Pfizer 4Q25 – Topline phase 2b VESPER-3 results of once-monthly GLP-1 RA; plans to launch 10 phase 3 obesity trials in 2026, with commercial launch targeted in 2028; DGAT2 inhibitor candidate ervogastat discontinued –
Executive Highlights
- Pfizer presented 4Q25 results this morning in a call led by CEO Dr. Albert Bourla, CSO Dr. Chris Boshoff, and CFO Mr. David Denton – see the press announcement, prepared remarks, presentation, and webcast.
- Emphasizing that the obesity market has the potential to reach $150 billion, Pfizer spotlighted its obesity portfolio, which expanded significantly in 4Q25. In November 2025, Pfizer acquired Metsera with an amended $10 billion offer following a bidding war against Novo Nordisk. In December 2025, Pfizer entered a licensing agreement with China-based YaoPharma to develop a small molecule GLP-1 RA. Pfizer plans to advance ~20 clinical studies in 2026, 10 of which will be phase 3 trials. In addition to the existing candidates once-daily oral GIPR antagonist (PF’6016) in phase 2 and undisclosed biologic PF‘9415 in phase 1, the obesity pipeline now includes:
- Once-monthly GLP-1 RA in phase 3;
- Dual amylin/calcitonin RA, with or without GLP-1 RAs, in phase 1/2;
- Injectable GIP RA, with or without GLP-1 RAs, in phase 1; and
- Oral GLP-1 RA, injectable GLP-1 RA, and oral small molecule GLP-1 RA in phase 1.
- Pfizer announced topline results of a phase 2b VESPER-3 trial (n=250), which evaluated once-monthly GLP-1 RA, PF’3944 (previously called MET-097i), in adults with overweight or obesity without diabetes. The trial met its primary endpoint, with PF’3944 demonstrating statistically significant, dose-dependent, and placebo-adjusted weight loss of up to 12% at Week 28. Full results will be presented at ADA 2026. Pfizer plans to launch 10 phase 3 studies of PF’3944 across weight management and comorbidities, with commercialization targeted for 2028. The first VESPER-4 study (n=3,500) was launched in December 2025 and will evaluate weekly PF’3944 for overweight or obesity without T2D.
- The revenue of SGLT-2 inhibitor Steglatro (ertugliflozin) is estimated to be $130 million, up 32% from 4Q24 and down 1% sequentially. US sales totaled $39 million and OUS sales totaled $91 million, which were both up 32% from 4Q24 and down 1% sequentially. In 2025, total sales are estimated at $530 million, down 4% from 2024. While Merck and Pfizer do not break out revenue separately, based on the assumption that total revenue is split 60/40 between Merck and Pfizer with a 30/70 split between US and OUS, we estimate Pfizer’s total revenue to be $52 million, with $16 million from the US and $36 million from OUS.
- Management affirmed full year 2026 guidance of $59.5-$62.5 billion, taking COVID products, loss of exclusivity, and Most Favored Nation policy into consideration. Pfizer plans to spend $10.5-$11.5 billion for R&D. During Q&A, management highlighted that Pfizer is embedding AI across all functions, including discovery, clinical trial execution, regulatory filing, marketing, and manufacturing, to increase productivity and lower costs.
Table of Contents
-
Top Highlights
- 1. Topline phase 2b VESPER-3 results: Once-monthly GLP-1 RA confers 12% placebo-adjusted weight loss at Week 28; full readout planned for ADA 2026
- 2. Pfizer expands cardiometabolic pipeline through M&A and licensing; 20 obesity trials planned for 2026
- 3. Merck-partnered SGLT-2 inhibitor Steglatro (ertugliflozin) sales total $130 million, up 32% YoY
- Analyst Q&A
- Close Concerns’ Questions
Top Highlights
1. Topline phase 2b VESPER-3 results: Once-monthly GLP-1 RA confers 12% placebo-adjusted weight loss at Week 28; full readout planned for ADA 2026
Pfizer announced topline results of the phase 2b VESPER-3 trial (n=250), which evaluated once-monthly GLP-1 RA, PF’3944 (previously called MET-097i), in adults with overweight or obesity without diabetes. The trial met its primary endpoint, with PF’3944 demonstrating statistically significant, dose-dependent, and placebo-adjusted weight loss of up to 12% at Week 28. Importantly, the trial achieved the key objectives, which were to demonstrate: (i) continued weight loss upon switching from weekly to monthly dosing; and (ii) favorable safety and tolerability profile despite switching to four-fold greater monthly dose vs. weekly dose. Full results will be shared at ADA 2026.
- VESPER-3 trial design and results. The study evaluated four treatment arms (see Figure 1), two of which were presented in the topline results today. Arms 1 and 3 administered weekly doses of PF’3944 for 12 weeks and switched to 3.2 mg or 4.8 monthly doses for the remaining duration of the study. At Week 28, PF’3944 conferred up to 12% placebo-adjusted weight loss without plateau (see Figure 2). Importantly, weight loss continued after switching from weekly to monthly dosing in both Arms 1 and 3. Based on these results, as well as other clinical trial data, Pfizer predicts that monthly dose of 9.6 mg would confer 16% weight loss at Week 28, and will be evaluated in the phase 3 VESPER-4 trial.
- Safety and tolerability profile. Overall, PF’3944 was well-tolerated and had a favorable safety profile, consistent with the GLP-1 RA class. GI side effects were mostly mild or moderate, with few reports of severe nausea or vomiting and no instance of severe diarrhea. Across Arms 1 and 3, 4.6% (n=5) discontinued due to treatment-emergent adverse events during the weekly phase, and another 4.6% (n=5) discontinued during the monthly phase (vs. none in placebo).
- During Q&A, management noted that participants were not allowed to titrate down, and thus real-world tolerability and safety profile will likely be more favorable. Moreover, there was no signal of increased discontinuations when switching from weekly to monthly dosing.
Figure 1. VESPER-3 titration scheme
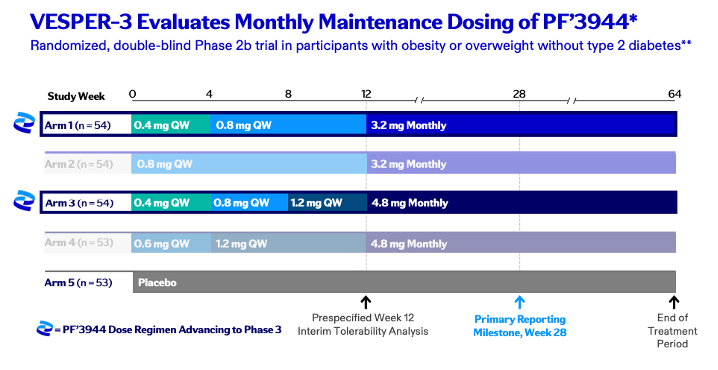
Source: Pfizer 4Q25 slides, page 14
Figure 2. VESPER-3 results and projected weight loss in phase 3
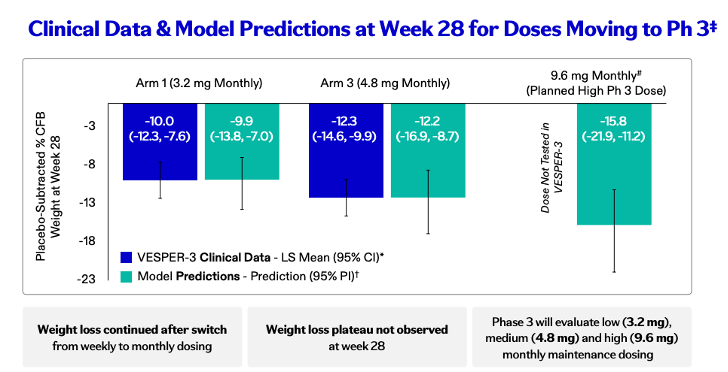
Source: Pfizer 4Q25 slides, page 15
- Previously, in the phase 2b VESPER-1 trial (n=239), PF’3944 1.2 mg conferred mean placebo-adjusted weight loss of 14.1% at Week 28 without titration. The candidate led to dose-dependent increase in GI events. The study had a total discontinuation rate of 2.9%.
- Pfizer plans to launch 10 phase 3 studies of PF’3944 across weight management and comorbidities, with commercialization targeted for 2028. These include: (i) VESPER-4 study (n=3,500) of weekly PF’3944 for overweight or obesity without T2D, launched in December 2025 and set to complete in May 2028; (ii) VESPER-5 of weekly PF’3944 for overweight or obesity with T2D; and (iii) VESPER-6, assessing monthly PF’3944 for overweight or obesity. Management detailed trial designs throughout the call and Q&A.
- Dosing and titration scheme. The phase 3 program will employ flexible titration scheme and evaluate higher doses. For example, the VESPER-4 trial will evaluate 2.4 mg weekly dose, while VESPER-6 will test 9.6 mg monthly dose. Of note, Pfizer’s model predicts that 9.6 mg monthly dose would confer ~16% weight loss at Week 28.
- CSO Dr. Boshoff explained that PF’3944 is structurally designed to have both high efficacy and extended half-life. Often, GLP-1 RAs rely on albumin – a common protein in blood plasma – to extend their half-lives. However, to optimize GLP-1 RAs’ engagement with GLP-1 receptors, albumin must be disassociated, limiting their half-lives. PF’3944 is unique because albumin is attached to a terminal end of the protein through lipidation, rather than in the middle of the protein, and remains bound during receptor engagement. This allows PF’3944 to have reduced clearance without reduced efficacy.
- During Q&A, management shared that monthly dosing of PF’3944 can be especially useful as a maintenance therapy. With lower injection burden, it can enhance convenience and treatment adherence.Moreover, Pfizer is evaluating other GLP-1 RA candidate in phase 1, which has a potential for as long as quarterly dosing.
2. Pfizer expands cardiometabolic pipeline through M&A and licensing; 20 obesity trials planned for 2026
In 4Q25, Pfizer significantly expanded its cardiometabolic pipeline through M&A and licensing agreement.Following an intense bidding war with Novo Nordisk in the fall, Pfizer acquired Metsera with an amended $10 billion offer in November 2025. In December 2025, Pfizer entered a licensing agreement with China-based YaoPharma to develop a small molecule GLP-1 RA in phase 1 trials with an upfront payment of $150 million and potential milestone payments up to $1.9 billion with tiered royalties on sales. In addition to the existing candidates once-daily oral GIPR antagonist (PF’6016) in phase 2 and undisclosed biologic PF‘9415 in phase 1, the obesity pipeline now includes:
- Once-monthly GLP-1 RA (PF’3944 or MET-097i) in phase 3;
- Dual amylin/calcitonin RA (DACRA; PF’3945 or MET-233i) in phase 2 as combination therapy with PF’3944 and in phase 1/2as monotherapy;
- GIP RA (PF’4696 or MET-034i) in phase 1 as monotherapy or in combination therapy with PF’3944;
- Oral GLP-1 RA (PF’6796 or MET-224o) and injectable GLP-1 RA (PF’6795 or MET-815i) in phase 1; and
- Oral small molecule GLP-1 RA (PF’2534 or YP05002) in phase 1.
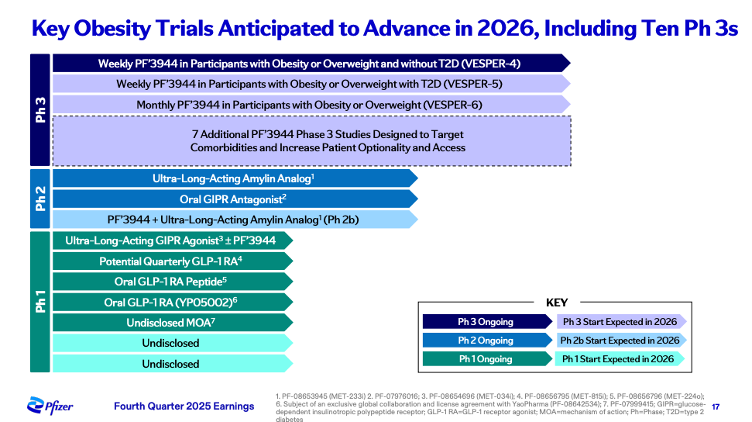
Pfizer plans to advance ~20 clinical studies in 2026, 10 of which will be pivotal phase 3 trials. Moreover, it expects to present phase 1/2 trial results evaluating the combination therapy of ultra-long-acting GLP-1 RA (PF’3944) and amylin analog (PF’3945) at ADA 2026 and launch a phase 3 combination study in 2027. See figure below for the key trials expected in 2026.
Several candidates for MASH were discontinued in 4Q25, including a DGAT2 inhibitor ervogastat (PF-06865571) evaluated in phase 2 and small molecule PNPLA3 modulator (PF-07853578) in phase 1. While there are currently no remaining MASH candidates in the pipeline, we imagine that incretin and amylin-based therapies could later be indicated for MASH.
See full pipeline updates in the table below.
| Product | Product Details | Status/Indication | Timeline |
| PF-08653944 (MET-097i) | Ultra-long-acting GLP-1 RA | Phase 3/Weight management | Topline results of phase 2 VESPER-3 announced in February 2025; phase 3 VESPER-4 (n=3,500) study launched in December 2025 |
| PF-08653944 (MET-097i) + PF-08653945 (MET-233i) | Ultra-long-acting GLP-1 RA + Dual amylin/calcitonin RA (DACRA) | Phase 2/Weight management | Phase 2 trial launched in March 2025, with completion expected in March 2027 |
| PF-08653945 (MET-233i) | Dual amylin/calcitonin RA (DACRA) | Phase 2/Weight management | Phase 1/2 trial launched in November 2024, with completion expected in April 2026 |
| PF-07976016 | Once-daily oral GIPR antagonist | Phase 2/Weight management | Phase 2 estimated to have completed in December 2025; phase 2 study completed enrollment in 2Q25; Advanced to phase 2 in people with obesity taking GLP-1 RA in 4Q24; Added to phase 1 in 4Q23 |
| PF-07999415 | Biologic, undisclosed | Phase 1/Obesity | Added to phase 1 in 2Q25 |
| PF-08654696 (MET-034i) +/- PF-08653944 (MET-097i) | GIP RA +/- GLP-1 RA | Phase 1/Weight management | Added to phase 1 in 4Q25 |
| PF-08656796 (MET-224o) | Oral GLP-1 RA | Phase 1/Weight management | Added to phase 1 in 4Q25 |
| PF-08656795 (MET-815i) | Injectable GLP-1 RA | Phase 1/Weight management | Added to phase 1 in 4Q25 |
| PF-08642534 | Small molecule GLP-1 RA | Phase 1/Weight management | Added to phase 1 in 4Q25 through licensing agreement with YaoPharma |
| PF-07328948 | Branched chain ketoacid dehydrogenase kinase (BCKDK) | Heart failure with preserved ejection fraction | Phase 2 trial launched in June 2025; Phase 1; Added to the pipeline in 4Q22 |
| PF-07293893 | Small molecule, new molecular entity | Phase 1/heart failure | Discontinued in 2Q25; Completed August 2024; Added to phase 1 in 1Q24 |
| PF-06882961 (danuglipron) | Oral GLP-1 agonist (once daily) | Phase 1/T2D/obesity | Discontinued in April 2025 following internal review and regulatory feedback |
| PF-06954522 | Small molecule, new molecular entity | Phase 1/T2D | Discontinued in 2Q25; Added to phase 1 in 3Q23 |
| PF-07853578 | Small molecule PNPLA3 modulator | Phase 1/MASH | Discontinued in 4Q25; Added to phase 1 in 1Q24 |
| PF-05221304 (clesacostat) / PF-06865571 (ervogastat) | ACC and DGAT2 inhibitor combination | Phase 2/MASH | Discontinued in 3Q25; Completed in February 2024; Phase 2 in NASH with fibrosis initiated June 2020, est. primary completion January 2024; Received US Fast Track designation in 2Q22; Phase 2acompleted April 2022 |
| PF-06865571 (ervogastat) | DGAT2 inhibitor | Phase 2/MASH | Discontinued in 4Q25; Completed February 2024; Phase 2 trial in NASH with fibrosis initiated June 2020, primary completion January 2024; Phase 1trial to characterize ADME properties completed August 2021 |
3. Merck-partnered SGLT-2 inhibitor Steglatro (ertugliflozin) sales total $130 million, up 32% YoY
The revenue of SGLT-2 inhibitor Steglatro (ertugliflozin) is estimated to be $130 million, up 32% from 4Q24 and down 1% sequentially. US sales totaled $39 million and OUS sales totaled $91 million, which were both up 32% from 4Q24 and down 1% sequentially. In 2025, total sales are estimated at $530 million, down 4% from 2024. While Merck and Pfizer do not break out revenue separately, based on the assumption that total revenue is split 60/40 between Merck and Pfizer with a 30/70 split between US and OUS, we estimate Pfizer’s total revenue to be $52 million, with $16 million from the US and $36 million from OUS.
While there was no mention of Steglatro in the 4Q25 call, we are curious if Pfizer and Merck will pursue potential pediatric indicationbased on a recent phase 3 trial (n=165) in patients with T2D (ages 10-17 years).
Analyst Q&A
On VESPER-3
Q (Chris Schott, JPMorgan): On the VESPER-3 data, can you elaborate any more on the tolerability you saw here? And maybe just specifically, is there anything more you can say about vomiting rates or any differences you saw between the mild or moderate dosing arms? If we consider the two doses that are moving forward from VESPER-3, it seems like you have a drug that clearly has solid weight loss. It's got monthly dosing. At the same time, that weight loss might be a bit below what you saw with the weekly Zepbound – what role do you see that that type of profile playing in the market?
A (Chris Boshoff, CSO): So obviously we will share the full tolerability data at our oral presentation at ADA in June. We are really encouraged by the observed distribution across weekly and monthly. And you could have expected potentially that when patients switch to a fourfold higher dose, we're going to have a higher number of sudden discontinuations and nausea and vomiting. We did a distribution between the monthly as well as the weekly. Just to remember for this study, there was no step-down titration was allowed, which is unusual for obesity trials. But that will obviously not happen in the phase 3 study. We will allow down titration. Regarding the different doses as we pointed out low and medium was presented today. The higher dose is already being tested in VESPER-4 because previous prediction models indicated that it will be well tolerated. And we should test 2.4 mg weekly, which is happening now and the monthly study will test 9.6 mg as pointed out.
Commercially, I think when you look at the clinical data. I think what it suggests to us very clearly is that ’3944 from an efficacy perspective has the potential to deliver efficacy. That's competitive with the standard of care and potentially best in class against what’s on the market. We think when you take that efficacy and then you combine it with a lower medication burden through a monthly dose, that's a value proposition that's going to resonate with patients, providers, and payers, because persistency and simplicity matter. And it also gives us the opportunity to switch patients from weekly onto monthly therapy. So we think ’3944 is going to be a compelling therapy, full stop. And then you add to that the opportunity that exists from the other assets that we have in our portfolio with our commercial capabilities to execute in the US and international, and I think it gives us a lot of confidence around the commercial potential.
A (Alexandre de Germay, CICO): That's right. Yes. What's really interesting in this category is actually the size of the market ex-US projected to be 150 billion. And 40% of that is actually ex-US. There are two things that are really interesting in this category that are unique and that reinforce the potential of this asset. First is the out-of-pocket category because in most countries, when we introduce the innovation, we have to go through reimbursement negotiation and often translate into price reduction. In this category, we see that there is high willingness to pay out of pocket across all mature markets, whether in Europe or in Australia or in Canada. And we see the price point being across $250 to $350, which is higher than what we had expected. And when we looked at the latest release from our competitors in this category, we see that there is highest willingness to pay from all those geographies, including actually also emerging markets where we also see high prevalence. The second thing is, the time to market, because it's going to be mostly an out of pocket category. The time after approval at the EMEA will be sentenced, where we will be able to actually commercialize those products. So that will drive also rapid penetration in the market.
Q (Vamil Divan, Guggenheim Securities): You just talked a little bit about this prior question around down titration in phase 3. Can you just elaborate a little bit more on that and how you're designing your phase 3 and allowing for flexibility as patients may be dealing with any sort of side effects? And maybe that improves overall the profile you see from phase 2. And then my other question is actually just beyond VESPER-3. You mentioned this will be at ADA. I'm curious what other data we may get from ADA, your internal programs or from the vaccine portfolio at ADA and possibly your internal. Do you expect to provide that phase 2 data there?
A (Chris Boshoff, CSO): Just a reminder again for the VESPER-3 data we presented today there's only two step-up doses. You used to four, five, step-up doses to get to the desired dose. In this study it was only two step-up doses. So the phase 3, design for VESPER-6 will test different iterations as well as, as we pointed out the additional dose of 9.6 mg which is currently being tested in VESPER-4 as 2.4 mg weekly. Regarding the next, the rest of the portfolio, we are obviously excited about the platform in general. It's a very differentiated platform. As you know, we previously presented data for the ultra-long-acting amylin ’3945 (also called MET-233i), where the observed additive weight loss when combining ’3944 and ’3945 was 5% at Day 8 and single-agent ultra-long amylin previous data showed at Day 36, 8.4% placebo-adjusted weight loss. So we should share later this year, including at ADA updated data on Amylin and potential early data for the combination of amylin plus ’3944. We also, as you know, in our portfolio, excited about the rest of the phase 2 programs which including a first in potential, first in class GIPR antagonist oral that was discovered conceptualized internally that's current in the randomized phase 2 experience and also the more broader phase 1 program of peptides, including an ultra-long GLP-1 that's potentially three monthly, quarterly that's currently in phase 1 as well as our additional oral portfolio including the oral GLP-1 recently acquired from YaoPharma.
Q (Steve Scala, TD Cowen): In the VESPER-3 data did the placebo arm gain weight or lose weight?
A (Chris Boshoff, CSO): Again, the full data will be presented ADA. But, in this case VESPER-3, actually the placebo arm was very stable. Not really up or down, but you'll see the data at ADA.
Q (Terence Flynn, Morgan Stanley): On the VESPER-3 data, I know you want to hold a lot of data until ADA, but just was wondering if you can provide any high level details on the baseline characteristics, so either BMI or gender mix. I know sometimes those can vary across studies. And then on the tolerability side, again one question when you have you no longer dosing intervals is the duration of GI side effects. And so any qualitative commentary there, if that's longer than one or two days? Thank you.
A (Chris Boshoff, CSO): Just to start with the demographics. The study was conducted in the US only. And I think, as you know, there are differences, especially in AE and tolerability discontinuations between US-only patient populations. So, that's one. The rest of the detailed demographics will be presented at ADA, but it's as expected from a small US- based phase 2 study. For tolerability, as we stated before, we are encouraged by the overall tolerability. It is similar to what you expect for GLP-1 class. But specifically, we can move to monthly with a distribution of AEs across weekly and monthly. That didn't give us alarm that switching to monthly suddenly, there's a cluster of discontinuations or significant AEs. As I pointed out earlier as well, there's no -- there's only one severe nausea -- one severe vomiting across the whole program, no severe diarrhea. So, overall, we're very encouraged by the safety profile. And again, ADA will share the whole AE profile.
Q (Jason Gerberry, Bank of America): Just based on today's, VESPER-3 update. Just kind of curious how you're thinking about the value add of the GLP – the GLP-1/amylin injectable combination relative to the monotherapy? And, you know, are you really looking to kind of compete in that ultra-high efficacy tier with agents like Lilly's Triple G? Or is the value-add potentially more in GLP-1 non-responders just sort of curious, because it seems like what you have with the monotherapy approach can make you competitive with Zepbound and maritime. So just sort of curious how you think about the combo and where that fits?
A (Chris Boshoff, CSO): Yeah, we will have optionality because we are developing in phase 1 through 3, both the single agent ’3944 as well as the combination ’3944 plus ’3945. Everything we've seen thus far suggests that to us to your point that we should get increase efficacy for the combination. And that's why we hope to update later data later this year. Start the phase 2 study this year and then next year start the phase 3 study for the combination.
A (Aamir Malik, Executive VP): Yes. Jason, so I think the quick answer would be, look, I think we're in the very early innings of a large market where there is still significant unmet need, right? There's more convenient dosing that's needed, higher weight loss for certain BMI patients. GI tolerability needs to improve, maintenance strategies, friction in the patient journey. So our belief is that there's not going to be one single asset that serves all those patients. People are going to have different starting points, goals, preferences on their dosing and route of administration, comorbidities, their willingness to pay, and what you need to win in a market like that is one you need a great portfolio of products that can serve all those patient needs. And two, you need really differentiated capabilities. And I think with Chris describing not only our data today, but some of the other things that we have in our portfolio, we have the first piece in place and emerging, and we feel very confident about our commercial capabilities, whether it's our field forces that are the top ranked in the US and already are seeing the majority of GLP-1 prescribers or the digital platforms that we are building, like Pfizer, for all that have touched over 25 million patients. So when you put that all together, we have a lot of confidence in our ability to win commercially in this market with these assets.
Q (Geoff Meacham, Citibank): Again, a few on the new data today, so when you look at the PK-PD, are you guys set with monthly being the longest dosing interval to preserve efficacy, or is it potentially -- is it feasible to extend to every two-month dosing? And then on your phase 3 plans, is it your sense these are likely to be the standard type of metabolic studies that we'd expect to do? Or would you pursue any maybe inflammation or neuropsych indications, or would you pursue GLP-1 active comparator studies? Just trying to think of how you could separate yourself in a broad phase 3 program. Thank you.
A (Chris Boshoff, CSO): So ’3944 is as we demonstrated, the first peptide that can be administered monthly, and potentially yes, we can go longer, but for ’3944, our aim is as a monthly maintenance therapy. As I mentioned, we do have another molecule, a peptide currently in phase 1, which has a pro-drug, a pro-peptide with a potential for three monthly administration, that's currently in phase 1. And we should in the next couple of months get additional PK-PD data from that molecule, which will be our potential opportunity to go to three monthly. The second question, the initial phase 3 programs VESPER-4 VESPER-5, and VESPER-6. VESPER-4 is the one in patients without T2D that's currently ongoing with weekly testing, including the high dose of 2.4 milligram weekly. VESPER-5 in patients with T2D, and VESPER-6, the study that will include monthly dosing. Beyond that, we plan to start seven studies. We haven't showed or revealed what these studies are going to be, but you're absolutely correct that beyond cardiovascular metabolic, we are looking at other opportunities to differentiate and also to differentiate with our combinations for instance, with amylin or with a GIPR currently in phase 1.
On other obesity and diabetes therapies
Q (Umer Raffat, Evercore ISI): First on the GLP monotherapy, could you remind us, if the 9.6mg monthly dose was a reaction to the data today? Or was that already being contemplated? And then secondly, on the emerging tolerability data for your GLP plus amylin combo, how are you feeling on that? And do you think you can fit the GLP plus amylin in a single pill? Thank you.
A (Chris Boshoff, CSO): Okay. So on the first question, a reminder that the 2.4 mg is already being tested as a weekly regimen. So it's a high dose in VESPER-4. And that decision was made based on the modeling based meta-analysis. And as you showed -- as we showed today, our modeling predicts very well between what we actually observed and what the modeling predicted for 3.2 mg and 4.8 mg. So we have confidence in the modeling also for 9.6 mg or the 2.4mg. Also, just a reminder that the combination is monthly. It's amylin plus GLP 1 ultra-monthly subcutaneous. So it's not in a pill. We do have an oral portfolio and we do have some other oral medicines discovered internally, which we've not revealed yet, but currently are oral medicines GLP-1 and GLP are not the amylin as oral.
We'll show data for the amylin plus GLP-1 monthly data for the ultra-long acting monthly data at ADA. The earlier data we've shown reminder of the combination of ’3944 plus ’3945 was 5% at Day 8. That was early data that was shown and will update those data later this year.
Q (Mohit Bansal, Wells Fargo): One more on the vascular program here. I would like to understand what kind of target profile you are looking at from the phase 3 trial. I'm asking because with the GLP- 1, you kind of see mid to high teens kind of weight loss with an optimized GLP-1. And if you try to push it beyond that, you could probably start to run into tolerability issues. What makes you think that this longer-acting GLP-1 could provide higher weight loss than that with a better tolerability? Or you think that monthly is probably the biggest differentiator here?
A (Chris Boshoff, CSO): So it's both. We expect competitive weight loss and the data we showed today, including with the predictions what to expect from the 9.6 mg to 16 mg weight loss predicted at Week 28 is highly competitive, tolerable to be highly competitive. And then, of course, monthly dosing, which will be highly differentiated. Just to point out, we are also planning a phase 2 study, which will evaluate switching. So patients already on weekly therapy doing well to switch those patients to monthly dosing.
A (Albert Bourla, CEO): Thank you, Chris. And this is not only ours, of course, weekly, monthly, but also any other GLP-1 RAs that are in the market, and they want to move after they achieve a weight loss into a maintenance with only one injection rather than with four. Of course, there's also the oral solutions, but that's going from one weekly to one daily pill. Some will do it, but I think our research shows that most would like -- if they are already used needle and they would like to switch mostly to a more convenient needle, which is once a month. Next question, please.
Q (Dave Risinger, Leerink Partners): Chris, could you talk a little bit more about MET233i, which I believe is now numbered ’3945 specifically, the bias of amylin relative to calcitonin. The implications for the efficacy and tolerability profile and the data we should expect at ADA. Thanks very much.
A (Chris Boshoff, CSO): So this is an ultra-long acting. Amylin, which was previously shown to have a monotherapy, efficacy of 8.4% placebo adjusted weight loss at Day 36. It's a dual molecule, so it's not biased to the placebo like tolerability was previously shown with the monotherapy. And that gave confidence for the starting the combination of ’3944 and ’3945 or -- previously, early data shown at Day 8, 5% weight loss. But obviously that's very early. So we will update those data later this year. This is important combination for us because we believe with this combination we can have best-in-class efficacy with a monthly dosing, which will be highly-differentiated for this combination.
Q (Michael Yee, UBS): Two questions. One for Chris and one for Dave. On the oral GLP-1 that you guys recently in-licensed, can you just remind us how much information you knew or what data you already had? I believe there's already a large phase 1 ongoing, so that should add some comfort there. But tell us about what you knew already on that molecule? And then for Dave, you reiterated $7 billion of capacity. Can you just talk about the ability to do more in the context of the recent dividend pause or at least dividend growth pause recently, given that that doesn't happen very often and how you think about your dividend. Thank you.
A (Dave Denton, CFO): Yes. So yes, clearly our focus is maintaining our dividend at the moment and growing our dividend over time. So it's a very important and critical structure and component of our capital allocation program. And again, we do have – coming into this year we had $6 billion in BD capacity is actually gone up a bit as we've announced the pending liquidation of the Veeva asset. So that actually is a good example of how we're looking at the set of assets that we have within Pfizer and understanding how we can best monetize them over time. So with that, I'll turn it over to Chris.
A (Chris Boshoff, CSO): Thank you very much. 5002 is the YaoPharma oral small-molecule, which is not under danuglipron scaffold. It's currently in Phase 1. We've acquired it through an exclusive global collaboration and license agreement with YaoPharma. We plan to conduct Phase 1 studies and also combination studies with our GIPR antagonist that's currently in a randomized experience in phase 2. And we currently transitioning all the work to the US to start the Phase 1 studies in the US, including manufacturing.
On AI development and investments
Q (Courtney Breen, Bernstein): Thanks so much for the question today. Just perhaps building on the conversation that was just taking place, as you talk about the 20-plus pivotal studies that are starting this year, we're seeing kind of a mid-point $11 billion guide for R&D in 2026. How do we think about 2027 as these studies start to annualize and then kind of combining that with the element that you just raised, Albert, of the AI investment, the 1,200 GPU deployment that you're making, kind of when and where will we begin to see impact from that strategy, and will that impact anything in the operations of R&D of the pivotal trials, or should we be thinking more about innovation on the research side of the long run? Thank you so much.
A (Dave Denton, CFO): Yeah, I guess contextually, if you just think about R&D as we cycle from 2025 into 2026, with the business development transactions that we've done, we've actually increased the burden and the load of work that needs to be done within our R&D infrastructure. At the same time, we're investing about $11 billion in R&D. So we're being able to be more productive in the infrastructure across R&D and take on more substrate to be able to focus on creating medicines for the end of the decade and beyond. So I think what we're trying to do is continue to refresh, re-improve the productivity across our R&D platform to invest those dollars back into R&D to continue to forward, advance the programs that we have underway and the programs that we're developing. As you know, 2026 is a big start year for us from a science perspective. We will continue to focus on those investments going forward.
Q (Evan Seigerman, BMO Capital Markets): Thank you so much for taking my question. I just wanted to touch on your comments around investment in AI. What are some metrics you're putting around that? And more broadly, I just want to ensure that this is going to drive a good return on your investment versus just kind of feeding into the hype.
A (Albert, Bourla, CEO): Yes. It's a very good question. And let me start, but then I will ask specific marketing achievements and R&D achievements through AI. In general, there are things in AI that the technology is ready now. And those are deploying very, very fast. And certainly, I cannot do everything, but certainly can do more than what it is used right now to do. And that has to do with how successful you are in implementing it, embedding it into your organizational footprint, embedding it into your business processes and also creating AI literacy among the employees that eventually are using this AI. While that clearly affects everything from enabling functions and maybe Dave can speak a little bit about the things that we are doing there. I mean, when I say enabling functions from finance, HR, legal, you name it. And of course, in R&D, where we have seen already significant productivity enhancements in marketing that it is helping us to maximize the ROI right now and in manufacturing, where a very big part of the savings that were achieved were achieved of a successful deployment of AI use case. Chris, do you want to give some specific examples?
A (Chris Boshoff, CSO): Yes. Thank you very much for the question. So as you pointed out, in R&D, we're embedding AI in each function, meaning in discovery, medical, regulatory, safety, pharmacovigilance, clinical trial execution; and we're recruiting and embedding AI engineers in each of those functions to work with the scientists and the clinicians, how to measure success, productivity, productivity speed and cost to be bring cost down by embedding AI and obviously accelerating speed.
Commercially, I think metrics are at the heart of everything that we're doing with AI. I'll give you two very specific examples. One is our field force productivity. We're using AI to not only help train our field forces, but also help make their time with physicians maximize. So we invest more time with physicians rather than behind screens. Second is on the marketing side, we measure MROI. And you've seen us be very disciplined, as Dave alluded to, in our SI&A spend, particularly as we're trying to grow revenue for a lot of our launch and acquired brands, and AI has absolutely helped us increase our MROIs by being much, much more targeted about where we invest.
A (Alexandre de Germay, CICO): Yeah, that's right. I mean every step of the way when we interact with our customer is subject to an improvement with AI. Let me give you an example pre-call planning for our rep is actually done better when it is done with AI. The quality of the interaction is listened so that we can re-run those interactions so that we can improve the quality of the interaction. We can also do targeting in a better way so that we have advanced targeting, thanks to AI. And finally, imagine that operating globally with very different regulatory requirements require every country to redo and re-assess every promotional pieces. With AI, we can do that instantly in all those markets. We don't need to re-run all those activities at every country. So that has massive impact on productivity and speed to market.
A (Dave Denton): Yeah. Maybe just two points. From an enabling functions perspective, I think about AI in us leveraging our vendors because we have big vendor technology platforms across our enterprise. And as they make investments in their platform, we're taking advantage of those and embedding those within our process, which is increasing our productivity. And then secondly, think about our business model. We have routine transactions, but we have a large number of products that are across literally hundreds of markets. So AI is allowing us to use those data sets to essentially automate some of those transactions to make it very efficient that today, we deploy resources to be able to do that. So now the technology is enabling us to be a lot more productive.
A (Albert Bourla, CEO): Evan, that's why we put it as one of the four imperative strategic priorities that we plan to do, which is to scale up because we have so big success. Many people are asking us, how is possible that Pfizer was able to take so much cost out of its operations without affecting the top line? And the answer is AI. We didn't just cut cost. What we did is we improved productivity and the main lever, of course, there were simplification efforts that also took place, but the main lever was the successful deployment of AI, where basically you are reducing the cost without that being seen in the activity. So very excited about the prospects of AI.
Close Concerns’ Questions
1. What comorbidities does Pfizer plan to evaluate PF’3944 in the phase 3 trials (e.g., T2D, MASLD, CKD, CVD, obstructive sleep apnea, and arthritic pain)?
2. Does Pfizer plan to test even higher doses of PF’3944 (above 2.4 mg weekly and 9.6 mg monthly) in phase 3 program to achieve greater weight loss >15%? How does the company’s model predict tolerability profile at higher doses?
3. Will the phase 3 program include active comparators, especially the longer cardiovascular outcomes trials?
4. What patient segments might Pfizer’s candidates address, such as those with high BMI or comorbidity burden or GLP-1 RA non-responders?
5. Is Pfizer interested in evaluating triple combinations, such as GLP-1 RA, amylin agonism, and GIP RA?
6. How does Pfizer believe dual amylin/calcitonin RA (DACRA; PF’3945 or MET-233i) is differentiated from other long-acting amylin agonists, like petrelintide, cagrilintide, and eloralintide?
-- by Kat Moon, Paul Moon, Monica Oxenreiter, and Kelly Close