ATTD-Asia 2025 Day #3 Highlights –
Executive Highlights
- The second annual ATTD-Asia conference concluded today in Singapore. A strong final day included discussions of functional T1D cures, further real-world AID data, and key evidence for expanding access to diabetes technology in order to improve health metrics.
- In a well-attended morning session, Breakthrough T1D’s Prof. Thomas Danne (CMO) shared his vision of “functional cures” for T1D, how to measure success, and what it will take to reach diabetes remission. Just a few years ago, automated insulin delivery was considered a revolution in diabetes care. Today, the landscape has become significantly more complex. Prof. Danne provocatively said, “I consider developing [Time in Range (TIR; 70-180 mg/dL)] as one of my big mistakes.” While TIR is a better measurement than A1c by capturing patients’ daily glycemic fluctuations and hypo- and hyperglycemia burden, the threshold of TIR ≥70%, which is equivalent to A1c <7%, is still associated with threefold increase in cardiovascular mortality and ~2.4-fold increase in all-cause mortality.
- Prof. Danne proposed a new classification system to assess diabetes interventions:
- Class 1 (remission) of “functional cure” refers to TITR >90%, Time below Range (TBR; <54 mg/dL) <1%, and positive patient-reported outcomes;
- Class 2 (prediabetes) refers to TITR >70% and TBR <1%; and
- Class 3 refers to TITR between 55-70%.
- Prof. Danne proposed a new classification system to assess diabetes interventions:
- Then, full 26-week RADIANT trial results were presented, showing sustained glycemic improvements with Omnipod 5 and FreeStyle Libre 2. The RADIANT trial initially enrolled children and adults (n=188) across 19 sites in Belgium, France, and the UK. All participants had at least one year of T1D and had been using MDI with CGM for at least three months. After two weeks of baseline data collection, participants were randomized 2:1 to either Omnipod 5 (n=125) or MDI with CGM (n=63) for 13 weeks. The extension phase demonstrated positive glycemic outcomes both for those continuing on Omnipod 5 and those newly switching from MDI. A1c remained stable at 7.2% for those continuously on Omnipod 5 from Weeks 13 to 26. Participants who switched from MDI to Omnipod 5 at 13 weeks saw their A1c decrease by 0.7% (from 8.0% to 7.3%) by 26 weeks (p<0.0001). Similar outcomes were observed regarding TIR.
- In a strong closing session, co-chair of the conference Prof. Moshe Phillip (Schneider Children's Medical Center, Israel) reflected on the strong focus on AI and machine learning (ML) at this year’s conference. He said that he expects ATTD-Asia 2026 to open with a discussion of AI and ML and encouraged all 750 participants from 54 countries to join in Kyoto, Japan next December.
The second annual ATTD-Asia conference took place in Singapore from December 9-11. See our Resource Hub and Day-by-Day Preview for the most up-to-date source of conference reporting.
Table of Contents
-
Top Highlights
- 1. *NEW* Toward a functional cure for T1D: Prof. Thomas Danne on TITR, T1D “remission”, and cell replacement therapies
- 2. *NEW* Full 26-week RADIANT trial results show sustained glycemic improvements with Omnipod 5 and FreeStyle Libre 2
- 3. *NEW* Real-world analysis identifies five optimal Omnipod 5 settings associated with improved glycemic outcomes
- 4. *NEW* MiniMed 780G delivers additional long-term health and economic benefits in Hong Kong and Australian adults with T1D
- 5. *NEW* Understanding bolus patterns as a key determinant of Omnipod 5 outcomes
- 6. Prof. Benjamin Wheeler on AID for those that need it the most
- 7. Prof. Catarina Limbert on ISPAD’s Declaration of Lisbon 2024: An imperative for action for childhood diabetes
- 8. Updates on T1D screening and monitoring: Screening in Japan and early-stage clinical service in Australia
- 9. Early insights into ketone patterns in T1D using continuous monitoring
- 10. Increasing rates of GDM are associated with higher maternal age and obesity
- 11. *NEW* Dr. Tom Wilkinson presents feasibility results of the second-generation Tandem Freedom FCL algorithm (n=10) in a three-day hotel setting
Top Highlights
1. *NEW* Toward a functional cure for T1D: Prof. Thomas Danne on TITR, T1D “remission”, and cell replacement therapies
In this well-attended morning session, Breakthrough T1D’s Prof. Thomas Danne (CMO) shared his vision of “functional cures” for T1D, how to measure success, and what it will take to reach diabetes remission. Just a few years ago, automated insulin delivery was considered a revolution in diabetes care. Today, the landscape has become significantly more complex, with rapid advancements across: (i) multi-hormonal, multi-sensor devices (e.g., ketone, cortisol, lactate, adrenaline); (ii) adjunctive therapies (e.g., SGLT-2 inhibitors, GLP-1 RAs, pramlintide); (iii) next-generation insulins (e.g., ultra-rapid, glucose-responsive, liver-targeted insulins); (iv) disease-modifying therapies; (v) cell therapies; (vi) and gene therapies. Furthermore, over the years, the field has learned that diabetes technology – including AID systems previously described as the “artificial pancreas” – is not a cure, as hypoglycemia, diabetic ketoacidosis (DKA), and device issues persist. Thus, Prof. Danne argued to move beyond technology-centric diabetes management and instead leverage various innovations to achieve optimal glucometabolic management with minimal burden on people with T1D.
- On measuring success, Prof. Danne provocatively said, “I consider developing [Time in Range (TIR; 70-180 mg/dL)] as one of my big mistakes.” While TIR is a better measurement than A1c by capturing patients’ daily glycemic fluctuations and hypo- and hyperglycemia burden, the threshold of TIR ≥70%, which is equivalent to A1c <7.0%, is still associated with threefold increase in cardiovascular mortality and ~2.4-fold increase in all-cause mortality. Given the residual long-term risks with TIR ≥70%, he advocated for a more demanding goal: Time in Tight Range (TITR; 70-140 mg/dL). Considering that people without diabetes spend 96% of their time in this range, Prof. Danne proposed a new classification system to assess diabetes interventions:
- Class 1 (remission) of “functional cure” refers to TITR >90%, Time below Range (TBR; <54 mg/dL) <1%, and positive patient-reported outcomes;
- Class 2 (prediabetes) refers to TITR >70% and TBR <1%; and
- Class 3 refers to TITR between 55-70%.
- With the new classification system, it is possible to assess current options on the market. For example, the bihormonal AID system achieves 80% TIR yet ~57% TITR (up from 56% and 34% at baseline, respectively), reinforcing once again that technology cannot be a cure for T1D. Vertex’s stem cell-derived islet transplantation VX-880 (zimislecel) with immunosuppression achieves 93% TIR but ~63% TITR (up from 50% and 27% at baseline, respectively). This suggests that stem cell-derived islets may still face challenges with residual insulin resistance and incomplete graft function and may continue to require AID or adjunctive therapy in many patients. Most impressively, an autologous transplantation of chemically induced pluripotent stem cell-derived islets (CiPSC-derived islets; published in Cell last year) achieved both TIR and TITR >90%, making it closer to a Class 1 functional cure for T1D.
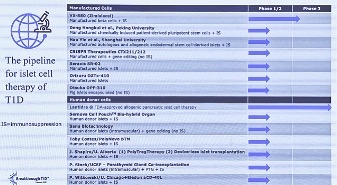
- Cell replacement therapies, like Vertex’s zimislecel and Sana Biotechnology’s hypoimmune islets, continue to advance in clinical development (see figure below). Such efforts are not without challenges, however. Most notably, immunosuppression can increase the risk of infections and certain cancers. Some immunosuppressive drugs can also impact lipids and blood pressure, potentially worsening cardiovascular health. Long-term duration of islets is also a big challenge, as only 8% of islet-transplanted patients remaining insulin-free, and 70% of deceased donor islets maintaining function after 20 years of follow up. Prof. Danne is hopeful that innovations in less toxic immunosuppression regimen, like Eledon’s anti-CD40L antibody tegoprubart, routine cancer screening, and antimicrobial and antiviral prophylaxis could mitigate such risks.
2. *NEW* Full 26-week RADIANT trial results show sustained glycemic improvements with Omnipod 5 and FreeStyle Libre 2
Prof. Pratik Choudhary (University of Leicester, UK) presented the extension phase results of the RADIANT study (n=187), comparing Omnipod 5 to MDI with FreeStyle Libre 2 CGM in people with T1D. Preliminary 13-week results were presented at ATTD 2025 by Dr. Emma Wilmot (University of Nottingham, UK). The RADIANT trial initially enrolled children and adults (n=188) across 19 sites in Belgium, France, and the UK. All participants had at least one year of T1D and had been using MDI with CGM for at least three months. After two weeks of baseline data collection, participants were randomized 2:1 to either Omnipod 5 (n=125) or MDI with CGM (n=63) for 13 weeks. In the extension phase, participants originally assigned to Omnipod 5 continued on the device, while those initially randomized to MDI switched to Omnipod 5 for an additional 13 weeks of study. Only one participant initially randomized to Omnipod 5 did not complete the extension phase.
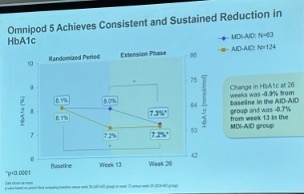
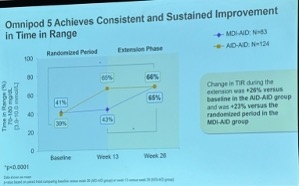
- For reference, 13-week preliminary results showed that Omnipod 5 led to a 0.8 percentage point greater reduction in A1c compared to MDI with CGM (from 8.1% to 7.2%; p<0.0001). Omnipod 5 also significantly improved Time in Range (TIR), with an average increase of 5.4 hours/day (+22%) compared to MDI with CGM (p<0.0001). Specifically, Omnipod 5 users experienced a 26% increase in TIR (from 39% at baseline to 65% at 13 weeks), while MDI with CGM users had a marginal 2% increase (from 41% to 43%).
- The extension phase demonstrated positive glycemic outcomes both for those continuing on Omnipod 5 and those newly switching from MDI. A1c remained stable at 7.2% for those continuously on Omnipod 5 from Weeks 13 to 26. Participants who switched from MDI to Omnipod 5 at 13 weeks saw their A1c decrease by 0.7% (from 8.0% to 7.3%) by 26 weeks (p<0.0001). Similar outcomes were observed regarding TIR (see figures below). By 26 weeks, those continuously on Omnipod 5 essentially maintained the TIR improvements seen by 13 weeks (culminating in a 27% increase from 39% to 66%), while those who switched to Omnipod 5 at 13 weeks saw a 23% increase (from 41% to 65%; p<0.0001). Prof. Choudhary highlighted the significance of these improvements, noting that the control group, which received a “higher-than-usual standard of care” during the course of the study with efforts to optimize MDI, still struggled to achieve target glycemic management. It was only after the introduction of AID that marked improvements were observed.
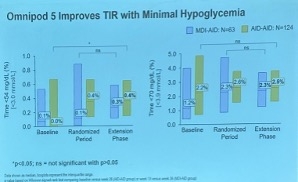
- There were no significant differences in Time below Range (TBR) or Time <54 mg/dL between the groups, with both meeting the non-inferiority endpoint. At 26 weeks, TBR was 2.5% for continuous Omnipod 5 users and 2.3% for those who switched at 13 weeks. A significant increase from baseline in Time <54 mg/dL was observed in continuous Omnipod 5 users by 26 weeks (from 0% to 0.4%; p<0.05). In those who switched at 13 weeks, Time <54 mg/dL was 0.3%, an increase that did not reach significance.
- One severe hypoglycemia event and one DKA event were reported during the trial, in the continuous Omnipod 5 group and MDI-switch group, respectively. This resulted in an event rate of 3.3 severe hypoglycemia events per 100 person-years for continuous Omnipod 5 users and 6.6 DKA events per 100 person-years for those who switched at 13 weeks.
3. *NEW* Real-world analysis identifies five optimal Omnipod 5 settings associated with improved glycemic outcomes
Dr. Lauren Huyett (Insulet) shared a three-month real-world analysis from over 176,000 Omnipod 5 users in the US and Europe, identifying five modifiable predictors of achieving >70% TIR. She emphasized that outcomes depend on both algorithm settings and user behavior adjustments, and that relying on conventional pump guidelines may limit system performance.
- A cloud-based dataset allowed a thorough analysis of predictors of successful glycemic management. The team analyzed three months of automatically uploaded Omnipod 5 data from January-March 2025 across the US and Europe (n=176,739). Baseline median TIR for the full cohort was 65%. The analysis compared users achieving ≥70% TIR (n=61,964) with those below target (n=114,775) and incorporated regression modeling to identify modifiable predictors of success. The team then derived data-driven cutoffs for each predictor to maximize the likelihood of achieving target TIR and create a practical framework for settings optimization.
- The analysis identified five cutoff values strongly associated with achieving TIR over 70%. These included:
- Boluses per day: ≥3-5;
- Percent time in automated mode: ≥90%;
- Target glucose: 110 mg/dL;
- Insulin-to-carbohydrate (I:C) ratio times total daily dose (TDD): ≤350; and
- Correction factor times TDD: ≤1500 mg/dL.
- When the three adjustable settings (target glucose, I:C ratio, correction factor) were optimized alone, median TIR rose to 72% with no increase in hypoglycemia. When combined with the two behavioral predictors (bolus frequency and time in automated mode), median TIR approached 80%, illustrating the synergistic effect of user engagement and settings. Dr. Huyett noted that these findings show the broader concept that all hybrid closed-loop systems still depend on consistent meal bolusing to achieve optimal outcomes.
- These findings reinforce that Omnipod 5 relies more on target glucose, I:C ratio, and correction factor than on basal rates. Unlike conventional pump therapy, where basal rates are foundational, Dr. Huyett said changing basal rates on Omnipod 5 does not affect automated insulin dosing once a user is in automated mode. Instead, the algorithm responds most strongly to: (i) target glucose, which guides both automated insulin delivery and correction boluses; (ii) the I:C ratio, which determines the size of user-initiated boluses; and (iii) the correction factor, which shapes corrective insulin responsiveness.
- For clinicians, these findings offer actionable guidelines for settings optimization and patient education. The five modifiable predictors provide a practical starting point for adjusting Omnipod 5 in routine care. Dr. Huyett closed by emphasizing that even slight adjustments, especially when combined with behavioral adjustments, can meaningfully shift TIR outcomes.
4. *NEW* MiniMed 780G delivers additional long-term health and economic benefits in Hong Kong and Australian adults with T1D
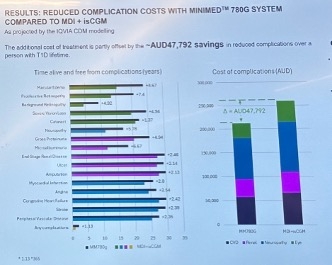
Prof. Elaine Chow (The Chinese University of Hong Kong, China) and Prof. Sarah Glastras (University of Sydney, Australia) both presented cost-effectiveness analyses demonstrating that the MiniMed 780G system is a cost-effective treatment strategy for adults with suboptimal controlled T1D in Hong Kong and Australia, respectively. These findings are driven by meaningful improvements in glycemia and reductions in acute and chronic complications. Using local cost inputs and a local payer perspectives, their analyses suggest that MiniMed 780G can meaningfully extend life expectancy and quality-adjusted survival, while partially offsetting device costs in multiple additional geographies (including Japan, with cost-effectiveness results there presented yesterday).
- The cohort model compared MiniMed 780G with MDI and isCGM in adults with high baseline A1c levels (≥8.0%). The analyses used the IQVIA Core Diabetes Model over a 60-year horizon, applying Hong Kong- and Australia-specific costs, compilation rates, and quality-of-life inputs. A 60-year horizon was used in the Hong Kong model, and a 50-year horizon was used for the Australian cohort. Adults in the modeled cohorts resembled those enrolled in the multicenter RCT it was based on (mean age of 33 years; diabetes duration of seven years; and baseline A1c of ~9%). For reference, the intervention arm achieved a 1.5% A1c reduction, compared to a 0.2% reduction with MDI and isCGM. Only direct medical costs were included, and cost-effectiveness was judged against Hong Kong and Australia’s willingness-to-pay thresholds. Prof. Chow explained that Hong Kong’s threshold is 1x gross domestic product (GDP) per capita, which is an incremental cost-effectiveness ratio (ICER) less than ~441,500 HKD (~$56,700) per quality-adjusted life year (QALY). For the Australian analysis, Prof. Glastras said that the country generally considers interventions under AUD $50,000 (~$33,200) to be cost-effective.
- In Hong Kong, MiniMed 780G users gained more life-years, QALYs, and had fewer complications than the standard care group. Across the modeled lifetime and compared to the MDI and isCGM group, AHCL use generated 1.4 additional life years, 2.4 additional QALYs, substantially fewer acute and chronic complications, and approximately three more years free of complications. Total incremental direct cost was 923,046 HKD (~$118 640), but 306,179 HKD (~$50,460) of this was offset by reduced complication costs. The resulting ICER of 392,602 HKD (~$50,460) per QALY gained falls below Hong Kong’s cost-effectiveness threshold, placing MiniMed 780G within accepted willingness-to-pay standards. Sensitivity analyses showed the results were consistent across variation in time horizon, treatment cost, and glycemic effect size, reinforcing confidence in the simulation’s conclusions.
- MiniMed 780G also reduced the incidence of diabetes-related complications in Australia, with a savings of AUD 47,792 (~$31,700), partially offsetting higher acquisition costs. Similar to Dr. Noriko Kodani yesterday, Prof. Glastras highlighted several specific extensions of normal function with MiniMed 780G, including years added to life free from retinopathy, nephropathy, and CVD complications (see figure below). Compared to MDI with CGM, direct costs were AUD 45,929 (~$30,500) higher with MiniMed 780G, with a total cost of treatment of AUD 93,721 (~$62,200). MiniMed 780G users were modeled to have 0.5 additional life years and 1.4 QALYs gained compared to MDI with CGM, resulting in an ICER of AUD 32,734 (~$21,700), below what is generally considered cost-effective in Australia. Sensitivity analysis also confirmed the robustness of the results.
- In their sessions, Dr. Chow and Dr. Glastras concluded that MiniMed 780G is a cost-effective strategy for improving long-term health in adults with poorly controlled T1D in Hong Kong and Australia. They emphasized that reductions in both acute and chronic complications drive much of the benefit, and that early adoption could meaningfully alter risk trajectories for this population. Looking ahead, expanded reimbursement for AID systems in Hong Kong and Australia may depend on continued evidence demonstrating both clinical and economic advantages.
5. *NEW* Understanding bolus patterns as a key determinant of Omnipod 5 outcomes
Dr. Lalantha Leelarathna (Imperial College London, UK) presented a single center real-world study of 103 adults initiating Omnipod 5, revealing significant improvements to TIR and highlighting that higher proportions of meal and correction boluses were strongly associated with better glycemic outcomes. The analysis also reinforced that Omnipod 5 performs consistently across socioeconomic stratifications and may offer particular benefit to individuals transitioning from MDI.
- Study design and primary outcomes. Participants were 39 years old on average with a mean diabetes duration of 18 years and baseline A1c values of 7.6%. About half initiated Omnipod use from MDI and half from insulin pump therapy, with 40% using a Libre CGM and 60% using a Dexcom CGM prior to Omnipod 5 start. System usage was high, with sensor availability reaching 95% and automated mode use at 97%, with a median of 5.1 daily boluses and 133 grams of reported carbohydrate intake. Across the four-week pre- and post-comparison, TIR improved by 15 percentage points (from 52% to 67%), accompanied by reductions in hypo- and hyperglycemia, glucose management indicator (GMI), and coefficient of variation (CV), all aligned with previously published Omnipod 5 data.
- User-driven insulin delivery was the strongest predictor of post-Omnipod 5 glycemic success, with higher bolus percentages consistently associated with higher TIR. Participants in the lowest quartile of bolus proportion (≤39 of total insulin; n=32) achieved a post-Omnipod 5 TIR of 56%, whereas those in the highest quartile (≥51% of total insulin; n=23) reached 77%. Dr. Leelarathna noted that the 21-percentage point difference occurred despite similar access to the algorithm. Time below Range (TBR) decreased across all bolus quartiles, and those delivering more bolus insulin experienced both higher TIR and larger reductions in hypoglycemia. Correlation analysis also confirmed a strong association between bolus percentage and TIR, suggesting that user-initiated insulin delivery remains a critical component of Omnipod 5 success.
- Several user characteristics, including BMI and carbohydrate entry, also predicted better outcomes, whereas socioeconomic deprivation saw no association. Higher BMI and higher carbohydrate entry frequency were both positively correlated with post-Omnipod 5 TIR, indicating that users that give the system more input had greater benefit. Importantly, the socioeconomic deprivation index showed no relationship with outcomes, underscoring that Omnipod 5 performs well across demographic and socioeconomic backgrounds. Additionally, users transitioning from MDI experienced larger TIR gains than pump users (+17% versus +12%), suggesting an advantage when moving directly from non-automated therapy.
- Dr. Leelarathna concluded that encouraging proactive bolusing by aiming for ≥45-50% of total insulin through meal and correction boluses, may meaningfully enhance Omnipod 5 outcomes. He emphasized that while the algorithm delivers strong baseline improvements, the highest glycemic improvements occur when users engage consistently with the system. Looking ahead, these findings support clinic workflows that prioritize bolusing education and real-time data review to help users maximize Omnipod 5 benefits.
6. Prof. Benjamin Wheeler on AID for those that need it the most
Prof. Benjamin Wheeler (University of Otago, New Zealand) discussed multiple key takeaways from the use of AID in New Zealand’s health system, which he characterized as unique.
- The CO-PILOT trial demonstrated the significant benefits of AID for youth with high A1c values, many of whom were experiencing economic deprivation. The multicenter, open label randomized controlled trial included 80 patients with T1D aged 7-25 years. The minimum A1c value for inclusion was 8.5%, with a mean A1c of 10.5% among participants. 40% of the patients were Māori or Pacific Islander, and 75% experienced economic deprivation. At 13 weeks, the mean A1c value decreased to 8.1% in the AID group (a 2.5% reduction) but remained steady at 10.6% in the control group on MDI. Patients in the AID group spent 8.4 more hours in Range (70-180 mg/dL). No instances of severe hypoglycemia or DKA occurred in the AID group compared to one and two events, respectively, in the control group. Future data to be presented also demonstrated key improvement to metrics such as TIR over a longer one-year time period. The trial reaffirms that initiating AID has significant benefits even for “non-traditional” or “non-ideal” candidates.
- Prof. Wheeler said that while AID remains the gold standard therapy for T1D, equity of access remains a major issue. New Zealand has offered public funding for insulin pumps since 2012, an essential service and unique opportunity for patients in the nation. However, a notable portion of patients lose access to insulin pumps after some time – approximately 4% nationwide year-to-year based on a 2020 study. Patients aged 10-29 and non-European patients were more likely to cease insulin pump use. In August 2024, Pharmac, a government medication funding agency, announced a decision to fully fund CGMs, the Tandem t:slim X2 and mylife YpsoPump insulin pumps, and insulin pump consumables for patients with T1D. Since this decision, Prof. Wheeler demonstrated a mean 1.4% A1c improvement among patients at a single clinic (n=1,500), with nationwide effects likely. 2,500 patients have initiated insulin pump use since the decision. This demonstrates the significant improvements to health metrics that are conferred by broader access to diabetes technology.
- “Innovation without access is irrelevant, access without equity is incomplete.” Prof. Wheeler reminded attendees that providers have a critical role in innovation but also in advocacy. His extensive research into real-world access to diabetes technology has demonstrated the health benefits of expanded access across racial and socioeconomic lines. Instead of predicting which patients will or will not do well with diabetes technology, Prof. Wheeler urged attendees to keep an open mind and keep equity at the heart of all they do.
7. Prof. Catarina Limbert on ISPAD’s Declaration of Lisbon 2024: An imperative for action for childhood diabetes
In an afternoon session, Prof. Catarina Limbert (Universidade NOVA de Lisboa, Portugal) discussed the 12 steps of the Declaration of Lisbon 2024. The declaration was issued at the 50th annual meeting of The International Society for Pediatric and Adolescent Diabetes (ISPAD) to continue to promote optimal health, social welfare, and quality of life for all children, adolescents, and adults with diabetes around the world. ISPAD recognizes the challenges of diabetes during the critical development period in youth and hopes to improve management and prevention around the world. The 12 pillars recognize key actions to be taken towards this goal.
- To advance precision diagnosis for all children in all stages of diabetes. Prof. Limbert said that precision diagnosis serves as the foundation for personalized diabetes care. Over 1.5 million children worldwide have already been screened for T1D across 15 major studies. As discussed in the 2024 ISPAD Clinical Practice Consensus Guidelines, both children’s age and the number of pancreatic autoantibodies should dictate the frequency and intensity of monitoring.
- To develop disease-modifying therapies to protect, enhance, or restore the residual beta-cell function aiming for a cure. Prof. Limbert highlighted teplizumab as the first-in-class therapy to delay the onset of T1D, which received FDA approval in November 2022 and a positive opinion from the EMA in November 2025. The median two-year delay in diabetes onset offered by the therapy is life changing for many children. Prof. Limbert said that future therapies will hopefully continue to move the field towards prevention and a cure for T1D.
- To make insulin and other evidence-based diabetes treatments more readily available. ISPAD regularly collaborates with medical and humanitarian organizations to bridge persistent gaps in diabetes care. Prof. Limbert highlighted the work of Action4Diabetes in particular, an NGO that provides insulin, medical supplies, digital education, and training for T1D in Southeast Asia. In Cambodia, Laos, Myanmar, the Philippines, Thailand, and Vietnam, diabetes supplies including insulin are not covered by government insurance, leading to Action4Diabetes’s life-changing work. Awareness of the condition also remains low among the public and even physicians, who mistakenly believe that T1D is extremely rare in the region. The organization has collaborated with the Helmsley Charitable Trust in the Philippines.
- To reduce the morbidity and mortality rate of short-term and long-term complications, including mental health diagnoses, as well as missed diagnoses related to diabetes. Prof. Limbert discussed the crisis of missed diagnoses: in low-resource settings, there is a shocking 27% mortality rate before T1D is ever diagnosed. Of 30,000 patients, this translates to 10,000 in Africa and 6,000 in Southeast Asia. As of 2025, a severe gap in life expectancy for patients with T1D persists, ranging from six to 66 years around the world. ISPAD also maintains a significant focus on mental health, with depression, anxiety, diabetes distress, and eating disorders common among people with T1D.
- To make person-centered and age-appropriate care and education accessible to all children, adolescents, and young adults with diabetes and their families. ISPAD recognizes the need for very specific care strategies for children and the need for age-appropriate education. Prof. Limbert said that multidisciplinary care teams that will work with a young patient with T1D and their entire family are essential.
- To increase the availability of appropriate diabetes technology, including continuous glucose monitoring equipment, insulin pumps, automated insulin delivery systems and other devices. Prof. Limbert and ISPAD as a whole recognize that CGM is the standard of care for children and adolescents with T1D. Increasing access to the technology around the globe is a pillar of diabetes care. Additionally, AID and future fully closed-loop systems should be made available to as many children with T1D as possible.
- To develop and encourage research on diabetes in this demographic around the world. ISPAD hopes to advance potentially curative therapies for T1D such as zimislecel (VX-880), which is now in pivotal development. For patients with impaired hypoglycemic awareness and severe hypoglycemic events, 83% of participants no longer used exogenous insulin after completing dosing in trials for zimislecel.
- To prepare and disseminate written guidelines and standards for practical and realistic diabetes care, psychosocial care, monitoring, nutrition, education, and consistent goal setting for young people with diabetes and their families — this should emphasize the crucial role of the team of health-care professionals and the community in these tasks globally. Prof. Limbert said that increased awareness of therapeutic guidelines around the world is essential for improving global T1D care. Guidelines should always be evidence-based and globally adaptable. ISPAD has 23+ guideline topics covering pediatric and adolescent diabetes care. The organization has recently updated its guidelines for T2D in youth as well, including screening starting at age ten or at puberty for youth with high BMI values and at least one other risk factor.
- To advocate for inclusive policies and a safe environment in schools, non-academic activities, and work settings. Prof. Limbert said that in her home country of Portugal, children with T1D remain barred from certain schools due to a lack of staff trained to manage T1D during the school day. Through the establishment of guidelines and consensus statements, ISPAD hopes to change this. ISPAD supports compliance with legal protections for children and adolescents with T1D to attend school, be safe at school, and to receive optimal medical management at school.
- To establish transitional care policies from pediatric to adult services for adolescents and young adults living with diabetes. ISPAD found that only 33% of healthcare centers utilized a transition readiness checklist between pediatric and adult diabetes clinics, and less than 25% had structured transition education for staff. This can lead to gaps in care and reduced patient comfort.
- To ensure and advocate for better conditions for children, adolescents, and young adults with diabetes who are facing life-threatening challenges due to man-made and natural disasters. Prof. Limbert said that disruptions to insulin supply during crises have rapid and catastrophic consequences. Children with diabetes must be prioritized by governmental and non-governmental healthcare providers during emergencies. She deemed this a crisis within a crisis, such as the insulin supply challenges seen during the Los Angeles wildfires in January 2025.
- To engage with governmental health care agencies to increase attention to children, adolescents, and young adults with diabetes. As resources for diabetes remain very limited in many low- and middle-income countries, collaboration between NGOs, charities, and governmental agencies is essential for ensuring long-term improvements to care. ISPAD supports the global alliance ALIGN-T1D approach to securing formal contracts with the Ministry of Health in different nations.
Prof. Limbert closed with a strong call to action, saying that the declaration is not just a document, it is a commitment that providers and organizations around the world have to improving pediatric diabetes care.
8. Updates on T1D screening and monitoring: Screening in Japan and early-stage clinical service in Australia
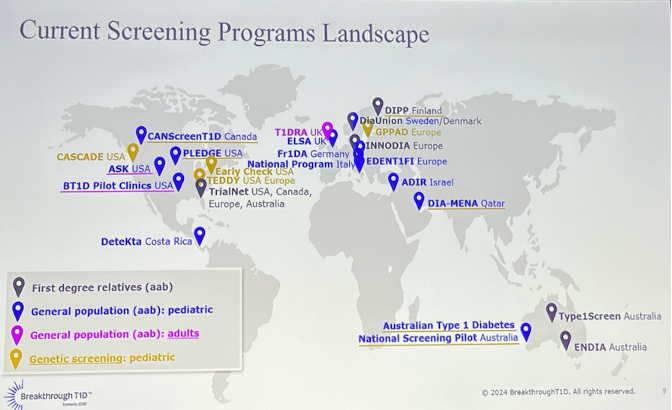
In this well-attended session, Dr. Anastasia Albanese-O’Neill (Breakthrough T1D), Prof. Elizabeth Davis (The Kids Research Institute, Australia), and Dr. Noriko Kodani (Japan Institute for Health Security, Japan) shared updates on early screening and monitoring for T1D. Dr. Albanese-O’Neill began by emphasizing that T1D is a progressive disease, characterized by stages 1 (normoglycemia with ≥2 autoantibodies), stage 2 (dysglycemia without symptoms), stage 3 (clinical diagnosis), and stage 4 (long-standing T1D). Each stage can have different interventions, with early detection and prevention or delay being the focus for stages 1 and 2 T1D. She further noted that T1D occurs often in people without family history (85%) and at any age, underscoring the impact of islet autoantibody screening in broad populations. Multiple screening programs exist globally (see figure below), but there are significant gaps in Asia, Africa, and most of South America.
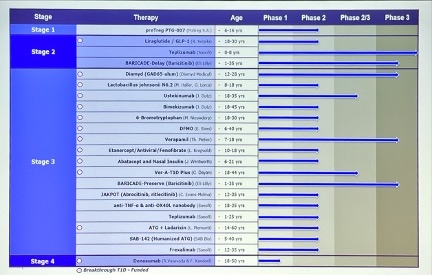
- Why is screening important? First, autoantibody screening and monitoring reduce diabetic ketoacidosis at diagnosis to approximately 3-8%, down from 30-46% in the general T1D population. Moreover, early detection offers patients opportunities to delay the onset of stage 3 T1D through the use of agents like Tzield (teplizumab), an anti-CD3 antibody, which is currently the only FDA-approved disease-modifying therapy. Excitingly, Dr. Albanese-O’Neill shared that there are many candidates in clinical trials that aim to delay the onset of stage 3 T1D, including GLP-1 RAs, baricitinib, verapamil, SAB-142, and more (see figure below). Finally, she underscored the importance of proper monitoring for people with early stage T1D, which clinicians can refer to the consensus guidance or abridged version from Breakthrough T1D.
- Dr. Kodani delivered updates on the ongoing PREP-T1D screening study in Japan. While T1D incidence in Japan is significantly lower (1.4-2.2 per 100,000/year) than in Caucasian populations (e.g., 36.5 per 100,000/year in Finland), the incidence in siblings of children with T1D remains comparable (3.3-3.8% vs. 6.7%). Hence, screening studies need to be started in Asian countries. PREP-T1D is a multicenter study that aims to define the prevalence of stages 1 and 2 T1D among first-degree relatives of people with autoimmune T1D in Japan. Conducted across 71 institutions, PREP-T1D has already identified 2,624 cases, far exceeding the target of 2,000. Dr. Kodani shared interim analysis (n=294) as of February 2025. She also pointed to the TIDE-J database study, which conducts monitoring for individuals with stage 1 or 2 T1D or single autoantibody positivity.
- Baseline characteristics and results. At baseline, participants were 29 years old, with 58% being female. 41% were parent of a children with T1D, while 29% were children and 30% were siblings. Interestingly, 5.7% of participants had an autoimmune thyroid disease. The study found 5.7% (n=11) to be autoantibody-positive, which is consistent with reports from other countries. Among 11 antibody-positive cases, seven were single-positive for ZnT8 antibody, and none had IAA positivity. In contrast, studies from other countries have generally reporter higher frequencies of GADA and IAA positivity. Full results of the study are expected in ATTD-Asia 2026.
- Prof. Davis shared her experience establishing an early-stage T1D (EST1D) clinical service in Australia. In Australia, there are multiple programs for early T1D detection, such as Type1Screen, T1D National Screening Pilot, TrialNet, and ENDIA. The increase in the number of children diagnosed with early-stage T1D prompted Prof. Davis’s team to establish an EST1D clinic to provide more tailored support to families. In doing so, Prof. Davis’s team identified four important needs to address: (i) education; (ii) psychosocial support for navigating uncertainty; (iii) access to clinical trials and disease-modifying therapies; and (iv) a plan for monitoring. For monitoring progression, A1c, OGTT, and repeat autoantibody monitoring remain as important tools. Prof. Davis also encouraged the use of CGMs, citing a survey that showed EST1D parents reported feeling empowered. Specifically, 10% time spent >140 mg/dL was associated with an 80% risk or progression to stage 3 T1D over one year in an ASK study.
9. Early insights into ketone patterns in T1D using continuous monitoring
Dr. Jennifer Ngan (University of Melbourne, Australia) presented early findings on ketone profiles in people with T1D without acute illness, using Abbott’s continuous ketone monitor (CKM) technology. The study utilized data from the two-week run-in period of the Australian PARTNER trial. While the data presented is not yet published, Dr. Ngan provided topline results, and we look forward to sharing more once published.
- Most participants maintained normal ketone levels (<0.6 mmol/L) throughout the run-in period. Baseline characteristics were not associated with ketone levels ≥0.6 mmol/L; however, there was a trend towards lower carbohydrate intake in the elevated ketone groups. Hyperglycemic episodes were poor predictors of ketosis.
10. Increasing rates of GDM are associated with higher maternal age and obesity
Dr. Yoo Lee Kim (CHA University, South Korea) presented results from a large retrospective review of factors associated with the development of GDM. Previous studies based in South Korea found a 5.1% prevalence of GDM over a three-year period (2012-2014). This longer-term, 10-year study sought to analyze the prevalence of GDM in the nation and how it has changed over time. The postpartum glucose metabolism status of women with GDM was also analyzed.
- Methods. A retrospective review of 22,019 medical records of women in South Korea from 2012-2021 were included. For those with singleton pregnancies, universal screening was performed using a 50-g glucose challenge test (GCT). For those with a result ≥140mg/dL, a three-hour 100-g oral OGTT was performed. GDM or normal glucose tolerance were diagnosed using the Carpenter-Coustan criteria. Postpartum glucose tolerance status was also assessed based on a 75-g OGTT performed 8-12 weeks after birth.
- The prevalence of GDM has increased over time along with maternal age, insulin resistance, and other factors. The prevalence of GDM increased significantly from 5.1% during the 2012-2014 time period to 5.9% over the subsequent seven years (p=0.0001). Maternal age increased from 33.2 years to 34.3 years over these time periods, as well as pre-pregnancy BMI (20.7 kg/m2 versus 21.1 kg/m2, p=0.0001). Of the patients where postpartum glucose tolerance testing was performed (48%), 54% had normal glucose tolerance, 19% had impaired fasting glucose, 25% had impaired glucose tolerance, and 1.4% had T2D.
- Mothers who demonstrated abnormal glucose metabolism had a significantly higher pre-pregnancy BMI and higher insulin resistance. Those with normal glucose tolerance had an average BMI of 22.4 kg/m2, versus 23.5 kg/m2 in those with impaired tolerance (p=0.0009). Insulin resistance as assessed by HOMA-IR was 1.32 versus 2.04, respectively (p=0.0001), where a score of 1 is considered “normal.”
- The authors suggest that the increasing prevalence of GDM and abnormal glucose tolerance may be related to increasing maternal age and obesity. Future studies both within South Korea and beyond may validate this hypothesis and encourage efforts towards awareness and prevention.
11. *NEW* Dr. Tom Wilkinson presents feasibility results of the second-generation Tandem Freedom FCL algorithm (n=10) in a three-day hotel setting
Dr. Tom Wilkinson (University of Otago, New Zealand) presented data on the second-generation Tandem Freedom fully closed-loop (FCL) AID system, following up on data on the first-generation system presented at ATTD-Asia last year. The Tandem Freedom algorithm is a new FCL algorithm in development (i.e., not an updated version of Control-IQ). The algorithm is a model predictive control (MPC) algorithm that makes glucose predictions every five minutes and determines the appropriate action, updating user settings at midnight each night.
- Previously, Prof. Martin de Bock (University of Otago, New Zealand) presented results from Tandem Freedom’s first-generation algorithm at ATTD-Asia 2024. In that study (n=10), TIR without meal boluses was slightly lower with Freedom than during the Control-IQ run-in period (55% vs. 62%). No instances of severe hypoglycemia or DKA were reported, and participants spent nearly all their time in automated mode (98.7%).
- Dr. Wilkinson presented results that included current t:slim X2 with Control-IQ users (n=10) in New Zealand, not on any non-insulin glucose-lowering agents other than metformin. Participants had a mean age of 39 years, diabetes duration of 16 years, and baseline A1c of 7.3%. As in the previous feasibility study, participants engaged in a one-week run-in period with Control-IQ followed by a 72-hour hotel stay with FCL use. Participants were provided three meals of unrestricted size a day and could have desserts with meals, as well as snacks between meals. Median meal sizes are shown in Table 1. Daily intake reached up to 339 g carbohydrate, 189 g protein, and 275 g fat. Participants were also encouraged to participate in ≥45 minutes of daily exercise in the late morning, along with supervised physical activity in the afternoon. There were no meal announcements of any kind by the user, nor were insulin boluses given for any meals or snacks.
Table 1: Median Meal Sizes
Meal | Carbohydrate | Protein | Fat |
Breakfast | 70.8 g | 36.7 g | 53.2 g |
Lunch | 53.8 g | 31.4 g | 40.0 g |
Dinner | 96.1 g | 67.6 g | 53.1 g |
Source: Dr. Tom Wilkinson’s presentation at ATTD-Asia 2025
- The Tandem Freedom FCL system demonstrated strong glycemic outcomes, particularly overnight. FCL was active 97.3% of the time. The median TIR was 61%, compared to 56% during the run-in period (which had a median of three user-initiated boluses). Overnight TIR was nearly 100% (96%), significantly higher than 70% during the run-in period (p=0.01). TBR was also significantly improved with FCL use (0.5%) compared to 1.8% during the run-in period. Moreover, total daily insulin was significantly reduced from 0.9 units/kg/day to 0.6 units/kg/day with the use of FCL (p<0.05). Dr. Wilkinson said that there was no sign of hyperglycemia related to the gentle exercise participants engaged in, and no DKA or severe hypoglycemic events were documented.
Figure 1: TIR Change Between Run-in and FCL Use

Source: Dr. Tom Wilkinson’s presentation at ATTD-Asia 2025
- The system responded quickly to meals. Most postprandial insulin was delivered within two hours for all meals, despite the lack of user-initiated announcements. For example, it delivered up to 80% of the postprandial four-hour insulin in the first two hours after breakfast (Table 2). Dr. Wilkinson concluded that the next-generation Tandem Freedom FCL system showed promising safety and glycemic outcomes in adults with T1D, particularly those with suboptimal glycemic management at baseline, even with high-carbohydrate, high-fat meals. He said the system could be particularly well-suited for individuals who struggle with consistent bolusing on HCL AID systems.
Table 2: Median postprandial insulin delivery with Tandem Freedom FCL
Meal | 1st Hour | 2nd Hour | 3rd Hour | 4th Hour |
Breakfast | 41.6% | 80.3% | 92.7% | 100% |
Lunch | 32.1% | 59.9% | 83.8% | 100% |
Dinner | 31.4% | 64.2% | 79.6% | 100% |
Source: Dr. Tom Wilkinson’s presentation at ATTD-Asia 2025
--by Riya Chatterjee, Jeremy Alkire, Nour Khachemoune, Kat Moon, Monica Oxenreiter, and Kelly Close