Roche 1Q26 – BGM sales grow for the first time in five years (+8%); Vabysmo sales up 13% with initial US recovery; full results for petrelintide expected at ADA 2026 –
Executive Highlights
- Roche presented its 1Q26 financial results on a call led by CEO Dr. Thomas Schinecker, CFO Dr. Alan Hippe, Roche Pharmaceuticals CEO Ms. Teresa Graham, and Roche Diagnostics CEO Mr. Matt Sause. See Roche’s press release, company presentation, and webcast.
- In 1Q26, Roche initiated the phase 3 ENITH-1 (n=2,000) and ENITH-2 (n=1,600) trials for enicepatide (CT-388; once-weekly dual GLP-1/GIP RA) in adults with overweight or obesity without and with T2D, respectively. In March 2026, topline results of the ZUPREME-1 trial (n=493) showed that long-acting amylin analog petrelintide led to 10.7% weight loss vs. 1.7% with placebo at 48 weeks. Roche reiterated plans to launch a phase 2 trial of a fixed-dose combination of petrelintide and CT-388 mid-year, as originally announced in 4Q25.
- The company reported growth in BGM sales in 1Q26 for the first time since 2Q21, with revenue growing 8% year-over-year to CHF 310 million (~$395 million). The company continues to invest in CGM as the broader market shifts to the technology; we are curious if management believes this will be standalone quarter and what geographies specifically drove this uptick in sales.
- Roche continues to develop its pipeline in liver health. In September 2025, the company announced its plans to acquire San Francisco-based 89bio, developer of the FGF21 analog pegozafermin for MASH. Roche plans to submit pegozafermin to the FDA for MASH with fibrosis stage F2 or F3 in 2028, as well as for MASH with fibrosis stage F4 in the same year.
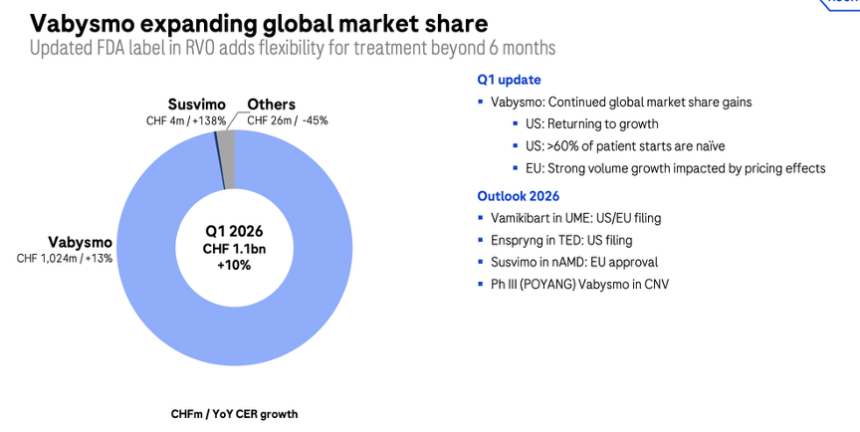
- In ophthalmology, Vabysmo (faricimab) returned to growth in the US in 1Q26. 1Q26 sales totaled CHF 1.0 billion ($1.27 billion), up 13% CER from 1Q25 but down 10% sequentially. 1Q26 marked a return to growth in the US for Vabysmo with a 4% sales growth for the quarter and low double-digit volume growth. Market share has also expanded.
- In 1Q26, sales for Susvimo (ranibizumab), a refillable eye implant of anti-VEGF, totaled CHF 4 million ($5.1 million), up over 2x (+138%) from 1Q25 and down 56% sequentially. Roche filed for regulatory approval in the EU for nAMD in 3Q25, with the decision expected in 2026. It plans to file for DME in the EU in 2027.
Table of Contents
- Technology Highlights
-
Therapy Highlights
- 1. Cardiometabolic pipeline: Phase 3 studies launched for enicepatide (CT-388); full results of CT-388, CT-868, and petrelintide expected at ADA 2026
- 2. Roche plans to submit FGF21 analog pegozafermin to the FDA for MASH with F2-F4 fibrosis in 2028; three phase 3 trials continue
- 3. Vabysmo continues to be a top growth driver with 13% CER growth
- 4. Susvimo: EU regulatory milestones remain key upcoming focus; sales up 132% CER
- Close Concerns’ Questions
- Diabetes-related Q&A
Technology Highlights
1. BGM sales grow 8% to CHF ~310 million as Roche prepares for CGM-driven growth
While Diabetes Care revenue was not shared[1], Roche reported growth in BGM sales in 1Q26 of 8% year-over-year. Given this reported decline, we estimate BGM revenue of CHF 310 million (~$395 million), consistent with recent quarters and up 3% sequentially. Growth in this quarter is notable, as Roche’s BGM revenue has seen a year-over-year decline for the prior nearly 20 quarters (since 2Q21). Nearly every quarter since 3Q21 has fluctuated between ~CHF 300-400 million. Without commentary in prepared remarks or during Q&A on Roche’s BGM business, we don’t know if this will be a standalone quarter or if further growth is expected in the coming quarters. We are also interested in whether growth reflects strength in more mature CGM markets or regions with lower CGM penetration, or a mix of both.
- Roche continues to invest in CGM as the market shifts to the technology. As part of Roche’s $50 billion US investment commitment, the company is developing a CGM manufacturing facility in Indianapolis. We remain interested in Accu-Chek SmartGuide’s US regulatory status and launch timeline.
2. Roche reiterates commitment to advancing AI capabilities
Roche is advancing AI capabilities across its company, from drug discovery to diagnostics and manufacturing, and to accelerate the development of new therapies and technologies. Management highlighted its long-standing (2016) collaboration with NVIDIA to process the massive amount of data generated by its DNA sequencing technology and new AI applications, including a new agreement to expand its GPU infrastructure in the US and Europe. Roche’s previous Digitalization Days and Pharma Days have detailed how its “Lab-in-the-Loop” AI/machine learning model has facilitated drug development, cutting report generation time by >60%, increasing screening yield by >10%, and reducing capital expenditures by making existing facilities more efficient.
Therapy Highlights
1. Cardiometabolic pipeline: Phase 3 studies launched for enicepatide (CT-388); full results of CT-388, CT-868, and petrelintide expected at ADA 2026
Source: Roche 1Q26 presentation, page 33
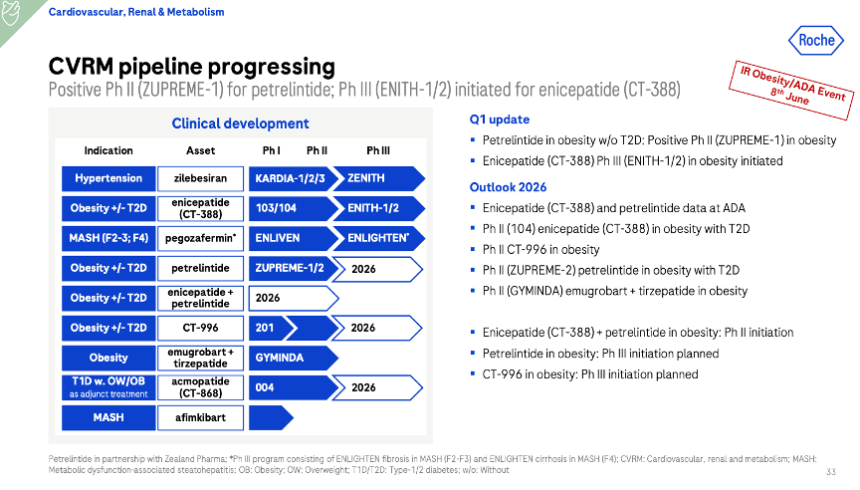
Roche boasts an expansive cardiovascular, renal, and metabolism (CVRM) pipeline, which includes candidates for obesity, hypertension, and MASH.
- Enicepatide (CT-388; once-weekly dual GLP-1/GIP RA): In 1Q26, Roche initiated the phase 3 ENITH-1 (n=2,000) and ENITH-2 (n=1,600) trials, which will evaluate enicepatide – a new name for CT-388 – in adults with overweight or obesity without and with T2D, respectively. Both studies are expected to be completed in August 2028. During Q&A, management said that the two phase 3 trials follow the standard design required by the FDA.
- In addition, a phase 2 trial (n=360) for CT-388 is underway in people with obesity and T2D, with expected completion in September 2026 – a delay from August 2026. Roche will also launch a phase 2 trial of a fixed-dose combination of petrelintide and CT-388 mid-year, as announced in 4Q25.
- This follows the phase 2 data (n=469) announced in January 2026, in which CT-388 demonstrated 22.5% weight loss at 48 weeks without signs of plateau. Full results will be presented at ADA 2026. Of note, in the phase 1b trial, CT-388 demonstrated ~19% weight loss at Week 24 in people with obesity but without diabetes. In those with obesity and T2D, CT-388 demonstrated a 3.0% reduction in A1c over 12 weeks compared with 0.2% on placebo.
- Acmopatide (CT-868; once-daily dual GLP-1/GIP RA): Roche plans to launch the phase 3 trial of acmopatide – a new name for CT-868 – for people with T1D and BMI ≥25 kg/m2. As announced in 4Q25, the decision is based on the 16-week phase 2 trial (n=111) completed in July 2025. Full results of the phase 2 trial will be presented at ADA 2026.
- CT-996 (once-daily oral GLP-1 RA): A phase 2 trial (n=340) continues to evaluate CT-996 for people with obesity and without diabetes. The trial is expected to be completed in July 2026, and the results will be available later this year. The phase 3 trial for obesity is expected to launch this year. As background, a phase 1 trial, CT-996 conferred ~7% weight loss at four weeks.
- Petrelintide (long-acting amylin analog): In March 2026, Roche and Zealand announced positive topline results of the ZUPREME-1 trial (n=493) of petrelintide, a Zealand-partnered long-acting amylin analog, in people with overweight or obesity. At Week 42, petrelintide led to 10.7% weight loss vs. 1.7% with placebo. Management emphasized that petrelintide had a placebo-like tolerability profile – in fact, the placebo group had a higher rate of discontinuation. Full data are expected at ADA 2026, and the phase 3 program will initiate in 2026.
- The 28-week phase 2 ZUPREME-2 trial (n=216) also examines petrelintide in people with overweight or obesity and T2D and is expected to be completed in August 2026, slightly delayed from June 2026, as marked in 4Q25.
- Management once again expressed confidence in combination treatments of petrelintide and other incretin-based therapies like CT-388, with the phase 2 trial expected to launch mid-year.
- Emugrobart (GYM 329, anti-latent myostatin antibody): Emugrobart aims to preserve muscle mass and prevent post-treatment weight regain. The phase 2 GYMINDA trial (n=234) continues to evaluate the combination of GYM 329 and tirzepatide in adults with obesity, and is expected to complete in July 2027, slightly earlier than the previously noted date, September 2027. Topline phase 2 results are expected in 2026.
- Zilebesiran (angiotensinogen inhibitor). While not mentioned in the call, the phase 3 CVOT ZENITH trial (n=11,000) continues to recruit participants to evaluate zilebesiran in patients with unmanaged hypertension on a diuretic and at least one other antihypertensive medication. The study is expected to complete in 2030. In the phase 2 KARDIA-1, KARDIA-2, and KARDIA-3 trials, zilebesiran conferred significant reductions in systolic blood pressure by 7-9 mmHg, sustained for over six months, in participants with unmanaged hypertension despite prior treatment.
2. Roche plans to submit FGF21 analog pegozafermin to the FDA for MASH with F2-F4 fibrosis in 2028; three phase 3 trials continue
Liver health remained unmentioned on today’s call, but Roche continues to develop its pipeline in this area. In September 2025, the company announced its plans to acquire San Francisco-based 89bio, developer of the FGF21 analog pegozafermin for MASH. The potential total transaction value was $3.5 billion and the offer period closed October 29, 2025.
- The deal brings pegozafermin into Roche’s cardiometabolic pipeline, adding a liver‑targeted, glycoPEGylated FGF21 analog. While pegozafermin remained unmentioned, the supporting slides provided a new regulatory submission timeline for the therapy. Roche plans to submit pegozafermin to the FDA for MASH with fibrosis stage F2 or F3 in 2028, as well as for MASH with fibrosis stage F4 in the same year.
- Previous results for the therapy have been strong. In the 24‑week phase 2b ENLIVEN study (n=222), pegozafermin produced improvements to both fibrosis and MASH resolution. Fibrosis improvement of at least one stage without MASH worsening was 26% (versus 7% with placebo) with a 30 mg dose of pegozafermin and 27% (versus 7%) with the 44 mg twice‑monthly dose. In addition, the percentage of patients with MASH resolution without the worsening of fibrosis also favored pegozafermin over placebo in both the 30 mg pegozafermin group (23% vs. 2%) and the 44 mg pegozafermin group (26% versus 2%). Three phase 3 trials are ongoing:
- ENLIGHTEN-Fibrosis (n=1,050) for the treatment of moderate-to-severe fibrosis (F2-F3) related to MASH. Topline histology data are expected in 1H27, and the trial is set to complete in February 2029.
- ENLIGHTEN-Cirrhosis (n=762) for the treatment of cirrhosis (F4) related to MASH. Topline histology data are expected in 2028, and the trial is set to complete in 2031.
- ENTRUST (n=360) for the treatment of severe hypertriglyceridemia. The trial is expected to be completed in April 2026.
3. Vabysmo continues to be a top growth driver with 13% CER growth
Vabysmo (faricimab) returned to growth in the US in 1Q26. 1Q26 sales totaled CHF 1.0 billion ($1.27 billion), up 13% CER from 1Q25 (see below) but down 10% sequentially. Vabysmo inhibits two signaling pathways: Ang-2 and VEGF-A and has now been on the market since January 2022, following its simultaneous FDA approval for nAMD and DME. The company attributed 10% of its 2026 sales growth thus far to Vabysmo.
- Ms. Graham said that 1Q26 marked a return to growth in the US for Vabysmo with a 4% sales growth for the quarter and low double-digit volume growth. Market share has also expanded. Since its initial approval the therapy has also gained FDA approval for RVO, and Ms. Graham again emphasized that over 60% of US patients starting the therapy are treatment-naïve. In previous quarters, Vabysmo performance had been impacted by the contraction of the US branded market, but Roche said it has begun to see the first signs of recovery. The company expects to see a gradual recovery of the branded market in the future.
- Outside the US, the therapy also continued to perform well.
- In Europe, despite temporary impacts from mandatory price cuts, volume growth was positive. The ongoing rollout of the prefilled syringe (PFS) formulation is expected to drive further growth in the region.
- In Japan, Roche Group member Chugai received approval for an expanded indication to treat angioid streaks (breaks or cracks in the layer of tissue behind the retina) in May 2025.
- In rest of the world, sales also grew, with Vabysmo increasing in market share globally. Roche especially reported strong uptake in China, following Vabysmo’s NRDL listing in January and rapidly expanding market share. Following the readout of the phase 3 POYANG trial (n=280) for a choroidal neovascularization (CNV) indication, a planned regulatory submission will occur this year, ahead of the company’s initial planned submission in 2027.
4. Susvimo: EU regulatory milestones remain key upcoming focus; sales up 132% CER
In 1Q26, Susvimo (ranibizumab) revenue totaled CHF 4 million ($5.1 million), up over 2x (+138%) from 1Q25 and down 56% sequentially. As background, Susvimo is an FDA-approved refillable eye implant that delivers an anti-VEGF ranibizumab to treat nAMD. It requires refills every six months and serves as an alternative to injections. While not mentioned in the call, Roche filed for regulatory approval in the EU for nAMD in 3Q25, with the decision expected in 2026. It plans to file for DME in the EU in 2027.
Close Concerns’ Questions
- Which geographies drove BGM growth in 1Q26?
- Did the company see strong performance of its BGMs in regions with limited uptake of CGM, or was revenue growth in the quarter driven by regions where use of continuous monitors has already become widespread?
- What additional indications will Roche evaluate its incretin-based candidates in?
- How might future trials of incretin-based candidates incorporate more flexible dosing to reflect real-world use?
- What are Zealand and Roche’s key considerations for designing the phase 3 trial of petrelintide?
- Will Roche investigate pegozafermin in combination with other therapies, as other companies have done in the CVRM arena?
Diabetes-related Q&A
On enicepatide (CT-388)
Q (James Quigley, Goldman Sachs): On CT-388, you started the phase 3 trials now. There are two of them that I've seen on ClinicalTrials.gov, and these look like traditional phase 3 designs. Can you confirm to what extent there is any flexible dosing here? Did you also consider adding semaglutide as a reference arm or even an active comparator to the study? Also, related to CT-388, what's the progress? What are the next steps in developing combinations with petrelintide? Is that still the plan, and when will we start to see some of that data?
A (Ms. Teresa Graham, Roche Pharmaceuticals CEO): On CT-388, you are right. The first two trials are relatively straightforward and standard against placebo, and that is because that is what is currently required for regulatory approval. So when you talk about bringing a new molecule into this space to the market, these are the trials that the FDA asks you to run. Therefore, that is what we are doing. We will be looking at other things going forward with CT-388, and more to come on our plans in that space. Then obviously, we're very excited about launching that fixed-dose combination that you've now heard us talk about several times.
A (Dr. Bruno Eschli, SVP & Head-Investor Relations): Regarding the combination development, this is to be kicked off in mid-year. So mid-year, we would expect the first patient.
On petrelintide
Q (Peter Verdult, BNP Paribas Exane): A couple of questions on your obesity portfolio. If we look through the lens of your R&D bar strategy about prosecuting best or first-in-class assets, I get why you're proceeding enicepatide (CT-388) forward. Interesting to hear more about the phase 3 development plans there. But I don't see how the amylin analog petrelintide can be considered first or anywhere near best-in-class. So I’m interested to hear more about your go-forward strategy there on amylin.
Just to check, is there any debate internally at Roche whether to make that sort of CHF 2 billion commitment to petrelintide for a full phase III development program?
A (Ms. Graham): First, we should talk about the fact that the amylin class is fundamentally different than the GLP-1 class. It serves a very different role in what we think is going to be a very heterogeneous obesity market. We do see a very different tolerability profile for petrelintide. So when you think about the 50% of the population globally that is going to have obesity by 2030, 2035, there is a certain portion of them that are not going to tolerate any kind of adverse event. Also, petrelintide in combination or in other uses could potentially be a really big benefit for those people who don't need to lose 20% of their body weight, but do need to lose in the low-teens, which is exactly where we saw the data come out for petrelintide, along with that placebo-like efficacy profile.
For us, as we look across the entire portfolio and the kind of offering that we want to bring to the market in terms of having a differentiated, holistic portfolio that addresses all of the different needs that patients will have, we think that there is a role for amylin to play and a role for petrelintide to play. More to come on exactly what our phase 3 trials will look like in the coming months. But I think we still continue to believe that there is a place for petrelintide.
(Dr. Thomas Schinecker, CEO, Roche Holding AG): We have announced that we will do a phase 2 combination of petrelintide and CT-388. Especially in combination, it's important to have molecules that are tolerable. We do see the potential between the molecules.
On the future outlook of the obesity market
Q (James Gordon, Barclays Capital Securities Ltd): About obesity, there are lots of different things going on in your pipeline, but we've seen some very low-cost GLP-1 generics launched in some places already, such as in India.
How do you think about obesity pricing the next decade, and what that might mean for your next-generation therapies by the time you launch? Where do you think a drug like petrelintide would be used, and could pricing now be tougher?
A (Ms. Graham): In terms of obesity pricing, this was very foreseeable. When we made the decision to enter this market, we assumed that by the time we got there, there would be significant price erosion. It's not unexpected that in certain parts of the world, you would have very low-priced options. But regardless, given the portfolio that we've put together, the clinical benefit that we think our products will provide, and the clinical differentiation that we believe that they'll represent, we do believe that there continues to be a very robust opportunity for us in obesity.
On Vabysmo
Q (Sarita Kapila, Morgan Stanley): Ahead of the Q4 data in DME, how should we think about competition to Vabysmo from Merck's MK-3000? The early data suggested a similar visual acuity improvement at 12 weeks versus 52 weeks of the Vabysmo. How should we think about the potential risk to AMD?
A (Ms. Graham): Vabysmo has done an exceptional job over the course of the last couple of years, establishing itself as the standard of care in retinal disease. We see that being consistently reinforced in all of the interviews and exchanges that we have with our retinal specialists. So, while it's always interesting to see another mechanism of action kind of enter the space, I think Vabysmo has set a high bar. They will have to sort of demonstrate that they can cross over that in the long term with their safety and efficacy data. Ophthalmology is a core area for us, but we do believe that, at the end of the day, people will need to see something that works better than Vabysmo. As of yet, we don't have anything in a phase III that's proven that.
Q (James Quigley, Goldman Sachs): What is the current bottleneck for the recovery or acceleration of Vabysmo sales in the US? We've sort of seen increased funding towards the back end of last year, but it seems to be taking a while to flow through to patients. What is going on here? Is that normal from what you've seen before? Have you started to see those bottlenecks lifting as we've gone through the quarter?
A (Ms. Graham): Vabysmo, just to reiterate, had a good quarter. 13% for the division. Back to growth in the US, 4% up. We continue to reiterate that we will see an acceleration from the 12% -- the growth that we saw overall last year.
Patient assistance foundations are not part of our commercial strategy, and we do not look at them when we think about sales. That having been said, what we have been hearing from the market is that, based on what happened last year, physicians have just gotten savvier about where to use patient assistance dollars, and they're using them for patients who truly need them. They're just thinking differently about how they're utilizing those funds as they're made available. But that is a completely different and separate thing from anything that we do on the commercial side, and I just want to be crystal clear about that.
Q (Michael Leuchten, Jefferies International): Just going back to the comment on Vabysmo US returning to growth, the revenue sequentially isn’t. So, there's 3% growth in Q1; it was 7% in Q4. So, when you say returning to growth, what's the variable that you're looking at that gives you that lead indicator that we're seeing that?
A (Ms. Graham): On Vabysmo, we saw a 4% increase in the US, but we saw a more significant volume increase. Again, this is a highly contracted market. So, those things can sometimes look a little bit different. We're also seeing the unbranded use of Avastin start to trickle down. So, that's another thing that kind of gives us confidence that the branded market may be coming back.
On AI investments
Q (Simon Baker, Rothschild): On the AI factory, could you give us an idea of how and when you will assess the impact, and how and when we will be able to assess the impact of your significant AI investments?
A (Dr. Schinecker): On AI, you saw on the slide from Bruno that you will have an update at Pharma Day. You'll see exactly how many molecules are ready in our pipeline, coming through the use of AI tools in research, and how we're going to really track that in the future, and how we can make it transparent for you, so that you can see the benefit that AI has already today. But I can say, our teams are now really utilizing AI constantly in research, and actually, a lot of the molecules have some sort of AI tools used in the development.
A (Dr. Eschli): It's fair to say it's early days. Basically, all new NMEs have one or another AI component to them, and we have established a system where we will track this progress. These molecules are to enter the clinic within the next couple of quarters. Then, of course, we have to wait one, two, three years to really collect enough data to get a feel for how this has impacted success rates, for example, or whether we were able to identify new drug targets, and many more questions to be asked. September is the point in time when we will really kick off this AI communication and provide some mid and longer-term perspectives.
-- Kat Moon, Jeremy Alkire, Nour Khachemoune, Monica Oxenreiter, Terry Vance, and Kelly Close