Arrowhead Pharma announces positive interim phase 1/2 results for RNA interference therapy in obesity –
RNA interfering therapies ARO-INHBE and ARO-ALK7 enhance visceral and liver fat mass loss; full trial results expected in 2026
California-based Arrowhead Pharmaceuticals announced this morning positive interim data from ongoing phase 1/2a trials evaluating its RNA interference therapies, ARO-INHBE (n=120) and ARO-ALK7 (n=126), for the treatment of obesity. See press release, webinar, and slides.
These candidates offer a novel mechanism to weight loss that is especially promising among people with insulin resistance at baseline. In the webinar, President and CEO Dr. Chris Anzalone, CMO and Head of R&D Dr. James Hamilton, and Prof. Carel le Roux (University College Dublin, Ireland) shared insights into the current obesity landscape, therapeutic rationale for targeting Activin E-ALK7 axis, trial results, and the key takeaways.
Table of Contents
- ARO-INHBE and ARO-ALK7 target a pathway that regulates fat storage
- ARO-INHBE reduces serum Activin E levels as intended and lowers visceral fat by 9.9% with a single dose
- When added to tirzepatide, ARO-INHBE doubles weight loss in people with obesity and T2D
- ARO-ALK7 monotherapy confers 14% reduction in visceral fat at Week 8
- Both candidates demonstrated favorable safety and tolerability profiles
- Prof. Carel le Roux highlights the future direction of obesity therapies in the webinar
- Relatively new competitive landscape involving Activin E suppression
- Close Concerns’ Questions
- Appendix A: Arrowhead proposes offering up to $625 million, consisting convertible senior notes and common stock
- Appendix B: Webinar Q&A
ARO-INHBE and ARO-ALK7 target a pathway that regulates fat storage
The therapeutic mechanisms involve ARO-INHBE and ARO-ALK7, which interfere with the Activin E-ALK7 pathway that regulates energy homeostasis in adipose tissue. In phase 1/2a trials, ARO-INHBE monotherapy led to visceral fat reduction by 10% (versus none with placebo) and liver fat loss by 39% (versus a 7.4% increase in placebo). Likewise, ARO-ALK7 demonstrated up to 14% weight loss (versus a 0.5% increase with placebo) at Week 8. Interestingly, in people with diabetes, ARO-INHBE and tirzepatide combination therapy conferred 9.4% body weight loss at Week 16 (versus 4.8% with tirzepatide alone) and enhanced fat distribution. Both candidates were well-tolerated and most adverse events were mild.
Specifically, ARO-INHBE inhibits hepatic expression of the INHBE gene which codes for Activin E, while ARO-ALK7 reduces the expression of the ACVR1C gene which codes for Activin receptor-like kinase 7 (ALK7). Both Activin E and ALK7 are known to regulate energy homeostasis in adipose tissue. Downregulation of these proteins has been associated with improved fat distribution and metabolic health markers in humans and in preclinical models.
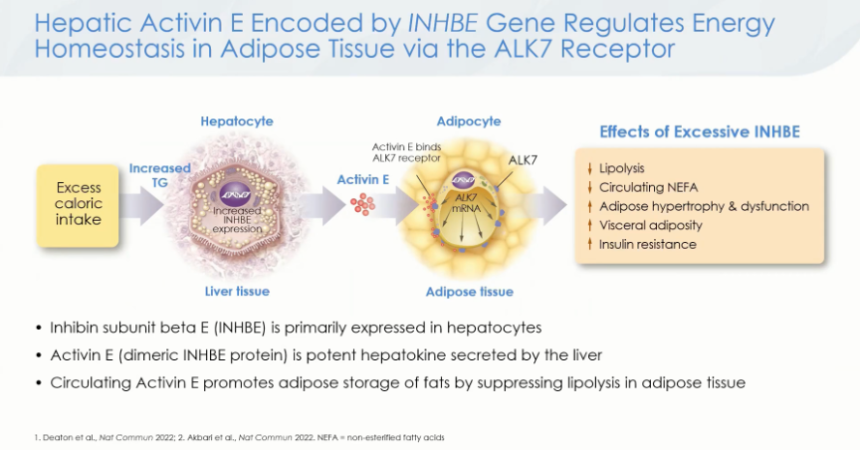
Figure 2. Activin E-ALK7 pathway regulates lipolysis in adipose tissue
Source: Arrowhead Pharmaceuticals KOL Webinar about ARO-INHBE and ARO-ALK7, slide 24
As shown in the figure above, the Activin E-ALK7 pathway stimulates fat storage in adipocytes and regulates visceral adiposity in the liver. Upon excess caloric intake, Activin E is expressed in liver tissue and secreted into the blood. Activin E then binds to the ALK7 receptor on adipocytes, which slows lipolysis (the breakdown of fat), stimulates adipocyte hypertrophy (an increase in size and remodeling of fat cells), and ultimately increases visceral adiposity and insulin resistance.
Previous studies have found that loss-of-function mutations of the INHBE gene are associated with improved waist-to-hip ratios and lower cardiometabolic risks in humans. Hence, ARO-INHBE and ARO-ALK7 therapies aim to disrupt the Activin E-ALK7 pathway to improve fat distribution and health.
ARO-INHBE reduces serum Activin E levels as intended and lowers visceral fat by 9.9% with a single dose
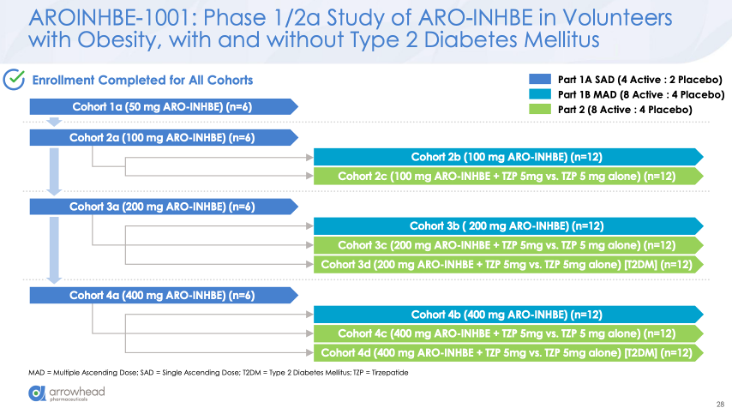
The phase 1/2a AROINHBE-1001 trial (n=120) evaluates ARO-INHBE in adults with obesity (Part 1) and in adults with obesity, with or without T2D, who are also taking tirzepatide (Part 2). The trial is ongoing, with completion expected in May 2026.
Figure 2. Trial design of the phase 1/2a AROINHBE-1001 study
Source: Arrowhead Pharmaceuticals KOL Webinar about ARO-INHBE and ARO-ALK7, slide 28
In Part 1, participants were 42 years old at baseline, with ~62% being female and 60% white. On average, baseline Activin E level was ~500 pg/mL, weight was 104 kg (229 lbs), BMI was 36 kg/m2, and A1c was 5.4%.
Single doses of ARO-INHBE conferred a dose-dependent reduction in Activin E levels by up to 85%. Moreover, doses lowered visceral fat by 9.9% (versus no change with placebo) and liver fat by 38.6% (versus a 7.4% increase) at Week 16. Meanwhile, total lean mass increased by 3.6% (versus a 1.6% increase) from baseline. Repeat doses of ARO-INHBE further lowered visceral adipose tissue, achieving a 13.5% reduction (versus 2.1% increase) at Week 16.
When added to tirzepatide, ARO-INHBE doubles weight loss in people with obesity and T2D
Arrowhead also shared interim results of Part 2 of the trial for participants with obesity and T2D (n=24). At baseline, participants were 52 years old, with half being female and 58% being white. Mean weight was 103 kg (227 lbs), BMI was 36.6 kg/m2, A1c was 7.4%, and Activin E was 662 pg/mL. Consistent with previous studies, higher Activin E levels were associated with insulin resistance, a high BMI, and a higher waist circumference in people with diabetes.
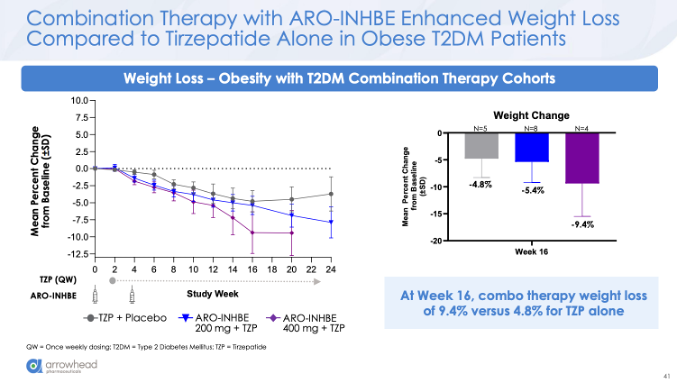
At Week 16, ARO-INHBE again conferred up to an 84% reduction in serum Activin E levels (versus none with tirzepatide alone) and, impressively, up to 9.4% body weight loss (versus 4.8%). Moreover, ARO-INHBE enhances visceral fat loss (23% versus 19% with tirzepatide alone), total fat loss (15% versus 8%), and liver fat loss (77% versus 48%) by Week 12.
Dr. Hamilton commented that, while preliminary, these findings show that ARO-INHBE is on track to “meet or beat” the fat loss seen in the SURPASS-3 MRI substudy. Moreover, targeting Activin E may be more efficacious in people with insulin resistance, as insulin is a strong inhibitor of lipolysis in adipose tissues. This candidate has the potential to address the lower weight loss often achieved among people with diabetes.
Figure 3. ARO-INHBE and tirzepatide confer greater weight loss at Week 16
Source: Arrowhead Pharmaceuticals KOL Webinar about ARO-INHBE and ARO-ALK7, slide 41
ARO-ALK7 monotherapy confers 14% reduction in visceral fat at Week 8
In the phase 1/2a AROALK7-1001 trial (n=126), ARO-ALK7 was similarly evaluated in adults with obesity (Part 1) and in adults with obesity, with or without T2D, who are taking tirzepatide (Part 2). Enrollment for Part 2 is ongoing, and the study is expected to complete in July 2026.
In Part 1, participants were 39 years old on average, with 72% being female and 64% white. Baseline weight was 105 kg (231 lbs), BMI was 36.6 kg/m2, and A1c was 5.4%. As intended, ARO-ALK7 decreased ALK7 gene expression by up to 88% (as measured by Alk7 mRNA). Interestingly, a single dose of ARO-ALK7 conferred up to a 13.6% reduction in visceral fat (versus a 0.5% increase with placebo) at Week 8.
During Q&A, Dr. Hamilton said that future work studying combination therapy will increase cohort sizes to increase statistical power. The company also plans to increase study duration to study plateauing versus continued fat mass loss.
Both candidates demonstrated favorable safety and tolerability profiles
ARO-INHBE was well-tolerated both as a monotherapy and in combination treatment with tirzepatide. Most treatment-emergent adverse events were mild, and none led to study discontinuation. GI event rates were similar between combination therapy and tirzepatide monotherapy. Importantly, laboratory measurements for liver enzymes (ALT), A1c values, and lipid levels remained stable in monotherapy and improved in combination with tirzepatide.
Likewise, ARO-ALK7 monotherapy was well-tolerated, with most treatment-emergent adverse events being mild. No clinically significant laboratory trends, such as A1c or ALT/AST changes, were found.
Prof. Carel le Roux highlights the future direction of obesity therapies in the webinar
While therapeutic advancements like the development of semaglutide and tirzepatide revolutionized obesity management, obesity remains a heterogeneous disease with multiple subtypes. For example, although BMI and CV risk are linearly associated, many people with low BMI present with high CV risk and vice versa. Prof. le Roux emphasized that future obesity care should recognize this heterogeneity and focus on visceral fat reduction, which is known to drive cardiometabolic disease. Combination therapies can further improve therapeutic efficacy and health outcomes. See figure below for an overview of the candidates in development.
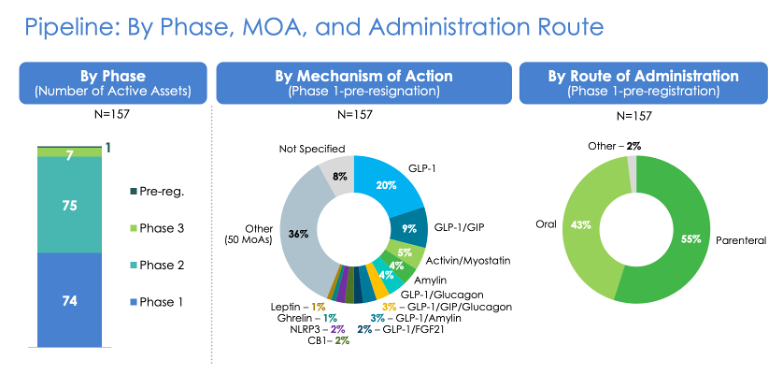
Source: Arrowhead Pharmaceuticals KOL Webinar about ARO-INHBE and ARO-ALK7, slide 19
Looking forward, Arrowhead plans to enroll more study participants and extend the follow-up period to one year to assess the drug’s durability. It also aims to launch phase 2b studies as soon as possible to evaluate their potential as add-on or maintenance therapies to tirzepatide or other GLP-1 RAs.
Relatively new competitive landscape involving Activin E suppression
Similar therapeutic approaches have historically only been preclinical – for example, iBio offered Activin E and myostatin as promising targets for obesity in animal studies and in preclinical studies in January 2025, though human studies have not yet been initiated. We imagine this approach to obesity management will continue to represent a promising target for the future.
Close Concerns’ Questions
- What patient population might benefit the most from this therapy, and how does Arrowhead hope to identify this subgroup?
- What other cardiometabolic benefits might ARO-INHBE and ARO-ALK7 offer?
- Given that both ARO-INHBE and ARO-ALK7 interfere with the Activin E-ALK7 pathway, how might they compare to each other with respect to efficacy, safety, and tolerability?
- What does Arrowhead envision the dosing frequency and titration scheme for ARO-INHBE and ARO-ALK7 to be?
- A recent study found that Activin E protects the liver from MASLD by inhibiting lipolysis in white adipose tissue. How might ARO-INHBE and ARO-ALK7 impact liver health?
- How do ARO-INHBE and ARO-ALK7 affect people with and without diabetes differently?
Appendix A: Arrowhead proposes offering up to $625 million, consisting convertible senior notes and common stock
Following interim results, Arrowhead announced plans for two independent public offerings on January 6, 2026: (i) $500 million of convertible senior notes due 2032; and (ii) $200 million of common stock.
Due to strong demand, Arrowhead upsized its offerings the next day, now consisting of: (i) $625 million (up 25%) of convertible senior notes due 2032; and (ii) 3.1 million shares priced at $64.50 per share. The net proceeds will be ~$608.2 million for the notes and ~$188.3 million for common stock.
$42.8 million of the note offering proceeds will be used to pay capped call transactions, while the rest would be used for R&D, manufacturing, commercialization, and more.
Appendix B: Webinar Q&A
Q (Mr. Prakash Agarwal, Cantor Fitzgerald): First question on the lack of weight loss with the INHBE monotherapy arm. Biologically, what could be the reason on why the monotherapy is not seeing weight loss while you are seeing good weight loss for the combo arm, especially in the obesity plus type 2 diabetes cohort?
And a quick clarification for anybody, when I look at the combo, the activin E reduction across the two doses is similar. The weight loss trajectory is a little bit different and it starts happening around Week 16. Can you confirm if there were any outliers in the 400-milligram cohort? Asking just because it's a small sample right now.
A (Dr. James Hamilton, CMO and Head of R&D): This is still at the hypothesis stage, but I would wager a guess that in people without diabetes their Activin E regulatory system is not as ramped up or as dysregulated as what we're seeing in the diabetic patients. And that may be why we're seeing more of a signal in the diabetics. That's our explanation right now. I think that probably needs to be more thoroughly tested. But that's the best answer I can give you right now for why we're seeing more of a signal in the diabetics.
Then for your second question: the lack of a knockdown dose response, at least based on the serum levels. It doesn't always tell us what's going on in the liver. There may be other mechanisms at play beyond just measuring the serum Activin E levels. We've seen that in some of our other programs – and I'm thinking about our ANGPTL3 program where knocked the serum level of knocked down with dose escalation didn't really change that much – there was a dose response for the meaningful biomarker for LDL cholesterol. There's still more that we need to sort out there.
Q (Jason Gerber, Bank of America): I'm curious when you see such a large reduction in liver fat? Can you elaborate a little bit more on the work you've done to characterize that this was fat burned and not redistributed to other tissues? On the Dexa scans, just wondering about any work you've done to further confirm that this is an increase in lean muscle mass and not driven by any increase in water in the muscles? Any commentary on that and variants maybe seeing across at the inter patient level, that'd be great.
A (Dr. Hamilton): First of all, we did MRI not Dexa. We did look at look for changes in fat in other compartments. What we were seeing particularly in the diabetic cohorts was a reduction across the board in liver fat, in the subcutaneous fat, in the visceral fat as well, and no increase in muscle fatty infiltration – which is one of the main reasons we looked at that parameter. It's not like the fat was being redistributed into the muscle or other locations. Those were really the main compartments that that we looked at.
We saw a modest increase in the lean mass in the healthy obese volunteers. In the diabetic patients, we're still getting some of those data in there that wasn't based on what we've seen so far. Really there’s not much of a difference in in lean mass changes between the combo arm and the TRS appetite alone. But I think we're still analyzing some of that. And I think we'll report that down the road.
Q (Luca, RBC): How are you thinking about the regulatory path from here. Assuming that this reduction in weight loss is observed only as an intercept time but not as monotherapy, do you plan to get the comp approved based on weight loss? Or are you still hoping to get the monotherapy potentially approved? Maybe with another endpoint like visceral stat, walk us through the big picture? How are you thinking about the regulatory path from here to get these drugs over the finish line? On a related note, it seems this is pretty safe all the way to 400mg. Is there a plan to go higher? Your competitors are going to higher doses.
A (Dr. Chris Anzalone, President and CEO): I'll take the second question first. It's something that we're discussing. We haven't decided definitively if we're going to go higher, we certainly have room to go higher based on our tox data are no ALS. It would be interesting to push the dose a little more and see if you can squeeze out any more PD effect or efficacy. So, we'll see. We haven't ruled it out yet.
In terms of the regulatory pathway, I think it still remains to be seen. We have not had any discussions with FDA or EMA about a regulatory pathway here. The pathway has a combination therapeutic in the diabetics with the GLP ones with an endpoint of additive weight loss. I think it seems like one of the more likely paths that we might take. But again, we'd have to discuss that with regulators and get their feedback on the details, like how much more weight loss do you need on top of the standard of care.
We'll also be in the phase two. We'll also be looking at the possible use of INHBE or ALK7 as a maintenance therapy and while that could start as a combination with the GP's, at some point the GP's would be withdrawn. At least, going forward that could be a monotherapy. Again, once the GP's withdrawn that's a possibility.
A (Dr. Hamilton): I would add one more thing. Chris mentioned that we are looking at monotherapy cohorts in diabetics, which we didn't look at in the initial SAD and MAD portion.
Q (Ms. Madison al-Saadi, B Riley): We now have data from seven inhibition approaches. Wondering if there's a scenario where you may combine these or would advance both of them in separate subtype populations. Secondly, did you report baseline total adipose tissue?
A (Dr. Hamilton): We did that report baseline total adipose tissue in this presentation, and we'll probably report that down the road either at a scientific conference or another data release. In terms of the combo of both INHBE and ALK7, I'd say we haven't ruled it out yet. Of course, they're both on the same access. So maybe you could get some additive effects. We did look at that in animals and the DIO (diet-induced obesity) model and really didn't see any additive effect when we combined INHBE knockdown with ALK7 knocked down. But that doesn't mean we might not study that at least in a cohort down the road.
When you talk about combinations, we're really excited about using our dimer approach to knock down two genes at once with the same drug either in the liver or in adipose. Those combinations are likely going forward with respect to whether we take both an INHBE and ALK7 into phase 2 or just one of those. Many of you had have heard me talk over the last year about choosing one to go forward into phase two. And right now, both are looking attractive to us. It is certainly quite possible, maybe even probable, that we will continue to develop both of these at this point.
Q (Mani Foroohar, Leerink): A couple of quick ones on sort of plans forward know people have talked about the diabetic versus non-diabetic dynamic. When you think about moving forward, when should we expect to see a more fulsome disclosure around baseline characteristics for various subpopulations diabetic, non-binary, diabetic, etc.?
And separately, when you think about moving into potentially a phase two, a more targeted study, how should we think about the selection of the baseline, his appetite dose moving up or down from where it is here in combination, you know, and would you potentially move that as well as moving the dose for arrow and Higbee. Would this be a multi arm study. How do you evaluate all those potential places that you could go, given that you have a number of doses for two different agents in combination?
A (Dr. Hamilton): In terms of the rest of the data, we'll probably present that at a conference this year. We haven't decided when or where, but that'd be the best forum for us to share the details of the baseline characteristics.
Then for phase 2, we haven't really decided yet if how we would handle the dose titration for the GOP if we would continue to titrate up to, you know, 15mg for appetite or the highest dose of semaglutide, we would opt to study both of those agents in combination with ARO-INHBE, maybe others as well, to see if there's any difference, if it depends on the GLP used, but have not decided on how we would do the dose titration.
Q (Mani Foroohar, Leerink): The other question that I've gotten is whether or not, given liver fat reduction signal, you would explore one or the other of these assets in MASH. Does it make sense to have a separate MASH study and how to think about that opportunity? Is that something that's in your strategic calculus?
A (Dr. Hamilton): It's certainly something that we thought about. It’s something our colleagues have brought up and have recommended, as well. The liver fat reductions that we're seeing actually, at both dose levels, the 400 and the 200 milligram dose levels are substantial. It's probably something you could build into a phase 2. That'd be my initial take that you could do some more extensive MRI evaluations, evaluate some noninvasive biomarkers for MASH.
Of course, we probably have to do a biopsy study down the road at some point for approval, but who knows. It seems like the approvable endpoints of that indication are a moving target as well. In any case, it's something that we would look at in a phase 2. I haven't definitively decided if there's a separate Mash pathway for this drug as of yet.
Q (Maury Raycroft, Jefferies): For both INHBE and ALK combos with tirzepatide, could you talk more about what the maintenance cohort study design would look like, and what are the doctor's expectations for what would happen with GLP-1 withdrawal? Also, what are some of the precedent examples for the regulatory path that you would leverage going forward?
A (Dr. Hamilton): On the first one, I don't have a clear answer. We haven't definitively decided on the design of that study yet. We'll probably discuss the details of the phase 2 designs that wouldn't down the road later this year. On the regulatory precedent, I don't think there's a whole lot out there yet in terms of what magnitude of additional weight loss would need to be achieved with a combination therapy. Would [we] … have to study the monotherapy of the investigational therapy separately? So, that still all remains to be determined when we have discussions with regulators.
A (Prof. Carel le Roux, University College Dublin, Ireland): On what would happen with GLP-1 RA withdrawal, it's unlikely that if you withdraw any one treatment, you're going to maintain all of the benefits because that's what we see with blood pressure. That's what we see with lipids. That's what we see with diabetes, etc. Although it's an important study to do and for us to get clarity on that, my expectation would be in the long term that we will continue with combination therapies, because that's exactly what we do with all chronic diseases.
Q (Mike Waltz, Morgan Stanley): Can you … comment at a high level on your view of this early data, maybe for both INHBE and ALK7? I know it's early, but where do you see these assets potentially fitting into your practice? Is it more combination, maintenance, or all the above?
A (Prof. le Roux): I would certainly think the combination approach is certainly the first thing that I would think of, especially because it's a completely different mechanism. As you've seen, the initial data suggests that it's going to be additive or even actually amplify some of the benefits.
Now, just remember that we have very, very small amounts of absolute visceral adiposity, maybe 1.5 kg, etc., and people with diabetes, of course it will be more. So, it's not surprising that you don't see an overall reduction in weight loss, but you see this very impressive improvements in visceral adiposity, as well as adipocytes that penetrate organs such as the liver, etc. Ultimately, when we are treating the disease of obesity, it's no longer about weight loss. It's about health gain. This is exciting because you can amplify the health gains that we are seeing already from the GLP-1 type of medications.
Q (Patrick Trucchio, H.C. Wainwright): You said that phase 2 is not gated by ongoing phase 1/2a work. I'm wondering what specific effect size are you powering phase 2 for people with diabetes? Would it be incremental weight loss, visceral fat reduction or composite endpoint? And did today's data change that assumption?
A (Dr. Hamilton): When we say that ‘this is not gating’, that to me means we're planning the studies now, designing the studies, and will submit those studies. We'll disclose the details in study design and powering that down the road, probably once we submit those studies, so I can't give you a definitive answer now on that.
Q (Patrick Trucchio): Based on what you're seeing so far, would you expect an incremental benefit versus GLP-1 beyond week 24? What biological signal gives you confidence in that trajectory?
A (Dr. Hamilton): Well, I don't know that. I don't think we know the answer to that [now]. It's one of the reasons why we wanted to extend the follow up in these studies. Right now, in the combination cohorts, we go out through Week 24 and we'd like to increase the size of those cohorts so we get a little bit more power, confirm the signal, and then follow them out longer, maybe through a year, to see if they plateau or continue to lose fat mass. Right now, we just we don't know the answer.
Q (Andrea Newkirk, Goldman Sachs): Just based on the initial data here and the benefit observed in the subpopulation with diabetes, can you just remind us what proportion of the overall obesity market this represents? And then, I'd be curious how you're thinking about continued development of ARO-INHBE or ALK7. Just more specifically, do you believe Arrowhead has the capacity to bring this forward independently, or would you look to out license this in some manner, either wholly as an asset or potentially even based on geography?
A (Dr. Anzalone): Just to give you broad numbers, in the Western world we have about 25 to 35% of the population that have the disease of obesity. The total percentage of people that have diabetes is approximately 8 to 10%. Now that's much higher if you go to the Middle East, where the percentage of patients with type 2 diabetes can be as high as 24, 25%, etc. But it's also important to understand that, especially when it comes to public payers, they're far more likely to pay for medications in people that have type 2 diabetes in comparison to people that have the disease of obesity but don't have type 2 diabetes. So, the population [for obesity] is smaller. But the chances for reimbursement for people with type 2 diabetes is always higher.
Regarding your question on taking this forward, we do have the capacity and it is our intention to continue to develop these and future obesity assets ourselves. You know, I think these are important drugs. And I think we have additional important drugs that will be developing in the near to mid-term that that we should, you know, hold on to and we should we should develop ourselves. You know, the fact that that, that at least out of the gate, you know, this this you know, the obese diabetic population is a is a specific population.
And, it makes, you know, these the next level studies a bit simpler, more straightforward. Because because it is … a bit more targeted, at least initially …
Q (Joseph Thome, TD Cowan): What proportion of your patients with diabetes, obesity and on GLP-1 do you think would be interested in an additive therapy like either the ALK7 or INHBE assets? In terms of payers, for combination approaches, do you expect that you would get any pushback without hard outcomes data, or will the increased reduction in, you know, fat and weight loss be sufficient to allow for combination use? Any thoughts from either you on that or the company?
A (Prof. le Roux): What we see at the moment is this about 20% of patients – we call them the enthusiasts who are really moving very rapidly to take on new medications. You could imagine that that leaves 80% of patients out there that's currently not taking really good medications, such as the GLP-1-based therapy. So, there's a huge amount for that to grow.
For those patients who are enthusiasts, we see that they take on new treatments very rapidly. These are really a substantial number of patients that I think would be very interested in this. Of course, the fact that you can provide the treatment at pretty irregular times, that also makes it very attractive because patients, for example, when they come to clinic, they can get the medications.
When it comes to reimbursement, you're correct that it'll be difficult for new medications to displace treatments with existing cardiovascular benefits and existing kidney benefits. But what we see is there remains an unmet need in that population. As I've shown, patients with T2D still have higher cardiovascular morbidity and mortality in comparison to patients that don't have type two diabetes. It's that health gain that could be driven by the reduction in visceral adiposity that may be very attractive to both clinicians, to patients, but also to payers.
Q (William Pickering, Bernstein): For ALK7, I understand you're just presenting the visceral fat data today, but could you maybe speak in qualitative terms about how the data looked for total fat, and whether that measure also supports your view that ALK7 might be a better target than Activin E?
A (Dr. Hamilton): At this point we don't have all the data available. So, you know, we're going to have to punt on that one. We'll disclose the rest of the ALK7 data when it's all been sort of cleaned and analyzed … at a meeting down the road.
[1] Added January 8, 2026
-- by Kat Moon, Elizabeth Rose, Nour Khachemoune, Monica Oxenreiter, and Kelly Close