ATTD-Asia 2025 Day #2 Highlights –
Executive Highlights
- The second annual ATTD-Asia conference continued in Singapore for a strong Day #2, with a focus on dual glucose-ketone (DGK) monitoring, CGM benefits, and prediabetes screening and interventions.
- Dexcom hosted an educational school featuring insights in glycemic management with CGM. Drawing upon their experience with CGM from its inception nearly 20 years ago, Profs. Moshe Phillip (Tel Aviv University, Israel) and Tadej Battelino (University of Ljubljana, Slovenia) highlighted its benefit for broad populations, including people on insulin therapy, not on insulin, or with prediabetes.
- At Abbott’s high-energy symposium, Prof. David O’Neal (University of Melbourne, Australia) outlined how pairing CGM with emerging CKM (dual glucose-ketone monitoring) could meaningfully change the way clinicians detect, prevent, and respond to diabetic ketoacidosis (DKA). Prof. O’Neal argued that CGM and CKM complement rather than replace each other, and that integrating ketone data into routine diabetes care could meaningfully reduce delays in DKA detection. Key factors, such as education, clear response algorithms, reimbursement decisions, and broader clinical evidence, will ultimately determine how quickly and effectively the anticipated DGK will become a standard tool in diabetes safety.
- Dr. Viral Shah (Indiana University) discussed CGM use for diagnosing early dysglycemia, including stage 2 T1D, pre-T2D, and gestational diabetes. Notably, he introduced a novel metric, CGM Dynamic Index (CDI), currently being developed and validated in a three-year study. CDI incorporates CGM data not captured in TIR, TAR, or TBR, such as the frequency, amplitude, and duration of hyper- or hypoglycemia.
- Dr. Manoj Chawla (Lina Diabetes Care Centre, Mumbai, India) highlighted early intervention strategies for people with pre-T2D, including GLP-1 RAs, SGLT-2 inhibitors, TZDs, α-Glucosidase inhibitors, as well as lifestyle modifications that ideally go along with all therapeutic interventions. Moving forward, Dr. Chawla expects the field will develop specific staging for pre-T2D, just like T1D progression has divided into stages 1 through 4 in some regions[1]. He also recognized the heterogeneity of prediabetes and encouraged CGM use to tailor interventions to each individual.
- Dr. Shah also discussed GLP-1 RA use in people with T1D. Dr. Shah reviewed past literature on GLP-1 RA use in T1D, including the ADJUNCT ONE and ADJUNCT TWO trials of liraglutide, a study on semaglutide, and the TIRTLE trial of tirzepatide. Existing literature has left him with more questions than answers: How should patients safely titrate to lower dose to achieve glycemic and weight goals, and how do GLP-1 RAs improve outcomes? More data on cardiorenal outcomes with semaglutide in T1D are expected in ATTD 2026.
The second ATTD-Asia conference is taking place in Singapore December 9-11. See our Resource Hub and Day-by-Day Preview for the most up-to-date source of conference reporting, as well as a look at what is coming next.
Table of Contents
-
Top Highlights
- 1. Dual glucose-ketone monitoring for earlier DKA detection and safer insulin therapy
- 2. Dexcom School: CGM as a champion in the battle against elevated glucose levels
- 3. Dr. Viral Shah introduces novel metric, CGM Dynamic Index, for diagnosing early dysglycemia
- 4. Teasing out the relationships between TITR, glycemic variability, and diabetes complications with Prof. Ramzi Ajjan
- 5. Beyond AID and CGM: Dr. Viral Shah reviews the evidence for GLP-1 RAs in T1D
- 6. Dr. Manoj Chawla reviews disease-modifying therapies for pre-T2D
- 7. Real-world use of MiniMed 780G in Japan and APAC: Insights on glycemic outcomes and user behaviors from Prof. O’Neal and Dr. Noriko Kodani
- 8. Glycemic rhythms and heart health: Prof. Ramzi Ajjan on using CGM to meaningfully reshape cardiovascular risk assessment
- 9. Benefits and practical challenges to the implementation of inpatient CGM from Prof. Spiros Fourlanos
- 10. Pathophysiology and interventions for prediabetes in multiple countries throughout Asian from Dr. Anoop Misra
- 11. AI, wearables, and gut health for prediabetes prevention from Prof. Elaine Chow
- 12. Preliminary data presented by Prof. Elizabeth Davis shows early AID onboarding improves glycemic outcomes in Australian pediatric T1D
- 13. MiniMed 780G found to be cost effective for Japanese adults with T1D compared to MDI with CGM
- 14. Dr. Viswanathan Mohan on the potential for charitable organizations to change the course of T1D in low- and middle-income countries
- 15. *NEW* The state of diabetes technology in Japan: CGM growth and AID challenges
Top Highlights
1. Dual glucose-ketone monitoring for earlier DKA detection and safer insulin therapy
At Abbott’s high-energy symposium, Prof. David O’Neal (University of Melbourne, Australia) outlined how pairing CGM with emerging CKM could meaningfully change the way clinicians detect, prevent, and respond to diabetic ketoacidosis (DKA). He said that current testing practices leave wide safety gaps, while dual-analyte data may capture a clearer, earlier, and behavior-shaping picture of metabolic risk.
- There are major gaps in ketone literacy that create a need for better monitoring tools. Prof. O’Neal began by revisiting mortality trends, discussing how DKA deaths surged during COVID-19 due to delayed detections and reduced access to point-of-care (POC) ketone testing. Even after the pandemic, global surveys show that many people with diabetes lack access to ketone strips and do not know DKA symptoms, leading to making unsafe decisions during high-risk scenarios. Standard blood ketone meters are accurate yet still require users to initiate testing and offers no pattern information. These limitations often prolong the time of recognition of rising ketones, especially when glucose levels remain deceptively normal.
- CKM provides real-time ketone trends and actionable alarms, compensating for missed metrics from glucose-only monitoring. Previewing the anticipated dual-sensor system from Abbott, Prof. O’Neal explained how CKM captures interstitial ketone dynamics continuously, with trend arrows and alarms likely capturing normal to urgent high levels of ketones, with a threshold not decided on yet. Early feasibility data show strong durability and up to 14-day wear with a single insertion. Real-world case examples show that ketone levels can climb to clinically meaningful levels while glucose remains well within range, making CGM alone insufficient for early detection. He presented cases where CKM identified rising ketones during SGLT-2 therapy or pump suspension long before symptoms developed, underscoring the inability of glucose data to reliably detect potential ketosis.
- Dual monitoring may address risk in SGLT-2 users, support safer AID use, and could prevent hospitalizations, yet key performance standards are still under development. Prof. O’Neal emphasized ongoing knowledge gaps, including no agreed-upon accuracy standards for ketone sensors and a limited understanding of “normal” ketone profiles across diabetes types. Regulatory pathways also remain undefined. Still, multiple NIH-funded studies are underway to evaluate CKM in SGLT-2 users, inpatient insulin-withdrawal scenarios, and renal impairment. Early data from the PARTNER cross-over trial, which will be presented tomorrow, aim to illustrate CKM’s value in real time.
- Prof. O’Neal closed by positioning dual glucose-ketone monitoring as a logical next step in DKA prevention. He argued that CGM and CKM complement rather than replace each other, and that integrating ketone data into routine diabetes care could meaningfully reduce delays in DKA detection. Multiple factors will determine success for dual glucose monitoring including:
- Quality of algorithms - clear response algorithms were mentioned;
- Payor approach (reimbursement decisions in the US);
- Investment in and approach to education; and
- Broader clinical evidence.
While multiple factors will ultimately determine how quickly and effectively the anticipated DGK will become a standard tool in diabetes safety, it was great to see future standards discussed.
2. Dexcom School: CGM as a champion in the battle against elevated glucose levels
The 2025 Dexcom School at ATTD-Asia featured a well-attended lunchtime presentation. Chairs of the conference Prof. Moshe Phillip (Tel Aviv University, Israel) and Prof. Tadej Battelino (University of Ljubljana, Slovenia) drew upon their experience with CGM from their first experiences with it in the early 2000s. Having seen the benefits of the technology over time as adoption has expanded, Profs. Phillip and Battelino are confident in its benefit for broad populations with diabetes and prediabetes. They discussed CGM for those on insulin therapy, those not on insulin, and those on prediabetes, even those decades before a diabetes diagnosis.
- CGM should serve as the standard of care for all insulin treated people with diabetes. Prof. Phillip began by emphasizing the importance of early CGM use at the time of diagnosis. A 2o19 study (n=396) demonstrated that CGM users had a significantly greater improvement in glycemic control compared to non-CGM users from 1-2.5 years after diagnosis. The MDI + CGM group had 1.5% lower A1c values on average than the MDI-only group, and the insulin pump + CGM group had 0.7% average lower A1c than the insulin-pump-only group. The MDI + CGM group also had significantly lower A1c values than the insulin pump only group (7.7% versus 8.7%). As the benefit of CGM was demonstrated regardless of insulin delivery method, Prof. Phillip said that CGM should be prioritized over other forms of diabetes technology in cases of resource scarcity. Emergency department visits were also significantly reduced for early adopters of CGM. A 2022 study confirmed the benefits of early CGM initiation: when the technology was adopted within the first year of T1D diagnosis, a significant improvement to A1c values was observed over seven years (7.6% in CGM users versus 9.8% in non-users). The early initiation of CGM may have a key role in optimizing glycemic control and decreasing long-term complications.
- Opportunities remain to further expand CGM use to people with T2D. As of 2017, Prof. Phillip said that approximately 2-3% of US adults with T2D used CGM. By 2020, this had risen to 8-10%, 13% by 2021, 20-25% among insulin-treated adults with T2D by 2022-2023, and 30% by 2023, based on Medicare data, for insulin-treated adults with T2D. Based on the demonstrated early benefits of CGM adoption, Prof. Phillip continues to support broader adoption of CGM among people with T2D.
- Prof. Battelino discussed the systemic harm caused by elevated glucose levels and the opportunity for CGM to detect the early development of this phenomenon. A 2023 large-scale (n=39,283) UK Biobank study demonstrated significant associations between elevated A1c values, differences in brain structure, and changes to cognitive abilities. A 2024 nationwide registry study also demonstrated a two-fold higher likelihood of cardiovascular disease events among those who would later be diagnosed with T2D – even three decades before diagnosis. This indicates that elevated glycemia eventually leading to the development of T2D confers significant risk upon patients, and that comprehensive preventative strategies should be initiated much earlier in individuals at risk of T2D.
- Given the long-term risk of elevated glucose levels, Prof. Battelino discussed opportunities for CGM use to drive long-term behavioral improvements. A recent study demonstrated that just two weeks of CGM use with structured education in a workplace-based setting helped patients lose weight, improved LDL cholesterol, and improved glycemia among individuals with T2D. In closing, Prof. Battelino again emphasized the risk of glucose levels that are even slightly elevated and the power for CGM to prevent such a trend. He called for CGM to be offered to all individuals with prediabetes, GDM, and all those with non-insulin treated T2D as well as traditional CGM users.
3. Dr. Viral Shah introduces novel metric, CGM Dynamic Index, for diagnosing early dysglycemia
In this afternoon session, Dr. Shah discussed CGM use for diagnosing early dysglycemia. Dr. Shah positioned CGM as a potential diagnostic tool for subclinical stage 2 T1D, stage 2 T2D (prediabetes), and gestational diabetes, as well as a predictor for progression into clinical diabetes. He highlighted ongoing research to define diagnostic thresholds using static and dynamic metrics. In doing so, Dr. Shah underscored the complexity of using CGM data, as factors like sex, age, and comorbid conditions impact glucose regulation.
- CGM offers both static and dynamic data. Static metrics include mean glucose, Time in Range (TIR), Time above Range (TAR), Time below Range (TBR), and coefficient of variation (CV), which capture nontemporal information about hyper- and hypoglycemia and glycemic variability. In T1D, where most research is done, TAR above 140 mg/dL is generally accepted as a threshold for increased risk of dysglycemia (stage 2 T1D) in people without clinical diabetes. This threshold is based on studies that found that people without diabetes spend 96% of their days below 140 mg/dL. Those who spend greater than 5% (high sensitivity) or 10% (high specificity) in TAR may be considered to have stage 2 T1D.
- Dr. Shah cautioned about the notion of “normal glucose value,” however. Glucose regulation – and by extension, CGM data – can vary by age, sex, race, BMI, comorbidities, and even menstrual cycle. Moreover, CGM devices are not interchangeable and have high variability. Therefore, a “normal” cutoff may not be applicable to a heterogeneous pool of individuals.
- Dynamic data can better capture glycemic trends that static data fail to incorporate, such as the frequency, amplitude, and duration of hyper- or hypoglycemia. Dr. Shah is currently working with Dr. Eslam Montaser, a mathematician at Indiana University to develop a novel metric, the CGM Dynamic Index (CDI). CDI is based on entropy modeling and time-series mathematics. In layman’s terms, 24-hour CGM data is divided into 15-minute segments, which are classified into eight glycemic states. The metric calculates the probability of transitioning between states (entropy) to ultimately reflect the frequency, amplitude, and speed of glycemic fluctuations. High CDI refers to unstable glucose and rapid transitions between states, while low CDI refers to stable glucose with minimal transitions. This index is now being validated in a Breakthrough T1D-funded longitudinal study that tracks the progression of participants with stage 1 and 2 T1D to stage 3 type 1 diabetes over four years. The study will evaluate whether CDI accurately identifies various stages of T1D and predicts the progression from stage 2 to stage 3 T1D compared to A1c and oral glucose tolerance test (OGTT). During Q&A, Dr. Shah clarified that while OGTT currently remains the gold standard for the diagnosis of diabetes, hopefully, CGM metrics will replace OGTT in the future.
4. Teasing out the relationships between TITR, glycemic variability, and diabetes complications with Prof. Ramzi Ajjan
Prof. Ramzi Ajjan (University of Leeds, UK) emphasized the importance of CGM-derived metrics beyond A1c and TIR, specifically examining the relationships between Time in Tight Range (TITR), glycemic variability (GV), and the risk of diabetes complications. He offered some valuable context on the metrics, saying that while TIR and TITR are correlated, it is non-linear and affected by other glycemic markers, including GV.
- Prof. Ajjan pointed out that TITR is valuable when tighter glucose management is clinically desired, as it helps normalize glucose levels more effectively to reduce the risk of complications. However, he emphasized that TITR’s usefulness depends on the long-term clinical goal. For example, achieving normoglycemia is not typically a practical goal for many patients (citing TITR >91% as a “normal” glucose level). For patients aiming to reduce their A1c to ≤7.0%, meanwhile, Prof. Ajjan said TIR is generally sufficient and often more appropriate for the general population. He specified that this is especially true for patients with low coefficient of variation (CV; ~18%), given the manner in which glycemic variability can partially mediate the relationship between TIR and A1c (explained further below). He acknowledged the concerns of some patients and clinicians who feel that aiming for TITR targets may introduce undue burden on patients who are still not yet meeting TIR targets.
- Turning then to glycemic variability (GV), Prof. Ajjan explained that the metric is a complex marker with multiple dimensions and is difficult to quantify accurately. He pointed out that there are over 30 metrics measuring GV, and some are more sensitive to hypoglycemia, while others, like MAGE (mean amplitude of glycemic excursions), focus on postprandial fluctuations. He also warned against over-relying on CV for assessing GV, as it can be influenced by glucose levels (higher glucose can make CV appear lower).
- Prof. Ajjan reviewed the evidence linking GV with diabetes complications. Increased GV is associated with a higher prevalence of diabetic retinopathy (DR) in T2D. However, this relationship was not seen in patients with LADA (latent autoimmune diabetes in adults), though he noted the sample size was small. Similarly, higher GV was linked to increased risk of peripheral neuropathy in both T1D and T2D. In terms of vascular health, higher GV, as measured by SD (standard deviation) and CV, correlates with greater intima-media thickness, which is a marker of cardiovascular risk. The association remains significant, though lower, even after adjusting for other risk factors. Additionally, an inverse relationship was found between ABI (ankle-brachial index) and GV, and higher MAGE was associated with CVD. Further, Prof. Ajjan discussed the possible role of insulin resistance (IR) in the relationship between GV and complications. As GV increases, so do levels of TNF (tumor necrosis factor) in patients with high IR, but not in those with normal IR. This interaction may contribute to vascular and other complications. He also mentioned emerging evidence suggesting that vitamin D deficiency may exacerbate the impact of GV on retinopathy, although more research is needed.
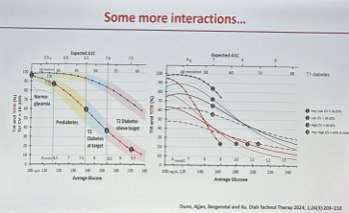
- Finally, Prof. Ajjan emphasized that while TITR is associated with a reduced risk of diabetes complications, its relationship with both TIR and outcomes are complicated by the effects of glycemic variability. He illustrated this with a comparison of TIR and TITR across varying levels of CV, showing that as CV increases (represented by the color blue for TIR and red for TITR in the figure below), the ability to maintain TIR declines. For example, at low mean glucose levels (~160 mg/dL) with low CV, TITR and TIR diverges significantly. In cases of high CV (>44%), it becomes impossible to achieve a TIR >70%, reaffirming the need to minimize glycemic variability to better achieve glycemic goals. As CV becomes higher, the gap between achievable TIR and TITR narrows.
5. Beyond AID and CGM: Dr. Viral Shah reviews the evidence for GLP-1 RAs in T1D
Dr. Viral Shah (Indiana University) argued that CGM and AID alone are insufficient to optimize glycemic management or reduce long-term complications in T1D, making the case for GLP-1 RA adjunct therapy. In the US, only about half of adults with T1D achieve an A1c <7.0% despite growing AID use, largely reflecting suboptimal daytime control, when people with diabetes are not eating, exercising, or stressed. Moreover, CVD mortality remains elevated in both T1D and T2D; although improving in T1D, individuals with T1D or T2D still lose about a decade of life compared to those without diabetes. Even with A1c <7.0%, CVD mortality is nearly three times higher than in the general population. Dr. Shah emphasized that while A1c matters, it is not the sole driver of cardiovascular risk, reinforcing that insulin alone is not enough and additional therapies are needed.
- Dr. Shah reviewed existing literature on multiple drug classes in T1D. He characterized metformin and DPP-4 inhibitors as “neutral” and noted the well-documented increased DKA risk with SGLT-2 inhibitors. He expressed optimism that continuous ketone monitoring could revive research on SGLT-2 inhibitors in T1D and potentially support future label changes. He then more extensively reviewed the current state of GLP-1 RA use in T1D. He said the literature has raised as many questions as answers, though recent findings have been “profound.” Key questions include how to safely titrate to lower doses that achieve glycemic and weight goals, and how GLP-1 RAs influence cardiovascular, renal, and liver outcomes – he teased upcoming ATTD 2026 data on cardiovascular and renal outcomes with semaglutide in T1D on this front as well.
- Dr. Shah spent most of his time reviewing the state of GLP-1 RA use in T1D. Existing literature has left him with more questions than answers – though he said recent data on the drug class in the population has been “profound.” These remaining questions include how to safely titrate to lower dose to achieve these glycemic and weight goals, and how GLP-1 RAs improve CVD, renal, and liver outcomes. He teased the presentation of data on CVD and renal outcomes with semaglutide in T1D at ATTD 2026.
- Dr. Shah reviewed the ADJUNCT ONE and ADJUNCT TWO trials of liraglutide in T1D. Although liraglutide did not meet the FDA’s required ≥0.4% A1c reduction versus placebo, achieving only 0.2-0.3% reductions (alongside increased symptomatic hypoglycemia), the trials yielded important lessons: CGM is essential for adjunct-therapy studies (with AID even better), GLP-1 RA dosing must be flexible, and insulin titration should be guided by A1c and CGM data. Additionally, higher discontinuation due to adverse events was associated with lower BMI, longer diabetes duration (>25 years), and lower daily insulin doses.
- He then reviewed his recently published study on semaglutide in adults with T1D and obesity, initiated not to pursue a label change but to demonstrate feasibility and encourage a phase 3 trial. Using a flexible titration protocol, 36% of participants on semaglutide met the primary outcome of TIR >70%, TBR <4%, and ≥5% weight loss (compared with none on placebo), a result he described as “pretty powerful.” The adjusted A1c reduction was 0.3%, though he noted that placebo participants experienced a large 0.8% drop from a baseline of 7.7%. Weight loss with this lower semaglutide dose occurred more slowly than the near-immediate improvements in A1c and TIR. Insulin doses declined by 25% from baseline, only 17% of which was attributable to weight loss and just 20% to reduced carbohydrate intake, leading Dr. Shah to suggest GLP-1-related beta-cell secretory effects as a likely explanation.
- Dr. Shah also noted a similar tirzepatide study with positive findings, TIRTLE, which was presented at EASD 2025.
6. Dr. Manoj Chawla reviews disease-modifying therapies for pre-T2D
In this packed morning session, Dr. Manoj Chawla (Lina Diabetes Care Centre, India) highlighted early intervention strategies for people with pre-T2D. Prediabetes is characterized by impaired glycemic regulation and elevated glucose levels, and is driven by insulin resistance, beta cell dysfunction, and increased hepatic glucose production. This early stage of metabolic dysfunction yields a window for disease modification before significant vascular and cellular damages are made. Dr. Chawla advocated for increased awareness about screening to identify people with prediabetes and reviewed disease-modifying therapies known to delay or prevent progression by: (i) targeting insulin resistance; (ii) preserving beta cell function; (iii) lowering postprandial hyperglycemia; or (iv) reducing weight.
- Lifestyle modification and metformin have long been recognized as foundational interventions for diabetes prevention, as assessed in the US, China, Finland, and India. Specifically, among Indians, Dr. Chawla noted that lower dose of metformin (500 mg/day versus 1,700 mg/day) was found to be equally effective at improving glucose tolerance in the Indian Diabetes Prevention Program (IDPP) compared to the US DPP. Moreover, in the D-CLIP study, lifestyle intervention and stepwise addition of metformin (for 72% of study participants) achieved 32% relative reduction in diabetes incidence at three years of follow up. Given the study results, India’s regulatory agency approved metformin for the additional indication of prediabetes; in the US, metformin is not FDA-approved for this indication. Finally, Dr. Chawla noted that technological advancements can improve and expand access to lifestyle interventions. One study found that AI-powered lifestyle coaching program was non-inferior to human-led programs.
- Beyond metformin, GLP-1 RAs, SGLT-2 inhibitors, and thiazolidinedione (TZD) have demonstrated benefits in preventing diabetes, especially when used in combination.
- GLP-1 RAs. In STEP trials, semaglutide 2.4 mg was associated with significant improvements in glucose metabolism and higher likelihood of achieving normoglycemia (84-90% versus 48-70% with placebo) among people with overweight or obesity and baseline prediabetes. Tirzepatide also demonstrated impressive glycemic benefits in this population. In the SURMOUNT-1 trial, tirzepatide reduced progression from prediabetes to diabetes by 94% at three years. Older generations of GLP-1 RAs like liraglutide similarly showed lower rates of three-year diabetes incidence (2% versus 6% with placebo).
- SGLT-2 inhibitors. According to a systematic review, SGLT-2 inhibitors are associated with a delayed progression or reduced risk of new-onset T2D, especially in people with pre-existing heart failure or chronic kidney disease. Given that SGLT-2 inhibitors yield significant cardiovascular and kidney protection, Dr. Chawla said that this drug class would be most beneficial for people with cardiorenal conditions.
- TZDs (e.g., pioglitazone). This drug class is a powerful insulin sensitizer but is limited by safety concerns, like increased risk of heart failure. In the ACT NOW study, pioglitazone was associated with 72% reduced risk of developing diabetes, with three-year incidence being 7.6% (versus 25% with placebo). However, Dr. Chawla cautioned that pioglitazone could cause weight gain, fluid retention, and chronic heart failure exacerbation and that careful risk-benefit assessment is needed.
- α-Glucosidase inhibitors (e.g., acarbose and voglibose). This drug can be especially beneficial for Asians who have high carbohydrate diets. In studies, voglibose conferred a 36% reduction in diabetes risk in people with impaired glucose tolerance. In a post-hoc analysis of the STOP-NIDDM study, acarbose was associated with lower cardiovascular outcomes (2.2% versus 4.7%), as well.
- In closing, Dr. Chawla reviewed the ADA Standards of Care regarding diabetes prevention. The ADA recommends metformin for T2D prevention with potential vitamin B12 supplementation. Given that people with prediabetes are also at increased risk for cardiovascular disease, they should undergo more thorough screening and treatments of modifiable risk factors. Pioglitazone could be considered especially for those with a history of stroke, insulin resistance, and prediabetes; however, its use requires careful benefit-risk analysis.
- Looking forward, Dr. Chawla expects the field will develop specific staging for pre-T2D, just like T1D progression is divided into stages 1 through 4. He also cautioned that prediabetes is a heterogeneous condition with variations in insulin sensitivity, beta cell function, and organ-specific fat distribution, and not all patients will have the same clinical risks or treatment responses. Therefore, it is important to tailor interventions to each individual such as through CGM use.
7. Real-world use of MiniMed 780G in Japan and APAC: Insights on glycemic outcomes and user behaviors from Prof. O’Neal and Dr. Noriko Kodani
In this afternoon expert session focused on diabetes technology, Prof. David O’Neal (University of Melbourne, Australia) and Dr. Noriko Kodani (Japan Institute for Health Security, Japan) presented real-world evidence on the use of MiniMed 780G in the Asia-Pacific (APAC) region, with a focus on Japan.
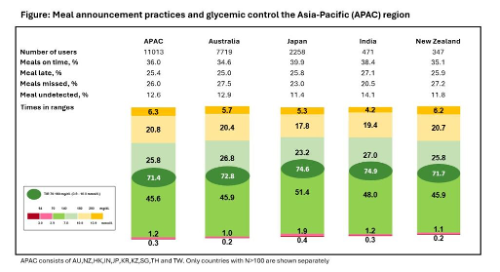
- Prof. O’Neal presented real-world data on meal announcement practices among MiniMed 780G users in APAC (n=11,013). Medtronic developed a meal detection algorithm, trained on over 60,000 meal events, which was tested on 155 users. The algorithm achieved a 91% true positive rate, with 62% of meals detected within 30 minutes and an average lag time of 13 minutes. Using CareLink Personal data from MiniMed 780G users in APAC (Australia, New Zealand, Japan, and India), meals were classified as: (i) “on time” (bolus within 15 minutes of detection); (ii) “late” (bolus within 90 minutes); (iii) “missed” (no bolus); or (iv) “undetected” (no meal detection). Only adults over 29 years were included. Prof. O’Neal reported minimal missing data.
- Findings were particularly notable in Japan and India. Across the four countries, 38% of meals were “on time,” 19% “late,” and 27% were “missed.” Japan and India had the highest on-time meal announcements (40% and 38%, respectively) and the lowest missed meals (23% and 21%). These two countries also showed the best glycemic outcomes: Japan had a 75% TIR and 51% TITR, while India had 72% TIR and 48% TITR. APAC users overall achieved 47% Time in Tight Range (TITR) and 72% TIR. Prof. O’Neal emphasized the significance of these findings by reminding the audience that TITR is more strongly correlated with complication prevention than TIR.
- Dr. Kodani then presented observational data comparing MiniMed 780G use in Japan (n=5,188), the US (n=117,275), and the global population (n=374,548) through April 2025.
- Both the Japanese and global cohorts showed strong glycemic outcomes, with additional improvements seen in users adopting recommended “optimal settings,” as discussed by Prof. Goran Petrovski at the Medtronic school yesterday as well. Japan had a lower adoption rate of optimal settings at just 6%, compared to 16% globally and 9% in APAC. Dr. Kodani suggested this was due to significant intra-institution variation.
- Although the Japanese population met consensus-recommended targets for Time below Range (TBR <70 mg/dL), TBR in this dataset was higher in Japan (2.5%) compared to the global population (<2%). This trend persisted even among users of the recommended settings. Dr. Kodani noted that about 10% of her patients struggle with hypoglycemia, a seemingly more common trend that likely contributed to this higher national TBR. However, the Japanese cohort showed parity with global users in meeting GMI (<7.0%) and TIR (≥70%) targets: 52% in Japan, 53% in the US, and 54% globally. Among those using optimal settings, 80% of Japanese users met TIR and GMI targets, compared to 70% of US and 73% of global users. However, Dr. Kodani said that participants in Japan had a lower proportion of users meeting all three targets (39% in Japan vs. 49% in the US and 48% globally). Dr. Kodani speculated that this frequent hypoglycemia might be due to the use of false carbohydrate entries by Japanese users, noting anecdotally that it is common in Japan to “split” prandial doses.
- The study also identified trends in the use of the temporary 150 mg/dL target and reported daily carbohydrate intake. Japanese users used the 150 mg/dL target more frequently than global users (4% vs. 2%), while US users were more likely to use lower target glucose settings (100 mg/dL or 110 mg/dL). Dr. Kodani explained that when patients transitioned from MiniMed 770G to 780G, many initially preferred a higher target (120 mg/dL) due to fear of hypoglycemia with the lower targets. However, over time, more than 80% of her patients have adjusted to the recommended 100 mg/dL target. This fear of hypoglycemia also led many Japanese users to prefer longer active insulin times (three or four hours), to avoid the correction bolus being absorbed “too early.”
- Interestingly, Japanese users reported a higher carbohydrate intake (207 g/day) compared to the US (144 g) and global (157 g) populations. Despite this, they had a lower total daily insulin dose (43 units vs. 61 units and 53 units, respectively) and a higher insulin-to-carbohydrate ratio (10.8 g/U vs. 8.4 g/U and 9.3 g/U), suggesting higher insulin sensitivity. Japanese users also reported a higher proportion of prandial insulin in their total daily dose (~70% vs. ~50% in the US). Dr. Kodani speculated that this higher insulin sensitivity may contribute to the higher TBR observed.
8. Glycemic rhythms and heart health: Prof. Ramzi Ajjan on using CGM to meaningfully reshape cardiovascular risk assessment
Prof. Ajjan (University of Leeds, UK) urged attendees to rethink how glycemia is assessed in people with diabetes and cardiovascular disease (CVD), emphasizing that reliance on A1c alone fails to capture critical risks such as hypoglycemia and glycemic variability. Speaking from his experience of collaboration with cardiologists, he said that CGM provides the granularity needed to evaluate and mitigate cardiovascular risks, far beyond what A1c can offer.
- Cardiologists remain unconvinced by A1c as an accurate cardiovascular risk metric, and Prof. Ajjan underscored why CGM provides a more actionable and practical glycemic profile. He explained that cardiologists prioritize interventions with clear-cut cardiovascular benefits, and decades of mixed A1c-lowering trials have removed enthusiasm for glycemia as a CVD target. He revisited the “U-shaped association” between A1c levels and mortality rates, reproduced in a 2024 dataset of 845 individuals with CVD and diabetes, showing that both very low and high A1c levels are associated with worse outcomes, making cardiologists uncertain about pursuing intensive glycemic targets. He also underscored why A1c is an imprecise metric, with A1c of 7.0% corresponding to average glucose values ranging from ~110 to ~170 mg/dL with no visibility into hypoglycemia or glycemic variability. For cardiologists who demand causal evidence, these limitations weaken A1c’s perceived effectiveness for CVD prevention.
- Glycemic variability (GV) is emerging as an independent cardiovascular signal and CGM is the only tool capable of reliably measuring it. Prof. Ajjan cautioned that GV has been inconsistently assessed using A1c and fasting glucose variability, BGM, and CGM altogether, even though only CGM-derived variability reflects accurate daily glucose fluctuations. He reviewed CGM-based evidence linking higher postprandial variability (e.g., elevated MAGE) with increased major adverse cardiovascular events (MACE) in acute coronary syndrome populations, including in individuals without diabetes. Addiitonal data suggest GV interacts with inflammation, thrombosis, and insulin resistance, reinforcing its relevance to vascular disease. He also highlighted Swedish registry findings showing that insulin-treated T2D patients using CGM experienced fewer myocardial infractions (MI), heart failure events, and strokes that non-CGM users.
- CGM can reduce hypoglycemia and offers an opportunity to modify a risk factor that cardiologists increasingly recognize as harmful. Across large observational studies, including an analysis of over 1.5 million people in South Korea, Prof. Ajjan highlighted that hypoglycemia increases the risk of MI, stroke, heart failure hospitalization, and all-cause mortality, with risk rising further after recurrent events. He referenced the LIBERATES RCT (n=141) showing identical A1c reductions between CGM and BGM groups, but a difference in over an hour per day reduction in hypoglycemia for those randomized to CGM. Interestingly, this reduction was pronounced among individuals on sulfonylureas, which was unexpected. Since most hypoglycemia reduction occurred within the first 48-72 hours of sensor use, he described CGM as a behavior-modifying intervention that enables rapid self-correction. He referenced recent ESC guidelines now explicitly recommend avoiding hypoglycemia in people with CVD, an important shift in cardiology perspectives.
- Just as SGLT-2 inhibitors are now widely viewed as cardiology drugs rather than diabetes drugs, Prof. Ajjan said he hopes CGM will eventually be regarded as a cardiology device, as an essential tool for CVD risk reduction rather than confined to diabetes care.
9. Benefits and practical challenges to the implementation of inpatient CGM from Prof. Spiros Fourlanos
Prof. Fourlanos (University of Melbourne, Australia) delivered a comprehensive overview of the accelerating usage of CGM in the hospital, emphasizing both the clinical benefits and the substantial workflow challenges that must be considered for real-world implementation. In-hospital CGM use and the continuation of pre-existing personal devices can meaningfully improve the detection of adverse glycemia, and as some trials demonstrate, overall TIR. However, these benefits coexist with substantial implementation hurdles. Ultimately, Prof. Fourlanos framed inpatient CGM as a promising but still-evolving frontier in diabetes care.
- Rising inpatient diabetes burden and widespread pre-admission CGM use are driving the need for structured hospital approaches. Prof. Fourlanos reminded attendees that inpatient diabetes prevalence now reaches 20-25% across Australia, the UK, and the US. Data in Asian regions remain limited. As of 2010, a Japanese dataset showed an inpatient diabetes prevalence of about 11%, highlighting regional gaps in surveillance. CGM adoption in the broader diabetes community has accelerated due to national subsidies from governments, leading to a rapid increase in admissions of patients already wearing CGM when they arrive. His group’s trial across multiple hospitals found that approximately 25% of adults with T1D were admitted while actively using CGM. He said that these admissions must be separated into two distinct categories: (i) patient-directed continuation of personal CGM devices; and (ii) hospital-directed telemetry CGM, each with different roles, responsibilities, and risk profiles.
- Inpatient CGM studies show glycemic benefits to TIR and hypoglycemia detection but results still remain mixed and require further RCTs. Prof. Fourlanos highlighted CGM telemetry RCTs, including US-based RCTs (n=110) and the Danish DIATEC study (n=166) presented at EASD 2025. He noted variable results but consistent directional benefits. DIATEC demonstrated one of the strongest effects, with a mean TIR of 78% in the CGM group versus 63% in the control group, accompanied by broader improvements across TIR, Time below Range (TBR), Time above Range (TAR), and increased insulin intensification as guided by CGM thresholds. By contrast, other RCTs showed narrower TIR gains or more pronounced reductions to recurrent hypoglycemia rather than global glycemic improvements. Beyond RCTs, Prof. Fourlanos discussed a retrospective observational study comparing over 100,000 CGM readings with approximately 5,500 POC tests, which showed that CGM detected hypo- and hyperglycemia 45-60 minutes earlier than POC. This often captured glycemic events at milder severity. He also noted compelling results from an inpatient closed-loop trial (n=136), which showed a TIR of 66% with AID versus 42% in the control group, raising the question not of whether inpatient AID will arrive, but when and for whom.
- International hospital guidelines increasingly support CGM for non-critical care patients, but safe implementation requires standardized workflows, staff education, and continued POC confirmation. Despite variation in global data, major organizations including the ADA and recent Australian guidelines now conditionally endorse continuing CGM in the hospital with parallel POC monitoring. Prof. Fourlanos emphasized the need for practical rules: (i) remove CGM only if the patient cannot participate (e.g., unconsciousness); (ii) defer but do not necessarily remove during periods of hemodynamic instability; and (iii) otherwise, use CGM as a patient prompt for confirmation POC checks. He continued to highlight persistent challenges such as the rapid turnover of clinical staff unfamiliar with CGM and inadequate documentation of patient-provider “memoranda of understanding,” which outline shared responsibilities for alerts. While CGM accuracy in hospitals is generally reassuring, issues such as sensor lag, interfering medications, and incorrect EMR data entry can also negatively impact reliability. Importantly, he said that systematic timestamp alignment showed that automated POC-to-EMR transfer of five minutes produced optimal MARD, whereas manual entry introduced a 10-minute delay, worsening accuracy metrics.
- Prof. Fourlanos closed by emphasizing that CGM use in hospital is still in its early stages. CGM is currently largely viewed in parallel to EMRs, and only a few centers operate real-time digital dashboards with device cloud EHR integration and specialized inpatient monitoring teams. He pointed to the iCoDE report, discussed at DTM 2025, as a roadmap for standardizing interoperability, visualization, and workflow frameworks necessary for safe and salable inpatient CGM use. While CGM increases short-term system costs, potential reductions to adverse events and infections also suggest meaningful long-term value. CGM has the potential to transform inpatient glucose management, but only with sustained support and intentional implementation aligned with patient needs.
10. Pathophysiology and interventions for prediabetes in multiple countries throughout Asian from Dr. Anoop Misra
In a fascinating afternoon session, Dr. Anoop Misra (Fortis Centre for Diabetes, Obesity and Cholesterol, New Delhi, India) delved into the prevalence, pathophysiology, and interventions for prediabetes in Asian populations. Prediabetes is characterized by dysglycemia and impaired glucose tolerance and serves as a critical window for T2D prevention and reversal to normoglycemia. Compared to white populations, Chinese, Filipino, and South Asians face higher prevalence of prediabetes. Moreover, within the Asian population, different ethnicities have distinct underlying pathophysiology. Indians are more likely to have impaired fasting glucose, while Malaysians, Indonesians, and Chinese were more likely to have impaired glucose tolerance. Dr. Misra further noted that prediabetes is “aggressive” in South Asians, as it converts to T2D twice as rapidly compared to white population. Likewise, reversal to normoglycemia with lifestyle interventions is significantly harder, occurring only in 30% of South Asians, compared to 50% in the white population. Dr. Misra discussed the reason behind this difference and reviewed lifestyle and therapeutic interventions to mitigate disease progression.
- South Asians have greater abdominal fat, including in the liver and pancreas. Hepatic fat is an especially strong predictor of dysglycemia. In an unpublished MRI-based study, each unit increase in hepatic fat was associated with 16% greater risk of prediabetes in Indians, Japanese, and Chinese. Pancreatic fat is also higher in people with prediabetes and is associated with inflammation, beta cell apoptosis, and reduced insulin secretion. This is because fat infiltration to the pancreas triggers release of cytotoxic cytokines (e.g., fetuin-a or hepatokine), which could cause lipotoxic stress and auto-apoptosis of beta cells.
- Several lifestyle and pharmacologic interventions can lower ectopic fat. In a 2022 study, SGLT-2 inhibitor dapagliflozin was found to reduce A1c from 11% to 6.5%, hepatic fat from 15.2% to 10.1%, and pancreatic fat from 7.5% to 7.0% at four months. In a follow-up study, metformin and dapagliflozin combination therapy demonstrated reduction in beta cell’s toxic signaling. Dr. Misra also emphasized the importance of lifestyle change, which led to a 27% reduction in diabetes incidence at 15 years of follow up in the DPP trial. Beyond lifestyle changes, GLP-1 RAs are a potent agent for diabetes prevention. Acarbose, metformin, and vitamin D have also demonstrated efficacy. Notably, vitamin D is known to increase telomerase activity and leukocyte telomere length, which slows aging and improve glycemic health.
11. AI, wearables, and gut health for prediabetes prevention from Prof. Elaine Chow
The energy of Wednesday morning’s session on AI was electric as attendees flocked to the largest convention room. Prof. Elaine Chow (The Chinese University of Hong Kong, China) provided a comprehensive, inspirational session integrating AI, lifestyle interventions, and key opportunities for CGM to address prediabetes. Prof. Chow first provided a sobering statistic based on a 2022 study: among Chinese individuals, a 20-year-old person with prediabetes will go on to have diabetes for 33 years of life on average, equivalent to 52% of remaining life years. This emphasizes the essential need for diagnostic criteria to screen and prevent the development of prediabetes and its progression to diabetes. Thus far, the field has focused extensively on lifestyle interventions for the prevention of prediabetes progression, as intensive lifestyle intervention reduces the risk of progression to diabetes by 40-50%. In reality, Prof. Chow said that these programs remain challenging to implement effectively in the real world as they are resource-intensive and lack personalization, resulting in poor retention rates. As a result, she wants to focus on prediabetes prevention, integrating rapidly advancing AI, CGM, and newfound approaches to nutrition and lifestyle.
- CGM metrics may be used to unify prediabetes screening efforts around the world. Prof. Chow said that definitions of prediabetes based on fasting plasma glucose levels and OGTT scores demonstrate a level of discordance, with 2003 ADA and 2006 WHO guidelines both using different cutoffs to define prediabetes. The 2009 International Electrotechnical Commission and 2010 ADA guidelines include A1c values as a metric, with discordance between 5.7% and 6.0% as the lower end of prediabetes. Prof. Chow said that this lack of alignment has contributed to challenges in preventing prediabetes progression around the world, in addition to a need for the earlier detection of beta cell dysfunction beyond what these metrics offer.
- Prof. Chow said that CGM is an essential tool for prediabetes screening. CGM offers dynamic measurements of both fasting and postprandial glucose levels and is an important step for accessibility compared to OGTT as it can be self-administered. As prediabetes is such a broad, global phenomenon, the accessibility benefits of CGM are likely to compound to significantly change public health. In specific metrics, GMI has demonstrated poor correlation with A1c values in people without diabetes. However, glucose variability has been demonstrated as a signature of dysglycemia. A 2018 study found that severe variability correlates with abnormalities in insulin secretion and resistance. Prof. Chow believes that this CGM-enabled metric offers great promise for wide-scale prediabetes detection.
- CGM metrics are meaningful endpoints for prediabetes intervention trials. Prof. Chow described fascinating data from a 2025 study published in Nature Metabolism that showed improved glycemic management using a diet rich in fermentable carbohydrates alongside metformin. The RCT involving participants with impaired glucose tolerance found that a diet with moderate fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP) combined with metformin, compared to a low FODMAP diet with metformin, resulted in improved glycemic outcomes. These included lower postprandial glycemia as assessed by postprandial incremental area under the curve, a CGM metric, higher GLP-1 secretion, and higher Butyricimonas virosa abundance. This bacterium has been associated with beneficial effects on metabolic disorders. Improved OGTT scores were also demonstrated. Prof. Chow said that CGM metrics will continue to play a key role in global movements to address prediabetes.
- The use of AI with CGM data offers personalized lifestyle interventions. Prof. Chow said that AI offers the unique opportunity to process very large amounts of data, including multidimensional inputs from wearables, apps, and geography. AI can also be used to identify trends and correlations between diet, activity levels, and glucose responses, and to then interpret individual metabolic responses for more accurate dietary predictions. A 2025 AI-enabled study identified distinct patterns of insulin resistance based on different glycemic responses to potatoes, rice, and grapes. AI can therefore offer very individualized CGM analysis to improve analysis of insulin resistance and prediabetes progression.
- Prof. Chow said that an AI-enabled diabetes prevention program could further contribute to personalization. As an example, she said that an AI notification could encourage a user to avoid fast food when geolocation detects certain restaurants, or to likewise encourage a user to exercise when proximity to a gym is detected. The future of diabetes prevention will incorporate pharmacology, digital lifestyle interventions, and human-AI interactions.
12. Preliminary data presented by Prof. Elizabeth Davis shows early AID onboarding improves glycemic outcomes in Australian pediatric T1D
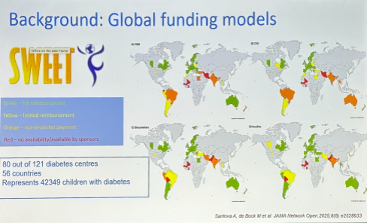
Prof. Elizabeth Davis (University of Western Australia) made a compelling case for dramatically earlier onboarding of AID in children with T1D, presenting an implementation model that has already helped bring AID to many across Western Australia. She opened by highlighting that while the just-published 2026 ADA Standards of Care now identifies AID as the preferred insulin-delivery method for T1D (Recommendation 7.25a), real-world access remains uneven globally. Data from the SWEET registry illustrate this gap: many countries lack reimbursement for, thereby limiting access to, both pumps and AID. In Australia specifically, CGM is subsidized for children, but insulin pumps are not, creating a significant barrier to guideline-aligned care.
- Prof. Davis reviewed evidence supporting early AID initiation, including studies showing strong outcomes when AID is started soon after diagnosis. However, she emphasized that these trials typically are conducted with far more resources than standard clinical settings and have not yet answered a key practical question: When should AID be initiated in routine care? She highlighted recent T1D Exchange data from 8,875 AID users offering some guidance on this, showing that early adoption (within six months) yielded better A1c outcomes than late adoption (after 13 months). With her equity lens clear throughout her session, Prof. Davis also highlighted data showing that early onboarding mitigated existing socioeconomic disparities, with children of the lowest SES quintile who started AID early achieved outcomes comparable to those from the highest socioeconomic strata.
- Motivated by this consistent and “indisputable” evidence base, Prof. Davis’ team designed a system-wide intervention to close the early-initiation gap. Serving 1,300 children in the statewide pediatric diabetes service, she said that they faced the reality that “we must learn to do things smarter” and launched an implementation study aimed at initiating AID within three months of diagnosis.
- To overcome key barriers including access, onboarding, and evaluation, the team redesigned their workflows and infrastructure. They partnered with industry to ensure availability of all four pumps cleared for use in Australia for participants (MiniMed 780G, t:slim X2, YpsoPump, and Omnipod 5), reallocated staff to match the new onboarding volume, and because early AID start shifted the educational burden to the beginning of care, they redeveloped teaching materials and incorporated new guidance on exercise with AID. Families were given time to choose their preferred system, reflecting the team’s commitment to patient choice.
- The team also confronted the practical realities of device-connected care in children, particularly smartphone use. Qualitative work with families revealed that many felt compelled to give their child a smartphone earlier than planned. Based on this feedback and internal discussions, they have decided that it is important to proactively counsel families about potential downsides of mobile phone use before starting AID, though how and when to have these conversations remain open questions.
- To date, 157 patients have participated in the study, with 93% now successfully onboarded and a median time to AID initiation of ~2.75 months. Prof. Davis noted that the process required substantial “change management” and that onboarding timelines improved over the course of the study, from a peak of around six months to onboarding for those recruited three months into the study to just over two months for those recruited most recently. While the precise optimal timing (within the first weeks vs. first few months) remains unclear, she showed A1c trajectories demonstrating that starting within the first six months offers clear advantages to short-term A1c compared to initiation at six to 12 months or later.
13. MiniMed 780G found to be cost effective for Japanese adults with T1D compared to MDI with CGM
Dr. Noriko Kodani (Japan Institute for Health Security) presented a cost-effectiveness analysis of MiniMed 780G versus MDI with CGM in Japanese adults with A1c >8.0%. The model drew on ADAPT RCT results, in which MiniMed 780G produced a 1.5% A1c reduction (from a baseline of 9.0%) at six months and 28% greater TIR than MDI with CGM (71% vs. 44%). Using the IQVIA Core Diabetes Model and a 55-year time horizon, reflecting the remaining lifespan of an average Japanese adult with T1D, the analysis adopted a Japanese health-care payer perspective, meaning it included only direct medical costs.
- Compared with MDI with CGM, MiniMed 780G’s reductions in long-term diabetes complications generated ¥2,857,914 (~$18,000) per-person savings over 55 years, partially offsetting higher treatment costs. MiniMed 780G use was associated with 2.87 incremental quality-adjusted life-expectancy (QALEs) gained and ¥12,670,490 (~$81,000) higher total direct costs versus MDI with CGM. The system was projected to provide substantial complication-free time, including over 10 more years free of proliferative retinopathy, nearly seven more years free of neuropathy, and over three more years free of congestive heart failure or myocardial infarction. This produced an incremental cost-effectiveness ratio (ICER) of ¥4,423,282 (~$28,000) per QALE-gained, below the commonly accepted ¥5,000,000 (~$32,000) willingness-to-pay threshold, indicating MiniMed 780G is cost-effective for Japanese adults with T1D not meeting glycemic targets. Sensitivity analyses showed the model was robust, with key drivers including: (i) the degree of reductions in fear of hypoglycemia; (ii) the treatment effect size, particularly for hypoglycemia event rates; and (iii) the underlying cost-effectiveness of the system.
- Dr. Kodani was optimistic that these findings will support reimbursement and broaden access to MiniMed 780G in Japan and the Asia-Pacific region, accelerating transitions from MDI. She also noted similar evidence from Singapore and upcoming data from Hong Kong (to be presented tomorrow) as signs of growing regional momentum for AID adoption.
14. Dr. Viswanathan Mohan on the potential for charitable organizations to change the course of T1D in low- and middle-income countries
In a moving afternoon presentation, Dr. Viswanathan Mohan (Dr. Mohan’s Diabetes Specialties Centre, Chennai, India) discussed therapeutic access, stigma, and the future of diabetes care in low- and middle-income nations (LMIC). In LMIC such as India, 70% of people pay for all of their diabetes treatment out of pocket, which presents extreme financial burden for millions of people. As of 2025, an estimated 800,000-941,000 people in India have T1D, however, this number may be a significant underestimation of true prevalence. Dr. Mohan said that India is likely the nation with the highest absolute numbers of the condition in the world. 100,000 of these people are children under 14 years of age. Despite this high prevalence, therapeutic resources remain limited. Dr. Mohan discussed the burden of diabetes in such conditions and delivered a compelling call to action.
- Financial challenges present very significant barriers to diabetes care in the region. Dr. Mohan said that diabetes therapies and technology are not covered by insurance in India, from CGM to even insulin. All treatment must be paid for out of pocket. At least 50% of PWD in India cannot afford diabetes management and need continual support. He discussed a disconnect between the framing of international consensus statements and life in India: while many leaders of diabetes care proclaim that everyone should have CGM, only 10% of PWD can afford CGM in India, and only 5% of patients can afford an insulin pump.
- In addition to financial challenges, access to technology is often delayed. Despite a desire for AID, only the MiniMed 780G system is approved in the nation, with about 2,000 users nationwide to date of the millions of PWD. Necessary accessories such as batteries for diabetes technology are also difficult to source for many patients.
- Aspects of culture also deeply impact diabetes care in India. Dr. Mohan said that awareness of T1D remains low among the general population – he described having many conversations with people who did not know that children without obesity could develop diabetes at all. Beyond this, a troubling trend that may be exacerbated by social media describes all medication as harmful, even encouraging patients with T1D to forgo insulin therapy. He described a devastating cycle of young patients receiving insulin for two to three weeks upon hospitalization for DKA, and later discontinuing insulin therapy until they are once again hospitalized. Out of desperation, many patients also turn to gurus, ingesting unmarked powders in hopes of a cure for diabetes, and instead becoming hospitalized for further complications.
- “The stigma is what’s killing people.” To combat misconception and stigma, Dr. Mohan discussed the importance of support groups and social media advocacy. He believes that forming community connections has had the greatest impact on his patients’ wellbeing. He has formed support groups and hosted motivational talks to facilitate discussion between young patients with diabetes and their families. He hopes to continue promoting acceptance of diabetes medications and positive attitudes towards treatment. He also hosts regular discussions on Facebook Live with the ability to reach patients in very rural areas.
- With limited government funding for diabetes care in India, Dr. Mohan believes that NGOs and charity organizations will be key to improving therapeutic access in India. Dr. Mohan is based in Tamil Nadu, the Indian state that continuously receives awards for superior governance, yet he has had difficulty in changing local policy regarding diabetes care. He described a series of meetings with government representatives in which he pushed for greater funding for diabetes care, yet decisions were made to fund other conditions such as sickle cell anemia. However, Dr. Mohan has worked with charities such as the Hinduja Foundation on the T1DI project to improve health metrics and overall wellbeing for PWD. The project has established a T1D registry, focusing on connecting with patients who may otherwise be “lost to follow up,” establishing support groups, and studying the development of complications in the area. By providing free treatment including free insulin, average BMI for patients who were malnourished when beginning the program has risen from 16.9 kg/m2 to 21.9 kg/m2 at year six on average, and average A1c values have improved from 9.9% to 8.7%.
- A dynamic discussion between Dr. Mohan, Prof. Tadej Battelino (University of Ljubljana, Slovenia), and Dr. Thomas Danne (Breakthrough T1D) weighed the benefits of once-weekly insulin versus AID in underserved communities. During Q&A, Dr. Danne acknowledged both the role of diabetes stigma in India and the high cost of diabetes education. He posited that once-weekly insulin dosing may limit stigma and provide substantial, cost-effective A1c benefits to millions of people who may not have the access to the education required for AID initiation. Dr. Mohan and Prof. Battelino concurred with the consideration of diabetes stigma, yet expressed their view that AID, especially a future fully closed-loop system, would also remove the need for expensive diabetes education and offer the greatest glycemic benefit. Prof. Battelino noted that high wealth inequality in India both contributes to the challenges of diabetes care in the nation and may offer opportunity. He hopes that wealthy individuals may be encouraged by the work of the T1DI project and organizations like Beyond Type One to make a difference to public health in the nation and the broader region.
15. *NEW* The state of diabetes technology in Japan: CGM growth and AID challenges
The use of diabetes technology in Japan was the central focus of this expert session. Dr. Takashi Murata (Tokai University Hachioji Hospital, Japan), a longtime advocate for technology in Japan’s diabetes ecosystem, provided a sweeping overview of the current landscape, framing the key challenges and opportunities which shape technology use in the country. The discussion explored recent progress in glucose monitoring alongside the structural, financial, and cultural barriers that continue to limit broader adoption of insulin pump-based therapies.
- Drawing on more than two decades of experience, Dr. Murata noted that the adoption of CGM has far outpaced that of insulin pumps in Japan. He attributed this gap to a combination of clinical inertia, persistent prejudice of pump therapy, and financial barriers. CGM penetration has now reached approximately 60% of the Japanese T1D population (that population totals ~110,000 people), according to the survey by IQVIA. By contrast, uptake remains low among people with T2D, reaching just 22% of those on intensive insulin therapy (~680,000 people) and 11% of those using basal insulin only (~420,000 people). While adoption is supported by Japan’s reimbursement structure, which limits co-pays for insulin users to 30% of the total CGM cost, coverage remains limited to those on insulin therapy. People with T2D who are not yet using insulin must pay 100% of the cost of the sensors.
- Turning to insulin pump therapy, Dr. Murata explained that adoption has increased steadily across the three systems currently available in Japan: (i) MiniMed 780G; (ii) Terumo’s Medisafe patch pump; and (iii) the TOP Corporation’s TOP-8200R. Among MiniMed users, the 780G is rapidly becoming the dominant system, although national use of any MiniMed system has been less than 15,000 people thus far in 2025. Dr. Murata said overall uptake of any system remains modest, highlighting perceptions among people with T1D that AID represents a significant financial burden. Monthly co-pays include both CGM costs and insulin pump rental fees – though these fees are waived for children, adolescents, and young adults. Lastly, Dr. Murata emphasized the continued impact of psychological burdens associated with wearing visible diabetes devices.
- To close, Dr. Murata pointed to a growing body of clinical and real-world evidence in Japan which supports the efficacy of diabetes technologies. These data include results from: (i) the REALJ study on Dexcom G6; (ii) the ESA-J study examining transitions from MiniMed 770G to 780G presented at the 68th Japan Diabetes Society meeting; and (iii) the ISCHIA study on the glycemic and quality of life benefits with Abbott’s FreeStyle Libre (1st generation) intermittently scanned CGM in T1D. Collectively, he projected, these findings are likely to further accelerate adoption in Japan.
--by Riya Chatterjee, Jeremy Alkire, Nour Khachemoune, Kat Moon, Monica Oxenreiter, and Kelly Close
[1]TZield is currently approved in eight countries including the US, UK, Canada, China, Israel, Saudi Arabia, UAE, and Kuwait.