Viking 1Q26 – VANQUISH‑1 and VANQUISH‑2 trials completed enrollment; oral VK2735 phase 2a data show up to 12% weight loss at Week 13; IND for amylin/calcitonin RA filed in 1Q26 –
Executive Highlights
- Viking Therapeutics reported its 1Q26 results on April 29, 2026, in a call led by CEO Dr. Brian Lian and CFO Mr. Greg Zante – see the press announcement and webcast.
- On subcutaneous VK2735 (a dual GLP-1/GIP RA), both the VANQUISH‑1 (obesity) and VANQUISH-2 (obesity and T2D) trials completed enrollment earlier this year. Baseline demographics for VANQUISH‑1 were presented at ECO 2026, and VANQUISH‑2 baseline demographics will be presented at EASD later this year. Management noted the smooth adoption of the auto‑injector device.
- On oral VK2735, a dual GLP-1/GIP RA, Viking presented full phase 2a VENTURE‑Oral results, which showed early, progressive weight loss up to 12% at Week 13 without plateauing. Moreover, up to 97% of treated participants (vs. 10% in the placebo group) achieved ≥5% weight loss, and up to 80% (vs. 5%) achieved ≥10%. The safety and tolerability profile was favorable, with 98% of TEAEs being mild or moderate and diminishing over time. The phase 3 program remains on track to initiate in 4Q26, following a supportive end‑of‑phase‑2 meeting with the FDA.
- The phase 1 VK2735 maintenance study completed enrollment in 1Q26. Viking added four more cohorts for subcutaneous dosing to study more dosing options (now including 10 mg, 15 mg, 17.5 mg, 20 mg, and 22.5 mg monthly, as well as 5 mg, 7.5 mg, and 10 mg every two weeks). Oral dosing was deferred to a second part of the study. Management emphasized that the study will inform the design of VANQUISH extension trials. Results for subcutaneous and oral dosing are expected in 3Q26 and 1H27, respectively.
- On VK3019, a dual amylin and calcitonin RA, Viking filed an IND in 1Q26 and expects to initiate a phase 1 trial in 2Q26. During Q&A, management said VK3019 has a differentiated mechanism and may especially benefit patients unable to tolerate GLP‑1 RAs or those with lower BMI.
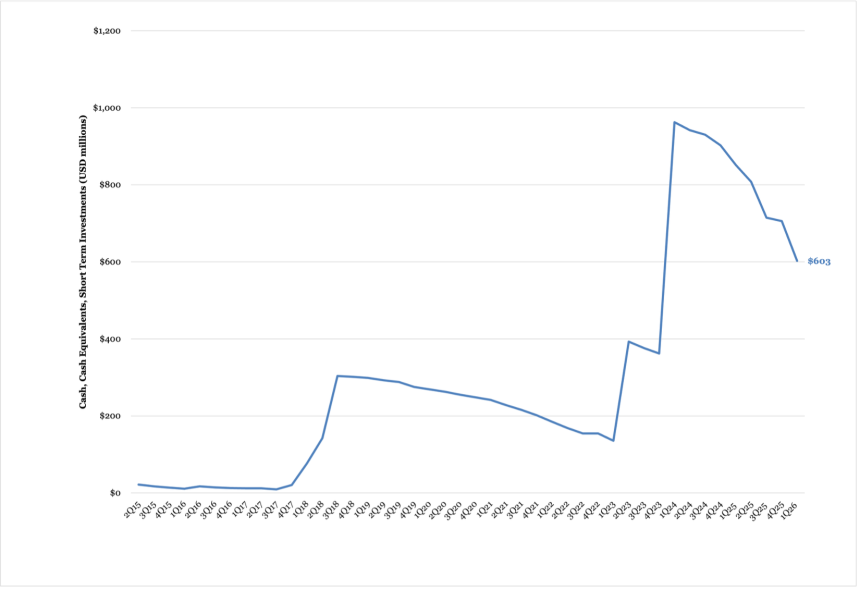
- Viking ended 1Q26 with approximately $600 million in cash and cash equivalents, down 29% from 1Q25 and down 15% sequentially. R&D expenses were $115 million, up more than 2x from 1Q25 and down 25% sequentially. Management stated the company has sufficient capital to support its three major ongoing trials.
Table of Contents
-
Pipeline Highlights
- 1. VANQUISH‑1 and VANQUISH‑2 trials completed enrollment for subcutaneous VK2735 in obesity and T2D
- 2. VENTURE‑Oral phase 2a results show up to 12% weight loss at Week 13; phase 3 initiation on track for 4Q26
- 3. Phase 1 maintenance study completes enrollment; trial includes more dosage options for subcutaneous VK2735
- 4. IND application filed for VK3019 amylin/calcitonin RA; initiation of phase 1 trial expected in 2Q26
- 5. Viking discontinues internal development of VK2809 for MASH; expressed interest in out-licensing at JPM 2026
- Financial Highlights
- Analyst Q&A
- Close Concerns’ Questions
Pipeline Highlights
1. VANQUISH‑1 and VANQUISH‑2 trials completed enrollment for subcutaneous VK2735 in obesity and T2D
Viking reported continued development of subcutaneous VK2735 (dual GLP-1/GIP RA) in 1Q26. On the call, management emphasized that the momentum established in 2025 for VK2735 has carried directly into early 2026. The phase 3 VANQUISH program has now fully completed enrollment, including the VANQUISH-1 trial for obesity and the VANQUISH-2 trial for obesity and T2D. Viking also highlighted the successful introduction of its auto‑injector device into the VANQUISH program.
- The 78-week VANQUISH‑1 trial (n=4,661) is investigating weekly doses of VK2735 at 7.5 mg, 12.5 mg, or 17.5 mg in adults with obesity. The company completed enrollment in 4Q25, and the trial is expected to be completed in 2027.
- Baseline demographics for the study were presented at ECO 2026. Sites in the US, EU, and the UK followed a diversity action plan to enroll a diverse population across race, ethnicity, gender, age, and BMI. Participants were on average 50 years old and 65% female. By race and ethnicity, most participants were white (74%), followed by Hispanic (23%) and Black (19%). Clinically, the average BMI was 38 kg/m2, 53% had prediabetes, and 15% previously used GLP-1 RAs.
- The 78-week VANQUISH‑2 trial (n=1,000) is investigating VK2735 (7.5 mg, 12.5 mg, or 17.5 mg) in adults with obesity and T2D. Enrollment was completed in 1Q26. On the call, management stated that baseline demographics for the trial will be presented at EASD 2026, and full results are expected in 2027.
In 1Q26, results from the phase 2 VENTURE trial (n-4,650), investigating injectable VK2375 for obesity with one weight-related comorbidity, excluding diabetes, were published in Obesity. On the call, management highlighted that participants achieved up to 14.7% mean weight loss after 13 weeks with no signs of plateau. The safety and tolerability profile showed that most adverse events were mild or moderate and resolved quickly.
2. VENTURE‑Oral phase 2a results show up to 12% weight loss at Week 13; phase 3 initiation on track for 4Q26
Viking presented results from the phase 2a VENTURE‑Oral dosing trial (n=280) on its oral VK2735 program. Oral VK2735 conferred early and progressive weight loss beginning at Week 1 and continuing through Week 13 without plateau. The highest dose achieved a mean reduction in body weight of 12.2% at Week 13. Up to 97% of treated participants (vs. 10% with placebo) achieved ≥5% weight loss, and up to 80% (vs. 5%) achieved ≥10% weight loss. A stepwise titration scheme by 30 mg increments was used to escalate to higher doses. The safety and tolerability profile was favorable, with 98% of TEAEs being mild or moderate and diminishing over time. On the call, management reiterated that there was no meaningful difference in GI‑related adverse events between participants receiving VK2735 and those on placebo.
- During Q&A, management said that the recent end‑of‑phase‑2 meeting confirmed its approach to the phase 3 program. The FDA did not request substantive changes; remaining work will focus primarily on fine‑tuning the manufacturing steps and preparing manufacturing capacity to produce oral VK2735 on a larger scale. The phase 3 oral program remains on track to initiate in 4Q26.
3. Phase 1 maintenance study completes enrollment; trial includes more dosage options for subcutaneous VK2735
Viking also provided an update on its phase 1 maintenance‑dosing study, which is designed to evaluate monthly, every‑other‑week, and weekly regimens to support long‑term weight management and inform the 52‑week extension phases of the VANQUISH trials. On the call, management said that the unique potency and pharmacokinetic profile of VK2735 may enable less frequent dosing than currently available agents. To ensure robust dose selection, Viking expanded the subcutaneous portion of the study from four to eight cohorts. The doses now include 10 mg (new), 15 mg (new), 17.5 mg, 20 mg, and 22.5 mg monthly, as well as 5 mg (new), 7.5 mg, and 10 mg (new) every two weeks. The company is also prioritizing the subcutaneous program ahead of the oral program, given its more advanced stage of development. The company completed enrollment for the study in 1Q26. The results for subcutaneous and oral VK2735 are expected in 3Q26 and 1H27, respectively.
4. IND application filed for VK3019 amylin/calcitonin RA; initiation of phase 1 trial expected in 2Q26
In 1Q26, Viking filed an Investigational New Drug (IND) application for VK3019, its novel amylin and calcitonin receptor agonist. Pending FDA clearance, the phase 1 trial is expected to initiate in 2Q26. The dual activation of the amylin and calcitonin receptors may offer a differentiated option for patients who are not candidates for GLP‑1 RA-based therapies, whether due to tolerability challenges or other clinical considerations. During Q&A, management also said VK3019 could benefit patients with lower BMI ranges (32-35 kg/m2). The initial program will include single ascending dose (SAD) and 28‑day multiple ascending dose (MAD) studies. Viking is also considering combination studies with VK2735.
5. Viking discontinues internal development of VK2809 for MASH; expressed interest in out-licensing at JPM 2026
Viking did not provide any updates on VK2809 (THR-ß agonist for MASH) during the call. At JPM 2026, Viking said that it does not intend to advance the candidate internally. VK2809 is available for out‑licensing, and Dr. Lian stated that there is external interest in the asset.
Financial Highlights
1. Viking ends 1Q26 with nearly $600 million in cash, down 29% from 1Q25 and down 15% sequentially
Viking ended 1Q26 with $603 million in cash and cash equivalents, down 29% from 1Q25 and down 15% sequentially. R&D expenses totaled $115 million, up more than 2x from $41 million in 1Q25, and down 25% sequentially from $154 million. The increase in R&D spend from 1Q25 was driven by clinical study execution, manufacturing for drug candidates, consultants, salaries and benefits, and preclinical studies, partially offset by lower stock‑based compensation. Viking reported a net loss of $158 million (vs. $46 million in 1Q25) with the increase attributable to higher R&D expenses, partially offset by lower G&A expenses.
Viking Cash and Cash Equivalents (2Q15-1Q26)
Source: Close Concerns’ Knowledgebase
Analyst Q&A
On injectable VK2735
Q (Nat Charoensook, Leerink Partners): Now that both VANQUISH-1 and VANQUISH-2 are fully enrolled, what baseline characteristics are you seeing, and are they consistent with your expectations? Are you seeing any differences in enthusiasm, screen failure rates, or retention between VANQUISH-1 and VANQUISH-2?
A (Dr. Brian Lian, President and CEO): So we're presenting the baseline demographics at two conferences this year. At the European Congress on Obesity, we have the VANQUISH 1 demographics. At EASD, we'll have VANQUISH 2 demographics. So I'll defer to those conferences for the demographic disclosures. But I don't think anything's kind of out of the ordinary with respect to the population relative to other studies. They're kind of down the middle of the fairway.
Q (Nat Charoensook, Leerink Partners): How should investors think about the expected weight loss in type 2 diabetes versus non-diabetic patients with obesity?
A (Dr. Lian): Hard to know. It's up to the individual to make that estimation. Generally, type 2 patients are a little bit more resistant to weight loss than non-type 2 patients. So I don't think that would be surprising to see in the weight loss data from these studies. I think we would probably see a more robust effect in the straight obesity and maybe a little bit lower efficacy in people with type 2 diabetes, just like everybody else has shown.
On oral VK2735
Q (Nat Charoensook, Leerink Partners): On the phase 3 initiation of oral VK2735, which is now expected in 4Q26, what changed versus prior expectation for 3Q26?
A (Dr. Lian): Nothing really changed. You know, we're moving incredibly fast and scaling up dramatically here. As you do that, you learn a lot about the process and efficiencies. Making 100 tablets is different than making a million tablets. So, you learn a little bit more about engineering processes and et cetera, which get optimized along the way, just to ensure you get the most efficient and cost-effective methods in place. All of that takes some time.
We feel good about the supply chain and the capacity and efficiencies, and where we're at in the development cycle. We look forward to initiating as early as possible in the fourth quarter.
Q (Jay Olson, Oppenheimer): Just to follow up on some of the factors that informed your decision to initiate the phase 3 oral study in the fourth quarter, did you want to see the results of the phase 1 maintenance study in the third quarter before starting the phase 3 oral study in the fourth quarter, or were there other factors involved?
A (Dr. Lian): For the oral study, no, we weren't planning to wait for the data. They're just independent factors. The maintenance data and the initiation of the oral studies, they were not related.
Q (Hardik Parikh, JPMorgan): I know in the past you've talked about working on reducing the number of tablets you'd have to take at a dose. I was wondering if you have any updates there on where you are in that progress?
You also mentioned the launch of another oral peptide. What are our takeaways from that launch in terms of just what it says about the overall market and then the role of oral peptides in general?
A (Dr. Lian): We would want to have no more than two tablets as the higher dose option. Lower doses would be one tablet. In the phase 2 trial, everybody took four tablets, and the feedback we received was that's just people weren't really satisfied with that: no more than two tablets.
We generally don't comment too much about competitive dynamics, but the launch of the current oral peptide has been very robust, and it supports this real, high interest in the oral modality. Interestingly, it's represented more as a market expansion than any sort of cannibalization of the injectable market. So it's been a very, very impressive launch.
A (Mr. Neil Aubuchon, Chief Commercial Officer): What we're seeing is that this is growing the market, so it just goes to show that there are significant opportunities still. It's too early to comment on the latest launch. I think it's just several weeks in, so we wouldn't comment on it anyway, but it's awfully early. It's going to be quite a competitive dynamic between these two companies, as you would expect.
The only thing I would also just remind you of is that both the orals on the market are GLP-1s, where ours is going to be a dual agonist oral. We expect to have the first dual agonist oral on the market, and I don't know if that's fully appreciated by folks in the ecosystem. We're pretty excited about the opportunity for our oral.
On the maintenance study
Q (Steven Seedhouse, Cantor Fitzgerald): First is just on the change from four to eight Sub-q maintenance cohorts in the ongoing study. I was hoping you could just elaborate on what doses and intervals the new eight cohorts are testing?
A (Dr. Lian): On the maintenance study, just given the importance of this study for implementation into the VANQUISH extensions, we decided to extend the cohorts and then defer the oral dosing to a second part. We'll retain those first four cohorts that we had earlier, which were 22.5 milligrams, 20 milligrams, 17.5 milligrams monthly, as well as 7.5 milligrams every other week. But we've added 15 milligrams monthly, 10 milligrams monthly, 10 milligrams every other week, and 5 milligrams every other week. We got a nice range of every other week and a broader range of monthly doses.
Q (Ryan Deschner, Raymond James): What were the key factors that went into selecting the 19 weeks as the Sub-q induction time period for the maintenance study?
A (Dr. Lian): It was really driven by the time to titrate to the 22.5 milligram dose. That was the highest dose, and we wanted to people – first get people up there and then keep them there for I think it's a three-week treatment time there and then transition everybody to the maintenance at the same time point. So that was sort of the rate-limiting factor, the time it took to titrate to the highest dose.
Q (Ryan Deschner, Raymond James): Just wanted to kind of feel out what the odds might be of. Would you add additional oral cohorts, potentially later on, in the maintenance study? Is that something that could be on the table?
A (Dr. Lian): We will be adding more cohorts to the oral portion of the study. We'll probably look at a few more doses as well as potentially alternative regimens.
Q (Annabel Samimy, Stifel): Obviously, with the addition of new cohorts, your maintenance study seems to have gotten a little bit more involved. And I guess I'm trying to figure out what the various possibilities are for that extension trial. Are you going to select one of these cohorts? Are you going to give the option for multiple cohorts going into the extension – the extension study? What is the purpose of having all these eight additional cohorts? I'm just trying to understand exactly what you intend to do with these cohorts going forward. Is it just for information purposes and their selection in the extension study?
Taking it forward, are you going to develop it any further past this extension study for possible inclusion in the label? Or is it just developing a wealth of data for physicians to draw on and sort of use the data as an art, rather than a very prescriptive formula for maintenance for these patients?
A (Dr. Lian): With the second question, at a minimum, we would hope to be able to publish the extension data from the VANQUISH extension utilizing some of these maintenance cohorts. So that would provide valuable information in the form of publications to clinicians and patients.
What do we expect to learn from the maintenance cohorts? Really, the best maintenance strategy to employ is every other week dosing, preferably. It seems like a lot of people are doing that now, just out in the real world. Is monthly going to be the better strategy, and if so, what dose?
We had only three-monthly doses and one every other week dose in the prior study. We thought to better inform the cohorts that would go into the extension of VANQUISH, and there will be more than one dosing arm in the extension studies for maintenance in VANQUISH. It just made sense to expand the subcutaneous cohorts and then defer the oral, since we weren't as time sensitive on the oral to a separate part of the study.
Q (Biren Amin, Piper Sandler): On the VANQUISH extension, when will the maintenance doses be introduced for the Sub-q? Will that be at week 78 or week 84? How long will you be evaluating those Sub-q doses?
Just a follow-on question. For the VANQUISH dose cohorts, in the treatment phase of 7.5 milligrams and 12.5 milligrams weekly, how do you think about the transition of those patients to maintenance doses, given the maintenance trial is evaluating 15 milligrams weekly and higher in that 19-week induction period?
A (Dr. Lian): For the first question, we'll transition people at 78 weeks. It won't be a sort of washout or anything like that out to 84 weeks. We plan to run the extension for 52 weeks. As far as the transition from 17.5 milligrams to whatever the maintenance dose might be. If you were to go from 17.5 milligrams to a higher 22.5 milligrams dose or something like that, there could be some incremental adverse events. That's not really what you see after a prolonged exposure like this, but those would all be things that we'll find out during the trial.
Q (Blake Gitler, BTIG): In regard to the Sub-q maintenance data coming in the third quarter, what does good look like to you guys, and are you comfortable reporting a modest regain? If so, is there a bar to the standard that qualifies as weight to retention?
A (Dr. Lian): I guess the way we look at it is best case scenario is that you see a continuation of weight loss when you transition to the maintenance regimen. It's just the slope might change a little bit. I think our base case, which is a great outcome, is just the real maintenance, you know. Less than really a few percent either way, up or down. And then the worst case would be you see a sharp rebound. So, those are kind of the general scenarios that we're looking at. And I think flatlining or relatively flat after the transition would be a really great outcome for us.
On VK3019, an amylin/calcitonin receptor agonist
Q (Jay Olson, Oppenheimer): On VK3019, can you just talk about your plans for the Phase 1 amylin program, or are you thinking about induction, maintenance, or combination? I guess what's kind of on the table there for your amylin program?
A (Dr. Lian): With the VK3019 molecule, the first study will be before you think about combos and that sort of thing. First, you want to understand the compound's basic properties. And so the first two studies will be a SAD study and then a MAD study.
We are initiating combo talks with the VK2735 compound. Longer term, I think that's a really promising area to look at. But the initial studies will just be single-agent. And it'd be kind of the playbook we used for VK2735 with a SAD followed by a 28-day MAD. Nice opportunity with this mechanism to potentially target people who are a little lower BMI 32 to 34, 35, or people who can't, maybe can't tolerate a GLP-1, and want to try something different. Both are very significant opportunities for the amylin program.
On spending
Q (Steven Seedhouse, Cantor Fitzgerald): If you wouldn't mind just quickly commenting on R&D, just for our modeling, maybe connecting the dots between the like $160 million-ish or so net loss versus about $100 million in net cash change. And I think folks specifically were expecting R&D to come down a bit this quarter from some one-time Phase 3 startup costs. So, I would just hope that you could clarify if you're expecting R&D costs to come down next quarter or if this is maybe the new run rate?
A (Mr. Greg Zante, CFO): On the OpEx and cash, for one, the disconnect on that a bit is really timing, a function of timing. There were just higher expenses and cash usage, and that stuff evens out over time. But looking ahead to this next quarter, I think our cash usage and expenses will be around where we were in quarter one, maybe a bit lower. But toward the second-half of this year, I would expect things to taper down a little bit.
The overall usage is still in line with our projections from our last call. And we would anticipate having cash into 2028 and through the catalysts we've talked about, including the oral Phase 3 data points. We remain funded as we expected, but we probably used a little bit more in the first quarter than I anticipated, but we are on track.
Close Concerns’ Questions
- What are the remaining items for initiating the oral VK2735 phase 3 program in 4Q26 following the supportive end‑of‑phase‑2 meeting?
- How does Viking plan to demonstrate the real‑world commercial advantage of a oral VK2735 over GLP‑1 RA oral formulations?
- What does Viking look for in potential partners for developing VK2809 for MASH? What is the expected timing for an out‑licensing deal?
--by Kayla Mathieu, Kat Moon, Esther Min, and Kelly Close