ISPAD 2025 Day #2 Highlights –
Executive Highlights
- The 51st Annual ISPAD Conference continued strong in Montreal on Thursday. Sessions throughout the day reflected thoughtful progress toward data-driven and equitable approaches to improving diabetes management and technology access.
- In T1D care, Prof. Alice Carr (Alberta Diabetes Institute) delivered a powerful metaphor of T1D as “the plane that never lands,” urging clinicians to tailor care across each stage of the disease rather than reacting only at diagnosis. She highlighted how precision medicine and disease-modifying therapies can transform care by identifying responders early (e.g., Abatacept benefit in high-secretor subgroups) and using biomarkers like proinsulin:C-peptide ratio (PI:C) to guide intervention timing. The key, she emphasized, is “doing the right thing for the right person at the right time.”
- T1D screening once again took the stage today through a discussion on how consensus guidelines and several emerging national programs (ELSA, SIRENA, and CanScreen, for example) are reshaping early detection strategies for T1D. Speakers highlighted how autoantibody and genetic-risk–based screening enables earlier education and care, reducing DKA risk at onset. Still, consistent follow-up infrastructure, insurance coverage, and public awareness remain key barriers. Panelists agreed that screening is most effective when paired with a clear action plan for those who test positive.
- In tech, global experts in a Medtronic symposium advocated for making AID the standard of care in pediatrics around the world, citing its potential to achieve tight “Time in Normoglycemia” (70–140 mg/dL). To do so, speakers underscored the need for team-based education, remote monitoring, and early intervention to sustain glycemic improvements after diagnosis. In Latin America, where CGM access remains below 10% in most regions, real-world data has shown impressive gains in TIR and Time in Tight Range with pump adoption, reinforcing the call for equitable technology access worldwide.
- Additionally, leaders from New Zealand, the US, and South Africa outlined the next phase of diabetes technology evolution: integrating adjunct therapies (GLP-1s, glucagon), achieving better device interoperability, and reiterating the call for ensuring global access to CGMs and AID systems. Real-world examples from New Zealand’s national AID rollout (95% uptake, mean A1c <6.9%) and South Africa’s CGM access initiatives underscore both the clinical impact and persistent inequities. As Prof. Martin de Bock summarized, “technology can only fulfill its promise when everyone can use it.”
We are thoroughly enjoying life here in Montreal! See our Resource Hub and Day-by-Day Preview for the most up-to-date source of conference reporting as well as a look at what is still to come. Additionally, see our coverage from the previous days’ sessions below:
- ISPAD 2025 Day #1 Highlights - T1D screening abounds; safe adoption of TITR in adolescent diabetes care; a new disease definition for pediatric obesity; INHALE-1 52-week topline results
Table of Contents
-
Top Highlights
- 1. Flying the whole route: Precision care for the progression of T1D
- 2. Harnessing diabetes technology to achieve normoglycemia in more children with T1D
- 3. A look into eye health and global disparities in diabetic retinopathy rates
- 4. The future of diabetes technology: Fully closed loop systems, seamless interoperability, and global access
- 5. Pros and cons of a general population screening for T1D
- 6. *NEW* Early AID initiation in Finland delivers two-year glycemic benefits in preschool-aged T1D
Top Highlights
1. Flying the whole route: Precision care for the progression of T1D
In a packed Thursday afternoon session, Dr. Alice Carr (Alberta Diabetes Institute, Canada) discussed a roadmap to precision medicines in T1D. She began her address with a powerful metaphor for a T1D diagnosis, describing it as “the plane that never lands.” Dr. Carr asked her audience to imagine arriving to an airport for a flight. The catch, she added, is once you reach the gate, you become a pilot for a flight that will not end. Whenever you encounter turbulence, she continued, you must make split-second decisions with potentially fatal consequences. Take-off (a T1D diagnosis) may feel abrupt, she noted, but the opportunity to act spans the life-long “flight path” (disease course). With the introduction of new, disease-modifying therapies in recent years, Dr. Carr emphasized that we now have the opportunity to tailor precision care to the roadmap that T1D staging gives us.
- Dr. Carr began with stage 3 T1D, or “cruising altitude.” She urged her audience to look beyond survival, towards personalization for insulin formulation and delivery, glucose monitoring technology, and psychosocial support. Dr. Carr, who has T1D herself, stressed that the lived experience of diabetes is more than just managing glucose. In the pediatric population, 40% of youth experience at least some diabetes distress, alongside 61% of their parents or caregivers. The best glycemic target, Dr. Carr continued, “is one that a person can achieve and sustain without living in fear, anxiety, or crisis.”
- At diagnosis, we hope for a “smooth takeoff” – but that begins with the right diagnosis. Yet, one in 15 youth are misdiagnosed. While the figure is lower than the estimated 40% of adults over 30 with T1D who may have been misdiagnosed with T2D, Dr. Carr stressed a need for investing in population-specific research and autoantibody and C-peptide testing accessibility as critical to making the right diagnosis (and delivering the right care) in pediatric populations.
- Disease-modifying therapies seek to preserve beta cell function at diagnosis. However, Dr. Carr highlighted, the natural history of disease development and individual response to immunotherapies is highly heterogeneous. This reality has critical implications in disease-modifying trials, including the TrialNet Abatacept Prevention study – which originally conferred that 12 months of Abatacept therapy did not delay progression in stage 1 T1D. However, when the trial population is stratified with more precise measures of beta cell function – specifically
 total or insulin secretion as a measure of beta cell responsiveness – high-secretors (>33 percentile total) on Abatacept delayed their disease progression by 15.8 months on average (p=0.005). When we lump populations together, the therapy seems like it has no effect. Acknowledging the heterogeneity in biology might better inform participant selection and reduce unnecessary exposure in non-responders.
total or insulin secretion as a measure of beta cell responsiveness – high-secretors (>33 percentile total) on Abatacept delayed their disease progression by 15.8 months on average (p=0.005). When we lump populations together, the therapy seems like it has no effect. Acknowledging the heterogeneity in biology might better inform participant selection and reduce unnecessary exposure in non-responders. - Dr. Emily Sims (Indiana University) highlighted the ratio between proinsulin (the precursor molecule to insulin) levels in fasting serum and C-peptide levels (PI:C) as a potential predictor for disease progression. While PI:C was not improved by Sanofi’s disease-modifying Tzield (teplizumab) in people with stage 2 T1D, high PI:C was predictive of rapid clinical diabetes progression in stage 2 disease. Further, PI:C tended to stay high in the same individuals and get progressively worse as they develop stage 3 disease. As such, Dr. Sims presented PI:C as a potential indicator to identify patients that may need more urgent treatment.
- Disease-modifying therapies seek to preserve beta cell function at diagnosis. However, Dr. Carr highlighted, the natural history of disease development and individual response to immunotherapies is highly heterogeneous. This reality has critical implications in disease-modifying trials, including the TrialNet Abatacept Prevention study – which originally conferred that 12 months of Abatacept therapy did not delay progression in stage 1 T1D. However, when the trial population is stratified with more precise measures of beta cell function – specifically
- “Precision medicine isn’t about doing more for everyone; it’s about doing the right thing for the right person at the right time.” The earlier the better, Dr. Carr added, stressing that the window for preserving beta cell function is likely even shorter in pediatric patients compared to adults during Q&A. In closing, Dr. Carr highlighted resource-smart screening, understanding heterogeneity, a correct diagnosis (and treatment), and adaptive care for success throughout the lifespan.
2. Harnessing diabetes technology to achieve normoglycemia in more children with T1D
In a Medtronic-sponsored symposium chaired by Dr. Jennifer McVean (Medtronic), speakers discussed difficulties in maintaining healthy glycemic levels in children with T1D, which have resulted in new definitions for ISPAD clinical practice guidelines for targets for A1c, Time in Range (TIR), and Time in Tight Range (TITR). Presenters included Dr. McVean, Prof. Thomas Danne (Breakthrough T1D), Dr. David Maahs (Stanford University), and Prof. Luis Eduardo Calliari (Santa Casa School of Medical Sciences, Brazil).
- To kick it off, Prof. Danne discussed ways in which Time in Normoglycemia (70-140 mg/dL) has the potential to ensure tighter TIR in both the short- and long-term. Normoglycemia is achieved by those without diabetes more than 96% of the time, which Prof. Danne highlighted in his argument that, as AID and CGM technology improves, TITR goals should be revised to closer match this ambitious target. He also clarified his shift away from TITR terminology, highlighting potentially negative associations with management being referred to as “tighter.”
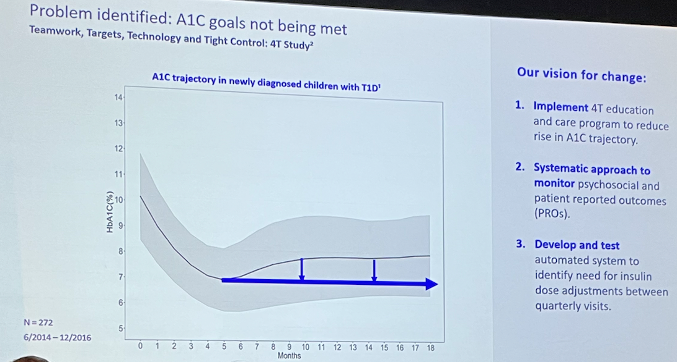
- Dr. Maahs discussed the importance of making AID systems the standard of care globally given their ability to help individuals reach recommended TIR and A1c thresholds. He highlighted how mean A1c in children newly diagnosed with T1D sharply declines upon the start of treatment, bottoming out near the recommended A1c threshold within a few months before regressing slightly (see figure below). In response to this need, he described the Timely Intervention in Diabetes Excellence (TIDE) study, which sought to better understand this glycemic response to AID initiation over time and harness AID systems to ensure that patients stay at or below target for longer. Ultimately, the program demonstrated the need for increased education for patients and families, a team-based approach to care, and remote monitoring to ensure accurate and consistent communication among patients, caregivers, and providers.
- To close, Prof. Calliari discussed the state of T1D care in Latin America, where CGMs are available to only as much as 10% of those with T1D, depending on the area. In private clinics, access can increase to nearly 90%, but the spread is not evenly distributed. With nearly 800,000 patients with diabetes in Latin America, this still translates to the vast majority not receiving standard care. Similarly, he said that only 1,500 patients in these areas use pumps or AID systems, and those that do are encouraged to bolus as much as possible. In his words, “Bolusing is best, but flexibility (with AID) is key.” He advocated for accelerated pump coverage and adoption in Latin America to mimic the positive population-wide glycemic outcomes seen elsewhere in the world.
3. A look into eye health and global disparities in diabetic retinopathy rates
In this interesting session on eye health, three researchers shared their latest findings about what drives the most common eye complication from diabetes, diabetic retinopathy (DR). Dr. Julia Busik (University of Oklahoma Health Sciences Center), Dr. Jamie Wood (University Hospitals), and Dr. Ritha Mbono (University of Yaoundé, Cameroon) discussed their clinical experiences and research, ranging from patient case studies to animal models.
- Dr. Busik focused on the role of lipids in DR progression and how dyslipidemia contributes to ocular complications in diabetes. Although DR has traditionally been viewed as rare in youth, recent studies like SEARCH and TODAY found alarmingly high rates well over 50% in youth. For both T1D and youth-onset T2D, patients developed DR within an average of 7.5 years after diabetes diagnosis, much faster than rates seen in adult populations with diabetes. Dr. Busik emphasized that current treatments such as anti-VEGF injections are only initiated at moderate to severe stages, when damage is largely irreversible, underscoring the need for earlier interventions and novel therapies. She described how retinal lipids, which are synthesized in the retina, play a critical role in maintaining vascular integrity. Her research highlighted that changes in ceramide composition drive retinal vascular leakage and inflammation. Animal studies demonstrated that targeting ceramide pathways can reverse blood-retinal barrier breakdown, suggesting that ceramide imbalance is a reversible hallmark of DR. Dr. Busik concluded by calling for lipid-based diagnostics, noting that ceramide tests may better predict risk than traditional cholesterol measures.
- Dr. Wood examined whether differences in glycation rates explain racial disparities in diabetes complications, particularly among youth. Using T1D Exchange data, Dr. Wood observed that non-Hispanic Black individuals have higher rates of diabetic complications, including retinopathy and kidney disease, and consistently higher A1c levels than White individuals. However, she noted that A1c tends to overestimate mean glucose levels in Black patients, reflecting variability in hemoglobin glycation rather than true differences in glycemic control. Dr. Wood explained the concept of “high” and “low” glycators and introduced the Hemoglobin Glycation Index (HGI) as a tool to quantify this gap. High glycators often exhibit greater insulin resistance and characteristics of “double diabetes.” While early studies linked high glycation to increased microvascular risk, newer evidence suggests that A1c variability may not directly predict complications. Dr. Wood also emphasized the need to move beyond A1c-centric targets, as using strict A1c goals can lead to more hypoglycemia in Black youth. Addressing social, behavioral, and biological factors together is essential to reduce disparities in diabetes outcomes.
- Dr. Mbono presented by simulcast on DR as a growing public health issue in Sub-Saharan Africa. She emphasized that DR is a leading cause of blindness among middle-aged and older adults and imposes severe socioeconomic consequences when working-age individuals lose their vision. Recent data indicate a 28% prevalence of DR among African adults with diabetes, with 10% experiencing sight-threatening disease. Risk factors include poor glycemic management, long duration of diabetes, comorbid hypertension or nephropathy, older age, and higher BMI. Dr. Mbono outlined key prevention strategies centered on improving access to multidisciplinary care, enhancing screening programs, and promoting education. She highlighted initiatives like the Diabetic Retinopathy Network (DR-NET) and telemedicine-based retinal screening, which have proven cost-effective and help expand access in resource-limited settings. Public awareness campaigns, universal health coverage, and routine screening at diagnosis and every two years were also recommended. Dr. Mbono concluded that prevention, caregiver training, and national screening programs are crucial to curbing the rising burden of diabetic blindness across Africa.
4. The future of diabetes technology: Fully closed loop systems, seamless interoperability, and global access
In this forward-looking session, Prof. Martin de Bock (University of Otago, New Zealand), Mr. John Walsh (SweetSpot), and Ms. Cathy Haldan (Foundation for Innovative New Diagnostics, South Africa) explored three key themes of progress: (i) automation to achieve fully-closed loop; (ii) interoperability; and (iii) the importance of equitable access to technology. Together, their presentations traced how the evolution of diabetes technology has shaped today’s state of diabetes management, and what it will take for automation to become universal, intelligent, and equitable for all users.
- Prof. de Bock framed the trajectory of diabetes technology as an evolutionary process, arguing that the next phase of automation will be dependent on adjunct therapies and better developed hardware. He described the “convergent evolution” of diabetes technology, across pumps, algorithms, and differing form factors, as evidence of potential for a successful design model. New Zealand’s policy providing fully funded AID to all people with diabetes led to 95% uptake and a national mean A1c <6.9%, which is exceptional, though only a minority achieve the new 6.5% target. Prof. de Bock charted system progressions from Medtronic’s 780G development, Tandem’s Control-IQ+, Omnipod 5, and CamAPS FX, emphasizing how most major systems can help users achieve near 65-70% TIR, but no algorithm can overcome the fundamental mismatch between insulin kinetics and post-meal glucose absorption.
- Prof. de Bock firmly believes adjuncts like GLP-1 RAs can address this problem by slowing gastric emptying to align glucose uptake with insulin action. Citing the ADJUST-T1D study (n=72), he highlighted semaglutide’s ability to improve TIR by 10 percentage points with weight loss in people with T1D and obesity. He also revisited glucagon, noting stable formulation could enable insulin delivery without fear of hypoglycemia. Finally, he pointed to open-source systems’ advantage, being free of commercial restrictions, achieving ~66% TIR in long-term studies.
- Mr. Walsh discussed interoperability as the backbone for safer and more efficient diabetes care. Mr. Walsh credited milestones like SMART on FHIR and FDA’s iCGM/ACE pump designations with enabling modern AID systems. Despite these advances, technical and ethical challenges persist, such as signal interference and Bluetooth range continue to compromise reliability, while privacy and consent frameworks lag behind AI’s rapid advances. Mr. Walsh emphasized the growing promise of multi-metabolite sensing, for integrating ketone and glucose for earlier DKA prediction and better contextual decision-making. He urged multidisciplinary collaboration to ensure interoperability is addressed as a priority as diabetes technology advances.
- Ms. Haldane spotlighted her team’s work to scale CGM use in low-resource settings of South Africa. While there was 30% annual growth in South Africa’s CGM market, only 16% of individuals with T1D have access, primarily through the private sector. Registry data from 42,000 children across 56 countries demonstrate that reimbursement directly correlates with lower A1c levels.
- Findings from the ACCEDE project (n=249) showed that periodic CGM use produced the largest A1c improvement, especially in youth, though gains stopped once access ended, underscoring the importance of maintaining availability even if use is periodic. Baseline A1c exceeded 12%, with half of the children experiencing DKA in the prior year. Willingness-to-pay gap analyses exposed a deep affordability gap, with optimal prices only 16% of current sensor cost. To build local capacity, the team launched online CGM training with the International Diabetes Federation, now reaching over 10,000 patients and clinicians globally. She emphasized that equitable access to CGMs will depend on sustainable financing and policy reform, as well as trust in the patient-provider relationship.
5. Pros and cons of a general population screening for T1D
In a Sanofi-sponsored session, Drs. Emily Sims (Indiana University), Parth Narendran (University of Birmingham, UK), Valentino Cherubini (Italian Society of Pediatric Endocrinology), Despoina Manousaki (CHU Sainte-Justine, Canada), and Rémi Rabasa-Lhoret (Montreal Clinical Research Institute, Canada) discussed the current state of the T1D screening. An extended Q&A featured questions related to the initiation of screening programs in organizations at a small scale and best practices for addressing common concerns.
- Currently in the US, T1D screening has gained momentum in recent months, following the recent publication of consensus guidelines about early stage T1D. Screening has been associated with decreased rates of DKA at the time of diagnosis, as well as an opportunity for patients and their families to become educated about T1D. As part of her talk, Dr. Sims discussed obstacles to general population screening, include a lack of consistency in screening processes across regions, insurance payer coverage, and a lack of education or guidance for a positive result. She said that the majority of screening in the current landscape are often already being seen for a different reason – a general population screen would include far more healthy individuals.
- Several screening programs were discussed including the ELSA program. This program tested 25,000 individuals in the UK: of these, 300 were screened positive for autoantibodies. 105 were categorized as stage 1 T1D, 31 with stage 2, and seven with stage 3. Participants mainly heard about the program through social media or their schools, a point which was pressed during the Q&A as to the potential for replication in future government-sponsored studies. First degree relatives of individuals with T1D were also considered ideal screening targets, despite the lack of strong familial correlation with T1D diagnoses (>15% of individuals with T1D have a first degree relative with T1D). Dr. Cherubini noted that Italy was the first country to pass a law mandating that clinicians offer screening to children under 18. This screening program was added to an already existing nationwide screening for Celiac’s disease.
- The Canadian CanScreen pilot program has two main arms: (i) the genetic risk score (GRS) arm; and (ii) the antibody (Ab) arm. GRS will be used to identify among newborns those who are genetically predisposed to be at higher risk of developing T1D. Those identified with a higher GRS are then moved forward into accelerated Ab testing. Children aged 2-12 years from the general population will be recruited throguh various approaches and will be be tested for Abs. Those who test positive will be retested annually for two or more autoantibodies, and those who screen negative will be encouraged to get tested again in the future – if possible, at least twice across their childhood. Children from both arms who will develop two or more autoantibodies will be moved to the metabolic follow-up arm and will have the option to participate in TrialNet or receive approved immunomodulatory medications.
- During the Q&A, many were interested in best practices, as well as the practicality of implementing a nationwide, general screen. Both questions and answered highlighted how essential it is for guidance on how to follow up if someone tests positive for autoantibodies: it is not enough to simply screen individuals. In response, TrialNet data was cited to show that the majority of people will not test positive for autoantibodies during screening; it remains important, however, to have an appropriate plan for those who do test positive. One audience member brought up the general lack of options for the delay of T1D in Canada, where teplizumab (Tzield) is approved but has only been given to three patients.
6. *NEW* Early AID initiation in Finland delivers two-year glycemic benefits in preschool-aged T1D
Dr. Anna-Kaisa Tuomaala (University of Helsinki and Helsinki University Hospital, Finland) shared a real-world analysis demonstrating that early use of AID systems in newly diagnosed preschoolers with T1D led to sustained improvements in A1c and TIR over two years. The findings add to growing support for introducing AID systems at diagnosis, even in very young children traditionally managed with MDI or manual pump therapy at first.
- Study design. Conducted at Helsinki University Hospital in Finland, where T1D incidence remains among the world’s highest (63 per 100,000 person-years in 2024), the study included 92 children diagnosed between 2021 and 2022, all younger than seven years. Participants were divided into two groups: those using AID in automated mode and those using non-automated insulin delivery systems (manual-mode AID, insulin pump, or MDI). Glycemic outcomes were collected at three-, six-, 12-, and 24-months post-diagnosis. Treatment decisions were made by clinicians, reflecting real-world practice rather than a fixed protocol.
- Baseline characteristics. Nearly half of participants (45%) were under three years old at diagnosis and a slight majority were male. Mean baseline A1c was 8.5%. At diagnosis, 46% initiated AID, 48% started MDI, and 6% used other regimens. As time progressed, users spent an increasing amount of time in auto-mode, from 22% of the time at three months to 62% at one year and 72% at two years. By two years post-diagnosis, AID users required less insulin, which Dr. Tuomaala interpreted as reflecting either differences in the duration of the honeymoon phase or a greater need for corrections in the AID group.
- Results. Non-AID users had slightly lower A1c values in the initial follow-up period, which Dr. Tuomaala attributed to strong caregiver engagement. However, after six months, glycemic trends diverged, with AID users seeing continuous improvement in A1c levels, while non-AID users began to show worse outcomes. By 24 months, the AID group demonstrated superior A1c and TIR values, though Time below Range (<70 mg/dL) remained comparable between groups. The data suggest that early initiation of automated systems may mitigate risks for dysglycemia in the very young. Dr. Tuomaala said that AID systems introduced soon after diagnosis may help families maintain glycemic stability, even as insulin requirements increase. This helps support smoother transitions and may potentially reduce the long-term risk of micro- and macrovascular complications.
--by Riya Chatterjee, Colson Duncan, Elizabeth Rose, Jeremy Alkire, Monica Oxenreiter, and Kelly Close