EASD 2025 Day #2 Highlights –
Executive Highlights
- EASD 2025 continued strong in Vienna with a packed schedule full of learnings in tech, therapy, and big picture. We highly recommend that you review in detail the EASD final program, and see our preview of upcoming sessions through the rest of this week.
- Prof. Chantal Mathieu (UZ Leuven, Belgium) officially opened the 61st EASD Annual Meeting and set the tone for the week with a wide-ranging Presidential Address that both celebrated the growth of EASD and set an ambitious agenda for the future. She welcomed over 13,500 participants and pointed to a record 2,170 abstracts submitted, with 1,354 accepted and over 1,900 presentations scheduled across the next five days. Describing the program as a “feast of science,” she emphasized that the meeting would span topics ranging from disease insights and treatment advances to disease modification, late-breaking clinical trial results, and implementation research.
- In tech, we got several updates on long-term glycemic outcomes with AID systems. Dr. Jennifer McVean (Medtronic) presented three-year real-world results (n=1,145) from MiniMed 780G users (≥16 years old) across Europe, the Middle East, and Africa (EMEA). Results demonstrated strong early glycemic improvements sustained throughout three years of MiniMed 780G use, achieving reductions in user burden with fewer user-initiated boluses and greater trust in the system. Prof. Jolien De Meuleeester (KU Leuven, Belgium) presented results from the INRANGE study, sharing two-year outcomes data on Tandem’s Control-IQ algorithm. Separately, Dr. Magdalena Bogun (Columbia University) presented a single-center observational study (n=163) evaluating the safety and accuracy of inpatient CGM for DKA management with IV insulin infusion compared to standard hourly point-of-care (POC) testing.
- In therapy, incretins were a core theme of the day. Dr. Silvio Inzucchi (Yale University) presented post-hoc analysis of the SOUL trial, evaluating cardiovascular benefits of Rybelsus (oral semaglutide) by baseline A1c and BMI in people with T2D and atherosclerotic cardiovascular disease (ASCVD) or chronic kidney disease (CKD). Dr. Kun He (Shandong First Medical University, China) presented full results of the phase 2 trial (n=61), evaluating dual GLP-1/GIP receptor agonist HRS9531 from Jiangsu Hengrui Pharmaceuticals in Chinese adults with overweight or obesity but not diabetes. In a spotlight session so crowded that attendees sat on the floor, panelists explored the science and clinical evidence of where incretin therapies fit in the T1D treatment paradigm. Prof. Riitta Veijola (University of Oulu, Finland) elaborated on the use of GLP-1 RAs in children with T1D, while Dr. Petter Bjornstad (University of Colorado) focused on the adult population. Prof. Jerry Greenfield (St. Vincent’s Hospital, Australia) concluded the session by explaining how GIP agonism enhances the effects of GLP-1 RAs in T1D, along with sharing unpublished data from the TIRTLE 1 trial of tirzepatide in adults with T1D and obesity.
- EASD’s Exhibit Hall also opened this morning, with nearly 70 organizations showcasing free health checks for LDL-cholesterol, healthy fruit giveaways, and even a heart-shaped photobooth, indicating the cardiovascular benefits of a drug (Wegovy) – so many of them in neon-lighted booths. Walkways were packed as attendees engaged with company representatives and eye-catching displays to learn more about technologies and therapies for diabetes and obesity. And, it’s Vienna – the country seems proud of it’s late night coffee houses (some of which are open as late as 2 am or even 4 am – even though it closes at 10 pm, Café Central gets big votes from us) amidst aromatic espresso stations In all, the 2025 EASD Exhibit Hall’s opening day highlighted the excitement and diverse themes that we witnessed throughout the day, from therapeutic benefits for diabetes comorbidities to far easier ways to take insulin and to titrate GLP-1.
Additionally, see our EASD 2025 Day #1 Highlights - Nine industry symposia highlight dual glucose-ketone monitoring, new CGM features, cardiometabolic comorbidities, incretin-based therapies, and SGLT-2 inhibitors.
Table of Contents
-
Therapy
- 1. Post-hoc analysis of SOUL trial finds CV benefits of Rybelsus (oral semaglutide) regardless of baseline A1c or BMI
- 2. Full phase 2 results of dual GLP-1/GIP RA HRS9531 for overweight or obesity without T2D
- 3. The role of incretin-based treatments in T1D management
- 4. ELSA study shows acceptability and feasibility of general population screening for pre-symptomatic T1D among children in the UK
- 5. Post-hoc analysis of phase 3 REDEFINE-1 trial: Long-acting amylin analog cagrilintide confers greater weight loss (12%) than placebo (2.3%)
- 6. Discussion with Dr. Alice Cheng, Prof. Francesco Giorgino, and Prof. Ezio Bonifacio on population-wide, age-indiscriminate screening for T1D
- 7. Insulin therapy and cardiorenal outcomes in T2D: A pooled analysis of CANVAS and CREDENCE
- 8. Phase 3 study finds A1c reduction and potential cardiorenal protection with berberine ursodeoxycholate
-
Technology
- 9. Three years of MiniMed 780G: Durable glycemic outcomes, reduced burden, and strengthened patient confidence
- 10. Glycemic improvements with Tandem’s Control-IQ at 12 months maintained at 24 months
- 11. Safety and accuracy of CGM for inpatient DKA management compared to hourly POC testing
- 12. International RCT finds CGM reduces risk of large-for-gestational-age infants in women with GDM
- 13. INLOOP study: One-year real-world outcomes with Diabeloop DBLG1 show durable glycemic and quality-of-life benefits
- 14. RADIANT adult sub-analysis (n=79): Omnipod 5 drives significant A1c and TIR gains vs. MDI with CGM, with A1c reaching 7.2% and an extra five-plus hours time “in range”
- 15. Exercise boosts TIR in CGM analysis of adolescents with T1D (n=3,069)
- 16. *NEW* Insulet-sponsored symposium emphasizes scalable onboarding strategies and real-world outcomes with Omnipod 5 in T1D
-
Big Picture
- 17. Prof. Chantal Mathieu delivers most-valuable EASD Presidential Address, extolling vision for personalized, global diabetes care
- 18. Under promise and over deliver: Dr. Dan Drucker on his philosophy for scientific research
- Preview
- 19. 57th Claude Bernard Lecture by the esteemed Professor Andrew Hattersley focuses on “precision diabetes”: Learning from the rare and applying to the common
- 20. Novel diabetes subgroup classifications and optimized treatment plans based on glucose variability patterns from CGM data
- 21. Fructose consumption may play a key role in the development of MASLD
- 22. Exhibit Hall opens with high energy, featuring aromatic coffee stations, free lipid tests, and photobooths
- 23. TANGO-DM RCT finds that updated WHO 2013 diagnostic criteria for GDM demonstrates no improvement to risk of large-for-gestational-age infants compared to 1999 criteria
- 24. Cause or consequence? Dr. Carmella Evans-Molina reviews whole pancreas changes in people with T1D
- 25. Fr1da study shows insights into single islet antibody prevalence and progression in children
- 26. *NEW* Higher A1c thresholds required to predict T1D progression in adults compared to children with positive islet autoantibody
- 27. *NEW* “The era of diagnosis”: Survival rates for T1D increased over decades
Therapy
1. Post-hoc analysis of SOUL trial finds CV benefits of Rybelsus (oral semaglutide) regardless of baseline A1c or BMI
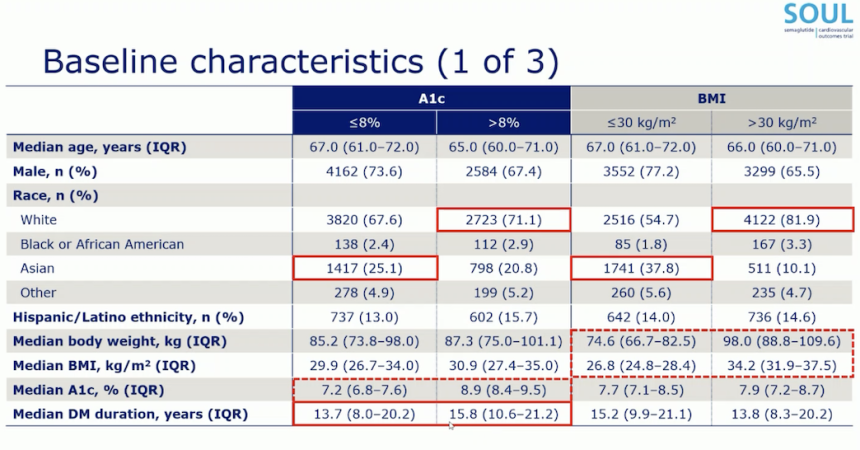
In this crowded morning session, Dr. Silvio Inzucchi (Yale University) presented post-hoc analysis of the SOUL trial, evaluating cardiovascular benefits of Rybelsus (oral semaglutide) by baseline A1c and BMI in people with T2D and atherosclerotic cardiovascular disease (ASCVD) or chronic kidney disease (CKD). As a reminder, the phase 3b SOUL trial (n=9,650) demonstrated a statistically significant and superior 14% major adverse cardiovascular events (MACE) reduction with oral semaglutide.
- Baseline characteristics. Participants were divided by A1c (≤8% or >8%) and BMI (≤30 kg/m2 or >30 kg/m2). Baseline age on average was similar across all groups, but low A1c and BMI groups had greater percentage of males (74% and 77%, respectively) than higher A1c and BMI groups (67% and 66%, respectively). By demographics, as shown in the figure below, Dr. Inzucchi noted that Asians were more likely to have lower A1c and BMI, while White people were more likely to have higher A1c and BMI. Clinically, higher A1c group was more likely to have longer duration of diabetes (16 vs. 14 years in lower A1c group) and on insulin treatment (64% vs. 42% in lower A1c group), which are expected.
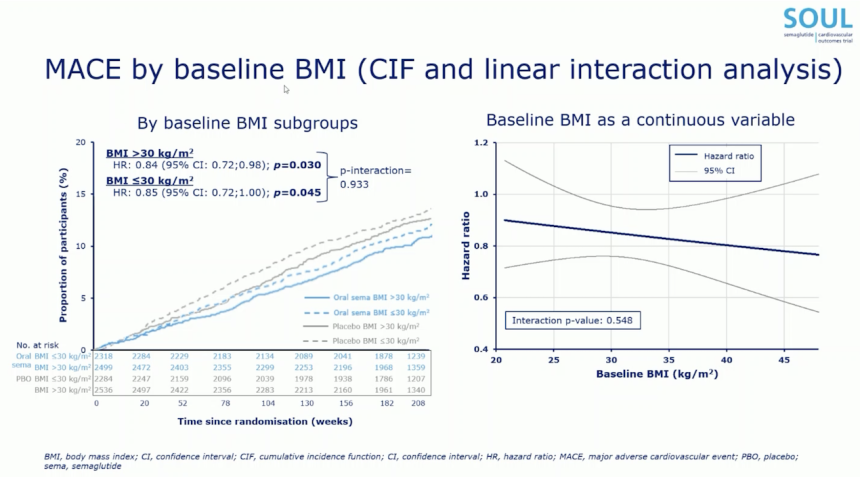
- CV benefits of oral semaglutide were consistent across baseline BMI but more pronounced with higher baseline A1c. By baseline A1c, oral semaglutide conferred 4% and 27% MACE reduction in lower (≤8%) and higher A1c (>8%) group, respectively (p=0.017). Linear interaction analysis, which treats baseline A1c as a continuous variable rather than categorical, found numerically greater MACE risk reduction at higher A1c (p=0.189). By baseline BMI, oral semaglutide conferred similar MACE reduction by 15% and 16% for lower and higher BMI groups (p=0.933). CV benefits of oral semaglutide were not influenced by baseline body weight (p=0.733) or baseline BMI as a continuous variable (p=0.548). Further exploratory analysis found that the change in A1c (p=0.502), BMI (p=0.257), and body weight (p=0.332) during the trial did not influence CV benefits of oral semaglutide.
2. Full phase 2 results of dual GLP-1/GIP RA HRS9531 for overweight or obesity without T2D
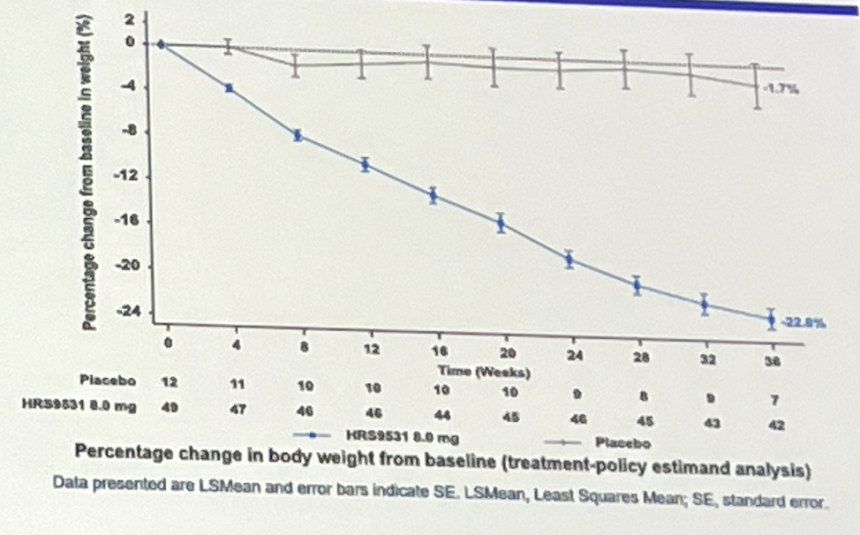
In a packed symposium, Dr. Kun He (Shandong First Medical University, China) presented full results of the phase 2 trial (n=61), evaluating dual GLP-1/GIP receptor agonist HRS9531 from Jiangsu Hengrui Pharmaceuticals in Chinese adults with overweight or obesity but not diabetes. This follows topline results that we reported on when announced in January 2025 that found that HRS9531 conferred a mean weight loss of 23% vs. under 2% weight loss in placebo at Week 36. HRS9531 is also evaluated in phase 3 trials for obesity and T2D. In July 2025, the company announced topline results of the phase 3 trial (n=567) for obesity, in which HRS9531 conferred placebo-adjusted mean weight loss of 16% from baseline of 93 kg (205 lbs) at Week 48. The company shared plans to submit New Drug Application (NDA) in China.
- Trial design and baseline characteristics. Chinese adults with obesity (BMI ≥28 kg/m2) or overweight with a weight-related comorbidity (BMI ≥24 kg/m2) were randomized to receive once-weekly subcutaneous injections of HRS9531 8 mg (n=49) or placebo (n=12). The primary endpoint was the change in body weight from baseline to Week 36. At baseline, participants were on average 33 years old, with ~70% being female. Clinically, participants had average baseline weight of 85 kg (187 lbs), BMI 31 kg/m2, A1c 5.4%, waist circumference 101 cm, and systolic blood pressure (SBP) 120 mmHg. They did not state what percentage of people, if any, had pre-T2D. We are very interested to know this given higher risk at lower BMI in some Asian populations.
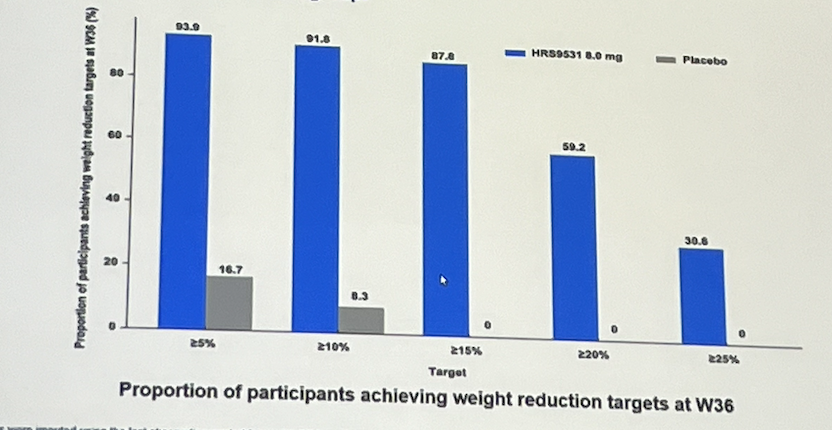
- Results. At Week 36, HRS9531 conferred a mean weight loss of 23% compared to virtually no weight loss, specifically just 1.7% weight loss, for those on placebo. Significantly higher percentage of participants achieved weight loss thresholds, as shown in the figure below. Notably, 88%, 60%, and 31% of HRS9531-treated participants achieved ≥15%, ≥20%, and ≥25% weight loss, respectively, compared to none in the placebo group. Moreover, HRS9531 reduced waist circumference (18 cm vs. 3 cm with placebo), BMI (7.1 kg/m2 vs. 0.7 kg/m2), SBP (14.3 mmHg vs. 5.2 mmHg), A1c (0.4 vs. 0.1 percentage points), and triglyceride levels (41% vs. increase by 45%) at Week 36. Safety findings were generally consistent with incretin-based therapies, with majority of treatment-emergent adverse events being mild and GI-related. Most common GI events included diarrhea (27% vs. none), nausea (25% vs. none), and vomiting (20% vs. none). Notably, no participants permanently discontinued treatment due to treatment-emergent adverse events. While the difference in A1c is not as large as differences in weight loss, we are sure patients who had the 0.4 drop were much more pleased than those who experienced just a 0.1 drop (though something is better than nothing, whether or not the 0.1 is even “accurate” would be a question). Yet again, CGM metrics would be extremely helpful to have with this trial.
3. The role of incretin-based treatments in T1D management
In a spotlight session so crowded that attendees sat on the floor, panelists explored the science and clinical evidence of where incretin therapies fit in the T1D treatment paradigm. Prof. Riitta Veijola (University of Oulu, Finland) elaborated on the use of GLP-1 RAs in children with T1D, while Dr. Petter Bjornstad (University of Colorado) focused on the adult population. Prof. Jerry Greenfield (St. Vincent’s Hospital, Australia) discussed how GIP agonism enhances the effects of GLP-1 RAs in T1D, along with sharing unpublished data from the TIRTLE 1 trial of tirzepatide in adults with T1D and obesity. The panelists all encouraged the need for GLP-1 RAs as an adjunctive therapy for T1D, especially given the challenges of meeting target A1c levels and addressing complications with insulin alone. Given what we know about hypoglycemia concerns, even for those fortunate enough to have CGM, we are still very wary about regulatory assessment by the FDA. We hope that CGM data can be reviewed in order to reinforce the degree to which glycemic improvement can be seen with GLP-1 (even in the midst of more hypoglycemia, which is manageable) – we are curious if there is dQ&A or other data showing the perceived and actual benefit / risk profiles.
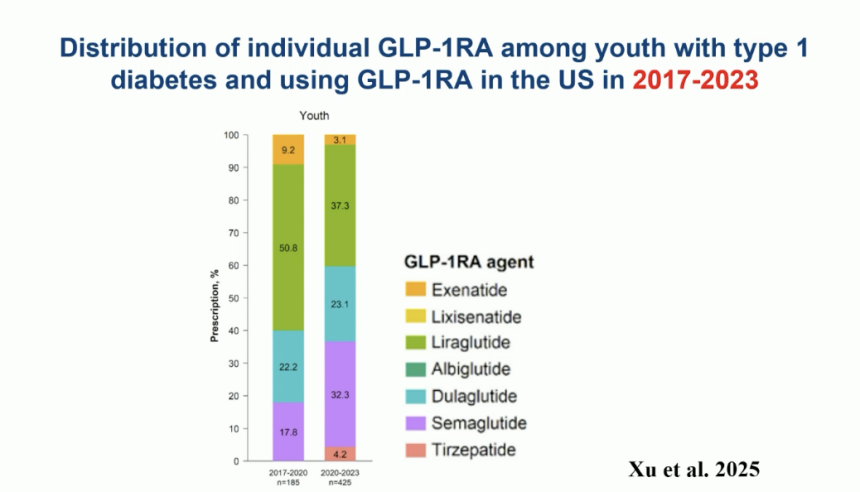
- Prof. Veijola on the use of GLP-1 RAs in children with T1D. GLP-1 RAs are currently approved for children with T2D ≥10 years and approved for children with obesity ≥6 years. While GLP-1 RAs are not approved for T1D, a 2025 study (“Trends in obesity and glucagon-like peptide-1 receptor agonist prescriptions in T1D in the US” by Jung-Im Shin, et. al. in Diabetes, Obesity, and Metabolism) showed that in the last 15 years, the prescriptions of GLP-1 RAs have significantly increased across all BMI categories among both youth and adults with T1D. When looking at the distribution of GLP-1 RA use among youth with T1D, liraglutide (Novo Nordisk’s Victoza) was the most prescribed treatment between 2017 and 2020, followed by dulaglutide (Lilly’s Trulicity), semaglutide (Novo Nordisk’s Ozempic), and exenatide (AZ’s Bydureon and/or Byetta). Although liraglutide remained the most prescribed treatment between 2020 and 2023, the distribution narrowed with increasing treatment of semaglutide and emerging numbers for tirzepatide. We wonder if this is the most popular because there is a perceived flatting of appetite by day when it is taken, which is some of what we hear from some people with T1D who are on it – they seem to appreciate the ability to turn this “on” or “off” from what we hear, though this is anecdotal.
- Beyond the use of GLP-1 RAs in children with T1D, Prof. Veijola also spoke on children with early-stage T1D. She referenced a 2021 study that showed the combination of anti-IL21 and liraglutide preserves beta cell function in adults newly diagnosed with T1D. Furthermore, she elaborated on a 2023 study (“Semaglutide in Early Type 1 Diabetes” by the esteemed Dr. Paresh Dandona, et. al., published in the NEJM in which Ozempic, started within three months of T1D diagnosis in adults, led to the elimination of prandial insulin in all patients and basal insulin in 70% of the study population! These findings highlight that GLP-1 RAs could also potentially help preserve beta cell function in children, alone or in combination with other treatments. Considering the limited evidence in children with T1D, Prof. Veijola encouraged large trials at various stages of T1D to determine the safety and efficacy of GLP-1 RAs in this population.
- Dr. Bjornstad on the use of GLP-1 RAs in adults with T1D. Dr. Bjornstad listed several reasons for needing GLP-1 RA treatment in T1D management, including: (i) inherent limitations of insulin with risks of hypoglycemia, fluctuations in glucose levels, and weight gain; (ii) gaps in glycemic management with most people with T1D unable to achieve A1c or TIR targets, even with AID systems; (iii) increasing metabolic complications like obesity, insulin resistance, and hyperinsulinemia; and (iv) proven CKM protection of GLP-1 RAs showing clear benefits in CV and kidney health. As he advocated for GLP-1 RAs, Dr. Bjornstad clarified that GLP-1 RAs would not compete with insulin or technology interventions but rather act as a synergistic treatment to help mitigate CKM in T1D.
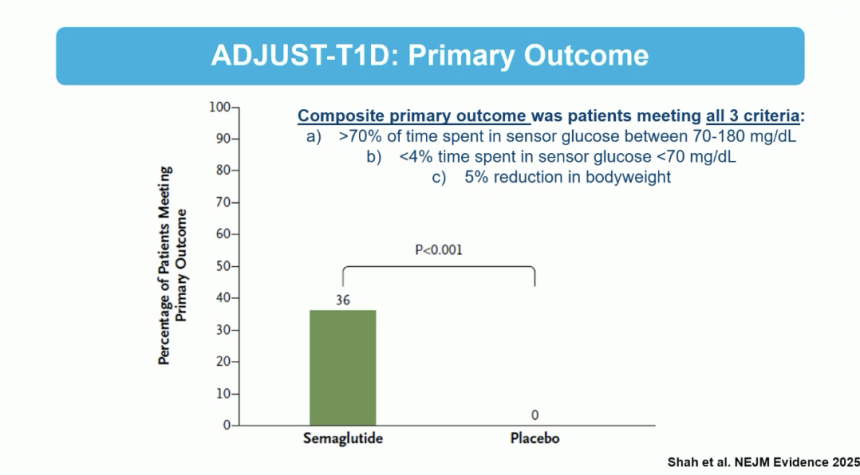
- To further illustrate the need for GLP-1 RAs, Dr. Bjornstad overviewed clinical trial data in T1D, including the most recently published results from the ADJUST-T1D trial presented at ADA 2025. As background, the trial evaluated the use of semaglutide as an adjunct to insulin in adults with T1D and obesity using AID. The composite primary outcome (achieving TIR >70%, TBR <4%, and ≥5% weight loss) was met by 36% of participants in the semaglutide group versus zero in the placebo group. Furthermore, A1c decreased by 0.7% from 7.8% at baseline to 7.1% in the semaglutide group compared to 0.3% from 7.7% at baseline to 7.4% in the placebo group.
- Dr. Bjornstad also outlined other trials investigating the use of GLP-1 RAs in T1D, including: (i) RESET1 of semaglutide in heart health; (ii) T1-DISCO of semaglutide in CV outcomes; (iii) REMODEL-T1D of semaglutide in kidney oxygenation and function; and (iv) OBES1TY of semaglutide in body weight, insulin dose requirements, and glucose levels.
- Prof. Greenfield on GIP/GLP-1 RA in T1D. In light of the emerging evidence of incretin-based treatments, Prof. Greenfield focused on the combination of GLP/GIP-1 RAs. Studies have shown that GLP-1 RAs reduce glucagon and increase C-peptide levels, while GIP RAs have no effect during hyperglycemia. In comparison, GIP RAs increase glucagon levels during hypoglycemia, serving as an ideal molecule for people with T1D. Turning to neurological effects, Prof. Greenfield shared data that shows how GIP RAs inhibit food intake and nausea in the central nervous system. Therefore, Prof. Greenfield emphasized that GIP RAs help blunt nauseating side effects of GLP-1 RAs in humans, explaining the greater tolerability of tirzepatide at doses higher than semaglutide.
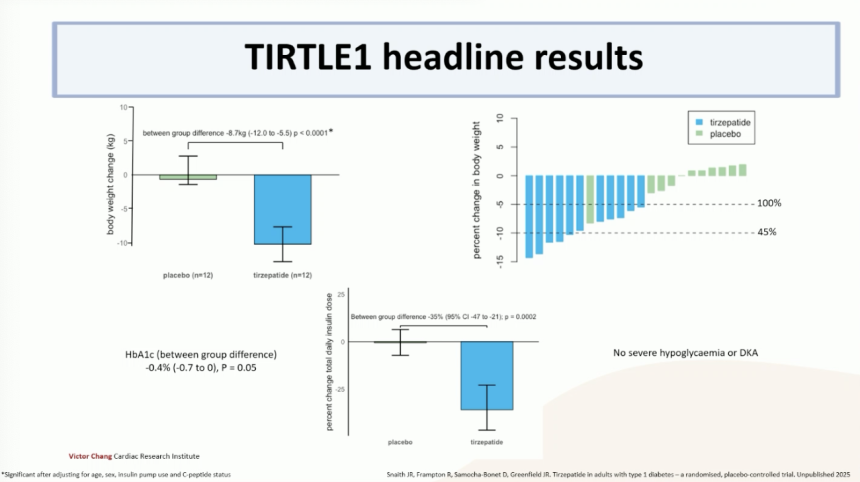
- Looking forward, several trials are underway to study the use of tirzepatide in T1D. Prof. Greenfield shared unpublished data of the TIRTLE 1 trial, which focused on the effect of tirzepatide on weight and metabolism in adults with T1D. Headline results showed that all trial participants saw ≥5% weight loss, and 45% of participants saw ≥10% weight loss. Furthermore, the mean A1c reduction was 0.4% with no severe hypoglycemia or DKA. Reflecting on these findings, Prof. Greenfield encouraged further trials on the effects of low-dose tirzepatide in people with T1D and without obesity, as well as tirzepatide on CV risk reduction.
4. ELSA study shows acceptability and feasibility of general population screening for pre-symptomatic T1D among children in the UK
During an oral session, Prof. Parth Narendran (University of Birmingham, UK) presented updated findings from the ELSA study (n=25,165) that was published in a preprint article in The Lancet last week. This study focused on the feasibility and acceptability of general population screening for pre-symptomatic T1D among children in the UK. Overall, results showed that the screening model was feasible with 91% of families completing confirmatory testing, 95% completing staging processes, and 84% attending follow-up education programming. Almost all families rated the experience positively. As the UK’s largest pediatric trial for population screening, the ELSA study provides insightful considerations for shaping future screening programs in the UK and international regions.
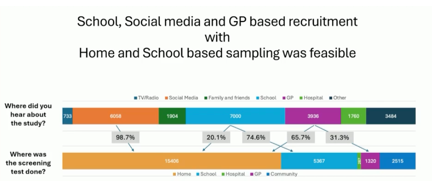
- Methods. Children across the UK were offered screening for autoantibodies with dried blood spot samples (DBS) in various settings that included: (i) schools; (ii) primary care physicians; (iii) social media; (iv) hospitals; and (v) community centers. Following positive DBS results, children were followed with a venous confirmation test for specific autoantibodies. Children who showed multiple positive autoantibodies received metabolic staging with an oral glucose tolerance test. The study defined feasibility based on the type of recruitment, uptake of screening, and demographic factors; acceptability was assessed through qualitative interviews with families following the study.
- Trial Results. Between November 2022 and 2024, the study enrolled 25,165 children. The median age was eight years, 52% were male, and 37% of families had a history of T1D. Recruitment worked well across schools, primary care settings, and social media platforms. In community settings, non-White ethnicities showed higher rates of participation; Black and South Asian populations had under-recruitment.
- Clinical Results. In the study, 98% of children screened DBS negative and 2% positive. 95% of children who screened positive received venous confirmation and metabolic staging. The study identified 56 single-antibody and 125 multiple-antibody children, and 85% completed education and support for diabetes management. Furthermore, 98% of the population found the screening acceptable, with a positive experience and willingness to recommend it to others. Some families particularly highlighted the overall convenient process of screening and the opportunity to become informed about a child’s risk status.
- Future outlooks. Reflecting on these findings, Prof. Narendran reminded that first-degree relatives are an effective target population for screening, especially as they were more engaged (i.e., 37% of ELSA participants) and showed greater participation for returning diagnosis kits. Furthermore, he emphasized that first-degree relatives are more likely to screen positive with a 3.7% diagnosis rate, compared to 2.2% for those with any relatives with T1D and 0.25% in the general population.
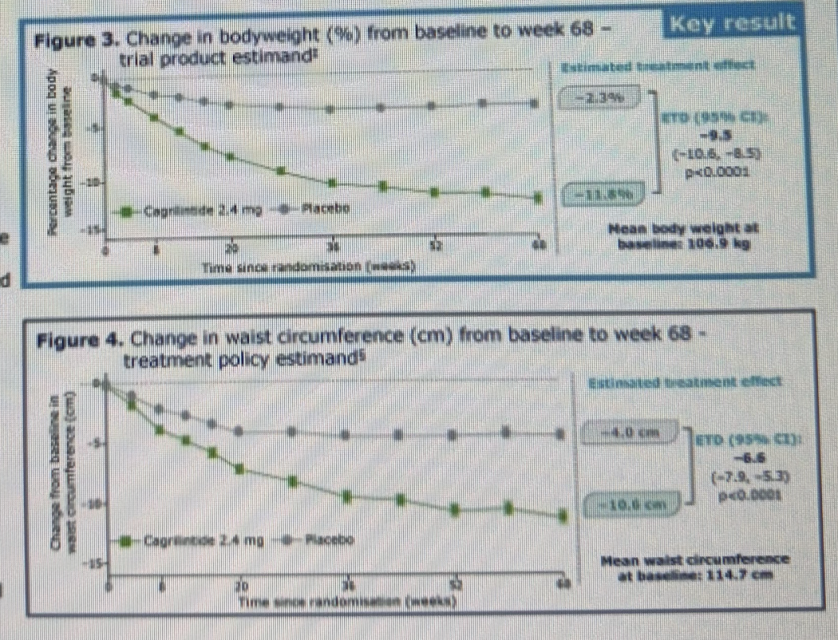
5. Post-hoc analysis of phase 3 REDEFINE-1 trial: Long-acting amylin analog cagrilintide confers greater weight loss (12%) than placebo (2.3%)
A poster by Dr. Timothy Garvey (University of Alabama at Birmingham) presented post-hoc analysis of the phase 3 REDEFINE-1 trial (n=3,417), demonstrating that once-weekly long-acting amylin analog cagrilintide 2.4 mg was both safe and effective in treating adults with obesity or weight-related comorbidities. Results were simultaneously announced in Novo Nordisk’s press release. As a reminder, full results of the REDEFINE-1 trial were presented at ADA 2025, demonstrating that CagriSema (a fixed combination of cagrilintide 2.4 mg and semaglutide 2.4 mg) conferred 20% weight loss, compared to 15% with semaglutide alone, 12% with cagrilintide alone, and 3% with placebo. This post-hoc analysis marks the first phase 3 trial data for cagrilintide monotherapy for obesity. Dr. Garvey highlighted that cagrilintide may serve as an alternative for those who do not tolerate incretin-based therapies. Novo Nordisk will advance cagrilintide into the dedicated phase 3 RENEW program, expected to begin in 4Q25.
- Study design and baseline characteristics. The post-hoc analysis included 302 participants with obesity who received cagrilintide, with a mean age of 47 years, BMI of 38 kg/m², and body weight of 107 kg (236 lbs). Of the participants who received cagrilintide, 66% were female and 71% were white. To be eligible, participants were required to have a BMI ≥30 kg/m² or ≥27 kg/m² with at least one weight-related comorbidity. Individuals with diabetes were excluded.
- Results. Participants receiving cagrilintide achieved average weight loss of 11.8% (12.5 kg or 28 lbs), compared to 2.3% (2.5 kg or 5.5 lbs) with placebo at Week 68. Notably, 31.6% of participants reached ≥15% weight loss versus 4.7% in the placebo group. Cagrilintide also reduced mean waist circumference by 10.6 cm versus 4 cm with placebo. Most common adverse events were mild-to-moderate and gastrointestinal (GI) events, which were more frequent in the cagrilintide group (54%) than the placebo group (40%). GI events included nausea (24% vs. 13%), vomiting (21% vs. 12%), diarrhea (15% vs. 12%), and constipation (7% vs. 4%). By discontinuation rates, only 1% of participants discontinued due to nausea, compared with 0.1% in placebo and 6% with CagriSema, suggesting improved tolerability.
6. Discussion with Dr. Alice Cheng, Prof. Francesco Giorgino, and Prof. Ezio Bonifacio on population-wide, age-indiscriminate screening for T1D
In this standing-room-only afternoon symposium sponsored by Sanofi and chaired by Dr. Alice Cheng (University of Toronto), Prof. Francesco Giorgino (University of Bari Aldo Moro, Italy) and Prof. Ezio Bonifacio (University of Dresden, Germany) discussed the evolving landscape of T1D screening. Speakers urged attendees to think about moving beyond family history and pediatric models to encourage a more inclusive and data-driven approach to T1D screening.
- Dr. Cheng cited that more than half of new T1D cases occur in adults, yet screening efforts and diagnostic algorithms remain largely pediatric-focused. The panel highlighted findings from the Diabetes Care paper published in July 2025, “Contrasting Adult and Pediatric Populations in a Cohort of At-Risk Relatives in The T1D TrialNet Pathway to Prevention,” which showed that adults with stage 2 T1D[1] progress to stage 3 at similar rates as children (5-year risk: 78% for both groups), challenging assumptions about disease trajectory and pacing.
- On misdiagnosis, Prof. Giorgino pointed to the prediabetes space and the need for better sensitivity in tools, while acknowledging that no perfect algorithm exists. Dr. Cheng further cited that of the 39% of T1D diagnosis that are missed in adults, 77% are misdiagnosed with T2D. Prof. Giorgino discussed the AABBCC approach (age, autoimmunity, body habitus, background, C-peptide, and comorbidities) as a practical framework, with a need for continued work on improving screening for T1D.
- Dr. Cheng then directed the focus to understanding population-wide screening protocols in Italy and Germany. Prof. Giorgino highlighted Italy’s 2023 mandate for universal pediatric screening for T1D and celiac disease. He emphasized that providing concrete incentives for population-level screening, such as significant DKA reduction, is imperative in making legislative progress. Prof. Bonifacio highlighted Germany’s success with its Fr1da study, which began in 2015 and screens children in Bavaria and other regions for early-stage T1D. Studies like this serve as a model to evaluate the feasibility of population-wide screening for T1D in children. Despite the progress, Prof. Bonifacio acknowledged that there needs to be more widespread infrastructure for screening and care of those diagnosed with early-stage T1D. Ultimately, speakers emphasized that only ~10% of people with T1D have a first-degree relative with the disease, and thus identifying the remaining 90% requires robust systems and multi-test strategies at a population level.
- Dr. Cheng called for advocacy and engagement, highlighting programs like TrialNet in North America that allow individuals to enroll in research and risk monitoring. She emphasized the role of clinicians and researchers in mobilizing at-risk populations and influencing policy to expand access to screening. Drawing on the successes of Italy and Germany, highlighted by Profs. Giorgino and Bonifacio, Dr. Cheng emphasized the need for legislators to hear from those directly affected by T1D.
7. Insulin therapy and cardiorenal outcomes in T2D: A pooled analysis of CANVAS and CREDENCE
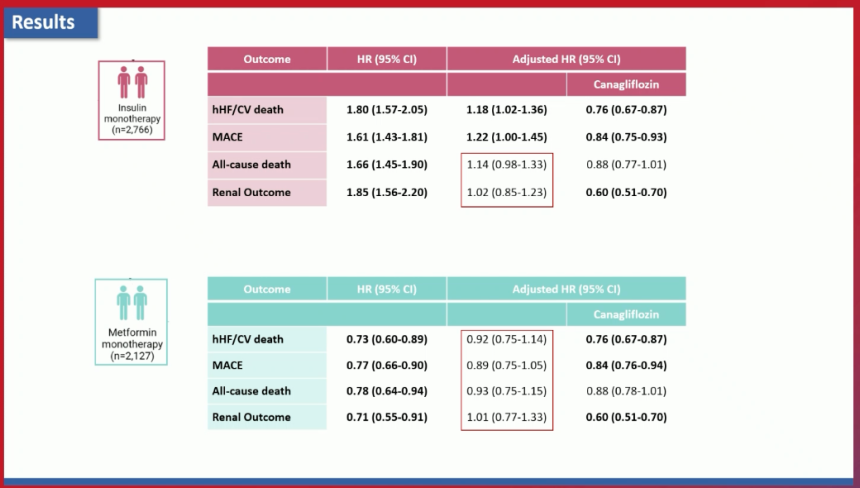
Using data from the CANVAS and CREDENCE trials, originally presented at ADA in 2017, Dr. Martina Chiriacò (University of Pisa, Italy) presented findings from an analysis assessing whether background insulin monotherapy has an impact on cardiorenal outcomes in people with T2D. As background, insulin therapy has been shown in some observational studies to increase the risk of cardiovascular disease. On the other hand, the ORIGIN study (n=12,537) found that insulin has a neutral effect on cardiovascular outcomes. Similarly, the effects of insulin therapy on renal outcomes and microvascular complications are unclear. In this analysis, pooled data from the CANVAS and CREDENCE trials investigating the SGLT-2 inhibitor canagliflozin were used to further assess the impact of insulin therapy on cardiorenal outcomes. Whereas CANVAS investigated cardiovascular outcomes for canagliflozin in adults with T2D and high CV risk, CREDENCE looked at renal outcomes for canagliflozin in adults T2D and CKD.
- Methods and baseline characteristics. Participants (n=14,530) were divided into three groups: (i) insulin monotherapy (n=2,766); (ii) metformin monotherapy (n=2,127); and (iii) other therapies (n=9,637). The cardiovascular outcomes assessed were heart failure/CV death, MACE, all-cause death, and renal outcomes. At baseline, the insulin monotherapy group had a less favorable cardiovascular profile. Participants in this group were older and had had diabetes for a longer duration. They also had higher A1c levels, higher blood pressures, greater history of heart failure and CVD, greater albuminuria, and lower eGFRs.
- Results. As shown below, univariate analyses (i.e., prior to adjusting for confounding variables) revealed that participants on insulin monotherapy, in comparison to all other participants, had significantly increased risk across all four outcomes assessed. That said, adjusted hazard ratios revealed no significant difference in risk for all-cause death and renal outcomes. Heart failure/CV death and MACE risk were also lower, though still significantly increased compared to participants on metformin monotherapy or other therapies. Importantly (and perhaps even more importantly hearing this again today, as we did back in 2017), J&J’s Invokana significantly reduced the risk of all four outcomes except all-cause death.
- Adjusted hazard ratios for participants in the metformin monotherapy group reinforced, in case there are lingering questions about the value of metformin, that metformin does not have a protective effect again cardiorenal outcomes. By contrast, canagliflozin reduced the risk of all cardiorenal outcomes assessed besides all-cause death.
8. Phase 3 study finds A1c reduction and potential cardiorenal protection with berberine ursodeoxycholate
In an overcrowded session, Dr. Linong Ji (Peking University) presented results of a phase 3 Symphony 2 trial (n=549) evaluating berberine ursodeoxycholate (HTD1801) in people with T2D. HTD1801 is a first-in-class anti-inflammatory metabolic modulator that activates AMP-activated protein kinase (AMPK; regulates cellular energy homeostasis) and inhibits the NLRP3 inflammasome. Designed to improve insulin resistance, glucose metabolism, and reduce liver fat and inflammation, this investigational drug is studied for metabolic diseases like T2D and metabolic dysfunction-association steatohepatitis (MASH). Previously, the Symphony 1 trial demonstrated significant A1c reduction (1.3 percentage points) with HTD1801 versus diet and exercise alone. The Symphony 2 trial aimed to evaluate the efficacy and safety of HTD1801 compared to placebo in people with T2D inadequately managed with metformin.
As background, berberine is used in traditional Chinese medicine and taken as a supplement to lower A1c and weight. However, as session chairs Dr. Athena Philis-Tsimikas (Scripps Whittier Diabetes Institute) and Dr. Aaron Novikoff (Helmholtz Zentrum Munich, Germany) mentioned, few robust trials have investigated the efficacy and safety of berberine until now.
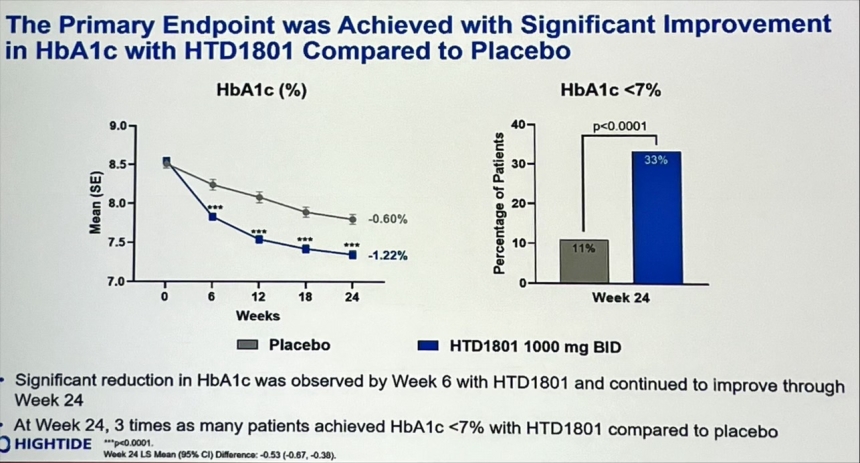
- Trial design and baseline characteristics. Conducted across 64 sites in China, the study randomized participants with A1c between 7.0-10.5% with stable metformin use to HTD1801 1000 mg twice a day (n=365) or placebo (n=184). The primary endpoint was change in A1c from baseline to Week 24, while secondary endpoints included change in fasting glucose, lipid levels, and inflammation markers. At baseline, participants were 56 years old, with 47% being female. Clinically, participants had average weight of 70 kg (154 lbs), six years of diabetes duration, and A1c of 8.5% despite metformin use.
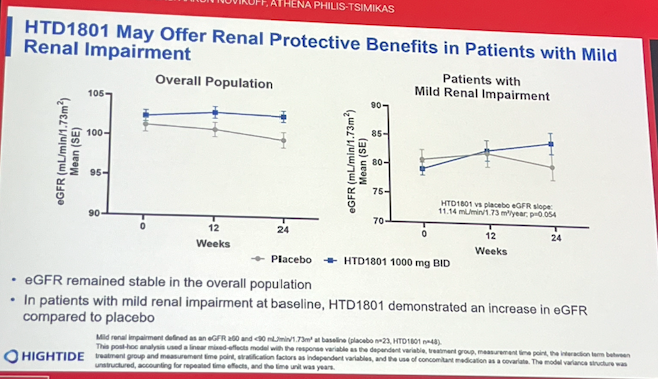
- Results. The trial met its primary endpoint, with HTD1801 conferring A1c reduction of 1.21 percentage points (vs. 0.68 percentage points with placebo; p<0.0001) at Week 24. Moreover, 33% of participants (vs. 11% in placebo group; p<0.0001) achieved A1c <7.0% at Week 24. HTD1801 also improved postprandial glucose and insulin levels, reduced LDL-cholesterol (0.35 mmol/L vs. increase of 0.01 mmol/L with placebo; p<0.0001), and lowered inflammation marker hs-CRP (p<0.01). Interestingly, Dr. Ji suggested that HTD1801 may offer renal protective benefits, as eGFR remained stable in the overall population and increased in patients with mild renal impairment (see figure below).
- Safety. Adverse events occurred in 75% of HTD1801 treatment group (vs. 68% in placebo group), while serious adverse events occurred in 4% (vs. 6%). Most common adverse events were diarrhea (23% vs. 1%). Low-grade hypoglycemia occurred in four participants receiving HTD1801 (vs. one in placebo).
Technology
9. Three years of MiniMed 780G: Durable glycemic outcomes, reduced burden, and strengthened patient confidence
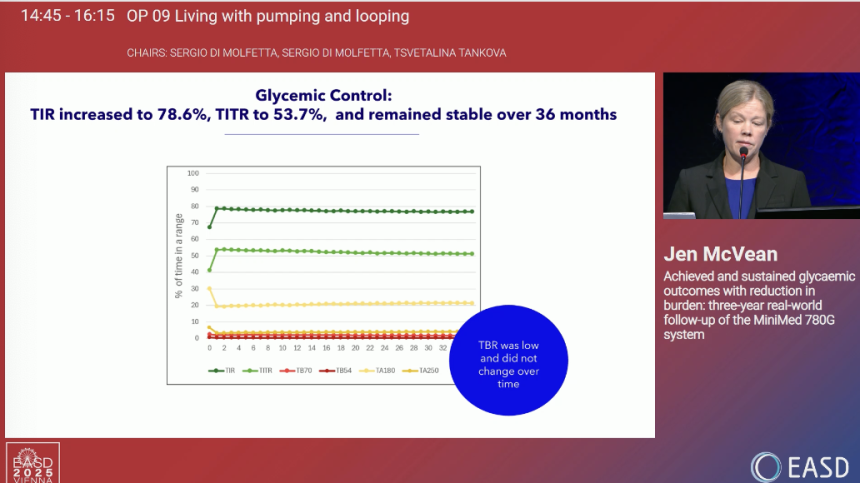
Dr. Jennifer McVean (Medtronic) presented three-year real-world results (n=1,145) from MiniMed 780G users (≥16 years old) across Europe, the Middle East, and Africa (EMEA). Participants had at least 10 days of CGM use prior to starting MiniMed 780G automated mode, and ≥10 days of CGM data per month. Results at 36 months demonstrated strong early glycemic improvements sustained throughout three years of MiniMed 780G use, achieving reductions in user burden with fewer user-initiated boluses and greater trust in the system. Dr. McVean said that these findings are especially important as we approach the fully closed-loop AID era, in that systems must be able to deliver the expected outcomes while building patient trust and reliance upon the systems.
- Early glycemic improvements across the board were sustained at 36 months of MiniMed 780G use. TIR increased rapidly from the “upper 60s%” at baseline to 79% and stayed stable throughout 36 months. TITR followed a similar pattern, increasing to 54% from a baseline of just over 40% and remaining ≥50% for 36 months. Time below Range (<70 mg/dL) decreased from 2.5% at baseline to 2.0% at one month and fell further to 1.8% at 36 months. Impressively, >75% of participants achieved target TIR >70%, and >50% achieved target TITR of >50%.
- Dr. McVean highlighted that these glycemic improvements occurred in the context of reduction burden. The percent of user-delivered insulin as a share of total delivered insulin fell from 52% to 42% at 36 months – first a rapid reduction, with a continual, gradual subsequent decrease. The amount of bolus insulin delivered automatically increased rapidly from none at baseline to 12% at one month and continued to increase over the course of the 36 months. Relatedly, user-initiated boluses fell from 5.6 per day at baseline to 4.8 per day, remaining relatively consistent over 36 months.
- User trust in the MiniMed 780G system also strengthened over the course of 36 months. The amount of time spent in automated mode, for example, remained in the mid- to upper-90% after its initial sharp rise after system initiation. At one month of use, ~40% of users were using the recommended glucose target of 100 mg/dL, reaching nearly 60% at 36 months. The recommended active insulin time of two hours had increased to 30% at one month, increasing to the mid-50% by study end.
10. Glycemic improvements with Tandem’s Control-IQ at 12 months maintained at 24 months
Prof. Jolien De Meuleeester (KU Leuven, Belgium) presented results from the INRANGE study, sharing two-year outcomes data on Tandem’s Control-IQ algorithm. Adults with T1D who started pump therapy using Control-IQ between October 2021 and December 2022 across 13 centers in Belgium were included in the study (n=473); 93% (n=442) had continued using Control-IQ at 24 months.
- Baseline characteristics. Over half (57%) of participants were men, with a mean age of 39 years and diabetes duration of 20 years. 47% were on MDI at baseline, and 53% had been on another AID system. Participants had a baseline A1c of 7.4% and TIR of ~59%.
- Results. Glycemic outcomes were consistent at 12 months and 24 months.
Metric | Baseline | 12 months | 24 months |
TIR | 59% | 71% | 71% |
TITR | 37% | 45% | 46% |
Time <70 mg/dL | 4.2% | 1.9% | 2.1% |
Time <54 mg/dL | 1.0% | 0.4% | 0.5% |
Time >180 mg/dL | 37% | 27% | 27% |
Time >250 mg/dL | 13% | 7% | 8% |
A1c | 7.4% | 6.7% | 6.7% |
- TIR. TIR increased from 59% at baseline to 71% at 12 and 24 months. The proportion of participants achieving target TIR >70% more than doubled – from 25% at baseline to 58% at 12 months and 56% at 24 months.
- TITR. A similar glycemic trend was observed with TITR, which increased from 37% at baseline to 45% at 12 months and 46% at 24 months. The proportion of participants achieving target TITR >50% nearly doubled, increasing from 18% at baseline to 30% at 12 months and 32% at 24 months.
- A1c. A1c fell from 7.4% at baseline to 6.7% at 12 months, which was maintained at 24 months. The proportion of participants achieving target A1c <7.0% nearly doubled, rising from 34% at baseline to 66% at 12 months and 64% at 24 months.
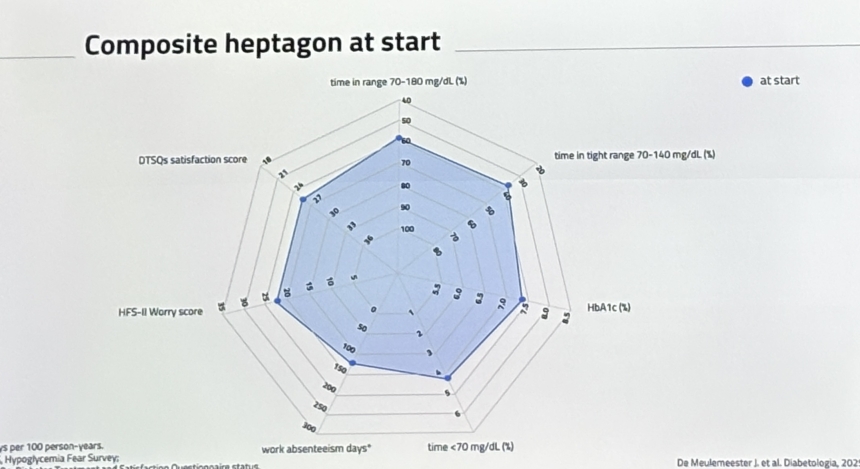
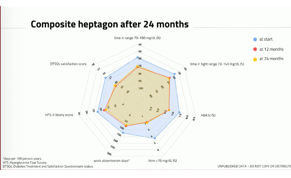
- Improvements to self-reported quality of life (QoL) at 12 months were also maintained at 24 months. Specifically, Control-IQ users reported significant improvements to physical and general health, as well as social function at 12 months. Significant improvements to physical health and social functioning were maintained at 24 months. Improvements to diabetes-specific QoL factors (see figure below) were all sustained at 24 months.
- Improvements in self-reported severe hypoglycemic events (SHE) and work absenteeism at 12 months were also sustained at 24 months. Self-detection of SHE had increased from four to 16 annual events at 12 months of use, and 15 annual events during the second year of Control-IQ use – a simply outstanding result. Similarly, the number of absentee days at work also nearly halved after 12 months of use – from 126 days to 73 days – and further fell to 69 days per year at 24 months. The confluence of these outcomes led to a maintenance of the composite heptagon – consisting of TIR, TITR, A1c, TBR, work absenteeism days, hypoglycemia fear survey worry score, and satisfaction score – at both 12 and 24 months of use (see figures below).

11. Safety and accuracy of CGM for inpatient DKA management compared to hourly POC testing
Dr. Magdalena Bogun (Columbia University) presented a single-center observational study (n=163) evaluating the safety and accuracy of inpatient CGM for DKA management with IV insulin infusion compared to standard hourly point-of-care (POC) testing. Conducted at the height of the COVID-19 pandemic, the study included 44 patients monitored with Dexcom G6 CGM in an ED stepdown unit and 119 patients monitored with hourly POC testing in the ED or ICU. CGM was initiated at what was characterized as “provider discretion”. A smartphone receiver was placed on the IV pole, and both clinicians and nurses carried smartphone receivers to access real-time CGM data. Providers were instructed to confirm CGM values >350 mg/dL with POC testing, and CGM was primarily used for treatment adjustments between 100–350 mg/dL (unlike “real life” given that patients were on IV drips, glucose levels under 100 mg/dL weren’t seen). Addressing concerns expressed during Q&A about the expected accuracy of Dexcom G6 use during DKA and severe hyperglycemia, Dr. Bogun said that CGM was typically inserted after glucose levels had fallen below 350 mg/dL, allowing clinicians to track fluctuations during IV insulin therapy until discharge.
- Baseline characteristics: Adult participants had a mean age of 49 years with a fantastic mix of both T1D (40%) and T2D (60%). A little over half, 54%, were male. Admission labs and labs at DKA resolution did not differ between groups. Overall, 36% of participants required ICU admission — 50% in the SOC group vs. none in the CGM group.
- CGM accuracy: While Dexcom G6 sensors showed a MARD of 17.4% during IV insulin treatment and 19.8% after DKA resolution, above the widely-accepted threshold of 10% for most commercially available CGMs in outpatient use, it would be great to know a little more about how the comparisons were created. Clarke Error Grid analysis found 99% of paired values in Zones A/B during treatment and 96% post-resolution.
- Clinical outcomes. Time to DKA resolution was similar between groups (12.8 hours with CGM vs. 12.0 with POC). Median hospital length of stay was comparable and said not to be statistically different though the difference, 120 hours vs. 99 hours, is one that patients may perceive as different – a full day! Median ICU stay in the SOC group was 28.5 hours. As expected, CGM patients required significantly fewer POC tests (median of five vs. 12; p<0.0001). Notably, hypoglycemic events were rare and not significantly different (0% vs. 3%), due to the insulin drip. Dr. Bogun emphasized that these findings demonstrate the safety of remote monitoring in hospital settings among people with diabetes admitted in DKA. She further hypothesized that the reduction in ICU admissions with CGM monitoring could lower system costs by reducing the time taken to conduct hourly POC glucose measurements (a dreaded task by many nurses as we understand it) without compromising outcomes. Presumably, a benefit would be to nursing productivity.
12. International RCT finds CGM reduces risk of large-for-gestational-age infants in women with GDM
Prof. Tina Linder (Medical University of Vienna, Austria) presented results from the GRACE trial, a large multicenter randomized controlled trial (RCT) evaluating the impact of CGM usage versus self-monitoring of blood glucose (SMBG) on obstetric outcomes in women with gestational diabetes (GDM). We can’t begin to believe how much better CGM use must be for women with diabetes, especially new diabetes – gestational diabetes!
- Study design. The open-label trial enrolled women with GDM (n=375) across four sites in Austria, Germany, and Switzerland. Participants were randomized 1:1 to either Dexcom G6 CGM (n=190) or SMBG (n=185). Women in the SMBG group also wore a blinded CGM for 10 days after randomization and again at 36-38 weeks’ gestation, while those in the intervention group used CGM continuously until delivery. The primary endpoint was the proportion of large-for-gestational-age (LGA) infants, with secondary endpoints including maternal/neonatal outcomes, insulin use, CGM metrics, and safety. We are interested in learning more about short-term differences in cost, which wasn’t discussed, so that appropriate investment can be considered.
- Results. LGA occurred in 3.5% of infants in the CGM group versus 10.3% with SMBG, representing a whopping, statistically significant reduction that persisted after adjustment for baseline characteristics and study site (to say nothing of, we’re sure better health will likely also persist, but of course, that is unknown and hardly measurable unless a longer-term trial could be designed). Mean newborn weight percentiles were also lower in the CGM group. As would be expected, women using CGM demonstrated better TITR (65-140 mg/dL[2]) between 36-38 weeks of gestation compared to baseline.
- Conclusion. Researchers concluded that CGM use lowers the risk of LGA infants in women with GDM and can help identify those who need intensified insulin therapy – to say nothing of, presumably, monitoring and taking care to prevent T2D. Prof. Linder emphasized that these findings, together with improved glycemic management, support CGM as a valuable tool and the standard of care in the management of GDM.
13. INLOOP study: One-year real-world outcomes with Diabeloop DBLG1 show durable glycemic and quality-of-life benefits
Prof. Maria Lytrivi (Université libre de Bruxelles, Belgium) presented results from the prospective INLOOP study that assessed real-world outcomes with Diabeloop’s DBLG1 AID system. The French-based system evaluated in the study consisted of Diabeloop’s DBLG1 algorithm, Roche’s Accu-Chek Insight pump, and the Dexcom G6 CGM. Roche’s Accu-Chek Insight pump uses pre-filled NovoRapid PumpCart cartridges and allows users to set “very low” basal rates (down to 0.2 U/hour). While the AID market in Europe is increasingly competitive, the Diabeloop algorithm – housed in a locked-down handset – has predictive low-glucose suspend, basal rate adjustment automation, automatic correction bolus features, and activity modes for quick adjustments, including ZENmode to temporarily raise target glucose (and ensure no lows). We are curious to see how these positive outcomes with the DBLG1 system will translate to the launch of the next-generation DBLG2 algorithm slated for next year, as well as any potential differences in real-world outcomes for DBLG1 users with ViCentra’s Kaleido patch pump – which is slightly smaller (5 cm x 3.5 cm x 1.25 cm and weighing 15 grams) than Insulet’s Omnipod 5 (5.2 cm x 3.9 cm x 1.45 cm and weighs 26 grams).
- The study enrolled 167 adults with T1D across 12 Belgian centers between May 2022 and September 2023. Participants had a mean age of 44 years, mean diabetes duration of 26 years, and mean BMI of 26 kg/m². In the study, 62% of the participants were female, 96% were CGM users at baseline, and 41% reported microvascular complications.
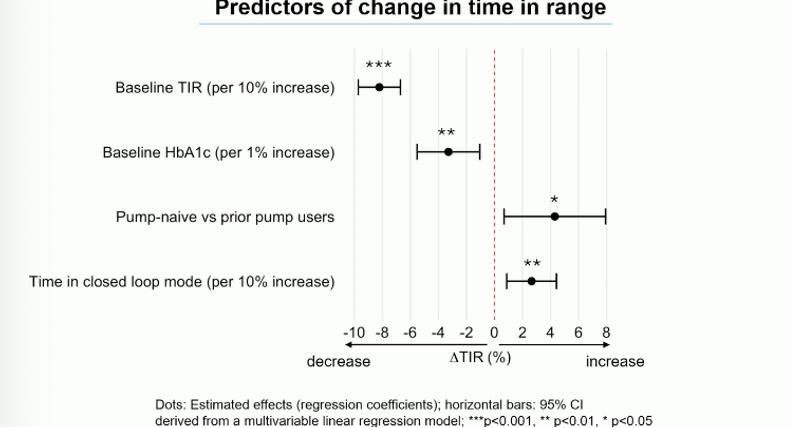
- Glycemic outcomes significantly improved at four months and were sustained at 12 months. Improvements in TIR were greatest in individuals with lower baseline TIR, higher baseline A1c, pump-naïve status, and higher automated mode use (see figure below).
- TIR improved from 57% at baseline to 70% at four months and was sustained at 69% at one year. The proportion of participants achieving TIR >70% more than doubled over that period, from 18% to 47%.
- Time in Tight Range (TITR; 70-140 mg/dL) rose in line increased meaningfully, though far less than TIR (not surprising given tighter targets), moving from 35% to 42% at one year, or seven percentage points compared to 29 percentage points for TIR, about 4x greater a move.
- Time below Range (TBR; <70 mg/dL) dropped from 3.7% to 1.4%, with 92% achieving the <4% target vs. 52% at baseline. The rate at which hypoglycemia and severe hypoglycemia have diminished in recent years is so gratifying for the field – next is working out how a far higher percentage of people with T1D (and T2D) can have access to AID.
- A1c dropped from 7.6% to 7%, 0.6 percentage points, and, strikingly, the proportion achieving A1c of <7% doubled, from 27% to 54%.
- Quality of life. After one year, participants reported moderate improvements in fear of hypoglycemia, treatment satisfaction, and diabetes impact, alongside small-to-moderate gains in overall problem areas and device satisfaction.
- Safety and discontinuation. Severe hypoglycemia fell markedly, with the proportion of participants affected dropping from 10% to 1% and the event rate declining from 116 to 8.6 per 100 patient-years. Most discontinuations occurred in the first four months (53%), mainly due to technical issues, system complexity, or alarm fatigue.
14. RADIANT adult sub-analysis (n=79): Omnipod 5 drives significant A1c and TIR gains vs. MDI with CGM, with A1c reaching 7.2% and an extra five-plus hours time “in range”
Prof. Bruno Guerci (University of Lorraine, France) presented an adult sub-analysis of the RADIANT study (n=79), which compared Omnipod 5 to MDI with FreeStyle Libre 2 CGM in people with T1D. The RADIANT trial originally enrolled 188 participants (children and adults) across 19 sites in Belgium, France, and the UK. All participants had ≥one year of T1D diagnosis and ≥three months of MDI with CGM use. After two weeks of baseline data collection, participants were randomized 2:1 to Omnipod 5 (n=125) or MDI with CGM (n=63) for just over three months (13 weeks). Overall, Omnipod 5 drove a 0.8 percentage point greater A1c reduction vs. MDI with CGM (falling from 8.1% to 7.2%; p<0.0001).
- Adult demographics. Adults in the study had a mean age of 40-41 years and a diabetes duration of ~20 years. Interestingly, most Omnipod 5 users selected the lowest glycemic target of 110 mg/dL for 57% throughout the study, and spent 99% of their time in automated mode. The groups were nearly evenly split by sex.
- In the new sub-analysis presented, Prof. Guerci highlighted that adults with higher baseline A1c (≥8.0%) saw a 1.1 percentage point greater treatment-adjusted A1c reduction with Omnipod 5 (falling from 8.7% to 7.5%) vs. MDI with CGM (from 8.6% to 8.5%), which had exactly the same drop in A1c of 0.1 percentage points. He also noted that gains in TIR were driven primarily by reduced rates of hyperglycemia: Omnipod 5 users saw a 23-percentage-point treatment-adjusted reduction in TAR (>180 mg/dL), falling from 57% to 33% compared to an increase from 54% to 56% in the MDI with CGM cohort. Furthermore, Omnipod 5 users experienced a 10-percentage-point reduction in Time >300 mg/dL (falling from 13% to 3.4%; reduction of 2.4 hours/day), whereas MDI with CGM users experienced a two-percentage-point increase (rise from 12% to 14%).
- Consistent with the full RADIANT population, no significant group differences were seen in TBR <70 mg/dL (2% with Omnipod 5 vs. 1.4% in adults using MDI with CGM) or Time <54 mg/dL (0.2% vs. 0.1%, respectively). However, Prof. Guerci noted that more Omnipod 5 users achieved target TBR <4% at 13 weeks (92% vs. 82%, respectively)
- Previously, topline results of the RADIANT trial were presented at ATTD 2025. Participants randomized to Omnipod 5 (n=52) achieved an A1c reduction by 0.9 percentage points (falling from 8.3% to 7.3%), compared to a 0.1 percentage point reduction with MDI with CGM (from 8.2% to 8.1%; n=27) – this A1c change is not only far smaller, but also not close to target. At 13 weeks, adults on Omnipod 5 achieved 65% TIR (up from 41% at baseline), while the MDI with CGM group averaged 42% TIR (down from 43%). This result represented a 23% baseline-adjusted difference, reflecting an increase of 5.6 hours/day spent in TIR.
15. Exercise boosts TIR in CGM analysis of adolescents with T1D (n=3,069)
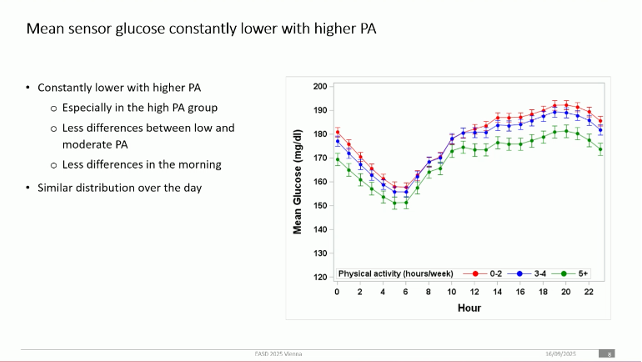
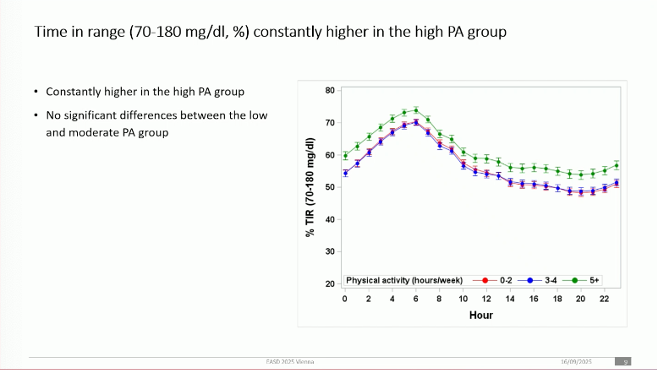
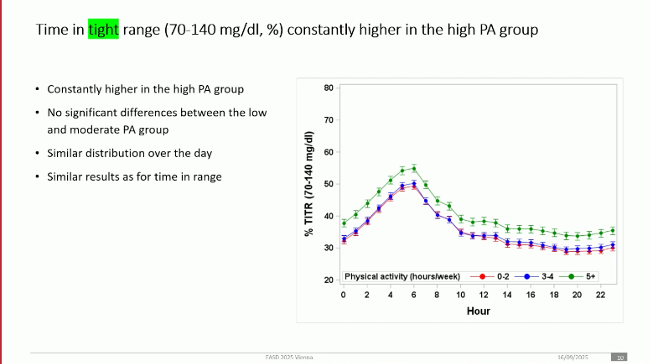
Dr. Alexander Eckert (University of Ulm, Germany) presented an analysis of CGM patterns in adolescents with T1D (n=3,069), stratified by physical activity level. Data were collected from >500 centers across Germany, Switzerland, and Austria between July 2023 and December 2024, including ~90% of children and adolescents with T1D. Participants were categorized by weekly activity: (i) low (<2 hours); (ii) moderate (3-4 hours); and (iii) high (≥5 hours). Dr. Eckert suggested that the lower-than-expected threshold for “high” weekly physical activity could represent an achievable target for youth with T1D, along with proper education on maintaining glycemic safety during exercise.
- Baseline characteristics. AID use was similar across groups (~two-thirds of participants). The high-activity group included more boys (63% vs. 47% [low] and 53% [moderate]). Mean age was 15 years with a baseline A1c of ~7.3%. Interestingly, baseline TIR rose modestly with more activity (58% low, 59% moderate, and 63% high).
- Higher activity was associated with lower mean glucose throughout the day, particularly in the afternoon and evening, along with higher TIR and TITR (70-140 mg/dL). These improvements were driven by less TAR (>180 mg/dL). Low and moderate activity did not show significant differences.
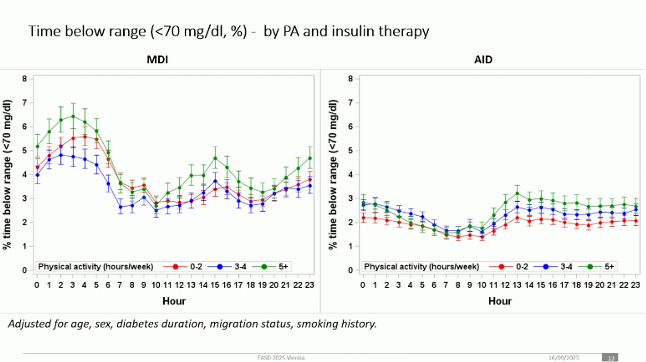
- MDI users showed higher glucose peaks in the afternoon and overnight, with larger differences by activity level. In contrast, AID users had smaller, steadier afternoon peaks and fewer differences across cohorts, reflecting tighter glycemic management (see figure below). A slightly higher risk of afternoon and overnight hypoglycemia with greater activity was noted, mainly in AID users. Still, Dr. Eckert emphasized that for most adolescents with T1D, the glycemic and overall health benefits of physical activity far outweigh the risks.
16. *NEW* Insulet-sponsored symposium emphasizes scalable onboarding strategies and real-world outcomes with Omnipod 5 in T1D
Prof. Pratik Choudhary (University of Leicester, United Kingdom) and Dr. Sandra Schlüter (Hannover Medical School, Germany) shared practical strategies for expanding access to AID systems, drawing on experiences with Omnipod 5 in both group-based and virtual settings. The pair engaged the audience with interactive polling and a case-based discussion, underscoring both the real-world benefits of AID and the logistical challenges of scaling initiation. Speakers repeatedly emphasized one theme throughout the session: given the simplicity of Omnipod 5, healthcare teams can rethink traditional workflows to onboard more patients simultaneously, without compromising safety or outcomes.
- Real-world outcomes mirror trial results, reinforcing Omnipod 5’s impact on both glycemic outcomes and quality of life. Prof. Choudhary and Dr. Schlüter referred to data from the RADIANT trial and compared it to results in their own clinics, showing mean Time in Range (TIR) improvements of >20 percentage points (from ~40% to >60%), with minimal hypoglycemia. They also emphasized the benefits conferred by using Omnipod 5’s optimal settings. In global datasets, patients using lower glucose targets (110 mg/dL) and more aggressive carbohydrate settings achieved median TIR of 74-77%. Prof. Choudhary and Dr. Schlüter also shared patient stories from their own clinics, including an individual with decades of poor management who saw their A1c levels fall from 10% to 6.9% after switching to Omnipod 5, with concurrent and significant quality of life improvements.
- Group-based onboarding approaches have improved access for many patients. In Leicester, the UK, Prof. Choudhary detailed how his team increased annual initiations from ~30 patients to more than 400 by moving sessions out of hospitals and into community centers, starting 20 patients at a time. Additionally, he said that his team was able to successfully scale onboarding by removing several common barriers, including: (i) removing carbohydrate counting; (ii) streamlining settings set-up; and (iii) harnessing cloud-based care to provide “light touch” follow-up support. In a similar vein, Dr. Schlüter said that she implemented smaller-group (four to six patients) sessions paired with structured safety training, peer-to-peer learning, and immediate system start-up. She noticed that peer support has been a powerful driver of sustained success, with some cohorts forming their own WhatsApp groups that continue long after onboarding. While audience polling suggested that only ~20-25% of patients in many European clinics are currently using an AID system, both speakers agreed that systems like Omnipod 5 should be available to all, challenging healthcare providers to now shift their attention to scaling adoption.
Big Picture
17. Prof. Chantal Mathieu delivers most-valuable EASD Presidential Address, extolling vision for personalized, global diabetes care
Opening the 61st EASD Annual Meeting, Prof. Chantal Mathieu (UZ Leuven, Belgium) set the tone for the week with a wide-ranging Presidential Address that both celebrated the growth of EASD and set an ambitious agenda for the future. She welcomed over 13,500 participants and pointed to a record 2,170 abstracts submitted, with 1,354 accepted and over 1,900 presentations scheduled across the next five days. Describing the program as a “feast of science,” she emphasized that the meeting would span topics ranging from disease insights and treatment advances to disease modification, late-breaking clinical trial results, and implementation research.
- “Rethinking diabetes” and an emphasis on precision medicine framed the scientific agenda. Prof. Mathieu urged the field to move beyond the rigid labels of T1D and T2D and instead view diabetes as a spectrum. Citing a recent Diabetologia publication on T1D heterogeneity, she emphasized that variability exists across all forms of diabetes. She highlighted the importance of diagnosing the individual rather than the type, pointing to precision medicine as the future of care. In her vision, the next era of diabetes care will be defined by individualized types and personalized treatment pathways.
- New initiatives reflect EASD’s ongoing investment in education, publishing, and global engagement. Prof. Mathieu introduced innovations such as “lab talks,” offering behind-the-scenes perspectives from leading researchers, and emphasized preparing the next generation through expanding the Early Career Academy. She announced new training opportunities including EASD’s first immunology course and a continuation of the technology school program to equip clinicians for immunology-based disease-modifying therapies. Prof. Mathieu also celebrated Diabetologia’s60th anniversary, while introducing Metabologia, a new open-access sister journal extending into obesity, complications, and immunology. Globally, she discussed the newly established Global Council and the Global Impact Prize, while commending the European Diabetes Forum (EUDF) under Prof. Stefano Del Prato’s (University of Pisa, Italy) leadership for elevating diabetes policy discussions across Europe.
- She underscored that the implementation of findings remains a central challenge for the field. Prof. Mathieu cautioned that research without translation will not demonstrate effective impact over time. She cited the upcoming release of the EASD’s first-ever guideline on diabetes distress as an actionable step toward bridging evidence and clinical practice. Developed in response to clinician input and the voices of people with diabetes, the guideline addresses an overlooked but critical need and hopes to inspire the publication of future implementation-focused guidelines
- Closing her presidency, Prof. Mathieu reflected on her term with gratitude and hope. She thanked colleagues, staff, and the executive board, announcing that Prof. Francesco Giorgino (University of Bari Aldo Moro, Italy) will succeed her as President of EASD in 2026. She finished with a message of hope: wishing the diabetes community not only good health, but also a peaceful world as EASD looks ahead to its next chapter. Prof. Mathieu has long been a trusted and thoughtful voice in the field – one whose commentary we have frequently sought on a range of topics. She will be deeply missed as EASD President, and we look forward to following her continued impact on the field. We also are eager to see what comes next as Prof. Giorgino assumes the role in 2026.
18. Under promise and over deliver: Dr. Dan Drucker on his philosophy for scientific research
In the first of eight “Lab Talks” at EASD this week, Dr. Dan Drucker (University of Toronto) shared his philosophy on research, emphasizing the importance of reproducibility. As background, Lab Talks are brand new to EASD this year and offer attendees the rare and valuable opportunity to hear esteemed lab heads share their perspectives on research and ask questions. There are two sessions daily — see below and here for the full list of speakers.
- Reproducibility in research: Creating a definition. Dr. Drucker highlighted that there are multiple ways to approach reproducibility in research. While it’s important to see whether other labs can reproduce a study’s findings, Dr. Drucker maintained that it’s more important that the original researcher is able to repeat their own findings. As for methods, Dr. Drucker felt that there is ultimately no “right” or “wrong” way to reproduce results, whether that’s using one of the many types of animal models available, human subjects, or other ways. The key for researchers, he said, is to define what reproducibility means to them. This can vary, which Dr. Drucker highlighted with a hockey analogy. In the Canadian NHL playoffs, the first team to win four of seven games is deemed the winner. Everyone accepts this, and no questions are asked. He then asked the audience whether this would apply to research (i.e., if you conduct an experiment seven times and get it right four of those times, does it work?). He said there is no right or wrong answer, but rather a philosophical issue and a matter of definition. For Dr. Drucker, reproducibility means producing the same findings every single time.
- Addressing the reproducibility crisis through a look within. Dr. Drucker pointed out the enormous pressure researchers and trainees now face to have impressive stories and publications in high profile journals. He said, “Honestly for me, that’s hard to do,” and instead shared that he prefers more “careful, small, and incremental” science, words which he said often appear in reviewer comments when a paper is rejected. The pressure to produce novel and appealing research has created a reproducibility crisis, and Dr. Drucker called on the audience to look internally (i.e., the researchers themselves) for the source of this crisis. Media releases for research studies can sometimes overhype and exaggerate findings, creating false hope and inflated expectations (e.g., “I just read that they’ve cured…”). He said that his lab tries not to feed into the hype, pointing out to audience members that they likely would not be able to find any press releases from the Drucker lab related to its involvement in discovering DPP-4 inhibitors or GLP-1 RAs, among others. His philosophy for scientific research, he said, is to under promise and over deliver.
- “Trust but verify.” Dr. Drucker and his lab have done extensive work on localizing the GLP-1 receptor, and he said that 80-90% of papers that describe attempts to localize the receptor are “flat out wrong” because the researchers did not take the time to validate the reagents used in the study. He said that many reagents (e.g., antibodies) researchers purchase to use in studies are allegedly trustworthy but not truly so, adding that some reagents being used in these localization studies are “useless” and still being used to publish papers in major journals.
- Publications: A tale of the tortoise and the hare. On publishing research in journals, Dr. Drucker said that while it is good to aspire to publish in top journals, at the end of the day, one can get just as far, if not farther, by publishing high-quality papers in “solid” journals. He showed how many of his major papers early on were all published in PNAS (PNAS currently has an impact factor of 9.1, while the Lancet’s is 88.5 and NEJM’s is 78.5).
- Industry funding and relationships. As Dr. Drucker summarized in the slide below, there are advantages and disadvantages to working with industry on research. In his case, he said that the benefits outweighed the risks, especially as government funding for scientific and medical research is less robust in Canada where he is based.
Preview
- Prof. Antonio Zorzano | 12:00 pm - 12:45 pm, Wednesday
- Prof. Mikael Rydén | 1:00 pm - 1:45 pm, Wednesday
- Prof. Miriam Cnop | 1:00 pm - 1:45 pm, Thursday
- Prof. Roberto Mallone | 2:00 pm - 2:45 pm, Thursday
- Prof. Guido Sebastiani | 10:15 am - 10:45 am, Friday
- Prof. Reiner Jumpertz-von Schwartzenberg | 11:45 am - 12:15 pm, Friday
We will include either this week or in our EASD full report the talk from Prof. Juleen Zierath, which also took place today, and that we were unable to report on live.
19. 57th Claude Bernard Lecture by the esteemed Professor Andrew Hattersley focuses on “precision diabetes”: Learning from the rare and applying to the common
Prof. Andrew Hattersley (University of Exeter, UK), was awarded the Claude Benard Lecture prize in recognition of his innovative leadership and lifetime achievements in diabetes research. This year’s award at EASD was handsomely underwritten by Sanofi, and the presentation began with a wonderful video of Prof. Hattersley at his lab in Exeter, reminiscing about his work there that began thirty years ago, starting in 1995! Prof. Hattersley received an extremely warm round of applause, to which he said, “Having been in the audience at EASD for 34 years and having watched my heroes give this lecture, it feels like a dream to be here on stage …” (and, he allowed, “also absolutely terrifying”). Prof. Hattersley’s lecture focused on the development of “precision diabetes” – methods of identifying diabetes subtypes that result in practical treatment differences and differentiated outcomes. He discussed neonatal diabetes – monogenic diabetes diagnosed within the first six months of life, MODY (Maturity-Onset Diabetes of the Young), non-autoimmune insulin deficient diabetes seen in African populations, adults who were diagnosed with T2D and later found to have T1D, and even the promising future of precision therapeutics. For many years now, we’ve regarded Dr. Hattersley as a major diabetes hero – and attended literaly dozens of his presentations that we have documented in our Close Concerns KnowledgeBase – so seeing this prize awarded felt incredibly exciting to us, as well as very inspirational.
- “Precision diabetes” was first explored with respect to neonatal diabetes - monogenic diabetes diagnosed within the first six months of life. Neonatal diabetes is about 2-3% of all pediatric diabetes. It was discovered that 50% of neonatal diabetes results from potassium channel mutations and can be treated very successfully with a high dose sulfonylurea. 90% of these patients eventually stop taking insulin and even discontinue blood glucose monitoring. After pioneering work by Prof. Hattersley’s team, today there are 453 known sub-types of neonatal diabetes that can be identified by genetic sequencing, resulting in the selection of the most appropriate treatment in each case. The University of Exeter offers free testing globally, having tested 3,569 patients from 114 countries to date.
- In a similar vein, testing for MODY can reveal genetic sub-types with the appropriate treatment options, and this approach has become the standard of care. MODY is commonly misdiagnosed – as 97-99% of people with a diabetes diagnosis do not have monogenic diabetes, it remains difficult to rationalize universal testing for MODY. Some presentations are well-known, such as diabetes with a renal development disease or neural deafness. For other cases, Prof. Hattersley has developed standards. For example, “T1D” patients that are three-antibody-negative have a 12% chance of having MODY. This rises to 33% if they have an A1c <7.5% or a parent with diabetes. There is also a MODY calculator for people with a T2D diagnosis – the probability of MODY rises with younger age at diagnosis and lower BMI.
- Certain subtypes of T1D are rarer and do not have differentiated treatment options. Prof. Hattersley explained that certain pancreatic endotypes have different C-peptide levels. There is also non-autoimmune insulin deficient diabetes that presents very similarly to “regular” T1D in slim young people. Prof. Hattersley discussed “YODA” – a trial of Young-Onset Diabetes in sub-Saharan African children who had T1D, where, strikingly, 65% of the participants had no islet autoantibodies. The investigators ruled out T2D, monogenic diabetes, ketosis, and malnutrition and also noted that this subtype was present in 16% of Black people with T1D in the USA.
- Getting the correct diagnosis is key – adults are often diagnosed with T2D, but in fact have T1D. For example, former UK Prime Minister Theresa May was diagnosed at 56. It may be difficult to correct this problem since T1D is such a rarity in older age groups, despite the fact that 50% of people with T1D develop it as adults. Studies show that within three years, almost everyone in this class is being treated correctly with insulin, although the diagnosis may still be incorrect.
- On the other hand, there are people diagnosed as “adult T1D” that actually have T2D. An antibody test can help clarify, and will distinguish patients that may have T2D or MODY. This is why Prof. Hattersley commented: “If you think it’s T1D, do the antibodies.” He also recommended that all longstanding “T1D” adults and insulin-treated people with “T2D” deserve a C-peptide test – just to make sure the diagnosis is correct and insulin is required.
- Finally, Prof. Hattersley turned to T2D – arguably the most challenging since it is well known to be polygenic. There are diverse presentations and treatment regimens present in T2D – but Prof. Hattersley continues to wonder if they are optimal. Years of work developing subtypes based on genetic and clinical factors were not successful in predicting treatment outcomes, but this year, Dr. John Dennis (University of Exeter, UK) developed a five drug model drawing upon his actuarial background (recently expanded to include semaglutide) that takes routine data such as age at diagnosis, sex, BMI, duration of diabetes, baseline A1c, eGFR, HDL and ALT and predicts the response of five treatments (DPP-4 inhibitors, SGLT-2 inhibitors, sulfonylureas, TZDs, and GLP-1 RAs) ‑ see chart below. The model has been tested with data from clinical trials and delivers a ~0.5% mean improvement in A1c compared to non-optimal glucose lowering, equivalent to a 2.5-year delay in treatment intensification. The model also delivered a reduction in five-year complications.
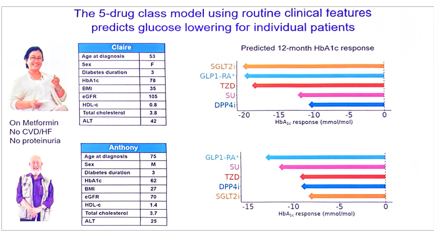
- The model had some surprising findings – for example, it predicts that GLP-1 RAs lower A1c the most compared to other therapies for 70% of females, but only 10% of males. How fascinating! GLP-1 RAs also tend to be less effective for those with higher BMI or lower age at diagnosis. What’s next, in terms of creating impact from these findings? As we understand it from Professor Hattersley, the next steps are to validate a software decision aid to be used in clinical practice. A test version can be found here. For the first time, this is practical precision diabetes for T2D. As we have seen for some years now, and reinforced mightily in Professor Hattersley’s lecture, it sure seems like “precision diabetes” has a promising future.
20. Novel diabetes subgroup classifications and optimized treatment plans based on glucose variability patterns from CGM data
Dr. Anuj Maheshwari (Hind Institute of Medical Sciences, India) and Dr. Shubhashree Patil (Diabetes and Wellness Clinic, India) presented data from a prospective observational study, identifying optimal treatment plans for five novel diabetes subgroups, classified after two weeks of CGM wear (n=527). The study was driven by the need to improve the personalization of diabetes care, with 40% of treatments failing due to inappropriate medication adherence and 60% of patients with similar A1c showing different glucose patterns. Both presenters said that treatment personalization based on CGM phenotype can reduce the trial-and-error associated with many first-line treatments. Most participants (87%) had already been diagnosed with T2D, and the remaining 13% had T1D diagnoses. Participants completed 14 days of CGM wear and a six-month follow-up evaluation. Almost 75% of patients with T2D were on baseline metformin, and the proposed optimal treatment plans below were considered as adjunct therapies.
- Dr. Maheshwari listed processes for clinical practice. Implementation requires: (i) a 14-day CGM assessment; (ii) automated subgroup classification with machine learning; (iii) clinical treatment selection depending on subgroup classification; and (iv) follow-up monitoring by specified subgroup outcomes. Participants in the subgroups were not randomized to different treatment options.
- The five novel diabetes subgroups and their optimized treatment courses included:
- Stable hyperglycemia (31%). This subgroup was characterized by consistently elevated glucose of 200-300 mg/dL and coefficient of variation (CV) <20%. It was often seen in those with advanced T2D. Dr. Maheshwari explained that the study identified primary treatment include long-acting insulin or high-dose metformin with lifestyle modifications focused on consistent carbohydrate intake. Ongoing monitoring should focus on A1c trends rather than daily variability.
- Postprandial spike (22%). This subgroup was characterized by excessive postprandial glucose excursions and delayed returns to baseline fasting glucose and was especially common in those with early T2D. Dr. Maheshwari emphasized that first-line treatment for those in this subgroup should include GLP-1 RAs, with prandial rapid-acting insulin if needed. Dr. Patil said that those who initiated GLP-1 RAs in this subgroup saw a 32% reduction in glycemic variability, significantly greater than the 9% reduction seen in those who initiated GLP-1 RAs classified to other subgroups (p<0.001).
- Brittle hypoglycemia (18%). Participants had frequent hypoglycemic episodes and glucose CV >35%, as well as unpredictable insulin sensitivity. They often had T1D or “advanced” T2D. Dr. Maheshwari said that optimal treatment for this subgroup should include hybrid closed loop (HCL) pump options. For regions or populations for which the technology is not available or affordable, CGM-guided insulin adjustments with hypoglycemia-aware algorithms should be used. Dr. Patil explained that participants in this subgroup using AID saw a 76% reduction in the number of hypoglycemic events compared to a 34% reduction in events with MDI (p<0.001). She also reported that those on AID had higher mean TIR and self-reported quality of life scores. As a sidenote, we are surprised that “brittle” continues to be used as a term to characterize even a “type” of complication of diabetes, though it is certainly better than characterizing diabetes this way or worse as a noun or as a “type” of diabetes that someone has! (It’s great not to see reference, for example, to “a brittle diabetic” or even “she has brittle diabetes” – etc!)
- Dawn phenomenon (16%). Dr. Maheshwari emphasized that participants with pronounced dawn phenomenon often go unrecognized in clinical care without CGM-based evaluation. He said that the participating clinics preferentially prescribed SGLT-2 inhibitors or intermediate-acting insulin for those in this subgroup. Upon SGLT-2 inhibitor initiation, those in this cohort saw a mean 28% greater reduction in morning hypoglycemia compared to baseline. Dr. Patil added that SGLT-2 inhibitor initiators in this subgroup saw a mean reduction in morning glucose of 63 mg/dL, significantly greater than the 18 mg/dL reduction seen in those classified to other subgroups. While the data was not provided, she said that they also saw stronger A1c reductions and greater differential weight loss of over 1 kg compared to other subgroups.
- Erratic fluctuators (13%). These “difficult-to-manage” participants were characterized by unpredictable glucose patterns throughout the day, with high glycemic variability without clear triggers. Dr. Maheshwari’s comprehensive treatment plan for those in this subgroup included: (i) rt-CGM (which is the only type of CGM used in most geographies, to our knowledge); (ii) combination therapy with “flexible dosing”; (iii) self-management education (presumably many have had this already); and (iv) endocrinologist-directed treatment co-management (presumably many already have this as well).
- Dr. Patil said that the CGM-based classification system by glycemic patterns predicted hospitalization risk significantly higher rates than traditional predictors including A1c, disease duration, and known risk factors (AUC ROC 0.83 vs. 0.67, respectively; p<0.001). Dr. Maheshwari reported a 35% improvement in treatment response rates, 45% reduction in medication changes, and 60% increase in patient treatment satisfaction. Furthermore, she said that treatment adherence increased from 73% to 89% and that the time to optimal therapy reportedly decreased with use of the CGM-based classification system. A multi-center study across 15 countries is currently planned (n=2,500) to validate these findings and help determine if participants may change subgroups with long-term treatment.
21. Fructose consumption may play a key role in the development of MASLD
Interest was high in this very “basic science”-heavy oral presentation by Dr. Florine Westerbeke (Amsterdam University, the Netherlands), whose work suggested a potential new physiological pathway for the development of metabolic dysfunction-associated steatotic liver disease (MASLD). Dr. Westerbeke began by emphasizing, as we have heard time and again, about MASLD’s worldwide prevalence, with the condition affecting approximately one-third (!) of the global population and expected to rise to 55% by 2040. Genetic factors such as the PNPLA3 and TM6SF2 genes[3] have been linked to the development of the condition, as well as related conditions like diabetes, obesity, and cardiovascular disease (CVD), and environmental factors including diet and the gut microbiota. In this work, Dr. Westerbeke and colleagues focused on the latter two factors, using RNA sequencing to identify fructose-associated gene expression changes related to MASLD. Fasting fructose levels were found to be higher in patients with MASLD, independent of fasting glucose levels, with a strong dietary component suggested for this effect. These levels have also been linked to mitochondrial dysfunction in patients with obesity. Fructose-associated toxicity related to the gut microbiome may also play a key role in MASLD pathogenesis.
- In the study, RNA sequencing was performed on liver, jejunum, and visceral adipose tissue (VAT) biopsies obtained during surgery that occurred during the BARIA study (n=304), a prospective bariatric surgery cohort. Plasma fructose levels were also measured in 39 subjects when fasting and two hours post-meal in a preoperative mixed meal test (MMT), as well as intraoperatively in peripheral and portal vein blood in 38 subjects. Differential gene expression analysis was performed for each tissue using DESeq2 to identify significant differences in the genes expressed in the tissues and gene expression changes associated with MASLD. The mean age was 48 years, 77% of participants were female, 24% had T2D, and 62% were found to have MASLD.
- Fructose metabolism by the liver leads to lipogenesis, alongside fermentation by the gut microbiota, which may play a key role in MASLD. Classically, the metabolism of fructose is known to create fatty acids in the body, known as lipogenesis. However, in the liver, this metabolic process is considered unregulated, as it bypasses the rate-limiting steps seen in glycolysis. With rapid hepatic fructose metabolism, the ChREBP/SREBP-1c genes are activated, leading to an upregulation of lipogenic enzymes. In the gut, excessive fructose can lead to its fermentation by the gut microbiota, leading to the production of ethanol and acetate, two toxic metabolites, and lipogenesis causing MASLD. The gut dysbiosis caused by these metabolites can have harmful systemic effects.
- MASLD is associated with higher fasting fructose levels, independent of glucose levels. This distinction was then used in the differential gene expression analysis to determine that 3,969 genes were differentially expressed in the liver in patients with MASLD, with the majority being downregulated.
- Using “functional enrichment” analysis[4],” the authors determined that increased fasting fructose levels are linked to mitochondrial dysfunction in patients with obesity. Downregulation of genes involved in all complexes of the electron transport chain in the process of oxidative phosphorylation was demonstrated, highlighting impaired energy metabolism in these individuals. Mechanistically, the key PPARGC1A gene, a master regulator of mitochondrial biogenesis, was identified as a link between increased fasting fructose levels and MASLD.
- Fasting peripheral fructose concentrations correlate with postprandial ethanol production, a sign of gut dysbiosis that can lead to lipogenesis and MASLD. In particular, these levels were associated with Streptococcus parasanguinis, which has previously associated with gut dysbiosis. This can result in impaired digestion and metabolism, and a decreased quality of life overall. In all, fasting fructose levels based on diet increase mitochondrial dysfunction and gut dysbiosis, which may represent a yet-underexplored pathway in the development of MASLD.
22. Exhibit Hall opens with high energy, featuring aromatic coffee stations, free lipid tests, and photobooths
EASD’s highly anticipated Exhibit Hall opened for Tuesday morning, with nearly 70 companies showcasing neon-lighted booths, aromatic coffee stations, free health checks for LDL-cholesterol, healthy fruit giveaways, and even a heart-shaped photobooth, indicating the cardiovascular benefits of a drug. Walkways were absolutely packed, similar to at ADCES, most recently, as attendees engaged with company and organization representatives and eye-catching displays to learn more about technologies and therapies for diabetes and obesity. Towards the center, attendees were also able to take pictures at the EASD’s official photobooth with the Wurstelprater (known as “Prater”), a large “recreational park” (that has had many lives) as the background – a few members of our team have joined in the fun here and taken their photos as well. In all, the 2025 EASD Exhibit Hall’s opening day highlighted the excitement and diverse themes that we witnessed throughout the day, from greater awareness for T1D screening to drugs’ benefits for diabetes comorbidities. If you’re here in Vienna, be sure to stop by! The Exhibit Hall will remain open until Thursday afternoon at 4:30pm.

23. TANGO-DM RCT finds that updated WHO 2013 diagnostic criteria for GDM demonstrates no improvement to risk of large-for-gestational-age infants compared to 1999 criteria
Prof. Rebecca Painter (Rotterdam, the Netherlands) presented results from the TANGO-DM trial, a multicenter RCT evaluating whether treating GDM (gestational diabetes mellitus) in women who meet the WHO 2013 diagnostic criteria versus the older WHO 1999 criteria improves pregnancy outcomes. The 2013 criteria recommend a lower fasting and a higher post-load threshold for GDM diagnosis (fasting plasma glucose (FPG) ≥92 mg/dL, 1-hour post-OGTT ≥180 mg/dL, or 2-hour post-OGTT ≥153 mg/dL) in comparison to the 1999 criteria (FPG of ≥126 mg/dL or a 2-hour plasma glucose (2-h PG) of ≥141 mg/dL), but the differences in outcomes based on these diagnostic criteria have not yet been analyzed.
- Study design and baseline characteristics. The trial randomized pregnant women across 21 hospitals (n=1,032; mean age 33 years) in the Netherlands between 2018 and 2024. Eligible participants had (i) a singleton pregnancy; (ii) were between 16 and 32 weeks of gestation; and (iii) had a 75-gram OGTT result discordant between the WHO 2013 and 1999 criteria. Women were assigned to either GDM treatment or routine prenatal care. Average fasting glucose was 4.2 mmol/L (76 mg/dL), with mean 1-hour and 2-hour OGTT results of 8.6 mmol/L (155 mg/dL) and 7.1 mmol/L (128 mg/dL), respectively.
- Results. Findings showed no significant difference in infants born large-for-gestational-age (LGA), which can be an adverse outcome in some cases. Among women in the GDM treatment group, 18% had an LGA infant versus 17% in the routine care arm, virtually no difference. That said, however, the treatment group was associated with greater healthcare use and increased use of pharmacotherapy. Neonates in the treatment arm were also more frequently tested for and diagnosed with hypoglycemia and more frequently admitted to the hospital as well. Importantly, there were no differences observed in very high birth weight (>4 kg/9 lbs), shoulder dystocia, or birth injury, all of which are substantial maternal and perinatal risks in women with GDM.
- Conclusion and implications. Treating GDM in women diagnosed only by the WHO 2013 criteria did not reduce risk of LGA infants compared to routine prenatal care. By contrast, treatment did increase pharmacotherapy use and neonatal interventions. Prof. Painter emphasized that adoption of the WHO 2013 criteria should be carefully reevaluated, and that these findings call into question whether expanding diagnostic criteria significantly improves outcomes for certain conditions. We await this eagerly!
24. Cause or consequence? Dr. Carmella Evans-Molina reviews whole pancreas changes in people with T1D
In a standing-room-only session, Dr. Carmella Evans-Molina (Indiana University) addressed the puzzle of T1D: is the problem limited to the ß-cell, or is the whole pancreas involved? Immune-mediated ß-cell loss is the central and “indisputable” driver of T1D pathogenesis, but accumulating evidence suggests that other pancreatic components – α-cells, δ-cells, and the exocrine pancreas – undergo widespread structural and functional changes in people with T1D. Dr. Evans-Molina acknowledged that we still do not know whether such findings are the cause of disease, contributors to progression, or a consequence of ß-cell loss.
- ß-cell dysfunction begins years before diagnosis. Subtle reductions in insulin secretion can occur up to six years before clinical diagnosis, often around the time of seroconversion. A period of relative stability follows, but in the two to three years preceding the progression to stage 3 T1D, C-peptide levels fall while glycemia rises, culminating in insulin dependence. Concurrently, disturbances in glucagon and somatostatin secretion contribute to metabolic instability and impaired counter-regulation.
- α-cell volume is preserved in T1D, but function and organization are impaired. Despite evidence that total α-cell volume remains intact, α-cells show striking changes in spatial organization, with many islets shifting toward insulin-negative/glucagon-positive profiles. At the same time, distinct molecular programs separate α-cells from ß-cells and favor their survival, meaning the mechanisms that destroy ß-cells do not necessarily affect α-cells. Yet, preserved mass does not equate to preserved function: α-cells lose the ability to suppress glucagon in hyperglycemia and show blunted, variable counter-regulatory responses. These defects drive hyperglucagonemia and worsening hyperglycemia, whose severity may be inversely related to residual ß-cell function.
- δ-cell mass and organization are altered in T1D, with possible functional consequences. δ-cells, the source of somatostatin, define the glycemic setpoint and exert strong control over insulin secretory patterns. Preclinical ablation models show that removal of the δ-cells lowers the glycemic setpoint and alters insulin secretion. In humans, islet studies reveal wide inter-donor variability, with δ-cells ranging from ~3% to ~20% of islet composition, and higher proportions linked to reduced insulin secretion. In T1D, it’s possible that δ-cell mass may modestly increase early in the disease progression, accompanied by dramatic increase of somatostatin in small endocrine objects. These observations suggest that δ-cell dysfunction actively contribute to hyperglycemia and metabolic instability, rather than merely being a byproduct of ß-cell loss.
- Exocrine pancreas mass and function are consistently reduced in T1D. Imaging and autopsy studies demonstrate reduced pancreatic volume, sometimes even before clinical diagnosis or in first degree relatives, and circulating enzyme levels (trypsinogen, lipase, amylase) are frequently decreased, signaling impaired exocrine function. Its cause, however, remains unsolved. Possible explanations include: (i) developmental defects; (ii) loss of insulin’s trophic effect on acinar cells; (iii) dysfunction by proximity to islet inflammation; or (iv) direct immune targeting of exocrine antigens. Evidence for exocrine autoimmunity also exists in some series. Dr. Evans-Molina concluded by asking if exocrine insufficiency should be recognized and treated in T1D, and if exocrine immunity could represent a novel therapeutic target?
25. Fr1da study shows insights into single islet antibody prevalence and progression in children
In an oral session, Prof. Sarah Schill (Technical University Munich, Germany) presented findings from the Fr1da study, which was extended in October 2019 to include the detection and follow-up of single islet autoantibody positivity. Given the importance of early intervention and treatment, the field has focused on improving public awareness and screening initiatives to diagnose T1D, defined as the presence of two or more confirmed positive islet autoantibodies. The current study assessed the prevalence, persistence, and outcomes of single islet autoantibody positivity and progression to early-stage or diagnosis of T1D.
- Methods. The study screened for autoantibodies using ELISA and LIPS assays, followed by confirmatory testing with radio-binding assays. The detection of a single autoantibody was determined using three to six times higher cut-off values than those used for multiple autoantibody positivity. The study recommended at least three years of annual follow-up for children who tested positive for a single islet autoantibody; three to four years of rescreening was recommended for children who tested negative.
- Results. Between October 2019 and March 2025, the study enrolled 104,276 children. Nearly the entire study population had sufficient blood samples for screening. 0.25% (~260) of children were diagnosed with early-stage T1D, and 22% of this population (~60) progressed to clinical diabetes. During a follow-up period, 9% of children no longer showed positive detection of autoantibody positivity, 12% developed early-stage T1D, and 79% remained positive for single autoantibody detection. After a median of two years, four children within the population who maintained single autoantibody positivity developed clinical diabetes. When 11,181 children who tested negative for autoantibodies in the first screening round were retested at a later age, 0.1% were positive for one autoantibody and 0.21% were diagnosed with early-stage T1D.
- Discussion. Reflecting on these results, Prof. Schill highlighted the importance of screening and follow-up among children with single islet autoantibodies to help detect clinical T1D diagnosis. Furthermore, Prof. Schill encouraged rescreening efforts to routinely follow children with single and multiple autoantibodies in the first screening. While the instructions are well understood, we imagine from the perspective of parents and guardians this might sound much easier than in practice – but certainly for the healthcare system, even saving a small number of DKAs is good.
26. *NEW* Higher A1c thresholds required to predict T1D progression in adults compared to children with positive islet autoantibody
In an oral session, Prof. Erin Templeman (University of Exeter, UK) shared findings on the comparison of A1c thresholds for predicting T1D progression between children and adults. Prof. Templeman explained that A1c increases with age due to both glycemic and non-glycemic related factors. Some of these factors may influence the predictive value of A1c thresholds for T1D progression, affecting strategies for monitoring and diabetes management among children and adults. Therefore, a study aimed to determine the effects of age on A1c thresholds for predicting the progression of T1D diagnosis among individuals with positive autoantibodies.
- Methods. The study included relatives who screened for autoantibodies in the TrialNet Pathway to Prevention study. Individuals who tested positive for autoantibodies received an oral glucose tolerance test (OGTT) and an A1c measurement among children and adults. Then, a model estimated the risk of T1D within age groups to assess differences between the cohorts.
- Results. There were 5,024 participants (26% adults) who tested positive for islet-autoantibodies. Among this population, 32% developed T1D, of whom 13% were adults. More adults had dysglycaemic HbA1c (³39 mmol/mol or ³5.7%) at screening compared to children (8.4% vs. 5.3%, p<0.001). The study showed an increased risk of developing clinical T1D with increasing A1c levels for both age groups. However, a higher level of A1c (HbA1c³42 mmol/mol or a modelled age-adjusted HbA1c³39 mmol/mol) was needed to identify adults at equivalent progression risk to children. For example, Prof. Templeman explained that children with A1c of 39 mmol/mol or 5.7%, which is the A1c threshold for stage 2 T1D, had a higher risk of developing T1D within 12 months compared to adults (39% vs. 15%, p<0.001).
- Discussion. While A1c remains a useful predictor for T1D progression, Prof. Templeman emphasized that the impact of age on A1c affects interpretations of risks. Therefore, she encouraged adjusting thresholds to optimize the use of A1c levels when building monitoring and management of autoantibody screening.
27. *NEW* “The era of diagnosis”: Survival rates for T1D increased over decades
In an engaging afternoon address, Dr. Astrid Lavens (Sciensano, Belgium) explored the “impact of the era of diagnosis” on T1D mortality trends. Ultimately, it was great to see in this presentation data on survival rates for those with T1D increasing. Although mortality rates for people living with T1D have markedly declined over the past two decades, age-standardized mortality rates for people with T1D remain two-to-five times that of people without diabetes, and up to 8.5 times higher for children and adolescents with T1D. This cross-sectional, real-world observational study sought to analyze mortality rates between 15- and 25-years post diagnosis among people living with T1D in Belgium diagnosed between (i) 1985-1998 (group A; n=345) and (ii) 1998-2009 (group B; n=948). Using a nationwide registry, researchers collected data on adults diagnosed with T1D before age 30 in Belgium between 2001-2022. A baseline profile on clinical, demographic, treatment, and complication data was collected 15 years after diagnosis for each participant. At 25 years post-diagnosis, investigators collected data on vital status and year of death. At baseline, group B (participants diagnosed between 1998-2009) had higher rates of obesity and were more likely to be on lipid-lowering therapy, compared to group A (those diagnosed between 1985-1998) (p<0.05; p<0.05). Group B were less likely to be on antihypertensive therapies (p<0.01). Group A had an average A1c of 8.3 compared to group B, whose mean A1c was 8.1 (p<0.05) – notably, despite the “close” numbers, this was a statistically significant difference. We assume CGM metrics are not available and that CGM was not used, though we are eager to find this out from the authors. While there was no difference in the rates of complications like diabetic retinopathy and albuminuria, differences in heart health did exist.
- Survival rates 25 years after diagnosis were far better for those diagnosed in the “later era” (1998-2009), which we assume stemmed from better heart health in second group, and despite no differences in the groups in terms of eye and kidney disease. Specifically, group A conferred a significantly higher incidence of mortality 25 years post-diagnosis compared to group B (see below; p<0.0079, a very significant p value). Standardized mortality rates (SMR), calculated by dividing observed deaths by expected deaths, also significantly differed between the two groups, with group A conferring an SMR of 4.14, while group B demonstrated an SMR of 2.28 at 25 years post-diagnosis. Interestingly, a slightly higher A1c (HR 1.08; p=0.0087) and age (HR 1.49; p=0.0019) 15 years post-diagnosis were associated with an increased risk for all-cause mortality 25 years post-diagnosis.
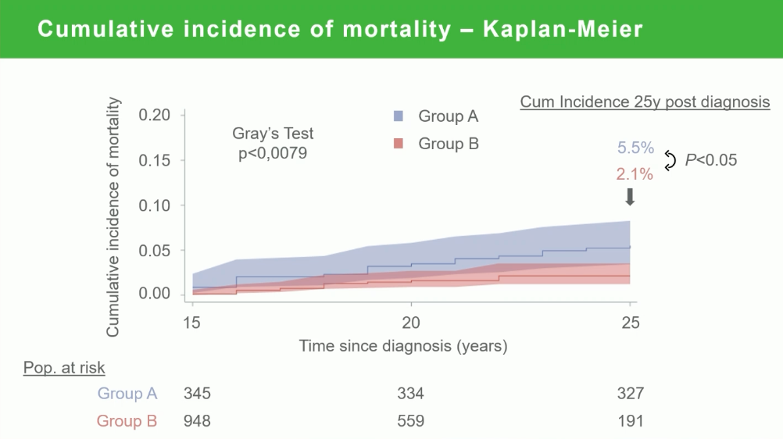
--by Riya Chatterjee, Kayla Mathieu, Elizabeth Rose, Jeremy Alkire, Nour Khachemoune, Katherine Moon, Monica Oxenreiter, and Kelly Close
[1] As a reminder, T1D is a progressive disease with several stages: stage 1 T1D refers to people with two or more islet autoantibodies and normal glucose level; stage 2 T1D for those with at least two autoantibodies and dysglycemia; and stage 3 for those with clinical diagnosis of T1D.
[2]We have always heard the range for TITR for pregnancy begins at 70 mg/dL and were curious to know why this was the TITR range used.
[3]PNPLA3 and TM6F2 are both involved in fat metabolism and are primarily found in liver and fat cells.
[4]As we understand it, this term is sometimes used to refer to “approaches that derive biological / functional meaning from lists of genes” – see “Pathways and gene sets: What is functional enrichment analysis?”