Changing the Course in Type One Diabetes 2025 Day #1 Highlights –
Executive Highlights
- Dr. Griffin Rodgers (NIDDK) and Dr. John Kaddis (City of Hope) opened the two-day conference, “Changing the Course in T1D,” by welcoming attendees to the NIH and igniting excitement for the groundbreaking research being conducted in type 1 diabetes (T1D). Today, thanks to initiatives like the Human Islet Research Network (HIRN), researchers have forged over 18,000 global connections across 109 institutions in 12 countries, fostering a robust ecosystem for discovery. HIRN’s mission to understand the mechanisms of beta cell loss in T1D and develop innovative strategies for prevention, protection, and replacement has not only advanced the science but also created career opportunities and funding mechanisms for researchers worldwide.
- Dr. Mark Atkinson (University of Florida) opened his discussion with a compelling narrative about the history of diabetes treatment, much of which laid the foundation for his 40 years of work in the field. Dr. Atkinson emphasized the dramatic evolution of T1D care, noting that while a cure remains elusive, advancements like home glucose monitors, rapid-acting insulin, insulin pumps, and continuous glucose monitors (CGMs) have significantly improved patients' quality of life. Despite these breakthroughs, Dr. Atkinson noted gaps in achieving therapeutic targets and the psychological and financial burdens faced by T1D patients.
- Dr. Julia Panzer (City of Hope) discussed how alpha cell glucagon secretion may be restored in T1D via paracrine signaling inhibition. She pointed out that glucagon secretion is the first and most important defense for hypoglycemia, and, in theory, T1D could be treated more aggressively with insulin if hypoglycemia was not a limiting factor. Studies have shown that glucagon secretion shows habituation (i.e., decreased secretion) when alpha cells are constantly stimulated. These findings have led to studies investigating whether inhibiting alpha cells via paracrine signaling and GIRK channels can “reset” these cells and restore glucagon secretion. While studies to date have only been conducted in pancreatic donor tissues, they have shown promise that alpha cells can return to higher levels of glucagon secretion after they are inactivated, or reset, by serotonin or somatostatin, which are secreted by beta and delta cells, respectively.
- In a session on the future of T1D research, UCSF’s Dr. Audrey Parent and Dr. Holger Russ (University of Florida) emphasized the importance of physiologically relevant modeling and cross-disciplinary collaboration as T1D is a multifactorial and complex autoimmune disease that remains poorly understood in its precise molecular and cellular mechanisms. Both speakers pointed to the need for a collaborative, iterative approach to accelerate innovation and refine strategies for prevention and treatment.
Table of Contents
-
Top Highlights
- 1. NIH welcomes hundreds of researchers, lauding the impact of collaboration in science
- 2. Research advances improve diabetes management, but T1D cure remains elusive
- 3. Restoring alpha cell glucagon secretion in T1D via paracrine inhibition with serotonin and somatostatin
- 4. Complexity of T1D necessitates collective, interdisciplinary approach
- 5. Microphysiological systems as a way to explore the complex immunopathogenesis of T1D
- 6. Up-regulation of HLA-B offers unique insight into T1D pathogenesis, with potential as an effective biomarker of disease progression
- 7. DYRK1A inhibitor harmine and GLP-1 RA exendin-4 in combination show synergistic effect in beta cell regeneration and potential for T1D reversal
- 8. Quick Take: Prof. Anette-Gabriele Ziegler on determinants of islet autoimmunity, primary prevention trials, and screening for T1D
Top Highlights
1. NIH welcomes hundreds of researchers, lauding the impact of collaboration in science
Dr. Griffin Rodgers (NIDDK) and Dr. John Kaddis (City of Hope) opened the two-day conference by welcoming attendees to the NIH and igniting excitement for the groundbreaking research being conducted in type 1 diabetes (T1D). Reflecting on the progress made over the past decade, Dr. Kaddis noted the transformative impact of global collaboration and community engagement. A decade ago, he said, the field faced significant challenges, including limited knowledge of early disease pathogenesis, an overreliance on mouse models, inadequate data sharing, and clinical trial endpoint failures[1]. Today, thanks to initiatives like the Human Islet Research Network (HIRN), researchers have forged over 18,000 global connections across 109 institutions in 12 countries, fostering a robust ecosystem for discovery. HIRN’s mission to understand the mechanisms of beta cell loss in T1D and develop innovative strategies for prevention, protection, and replacement has not only advanced the science but also created funding mechanisms for researchers worldwide as well as career opportunities. Dr. Kaddis emphasized that this vibrant, collaborative, and programmatically rich environment is critical for realizing the ultimate goal: preventing T1D before it begins.
Dr. Rodgers further highlighted the revolutionary transformation initiated by HIRN since its inception in 2014, which has dismantled research silos and fostered integration through specialized consortia such as CBDS, CMAS, CHIB, CTAR, and CC&BC. These efforts have been bolstered by the establishment of a coordinating center (HIREC) and the development of PanKbase, a critical resource for data sharing. He noted the pivotal role of the HPAC program, launched in 2016, which aimed to deeply phenotype the human pancreas and make these invaluable datasets accessible to the broader research community. Dr. Rodgers emphasized that, of course, HIRN was never designed to be stagnant but rather to evolve dynamically, expanding and contracting in response to the field’s ever-changing needs.
2. Research advances improve diabetes management, but T1D cure remains elusive
Dr. Mark Atkinson (University of Florida) opened his discussion with a compelling narrative about the history of diabetes treatment, much of which laid the foundation for his 40 years of work in the field. He began with a story about Dr. Frederick Allen, who pioneered early diabetes management by experimenting with starvation diets in animals and eventually applying these techniques to humans in combination with intense exercise (i.e., measuring the impact of an hour of running up and down the stairs following the only meal for the day). The breakthrough discovery of insulin by Drs. Frederick Banting and Charles Best was a turning point, transforming diabetes from a fatal disease into a manageable condition. Dr. Atkinson emphasized the dramatic evolution of T1D care, noting that while a cure remains elusive, advancements like home glucose monitors, rapid-acting insulin, insulin pumps, and continuous glucose monitors (CGMs) have significantly improved patients' quality of life.
- To illustrate the progress, Dr. Atkinson shared the story of Brenda Martinez, a Joslin Medalist diagnosed with T1D in 1957 at the age of six. Brenda’s journey reflected the monumental strides in diabetes management, from the rudimentary methods of urine testing and rigid insulin schedules to the flexibility afforded by modern CGMs and insulin pumps. Dr. Atkinson tied Brenda’s story to broader themes of research-driven discovery, emphasizing how innovations in the field have transformed lives within a single generation.
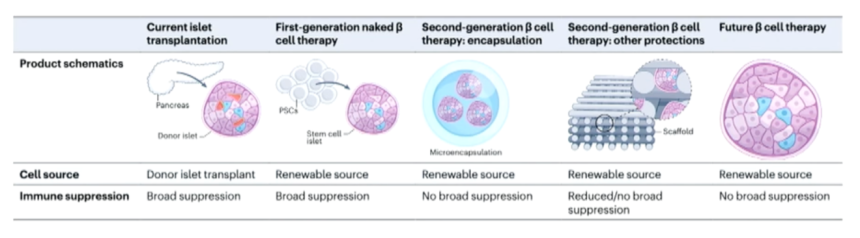
- Dr. Atkinson concluded his presentation with a discussion of current research priorities and ongoing challenges in T1D. He outlined the role of genetics in T1D susceptibility, the need for improved biomarkers, and the complexities of staging the disease to enable earlier interventions. He highlighted promising advances in immune therapies, such as Tzield, and the potential of islet transplantation and stem cell research. Despite these breakthroughs, Dr. Atkinson noted gaps in achieving therapeutic targets and the psychological and financial burdens faced by T1D patients. He emphasized the role of initiatives like the Human Islet Research Network (HIRN) in advancing understanding, improving management, and ultimately altering the trajectory of T1D.
3. Restoring alpha cell glucagon secretion in T1D via paracrine inhibition with serotonin and somatostatin
Dr. Julia Panzer (City of Hope, Duarte, California) discussed how alpha cell glucagon secretion may be restored in T1D via paracrine signaling inhibition. Dr. Panzer pointed out that glucagon secretion is the first and most important defense for hypoglycemia, and, in theory, T1D could be treated more aggressively with insulin if hypoglycemia was not a limiting factor. While there is a loss of beta cells in T1D, resulting in a lack of insulin, there is no significant loss of alpha cells or glucagon content. Therefore, Dr. Panzer said alpha cell dysfunction in T1D is likely related to defective glucagon secretion arising from a loss of paracrine signaling (i.e., cell-to-cell communication between alpha and beta cells). She explained that alpha cells are currently understood to alternate between secretory and inactive states. When alpha cells are electrically excited past a threshold, an action potential is triggered that leads to glucagon secretion. Studies have shown that glucagon secretion shows habituation (i.e., decreased secretion) when alpha cells are constantly stimulated. These findings have led to studies investigating whether inhibiting alpha cells via paracrine signaling with serotonin (found in beta cells) or somatostatin (found in delta cells) can “reset” these cells and restore glucagon secretion. While studies to date have only been conducted in pancreatic donor tissues, they have shown that alpha cells can return to higher levels of glucagon secretion after they are inactivated, or reset, by serotonin or somatostatin.
- On the mechanism of alpha cell inhibition, Dr. Panzer gave an overview of G protein-gated inwardly rectifying potassium (GIRK) channels. These channels found on alpha cells are activated by serotonin and somatostatin, among other neurotransmitters. Activation of these channels has been shown to inhibit glucagon secretion, and vice versa. To further support this finding, Dr. Panzer shared data showing that when GIRK channels are blocked, serotonin and somatostatin are no longer able to inhibit glucagon secretion.
- On next steps, Dr. Panzer discussed testing this in vivo, which may be challenging if mice do not have GIRK channels in their alpha cells. There is also potential for repurposing FDA-approved drugs and testing new compounds in T1D alpha cell donors.
4. Complexity of T1D necessitates collective, interdisciplinary approach
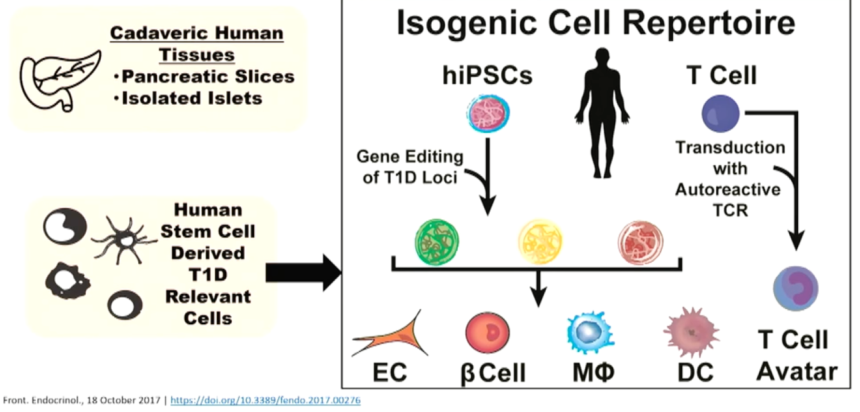
In a session on the future of T1D research, Dr. Audrey Parent (UCSF) and Dr. Holger Russ (University of Florida) emphasized the importance of physiologically relevant modeling and cross-disciplinary collaboration as T1D is a multifactorial and complex autoimmune disease that remains poorly understood in its precise molecular and cellular mechanisms. They agreed that leveraging novel technologies and disease models that integrate diverse human cell types has the potential to revolutionize the field, enabling researchers to stratify T1D more effectively and identify biomarkers for disease progression and intervention. Dr. Russ highlighted the importance of understanding the interactions between immune and beta cells and the triggers that amplify autoimmune responses, while Dr. Parent underscored the potential of tools like multicellular platforms and tissue-on-a-chip to replicate human physiology. Both speakers pointed to the need for a collaborative, iterative approach to accelerate innovation and refine strategies for prevention and treatment.
- Dr. Parent focused on the translational aspects of T1D research, stressing the need for tools that replicate the cellular environment and allow researchers to understand the interplay between beta cells and the immune system. She discussed the promise of immunomodulation and cell replacement therapies to restore and protect beta cell function. However, she also acknowledged challenges, such as delivering drugs with specificity and matching treatments to individual disease stages. Dr. Parent highlighted the role of networks like HIRN in driving forward innovation through collaborative research, which she believes is critical to bridging the gap between laboratory discoveries and patient care.
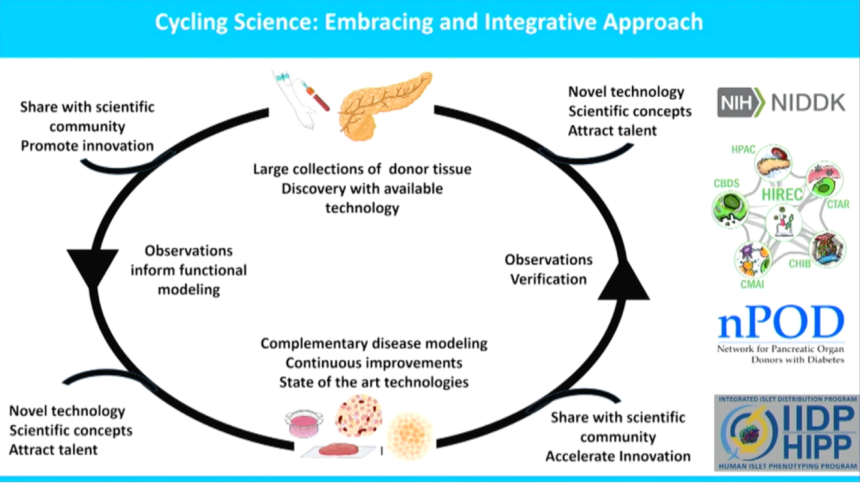
- Dr. Russ, on the other hand, delved deeper into the underlying mechanisms of T1D, focusing on the abundant pancreatic changes and cellular stress factors associated with disease onset. He stressed the need to study how genetic risk factors and cellular interactions contribute to disease progression. Dr. Russ highlighted the importance of breaking down scientific siloes and fostering team science to investigate the interplay of immune and beta cells. He also outlined a roadmap for improving patient care, which includes in-depth phenotyping of pancreatic tissues, expanding research to other relevant organs, and validating findings through large datasets. Dr. Russ concluded by advocating for a continuous cycle of research and refinement, emphasizing the importance of collaboration and innovation in unraveling the complexities of T1D.
5. Microphysiological systems as a way to explore the complex immunopathogenesis of T1D
Dr. Cherie Stabler (University of Florida) explored advancements in microphysiological systems (MPS) for studying T1D, focusing on the immunopathogenesis of the disease and the limitations of current tools. T1D's pathogenesis involves complex, human-specific pathways, including antigen-presenting cell (APC) activity, adaptive immune responses, and soluble gradients that direct cellular interactions. While animal models like NOD mice provide foundational insights, they lack full translational relevance to human systems. Existing in vivo and in vitro methods, such as humanized mouse models and 2D cell cultures, have limitations, including high costs, limited temporal insights, and non-physiological conditions.
- To address these challenges, Dr. Stabler described a novel “Diabetes-on-a-Chip” platform that aims to replicate human pancreatic environments and immune interactions in 3D systems. Vascularized mini-organs (VMOs) and microphysiological systems that support islet-immune integration offer improved beta cell function and robust insulin secretion. These platforms enable advanced imaging, controlled microenvironments, and real-time tracking of T-cell motility and antigen-specific interactions, providing key insights into immune cell behavior and islet viability. The shift to 3D models and the integration of biosensors highlight the potential for translational research to offer a more accurate and scalable approach to studying T1D and evaluating immune therapies.
6. Up-regulation of HLA-B offers unique insight into T1D pathogenesis, with potential as an effective biomarker of disease progression
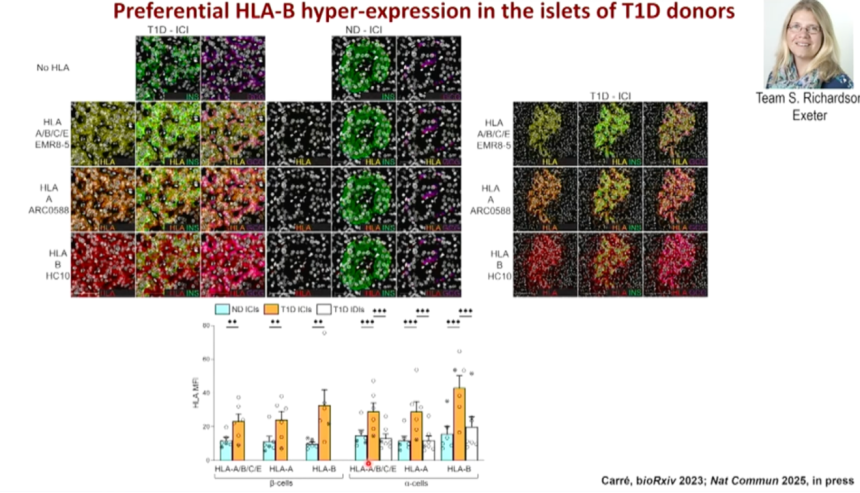
With a presentation title that garnered laughs (“The Menage à Trois between Beta Cells, T Cells, and Interferons”), Dr. Roberto Mallone’s (Universite Paris Cite, France) presentation examined the interplay between beta cells, T cells, and interferons in T1D. He focused on the immunological and molecular dynamics underpinning disease progression. While autoimmune islet-reactive CD8+ T cells circulate in all individuals in a largely naïve state, they are enriched in the pancreas in T1D patients, where they exhibit a distinct T1D-specific signature. This signature involves the upregulation of HLA class I molecules, driven by interferons (IFNs), particularly IFN-alpha, which enhances the antigenic visibility of beta cells. Current research in this area has leveraged innovative in situ tetramer staining and in vitro models to demonstrate that IFN-alpha-treated beta cells present neo-antigenic peptides, many of which are post-translationally modified and derived from insulin granule proteins.
- Dr. Mallone shared key findings that highlight the role of HLA-B ligands in skewing peptide presentation and preferentially activating HLA-B-restricted CD8+ T cells, which exhibit heightened cytotoxicity toward beta cells. In contrast, alpha cells, despite similar antigenic visibility, remain largely unaffected, suggesting distinct immunological vulnerability. The study identifies a so-far neglected repertoire of antigenic peptides presented by HLA-B that recruits a distinct set of autoimmune CD8+ T cells that may play a major pathogenic role in T1D, and provide better circulating biomarkers of ongoing autoimmunity against inflamed beta cells and novel immunotherapeutic targets.
7. DYRK1A inhibitor harmine and GLP-1 RA exendin-4 in combination show synergistic effect in beta cell regeneration and potential for T1D reversal
Dr. Adolfo Garcia-Ocaña (City of Hope) highlighted the role of DYRK1A inhibition in beta cell proliferation in diabetes and potentially even T1D reversal. As background, DYRK1A is a protein kinase that phosphorylates NFAT transcription factors, which then inhibits beta cell proliferation. DYRK1A, therefore, offers promise as a therapeutic target for beta cell inhibition. Indeed, harmine, a naturally occurring alkaloid compound found in some plants, has been shown to inhibit DYRK1A and stimulate beta cell proliferation. For multiple years now, there has been excitement around even greater proliferation when harmine is administered in combination with a GLP-1 RA, namely exendin-4 (see our coverage from the Beta Cell Summit 2023 and nPOD 2019). Dr. Garcia-Ocaña pointed out that this synergistic effect also means lower doses of harmine can be used, which may be important given that some alkaloids, including harmine, may become toxic to humans at high levels.
- Recent research on harmin and exendin-4 combination therapy shows their efficacy in vivo. Research by Rosselot, C. et al in Science Translational Medicine in July 2024 demonstrated that mice implanted with human islets show increased beta cell volume when treated with harmin alone and an even greater increase in volume when treated with both harmin and exendin-4. As with in vitro studies, exendin-4 alone had no effect on beta cell volume. It is worth noting that alpha cell volume did not increase, suggesting a beta cell-specific effect. Beta cell volume was observed to persist for at least one month after treatment. A phase 1 trial published in Journal of Psychopharmacology in October 2024 has shown that harmine can be safely administered up to a certain dose without adverse events. At higher doses, harmin was associated with vomiting, drowsiness, and psychoactive effects.
- On T1D reversal, harmin and exendin-4 in combination have also been shown to reduce beta cell death caused by cellular stress and cytokines. Dr. Garcia-Ocaña shared unpublished data showing that treatment has been associated with decreased inflammation, cytokine activity, and immunogenicity markers. In NOD (non-obese diabetic) mice with early-onset T1D, treatment with an anti-CD3 antibody (e.g., teplizumab), harmine, and exendin-4 was shown to restore normoglycemia.
8. Quick Take: Prof. Anette-Gabriele Ziegler on determinants of islet autoimmunity, primary prevention trials, and screening for T1D
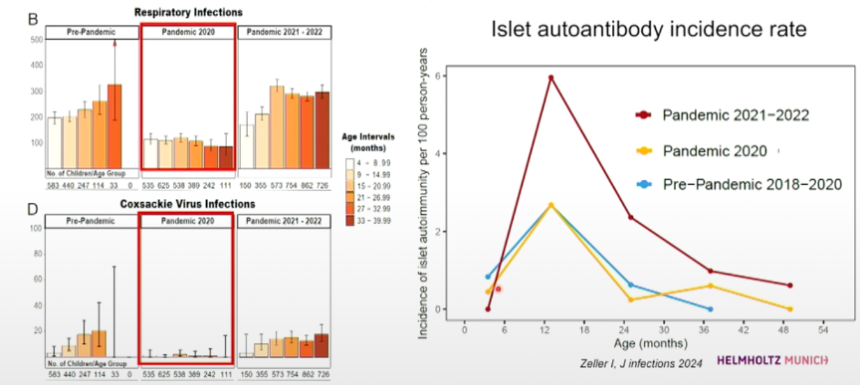
Islet autoimmunity, a precursor to T1D, exhibits a peak incidence in early childhood, particularly between one to two years of age, as revealed through longitudinal birth cohort studies such as BABYDIAB, TEDDY, and POinT. This period is characterized by heightened vulnerability due to genetic, metabolic, and environmental factors. Per Prof. Anette-Gabriele Ziegler (Helmholz Munich Diabetes Center, Germany), genetic predisposition plays a significant role, though its influence diminishes with age, while alterations in glucose metabolism, including beta-cell stress and injury, coincide with seroconversion. Early life inflammation and infection, particularly viral respiratory infections and prolonged enterovirus B exposure, significantly increase autoimmunity risk, with evidence suggesting that inflammation enhances autoreactivity through mechanisms such as cytokine production and immune activation. The COVID-19 pandemic provided natural insights, with reduced infections correlating with decreased autoimmunity risk, while SARS-CoV-2 infections elevated the risk significantly, especially in infants. Maternal influences, including protective epigenetic modifications, also modulate risk, underscoring the importance of genetic screening and early prevention strategies such as those implemented in the GPPAD platform.
--by Monica Oxenreiter, Elaine Young, and Kelly Close
[1] See “Macrogenics-Eli Lilly's teplizumab fails to meet phase 3 primary efficacy endpoint – October 22, 2010” as one example and “Tolerx and GSK Announce Poor Efficacy in DEFEND-1 – March 14, 2011” as another