Structure Therapeutics announces positive topline results from phase 2b ACCESS trial of oral small molecule GLP-1 RA aleniglipron –
Aleniglipron achieved a mean placebo-adjusted weight loss of 11.3% with the highest dose in the phase 2b obesity trial; 15.3% weight loss seen in an exploratory phase 2 trial of higher doses
South San Francisco-based Structure Therapeutics announced today positive topline results from its 36-week phase 2b ACCESS trial (n=220) of aleniglipron (GSBR-1290), a once-daily oral small molecule GLP-1 RA, in adults with obesity. Structure Therapeutics held a conference call today, led by CEO Dr. Raymond Stevens and VP of Clinical Development Dr. Blai Coll to discuss these results. See the webcast and presentation slides.
Participants on aleniglipron achieved a placebo-adjusted mean weight loss of 11.3% (~27.3 lbs; 12.4 kg) at the 120 mg dose, with a roughly 10.4% treatment discontinuation rate due to adverse events. In the exploratory phase 2 ACCESS II trial (n=82), which assessed a higher dose of 240 mg, participants lost up to 15.3% (~35.5 lbs; 16.1 kg) at 36 weeks, with a safety and tolerability profile similar to other GLP-1 RAs (i.e., primarily GI-related side effects).
Results from ACCESS and ACCESS II trials, as well as complementary results from the phase 3 ACCESS-OLE (n=41) trial and phase 2 body composition trial (n=71), will inform an upcoming phase 3 trial. Structure Therapeutics plans to request a Type B end-of-phase 2 meeting with the FDA in 1H26 to finalize the phase 3 design. The company also expects to initiate the phase 3 program by mid-2026, positioning aleniglipron as a potentially scalable and more accessible oral obesity therapy.
Table of Contents
- Aleniglipron demonstrated dose-dependent weight reduction in the phase 2b ACCESS trial
- Higher dose aleniglipron conferred even higher body weight reductions
- Results follow phase 2a trial, in which aleniglipron achieved 6.2% weight loss at 12 weeks
- Multiple leaders provide insightful commentary in the press release and conference call
- ACCESS-OLE and body composition trials provide complementary results
- Close Concerns’ Questions
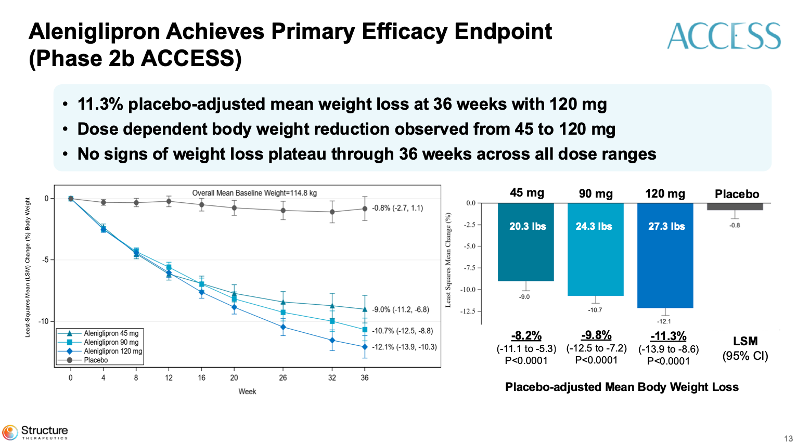
Aleniglipron demonstrated dose-dependent weight reduction in the phase 2b ACCESS trial
In the phase 2b ACCESS trial (n=220), participants receiving the 45 mg dose achieved a mean percent body weight reduction of 9%, while those on 90 mg and 120 mg achieved 10.7% and 12.1% reductions, respectively. The placebo group saw a 0.8% weight reduction over the same period. When adjusted for placebo, aleniglipron conferred 8.2% weight loss at 45 mg, 9.8% at 90 mg, and 11.3% at 120 mg, with all comparisons reaching statistical significance.
Secondary endpoints demonstrated that 86% of the aleniglipron 120 mg group achieved a weight loss of ≥5%, and 70% achieved a weight loss of ≥10%. Aleniglipron also demonstrated A1c reductions (0.28% to 0.37%) and improvements in systolic blood pressure (6.4 to 7.5 mmHg).
Source: Structure Therapeutics’ presentation slides
Higher dose aleniglipron conferred even higher body weight reductions
In the phase 2 ACCESS II trial (n=82), participants receiving the 120 mg dose achieved a mean percent body weight reduction of 13.1%, while those on 180 mg and 240 mg achieved 13.3% and 14.2% reductions, respectively. In contrast, the placebo group experienced a 1.0% weight gain over the same period. When adjusted for placebo, aleniglipron conferred 14.1% weight loss at 120 mg, 14.4% at 180 mg, and 15.3% at 240 mg, with all comparisons reaching statistical significance.
In both trials, the most common adverse events were nausea and vomiting. 65% of participants on the 120 mg dose reported experiencing nausea at least once, and 32% reported vomiting. These events were most frequent during the titration phase, which is common for therapies in the oral GLP-1 RA class.
Results follow phase 2a trial, in which aleniglipron achieved 6.2% weight loss at 12 weeks
Today’s topline results follow phase 2a data (n=64) from June 2024, in which aleniglipron achieved a mean placebo-adjusted weight loss of 6.2% in the 12-week trial and 6.9% in the 12-week pharmacokinetic study. At the time these results were released, Dr. Coll said in a conference call that the company is encouraged by the efficacious results, believing aleniglipron has best-in-class potential as an oral GLP-1 receptor agonist.
Aleniglipron has also been under investigation for T2D, with phase 2a results (n=54) in December 2023 showing a significant A1c reduction at Week 12 (1.01-1.02%, placebo-adjusted) from a baseline of about 8%. Furthermore, aleniglipron demonstrated a significant and clinically meaningful reduction in weight at Week 12 (3.26% to 3.51%, placebo-adjusted) from a baseline of about 200 lbs (90.7 kg). Weight continued to decrease through Week 12. We’re curious about the progress of aleniglipron in T2D, as Structure Therapeutics doesn’t list the treatment as under study for T2D in its pipeline.
Multiple leaders provide insightful commentary in the press release and conference call
In today’s press release, Dr. Julio Rosenstock (Chair of the ACCESS Steering Committee) expressed encouragement about the data, noting no evidence of a weight plateau by Week 36. Dr. Rosenstock also expressed optimism that larger, longer-term studies will confirm the 15.3% weight loss in the ACCESS II trial. He emphasized that once-daily oral, non-peptide GLP-1 RAs, such as aleniglipron, have the potential to increase access to obesity treatments globally. Dr. Stevens further elaborated on this point during the conference call, noting that aleniglipron can be shipped and stored at room temperature, has no fasting requirements, and is intended to provide dosing flexibility, underscoring its accessibility.
Mr. Joe Nadglowski (President and CEO of the Obesity Action Coalition) highlighted the persistent barriers to obesity care and praised aleniglipron’s potential to expand treatment options. He described the results from the ACCESS trial as an advancement in the GLP-1 RA landscape that has the potential to provide more accessible options for people living with obesity.
Competitive landscape of oral GLP-1 RAs continues to expand
Aleniglipron enters a competitive field of oral small-molecule GLP-1 RAs. Oral options may provide a promising alternative to injectable GLP-1 RAs, helping to improve convenience, reduce the burden for needle-averse patients, and address challenges related to scalability. Oral GLP-1 RAs that have made significant progress in the recent months include:
- Lilly’s orforglipron achieved positive topline results in the phase 3 ATTAIN-1 and ATTAIN-2 trials for people with obesity and T2D.
- AstraZeneca’s AZD5004 is currently in phase 2b trials for AZD5004 (VISTA trial for obesity and SOLSTICE trial for T2D). Data from both trials are expected in 1H26, with expectations to enter phase 3 trials pending results.
- Roche’s CT-996 (once-daily oral GLP-1 RA) is in a phase 2 trial (n=340), which launched in July 2025. The trial is expected to be completed in July 2026. Previously, in a phase 1 trial, CT-996 demonstrated ~7% weight loss at four weeks.
ACCESS-OLE and body composition trials provide complementary results
In addition to the primary ACCESS and ACCESS II trials, Structure Therapeutics reported findings from two ongoing complementary studies: (i) phase 3 ACCESS-OLE (n=41) trial; and (ii) phase 2 body composition trial (n=71). In both studies, participants who began on a placebo transitioned to a 2.5 mg dose and were titrated monthly to a 120 mg dose. The ACCESS-OLE study found that, after eight weeks, participants maintained and, in some cases deepened, their weight loss across 44 weeks, with no evidence of weight plateau. In the 10-week preliminary results, the low starting dose meaningfully improved tolerability compared to the 5 mg starting titration dose in the ACCESS and ACCESS II studies.
Close Concerns’ Questions
- Will Structure Therapeutics prioritize the 120 mg or 240 mg dose for phase 3 trial, and how will tolerability trade-offs be managed?
- Has there been any progress with aleniglipron for T2D?
- What pricing and access strategies will Structure Therapeutics pursue to differentiate aleniglipron in the emerging landscape for oral GLP-1 RAs?
- If aleniglipron demonstrates durable fat‑mass targeting in body composition studies, how might this reshape payer definitions of “meaningful weight loss” and influence coverage criteria?
--by Kayla Mathieu, Esther Min, Monica Oxenreiter, and Kelly Close