ADA publishes 2026 Standards of Care –
Executive Highlights
- The American Diabetes Association released today its annual Standards of Care document. The ADA also published a Summary of Revisions, providing a concise overview of the major revisions included in this year’s updates.
- The ADA Standards of Care represent the first step towards changing the landscape of diabetes management. While there is certainly therapeutic inertia when it comes to implementing many of these changes, having these updated recommendations in place is the first step toward seeing them in daily practice across patients, clinicians, and payers. As always, we hope the SOC is widely read ahead of the new year, and we will do our part to spread awareness of the changes. We also look forward to covering future sessions at scientific conferences translating these updates, aided by an abridged Standards of Care document for primary care physicians and through various forms of media that aim to explain SOC updates more simply.
- In tech, the Standards of Care strengthened its recommendations on AID in T2D and its promotion of early technology adoption. The opening sentence of the “Initiation of Device Use” section now definitively states that technology “should be initiated soon after the time of diagnosis and anytime thereafter.” The ADA simplified its recommendations for CGM initiation at onset, moving beyond a focus on combination therapy including insulin and GLP-1 RAs to now recommend CGM at diabetes onset for adults using insulin, for noninsulin therapy that can cause hypoglycemia, or for any therapy where CGM aids management. It also removed recommendations requiring the presence of certain C-peptide levels, islet autoantibodies, or duration of insulin use before AID or insulin pump initiation in T2D.
- In CGM, the 2026 recommendations, when compared with 2025 language, reflect a more universal stance that the devices should be available regardless of what therapy is being used.
- In AID, the 2026 Standards of Care reaffirm the critical role of the technology for individuals with T1D and strengthened recommendations for insulin pump use in T2D. Notably, citing several pivotal trials published in 2025, Recommendation 7.25a designates AID systems as “the preferred insulin delivery system” for all people with T1D, as well as for adults and children with T2D who are currently using MDI, insulin pumps, or sensor-augmented pump therapy.
- There are also important updates in pregnancy and inpatient use. Dig in below!
- In therapy, the Standards of Care included updates on screening and pharmacologic management of T2D and comorbidities that span obesity, cardiovascular disease (CVD), chronic kidney disease (CKD), metabolic liver diseases, and microvascular complications. Incretin-based therapies were spotlighted for their benefits beyond glycemic health and weight loss, such as heart failure, metabolic dysfunction-associated steatohepatitis (MASH), cardiorenal risk reduction, and peripheral artery disease. The Standards of Care also strengthened its emphasis on routine screening for complications, individual treatment goals, and patient education.
- On CKD, GLP-1 RAs were recommended for adults with T2D and ASCVD or CKD (eGFR <60 mL/min/1.73 m2), as well as those with advanced CKD (eGFR <30 mL/min/1.73 m2) due to lower risk of hypoglycemia and proven CV benefit. Moreover, early SGLT-2 inhibitor use and/or simultaneous initiation of SGLT-2 inhibitors and nsMRA are recommended for this population.
- On heart failure (HF), GLP-1 RA or dual GLP-1/GIP RA are recommended for adults with T2D, obesity, and symptomatic HF with preserved ejection fraction (HFpEF) regardless of A1c values. For the treatment of more advanced HF, nsMRA is advised for reducing worsening HF events.
- On the liver, GLP-1 RAs or dual GLP-1/GIP RAs are recommended for adults with diabetes and MASLD or MASH.
- On acute hyperglycemic crises, the Standards of Care offered greater clarity on risk factors, screening, and management strategies for diabetic ketoacidosis. Notably, people with diabetes are recommended to use blood ketone monitoring and to seek medical attention if they cannot drink fluids, experience altered mental status, or struggle to improve blood glucose or ketone levels.
- On weight management, two important changes were added among others. When administering pharmacotherapy, Recommendation 8.20 stresses the importance of personalizing titration to balance efficacy, health benefits, and tolerability. Importantly, optimal treatment dose may not be the maximum approved dose. Secondly, new section was added for the treatment of obesity in people with T1D. Recommendation 8.29 supports the use of incretin-based therapies and/or metabolic surgery in adults with T1D with BMI ≥30 kg/m2 or BMI ≥27.5 kg/m2 in Asian Americans. When initiating incretin-based therapies, patients should be counseled about: (i) increased risk of hypoglycemia and reduction in insulin requirements; (ii) the importance of maintaining carbohydrate intake; and (iii) routine testing of excess ketone body production. Dose titration for people with T1D should be approached with close monitoring in insulin requirements and hypoglycemic events.
- For a look at how far diabetes has come, check out our SOC coverage from years past – 2025, 2024, 2023, 2022, 2021, 2020, 2019, 2018, and 2017. It’s been particularly exciting over the past several years to watch the Standards of Care shift toward strategies for complication prevention specifically alongside broader glycemic management with evolving diabetes therapies and technologies, with increasing focus on heart and kidney risk reduction and weight management. We’ve also been grateful to see evolving guidelines on managing patients impacted by SDOH, mental health, and on how to engage in meaningful diabetes advocacy. The impressive document totals 377 pages, up 15% from 328 pages in 2025[1].
The American Diabetes Association released today its annual Standards of Care document. Here, we review and contextualize the most notable updates from the 2026 Standards of Care, broken down into diabetes therapy, technology, and big picture themes. Read on for our coverage of the most important changes, ranging from CGM for non-insulin T2D, AID for insulin-using T2D, MASH, and expanded therapeutic options for glycemic targets.
Table of Contents
-
Diabetes Technology
- 1. ADA expands eligibility for CGM and reframes device categories
- 2. ADA’s recommendations for AID use in T2D strengthens
- 3. Strengthening early initiation and education in diabetes technology
- 4. AID and CGM in pregnancy: ADA adds new RCT evidence and clarifies expanded use cases for AID
- 5. Specific perioperative care recommendations provided for hospitalization and surgery
- 6. Diabetes device support: The ADA simplifies recommendations on device support for youth and reiterates recommendations on open-source AID
-
Diabetes Therapy
- 7. Broader range of conditions such as CKD, MASLD, and post-transplantation diabetes now included for incretins
- 8. Outpatient prevention and management of acute hyperglycemic crises, including DKA
- 9. Obesity and weight management: Weight loss goals, personalized titration schemes, and new guidance for people with T1D
- 10. CV risk management and prevention for hypertension, ASCVD, CKD, and heart failure
- 11. Expanding kidney protection strategies through frequent monitoring, updated therapy landscape, and guidance for advanced CKD
- 12. GLP-1 RA recommendations for the treatment of MASH are tailored to reflect recent approvals
- 13. Microvascular complications: An emphasis on early, holistic care for the eyes and limbs
-
Big Picture
- 14. Systems to support population health: Stronger shared decisions and team-based support
- 15. Expanded staging, autoimmune screening, and cancer therapy-related guidance
- 16. CGM metrics for use in presymptomatic T1D are redefined alongside recommendations of metformin for cancer and steroid therapy
- 17. Multiple recommendations on health behaviors seek to help patients facilitate their diabetes management
- 18. Further emphasis on comprehensive medical evaluation and assessment of comorbidities for diabetes care
- 19. The ADA updates guidance on diabetes management in older adults, including CGM for insulin-treated T2D and expanded assessment guidance
- 20. Increasing differentiation of T1D and T2D guidelines for children and adolescents, with greater emphasis on patient education
Diabetes Technology
1. ADA expands eligibility for CGM and reframes device categories
The 2026 Standards of Care introduce more expansive recommendations with broader eligibility for CGM use across treatment regimens. Recommendation 7.15 now states that CGM “is recommended at diabetes onset and anytime thereafter for children, adolescents, and adults on insulin therapy” (Level A). The recommendation further expands eligibility to include individuals on non-insulin therapies that may cause hypoglycemia (Level C) and for any diabetes treatment where CGM helps in management (Level C). This marks a notable shift from the 2025 Standards of Care, which advised healthcare providers to “consider” CGM in adults with T2D on non-insulin therapy, even those with increased risk of hypoglycemia. Compared with 2025 language, the 2026 recommendations reflect a more universal stance that CGM should be available across the spectrum of diabetes therapies, with device choice tailored to individual needs and circumstances, such as insurance coverage or access (Level E). For people using CGM, the ADA maintained subsequent recommendations, reiterating the importance of daily use when possible (Recommendation 7.16), uninterrupted access to supplies (Recommendation 7.16), proactive management of skin reactions (Recommendation 7.19), and education on accuracy and interfering substances (Recommendation 7.20).
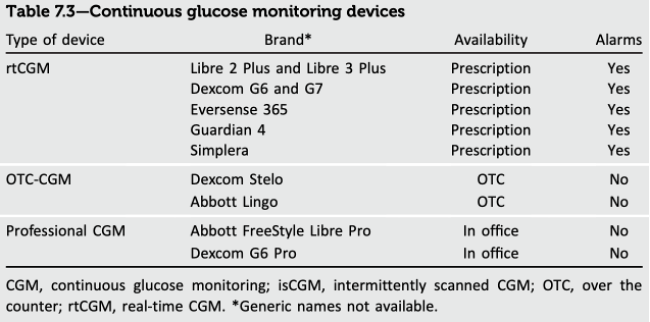
- The ADA reframed CGM definitions by revising Table 7.3, distinguishing among: (i) prescription real-time CGM (rtCGM); (ii) over-the-counter (OTC)-CGM; (iii) and professional CGM, now listing specific brands, availability channels, and alarm functionality within each category. Prescription rtCGM for diabetes management includes (i) Freestyle Libre 2 Plus and Freestyle Libre 3 Plus; (ii) Dexcom G6 and G7; (iii) Eversense 365; (iv) Guardian 4; and (v) Simplera, all of which have alarms. Dexcom’s Stelo and Abbott’s Lingo remain the two OTC-CGMs options, both without alarms. For professional CGMs applied and obtained only in office, Abbott’s Freestyle Libre Pro and Dexcom’s G6 Pro are listed, both without alarms. Notably, the revised table reorganizes CGM by prescription vs. OTC availability rather than rtCGM vs. intermittently scanned CGM (isCGM) as in the previous table structure. The 2026 Standards acknowledge that “most available prescribed CGM devices have similar characteristics,” such as continuous data transmission and alerts with no scanning required and described iCGM-based systems as older options.
- OTC CGM options received expanded contextual explanation in 2026, including clarification that these sensors, Dexcom’s Stelo and Abbott’s Lingo, can be used by “those without diabetes or with prediabetes who wish to assess their glycemic responses to lifestyles.” The ADA also specifies that because OTC CGM devices lack alarms they can be used by “people not taking diabetes medications that increase the risk of hypoglycemia.” This is a more explicit description than in 2025, where OTC CGM was defined by lack of alarms and use for people with prediabetes or diabetes not using insulin.
- Following a great deal of movement on the interoperability front this year, the detailed 2025 list of specific AID integrations with CGM systems is removed in 2026. The 2026 Standard states that “the exact CGM that integrates with any given device varies, and available options should be explored with individuals when choosing an integrated system.” This shift in framing suggests an effort to maintain generality in recommendations amid a rapidly evolving device landscape.
- Recommendations for CGM use in 2026 continue to be supported by largely the same RCTs and real-world evidence cited in the 2025 Standards of Care, with added emphasis on the consistency of benefit across diverse populations. The ADA now explicitly notes that the benefits of CGM “have been shown regardless of age, sex, education or income levels, or baseline diabetes characteristics,” supporting CGM as a core diabetes technology for diverse populations.
2. ADA’s recommendations for AID use in T2D strengthens
The 2026 Standards of Care reaffirmed the critical role of AID systems for individuals with T1D and strengthened recommendations for insulin pump use in T2D. Recommendation 7.25a designates AID systems as “the preferred insulin delivery system” for all people with T1D, as well as for adults and children with T2D who are currently using MDI, insulin pumps, or sensor-augmented pump therapy. In contrast, the 2025 Standards of Care had specified that AID systems “should be the preferred insulin delivery method to improve glycemic outcomes and reduce hypoglycemia and disparities in youth and adults with T1D” (Recommendation 7.26; Level A), and “insulin pump therapy, preferably with CGM, should be offered” to youth and adults with T2D on MDI who can safely use the device (Recommendation 7.27; Level A). This sentiment is reiterated in Recommendation 9.27, which was changed to recommend offering AID for all adults with T1D and T2D on insulin, depending on patient and provider preferences. Furthermore, Recommendation 7.25a now says that AID systems are the “preferred insulin delivery system” for individuals with other forms of insulin-deficient diabetes beyond T1D (Level B, C, D, E; previously just Level E). Additionally, Recommendation 7.25b introduces a new point, suggesting that AID systems can be “considered” for individuals with T2D on basal insulin who are not meeting their glycemic targets.
- These strengthened recommendations are driven by the incorporation of new pivotal data for additional AID systems. For T2D, the Standards of Care now cite two significant clinical trials: Tandem’s 2IQP trial and Insulet’s SECURE-T2D trial. Both were published this year and supported FDA clearance for their respective AID systems for use in adults with T2D.
- For reference, in August 2024, Insulet announced that Omnipod 5 received FDA clearance for use by individuals with T2D on intensive insulin or basal-only insulin therapy. With this clearance, Omnipod 5 became the first AID system to receive marketing authorization for T2D, marking a transformative moment for diabetes management among individuals with T2D on insulin. Multiple other major insulin pump manufacturers soon joined. In February 2025, the FDA cleared Control-IQ+ for use by individuals with type 2 diabetes (T2D) aged 18 years and older. Control-IQ+ is cleared for all individuals with T2D on insulin therapy. In September 2025, Medtronic also received approval from the FDA for the use of MiniMed 780G in T2D.
3. Strengthening early initiation and education in diabetes technology
Section 7 of the 2026 Standards of Care brought forward several key updates to diabetes device principles, including a more explicit focus on the early initiation of CGM and AID systems across all diabetes types, beginning at diagnosis. As part of a notable addition, the opening sentence of the “Initiation of Device Use” section in the 2026 Standards of Care now states that diabetes technology “should be initiated soon after the time of diagnosis and anytime thereafter.” This is a more definitive recommendation compared to the section’s opening sentence in the 2025 Standards of Care (which is still present in the 2026 iteration, just now as the second sentence), which stated that CGM and BGM “should be considered from the outset of the diagnosis of diabetes that requires insulin management.” Additionally, the 2026 recommendations present a more direct stance on the early initiation of AID systems, stating clearly that early use of AID therapy “has been shown to be beneficial.” In contrast, the 2025 Standards of Care suggested that early initiation of AID systems or insulin pumps “should be considered, especially in youth.” Further supporting early AID adoption, the 2026 Standards include a new recommendation (7.8a) that removes previous requirements for C-peptide levels (Level B), islet autoantibody presence (Level B), or duration of insulin therapy (Level C) before initiating insulin pump or AID therapy. This sentiment on C-peptide levels was stated in the discussion section of the 2025 Standards of Care for individuals with T2D, but now warrants its own recommendation. Section 9 also includes recommendations to initiate CGM early, with Recommendation 9.25 being updated to recommend CGM at the time of diabetes onset for adults with diabetes on insulin therapy, on noninsulin therapies that can cause hypoglycemia, or on any course of diabetes management where CGM aids in management. The choice of device should be based on the individual’s circumstances, preferences, and needs. Previous recommendations focused on combination therapy including insulin and GLP-1 RAs.
- The 2026 Standards of Care also reiterated the critical role of education in the initiation and continued use of diabetes technology. The 2026 recommendations now separate education guidelines for CGM and AID system;Recommendation 7.3b, for example, specifically outlines that when prescribing an AID system, healthcare providers must ensure that people with diabetes and their caregivers receive thorough training. This includes education on how to use and troubleshoot the system, as well as how to leverage integrated data to monitor and adjust therapy. The discussion section includes more detail to further emphasize the need for detailed training on AID systems, highlighting that while some youthwith T1D have successfully self-initiated tubeless AID systems, most individuals still require guidance from a certified diabetes care and education specialist (CDCES). The recommendations also reiterated the ongoing need for education among healthcare professionals about the availability, recommended use, and periodic software/hardware updates of diabetes devices, underscoring the rapidly evolving landscape of diabetes technology.
- Simultaneously, the 2026 Standards of Care also appears to adopt a slightly more cautious tone in Recommendation 7.8. Specifically, it altered language that clinicians should “consider” (2026) insulin pump and AID depending on caregiver’s needs and preferences (Level C), compared to the ADA “recommending” insulin pump and AID depending on caregiver’s needs and preferences (Level C). While this represents a nuanced change, we wonder if this reflects the ADA’s effort to balance growing evidence supporting early pump and AID use with real-world barriers such as device burden, caregiver capacity, health literacy, and insurance constraints.
4. AID and CGM in pregnancy: ADA adds new RCT evidence and clarifies expanded use cases for AID
The 2026 Standards of Care expand pregnancy guidance for both CGM and AID by incorporating new RCT evidence in GDM, clarifying evidence gaps for T2D pregnancy, and adding new considerations for how AID may be used during pregnancy and postpartum.
- For CGM, the ADA maintains Recommendation 15.10 for pregnant individuals with T1D (Levels A and B) but expands its discussion of CGM use in T2D and GDM pregnancies. While the ADA continues to state that evidence is insufficient to recommend CGM for all pregnant women with T2D or GDM, the 2026 Standards of Care updates findings from two recent RCTs in GDM. The DipGluMo RCT (n=302) found no difference in composite perinatal outcomes between CGM and BGM in GDM, although CGM use was preferred by participants, while in contrast, another RCT (n=111) showed higher 24-hour TIR and lower mean glucose with CGM use compared to standard care.
- As in 2025, the ADA stated that adequately powered RCTs exclusively evaluating CGM use in pregnant individuals with T2D are currently not available and that CGM-based glycemic targets for T2D and GDM have not yet been defined. It was reiterated from 2025 that CGM use in individuals with T2D or GDM should be individualized based on treatment plan, pregnancy context, and patient preferences.
- Recommendations allowing CGM metrics to be used alongside BGM (15.12; Level E) and warning against use of estimated A1c or GMI in pregnancy (15.3; Level C) remain unchanged.
- There was great focus on the challenges of AID use in pregnancy, emphasizing that nearly all FDA-cleared systems still rely on glucose targets higher than the goals recommended in pregnancy and lack pregnancy-specific algorithms. The ADA again notes that one pregnancy-specific AID system is FDA-approved but not commercially available in the US, referring to the CamAPS FX system, approved in May 2024. While recommendations (15.19 and 15.20) remain unchanged, the ADA adds new guidance stating that some pregnant individuals with T1D may derive glycemic benefit from AID systems not approved for pregnancy, such as reduced hypoglycemia or improved TIR, when carefully selected and counseled about individual risks and benefits.
- Recommendation 15.19 continues to support AID systems with pregnancy-specific glucose targets for pregnant individuals with T1D (Level A), supported by the AiDAPT study results showing an additional 2.5 hours/day in Range (68%), 20% lower TAR, and 0.3% lower A1c compared with standard care. Recommendation 15.20 remains unchanged, but with extended guidance for assistive techniques in non-pregnancy-specific AID systems. It was stated that assistive techniques may include strategic switching between SAP or manual mode and automated mode at different times of day or stages of pregnancy to achieve intended glycemic goals.
- The ADA also incorporates new intrapartum and postpartum data. A prespecified analysis (n=95) showed improved intrapartum TIR and similar early postpartum TIR with AID compared with standard insulin therapy without severe hypoglycemia. A six-month postpartum extension of AiDAPT (n=57) demonstrated higher TIR and lower mean glucose with AID, again without differences in hypoglycemia. Strategies for postpartum adjustment of AID pump settings have now been described.
5. Specific perioperative care recommendations provided for hospitalization and surgery
Hospital care related to diabetes remains challenging, for both diabetes-related and non-diabetes related hospitalizations such as elective surgery. A new section on perioperative care was added this year to discuss glycemic goals before, during, and after surgery or hospitalization. Previously, perioperative care was discussed without the inclusion of specific recommendations.
- Recommendation 16.14 was added to recommend a preoperative A1c goal of ≤8.0% in the three months preceding surgery. An individualized risk-to-benefit assessment should be performed as well, and a 14-day GMI metric of ≤8.0% or Time in Range of ≥50% may also be used.
- Recommendation 16.15 was added to recommend the monitoring and maintenance of blood glucose levels between 100 and 180 mg/dL before, during, and after surgery. Specific goals may also differ on an individual level depending on the surgery, risk of hypoglycemia, and glucose-lowering therapies taken by the patient.
- Recommendation 16.18 was updated to consider the needs of patients not being discharged to their home. Previously, a structured discharge plan tailored to the individual was recommended. Now, the capabilities of the facility caring for patients with diabetes after discharge should be specifically considered.
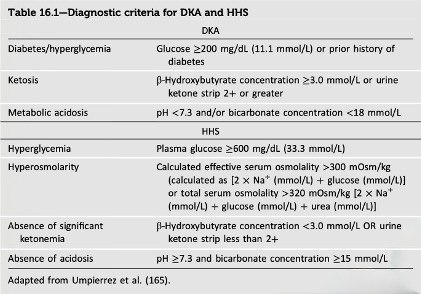
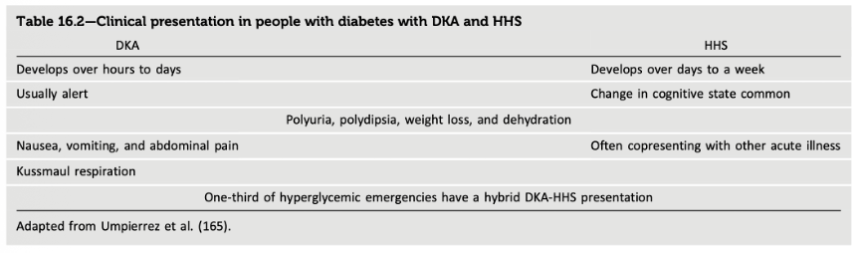
- Tables 16.1-16.2 were added to detail specific criteria for assessing DKA and hyperglycemic hyperosmolar state (HHS; see below). Previously, only management suggestions such as the administration of intravenous fluids, insulin, and electrolytes were provided.
6. Diabetes device support: The ADA simplifies recommendations on device support for youth and reiterates recommendations on open-source AID
Section 7 of the 2026 Standards of Care simplified its recommendations regarding the support of children and adolescents in school settings. Recommendation 7.6 specifies that these individuals should receive support in using diabetes technology, including AID systems, at school; the recommendation previously stated that “students” should be supported in this way “as recommended or prescribed by their health care team.” Recommendation 7.7, meanwhile, now extends this guidance to individuals aged ≥18 years, stating that they should receive reasonable accommodations in educational and work settings to manage their devices and respond to high or low glucose levels.
- Additionally, the ADA has also maintained its previously strengthened and streamlined recommendations regarding open-source AID systems. In the 2025 Standards of Care, the ADA had updated its language to specify that “open-source automated insulin dosing is the preferred term when referring to any open-source system,” moving away from the “do-it-yourself” label used in prior versions. This change reflects both evolving language preferences and advocacy from the open-source community. The ADA continues to recommend that healthcare providers “support and provide diabetes management advice” to individuals using open-source systems, maintaining the Level B evidence grade in the 2025 Standards of Care, strengthened from Level E in years past. However, the 2026 Standards of Care expand on the real-world data supporting open-source AID systems, now citing large-scale studies involving the OpenAPS heuristic algorithm, as well as a multicenter RCT supporting open-source use in T1D.
Diabetes Therapy
7. Broader range of conditions such as CKD, MASLD, and post-transplantation diabetes now included for incretins
Section 9 of the 2025 Standards of Care was updated with new treatment algorithm for comorbidities, including heart failure, chronic kidney disease (CKD), and MASH/MASLD. Notably, GLP-1 RAs have been newly recommended across all of these indications, based on clinical trial results and approvals. Section 9 also included a few updated recommendations for diabetes technology use, as noted above.
- Recommendations 9.9a and 9.9b were newly added this year to recommend the use of a GLP-1 RA or a dual GLP-1/GIP RA with demonstrated benefit for HF in adults with T2D, obesity, and symptomatic heart failure with preserved ejection fraction (HFpEF). Per the updated Standards, this should occur regardless of A1c values. Previously, recommendations had focused on the incorporation of SGLT-2 inhibitors.
- In September 2024, semaglutide received a positive recommendation by the European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) for a label update to reflect its efficacy on HF, based on the results from STEP HFpEF (n=529) and STEP HFpEF-DM (n=616). Novo Nordisk has also submitted an application for this indication to the US FDA.
- In November 2024, full results of the phase 3 SUMMIT trial (n=731), which evaluated tirzepatide (5 mg, 10 mg, or 15 mg) in adults with HFpEF and obesity were presented. At 52 weeks, tirzepatide achieved statically significant improvements in both primary endpoints, with a reduction in the risk of heart failure outcomes and improvements in heart failure symptoms and physical limitations compared to placebo.
- Recommendation 9.11 was updated to include recommendations for adults with T2D and advanced CKD (eGFR <30 mL/min/1.73 m2). GLP-1 RAs are preferred for glycemic management due to lower risk of hypoglycemia and proven cardiovascular benefit. Individuals on dialysis can be initiated or continued on this therapy.
- Recommendation 9.12 was updated to include recommendations around MASLD. For adults with T2D, MASLD, and overweight or obesity, GLP-1 RAs with benefits for MASH should be considered, or a dual GLP-1/GIP-1 RA with proven benefits.
- Recommendation 9.13a was changed to recommend a GLP-1 RA for glycemic management over a pioglitazone or dual GLP-1/GIP RA for adults with T2D and biopsy-proven MASH.
- Recommendation 9.24 was significantly updated to include healthy behaviors, DSMES, avoidance of therapeutic inertia, and social determinants of health as essential parts of the treatment plan for all PWD in addition to pharmacotherapy.
The Standards also offered insights on more specific populations, such as people undergoing cancer treatment, those on glucocorticoid treatment, and those with post-transplantation diabetes. Specifically, Recommendations 9.33-9.35b were updated with recommendations for glycemic management during cancer treatment. Individuals who develop hyperglycemia through immunotherapy should be assessed for the immediate initiation of insulin therapy due to the risk of DKA. Metformin should be considered in cases of hyperglycemia due to mTOR inhibitors or PI3K inhibitors. However, use of insulin should be reserved for severe cases for patients taking PI3K inhibitors due to potential efficacy impacts.
- Recommendation 9.36 was added for individuals undergoing glucocorticoid treatment. Additional glucose-lowering therapies should be adjusted or initiated to maintain individual glycemic goals.
- Recommendations 9.37-9.38c discuss post-transplantation diabetes. Insulin is preferred in a postoperative setting, or a DPP-4 inhibitor can be considered for mild hyperglycemia. Medication selection may differ based on the transplanted organ, and non-insulin therapies may also be considered for long-term management. A GLP-1 RA may also be considered for long-term cardiometabolic benefit. If long-term goals cannot be maintained, consider adding insulin.
8. Outpatient prevention and management of acute hyperglycemic crises, including DKA
In Section 6, the ADA expanded guidance on setting glycemic goals and managing hypoglycemia and hyperglycemic crises. The subsection on hyperglycemic crises, which was first introduced last year, has been expanded to address increasing incidence of life-threatening DKA and hyperglycemic hyperosmolar state (HHS)[1], with updates centered on outpatient prevention and management. Notably, Table 6.8, “Diagnostic criteria for DKA and HHS,” from last year’s Standards of Care was removed.
- On monitoring, guidelines support the use of blood ketone monitoring in place of urine ketone monitoring for individuals at risk of DKA, evidenced by a 6-month RCT which demonstrated a ~50% reduction in hospitalization risk.
- On the risk assessment, expanded guidelines now include additional factors associated with increased rates of DKA: (i) female sex; (ii) belonging to an underrepresented racial or migratory group; (iii) greater A1c; (iv) greater daily insulin intake; (v) public insurance; (vi) aged 10-14 years; and (vii) a prior episode of DKA.
- On management, guidance now indicates that individuals at risk of DKA should immediately seek medical attention if: (i) they are unable to tolerate oral hydration; (ii) experience ongoing emesis; (iii) unable to improve blood glucose and/or ketone levels with insulin; (iv) experience altered mental status; and (v) show signs of worsening illness.
The subsection, “Incurrent Illness,” was updated to include criteria on specific classes of diabetes medication during acute crisis. Clinicians should consider holding: (i) metformin and SGLT-2 inhibitors when oral intake cannot be maintained or during a potential acute kidney injury; (ii) GLP-1 RAs in illnesses with significant gastrointestinal symptoms; (iii) thiazolidinediones during heart failure exacerbation or other conditions with associated hypervolemia; (iv) sulfonylureas when prescribing select antimicrobials.
- Recommendation 6.17 was added to promote the addition of oral glucose to first aid kits in institutions and public settings for the treatment of acute hypoglycemia.
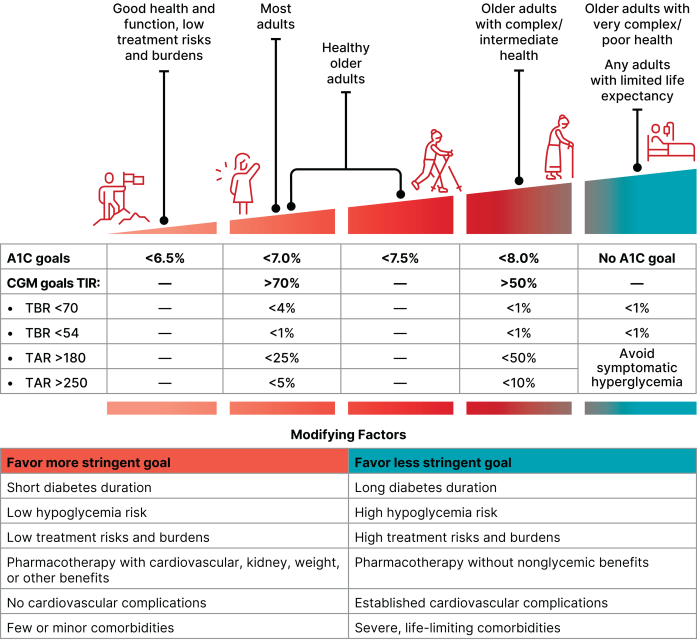
Finally, the Standards continued to endorse personal care. Figure 6.1 was expanded to include individual glycemic goals based on CGM metrics, health status, and other “person- and treatment-specific factors.”
9. Obesity and weight management: Weight loss goals, personalized titration schemes, and new guidance for people with T1D
In the obesity and weight management section (Section 8), the ADA updated guidelines on screening, treatment goals, alternative lifestyle programs, and treatment options for weight loss, including two new recommendations on individualized dose titration for obesity pharmacotherapy and weight management options for people with T1D. On screening and monitoring, Standards of Care now recommends annual screening for overweight or obesity using BMI. Furthermore, additional assessments, including anthropometric measures like waist-to-hip ratio or direct measures like dual-energy X-ray absorptiometry (DEXA) or bioelectrical impedance analysis, should be used to confirm excess adiposity, if feasible (Recommendation 8.2a). This emphasis on anthropometric measures reflects similar recommendations by the Lancet Diabetes & Endocrinology Commission’s new diagnostic criteria. On treatment goals, Recommendation 8.5 clarifies that weight loss of 5-7% of baseline weight, rather than 3-7% from last year’s Standards of Care, improves glycemia and other immediate cardiovascular (CV) risk factors.
- On lifestyle changes, Standards of Care maintained its recommendation for high-frequency counseling for nutrition and physical activity when available (Recommendation 8.8a). Recommendation 8.8b was updated to further clarify that alternative lifestyle programs, such as remote or telehealth visits and mobile app, could be considered when the former is limited. Recommendation 8.14 was updated to suggest regular counseling and monitoring to ensure that individuals aiming to lose weight are getting adequate nutrition, including protein and micronutrients.
- On pharmacotherapy, the newly added Recommendation 8.20 stresses the importance of personalized dose titration scheme to balance efficacy, health benefits, and tolerability. Importantly, optimal treatment dose may not be the maximum approved dose. This inclusion echoes sentiment from a symposium from ADA 2025 on the new Standards of Care for Obesity. In the symposium, speakers univocally emphasized that patients have different treatment goals and respond to drugs differently, and that dosage for obesity pharmacotherapy should be tailored to individuals.
- Recommendation 8.21 was revised to encourage combination treatment for people with diabetes not reaching weight loss goals. Other interventions include lifestyle management programs, metabolic surgery, and alternative pharmacologic agents, such as phentermine, orlistat, phentermine/topiramate, and naltrexone/bupropion.
- On concomitant medications, Recommendation 8.15 encourages clinicians to collaborate with other care team members and minimize the use of weight-promoting drugs. These include antipsychotics, antidepressants, glucocorticoids, injectable progestins, and some anticonvulsants. The ADA states that such use could counteract the effectiveness of weight loss drugs in people with diabetes.
- Table 8.2 has been updated with costs of obesity pharmacotherapies as of July 2025.
- In people with T1D, a new section, “Treatment of Obesity in Type 1 Diabetes” has been added. In this section, Recommendation 8.29 supports obesity management strategies used for general adult population, such as incretin-based therapies (Class B) and metabolic surgery (Class C), in adults with T1D with BMI ≥30 kg/m2 or BMI ≥27.5 kg/m2 in Asian Americans. This update is based on a high prevalence of overweight (30-40%) and obesity (15-30%) for people with T1D – comparable to the general adult population – as well as clinical trials and observational studies. The Standards of Care further emphasizes that when initiating GLP-1 RAs or dual GIP/GLP-1 RAs, patients should be counseled about: (i) increased risk of hypoglycemia and reduction in insulin requirements; (ii) the importance of maintaining carbohydrate intake; and (iii) routine testing of excess ketone body production. Moreover, dose titration for people with T1D should be approached with close monitoring in insulin requirements and hypoglycemic events.
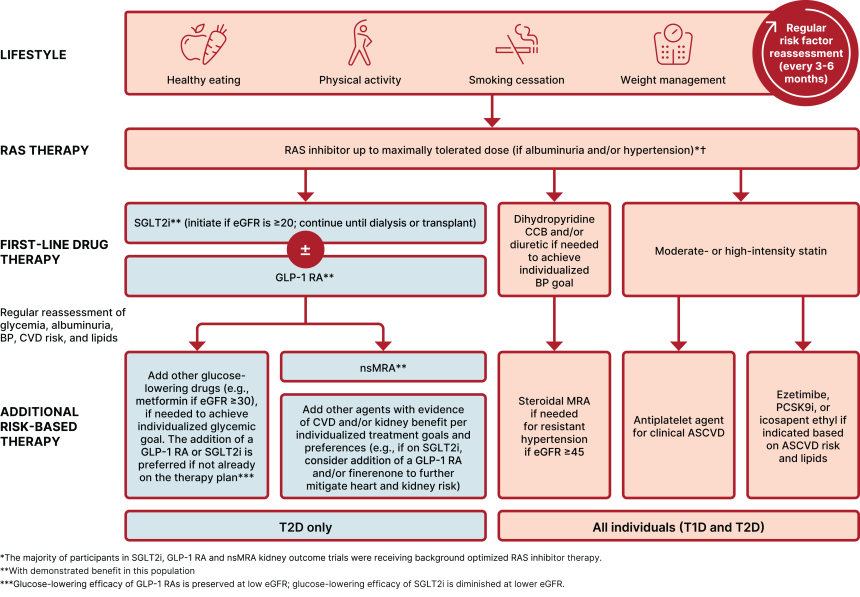
10. CV risk management and prevention for hypertension, ASCVD, CKD, and heart failure
Section 10 on cardiovascular disease (CVD) and risk management included several updates, most extensively on GLP-1 RA and mineralocorticoid receptor antagonist (MRA) use in people with T2D and chronic kidney disease (CKD) or heart failure (HF). The ADA also modified recommendations for: (i) screening frequency for eGFR and uACR; (ii) systolic blood pressure (SBP) target; and (iii) treatment algorithm for lipid management.
- In people with T2D and CKD, several recommendations were modified to specify screening frequency and management strategies. Recommendation 10.11 newly suggests monitoring for drop in eGFR, in addition to increase in serum potassium levels, when using ACE inhibitors, ARBs, and MRAs for the treatment of hypertension or CKD (severely increased albuminuria and/or eGFR <60 mL/min/1.73 m2). On therapies, Recommendation 10.40c was added to include recommendation for GLP-1 RAs in people with T2D and ASCVD or CKD based on clinical trial results, including the phase 3 FLOW trial, in which semaglutide reduced kidney disease progression and kidney or CV-related death by 24% in people with T2D and CKD.
- On heart failure, GLP-1 RAs and nonsteroidal MRA (nsMRA) emerged as important therapies for prevention and management. Recommendation 10.44c was revised to include GLP-1 RAs, in addition to SGLT-2 inhibitors, for prevention of HF in people with T2D and asymptomatic HF. Moreover, Recommendation 10.44d and Recommendation 10.44e were added and revised, respectively, to clarify benefits of dual GLP-1/GIP RA on HF events and symptoms, as well as GLP-1 RAs on symptoms for people with T2D, obesity, and symptomatic HF with preserved ejection fraction (HFpEF). These updates are based on the STEP HFpEF-DM and SUMMIT trial results. For the treatment of more advanced HF, nsMRA was newly added to Recommendation 10.44h for reducing worsening HF events for people with diabetes and HFpEF or HF with mildly reduced ejection fraction (HFmrEF). Figure 10.5 was added to provide an overview of prevention and treatment algorithm for symptomatic HF in people with diabetes.
- On lipid management and blood pressure, Standards of Care provided greater clarity on therapeutic targets and treatment options. Recommendation 10.32 now advises against the use of fibrate, niacin, or dietary supplements containing n-3 fatty acids in people on statin therapy was, given the lack of additional CV benefits. Figure 10.6 was added to show prevention strategy of ASCVD in people with T2D. Importantly, for people with established or high ASCVD risk, high-intensity statin, GLP-1 RAs, and SGLT-2 inhibitors are recommended.
- On blood pressure, Recommendation 10.4 was revised to include a new systolic blood pressure (SBP) target of <120 mmHg for people with high CV or kidney risk. In the general population with diabetes, SBP <130/80 mmHg is recommended. Recommendation 10.6 was modified to emphasize the importance of titrating BP-lowering therapies for individualized treatment goals.
11. Expanding kidney protection strategies through frequent monitoring, updated therapy landscape, and guidance for advanced CKD
The chronic kidney disease (CKD) and risk management section (Section 11) of the Standards of Care shares updated guidelines to screening frequency, therapeutic algorithm, and safety monitoring. The updates include expanded use of SGLT-2 inhibitors and GLP-1 RAs, as well as clearer safety guidance for advanced CKD and pregnancy.
- On kidney function monitoring and blood pressure targets, Recommendation 11.1a now clarifies the frequency of kidney function assessment, reinforcing annual UACR and eGFR screening for most people with diabetes and risk-based monitoring (one to four times per year) based on CKD stage and albuminuria category. Moreover, Recommendation 11.5 provides blood pressure guidance, setting a goal of <130/80 mmHg and encouraging <120 mmHg systolic when safely achievable.
- On therapeutic guidance, Recommendation 11.6a clarifies substitution strategies for ACE inhibitors or ARBs in cases of intolerance, while 11.6b outlines monitoring protocols for eGFR decline and potassium shifts when initiating ACE inhibitors, ARBs, or MRAs. Recommendation 11.8 now emphasizes potassium monitoring one month after starting a nonsteroidal mineralocorticoid receptor antagonist (nsMRA), such as finerenone, as supported by FIDELIO-DKD and FIGARO-DKD, which demonstrated reductions in CKD progression and cardiovascular events.
- A new recommendation (11.9) supports simultaneous initiation of an SGLT-2 inhibitor and nsMRA in individuals with T2D, UACR ≥100 mg/g, and eGFR between 30-90 mL/min/1.73 m² already on RAS inhibitor therapy, reflecting synergistic benefit seen in CREDENCE, DAPA-CKD, and EMPA-KIDNEY trials. These trials expanded the evidence base for SGLT2 inhibitors, showing kidney and cardiovascular protection down to eGFR ≥20 mL/min/1.73 m² and in people with advanced albuminuria.
- Recommendation 11.11a affirms that SGLT-2 inhibitors may be continued safely in individuals with eGFR <20 mL/min/1.73 m² and not yet on dialysis. Recommendation 11.11b suggests GLP-1 RA use in people on dialysis for cardiovascular benefit, given that the agent is not dependent on kidney clearance. This reflects evidence from the FLOW trial of semaglutide, which demonstrated 24% reductions in kidney disease progression and death from kidney disease or CVD in people with T2D and CKD.
- Figure 11.2 has been updated to reflect that most participants in kidney outcome trials were on optimized RAS inhibitor therapy in the background, reinforcing its foundational role in CKD management.
- Pregnancy-related guidance is detailed in Recommendation 11.10, which is advised against kidney-protective agents that could potentially cause harm pregnant women or sexually active women of childbearing age who do not use reliable contraception.
12. GLP-1 RA recommendations for the treatment of MASH are tailored to reflect recent approvals
The comprehensive medical evaluation and assessment of comorbidities section (Section 4) was updated to reflect updates to FDA approvals for the treatment of MASH, as well as to enhance screening for MASLD risk in broader metabolic care.
- Recommendation 4.26 was updated to specifically recommend the use of GLP-1 RAs with demonstrated benefits in MASH for adults with T2D, MASLD, and overweight or obesity. Alternatively, the guidelines also recommend the use of a dual GLP-1/GIP RA with potential benefits in MASH. These are recommended alongside lifestyle interventions for weight loss for the treatment of obesity. Recall that in August 2025, the FDA approved Wegovy (semaglutide 2.4 mg) for MASH in adults with moderate to advanced liver fibrosis (stages F2 to F3 fibrosis). The approval was based on Part 1 of the phase 3 ESSENCE trial (n=1,200), in which Wegovy conferred a statistically significant and superior improvement in liver fibrosis, as well as resolution of steatohepatitis with no worsening of liver fibrosis compared to placebo. Wegovy is currently the only GLP-1 RA with FDA-approved liver benefit.
- Figure 4.3, the MASLD treatment algorithm, was also updated to recommend the use of GLP-1 RAs alongside resmetirom for patients with F2-F3 MASH.
- Recommendation 4.27a was tailored to recommend GLP-1 RAs for glycemic management for adults with T2D and biopsy-proven MASH, or those at high risk for liver fibrosis based on noninvasive tests. This decision was made due to the beneficial effects of GLP-1 RAs for MASH, and signals a shift from the 2025 recommendation, which favored either a pioglitazone, a GLP-1 RA, or a dual GLP-1/GIP RA. This year’s recommendation notes that pioglitazones or dual GLP-1/GIP RAs may also be considered but recommends GLP-1 RAs as the primary therapy.
- Figure 4.1, the decision cycle for person-centered glycemic management in T2D, was updated to include MASLD. Specific factors should be considered that impact treatment choice for T2D, including impact on weight, hypoglycemia, and cardiovascular and kidney protection as mentioned in 2025. This year, MASLD was added as a specific factor impacting treatment choice.
13. Microvascular complications: An emphasis on early, holistic care for the eyes and limbs
For microvascular complications, the ADA strengthened its emphasis on early, holistic care for retinopathy, neuropathy, and foot complications. Section 12 newly included results from the 40-year DCCT/EDIC (Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications) study, which found that early intensive glycemic management (A1c ~ 7%) offered microvascular benefits for ten years after A1c convergence, compared to conventional management (A1c ~ 9%). The Standards of Care cites a new concept, “metabolic memory,” which hypothesizes that longer period spent in normoglycemia has lasting effects even when A1c rises over time.
On eye health, the subsection, “Adjunctive Therapy,” discussed clinical considerations for aspirin, statins, pioglitazone, and rosiglitazone use. ADA specifies that aspirin does not increase the risk of retinal hemorrhage. It also recommends statins for people with T2D, including those with retinopathy at diagnosis. Pioglitazone and rosiglitazone may be associated with worsening diabetic macular edema (DME), however. On GLP-1 RAs, language was expanded to discuss mixed study results on whether the therapy is associated with the development of nonatretic anterior ischemic optic neuropathy, glaucoma, neovascular age-related macular degeneration (AMD), and diabetic retinopathy (DR) progression.
On neuropathy, Recommendation 12.22a was added to encourage the use of combination therapy for additional relief of neuropathic pain. Diagnosis criteria for neuropathy was updated to include the Ipswich touch test, aligning more closely with the “Foot Care” subsection.
On foot care, the ADA has strengthened its language on prevention and management of diabetic foot complications, describing it as a “a centerpiece of diabetes care.” Guidance was expanded on the Wound Ischemia foot Infection (WIfI) staging system for diabetic foot lesions to stage PAD severity, predict diabetic foot ulcer healing, and assess amputation risk. On treatment, adjunctive advanced therapies were identified to be particularly useful for diabetic foot ulcers unresponsive to care. Language was updated to underscore risk assessment and prompt management of complications, particularly infection.
On peripheral artery disease (PAD), language was expanded to emphasize holistic and interventional approaches in management people with diabetes and PAD. Emerging evidence was added for GLP-1 RA therapies, which have been shown to reduce lower-extremity amputations in the phase 3 STRIDE trial.
Big Picture
14. Systems to support population health: Stronger shared decisions and team-based support
- Strengthening shared decision-making and financial awareness. Recommendation 1.1 is revised to more explicitly incorporate “shared decision-making based on individual values,” preferences, prognoses, comorbidities, and informed financial considerations in all treatment decisions (Level B). While 2025 already highlighted the value of timely and evidence-based care within the context of social determinants, the 2026 update places a focus on shared decision-making as a structural requirement for high-quality population health systems.
- Embedding continuous quality improvement as a core system function. Recommendation 1.5 expands on last year’s focus by calling for a culture of “continuous” quality improvement, supported by benchmarking programs and interprofessional teams (Level A). This new emphasis on sustained quality improvement reflects the growing use of standardized workflows and real-time data systems to close gaps in care. Unlike 2025’s language, which emphasized implementing quality improvement initiatives, the 2026 standards stress the need for durable, scalable processes that health systems can refine over time.
- Expanding team-based support through digital tools and enhanced roles for older adult care. Two additional updates highlight the evolving structure of interprofessional teams. Recommendation 1.8 now explicitly includes “digital self-management tools or coaches” as appropriate sources of additional support, aligning with the Standards of Care with increasing use of remote coaching platforms and virtual DSMES models. Recommendation 1.9 expands the scope of community health workers (CHWs) to include support for kidney disease risk factors, extending their role beyond diabetes and cardiovascular disease to wider cardio-renal-metabolic field. (Levels A/B). Lastly, Table 1.1 is updated to specify additional team members whose expertise is especially relevant for older adults.
15. Expanded staging, autoimmune screening, and cancer therapy-related guidance
Section 2 of the 2026 Standard of Care introduces targeted changes to diabetes diagnosis, including a sharper focus on the early identification of T1D, refined protocols for cancer therapy-induced hyperglycemia, and expanded staging language that better reflects evolving clinical practice.
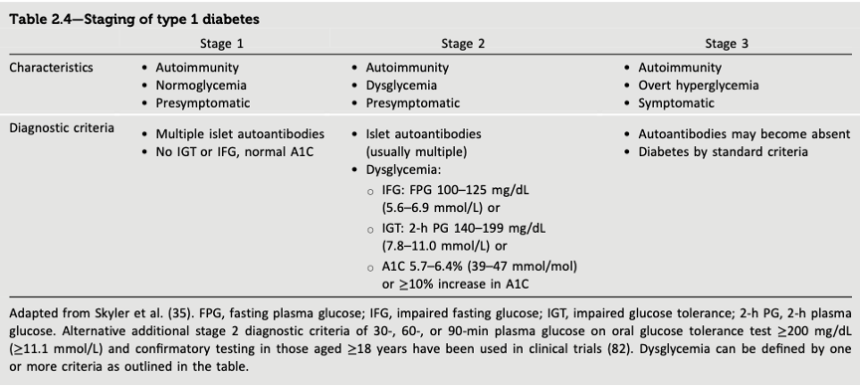
- The changes include clarification of T1D staging and autoantibody screening. Recommendation 2.8 was split into two components to emphasize prompt evaluation for stage 3 T1D in individuals with one or more islet autoantibodies. The update reinforces the importance of early metabolic testing to avoid delays in diagnosis and treatment. Recommendation 2.8b, meanwhile, maintains guidance for referral to specialized centers for individuals with multiple autoantibodies and no overt diabetes symptoms. Supporting data from Table 2.4 formalize the three-stage model of T1D in the ADA Standards of Care.
- Section 2 also includes new guidance for cancer therapy-induced diabetes. Recommendations 2.19–2.22 introduce structured screening protocols tailored to specific classes of anticancer therapies, reflecting growing recognition of treatment-induced hyperglycemia.
- Recommendation 2.19 (ICIs, PI3K, mTOR inhibitors): People initiating immune checkpoint inhibitors (anti–PD-1/PD-L1), PI3K inhibitors, or mTOR inhibitors should receive counseling and education on the risk of hyperglycemia and hyperglycemic crises, with emphasis on symptom recognition and early detection.
- Recommendation 2.20 (ICIs): Individuals treated with ICIs should have fasting or random plasma glucose checked before treatment initiation and at each visit, or if symptoms of hyperglycemia develop during or after therapy.
- Recommendation 2.21 (PI3K inhibitors): For those starting PI3K inhibitors, fasting or random plasma glucose and A1c should be measured before treatment, with weekly random glucose checks during the first two weeks and every four weeks afterwards. A1c should be reassessed every three months during the course of the therapy.
- Recommendation 2.22 (mTOR inhibitors): In people treated with mTOR inhibitors, fasting or random plasma glucose should be measured before therapy and at each visit throughout treatment, with A1c considered every three months.
- Expanded monitoring for glucocorticoid-induced hyperglycemia. Recommendation 2.18 reinforces the need to monitor postprandial or random plasma glucose in individuals receiving long-term or recurrent glucocorticoid therapy. This update reflects evidence that fasting glucose may underdiagnose steroid-induced hyperglycemia.
- Supporting updates reinforce staging and confirmatory testing. Recommendation 2.9 introduces guidance for individuals with a single confirmed IA-2 autoantibody, recommending monitoring similar to multi-antibody-positive individuals due to a comparable risk of progression. The recommendation suggests repeat antibody testing every six months to three years for people with a single confirmed islet autoantibody.
16. CGM metrics for use in presymptomatic T1D are redefined alongside recommendations of metformin for cancer and steroid therapy
Section 3 introduces targeted updates to risk monitoring, lifestyle guidance, and pharmacologic prevention,including new recommendations for individuals receiving PI3Kα inhibitors or high-dose glucocorticoids, primarily for cancer treatment. These changes reflect a broader prevention framework that now spans T1D and T2D, therapy-induced hyperglycemia, and cardiovascular risk.
- Enhanced presymptomatic T1D monitoring. Recommendation 3.2 was modified to include that CGM metrics may now be considered alongside A1c values and oral glucose tolerance test (OGTT) scores in individuals with presymptomatic T1D depending on age, autoantibody profile, and glycemic status.
- Clarified referral and weight-loss targets. Recommendation 3.3 now clarifies that people with overweight or obesity and also at high risk of T2D should be referred to a diabetes prevention program to achieve and maintain ≥5–7% body weight reduction. This should be achieved through a reduction in calorie consumption and ≥150 minutes per week of moderate physical activity. Recommendation 3.4 now emphasizes the importance of dietary patterns with the strongest established evidence base for reducing T2D, specifically Mediterranean and low-carbohydrate dietary approaches.
- Recommendation 3.6 clarifies that certified technology-assisted diabetes prevention programs delivered via smartphones, web apps, or telehealth are now explicitly supported based on individual preferences.
- Proactive metformin for therapy-induced hyperglycemia. Recommendation 3.8 was added this year, stating that metformin may be considered to prevent hyperglycemia in high-risk individuals receiving PI3Kα inhibitors for which hyperglycemia is a common dose-limiting adverse event. Recommendation 3.9 was also newly added and states that metformin may be considered to prevent hyperglycemia in individuals receiving high-dose or long-duration glucocorticoid therapy, especially when additional diabetes risk factors are present.
17. Multiple recommendations on health behaviors seek to help patients facilitate their diabetes management
With a focus on the behaviors that drive health outcomes, the ADA updated Section 5 with multiple recommendations on how to help patients facilitate their own diabetes management. One of the important revisions in this section includes Recommendation 5.4, which has been updated to encourage the use of DSMES to support and meaningfully engage in beneficial health behaviors. This update reflects the idea that HCPs shouldn’t only be responsible for providing health information but also addressing behavior-change techniques to help patients adopt and maintain healthy lifestyle changes. Additionally, Recommendation 5.5 has been modified to state that DSMES should be culturally and socially appropriate, based on the patient's preferences and needs. Furthermore, it states that DSMES participation should be communicated to the entire diabetes care team, reinforcing the importance of interdisciplinary work.
- With a greater focus on weight loss, Recommendation 5.12 has been revised to advise that an overweight or obesity treatment plan, including nutrition, physical activity, and behavioral health support, should be provided and aim for at least a 5-7% weight loss from baseline body weight. Previously, this recommendation applied to those aiming for at least 3-7% weight loss. Also regarding weight loss, Recommendation 5.23 was amended to recommend counseling and regular monitoring for individuals pursuing intentional weight loss, with emphasis on adequate nutrition intake. The focus on this educational intervention includes attention to preventing protein insufficiency and micronutrient deficiency. Recommendation 5.34 was also modified to encourage greater physical activity, with the goal of more patients meeting current activity guidelines. In particular, HCPs are advised to tell patients that prolonged sitting should be interrupted at least every 30 minutes for blood glucose and other benefits.
- On mental health, Recommendation 5.45 has been updated to suggest referral to a behavioral health professional if diabetes distress has not been adequately addressed during an appointment. Furthermore, Recommendation 5.46 was updated to recommend screening for anxiety symptoms at least annually in people with diabetes, and HCPs are encouraged to address anxiety symptoms within the scope of their practice.
- Focusing on complications, Recommendation 5.47 was updated to suggest screening in individuals at high risk for hypoglycemia or with severe or frequent hypoglycemia for fear of hypoglycemia. This screening is recommended at least annually or when clinically indicated to prevent avoidance of glucose-lowering interventions. Finally, Recommendation 5.56 was amended to encourage screening for sleep health in people with diabetes and those at risk. This update aims to understand and address challenges in diabetes self-management that interfere with sleep.
18. Further emphasis on comprehensive medical evaluation and assessment of comorbidities for diabetes care
The 2026 Standards of Care provides several updates on comprehensive medical evaluation and assessment of comorbidities (Section 4). Previously, the Standards of Care emphasized the importance of assessing glycemic status and previous treatments for people with diabetes. The updated Recommendation 4.3 now encourages a more comprehensive assessment for initial visits and follow-up appointments. Furthermore, Recommendation 4.4 emphasizes the identification of available resources, in addition to the previously mentioned care partners and support systems for diabetes management. The focus of this section remains on engaging other members of the healthcare team to support comprehensive data care, along with referrals for appropriate screening of complications, comorbidities, and treatment efficacy. Overall, the document reminds that glycemic management is a part but not the only goal of clinical encounters.
- Updates include greater focus and refinement on bone health. Recommendation 4.13a was revised to recommend considering an osteoporosis drug in older adults with an increased risk of fracture with a T-score ≤-2.5. As background, the fracture risk in people with T1D increases 4.35 times for hip fractures, 1.83 times for upper-limb fractures, and 1.97 times for ankle fractures. These risks are further exacerbated in people with T1D with microvascular complications or neuropathy compared to those without. Similarly, in people with T2D, hip fracture risk is increased by 1.79 times, and overall risk throughout their lifetime is 40-70% higher than in people without diabetes. As the risk of fractures increases with age, the addition of an osteoporosis drug may help alleviate further complications.
- Additionally, Recommendation 4.13b was added to state that treatment (e.g., alendronate, risedronate, ibandronate, or denosumab) may be considered in adults with diabetes who have a T-score between -2.0 and -2.5, in the presence of additional fracture risk. This recommendation was added because the T-score underestimates the fracture risk in people with diabetes, as it doesn’t capture diabetes-related impairments in bone quality or fall risk.
19. The ADA updates guidance on diabetes management in older adults, including CGM for insulin-treated T2D and expanded assessment guidance
Importantly, the 2026 Standards of Care features more specific guidance for older adults with diabetes and geriatric syndromes or other functional impairments.
- Expanding its guidance on hypoglycemia management, Recommendation 13.5 has been updated to now recommend CGM for older adults with insulin-treated T2D, building on its previous recommendations for T1D (also reflected in the updated recommendations to Section 7 noted above) to reduce treatment burden and improve glycemic outcomes.
- On blood pressure treatment goals, Recommendation 13.9 has been updated with a more specific, on-treatment blood pressure target for older adults of under 130/80 mmHg. A more relaxed blood pressure goal (e.g. <140/90 mmHg) is now recommended for older adults with poor health, limited life expectancy, or increased risk of adverse effects from antihypertensive therapy.
- Regarding overall lifestyle management, Recommendation 13.11 has been divided into two subsections: (i) Recommendation 13.11a on healthy eating has been expanded with specific guidance on protein intake; and (ii) Recommendation 13.11b offers specific recommendations for older adults engaging in physical activity to help maintain lean body mass during weight loss.
- On the assessment of older adults with diabetes, the ADA added Table 13.1, which offers a summary of specific guidance in assessing older adults with diabetes for geriatric syndromes and other functional impairments. Figure 13.2 (see below) has also been added to illustrate a stepwise approach for: (i) assessing difficulties in the diabetes treatment plan; (ii) reevaluating glycemic goals through shared decision-making; (iii) simplifying or modifying the treatment plan; and (iv) reassessing patient burden or safety of any interventions.
20. Increasing differentiation of T1D and T2D guidelines for children and adolescents, with greater emphasis on patient education
The 2026 Standards of Care introduced several key updates to adolescent guidelines, notably including clearer distinctions between T1D and T2D guidance, more specific guidance on exercise and nutrition, and a greater emphasis on structured transition programs to support continuity of care. The ADA also turned more focus to the transition from adolescent to adult care in the subsection “Transition From Pediatric to Adult Care for All Children and Adolescents with Diabetes,” updating its recommendations to support the use of digital tools and structured transition programs to better support these patients’ continuity of care between pediatric and adult clinics.
- Compared to the 2025 Standards of Care, the 2026 Standards of Care placed an emphasis on distinct management for T1D and T2D, including a reorganization of Section 14. Table 14.1 was added to summarize the most recent T1D- and T2D-specific guidelines for managing diabetes-associated conditions in children and adolescents, including lipid screening, microalbuminuria, retinopathy, and neuropathy.
- The 2026 Standards of Care also emphasized the importance of patient and caregiver education on nutrition and exercise. On nutrition, guidelines were modified to reinforce comprehensive, tailored education both at diagnosis and during annual follow-up, including on the impact of different macronutrients on insulin dosing, glycemic excursions, and long-term outcomes (Recommendation 14.2). Additionally, the ADA updated its language in the subsection, “Physical Activity and Exercise,” to strengthen its support for over one hour of moderate-to-vigorous activity daily. The subsection also includes new guidance on strategies to prevent exercise-related hypoglycemia and hyperglycemia.
- Pharmacologic guidelines, included in the subsection “Type 2 Diabetes in Children in Adolescents,” now include updated FDA approval status and RCT discussion for GLP-1 RAs, SGLT-2 inhibitors, and dual GIP + GLP-1 RAs. The 2026 Standards of Care’s guidelines of bariatric surgery have also been expanded to include follow-up data exceeding 10 years.
- On T1D screening, new evidence from SEARCH for Diabetes in Youth (SEARCH), Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) and T1D Exchange studies were added to refine the timing and frequency of guidelines.
-- by Riya Chatterjee, Kayla Mathieu, Elizabeth Rose, Jeremy Alkire, Nour Khachemoune, Kat Moon, Esther Min, Monica Oxenreiter, and Kelly Close
[1] HHS is diagnosed with severe hyperglycemia (≥600 mg/dL), hyperosmolarity, and the absence of acidosis or significant ketonemia.