age, sex, A1c, creatinine, SBP, diabetes medication use, and smoking.
- Dr. Wong also emphasized the utility of the AHA PREVENT calculator for estimating 10- and 30-year risk of total CVD, ASCVD, and heart failure. The model also allows for refined risk stratification using optional inputs like uACR, A1c, and social deprivation index (SDI). Dr. Wong positioned PREVENT within the CKM Syndrome staging framework, noting that over 85% of US adults fall into CKM stages 1 or 2, underscoring the importance of early identification and personalized risk assessment. The PREVENT calculator provides a clear cutoff: individuals with a 10-year CVD risk ≥20% are automatically classified as stage 3 CKM. Dr. Wong emphasized that this is a pivotal transition point, as stage 3 represents subclinical disease or high predicted risk, where intervention intensity should escalate.
- In addition to risk scores based on clinical and social factors, Dr. Wong advocated for screening subclinical atherosclerosis particularly using coronary calcium testing that can be used as a diagnostic tool to stage ASCVD – from stage 0 to stage 4 based on calcium scores ranging from 0 to 1000 or more with more intensive recommendations for LDL-C lowering and other interventions with more advanced stages of disease. At 10 years, a baseline CAC >100 is associated with over a 7.5% risk of developing ASCVD events where there is net clinical benefit from statin use. In people with diabetes, CAC was similarly associated with ASCVD events, but in those with CAC=0 and diabetes duration under 10 years, 90% remain free of ASCVD event after 10 years. Importantly, CAC testing has been shown to improve CV outcomes. In the EISNER trial (n=2,137), those who underwent scans CAC screening had less increase in Framingham Risk Score (0.002 increase) than those who did not (0.7 increase; p=0.003). He looks forward to results of the ROBINSCA trial (n=28,928), which will assess five-year outcomes for people who screened with the Systematic COronary Risk Evaluation (SCORE), coronary calcium imaging, or no screening.
- Importantly, AI technology now allows for opportunistic testing of CAC and other cardiometabolic imaging parameters including cardiac chamber sizes and liver and visceral fat, which can be measured in those with existing scans (both gated and non-gated) often done for non-cardiac reasons. These measures improve the prediction of outcomes including ASCVD, heart failure, atrial fibrillation, and diabetes over standard assessments. More than 19 million US adults receive chest CT scans for other reasons providing substantial opportunity for assessment of cardiometabolic risk in those who would not otherwise be assessed.
5. Combination therapies for CKD and T2D: Dr. Jennifer Green spotlights clinical insights from the phase 2 CONFIDENCE trial
In this packed symposium, Dr. Jennifer Green (Duke University) highlighted findings from the phase 2 CONFIDENCE trial (n=784). Dr. Green began by sharing the four pillars of chronic kidney disease (CKD) and T2D, which include ACEi or ARBs, SGLT-2 inhibitors, nonsteroidal mineralocorticoid receptor agonist (ns-MRA), and GLP-1 RAs. However, less is known about approaches to combining therapies. Given that people with CKD and T2D are a high-risk population, study investigators aimed to mimic the approach taken to treat hypertension, for which multiple therapies would be initiated simultaneously to: (i) achieve faster and greater blood pressure (BP) reduction; (ii) reduce CV outcomes; and (iii) potentially improve tolerability and adherence. The CONFIDENCE study evaluated the efficacy and safety of a combination therapy of ns-MRA finerenone and SGLT-2 inhibitor empagliflozin in people with CKD and T2D, compared to finerenone or empagliflozin alone.
- As published in NEJM in June 2025, the study demonstrated that simultaneous initiation of finerenone deliver early and additive benefits on kidney health with favorable safety effects. At baseline, patients were 67 years old, with 25% being women. The mean systolic blood pressure (SBP) was 135 mmHg, BMI was 29 kg/m2, eGFR was 54 mL/min/1.73 m2, uACR was 579 mg/g, A1c was 7.3%, and mean serum potassium was 4.5 mmol/L. By medical history, 28% had ASCVD, 88% had hypertension, and 16% had diabetic retinopathy. Moreover, 98% were on ACEi/ARBs and 23% were on GLP-1 RAs. Dr. Green highlighted that the trial had a diverse group of participants, including 46% who were Asian, 44% White, and 8% Black. On trial design, Dr. Green noted that the primary endpoint was change in uACR given its association with kidney disease and feasibility of the trial. An outcomes trial, she added, would have required an enrollment of over 40,000 particpants with a follow up of at least three years.
- Simultaneous initiation of finerenone and SGLT-2 inhibitor conferred 52% reduction in uACR from baseline, which reflected a 32% greater reduction compared to empagliflozin monotherapy and 29% greater reduction in finerenone monotherapy. Moreover, 70% of patients achieved over 30% reduction in uACR with simultaneous initiation, compared to 52% each for the monotherapies. These benefits were consistent across baseline KDIGO categories (kidney risks) and GLP-1 RA use. Dr. Green commented that these results are consistent with a smaller study that compared combined dapagliflozin and balcinrenone treatment (33% reduction in uACR) to dapagliflozin monotherapy (23%).
- Safety. Potassium levels increased in the combination and the finerenone groups and returned to baseline after drug withdrawal. Dr. Green emphasized that the treatment-emergent hyperkalemia, however, was lower in the combination group by 18%, compared to the finerenone group alone. Moreover, there were very few hyperkalemia events leading to permanent discontinuation – one each in the respective groups. Dr. Green also highlighted that the combination therapy lowered SBP but caused few hypotensive events. She shared that more findings about intensive ambulatory blood pressure monitoring in a trial subgroup will be published in near future.
6. The impact of hypercortisolism on insulin resistance in people with diabetes
Dr. Vivian Fonseca (Tulane University) provided an overview of the impact of excessive cortisol levels on insulin resistance. Hypercortisolism is associated with a wide spectrum of comorbidities across the immune, reproductive, cardiovascular, and nervous systems. It exists as a continuum, with heterogeneous presentations and increasing risks of comorbidities, even in the absence of apparent features of hypercortisolism. For example, excessive levels of cortisol can cause “localized obesity,” characterized by the accumulation of visceral fat without obvious signs of obesity. Hypercortisolism ultimately contributes to insulin resistance, which drives metabolic syndromes affecting the liver, adipose tissue, and cardiovascular health. Therefore, studies have focused on how excess cortisol levels impair glucose metabolism and impact body systems that antidiabetic treatment targets. Recent findings have particularly looked at hypercortisolism in people with diabetes, leading to a consensus that it may be worth screening those with difficult-to-manage glycemic levels for underlying hypercortisolism.
- This effort eventually led to the CATALYST trial, for which Part 1 (n=1,113) revealed that nearly one-quarter of individuals with difficult-to-manage T2D have underlying hypercortisolism. In April 2025, published results revealed that hypercortisolism, defined by a post-dexamethasone suppression test (DST) cortisol level >1.8 µg/dL, was identified in 24% (252 of 1,057) of the study participants with T2D whose A1c remained >7.5% despite treatment with multiple glucose-lowering medications. The prevalence increased to 33% among participants with cardiovascular disease and to 37% among those on three or more blood pressure-lowering drugs.
- Dr. Fonesca concluded that hypercortisolism is closely related to insulin resistance. Given this relationship, he reviewed several studies that have shown insulin sensitizers and weight loss can counteract the effect of cortisol levels on insulin resistance. While not mentioned in depth during his presentation today, Part 2 (n=252) of the CATALYST trial investigated the efficacy of Korlym (mifepristone), a glucocorticoid receptor antagonist that decreases cortisol-mediated signaling and the clinical effects of hypercortisolism. Results showed that at Week 24, the mean A1c decreased from 8.6% to 7.1% with mifepristone, compared to a decrease from 8.4% to 8.4% with placebo. Overall, Dr. Fonesca emphasized that the treatment of hypercortisolism may improve insulin sensitivity, but the underlying mechanisms require further elucidation.