Structure Therapeutics announces positive topline results from phase 2 ACCESS II trial of oral small molecule GLP-1 RA aleniglipron –
Aleniglipron demonstrates up to 16.3% weight loss at Week 44; phase 3 program expected in 2H26
South San Francisco-based Structure Therapeutics announced March 16, 2026 topline results from the phase 2 ACCESS II trial (n=82) of higher doses of its once-daily oral small molecule GLP-1 RA, aleniglipron, for people with obesity and at least one weight-related comorbidity (press release, webcast, presentation). The therapy delivered the highest efficacy reported to date for an oral GLP‑1 RA, with weight loss outcomes approaching injectable‑class performance. Aleniglipron continued to demonstrate a tolerability profile that is consistent with the GLP-1 RA class and a compelling safety profile with no off-target events. The company has an end-of-phase 2 meeting with the FDA scheduled for 2Q26 and plans to initiate phase 3 trials in 2H26.
During Q&A, management said full results from the ACCESS II trial will be presented at an upcoming medical conference. Dr. Raymond Stevens and Dr. Blai Coll also discussed insights on the upcoming phase 3 trial and two ongoing complementary trials: (i) ACCESS-OLE (n=41); and (ii) the phase 2 body composition trial (n=71). In all, there were nearly 15 questions, from a range of investors curious about short and long-term milestones. The team will be back shortly to discuss the detail and nuances that we noticed stemming from the dozen-plus queries.
Table of Contents
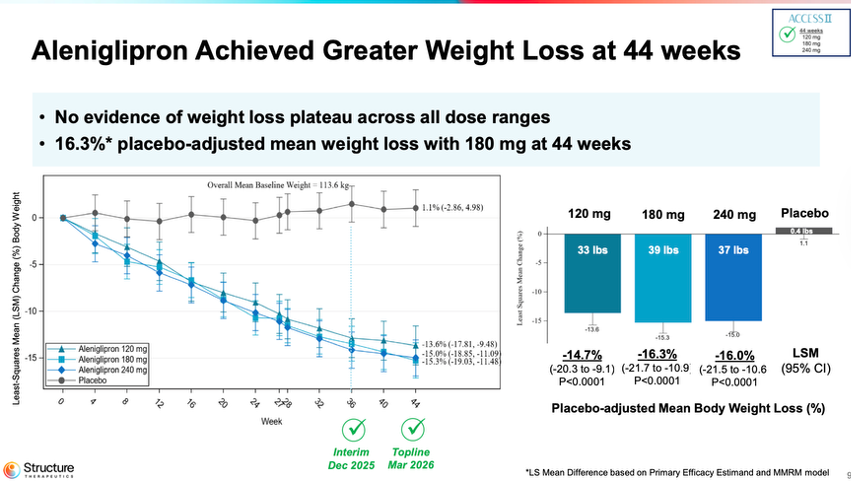
ACCESS II study - At Week 44, aleniglipron conferred weight loss up to 16.3% pbo-adjusted with no plateau
At 44 weeks, aleniglipron achieved placebo-adjusted mean weight loss of 14.7% (33 lbs) at 120 mg, 16.3% (39 lbs) at 180 mg, and 16.0% (37 lbs) at 240 mg, compared to a 1.1% increase on placebo. There was no evidence of a weight loss plateau.
Tolerability remained consistent with the GLP-1 RA class. Among participants who reached ≥120 mg between Weeks 28-44, one AE-related discontinuation (3.7%) occurred. In addition, across more than 625 exposed participants, aleniglipron has shown no drug-induced liver injury, persistent liver enzyme elevations, or cardiovascular side effects.
During Q&A, management shared insights on the upcoming phase 3 trial, which will start with the 2.5 mg dose and include the four-week titration steps. The final doses for the phase 3 trial are yet to be determined.
Source: Structure Therapeutics’ presentation slides
Results build on findings from the phase 2 ACCESS trial
These findings build on the December 2025 results from the 36-week phase 2b ACCESS trial, in which aleniglipron achieved a placebo-adjusted mean weight loss of 11.3% (~27.3 lbs; 12.4 kg) at the 120 mg dose, with a roughly 10.4% treatment discontinuation rate due to adverse events. In the then exploratory phase 2 ACCESS II trial (n=82), participants receiving the 120 mg dose achieved a mean percent body weight reduction of 13.1%, while those on 180 mg and 240 mg achieved 13.3% and 14.2% reductions, respectively.
Aleniglipron continues to be investigated in the ACCESS OLE and body composition trials
Structure Therapeutics also shared results of two ongoing complementary studies: (i) the phase 3 ACCESS-OLE (n=41); and (ii) the phase 2 body composition trial (n=71).
In the open-label extension (OLE) study, participants on aleniglipron continued to demonstrate weight loss through 56 weeks. Participants previously treated with aleniglipron in the ACCESS trial achieved weight loss up to 16.2% (40.5 lbs) at 120 mg with no signs of plateau. AE‑related discontinuation rates of 2% were seen across all arms in the OLE.
Participants who transitioned from placebo and initiated treatment at the lower 2.5 mg starting dose experienced favorable tolerability, further validating the tolerability improvement seen with starting low and titrating slowly. The study is expected to complete in August 2026.
The phase 2 body composition trial evaluates how aleniglipron affects body composition in people with obesity (BMI ≥30 kg/m2). Structure Therapeutics reported that aleniglipron conferred 6.8% weight loss at 20 weeks, and AE‑related discontinuations were 3.4%. The study is expected to complete in October 2026. During Q&A, management said data on lean muscle loss vs. fat loss in patients is not yet available. However, the company expects to report results at the end of the study.
Analyst Q&A
Q (Yasmeen Rahimi, Piper Sandler): Clearly the strategy of starting low and going slow seems to be working really well and that you're not reaching a plateau. Could help us understand if you can do any modeling to figure out orfoglipron's differentiated weight plateauing effect? In other words, can you model and see, is it 1.5 years that you reach plateau? Is it 2 years? Is there any evidence? And then also, is there any mechanistic rationale for the lack of plateauing effect?
Dr. Blai Coll, CMO: Yes. Thanks for your question. So absolutely, that's what we're doing right now. It's using that 44-week ACCESS II and all the way to 56 in the ACCESS OLE to inform the model that will help us predict the level of efficacy. We don't see a plateauing effect as of yet to week 44 and 56, and this is a differentiated element, and we're very pleased with the results. Potential mechanisms of action there behind that clinical observation is that, as you know, we have seen proportional exposure all the way to 240 milligrams of aleniglipron, and that can be behind that additional body weight reduction that we're seeing beyond 36 weeks. Thanks for the question. Hopefully, I covered everything that you were asking.
Q (Evan Seigerman, BMO Capital Markets Equity Research): I wanted to touch on the difference between 180 milligram and 240-milligram doses clearly both performing the same. Do you have a hypothesis as to what's happening here? Are we getting pharmacological saturation? Is there something else nuanced in the data?
Dr. Coll: Thanks Evan for the question. This is Blai again. I'll take the question. So yes, as you well pointed out, we don't see differences in efficacy between 180 mg and 240 mg. The results in efficacy and body weight reduction are comparable at the end of the 44 weeks. Interestingly, though, what we're seeing is that the pattern of efficacy is very similar between 180 mg and 240 mg. But then tolerability-wise, which is always the things that we need to couple with the efficacy, the 180 milligrams behaves very, very similar to what we've seen for 120 mg. At the end of the day, I think the most important conclusion of ACCESS II is that we're getting available -- highly available data to inform the design of the phase 3 to design the modeling and that ultimately will result in the identification for the top dose for phase 3.
Q (Seamus Fernandez, Guggenheim Securities): Actually, Ray, I wanted to talk a little bit about the scalability of the product. I know this is something that we've talked about before, not really finding a lot to critique in the data. So I wanted to provide a better understanding of how you've approached the scalability to reach 100 million patients or more. I know that comes down to the design of the molecule, but there's a lot that goes into this. Could you the help investors think about what it takes to get to 100 million patients in this market?
Dr. Raymond Stevens, CEO & Director: Thank you, Seamus, for the question. We were in the fortunate position. GLP-1 receptor is very well characterized. The peptides, we sit on the shoulders of giants, as they say, with all the characterization of the peptides over the years. We were in the fortunate position to be able to really focus on design early on at the very beginning as we're thinking about design principles, not just efficacy, not just safety, not just tolerability, but also at the very beginning, we thought about manufacturing.
So as an example, we felt it was important for manufacturing not to have any chiral centers that require chiral separation, just as one representative example. This is an important step in the manufacturing. So we were able to remove any of those chiral centers that would require chiral separation. That's one example. Again, as I highlighted in my closing remarks, the chemist and our manufacturing team, they've just done a phenomenal job at the synthetic route at optimizing based on the molecule itself, the entire process to really allow us to be able to scale this to the global needs that are required.
Q (David Risinger, Leerink Partners): Could you please provide some color on how you're thinking about the go-forward start low and go slow strategy for Phase III? Specifically, what period of time do you envision titrating patients from 2.5 mg at day 0 to 180 milligrams in phase 3?
Dr. Coll: Yes. So good question. Thanks, Dave. So the plan is based on the data that we've released today and back in December, as we've communicated, starting at 2.5 milligrams is the most optimized starting dose for aleniglipron. We plan to keep the 4-week titration steps. And as released today, we're not planning to titrate and escalate the dose every time we titrate more than 2.5 fold. This is the combination of starting at a low dose at 2.5 mg and going slowly to reach the target doses. The final doses for phase 3 are still to be determined. This is currently ongoing work at Structure Therapeutics with the data we just released plus the modeling that we're actively pursuing.
Two additional comments there is that it's important to see not only that we're optimizing the tolerability, we're reducing significantly the number of AEs leading to discontinuation with these current titration steps, but we're also seeing early signs of body weight reduction. And this is the 2 factors that we're laser-focused on. We know contacting with clinical investigators and data from the market research that it's, of course, it's very, very important to optimize tolerability while you're also seeing effects in terms of body weight reduction. And this is what the data is pointing out right now.
Dr. Stevens: And Dave, you and I have had this conversation before about the titration schedule and how long a titration schedule should be. Based on our research, what we found is what's most important is that patients will get bored if they do not see weight loss after 4 weeks or 8 weeks. And so that's something that's really important to consider. What I really like about the data that we're showing today and back to the December data is that we are seeing weight loss at the starting dose of 2.5 milligrams. And even better, what I like is we're seeing this very nice smooth linear weight loss from the very beginning, starting at 2.5 mg all the way out to 30 milligrams to date. And we see similar curves with the longer studies to 44 weeks and 56 weeks.
So we think that's really important. It's better than these exponential weight losses that we see where people lose half of their weight is due to water loss and it's very rapid. So we really like the profile that we have, and we believe that the data that we've shown patients will lose weight at the very beginning, starting at 2.5 mg and that will keep them very engaged as they progress through going on aleniglipron.
Q (Terence Flynn, Morgan Stanley): Any thoughts on where you might present the full ACCESS data? Is it likely at ADA? Or is there another venue that you guys are considering? I would love your latest thoughts, Ray, on potential partnership discussions and what that might look like?
Dr. Coll: Ray, do you want to take the first one, and I'll take the second.
Dr. Stevens: Sure. Thanks, Terence. Yes, I think medical conferences later in the year, and you're mentioning ADA, there's also EASD and Obesity Week in the fall. We have a lot of exciting data and we'll be informing as appropriately. But yes, that's a reasonable assumption.
Dr. Coll: Terence, on your second question, in regards to strategics, so we continue to interact with strategics.
The data that we demonstrated today and back in December shows very strong best-in-class efficacy for aleniglipron. We'll continue those dialogues. We also have the Amylin Program that will start having data readouts in the second half of this year. So we'll keep you updated as that progresses.
Q (Prakhar Agrawal, Cantor Fitzgerald): It seems like the second half update will be just that. So maybe if you could talk about what will be disclosed at this update? How are you thinking about the MAD readout timing? Where are you with the chronic stock studies with the oral amylin? Clarification of the liver enzyme, there were ALT, AST elevations of 5x upper limit of normal, a few cases, but if you can clarify whether these were transient and whether patients have discontinued the drug?
Dr. Coll: Sure. Thanks, Prakhar. In regards to the oral amylin, yes, we're guiding to second half results from the single ascending dose. Currently, designing multiple ascending dose, the multiple ascending dose design will largely depend on the findings on the single ascending dose.
So more to come on that end. Highly scrutinized program, of course, very excited and we're very excited about the progress of these programs so far. So more to come on that end. In terms of the ALT, AST elevations, we're not seeing a different pattern compared to what we released in December.
So all the fluctuations that participants continue on study drug and the ALT, AST come back to normality. So very, very pleased to see that there's no events of DILI that the participants that experience any of those despite not stopping study drug or discontinuing drug or reducing the dose the ALT, AST levels got back to normality.
Dr. Stevens: And Prakhar, just as a reminder, back at the beginning of the year, we did update our corporate deck on the Amlin Program, and we did share the schema of the titration scheme. So that continues to be work in progress. We are right on schedule. As they say, with Phase I, no news is good news in that study.
Q (Samantha Semenkow, Citigroup): If you take a look forward, how are you thinking about what a competitive profile would look like from like an efficacy and tolerability profile for oral amylin? Could you give some thoughts around both the monotherapy and potential combination view for that asset?
Dr. Stevens: Yes. Let me give Blai a little bit of a break here. And then Blai you can add on to anything that I missed. So first of all, Sam, and Prakhar, thank you guys for asking about amylin, even though this call was for aleniglipron. We know there's a lot of interest in amylin these days. The way that we're sort of looking at this is we still believe very much in the amylin mechanism for a number of different reasons. one, the safety profile and tolerability is very strong from the data that we've seen to date. And so that, we think, is really important. Second, there is a subset of the population that do not respond to GLP-1s. And so we feel for those individuals, we think amylin is a potential option for them.
And then lastly, we have presented previously at international medical conferences, the combination of our oral GLP-1 together with our oral amylin, and we see this very synergistic effect between the two, so for additional weight loss if one wants to go to that level. So I think in terms of tolerability advantages, we continue to be intrigued by the selective weight loss, which we think is also an important area. There's a number of reasons why we remain excited about amylin and in the combinations. Blai, anything else you want to add to that?
Dr. Coll: No. Just one comment, Sam. I think good question on how we're developing the amylin. We'll develop as monotherapy for now, but also with the intent to combine, as we've said in the opening remarks, we have the ability to have that combination of different mechanisms of action that, as Ray alluded to, can potentially be synergistic. And that's the plan that we have for the amylin program.
Q (Jonathan Wolleben, Citizens JMP Securities): Could you talk about the differential properties between aleniglipron and orforglipron and the results you're seeing here with the clinical profiles, just to better understand what's going on mechanistically here?
Dr. Stevens: Yes. I'll start at sort of a very high level. We see 4 different reasons for differentiation. Clearly, efficacy stands out. This is the most efficacious oral GLP-1 out there from the data that we've shown now. Second, in terms of off-target safety, very pleased with the profile. We think that in terms of tolerability, similar in regards to tolerability. Third, manufacturing, something that was asked earlier on, really, really proud and pleased with the manufacturing that we've been able to accomplish for aleniglipron. That is a distinct advantage. The lower cost of goods and scalability is quite significant. Then fourth, combinability. The differentiation with combinability, we -- not only did we design this molecule to be efficacious, safe, manufacturing at scale that's needed, lower cost of goods, but we also designed it so it was very combinable with other molecules, whether it's other incretins and weight loss or non-incretin molecules as we look forward in life cycle management. So those are the 4 different reasons why we believe it's highly differentiated.
Q (Roger Song Jefferies): We already see the 2.5 mg starting dose all the way to 20 weeks for the tolerability. Just curious about the expectation about longer follow-up. Do we expect to see some late incidence of the GI AE, particularly from those new patients versus the existing patient will change the profile?
On the phase 3 design, knowing you will have diabetes and then potentially the SWITCH maintenance data coming up in the second half. I understand it's not gating factor for the phase 3 start, but how those data will inform the Phase III and how much you will change the phase III with those data?
Dr. Coll: Thanks, Roger. I'll take the question. So on start of 2.5 and up to 20 weeks, yes, we will see more incident events. And what we're seeing right now, and this is also consistent with what orforglipron saw, it's more of a random effect over time. There's no a temporal trend anymore when you find the right starting dose and the right titration steps as we've been showing with starting at 2.5 mg and going all the way to the 30 milligrams with those 20 weeks. And so yes, we will be seeing most likely an increased incidence there. But the most important thing is that we are keeping the number of AEs leading to discontinuations very, very low. This is the hardest endpoint or the most robust endpoint, and we're very pleased with that data.
Number two, on the phase 3 design, there's nothing gating. We're collecting information on the SWITCH, but we don't see that as a key factor for informing the phase 3. And the type 2 diabetes phase 2, we need to get that data and having the exposure at higher doses than 90 milligrams for type 2 diabetes, but it's not gating. We're all ready. We have all the data ready to have the interactions with the regulatory agencies.
Q (Andy Hsieh, William Blair): On slide 16, you see a precipitous drop from week 52 to week 56. I'm just curious about what's happening here. At the bottom, you said no statistical model applied. So if you can just kind of clarify for us what that means in terms of plotting out the chart?
Dr. Coll: Yes. Thanks, Andy. This is Blai. I'll take the question. So the 90 milligrams in OLE, you see that drop between weeks 52 and 56. Taking into account that at these 2 different time points, we see different patients. And so this is probably the reason why we're seeing such a dramatic difference. This is an open label, it's interim and not all the patients have completed week 56. So that's one of the reasons why we see some differences that most likely will stabilize over time. At this point, though, after 20 weeks of median follow-up in the open-label extension, we will see potential differences in the final numbers. But directionally, I think we're very, very strong in the levels of efficacy.
And then the second question in regards to the nature of this data, this is descriptive. It's not modeled. There's no LSM or MMRM statistical approach here for multiple reasons. One, it's -- because it's an interim and it's an observational study, and that's why we don't have any modeling applied yet.
Dr. Stevens: Andy, one follow-up on that. The 90 milligrams is going to 120 milligrams. So those 2 curves, the 120 milligrams, they should converge at some point. And I think we're starting to see that in addition to it is a median 20 weeks. So we're getting a range of participants at different levels.
Q (Corinne Jenkins, Goldman Sachs): Could you speak to how you're thinking about determining a go-forward top dose given the weight loss you see at all 3 top doses really depending on the time point is reaching about 16% weight loss? What are the implications for the duration of the phase 3 depending on which top dose you kind of go forward with given that start low, go slow titration strategy?
Dr. Coll: Thanks, Corinne. Yes, as we've indicated, we're very pleased with the characterization in the dose range finding studies from 45 milligrams to 240 milligrams. We're currently work ongoing on the definition of what will be the top dose. But I think the data is very, very consistent and very compelling in both in terms of efficacy and the tolerability management for that 120 mg or higher doses. So that's for the top dose implications on that top dose in terms of the duration. I think it's very clear that based on the FDA guidance, we'll need to do a 52 weeks maintenance once we achieve the target dose and then starting at a low dose and titrating slowly to optimize that tolerability, but it will not significantly alter the overall duration of those studies.
Q (Jayed Momin, Stifel, Nicolaus & Company): This is Jayed on for Annabel. Congrats on the great data. Just one question from us. On the body composition trial, I know the interim analysis, but were you able to get any early insights into lean muscle loss versus fat loss in these patients?
Dr. Coll: Thanks, Jayed. Unfortunately, we don't have the data yet because the collection of the DEXA are still blinded, and we look forward to report the results at the end of the study, but we don't have that data as of yet available.
Q (Hardik Parikh, JPMorgan Chase): With this update, what aspects of aleniglipron's tolerability profile, do you have more confidence now? What are still the major unanswered questions for you guys? I know the 2.5 mg starting dose, we saw some encouraging signs on discontinuation rates and vomiting, while we saw some higher rates for other GI events, including the placebo arm, as you mentioned. How do you think the aleniglipron's tolerability profile can still change going forward in the phase 3 versus what you saw in the OLE and the body comp studies?
Dr. Coll: Thanks, Hardik. I'll take that and Ray please feel free to chime in. We're very pleased with the results of the tolerability that we're seeing starting at 2.5 mg, maintaining the 4 weeks and not escalating more than 2.5 fold. We're seeing decreases in nausea, seeing decreases in vomiting. And as we've said in the call, most importantly, we're seeing a dramatic reduction in the number of AEs leading to study drug discontinuations that at the end of the day, I think it's the key pillar for a successful phase 3 program. Of course, there are learnings from the open-label extension. There are learnings from the body composition that we're including in, or we're planning to include in the protocols for phase 3 that we'll continue optimizing those results. But we're very pleased with where we are right now at the completion of the dose range finding studies. Ray, anything else to add?
Dr. Stevens: Yes. This gives me the opportunity to really praise Blai and the clinical team overall. They've shown tremendous innovation and creativity in the design of these studies for example, including the open-label extension when we released the data back in December, really taught us the power of participants and knowing that they can continue on a study and seeing that really high continuation rate of people wanting to continue on aleniglipron.
So I think that was really powerful. We learned that lesson. It was kind of what I described as an experiment within an experiment. Here, we have the same situation between the body composition study and the open-label extension starting at 2.5 milligrams, Blai and the team have continued to evaluate different variables.
At the end of the day, what all this data is really for is for us to design the best possible phase 3. And I think we have probably one of the most comprehensive Phase II data sets where we've explored a number of different things to give us that very successful possibility, probability of completing phase 3 with the TPP of exactly what we want.
Q (David Risinger, Leerink Partners): Yes. I just had a question on Slide 18, please. So in the right column, the placebo crossover data was a little peculiar. Do you have any color on the conflicting figures, which show nausea 40% and vomiting at 0%?
Dr. Coll: Yes, Dave, this is Blai. Thanks for the question. So this is the overall incidence that we've seen on those participants that started on aleniglipron at week 36. As we've indicated that 40% of nausea, it can be highly subjective. We're not seeing any events of vomiting there. Now whether the protocols are very, very similar. This is the same protocol that we use for ACCESS. It's very similar to the body composition study.
Those participants maybe influenced by being in the study for the 9 previous months receiving placebo, so highly motivated and we're also seeing some preliminary signs of sites not being very aggressive in terms of the up titrations if there's any symptomatology of nausea and those down titrations persist longer compared to the body composition.
These are learnings that we can incorporate into the phase 3. This is the most important thing in addition to the low number, very low number of AEs leading to discontinuation. As you see here, we don't see anybody discontinuing up to 20 weeks of follow-up, which is, again, as we've said, it's the most important factor.
Close Concerns’ Questions
- How might the phase 2 ACCESS II trial results inform the phase 3 design, including the dosage, titration scheme, and additional endpoints?
- With tolerability representing an important key differentiator in oral GLP‑1 RA development, how does Structure Therapeutics plan to reduce AE‑related discontinuation rates?
- Is Structure Therapeutics interested in developing combination therapies with other incretin or amylin-based drugs?
- How does aleniglipron affect cardiometabolic markers, including the lipid profile and blood pressure?
--by Kayla Mathieu, Kat Moon, Monica Oxenreiter, and Kelly Close