AACE 2026 Day #2 Highlights –
Executive Highlights
- The American Association of Clinical Endocrinology (AACE) 2026 continued with a full day of sessions covering updated T2D algorithms, diabetes technology, obesity care, cardiovascular risk, early-stage T1D, and endocrine underdiagnosis.
- Dr. Susan Samson (Mayo Clinic) reviewed the 2026 AACE algorithm for adults with T2D, emphasizing the shift from glucose-centric management toward a complications- and comorbidity-driven framework. The e updated algorithm prioritizes organ-specific risk, including ASCVD, heart failure, CKD, stroke, and MASLD, guiding therapy selection toward agents with demonstrated benefit across these domains. Notably, the framework places greater emphasis on real-world usability, including patient-led insulin titration and practical treatment pathways.
- In a standing-room-only session, Dr. Viral Shah (Indiana University) made a compelling case for GLP-1 RAs as adjunctive therapy in T1D with obesity. He challenged the notion that these therapies are inherently off-label, emphasizing that cardiometabolic indications, such as obesity, CKD, and heart failure, remain valid regardless of diabetes type. Data from the ADJUST-T1D trial demonstrated improvements in A1c, Time in Range (TIR), weight (~9 kg reduction), and insulin dose (~25% decrease), alongside early signals of cardiometabolic benefit. Taken together, the data suggest that insulin alone is insufficient to address the growing overlap of obesity, insulin resistance, and cardiovascular risk in T1D. Debates added nuance across rapidly evolving areas.
- Diabetes technology sessions underscored the expanding role of AID in T2D. Drs. Grazia Aleppo (Northwestern University) and Diana Isaacs (Cleveland Clinic) reviewed new ADA guidance positioning AID as the preferred insulin delivery method for many individuals with T2D using insulin. Both speakers discussed practical considerations for implementation, including simplified onboarding strategies, “carbohydrate awareness” over precise counting, and system-specific optimization. For individuals with high insulin requirements, reservoir limitations may necessitate concentrated insulin use, though this introduces additional complexity and requires careful adjustment.
- Additional sessions addressed underdiagnosis in hypercortisolism and the growing role of CGM and AID in perioperative care. Across both topics, speakers pointed to a gap between guideline recommendations and real-world implementation, driven by diagnostic complexity, workflow challenges, and variability in clinician familiarity. As diabetes technology and endocrine care continue to evolve, bridging this gap will be essential to translating innovation into consistent clinical practice.
See the conference agenda, registration, and our preview for what to expect in the days ahead.
Table of Contents
- 1. AACE 2026 algorithm update for adults with T2D: Expanding from glycemic management to a fully integrated cardiometabolic, complications-driven framework
- 2. Dr. Viral Shah on the use of GLP-1 RAs for obesity and cardiometabolic management in T1D
- 3. To BMI or not to BMI: An outdated metric or an important assessment tool in the management of obesity?
- 4. Weekly basal insulin debate: Adherence and simplicity in T2D weighed against hypoglycemia risk and physiologic mismatch in T1D
- 5. CGM in gestational diabetes: Debate highlights clear benefits in high-risk patients, but mixed evidence limits broad adoption
- 6. AID enters the T2D guidelines as clinical trial and real-world data show rapid gains in TIR
- 7. Addressing cardiovascular risk in T1D: Statins, non-statins, and beyond
- 8. Dr. Linda DiMeglio on transforming early‑stage T1D through screening and disease‑modifying therapies
- 9. Disrupting the status quo of underdiagnosis in hypercortisolism cases
- 10. CGM and AID in the perioperative setting: Growing guideline support contrasts with variable real-world adoption
1. AACE 2026 algorithm update for adults with T2D: Expanding from glycemic management to a fully integrated cardiometabolic, complications-driven framework
Dr. Susan Samson (Mayo Clinic) presented the 2026 update to the AACE algorithm for management of adults with T2D, outlining how rapidly evolving evidence has accelerated a shift from glucose-centric care toward a broader, complications and comorbidity-driven framework. Drawing on new clinical trial data, Dr. Samson shared updated obesity and dyslipidemia guidance and expanded therapeutic indications. The algorithm reflects a more integrated, real-world approach that prioritizes individualized care across the cardiometabolic spectrum.
- The 2026 algorithm guides therapy selection based on organ-specific risk rather than glycemia alone. Dr. Samson described how the approach now systematically considers conditions such as atherosclerotic cardiovascular disease (ASCVD), heart failure, chronic kidney disease (CKD), stroke, and metabolic dysfunction-associated steatotic liver disease (MASLD), directing clinicians toward therapies with demonstrated benefit in each domain. This evolution is supported by a rapid expansion of new clinical evidence and drug indications, with incretin-based therapies and SGLT-2 inhibitors now used across cardiovascular, renal, obesity, and liver disease. As a result, medications originally developed for glucose lowering are increasingly positioned as multi-system therapies, requiring clinicians to take a broader view when selecting treatment.

- The algorithm also reflects a shift toward more individualized assessment, both in how glycemia is measured and how diabetes itself is classified. While A1c remains a central benchmark, Dr. Samson discussed the growing role of CGM and metrics, such as Time in Range, to better capture daily glycemic variability and guide treatment decisions. In parallel, a new structured classification framework encourages clinicians to confirm a T2D phenotype and consider alternative etiologies, including T1D in adults, latent autoimmune diabetes in adults (LADA), monogenic diabetes, endocrinopathies, and pancreatic disease. This addition responds to frequent real-world misclassification, which can delay appropriate therapy and alter disease trajectories.
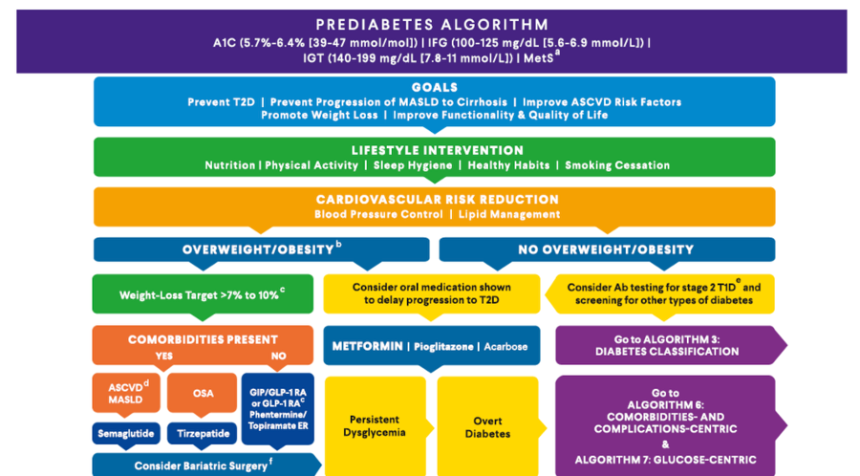
- Early-stage disease and cardiometabolic risk are addressed more proactively, with prediabetes management increasingly tied to obesity and risk reduction strategies. Lifestyle intervention remains foundational, but the algorithm more clearly incorporates weight-loss driven approaches and the use of agents such as GLP-1 RAs in high-risk individuals to delay progression. At the same time, dyslipidemia guidance reinforces LDL lowering as the primary target for cardiovascular risk reduction, with stepwise intensification of therapy and less emphasis on triglycerides outside of pancreatitis risk.
- The algorithm continues to provide practical guidance for treatment escalation, including early insulin use in cases of severe hyperglycemia and tools to support patient-led titration. Dr. Samson described approaches for initiating basal insulin in individuals with significant glucose toxicity, with strategies that help patients to adjust dosing based on home glucose data. The update incorporates real-world considerations such as access, cost, and usability, with integrated therapy tables and obesity guidance designed to make the algorithm more actionable across clinical settings.
- We were lucky to attend a “Meet the Authors” session earlier today in the Exhibit Hall, where Dr. Samson was joined by several consensus coauthors to discuss the framework in real time – the magic of AACE! This valuable interactive session helped providers in the audience discuss specific case studies, as well as understand how the consensus was formed. The entire audience walked away far more informed on how to implement this guideline in clinical practice.
2. Dr. Viral Shah on the use of GLP-1 RAs for obesity and cardiometabolic management in T1D
In this standing‑room‑only session, Dr. Viral Shah (Indiana University) delivered an evidence‑driven case for the use of GLP‑1 RA as adjunctive therapy in adults with T1D and obesity. He opened by challenging the common misconception that GLP‑1RA use in T1D is inherently “off‑label.” Citing the ADA Standards of Care, he emphasized that a diagnosis of T1D does not preclude the presence of insulin‑resistant or obesity‑related phenotypes, and that individuals with T1D may appropriately be categorized as having features of both T1D and T2D to facilitate access to therapies with weight and cardiometabolic benefits. He further clarified that GLP‑1 RA use for obesity with T1D is still considered on‑label, and that SGLT-2 inhibitors used for CKD or heart failure are also on‑label, regardless of diabetes type, with only glycemic‑specific use being off‑label.
- Dr. Shah outlined why adjunctive therapies are needed. Even with modern AID systems, only about 50% of adults achieve an A1c <7.0%, and daytime glycemic management remains a persistent challenge. Obesity prevalence in T1D now mirrors the general population, with more than half of adults having overweight or obesity, and cardiovascular mortality remains substantially elevated, even among those meeting glycemic targets. Insulin alone, he argued, cannot address the intertwined burdens of weight, insulin resistance, and cardiovascular risk.
- He showed emerging evidence from the ADJUST‑T1D trial (n=72) of semaglutide in adults with long‑standing T1D and obesity. Semaglutide produced meaningful improvements across multiple domains, with 36% of participants achieving the composite primary endpoint (TIR >70%, Time <70 mg/dL <4%, and ≥5% weight loss) versus none on placebo. A1c improved by 0.3%, TIR increased by nearly 9 percentage points, and body weight decreased by 9 kg (~20 lbs) over 26 weeks. Insulin requirements fell by ~25%, with reductions beginning in the first week at the 0.25 mg dose. Mediation analyses showed that early glycemic improvements were not explained by weight loss, suggesting a direct metabolic effect. He highlighted that multiple trials are now underway, including T1‑DISCO, RT1D, and SURPASS‑T1D, which will define long‑term cardiovascular, renal, and metabolic effects of GLP‑1RA therapy in T1D.
- Dr. Shah also highlighted early cardiometabolic signals from the ADJUST T1D- CV trial, with semaglutide producing reductions in total cholesterol, non‑HDL cholesterol, LDL cholesterol, systolic blood pressure, and estimated 5‑year CVD risk. Although short‑term and exploratory, these findings point toward a broader role for GLP‑1RA therapy in reducing cardiovascular burden in T1D.
- Dr. Shah also addressed safety, indicating that across the trial, no DKA events occurred, and severe hypoglycemia rates were similar between semaglutide and placebo. He emphasized the importance of 20-30% insulin dose reduction at initiation, especially in AID users, and noted that carbohydrate intake decreased modestly (~30 g/day) but did not fully explain insulin reductions.
3. To BMI or not to BMI: An outdated metric or an important assessment tool in the management of obesity?
We greatly enjoyed today’s debate, “Should we continue to use BMI when talking about obesity?” Dr. Donna Ryan (Pennington Biomedical) and Dr. W. Timothy Garvey (University of Alabama, Birmingham) took opposing sides in a hotly debated topic: the continued role of BMI in the management of obesity. Historically, BMI emerged as a practical and scalable proxy for body fat, gaining prominence through actuarial data and epidemiologic studies linking weight categories to mortality risk. Its simplicity and strong association with population-level morbidity and mortality have cemented its use in public health systems and clinical coding. However, today’s debate from two highly esteemed key opinion leaders underscores a paradigm shift: obesity is increasingly defined not merely by body size, but by the presence of excess or dysfunctional adipose tissue that impairs health.
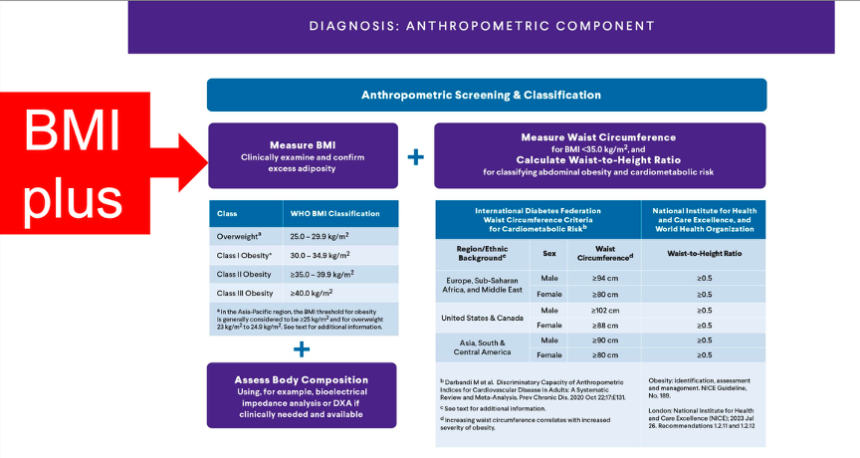
- Dr. Ryan argued in favor of retaining BMI as a foundational tool in managing obesity, emphasizing its historical utility, accessibility, and continued relevance in large-scale surveillance and clinical infrastructure. She acknowledged well-established criticisms like BMI’s inability to distinguish between fat and lean mass or to account for fat distribution but maintained that these limitations do not negate its value as a screening measure. Instead, she advocated for a “BMI-plus” framework, in which BMI is complemented by additional anthropometric indicators (such as waist circumference or waist-to-height ratio) and clinical assessments of metabolic, functional, and psychological health. Dr. Ryan situated this approach within evolving frameworks such as those proposed by the EASO and the Lancet Commission, arguing that while refinement is necessary, abandoning BMI outright would be impractical given its integration into electronic health records, diagnostic coding systems, and public health monitoring.
- In contrast, Dr. Garvey was far more critical of the metric, emphasizing the inadequacy of BMI as a standalone diagnostic tool for individual patients. He aligned more with a pathophysiologically grounded definition of obesity, focusing on adipose tissue dysfunction and its clinical consequences rather than body size alone. Dr. Garvey highlighted phenomena such as “metabolically healthy obesity” and “normal weight obesity,” which expose the discordance between BMI and actual health risk. Even further, with today’s technologies like DEXA, MRI, and bioelectrical impedance analysis (BIA), clinicians can achieve a more accurate understanding of metabolic complications and disease burden. From this perspective, reliance on BMI risks both overdiagnosis and underdiagnosis, supporting Dr. Garvey’s position that we should move away from this metric as a defining characteristic of obesity. Currently, he added, staging paradigms for disease severity are based on the presence and severity of complications, not BMI. A wholistic approach to care (beyond BMI) is entrained by either using the diagnostic term Adiposity-Based Chronic Disease (ABCD) or by conceptualizing the disease in this way.
4. Weekly basal insulin debate: Adherence and simplicity in T2D weighed against hypoglycemia risk and physiologic mismatch in T1D
In a lively point-counterpoint session, Dr. Carol Wysham (University of Washington) and Dr. Cecilia Low Wang (University of Colorado) debated the role of once-weekly basal insulins, drawing a sharp distinction between the clear use in T2D and unresolved safety concerns in T1D. The discussion moved beyond trial results to address real-world challenges, including adherence, provider hesitation, and physiologic variability, ultimately framing weekly insulin as a promising but population-specific therapy.
- In favor, Dr. Wysham framed once-weekly basal insulin as a pragmatic solution to persistent gaps in insulin initiation and adherence in T2D. She underscored that basal insulin remains underutilized and often introduced too late, with patient resistance continuing to limit uptake. Even when initiated, glycemic outcomes remain suboptimal, driven in part by missed doses and the burden of daily injections. She discussed real-world adherence challenges, from busy schedules to social discomfort, noting that even a few missed doses per month can meaningfully worsen glycemic outcomes.
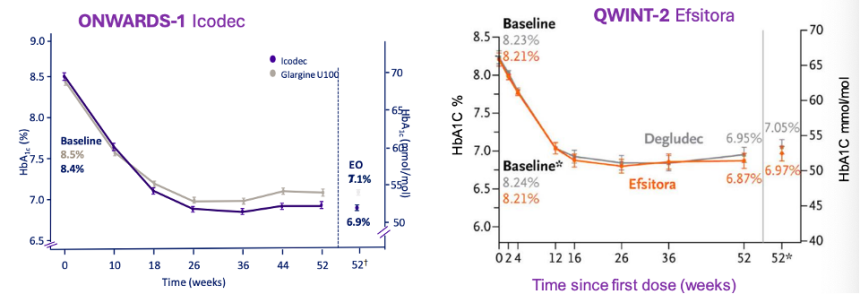
- Clinical trial evidence supports comparable glycemic efficacy and safety in T2D, alongside strong patient preference for weekly dosing. Dr. Wysham reviewed the ONWARDS (insulin icodec) and QWINT (insulin efsitora alfa) programs in T2D, highlighting consistent non-inferiority compared to daily basal insulin, with A1c reductions in the 1%-1.5% range and no meaningful increase in severe hypoglycemia. She said that superiority was achieved in several trials, while weight gain and adverse event profiles were comparable. CGM metrics demonstrated improvements in Time in Range (TIR) and reductions in hyperglycemia, reinforcing clinical effectiveness beyond A1c alone. Patient-reported outcomes emerged as a key differentiator, with strong preference for weekly dosing, improved satisfaction, and reduced treatment burden.
- Pharmacokinetics were positioned as a key factor of weekly dosing, yet they introduce new clinical considerations around titration and onset. Dr. Wysham described how albumin binding and prolonged half-life (eight days for insulin icodec and 17 days for insulin efsitora alfa) allow for sustained insulin exposure, with relatively flat glucose-lowering effects across the week. However, she acknowledged practical nuances, including delayed time to steady state without loading doses and the need for thoughtful titration strategies, particularly in individuals far from glycemic targets. These features introduce a different clinical workflow compared to daily insulin, requiring provider familiarity and comfort with longer-acting pharmacodynamics.
- The argument against once-weekly insulin emphasized that these pharmacologic properties may pose safety challenges in T1D, where insulin requirements are more dynamic and tightly regulated. Dr. Low Wang highlighted that once-weekly insulin is currently approved only for T2D in the US, reflecting important differences in physiology and risk tolerance. In T1D, the absence of endogenous insulin and greater day-to-day variability in insulin needs make prolonged exposure more difficult to manage. While weekly insulins are engineered to deliver evenly distributed effects, she demonstrated that real-world pharmacodynamic profiles deviate from this ideal, with relatively higher insulin activity in the first few days post-injection and lower activity toward the end of the week.
- Drawing on early trials and prior FDA advisory discussions, Dr. Low Wang showed that hypoglycemia rates track closely with early post-dose peaks, with higher rates of level 2 and combined level 2/3 hypoglycemia compared to daily insulin when used in T1D. While A1c reductions and TIR are comparable between weekly and daily insulin, she argued that efficacy alone is insufficient if hypoglycemia risk remains elevated, particularly in a population already at a higher risk for severe events.
- Implementation challenges further complicate the use of weekly insulin in T1D, given the misalignment between fixed weekly dosing and daily variability in insulin needs. Dr. Low Wang noted that proposed mitigation strategies, including CGM integration or adjusting insulin exposure across the week, would add complexity to an already intensive management paradigm and have not been rigorously studied. She also raised concerns about real-world feasibility, including CGM access challenges, provider familiarity with newer insulin formulations, and the potential for misclassification between T1D and T2D, which could expose higher-risk individuals to unintended hypoglycemia.
5. CGM in gestational diabetes: Debate highlights clear benefits in high-risk patients, but mixed evidence limits broad adoption
In a focused debate, Dr. Sarit Polsky (Barbara Davis Center for Diabetes) and Dr. Kevin Borst (Cleveland Clinic) examined whether CGM should become standard of care in gestational diabetes (GDM), ultimately converging on a more targeted approach: CGM offers clear benefit in select populations, but evidence remains insufficient for universal adoption.
- CGM is beneficial for the dynamic physiology of pregnancy, with the strongest case in insulin-requiring patients and at high-risk individuals. Dr. Polsky opened the pro statement by grounding her argument in the reality of glycemic management during pregnancy: tight glycemic targets and rapidly shifting insulin requirements, driven by rising placental hormones, make intermittent BGM measurements insufficient. By capturing continuous trends, CGM is better positioned to keep pace with these changes.
- Pooled data from the CONCEPTT RCT (n=200) and a Swedish observational study (n=186) showed a 7% increase in Time in Pregnancy Range (TIPR), associated with reductions in large-for-gestational-age (LGA) births, neonatal hypoglycemia, and prolonged (>24 hours) NICU admissions.
- In the Steady Sugar RCT (n=120), CGM users spent more Time in Pregnancy Range, reported higher satisfaction, and experienced fewer hyperglycemic events, alongside reductions in preterm births, LGA, and NICU admissions compared to the BGM group.
- The GLAM study (n=760) demonstrated a 14% difference in tighter Time in Range (TIR; between 63-120 mg/dL) between women who did and did not develop GDM, with Time >140 mg/dL showing the strongest predictive performance at 15-16 weeks and 21-22 weeks, raising the possibility of CGM for earlier screening.
- Evidence of CGM use in GDM is limited, with ongoing concerns around cost, burden, and clinical impact. Dr. Borst stressed access barriers and cost, noting CGM was roughly three times more expensive than BGM in one RCT ($431.89 vs. $108.23 over eight weeks), raising questions about scalability and cost-effectiveness.
- Burden and usability. Dr. Borst described the initial GDM visit as already cognitively demanding, with CGM adding complexity and potentially increasing anxiety due to alarms. In the CONCEPTT trial, 80% of users reported device frustrations and 50% experienced skin reactions, alongside increased provider contact.
- Accuracy and standardization. He raised the issue of interstitial glucose lag, potentially worsened by edema in later pregnancy, and pointed out that standard MARD thresholds have not been validated for GDM. Reduced accuracy at low glucose has been observed with Freestyle LibrePro and Medtronic iPro2, and optimal CGM metrics for pregnancy remain undefined.
- Clinical outcomes. Data from the DipGluMo study (n=299) found no significant difference between CGM and BGM across perinatal outcomes, including LGA, macrosomia, neonatal hypoglycemia, and stillbirth.
- Dr. Polsky led with the updated international consensus statement, which defines a TIPR target of >90% within 63-140 mg/dL, addressing prior concerns around lack of standardization. She also pushed back on psychological burden, citing CONCEPTT trial data showing reduced hypoglycemia avoidance behavior among CGM users. She highlighted key limitations of DipoGluMo: late initiation (~28 weeks), low insulin use, single-sensor design, and limited power for neonatal outcomes, but noted that participants in both arms preferred sensor use. Additional data from the GRACE RCT (n=375) showed lower LGA rates with CGM, supporting a potential role for CGM-guided treatment intensification.
- Dr. Borst acknowledged CGM’s ability to identify more individuals meeting diagnostic threshold, such as in GLAM, but argued this raises questions around clinical use. On Steady, he said that the primary outcome of TIPR did not translate to improved clinical outcomes, which is ultimately the metric that matters. He closed by anchoring to the ADA 2026 guidelines, which explicitly state there is insufficient evidence to support CGM use in all people with GDM.
- From the floor: Both speakers agreed that insulin-requiring patients represent the clearest use case and that confirmatory capillary blood glucose check is warranted whenever a sensor reads low.
- CGM’s role in diagnosis or as a complement to the oral glucose tolerance test (OGTT) remains early, with insufficient data. Notably, no head-to-head comparisons across CGM systems in pregnancy-associated diabetes currently exist.
6. AID enters the T2D guidelines as clinical trial and real-world data show rapid gains in TIR
Drs. Grazia Aleppo (Northwestern University) and Diana Isaacs (Cleveland Clinic) outlined the expanding role of AID in T2D, pairing new guideline support with clinical trial data and detailed case examples. The data showed how AID can rapidly improve TIR, reduce A1c levels, and often lower total daily insulin dose with more optimized delivery. Both speakers also noted that successful use depends on matching the right system to the right patient and knowing which levers to adjust when targets aren’t met.
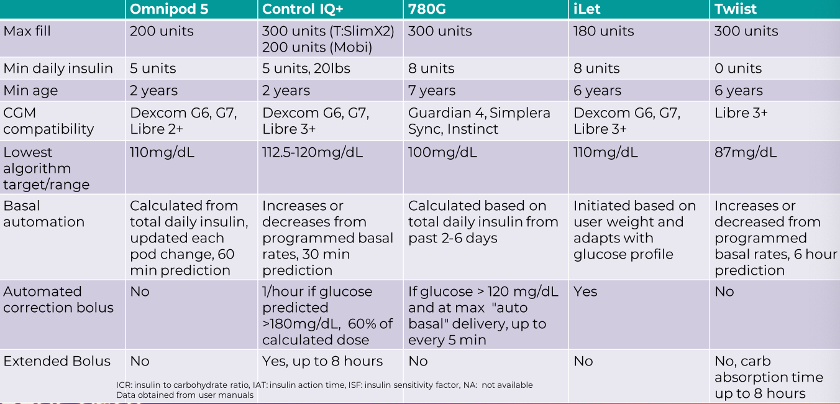
- The updated guidelines reflect a growing evidence base across Omnipod 5, Control-IQ+, and MiniMed 780G. Dr. Aleppo opened by pointing to the 2026 ADA Standards of Care, which now identify AID as the preferred insulin delivery method for adults with T2D using insulin. The SoC recommend considering AID for select people with T2D on basal insulin who are not meeting individualized goals. Dr. Isaacs then reviewed the trial data behind this shift: (i) SECURE-T2D (n=305) showed Omnipod 5 reduced A1c from 8.2% to 7.4% and improved TIR from 45% to 66%; (ii) the randomized 2IQP trial (n=319) showed Control-IQ+ improved A1c by an adjusted 0.6% and TIR by 15% versus the control; and (iii) IMPACT2D (n=95) showed MiniMed 780G reduced A1c to 7.9% to 7.2% and increased TIR from 72% to 80%.
- Implementation hinges on practical setup, access, and understanding how each algorithm behaves.Common initiation approaches include using ~75% of prior total daily dose or ~0.5 units/kg/day, along with standard formulas for correction factor and carbohydrate ratio. However, clinicians were encouraged to prioritize “carbohydrate awareness” over precise carbohydrate counting for many people with T2D. Access has improved, especially via pharmacy channels, though Dr. Isaacs noted that DME pathways and Medicare requirements can still limit uptake. Notably, for individuals requiring large insulin doses, reservoir limitations (typically ~180-300 units) may necessitate use of concentrated insulin, which requires careful dose adjustment and added education. U500 insulin may be considered in extreme cases, but its pharmacokinetics are less compatible with AID algorithms and increase complexity. At the same time, each system requires a different optimization approach. Some systems rely more on programmed basal settings, like Control-IQ and twiist, while systems such as Omnipod 5 and MiniMed 780G rely more on automated corrections and targets.
7. Addressing cardiovascular risk in T1D: Statins, non-statins, and beyond
In this packed case-based session, Dr. Elias Siraj (Eastern Virginia Medical School) and Dr. Vishnu Priya Pulpati (Warren Clinic Endocrinology) discussed cardiovascular risk management in T1D. The session garnered strong audience participation as speakers worked through real-world scenarios to illustrate how guideline recommendations translate to the clinic.
- Dr. Siraj maintained that the elevated cardiovascular risks associated with T1D justify an assertive approach to statin use. Young patients with T1D face four times the all-cause mortality and eight times the cardiovascular mortality compared to peers, as demonstrated in a Danish cohort study. Dr. Siraj cited Scandinavian registry data showing substantially higher events and mortality compared with T2D and peers without diabetes at the same age. He noted that even when LDL levels appear “normal,” patients may still carry an elevated CVD burden. Drawing on the UK Heart Protection Study, he noted that statins reduce major cardiovascular events and mortality in T1D by roughly 20-25%, supporting LDL goals of <100 mg/dL for primary prevention and <55-70 mg/dL for very high-risk or secondary prevention. Guideline-driven cases illustrated when to initiate statins, according to age, labs, and additional risk factors.
- In clinical trials, statin intolerance is only about 1-2%, which is far less than the rates encountered in routine practice. He reviewed strategies such as switching to hydrophilic statins and lowering or intermittently dosing statins before declaring complete intolerance. He also touched on evolving guidance around statin use in high-risk women of childbearing age and during pregnancy.
- Turning to non-statin therapies, Dr. Pulpati framed these agents as essential tools for high-risk or statin-intolerant patients with T1D. She reviewed data from the IMPROVE-IT trial (n=4,933) and RACING trial (n=1,398) to show that combining moderate-intensity statins with ezetimibe can match or exceed high-intensity statins in achieving LDL targets. These therapies often have better tolerability, especially for patients with T1D, who may be “hyper-absorbers” of cholesterol. She highlighted bempedoic acid, which lowered LDL and risk of major cardiovascular events without worsening glycemia in the CLEAR Outcomes trial (n=6,373) and the role of PCSK9 inhibitors, including inclisiran and alirocumab, in the ORION (n=3,660) and ODYSSEY OUTCOMES (n=5,444) trials. She closed by widening the lens beyond LDL, recognizing Lp(a), ApoB, and triglyceride-rich lipoproteins as additional drivers of ASCVD risk that warrant attention in comprehensive cardiovascular risk management in T1D.
8. Dr. Linda DiMeglio on transforming early‑stage T1D through screening and disease‑modifying therapies
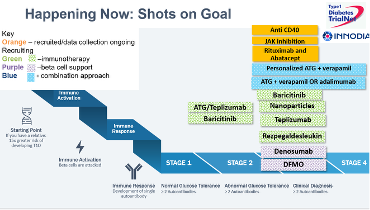
In this plenary session, Indiana University's Dr. Linda DiMeglio delivered a most inspiring 2026 Alan J. Garber Lecture, including an overview of early stage T1D, spanning screening, monitoring, and available and disease‑modifying therapies. She emphasized that presymptomatic T1D is now a diagnosable and actionable condition, anchored in the established staging framework (stages 1-3) and driven by islet autoantibody detection. Across multiple cohorts, individuals with ≥2 autoantibodies face a ~44% five‑year and ~70% 10‑year risk of progression to clinical (stage 3) T1D, independent of family history.
- Dr. DiMeglio discussed the accelerating global shift toward population‑level screening. Italy’s nationwide screening mandate for T1D and celiac disease in the pediatric population provides an example for what a broad-based population screen would look like. She also highlighted the forthcoming Breakthrough T1D consensus guidance recommending multiple screening points, at: (i) ages 2-4; (ii) at 6-8 years if IAb is negative; and (iii) ages 10-15 years. Following this protocol increases sensitivity to ~80% when all three windows are used. She stressed that the primary purpose of monitoring is to prevent DKA at diagnosis with timely recognition of the onset of stage 3 T1D.
- Adults remain a critical gap, with up to 40% of individuals developing T1D after age 30 initially misclassified as T2D. This reinforces the need for antibody testing and careful staging in this population. Importantly, she underscored that monitoring protocols for adults differ substantially from pediatrics. Adult data are sparse, misdiagnosis is far more common, and adults lack the structured, evidence‑based monitoring pathways that now exist for children. Whereas pediatric guidance specifies clear intervals for repeat autoantibody testing, metabolic checks, and escalation to endocrinology, adult guidance is limited to expert‑opinion recommendations, such as annual metabolic monitoring only when additional risk factors are present. This asymmetry reflects both the higher-quality evidence base in children and the urgent need to build comparable monitoring frameworks for adults.
- On the broader therapeutic landscape, Dr. DiMeglio also spotlighted yesterday’s FDA decision to expand approval of Tzield (teplizumab) to include children aged ≥1 year with stage 2 T1D, a major regulatory milestone that broadens access. Dr. DiMeglio was candid: while teplizumab provides clear proof‑of‑concept, most monotherapies have not produced durable preservation of beta‑cell function. These realities point toward precision medicine, combination therapy, and longer‑duration regimens rather than single‑course interventions. She highlighted multiple ongoing studies, including abatacept + rituximab combinations, which she is particularly excited about given that it simultaneously targets T‑cell stimulation and B‑cell-mediated autoimmunity.
- Still, she noted that the field has not yet had its “home run” just yet, emphasizing that despite encouraging signals, there still exists a need for more potent, durable, and combinatorial approaches.
9. Disrupting the status quo of underdiagnosis in hypercortisolism cases
In this industry-sponsored session, Dr. Ricardo Correa Marquez (Cleveland Clinic), Dr. Laurence Kennedy (Cleveland Clinic), and Dr. Karl Nadosky (Endocrine Clinic) participated in a panel discussion focused on hypercortisolism. Dr. Kennedy described hypercortisolism as a heterogeneous, spectrum disorder encompassing both neoplastic and non-neoplastic etiologies. While classical phenotypes are more typical of conditions such as Cushing’s disease, ectopic ACTH secretion, and adrenal carcinomas, a substantial proportion of patients lack overt physical features. Despite this, both groups experience significantly elevated cardiometabolic morbidity and mortality, with an approximately three-fold increase in mortality risk, largely driven by elevated rates of cardiovascular disease. The growing use of cross-sectional imaging has increased incidental detection of adrenal abnormalities, further emphasizing the need for heightened clinical awareness beyond textbook presentations.
- Dr. Nadosky focused on the status quo in management: persistent delay in diagnosis, often spanning several years, due in part to complex and resource-intensive diagnostic algorithms that are impractical in many clinical settings. All speakers emphasized the importance of recognizing “multiple and progressive features,” particularly in patients with treatment-resistant or atypical cardiometabolic conditions, such as worsening or difficult to treat T2D, hypertension at a young age, or unexplained weight gain. Case studies illustrated how subtle, progressive metabolic deterioration, despite standard interventions, should prompt further evaluation. Emerging evidence from studies such as CATALYST and MOMENTUM suggests that targeted screening of high-risk populations (e.g., patients with difficult-to-control diabetes or resistant hypertension) can improve detection rates, especially given that reliance on classical physical signs alone may miss over half of affected individuals.
- From a diagnostic standpoint, Dr. Correa Marquez advocated for a pragmatic, stepwise approach integrating clinical suspicion with biochemical and imaging data. The overnight dexamethasone suppression test was highlighted as the most sensitive first-line screening tool, while acknowledging that commonly used measures such as urinary free cortisol or late-night salivary cortisol may yield false negatives in milder forms of disease. Measurement of plasma ACTH, alongside adjunctive biomarkers like DHEA-S, can help differentiate ACTH-dependent from ACTH-independent causes and guide subsequent imaging. Overall, the session underscored the need for simplified, clinically grounded diagnostic strategies that integrate patient history, evolving comorbidities, and judicious use of testing to reduce missed or delayed diagnoses of hypercortisolism.
10. CGM and AID in the perioperative setting: Growing guideline support contrasts with variable real-world adoption
In a standing-room-only session, Dr. Lubaina Presswala (Memorial Sloan Kettering Cancer Center) explored the evolving role of CGM and AID systems in the perioperative setting, combining guideline review, real-world evidence, and new survey data across US institutions. Her presentation highlighted a clear dichotomy: while professional societies increasingly support the use of diabetes technology during surgery, real-world implementation remains highly variable. Dr. Presswala attributed this gap to limited standardization, workflow integration challenges, and a lack of evidence for newer systems.
- Guidelines increasingly support continuation of CGM and AID in select perioperative settings, with decisions driven by procedure type and patient status. Across AACE, the ADA, the Endocrine Society, and Joint British Diabetes Societies for Inpatient Care (JBDS-IP) guidance, a consistent theme emerged: individuals who are clinically stable and capable of self-management may continue insulin pump therapy, particularly for shorter procedures (<2-3 hours) or those involving minimal physiologic disruption. Glycemic targets are broadly consistent at ~100-180 mg/dL, with use of activity mode or temporary targets used perioperatively to reduce hypoglycemia risk. Decisions ultimately depend on procedure duration and patient status, with longer or more complex surgeries typically requiring transition to IV insulin.
- Device functionality and evidence support perioperative use, but gaps in clinician familiarity and data limit consistency.
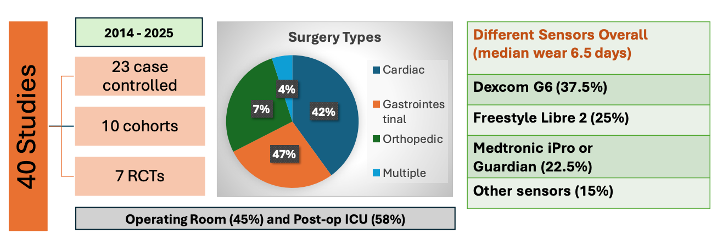
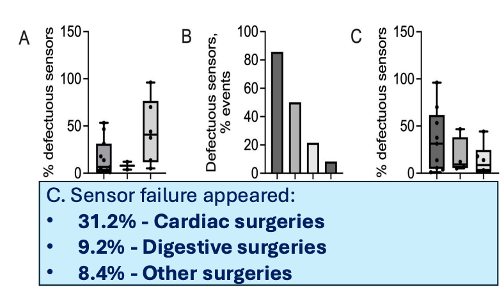
- On CGM, Dr. Presswala reviewed evidence supporting safety and accuracy in the perioperative setting, while noting heterogeneity across studies. A systematic review of 40 studies and ~2,400 patients demonstrated strong clinical accuracy (Clarke Error Grid ~98.6-99.1% in safe zones[1]) and acceptable numerical accuracy (MARD ~13.4%-18.2%), consistent with inpatient performance benchmarks. CGM was generally non-inferior to point-of-care glucose and associated with improved hyperglycemia detection and fewer recurrent hypoglycemia events. However, variability across procedures, sensor types, clinical settings, and technical challenges, such as signal loss and interference, continues to complicate interpretation and standardization.
- On AID systems, early data suggest strong perioperative performance, supported by dynamic insulin adjustment capabilities. Dr. Presswala said that hybrid closed-loop systems use CGM-integrated algorithms to automatically modulate insulin delivery, including more conservative dosing in activity mode to reduce hypoglycemia risk. In a prospective cohort of adult patients with diabetes undergoing surgery (n=15) using MiniMed 780G, Time in Range reached ~99.6% intraoperatively with no hypoglycemia and rapid return to baseline glycemia postoperatively. These findings support continued AID use during surgery, with larger randomized studies needed to confirm performance across broader surgical settings.
- Real-world practice diverges from policy, with significant variability across institutions. Dr. Presswala shared preliminary outcomes from a cross-sectional survey of 35 institutions, revealing that while ~84% report having policies or workflows for perioperative technology, agreement drops to ~61% when examining actual clinical practices. Glucose monitoring and hypoglycemia protocols were highly consistent, but significant variability was seen around pump continuation, duration limits, intraoperative adjustments, and clinician discretion. Notably, Dr. Presswala said 70-80% of respondents indicated that pump removal decisions often fall to anesthesiologists or surgeons, underscoring the influence of provider familiarity and comfort rather than standardized protocols.
- Dr. Presswala concluded by reinforcing that national societies recommend multidisciplinary teams to establish institutional policies for safe AID use, yet current practices remain inconsistent and largely based on older technology, pointing to a clear need for updated guidance and greater standardization as newer systems enter clinical use.
-- by Milenka Men, Riya Chatterjee, Kayla Mathieu, Monica Oxenreiter, and Kelly Close
[1] Clarke Error Grid Analysis evaluates the clinical accuracy of glucose measurements.