AACE 2026 Day #3 Highlights –
Executive Highlights
- AACE 2026 continued today in lively Las Vegas, with Friday bringing high energy across the program and strong engagement as the community looks ahead to next year’s meeting in San Diego, California. Sessions spanned GLP‑1/GIP innovation, T1D cell therapy, MASLD/MASH care, obesity pharmacotherapy, and pediatric metabolic health.
- Dr. Aaron Kowalski (Breakthrough T1D) offered an inspiring and forward‑looking overview of cell therapy in T1D, arguing that scalable cures are moving meaningfully closer to clinical practice. He highlighted the limitations of current AID systems, the promise of stem‑cell–derived islets, immune‑evasive and targeted immunomodulatory approaches, and the manufacturing and policy infrastructure needed for broad adoption.
- Dr. Anne Komé (University of North Carolina) delivered a highly practical session on microdosing GLP‑1 RAs, outlining how fractional dosing, interval extension, and dose‑splitting are emerging as clinician‑guided strategies amid shortages, high costs, and expanding indications. She emphasized safety boundaries and urged clinicians to avoid compounded products as patient‑driven workarounds increase.
- In obesity and liver‑focused sessions, Dr. Domenica Rubino (Washington Center for Weight Management and Research) and Dr. Nadege Gunn (Iterative Health) underscored obesity as a multisystem disease and elevated liver assessment as essential metabolic care. In addition, pediatric discussions highlighted the need for earlier pharmacotherapy, structured evaluation, and attention to MASLD/MASH risk in youth.
- Industry‑sponsored sessions showcased expanding therapeutic options across obesity and liver disease. Dr. Carlos Campos (UT Health Science Center) presented Foundayo (orforglipron) as a once‑daily oral GLP‑1 RA enabling earlier obesity intervention, while Drs. Priya Jaisinghani (NYU Langone) and Julio Gutierrez (Scripps Health) highlighted resmetirom’s role in treating noncirrhotic MASH with F2-F3 fibrosis.
See the conference agenda, registration, and our preview.
Table of Contents
- 1. Cell therapies in T1D move closer to clinic, as Breakthrough T1D CEO Dr. Aaron Kowalski outlines path to scalable cures
- 2. Microdosing GLP‑1 RAs as a practical strategy amid access barriers
- 3. Obesity as a multisystem disease: Why liver assessment is essential in metabolic care
- 4. Lilly’s Foundayo shows meaningful weight loss and positions oral GLP-1 RAs for earlier obesity intervention
- 5. Liver health: The new frontier in cardiometabolic management
- 7. Pediatric obesity management: Pharmacotherapy, surgery, and breaking down barriers
Top Highlights
1. Cell therapies in T1D move closer to clinic, as Breakthrough T1D CEO Dr. Aaron Kowalski outlines path to scalable cures
In an inspiring morning session, Dr. Aaron Kowalski (Breakthrough T1D) reframed the long-standing narrative that a “cure is always around the corner,” arguing that cell therapies in T1D are now meaningfully approaching clinical reality. Drawing on both rapid scientific progress and his own 40+ years living with T1D, Dr. Kowalski positioned cell therapy as a scalable, next-generation solution that could complement today’s most advanced technologies. His talk spanned from disease staging and persistent unmet needs to manufacturing challenges and policy barriers, ultimately underscoring that success will depend as much on clinical adoption and access as on scientific innovation.
- Despite major advances in AID and CGM, T1D management remains fundamentally constrained by non-physiologic insulin delivery, leaving significant unmet need. Dr. Kowalski pushed back on the notion that current tools are “good enough,” stating that subcutaneous insulin delivery cannot replicate endogenous beta cell function. Even with the most advanced AID systems, individuals continue to experience hyperglycemia, hypoglycemia, and glycemic variability that contribute to long-term complications. Real-world data reflect this gap. Average A1c in young adults remains above 8.0%, with fewer than one-third achieving <7.0%, and outcomes are worse in lower socioeconomic and underrepresented populations. Importantly, he reframed success beyond glycemic metrics, noting that people with T1D often prioritize the constant cognitive and emotional burden of disease over A1c itself, a point he illustrated with a personal anecdote of overnight device failures. Taken together, he acknowledged that the field must rethink risk-benefit tradeoffs, as novel therapies may offer meaningful reductions in
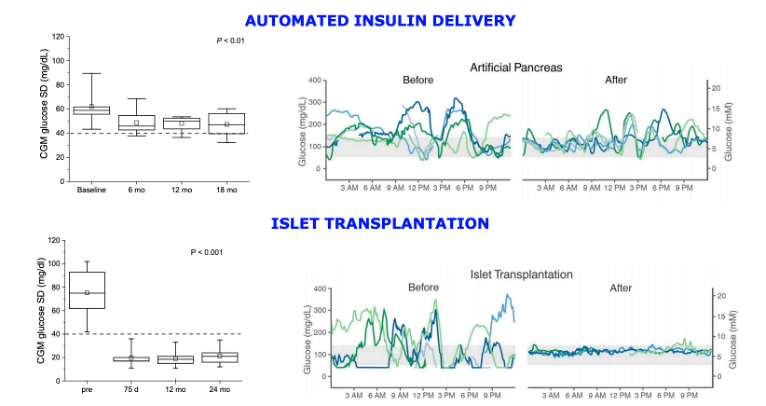
Iboth burden and complications. - Cell replacement is already clinically validated, but donor-derived islet transplantation approaches have been limited by scalability and immunosuppression. Dr. Kowalski reminded the audience that “cure” is not theoretical. Islet transplantation has restored near-normal glycemia and insulin independence for decades, often lasting up to 10 years. However, reliance on donor pancreases and chronic immunosuppression has restricted use to a small, high-risk population, with only ~5,000 procedures performed globally over 25 years. The only FDA-approved therapy, Cell Trans’ Lantidra, and ongoing efforts such as Vertex’s stem cell-derived islet program zimislecel, use intraportal infusion to restore physiologic insulin and glucagon secretion with far greater glycemic stability than AID systems. Still, access remains tightly limited, often to individuals with severe hypoglycemia. Dr. Kowalski criticized these criteria as overly restrictive. He emphasized that expanding eligibility and eventually moving beyond donor-derived cells will be critical for broader impact.
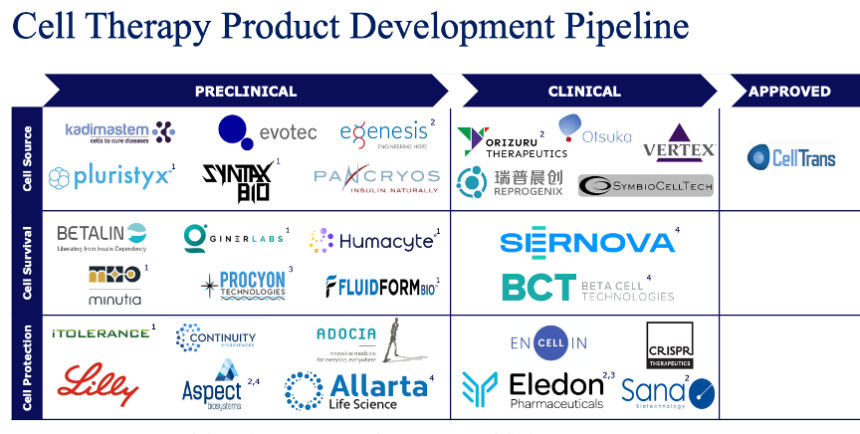
- The next generation of cell therapy is focused on three core challenges: (i) immune protection; (ii) scalable cell manufacturing; and (iii) durable engraftment. A major theme of his talk was the shift toward renewable, stem cell-derived islets paired with safe, more targeted immunomodulation. Dr. Kowalski highlighted emerging therapies such as Eledon’s anti-CD40 ligand, tegoprubart, which may replace traditional calcineurin inhibitors with a significantly improved safety profile. He also pointed to similar efforts from companies like Sanofi developing next-generation immunotherapies with favorable tolerability profiles. In parallel, gene-editing approaches from companies such as Sana Biotechnology aim to create “immune-evasive” cells, with early human data showing sustained C-peptide production without immunosuppression, which he highlighted as very encouraging. Encapsulation strategies remain under investigation to physically shield cells, but maintaining adequate oxygenation continues to be a challenge.
- As efficacy becomes increasing clear, scalability and delivery are the primary barriers to widespread adoption. While stem cell-derived islets can now be generated reliably, Dr. Kowalski described manufacturing at scale as the “chicken noodle soup problem,” straightforward in small batches, but complex to industrialize. With ~1.6 million individuals with T1D in the US alone, the field must address production capacity, quality control, and supply chain logistics. Breakthrough T1D is actively partnering organizations such as the Advanced Regenerative Manufacturing Institute (ARMI) and Cedars-Sinai Biomanufacturing Center (CSBC) to accelerate scalable production. At the same time, clinical delivery models are evolving, with a shift toward “hub-and-spoke” systems and specialized centers of excellence to perform procedures.
- Clinical adoption, policy alignment, and patient demand will ultimately determine how quickly these therapies reach practice. Dr. Kowalski closed by emphasizing that regulatory pathways, reimbursement, and clinician engagement will be critical. He suggested that patient demand may be underestimated, especially as safer immunomodulatory approaches reduce perceived risk. Breakthrough T1D is actively preparing for this transition through Project ACT, which focuses on clinician education, clinical trial navigation tools, and efforts to standardize care pathways, including the development of specialized training programs. With Vertex’s pivotal trial ongoing and multiple parallel approaches advancing, Dr. Kowalski projected that key readouts could arrive within the next 12-24 months, raising the possibility that cell therapies may begin entering clinical practice within just a few years.
2. Microdosing GLP‑1 RAs as a practical strategy amid access barriers
In this popular session, Dr. Anne Komé (University of North Carolina) delivered a highly practical presentation on microdosing GLP-1 RAs, framing it as a tailored strategy emerging in response to unprecedented demand, expanding indications, and persistent access barriers. She opened by reviewing the rapid evolution of the GLP‑1 RA class, from early exenatide products in 2005 to today’s dual and triple agonists, and noted that indications have broadened far beyond T2D to include obesity, cardiovascular risk reduction, OSA, MASH, and CKD. She emphasized that this therapeutic boom has coincided with “the best of times and the worst of times.” Superior efficacy and shifting societal attitudes have driven massive uptake, but shortages beginning in late 2021, manufacturing issues with semaglutide autoinjectors, high cash prices, and insurance exclusions have forced clinicians to adopt unconventional strategies. She highlighted that weight regain after therapy discontinuation remains a real concern, with an 11.6% regain in the STEP‑1 trial of semaglutide and 14% in the SURMOUNT‑4 trial of tirzepatide, further motivating interest in flexible dosing approaches.
- Dr. Komé then outlined the rationale and mechanics of microdosing, which includes using fractional or lower‑than‑labeled doses to improve tolerability, extend supply, or navigate cost and coverage challenges. She explained that semaglutide multi‑dose pens contain 72 unnumbered “clicks”, enabling precise titration from as low as 0.06 mg (9 clicks), and that tirzepatide vials allow dose‑splitting in 0.05-0.60 mL increments.
- She illustrated these dosing options with real‑world cases. One patient with T2D who successfully restarted semaglutide after a 30‑day washout using microdoses of 0.0625 mg and 0.125 mg for two weeks each, followed by 0.25 mg dosing until follow-up. She also described the case of a long‑term responder who extended her tirzepatide interval from 7 to 10 to 14 days, maintaining her weight within 5 pounds
lbof goal. She noted that mathematical modeling suggests patients may retain ~75% of weight loss when shifting from weekly to every two-week dosing, though GI symptoms may recur more prominently after longer intervals.
- She illustrated these dosing options with real‑world cases. One patient with T2D who successfully restarted semaglutide after a 30‑day washout using microdoses of 0.0625 mg and 0.125 mg for two weeks each, followed by 0.25 mg dosing until follow-up. She also described the case of a long‑term responder who extended her tirzepatide interval from 7 to 10 to 14 days, maintaining her weight within 5 pounds
- On cost, Dr. Komé stated that even with cash‑pay programs bringing semaglutide as low as $199 for starter pens and tirzepatide vials at $299-$449 per month, many patients still face abrupt coverage losses, quantity limits, or pharmacies that only stock initiation doses. Against that backdrop, she showed how fractional dosing can stretch supply without new prescriptions, help patients avoid compounded products, and maintain therapy when insurance exclusions hit mid‑year. She highlighted one case of a 76‑year‑old man who lost his $0 tirzepatide copay and, together with his wife, also on tirzepatide under the same plan, turned to single‑dose vials to stay on treatment. He drew up roughly 10 mg weekly while his wife drew 2.5 mg from the same 15 mg vial, a workaround that kept both on therapy. By March 2026, the patient even asked to switch to the new multi‑dose pens. Her message was that cost pressures aren’t theoretical; they shape adherence, safety, and outcomes in real time, and microdosing offers a structured alternative to the unsafe workarounds patients increasingly attempt on their own.
- During Q&A, one question focused on whether patients who cannot tolerate injectable GLP‑1 RAs could “split the dose” of the oral formulations, and Dr. Komé was unequivocal that she would not recommend splitting Rybelsus or Foundayo tablets because disrupting the SNAC absorption technology would render them ineffective. She added that alternate‑day oral dosing may eventually be studied, but for now she advises sticking to FDA‑approved daily dosing if patients can afford it.
- She closed by reviewing the “dos and don’ts” of microdosing, stressing the need for extensive counseling, aseptic technique, and avoidance of compounded incretin products, which have been linked to safety events and prompted FDA action earlier this year. Dr. Komé noted that many of the questions she now receives come from patients influenced by telehealth weight‑loss programs like Ro, WeightWatchers, and Hims & Hers, as well as Reddit and TikTok threads promoting unsupervised dose‑splitting, which is why clinicians need a clear grasp of what to do and not to do with microdosing before patients attempt unsafe workarounds on their own.
- She cautioned that microdosing carries risks, including contamination, dosing errors, uncertain cardiorenal benefit at subtherapeutic doses, and should be avoided in patients with visual, dexterity, or cognitive limitations. Still, she underscored that for the right patient, microdosing can improve tolerability, reduce waste, extend supply without new prescriptions, and offer a safer alternative to unregulated compounded products. Her final message: as GLP‑1 RA use expands across metabolic and non‑metabolic conditions, clinicians must be equipped to guide patients through off‑label strategies with precision, safety, and transparency.
3. Obesity as a multisystem disease: Why liver assessment is essential in metabolic care
In this Boehringer Ingelheim-sponsored breakfast product theater, Dr. Domenica Rubino (Washington Center for Weight Management and Research) and Dr. Nadege Gunn (Iterative Health) outlined the multisystem burden of obesity and the central role of liver health, particularly MASLD and MASH, in metabolic care. Dr. Rubino opened by positioning obesity as a chronic, progressive disease marked by excessive fat accumulation and ectopic fat deposition across multiple organs. She emphasized that obesity is a systemic condition with multi‑organ impact. She highlighted the rising prevalence of obesity: with 43% of adults living with obesity in 2020, the prevalence is projected to reach 61% by 2050. Adults with obesity have markedly higher risks for cardiovascular disease and an 8‑fold higher risk of T2D. She also underscored that adults with obesity have a 5.5 times greater risk of developing MASLD and are 2.3 times more likely to have at‑risk MASH, setting the stage for why liver assessment must be integrated into obesity care.
- Dr. Gunn then walked through the modern definition, epidemiology, and clinical consequences of MASLD and MASH. She reiterated that MASLD is defined by a ≥5% hepatic steatosis plus ≥1 metabolic risk factor, and that MASH represents the aggressive form, characterized by steatosis, inflammation, and ballooned hepatocytes. She emphasized that 70% of individuals with T2D have MASLD, while 34% of adults with obesity have MASH. She highlighted a diagnostic gap, given that 76% of adults with obesity have undiagnosed liver disease, and explained why the fibrosis stage is the clinical “tipping point.” Adults with MASH typically progress one fibrosis stage every seven years, but some progress far more rapidly. She also reviewed data showing that in older adults with T2D, obesity substantially amplifies liver risk. She highlighted the role of FIB‑4 score as a first‑line tool, and noted that higher scores predict not only liver events but also cardiovascular and all‑cause mortality.
- Dr. Rubino closed by returning to holistic, collaborative obesity care and the central role of primary care in screening, risk stratification, and coordinated management. She emphasized that lifestyle intervention remains foundational and that weight reduction decreases visceral and ectopic fat stores that drive metabolic dysfunction. She highlighted data from a MASH cohort study (n=261) showing that even <5% weight loss produced histologic improvements in 35% of patients, while ≥10% weight loss yielded 100% steatosis improvement and 90% resolution of steatohepatitis. She noted that fibrosis regression is more difficult, reinforcing the need for early detection before advanced fibrosis develops.
- On multidisciplinary care, Dr. Rubino stressed that primary care clinicians are uniquely positioned to integrate obesity treatment, MASLD/MASH screening, and multidisciplinary referral pathways. She emphasized that even solo practitioners can build an external multidisciplinary approach by identifying reliable hepatologists, endocrinologists, cardiologists, GI specialists, dietitians, behavioral therapists, and physical therapists to support patients. She stated that every patient with obesity should have their liver assessed, and restoring health requires coordinated, individualized, whole‑person care.
4. Lilly’s Foundayo shows meaningful weight loss and positions oral GLP-1 RAs for earlier obesity intervention
In a Lilly-sponsored product theater, Dr. Carlos Campos (University of Texas Health Science Center) introduced the newly approved Foundayo (orforglipron) as part of a push toward earlier intervention in obesity care, noting that the condition remains significantly under-treated despite its recognition as a chronic, progressive disease. He highlighted the biologic challenges of weight loss, describing a “hormonal conspiracy” driven by metabolic adaption and set-point defense that makes sustained weight reduction difficult without pharmacologic support.
- Against this backdrop, Foundayo, Lilly’s once-daily oral, non-peptide GLP-1 RA, was positioned as a more convenient alternative to injectable therapies, with no food or water restrictions. In the phase 3 ATTAIN-1 trial (n=3,127), the highest dose achieved ~11.1% mean weight loss at 72 weeks, with more than half of participants ≥10% weight loss, alongside improvements in cardiometabolic markers. Safety findings were consistent with the GLP-1 RA class, with gastrointestinal adverse events most common and discontinuation rates of ~6%-10%. Dr. Campus also pointed to LillyDirect as a streamlined pathway to improve access through transparent pricing and simplified prescribing. Collectively, the session highlighted Foundayo as both a therapeutic advance and a potential catalyst for shifting obesity care toward earlier, more accessible intervention.
5. Liver health: The new frontier in cardiometabolic management
In this morning session, Dr. Aman Rajpal (Alameda Health) focused on translating current evidence into practical strategies for identifying, screening, and managing MASLD/MASH in routine clinical care. Using real-world cases, the discussion emphasized that patients with cardiometabolic risk factors, such as obesity, prediabetes or T2D, dyslipidemia, and conditions like PCOS, should be proactively screened for liver health. A key takeaway from the session was that normal liver enzymes do not rule out disease; even “normal” ALT values can mask underlying pathology. First-line risk stratification with noninvasive tools like FIB-4 remains essential due to its accessibility, but Dr. Rajpal urged clinicians to recognize its limitations, particularly in younger patients where it may underestimate fibrosis risk (given the overweighting of age in lowering FIB-4 scores). When suspicion remains, additional testing with elastography or serum biomarkers is necessary.
- Dr. Rajpal presented several case studies to describe how to apply the recently updated guidelines. The goals of MASH treatment extend beyond the liver to include weight reduction, glycemic management, lipid management, and blood pressure optimization, alongside liver-specific outcomes like fibrosis regression and reduced liver fat. Ultimately, effective care requires a coordinated, multi-modal approach: identifying high-risk patients early, using layered diagnostic tools, addressing underlying drivers such as obesity, and tailoring therapy to reduce both hepatic and cardiovascular complications.
6. Madrigal product theater: The role of liver-directed therapy in MASLD/MASH
The Madrigal-sponsored product theater, led by Drs. Priya Jaisinghani (NYU Langone) and Julio Gutierrez (Scripps Health), centered on the clinical role of Rezdiffra (resmetirom), a thyroid hormone receptor-β agonist approved for adults with noncirrhotic MASH and moderate-to-advanced fibrosis (F2-F3). Dr. Gutierrez described the fibrosis stage as a “critical inflection point” in disease progression, associated with substantially elevated risks of liver-related morbidity and mortality, up to 10-17 times higher than those without fibrosis. Given the often silent nature of MASLD and MASH, including normal liver enzyme levels in many cases, they underscored the importance of proactive, risk-based screening strategies, particularly in populations with T2D and other cardiometabolic conditions. The discussion reinforced current guideline recommendations to use noninvasive tests such as FIB-4 as an initial population-level screening tool, followed by elastography or specialty referral for those at intermediate or high risk.
- Dr. Gutierrez discussed clinical trial data from the MAESTRO-NASH phase 3 study, which demonstrated that resmetirom achieved statistically significant improvements in fibrosis without worsening steatohepatitis at 52 weeks, alongside favorable trends in liver enzymes and lipid parameters. Drs. Jaisinghani and Gutierrez also addressed real-world implementation challenges, including underdiagnosis, limited specialist access, and the need for endocrinologists and primary care clinicians to take a more active role in screening and management. While cost and access remain barriers, the presenters noted expanding insurance coverage and patient support programs and suggested that the future of MASH treatment will likely involve combination pharmacotherapy and long-term disease management strategies.
7. Pediatric obesity management: Pharmacotherapy, surgery, and breaking down barriers
Dr. Alaina Vidmar (Children’s Hospital Los Angeles) delivered an insightful session on pediatric obesity management that was both practically grounded and clinically rich. A central theme was the limited translatability of adult data to pediatric populations, underscored by her reminder that “these are not small adults,” and the need to reevaluate evidence, access, and treatment contexts the children and adolescents.
- Pharmacologic therapy increasingly centers on GLP-1 RAs and emerging dual agonists. Daily liraglutide has demonstrated meaningful BMI reductions in children aged 6-12, and weekly semaglutide has shown similar efficacy to adolescents. Tirzepatide has shown both glycemic and weight benefits in youth with T2D, reflecting an emerging principle that more potent agents earlier in the disease course may yield more favorable outcomes. For patients where injectables are inaccessible, oral agents are effective either separately or in combination. Naltrexone/bupropion, when used with psychiatric consultation, offers the added dual benefit of addressing both weight and mental health. For hypothalamic obesity syndromes, setmelanotide and genetic testing are opening the door to genotype- and phenotype-specific approaches.
- For adolescents with severe obesity, laparoscopic sleeve gastrectomy has emerged as a highly effective and safe modality, with growing long-term data in pediatric cohorts. Outcomes in youth with T2D are particularly striking, with many achieving remission or significant improvement, especially compared to the limited durability of pharmacological therapy alone. Safety data indicate low perioperative mortality and acceptable complication rates, with long-term nutritional risks that are manageable through structured follow-up. Despite this, bariatric surgery remains dramatically underutilized in eligible adolescents. Dr. Vidmar’s team at the Children’s Hospital in Los Angeles has started a bariatric surgery program, working to normalize sleeve gastrectomy as a proven, guideline-supported intervention rather than a last resort.
- Across all treatment modalities, substantial challenges continue to constrain implementation and equity.Coverage for GLP-1 RAs and emerging incretin-based agents is highly variable by state, payer, and indication, and even when covered, prior authorization denials and supply interruptions are common. Off-label prescriptions often encounter pharmacy skepticism and payer pushback. Weight stigma compounds these barriers. Dr. Vidmar’s practical response has been to build infrastructure to directly address these challenges: EHR prescription templates pre-specifying “pediatric obesity,” documented family consent for off-label use, and proactive notes on out-of-pocket payment options and GoodRx coupons where relevant. Her broader message was that clinicians are active partners in dismantling stigma and advocating for improved care access.
--by Milenka Men, Riya Chatterjee, Kayla Mathieu, Monica Oxenreiter, and Kelly Close