EASL 2025 Day #3 Highlights –
Executive Highlights
- The EASL (European Association for the Study of the Liver) Congress accelerated into Day #3, featuring new results on Akero’s FGF21 analog efruxifermin and a themed focus on MASH cirrhosis. We look forward to further results tomorrow during a number of Late Breaker presentations.
- Dr. Mazen Noureddin (Houston Research Institute) presented phase 2b trial results (SYMMETRY) for efruxifermin, a bivalent fibroblast growth factor 21 (FGF21) analog for MASH. Results were simultaneously published in NEJM. 39% of participants saw fibrosis improvement, while no statistical significance of primary outcomes was observed. To date, therapies that target fibrosis in cases of MASH cirrhosis have not demonstrated efficacy. Based on subgroup findings, the study’s 50-mg dose has been selected for a confirmatory phase 3 study in participants with compensated cirrhosis, which is currently enrolling (NCT06528314). This study will include an assessment of liver-related outcomes and all-cause mortality. The high proportion of phase 2b study participants with T2D (80%) suggests that MASH-related findings from this work will have particular relevance for people with T2D, and we will continue to follow the phase 3 trial.
- In an intriguing presentation, Prof. Cyrielle Caussy (Lyon University, France), assessed the correlation, independent of traditional risk factors, between the severity of MASLD with prevalence of chronic kidney disease (CKD) in patients with T2D and/or obesity. She described chronic kidney disease (CKD) as a commonly-neglected complication in patients with metabolic disorders. The study involved people with T2D and/or obesity (n=787) and used non-invasive diagnostic tools such as FibroTest and the Enhanced Liver Fibrosis (ELF) test for quantifying liver disease severity. A subsection of patients also underwent liver biopsy for additional histological confirmation. The proportion of patients with CKD increased with MASLD severity. With high risk of advanced fibrosis (AF) associated with MASLD, over 50% of participants also had CKD. With moderate risk, the proportion was approximately 40%, and with low risk, about 35% of patients also had CKD. The study suggests that MASLD may contribute to CKD progression, not simply coincide with it.
- Prof. Philip Newsome (King’s College London, England) began an early morning session with a difficult debate: is it better to treat the liver or treat global metabolic health? He reminded the audience that the majority of patients with MASLD or MASH have co-existing obesity, insulin resistance, T2D, or dyslipidemia, and that cardiovascular disease (CVD) accounts for 29% of mortality in MASH. Given that fibrosis treatment may be less impactful than cardiovascular treatment on overall outcomes, then metabolic management is a priority in MASH treatment. However, broader metabolic therapies will not resolve liver disease in all cases, hence the need for liver-directed therapies. Prof. Newsome noted therefore that patients with liver disease and diabetes require a holistic approach to treatment. He emphasized durability, adherence, and global scalability of all treatments, believing that both liver-directed therapies and metabolic therapies are essential for MASLD management.
For the latest from Amsterdam, be sure to monitor our resource hub. Check out our preview for a look at what’s coming on the final, exciting day!
Table of Contents
-
Top Highlights
- 1. Phase 2b trial results for Akero’s FGF21 analog efruxifermin: 39% saw fibrosis improvement; no statistical significance of primary outcome
- 2. The severity of MASLD is associated with chronic kidney disease in patients with T2D and/or obesity
- 3. Prof. Philip Newsome on the difference between treating liver health specifically or broader metabolic health
- 4. The evolving landscape of drugs for MASH cirrhosis
- 5. Does MASLD increase the risk of cardiovascular disease above and beyond shared risk factors?
- 6. Jean-Pierre Benhamou Clinical State-of-the-Art Lecture: The promise and pitfalls of non-invasive testing
Top Highlights
1. Phase 2b trial results for Akero’s FGF21 analog efruxifermin: 39% saw fibrosis improvement; no statistical significance of primary outcome
Dr. Mazen Noureddin (Houston Research Institute) presented phase 2b trial results (SYMMETRY) for efruxifermin, a bivalent fibroblast growth factor 21 (FGF21) analog for MASH. Results were simultaneously published in NEJM. While previously thought to be irreversible, a reduction in fibrosis has been observed in cirrhosis caused by viral infection. Reducing fibrosis is key to improving liver-related outcomes. To date, therapies that target fibrosis in cases of MASH cirrhosis have not demonstrated such improvement.
- Study design. The study was a phase 2b, randomized, placebo-controlled, double-blind trial of adults (n=181) with MASH and biopsy-confirmed compensated cirrhosis. Patients received efruxifermin 28 mg or 50 mg subcutaneously once daily, or placebo. The primary outcome was a reduction of fibrosis of one stage or greater without the worsening of MASH by Week 36. Secondary outcomes included: (i) a reduction of fibrosis of one stage or greater without the worsening of MASH by 96 weeks; (ii) MASH resolution; (iii) fibrosis markers; and (iv) liver injury markers. 154 patients remained in the intervention group by Week 36, and 134 completed the full 96 weeks.
- Baseline characteristics. All patients either had T2D (80% of participants), or two components of metabolic syndrome (obesity, dyslipidemia, elevated blood pressure, or elevated fasting glucose level). Average BMI was 36 kg/m2, and 27% of participants also used GLP-1 RAs.
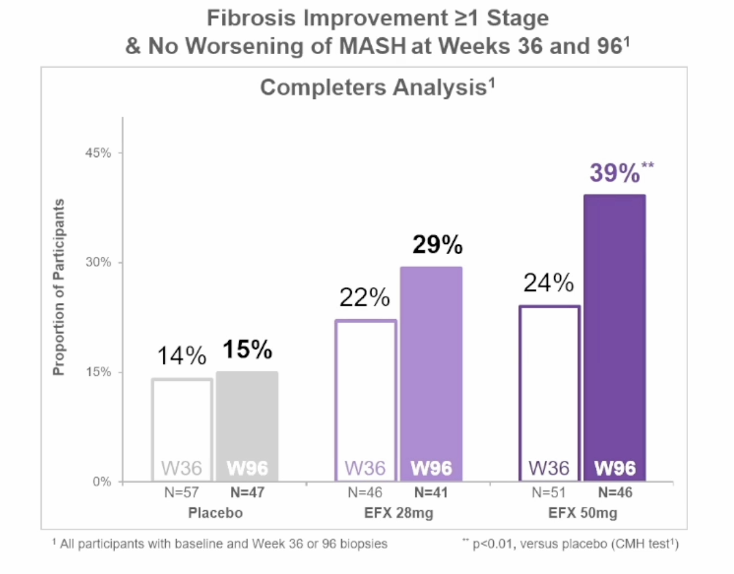
- Results. 18% of patients in the 28-mg efruxifermin group demonstrated improvement (p=0.62) in fibrosis reduction of one stage or greater, 19% in the 50-mg efruxifermin group (p=0.52), and 13% in the placebo group. Differences between intervention and placebo were not significant in the primary endpoint. At Week 96, one of the secondary study endpoints, a reduction in fibrosis without worsening of MASH occurred in 29% of the 50-mg efruxifermin group, 21% of the 28-mg efruxifermin group, and 11% in placebo. No formal hypothesis testing of secondary outcomes was conducted, so no statistical conclusions could be drawn in this case. Gastrointestinal adverse events were more common with efruxifermin; most events were mild or moderate with 19% of participants reporting diarrhea in the 28-mg group and 30% in the 50-mg group.
- Analysis. In this trial, the use of efruxifermin did not result in a significant reduction in fibrosis without the worsening of MASH at Week 36. However, in the subgroup analysis of participants who completed the 96-week study period, it appears that the 50-mg dose may be beneficial for fibrosis reduction at 96 weeks. Efruxifermin was also associated with improvements in histological findings, noninvasive markers of liver injury and fibrosis, and markers of glucose and lipid metabolism. Based on the subgroup findings, the 50-mg dose has been selected for a confirmatory phase 3 study in participants with compensated cirrhosis, which is currently enrolling (NCT06528314). This study will include an assessment of liver-related outcomes and all-cause mortality. The high proportion of phase 2b study participants with T2D (80%) suggests that MASH-related findings from this work will have particular relevance for people with T2D, and we will continue to follow the phase 3 trial.
2. The severity of MASLD is associated with chronic kidney disease in patients with T2D and/or obesity
In this intriguing presentation, Prof. Cyrielle Caussy (Lyon University, France), assessed the correlation, independent of traditional risk factors, between the severity of MASLD with prevalence of chronic kidney disease (CKD) in patients with T2D and/or obesity. She described chronic kidney disease (CKD) as a commonly-neglected complication in patients with metabolic disorders. The study involved people with T2D and/or obesity (n=787) and used non-invasive diagnostic tools such as FibroTest and the Enhanced Liver Fibrosis (ELF) test for quantifying liver disease severity. A subsection of patients also underwent liver biopsy for additional histological confirmation.
- The proportion of patients with CKD increased with MASLD severity. With high risk of advanced fibrosis (AF) associated with MASLD, over 50% of participants also had CKD. With moderate risk, the proportion was approximately 40%, and with low risk, about 35% of patients also had CKD. This relationship held even after adjusting for age, sex, and race, suggesting that MASLD may be playing a more direct role in kidney injury, independent of these demographic risk factors.
- Degree of obesity was not consistently accounted for in baseline risk correction, but trends indicated that worsening liver disease and CKD co-occur more frequently in those with overlapping metabolic dysfunction.
- The study suggests that MASLD may contribute to CKD progression, not simply coincide with it. This strengthens the hypothesis that metabolic liver disease is possibly a driver of multi-organ damage in patients with T2D and obesity. This finding has implications for integrated disease management strategies and highlights the urgent need for further research using non-invasive markers and large-scale trials. Identifying and treating MASLD early may help prevent or slow CKD progression, reducing the burden of end-organ complications in patients with diabetes and obesity.
Future directions include a four-year follow-up study focused on kidney outcomes to better understand the long-term impact of MASLD on renal function. Prof. Caussy also discussed incorporating genetic profiling and gut microbiome analysis to explore deeper mechanistic links, particularly looking into toxic lipids and systemic inflammation.
3. Prof. Philip Newsome on the difference between treating liver health specifically or broader metabolic health
Prof. Philip Newsome (King’s College London, England) began an early morning session with a difficult debate: is it better to treat the liver or treat global metabolic health? He reminded the audience that a majority of patients with MASLD or MASH have co-existing obesity, insulin resistance, T2D, or dyslipidemia, and that cardiovascular disease (CVD) accounts for 29% of mortality in MASH. Given that fibrosis treatment may be less impactful than cardiovascular treatment on overall outcomes, overall metabolic management is needed in MASH treatment. Weight loss has demonstrated significant improvement, with up to 90% of patients achieving resolution of steatohepatitis after >10% body weight loss in a 2015 study. There have since been a number of studies exploring MASH-related benefits of drugs with weight-loss benefits.
- In June 2024, the phase 2 SYNERGY trial demonstrated liver outcomes driven by metabolic improvement through the use of tirzepatide. Using 5-15 mg doses, 44-62% of patients demonstrated resolution of MASH and no worsening of fibrosis after 52 weeks, compared to 10% in placebo. A decrease of ≥1 fibrosis stage and no worsening of MASH in 51-55% of patients, depending on dosing, was also observed compared to 30% in placebo.
- In the April 2025 phase 3 ESSENCE trial, semaglutide 2.4 mg (weekly) demonstrated resolution of steatohepatitis with no worsening of liver fibrosis in 63% of patients compared to 34% in placebo at 72 weeks. Reduction in liver fibrosis with no worsening of steatohepatitis occurred in 37% of patients in the intervention group compared to 22% in placebo.
- Addressing “the root of the problem,” weight loss demonstrated significant improvement to liver outcomes. This is in conjunction with the additional cardiovascular benefits provided by these drugs, including protective effects on heart function and the prevention of adverse cardiac remodeling.
- Broader metabolic therapies may not resolve liver disease in some cases. Prof. Newsome addressed patients with liver disease who may not respond to GLP-1 RA treatment, as well as those who discontinue treatment due to side effects, which therefore necessitates liver-targeted therapies. He also pointed to a particular subsection of patients that demonstrated weight loss when taking GLP-1 RAs, but no improvement to liver disease, saying that it may not be sufficient to target insulin resistance and weight loss alone in this population. Advanced fibrosis and cirrhosis may also require additional treatment, as therapies such as semaglutide have not demonstrated an improvement in fibrosis or MASH resolution in patients with cirrhosis.
- However, Prof. Newsome sees great promise in combined GLP-1/glucagon dual receptor agonists, where glucagon acts directly on the liver to promote fatty acid oxidation and reduce lipid synthesis in hepatocytes, in addition to the systemic benefits of the GLP-1 RA aspect. Different ratios of this combination may provide the option of personalized therapies, such as pemvidutide (1:1), cotadutide (5:1), and survodutide (8:1), three combination therapies currently in development. He proAs an example, Prof. Newsome said that a high-glucagon-GLP-1 ratio drug may not be ideal for patients with diabetes due to the impact on glycemia and may choose a therapy with a lower glucagon:GLP-1 ratio while still capturing its liver benefits. A 2024 study demonstrated that survodutide led to improvement in liver fibrosis with no worsening in MASH for 30-42% of patients with fibrosis, compared to 18% in placebo. He also noted the promise of FGF21 analog efruxifermin, which demonstrates improvement in liver cirrhosis, with full results from a phase 2b trial also presented at EASL Day #2.
- Prof. Newsome noted that patients with liver disease and diabetes require a holistic approach to treatment as compared to patients with more advanced fibrosis but fewer related co-morbidities. The management of metabolic syndrome should be a core tenent of MASLD treatment, and Prof. Newsome continued to reflect on trends towards weight-regain following GLP-1 RA discontinuation and the challenges that this may introduce for long-term treatment. He emphasized durability, adherence, and global scalability of all treatments, believing that both liver-directed therapies and metabolic therapies are essential for MASLD management.
4. The evolving landscape of drugs for MASH cirrhosis
Dr. Mary Rinella (University of Chicago) presented on the evolving landscape of drugs for MASH cirrhosis, sharing what she considered cause for excitement and many opportunities still to come. Cirrhosis is a late-stage form of severe liver scarring, with elevated risk of complications related to fibrosis, which describes any degree of liver scarring. Over 80% of patients with cirrhosis have impaired glucose tolerance and about 30% of the population with cirrhosis has T2D. Therapies that aim to improve fibrosis within the context of MASH cirrhosis have not demonstrated efficacy to date. Dr. Rinella described the cirrhosis population as “as wide and more complex” as the rest of the fibrosis spectrum combined, which complicates research as well as disease management. She highlighted three therapies in late-stage development with particular promise for improving cirrhosis.
- Results of the FGF21 analog efruxifermin phase 2b cirrhosis trial (SYMMETRY) were presented just hours after Dr. Rinella’s talk, demonstrating that the use of efruxifermin did not result in a significant reduction in fibrosis without the worsening of MASH at Week 36. In a subgroup analysis of participants who completed the 96-week study period, 39% of the participants taking 50-mg dose demonstrated statistically significant fibrosis improvement.
- Belapectin, a galectin-3 inhibitor, demonstrated a statistically significant improvement in the number of participants with new varices[1] at Week 78, but failed to demonstrate significance of other metrics in its phase 2 cirrhosis trial. Prior presentations by study author Dr. Naim Alkhouri (Arizona Liver Health) have suggested that the distinct mechanism of action of belapectin as a galectin 3 inhibitor positions it favorably as a candidate for combination therapy in MASH cirrhosis.
- In a phase 3 open label compensated cirrhosis study arm, resmetirom demonstrated an absolute change in vibration controlled transient elastography (VCTE) score of -6.7 kPa, which was statistically different from baseline. VCTE scores range from 2 kPa in healthy individuals to 75 kPa in the most severe cases of liver cirrhosis.
- Dr. Rinella also sees broad opportunity to come, with a number of candidates for MASH cirrhosis in the pipeline. See below for a summary of these candidates.
Drug Candidate | Population | Primary Endpoints | Estimated Completion |
| Resmetirom | Compensated Cirrhosis (biopsy and/or NIT) N~700 2 arms - 3:1 allocation | Time to First clinical outcome: all-cause mortality, liver transplant, MALO, MELD progression | Q1 2027 |
| Pegozafermin | Compensated Cirrhosis (biopsy-proven) N~762 2 arms | ≥1 stage fibrosis improvement at Month 24 Time to first clinical outcome event | Q3 2028 |
| Efruxifermin | Compensated Cirrhosis N~1150 2 arms - 2 cohorts | Time to first clinical outcome event ≥1 stage fibrosis improvement w/o worsening of MASH at Week 96 (cohort 1 only) | Q4 2029 |
| Survodutide | Compensated Cirrhosis N~1590 2 arms - 2:1 allocation | Time to first clinical outcome event: all-cause mortality, liver transplant, MALO, MELD progression, progression to clinically significant portal hypertension | Q3 2029 |
Table 1: Phase 3 Programs in Compensated MASH Cirrhosis (Prof. Mary Rinella, EASL 2025)
5. Does MASLD increase the risk of cardiovascular disease above and beyond shared risk factors?
In a systematic review and meta-analysis, Dr. Alexander Hung (University College London, England) examined to what degree MASLD increases the risk of cardiovascular disease (CVD) independently of the effect of shared metabolic risk factors, such as T2D, obesity, hypertension, and dyslipidemia. After controlling for the presence of common metabolic conditions, evidence suggested that MASLD may be a contributing factor in CVD progression. However, the strict exclusion criteria applied somewhat limited the number of eligible studies, with a total of nineteen studies included. The analysis supported growing signs that MASLD increases the risk of cardiovascular disease, yet it remains uncertain whether MASLD is a true independent risk factor or a marker of broader metabolic dysfunction.
- All studies utilized imaging, elastography or biopsy to diagnose MASLD, with none relying upon ICD codes or non-invasive scores. However, whilst confounding variables such as age, sex, presence of hypertension or diabetes, BMI, HDL-cholesterol and triglycerides were considered in all studies, some including smoking and severity of liver disease were not consistently measured. All studies included non-MASLD control groups, and only longitudinal prospective or retrospective cohort studies were included.
- MASH was not clearly distinguished or significantly underrepresented in the majority of the studies. Seeing as MASH may carry a higher risk profile than MASLD alone, this weakens the study’s ability to generalize its findings across the full spectrum of liver disease severity.
- Overall, given the complex interplay between liver disease, T2D, and obesity, a strong argument exists for closer integration of liver health into cardiovascular risk assessments.
6. Jean-Pierre Benhamou Clinical State-of-the-Art Lecture: The promise and pitfalls of non-invasive testing
Prof. Annalisa Berzigotti (University of Bern, Switzerland) delivered a moving and informative tribute lecture discussing the promise and pitfalls of non-invasive testing (NITs). She paid tribute to an emeritus, trailblazing hepatologist, Prof. Jean-Pierre Benhamou who served as secretary of EASL from 1967 to 1970 and president in 1993. He is celebrated for his skills as a clinician, in teaching, and as an administrator. He passed away in 2008. Prof. Berzigotti highlighted the expanding contribution of NITs at a time when liver biopsy, historically the gold standard of testing, is being progressively replaced by safer, scalable diagnostic methods.
- Liver fibrosis is the strongest predictor of outcomes in chronic liver disease, independent of etiology. Although biopsy is beneficial for explaining disease progression, it is invasive, carries risks, and is subject to sampling errors. As metabolic-associated liver disease surges around the world, there remains an urgent need for non-invasive, affordable, and reproducible methods that can diagnose at-risk individuals early and track disease longitudinally.
- Non-invasive tests are grouped into several categories, among them the blood-derived biomarkers (e.g., FIB-4 and ELF), imaging methods like elastography (encompassing FibroScan and MR elastography), and more recently multi-omic data approaches. Of particular note is that elastography has revolutionized hepatology with a rapid and reliable method of estimating liver stiffness as an indicator for fibrosis as well as portal hypertension. Tests such as transient elastography have shown high predictive accuracy for advanced fibrosis and cirrhosis and are now incorporated into international clinical guidelines.
- One key concept introduced was the "rule of five." This concept uses a system of thresholds for platelet count and liver stiffness to determine the risk of complications, including clinically significant portal hypertension. Those showing a stiffness of >25 kPa or low platelet counts are at greater risk of developing portal hypertension and will need further evaluation. For patients in the intermediate "gray zone" (15–20 kPa), further testing, i.e., measurement of spleen stiffness or certain blood-based scores (e.g., the VITRO score), can further stratify risk.
- Prof. Berzigotti also highlighted the fact that NITs are not just beneficial for diagnosis, but also for monitoring and determining prognosis. Serial measurements over time may guide treatment decisions and forecast disease progression.
- Although NITs are effective, their application requires clinical judgment in consideration of the prevalence of the condition in the population, disease setting, and individual patient characteristics, said Prof. Berzigotti. Recent advances in artificial intelligence and omics are promising, but still in their infancy with challenges related to cost, complexity, and validation.
- Non-invasive testing has transformed the field of hepatology, offering a patient-friendly, scalable, and clinically meaningful approach to liver disease management. Yet, as Professor Berzigotti underscored, these instruments are meant to complement, and not replace the physician's judgment, experience, and familiarity with the patient.
--by Nour Khachemoune, Andrew Serrano, Monica Oxenreiter, and Kelly Close
[1] Varices are swollen blood vessels in the esophagus or stomach, which often occur in patients with cirrhosis and may be used as an indication of disease severity.