WCIRDC 2025 Day #2 Highlights –
Executive Highlights
- The 23rd annual World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease (WCIRDC) conference continued strongly today, with significant focus on obesity, insulin resistance, and comorbidities. We were particularly excited to attend the intimate “Meet the Experts” sessions, as well as the bustling reception at the poster hall. We continue to be inspired by the wealth of scientific intellect and clinical pearls at this meeting!
- On obesity and metabolic dysfunction, several speakers focused on pathogenic mechanisms and novel therapeutic targets. Dr. Samuel Klein (Washington University St. Louis) addressed the mechanisms behind how body weight loss improves metabolic function, including reduction in extracellular matrix remodeling and inflammation.
- Dr. Jorge Plutzky (Mass General Brigham, Harvard University) explained how angiogenesis – new blood vessel formation – contributes to health and disease, including cardiometabolic issues. While a fundamental biological process, excessive or insufficient angiogenesis can cause or contribute to various diseases, such as ischemia, retinopathies, and even obesity; efforts at therapeutic targeting of angiogenesis in these settings continue.
- Dr. Richard Pratley (Advent Health) highlighted the role of duodenum in understanding metabolic dysfunction. The duodenum protects organs from the “internal microbiome world” and conducts multiple functions, including motility; (ii) secretion; (iii) absorption; (iv) sensing; (v) communication; and (vi) immunity crucial for cardiometabolic health.
- “Meet the Experts” sessions featured Drs. Pam Taub (UCSD), Richard Pratley (Advent Health), Ralph DeFronzo (UT San Antonio), and Yehuda Handelsman (Metabolic Institute of America), who focused on cardiometabolic health, diabetes, hypercortisolism, and lipid management, respectively.
- Dr. Taub highlighted the importance of imaging techniques like CT coronary angiography to inform secondary prevention.
- Dr.Pratley shared his perspectives on why the evoke/evoke+ trials were not successful and encouraged careful GLP-1 RA use in frail older adults.
- Dr. DeFronzo spotlighted cortisol as the “forgotten hormone” that may be an underlying factor for insulin resistance.
- Dr. Handelsman advocated for early and simultaneous initiation of therapies to improve cardiometabolic outcomes.
- Several talks highlighted treatment options for comorbidities, such as obesity with MASLD or T2D with chronic kidney disease or heart failure. A liver-focused symposium spotlighted incretin-based therapies, Rezdiffra (resmetirom), and pioglitazone as available treatments for MASLD in people with obesity. In the prespecified analysis of the FINE-HEART pooled study, finerenone improved outcomes regardless of baseline A1c or antihyperglycemic drug use.
- On technology, Drs. Vivian Fonseca (Tulane University) and Seth Martin (Johns Hopkins University) shared visions for how AI can reshape diabetes and cardiometabolic care. For example, AI is integrated in automated insulin delivery systems and offers lifestyle coaching. Both speakers emphasized that technology is not a replacement for clinicians, but an ally that can augment judgment, empower patients, and enable more adaptive, equitable care.
Table of Contents
- 1. Expanding real-world cardiometabolic care: Dr. Pam Taub on the potential of imaging
- 2. Dr. Jorge Plutzky explains the role of angiogenesis on cardiometabolic health
- 3. Transforming diabetes care through AI‑driven insulin models, decision support, and digital prevention
- 4. Mechanistic impacts that may explain how body weight reduction improves metabolic function in the eyes of Dr. Samuel Klein
- 5. The role of the duodenum in metabolic dysfunction by Dr. Richard Pratley
- 6. Dr. Richard Pratley on Evoke trial results, muscle loss, and geriatric diabetes care
- 7. Bayer’s Kerendia (finerenone) improves morbidity and mortality in people with T2D in people with either CKD or HF, irrespective of baseline A1c in a pooled analysis
- 8. Liver and obesity: From shared pathogenesis to screening and management by Drs. Jennifer Green, Robert Kushner, and Amreen Dinani
- 9. Dr. Brian Feldman explains moving beyond lifestyle interventions to harness thermogenic fat in pediatric obesity
- 10. Cortisol: The “forgotten hormone” and the potential underlying factor that impacts insulin resistance
- 11. In utero exposure to maternal hyperglycemia and genetic risk independently increase T2D risk in adolescents, according to the HAPO study
- 12. Dr. Yehuda Handelsman on hypertension and lipid management
1. Expanding real-world cardiometabolic care: Dr. Pam Taub on the potential of imaging
In this “Meet the Expert” session, Dr. Pam Taub (University of California San Diego) discussed the future of cardiometabolic care. She opened by inviting audience participation, emphasizing that the cardiometabolic care inherently requires diverse perspectives and multidisciplinary solutions.
- Dr. Taub began with describing the ongoing shift in cardiology’s mindset towards metabolic disease. For many years, cardiology was resistant to integrating diabetes care. Yet, she argued, the field’s mindset was overly simplistic and failed to consider the underlying pathophysiology or wealth of emerging data. Encouragingly, she noted that cardiologists today have increasingly engaged with managing cardiometabolic disease alongside heart health.
- While cardiometabolic care is critical to improving patient outcomes, Dr. Taub noted that implementation remains difficult. Cardiology clinics are traditionally fueled by highly billable procedures. With health systems in the US prioritizing revenue in deciding which services to support, many have found difficulty opening clinics devoted to obesity or cardiometabolic care. Historically, such clinics have focused on downstream management, but Dr. Taub highlighted that they too can sponsor revenue-generating services today, including: (i) renal denervation (a highly billable, catheter-based procedure to treat resistant hypertension); and (ii) echocardiograms. With renal denervation now covered by Medicare, conditional to management by cardiometabolic or obesity clinics, such clinics have revenue-generating potential in this financially incentivized health system.
- Modern imaging techniques are essential to secondary prevention, Dr. Taub continued. To illustrate the power of imaging – which also stands as a highly billable procedure – she shared an anecdote from a concierge subgroup within her health system. Dr. Taub and her colleagues at UCSD came up with a list of evidence-based tests, including clinically-relevant biomarkers and a CT coronary angiography. Although all patients were asymptomatic and closely managed by their concierge doctor, imaging uncovered significant plaque in multiple individuals, prompting clinicians to intensify therapy and lower LDL targets. Moreover, in some cases, patients needing major cardiovascular interventions (e.g. coronary artery bypass surgery) were identified.
- Reflecting on her experience, Dr. Taub stressed that “imaging is what’s going to take off in the next five to 10 years.” She believes that CT coronary angiography should become guideline-based therapy for screening, similar to colonoscopies for cancer screening. Utilizing incidental CT results can help identify high-risk, asymptomatic population with calcification or atherosclerosis.
- On the professional guidelines, Dr. Taub took a moment to criticize the currently accepted practice. She considers the AHA’s PREVENT score “a horrible risk score,” citing studies that found the PREVENT score to significantly decrease treatment eligibility for many at-risk adults. For example, one study (n=7,765) showed that the PREVENT score would reclassify 53% of adults into lower CV risk categories and only 0.41 % would be reclassified into higher risk categories, which could limit statin use and incur ~107,000 myocardial infarction or stroke events over ten years. Moreover, the PREVENT score underestimates ASCVD risk among young adults, with less than 10% of young adults who later had an MI identified as eligible for statin therapy. She argued that professional societies are doing clinicians a “disservice” by promoting a tool that underestimates risks, while separate predictors, like a CT coronary angiography or calcium score, far better equip clinicians to identify and treat high-risk patients.
2. Dr. Jorge Plutzky explains the role of angiogenesis on cardiometabolic health
In this afternoon session, Dr. Jorge Plutzky (Harvard University) discussed the role of angiogenesis on cardiometabolic health. Angiogenesis – formation of new blood vessels – is a fundamental biological process essential for embryonic development, normal physiology, oxygen delivery, and tissue survival. However, excessive or insufficient angiogenesis can cause or enable various diseases, such as ischemia, retinopathy, vascular tumors, and cancers. Thus, angiogenesis is a promising therapeutic target.
- Angiogenesis is a highly regulated response. Upon sensing hypoxia (lack of oxygen), inflammatory markers, or hemodynamic stress, endothelial cells stimulate growth factor signaling pathways that induce angiogenesis. The pathway is complex and involves a range of molecules, such as: (i) growth factors (e.g., vascular endothelial growth factors [VEGF], angiopoietins); (ii) receptors (e.g., VEGFR, TIE receptors); (iii) integrins for cell-to-cell adhesion; and (iv) ephrin and Notch receptors for cell-to-cell communication.
- Limited or excessive angiogenesis can cause various diseases. Insufficient angiogenesis can cause ischemic diseases (inadequate blood supply), such as peripheral arterial disease or chronic diabetic foot complications, where tissues die from inadequate oxygen supply. Excessive angiogenesis, on the other hand, can lead to diabetic retinopathy and vascular tumors. For example, diabetic retinopathy could be caused by loss of pericytes (cells surrounding capillaries), endothelial cell dysfunction, or changes in basement membranes, leading to neovascularization that threaten vision loss.
- Dr. Plutzky explained that angiogenesis may play a role in obesity and cardiometabolic disease, as well. Adipose tissues are highly vascularized and interact with the systemic circulation, producing endocrine signals that influence inflammation, insulin resistance, and atherosclerosis. He introduced an increasingly supported hypothesis, which suggests that obesity induces adipose tissue hypoxia and downstream metabolic dysfunction. For example, one study found that excess fat mass is associated with limited oxygen availability for adipose tissue, which then stimulates angiogenesis, inflammation, metabolic dysfunction, and atherogenesis. Dr. Plutzky concluded that targeting the angiogenesis pathway, such as VEGF or novel therapeutic target FAM222A, could mitigate diseases.
3. Transforming diabetes care through AI‑driven insulin models, decision support, and digital prevention
In a compelling showcase of AI’s clinical utility, Drs. Vivian Fonseca (Tulane University) and Seth Martin (Johns Hopkins University) presented complementary visions for how artificial intelligence (AI) can reshape diabetes and cardiometabolic care, from insulin dosing to lifestyle coaching. Both speakers emphasized that technology is not a replacement for clinicians, but a pragmatic ally that can augment judgment, empower patients, and enable more adaptive, equitable care.
- Dr. Fonseca highlighted the integration of AI into automated insulin delivery (AID) systems, where continuous glucose monitoring, insulin dosing, carbohydrate intake, and exercise data feed into digital twin models and adaptive control algorithms. Dr. Fonseca highlighted one study (n=72) which showed that AI allowed patients and providers to replay “what‑if” scenarios in silico, fine‑tuning insulin parameters to improve time in range from 73% to 77%, A1c from 6.8% to 6.6%, and mean glucose from 152 mg/dL to 146 mg/dL. Dr. Fonseca cited another study (n=27,904) which found that AI‑driven clinical decision support can guide pharmacotherapy, specifically in T2D, by translating patient data – such as comorbidities, lab values, and demographics – into individualized treatment recommendations aligned with guideline‑based care.
- Importantly, he stressed that equity must be central to AI deployment, with models incorporating social determinants of health to avoid widening disparities. Dr. Fonseca’s vision positions AI as a tool for personalization at scale, linking mechanistic insights directly to real-world outcomes. Dr. Fonseca cited a Wall Street Journal article titled “I Finally Have a Physician Who’s Available and Who Gets Me. Meet Dr. Grok,” which reflects growing public interest in AI chatbots as virtual physicians and tools that offer constant availability and personalized engagement, in contrast to time-constrained human clinicians.
- Dr. Martin highlighted the use of AI to scale lifestyle interventions for cardiometabolic prevention, presenting data from a randomized trial comparing a fully automated, AI-led Diabetes Prevention Program (DPP) to traditional human coaching. In the study (n=368), adults with prediabetes and overweight or obesity were randomized to either AI-led DPP or human-led DPP. Those in the AI-led DPP group achieved noninferior results on a composite outcome of: (i) ≥5% weight loss; (ii) 4% weight loss with 150 minutes of weekly physical activity; or (iii) an absolute A1c reduction of ≥0.2 percentage points with A1c maintained at <6.5%. Dr. Martin highlighted the behavioral design of an AI coach that offers personalized push notifications for users to walk after screen time, choose healthier restaurants, or track weight daily, while mimicking the cadence and tone of human support.
- Dr. Martin also highlighted the Corrie Lipids Program, a digital health‑enabled implementation initiative designed to optimize LDL‑c management through patient‑facing apps, clinician dashboards, and a rapid therapy intensification pathway. In addition, he referenced the phase 2 RESILIENT trial (n=400), which showed that mobile health cardiac rehabilitation – delivered via tablet-based software, Fitbit monitoring, and weekly therapist calls – modestly improved 6-minute walk distance in adults aged 65 and older with coronary artery disease, with a treatment effect of 15.6 meters.
- Dr. Martin closed by framing digital transformation as a clinical imperative in cardiometabolism. He urged clinicians to embrace the technologies already embedded in patients’ daily routines, including smartphones, wearables, and remote platforms, not as replacements, but as tools that extend reach and reinforce human connection. In his view, the future of care will depend on clinicians who can integrate digital tools with empathy and clinical judgment, using AI to personalize prevention while preserving the relational core of medicine.
4. Mechanistic impacts that may explain how body weight reduction improves metabolic function in the eyes of Dr. Samuel Klein
In a morning session, Dr. Samuel Klein (Washington University St. Louis) addressed the mechanisms behind how body weight reduction improves metabolic function. While the metabolic benefits of weight loss are widely understood, the underlying pathways are not clear. Dr. Klein acknowledged that this uncertainty would persist even after his presentation. However, he continued to highlight the well-established relationship between weight loss and improved insulin sensitivity, citing a 2016 study that showed even a modest 5% weight loss can improve insulin sensitivity in people living with obesity. The study showed that progressive weight loss (i.e., 11% and 16%) leads to even greater improvements across liver and muscle insulin sensitivity, as well as beta cell function.
- Decreasing adipose tissue mass alone does not lead to metabolic benefits of weight loss. Dr. Klein previously conducted a 2004 study that measured the effects of large-volume liposuction on glucose production and disposal. Results demonstrated no difference in insulin sensitivity before and after the surgical procedure, suggesting that weight loss due to fat removal has no effect on insulin sensitivity. A follow-up 2010 study evaluated whether the reduction of visceral adipose tissue through the surgical removal of the omentum, a fold of peritoneum, improves metabolic function in people with obesity. Similar to the previous study, findings showed no difference in insulin sensitivity and metabolic function from the reduction of visceral adipose tissue through omentectomy. These results further reinforce that the metabolic benefits of weight loss likely depend on underlying biological mechanisms rather than fat loss alone.
- Potential mechanisms that may explain the metabolic benefits of weight loss. Dr. Klein expanded on findings from his recently published study in Diabetes Care, which examined the biological mechanisms of adipose tissue that may drive the beneficial outcomes of weight loss. The study found that weight loss: (i) decreased adipose tissue gene expression of ones involved in extracellular matrix remodeling; (ii) didn’t change expression of immune cells or inflammation related genes except SERPINE 1, which encodes plasminogen activator inhibitor (PAI-1); (iii) decreased expressions of PAI-1 and leptin, while increased plasma high-molecular weight adiponectin; and (iv) decreased concentration of plasma small extracellular vesicle (sEV) and sEV content of miRNAs thought to inhibit insulin action. Regarding PAI-1, Dr. Klein explained that higher PAI-1 levels are strongly associated with insulin resistance; therefore, PAI-1 may be considered an important biomarker for insulin sensitivity and metabolic function. He also commented that the reduction of sEV may improve insulin sensitivity by decreasing signals that interfere with insulin mechanisms.
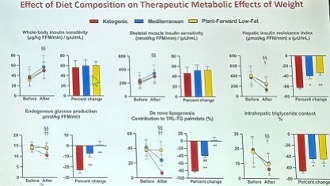
- The effect of diet composition on the therapeutic metabolic effects of weight loss. Dr. Klein concluded the session by reviewing unpublished results from a study that assessed the metabolic effects of macronutrient qualities. The study provided participants with packaged meals, and they were assigned to receive either a ketogenic, Mediterranean, or plant-forward and low-fat diet. While results showed improvements in whole-body and skeletal muscle insulin sensitivity across all groups, no significant difference was observed between them. However, in comparison to the Mediterranean and plant-forward groups, the ketogenic group showed significant improvements in hepatic insulin resistance, endogenous glucose production, de novo lipogenesis, and intrahepatic triglyceride content. These results highlight that a ketogenic diet may confer greater liver-specific benefits, in addition to demonstrating similar weight loss seen across other diet groups.
5. The role of the duodenum in metabolic dysfunction by Dr. Richard Pratley
Dr. Richard Pratley (Advent Health) presented on the duodenum, an “underappreciated organ” that is often overlooked in understanding metabolic dysfunction. The duodenum serves a crucial role in the body, protecting organs from the “internal microbiome world,” similar to how skins protect the outer body. Additionally, the duodenum possesses multiple functions, including: (i) motility; (ii) secretion; (iii) absorption; (iv) sensing; (v) communication; and (vi) immunity. Dr. Pratley further emphasized the duodenum’s adaptability to environmental changes by referring to a 2018 study, in which the duodenum in mice models showed alterations in nutrient transport and changes in enteroendocrine hormones in response to variations in nutritional intake.
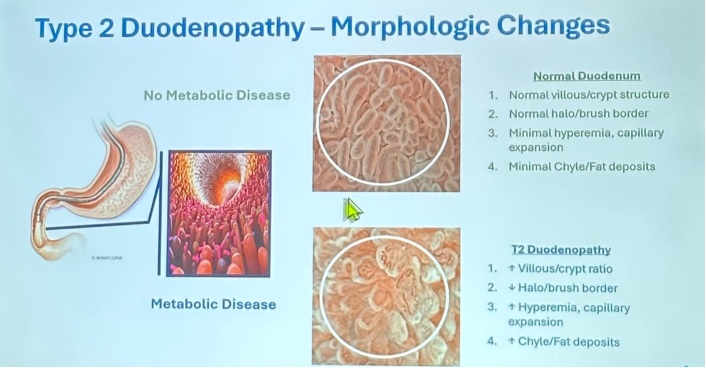
- Morphologic changes of the duodenum in T2D. Comparing the duodenum morphology between people with T2D and healthy controls, Dr. Pratley highlighted key differences. Those with T2D exhibit: (i) increased villous/crypt ratio; (ii) decreased halo/brush border; (iii) increased hyperemia and capillary expansion; and (iv) increased chyle/fat deposits. Dr. Pratley then suggested that the increased gut dysbiosis, inflammation, stromal hypertrophy, and leaky tight junctions contribute to the dysfunction of the duodenum, ultimately leading to insulin resistance. Insulin resistance then impacts glycemic management, affecting dysfunction across the enteroendocrine, enteric nervous system, and GI mobility. These impacts collectively lead to hepatic and peripheral insulin resistance, as well as a decrease in beta cell function.
- The duodenum represents an additional target for metabolic diseases. Dr. Pratley said that Dr. Ralph DeFronzo (University of Texas San Antonio) should include duodenopathy and update his “ominous octet” to the “terrible ten,” positioning the duodenum as an important organ to understand disease-modifying effects. While multiple approaches are under development to treat duodenopathy, there are more unanswered questions about the pathogenesis and role in metabolic function. For example, Dr. Pratley questioned whether duodenopathy represents a primary consequence of T2D and whether it’s related to nutrients or toxic exposures. Furthermore, he inquired about the relationship between duodenopathy and insulin resistance, systemic inflammation, MASLD/MASH, CVD, and CKD. Finally, he questioned how weight loss and diabetes treatments could affect duodenopathy.
- GIP and GLP-1 localization in the gut. The GIP and GLP-1 have been well-characterized in the gut, with greater expression of GIP in the duodenum and smaller expression distally in the small intestine; on the other hand, GLP expression diminishes progressively along the intestine, with the highest density in the duodenum. Despite the distal distribution of GLP-1, its secretion increases within minutes of food intake due to the signaling within the gut. Notably, studies have found no significant differences in GIP, GLP-1, or secretin expression between people with diabetes and healthy controls, suggesting that the pathophysiology of diabetes is not necessarily related to hormone secretion but rather to hormone responsiveness. Overall, Dr. Pratley highlighted the interconnectedness of the enteric nervous system, immune system, and intestinal epithelium.
6. Dr. Richard Pratley on Evoke trial results, muscle loss, and geriatric diabetes care
In this intimate “Meet the Experts” session, where attendees sat in a circle, Dr. Richard Pratley (AdventHealth) offered a sweeping look at non‑traditional diabetes types, emerging therapies, and broader implications of GLP‑1 RAs. The discussion underscored how diabetes care increasingly intersects with neurology, geriatrics, and more, reminding clinicians that individual clinical contexts and timing are as critical as the therapies themselves. Two topics in particular struck us while listening to Dr. Pratley, including his perspective on the evoke/evoke+ trials and his cautionary insights on frail older adults receiving GLP‑1 RA therapy.
- Dr. Pratley gave valuable insights on the recent results from the phase 3 evoke and evoke+ trials (n=3,808). In the trials, semaglutide improved certain biomarkers of neuroinflammation and neurodegeneration, but did not significantly slow disease progression as measured by the Clinical Dementia Rating-Sum of Boxes (CDR‑SB). The one‑year extension phase was discontinued, underscoring the challenge of intervening once cognitive decline is already underway. Reflecting on the results, Dr. Pratley emphasized that the promise of GLP‑1 RAs in Alzheimer’s disease may hinge on timing. He believes that treatment was likely introduced far too late in the disease progression. Dr. Pratley reminded the audience that over the past decades, clinical research on Alzheimer’s disease failed to demonstrate consistent success because many targeted beta amyloid removal after neurons had already degenerated. He drew a parallel to GLP‑1 RAs, noting that even if this class showed biomarker improvements, they cannot restore lost function once neuronal death has occurred. Thus, he emphasized the need to target early cognitive decline with future candidates and trials.
- Turning to the realities of patient care, Dr. Pratley underscored how trial populations often diverge from clinical practice, especially in older and more vulnerable adults, despite that nearly 30% of adults over 65 have diabetes. While trials like PIONEER (n=703) on oral semaglutide included a significant percentage of older adults (mean age of 55 years), many earlier studies lacked long-term exposure data and diversity across age, leaving clinicians with limited guidance on how these drugs perform in geriatric settings. Dr. Pratley cautioned that although GLP-1 RAs often improve outcomes in trials, their effects in frail older patients can be unpredictable. In his own clinic, he has seen older individuals become weak and lose appetite after starting GLP-1 RA therapy, requiring discontinuation. This underscores the need for careful judgment and individualized care when translating trial results into practice. Dr. Pratley urged clinicians not to let protective instincts prevent access to beneficial therapies, but to remain vigilant about the unique vulnerabilities of older adults. See our previous coverage from WCIRDC 2024 for a debate between Dr. Pratley and Dr. Samuel Klein (Washington University in St. Louis) on the significance of lean mass loss with GLP-1 RAs.
7. Bayer’s Kerendia (finerenone) improves morbidity and mortality in people with T2D in people with either CKD or HF, irrespective of baseline A1c in a pooled analysis
In this engaging evening session, Dr. John Ostrominski (Harvard University) presented a prespecified pooled analysis evaluating finerenone across major heart failure (HF) and chronic kidney disease (CKD) trials. Diabetes is a major driver of cardiovascular-kidney-metabolic (CKM) epidemiology. Specifically, high fasting plasma glucose is the leading attributable risk factor for CKD worldwide, followed by BMI and elevated systolic blood pressure. Furthermore, T2D is an important risk factor for HF, conferring substantially higher risk of the disease roughly five to 10 years earlier than those without diabetes. T2D, CKD, and CVD commonly and increasingly converge, underscoring the importance of dedicated research targeting these “clinically relevant and high-risk intersections.”
- Given that T2D is a heterogeneous spectrum, Dr. Ostrominski emphasized the need to understand how novel therapies, such as finerenone, perform across the diverse patient profiles. Previously, studies had not comprehensively evaluated whether finerenone’s safety or efficacy vary by baseline glycemic levels or background glucose-lowering therapy, prompting the development of the FINE-HEART pooled analysis. The three aims of the study were: (i) to characterize clinical profiles of people with T2D across finerenone outcomes trials; (ii) determine whether baseline A1c modifies finerenone’s effects; and (iii) assess whether finerenone’s effects differ depending on glucose-lowering treatment regimens.
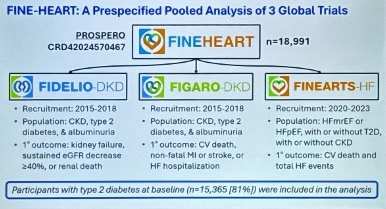
- FINE-HEART study pooled data from three global finerenone trials – FIDELIO-DKD, FIGARO-DKD, and FINEARTS-HF – to establish a cohort of 15,365 participants across the broad spectrum of T2D. Across the pooled population, baseline A1c did not significantly modify outcomes, including CV death, nonfatal MI, nonfatal stroke, HF hospitalization, new-onset atrial fibrillation, or all-cause hospitalization. Similarly, background glucose lowering-therapy – whether stratified by therapy or number of agents – did not influence finerenone’s effects on CV death, the kidney composite endpoint, HF hospitalization, or MACE. Finally, the analysis also found no significant interaction with baseline SGLT-2 inhibitor or GLP-1 RA use, though the uptake of these therapies was notably low (<10% in the analyzed population).
- Clinically, finerenone’s benefits on cardiovascular and kidney outcomes appeared consistent regardless of baseline A1c or glucose-lowering therapies. Nevertheless, Dr. Ostrominski highlighted two key limitations of the study: (i) the inability to rigorously evaluate all unique glucose-lowering regimens (given the small number); and (ii) low background SGLT-2 inhibitor and GLP-1 RA use due to when the trial was held. Even so, the findings reinforce finerenone as a valuable therapy in reducing morbidity and mortality in people with T2D and either CKD or HF, independent of glycemic levels at baseline or glucose-lowering therapy use.
8. Liver and obesity: From shared pathogenesis to screening and management by Drs. Jennifer Green, Robert Kushner, and Amreen Dinani
In this BI-sponsored breakfast symposium, panelists Drs. Jennifer Green (Duke University), Robert Kushner (Northwestern University), and Amreen Dinani (Duke) discussed the pathogenesis underlying obesity and liver disease, as well as screening and management strategies. Dr. Kushner began by introducing the Lancet Diabetes & Endocrinology Commission’s new diagnostic criteria of “clinical obesity,” which includes metabolic dysfunction-associated steatotic liver disease (MASLD) as one of the clinical manifestations of excess adipose tissue. MASLD is a progressive disease caused by accumulation of insulin-resistant adipose tissue (steatosis) that develops into cirrhosis via scarring (fibrosis) from mitochondrial dysfunction and inflammation. MASLD shares common risk factors with cardiovascular disease (CVD) and increases the risk of diabetes, chronic kidney disease, and liver-related events. Therefore, it is important to diagnose and intervene early in disease progression.
- Screening for MASLD and MASH is recommended for individuals at high risk, such as those with T2D, obesity, or family history of cirrhosis due to MASLD or MASH. Dr. Dinani stressed that MASLD screening should be done in people with T2D regardless of liver test results, as the enzyme levels may be affected later in disease progression. Panelists encouraged using the FIB-4 score to assess the risk of advanced liver fibrosis using age, AST, ALT, and platelet values. Individuals with FIB-4 score <1.3 are unlikely to have advanced fibrosis, while those with >2.67 are likely to have advanced fibrosis. For patients with elevated, clinicians can further assess liver stiffness via elastography or enhanced liver fibrosis (ELF) test and refer to hepatologists.
- On management, panelists highlighted lifestyle modifications, bariatric surgery, and pharmacotherapy. Lifestyle changes include caloric deficit, weight loss, and exercise. Dr. Kushner especially advised against fruit juices and table sugar high in fructose content, as well as heavy alcohol consumption. Given that weight loss is associated with steatosis improvement, MASH resolution, and fibrosis regression, bariatric surgery is also beneficial. Indeed, according to the BRAVES study (n=431), individuals who underwent bariatric surgery experienced 3.6 times greater MASH resolution compared to the lifestyle group at one year of follow up. Dr. Green encouraged considering surgery earlier than later, as patients generally have better health to tolerate surgeries and can reap a wide range of cardiovascular-kidney-metabolic benefits.
- On pharmacotherapy, panelists discussed semaglutide and resmetirom as two FDA-approved therapies, as well as emerging treatments.
- Incretin-based therapies. Semaglutide was approved in August 2025 based on the Part 1 of the phase 3 ESSENCE trial (n=1,200). In the study, 37% of the semaglutide group experienced improvement in liver fibrosis with no worsening of steatohepatitis vs. 23% with placebo at Week 72, and 63% of the semaglutide group achieved resolution of steatohepatitis with no worsening of liver fibrosis vs. 34% with placebo. Given the pleiotropic effects of GLP-1 RAs on the brain, heart, kidney, and more, this drug class is highly recommended. Panelists shared excitement about tirzepatide (dual GLP-1/GIP RA), which showed promising benefits in the phase 3 SURPASS-3 substudy and phase 2 SYNERGY-NASH.
- Rezdiffra (resmetirom), thyroid hormone receptor-β agonist, received FDA-approval in 2024 based on the MAESTRO-NASH trial (n=966), in which Rezdiffra reduced hepatic triglycerides and improved both MASH resolution and fibrosis in people with MASH with moderate to advanced fibrosis (F2-F3).
- Pioglitazone has shown to improve liver enzymes, steatosis, inflammation, fibrosis (p=0.04), and MASH resolution in a phase 4 study (n=176). Because pioglitazone may cause weight gain, panelists encouraged combined use with SGLT-2 inhibitors and GLP-1 RAs.
- Emerging pharmacotherapies include:
- Incretin-based therapies, such as tirzepatide (GLP-1/GIP RA), survodutide (GLP-1/glucagon RA), efinopegdutide (GLP-1/glucagon RA), and pemvidutide (GLP-1/glucagon RA);
- PPAR agonists, including lanifibranor (Pan-PPAR agonist), chiglitazar (Pan-PPAR agonist), and saroglitazar (PPAR- α/γ agonist);
- FGF21 analogs, such as pegozafermin and efruxifermin; and
- Denifanstat (fatty acid synthase inhibitor) and ION224 (DGAT2 antisense inhibitor).
- Throughout the symposium, panelists shared advice on how to communicate with patients about managing obesity and MASLD without exacerbating stigma. Dr. Kushner emphasizes to his patients that obesity is a chronic condition with many biological mechanisms that make weight loss difficult – thereby taking blame away from patients. Despite recent changes in nomenclature, Dr. Dinani said that she often “cringes” with the phrase “fatty liver”, given the stigma associated with the word “fat.” Thus, when using this phrase with patients, she makes effort to translate the underlying science to patients. Dr. Green stressed that patients may feel confused, intimidated, or surprised when first diagnosed with MASLD, which could deter patients from retaining clinical advice on lifestyle changes and treatment options. Hence, it is important for clinicians to follow up on patients’ understanding on a regular basis. She also advocated for early screening and detection of MASLD, as there are more opportunities to prevent disease progression.
9. Dr. Brian Feldman explains moving beyond lifestyle interventions to harness thermogenic fat in pediatric obesity
In this packed morning session, Dr. Brian Feldman (Yale University) delivered an overview of emerging strategies to treat obesity and T2D in children. He prefaced with the sobering fact that we have transitioned to an era of treating these metabolic diseases in children as opposed to preventing them, given that 20% of children and adolescents now live with obesity. Dr. Feldman emphasized that pediatric physiology demands tailored approaches, stating, “Kids are not just small adults.” The pubertal phase is a critical window where insulin sensitivity naturally declines, and when combined with obesogenic environments and genetic predisposition, this can accelerate the onset of metabolic dysfunction. The rise in pediatric obesity is multifactorial, and while lifestyle interventions remain foundational, Dr. Feldman underscored that they are no longer sufficient on their own.
- Dr. Feldman reviewed data from the SURMOUNT-1 trial (n=2,539), in which tirzepatide 15 mg conferred up to 17.9% weight loss. While the study was conducted in adults, he focused on the challenges of sustaining benefits during off-treatment periods, which would be particularly important to consider in the context of prescribing a chronic medication for children. Pediatric data remain limited, though early signals are emerging. In a real-world study (n=74) of liraglutide in children aged six to 12 years, participants achieved meaningful reductions in BMI and waist-to-height ratio, with 82.6% reaching ≥5% BMI reduction and nearly half achieving ≥10%. However, with most studies done in adults and response variability evident even in pediatric cohorts, he argued that the current therapeutic toolbox is too narrow.
- Dr. Feldman’s lab is exploring the other side of the energy balance equation: increasing energy expenditure through thermogenic fat. Beige adipocytes, which can uncouple mitochondrial respiration to release heat instead of storing energy as ATP, offer a promising avenue. A key focus of Dr. Feldman’s research is the role of glucocorticoids, which act as negative regulators of beiging of adipose tissue, shifting white adipocytes toward brown-like properties. Patients with excess glucocorticoids exposure exhibit significantly increased fat mass and metabolic dysfunction. Given that glucocorticoids are among the most prescribed anti-inflammatory therapies, Dr. Feldman called for a deeper understanding of their impact on adipose biology. His lab has identified Klf15 as a glucocorticoid-regulated transcription factor that suppresses beiging. Recent data suggest that targeting Klf15 in white adipocytes may be sufficient to induce beige characteristics in vivo. These findings open the door to novel physiology-informed interventions that extend beyond calorie restriction and rewire energy metabolism at the cellular level.
10. Cortisol: The “forgotten hormone” and the potential underlying factor that impacts insulin resistance
During the “Meet the Experts” session, Dr. Ralph DeFronzo (UT Health San Antonio) spotlighted cortisol as the “forgotten hormone.” Referring to yesterday’s presentation by Dr. Vivian Fonesca (Tulane University), who provided an overview of the impact of excessive cortisol levels on insulin resistance, Dr. DeFronzo emphasized the importance of studying cortisol levels in people with diabetes. He began the session by explaining that not a lot of attention has been focused on hypercortisolism in the US, whereas, in comparison, several studies in the EU have highlighted the prevalence of high cortisol levels and the importance of glycemic management. Indeed, Part 1 (n=1,113) of the CATALYST trial revealed that 24% of individuals with difficult-to-manage T2D had underlying hypercortisolism, despite treatment with multiple glucose-lowering treatments. Part 2 (n=252) of the trial then positioned Korlym (mifepristone), a glucocorticoid receptor antagonist, as a promising treatment for hypercortisolism. At Week 24, the mean A1c decreased from 8.6% to 7.1% with mifepristone, compared to a decrease from 8.4% to 8.4% with placebo. Referring to the high prevalence of hypercortisolism and the efficacious results of mifepristone, Dr. DeFronzo elaborated on the trial design, the mechanistic impact of cortisol, and considerations for future studies.
- The concerning prevalence of hypercortisolism. Before conducting the CATALYST trial, Dr. DeFronzo underestimated the proportion of people with T2D affected by hypercortisolism. Given the NHANES data of an estimated 40 million people with diabetes, 25% (10 million) live with A1c >8%. Half of this population (5 million) is on oral medications, and therefore, applying findings from the CATALYST trial, approximately 1.2 million people live with hypercortisolism in the US. Dr. DeFronzo has clearly seen this high prevalence in his clinical trial center, where 13 out of the first 33 study participants were diagnosed with hypercortisolism. Given these findings, Dr. DeFronzo said the following “big four” characteristics should serve as a “light bulb” for HCPs to detect hypercortisolism: (i) difficult-to-manage diabetes; (ii) overweight or obesity, specifically related to visceral fat; (iii) hypertension; and (iv) osteoporosis or history of fractures. Dr. DeFronzo said he might even consider expanding these characteristics to include psychiatric conditions, as cortisol impacts the central nervous system.
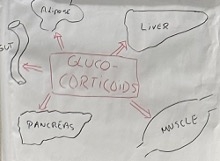
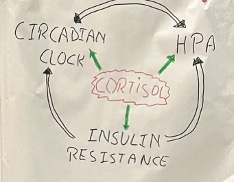
- The mechanistic impact of cortisol level on multiple organs. Referring to his hand-drawn diagram (see below), Dr. DeFronzo detailed the mechanisms of how cortisol impairs metabolic health. In skeletal muscle, cortisol reduces GLUT4 translocation, decreasing glucose uptake into the muscle. In the liver, cortisol stimulates gluconeogenesis and glycogenolysis. Furthermore, cortisol impairs insulin synthesis and secretion in the pancreas, as well as reduces resistance to GLP-1. Cortisol also inhibits GLP-1 synthesis in the gut, stimulates lipolysis, and increases free fatty acids, thereby worsening insulin resistance and promoting hepatic fat accumulation.
- The “endless circuit” of hypercortisolism, the hypothalamic-pituitary-adrenal (HPA) axis, and insulin resistance. Presenting another hand-drawn diagram (see figure below), Dr. DeFronzo explained that cortisol could interfere with the circadian clock, which then overreacts the HPA and eventually induces insulin resistance. Alternatively, insulin resistance would interfere with the circadian clock and activate the HPA. With either explanation, the following question remains: Where does the problem start? While this question remains unanswered at the moment, Dr. DeFronzo expressed confidence that adrenal conditions influence the development of diabetes and that insulin resistance contributes to the oversecretion of cortisol. Finally, once the process of the “endless circuit” begins, all the multifaceted factors interact with one another.
11. In utero exposure to maternal hyperglycemia and genetic risk independently increase T2D risk in adolescents, according to the HAPO study
In this joint session with Diabetes Care, Dr. Abigayil Dieguez (Northwestern University) examined how in-utero exposure of maternal hyperglycemia and genetic risk for T2D contribute to impaired glucose tolerance and T2D in early adolescence. T2D is a growing crisis in children with a nearly 5% increase in annual incidence of T2D in youth. In children, the disease is characterized by a faster disease progression with earlier onset to complications. Thus, Dr. Dieguez underscored the critical need for early-life risk stratification to inform clinical management.
- To better understand contributors to youth-onset T2D, Dr. Dieguez and her colleagues(senior author: Marie-France Hivert, MD, MMSc) investigated two independent risk pathways in participants from the HAPO follow-up study cohort (n=4,160): (i) in-utero exposure of maternal hyperglycemia (gestational diabetes); and (ii) genetic risk for T2D. On the latter, researchers determined a genetic risk score for T2D with the weighted sum of risk alleles from T2D-Global Genetics Initiative.
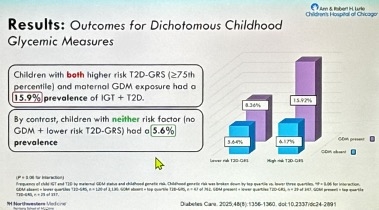
- Results. Both material hyperglycemia and higher genetic risk score for T2D were independently associated with impaired glucose tolerance or incident T2D in adolescence (p<0.05). These risk factors also corresponded to elevated glucose levels across all OGTT timepoints. Furthermore, exposure to maternal hyperglycemia and T2D-GRS were associated with reduced beta cell function and insulin sensitivity. Strikingly, adolescents with both high T2D genetic risk (≥75th percentile) and maternal GDM exposure had a 16% prevalence of impaired glucose tolerance or T2D, compared to 6% among those with neither of the risk factors.
- Clinically, in-utero exposure to maternal hyperglycemia and elevated T2D genetic risk operate as independent risk factors, yet exhibit additive effects when combined – nearly tripling the likelihood of impaired glucose tolerance or T2D in youth. Dr. Dieguez concluded that integrating these early-life markers could enable targeted preventative interventions for children at the highest risk.
12. Dr. Yehuda Handelsman on hypertension and lipid management
In this concurrent “meet the experts” session, Dr. Yehuda Handelsman (Metabolic Institute of America) discussed lipid and hypertension management. He began that the fields experienced little innovation for years but is now entering an exciting period with new therapeutic targets, emerging treatments, and investment from the pharmaceutical industry. New topics include Lp(a) – a highly atherogenic particle and an independent risk factor for ASCVD – ANGPTL3 inhibitors for familial hypercholesterolemia, APOC3 inhibitors for severe hypertriglyceridemia, and oral PCSK-9 inhibitors in development for LDL cholesterol reduction.
- Amid expanding treatment options for cardiometabolic health, Dr. Handelsman encouraged early and simultaneous initiation of combination therapy to improve outcomes. In the phase 3 CONFIDENCE trial (n=784), SGLT-2 inhibitors and finerenone combination therapy conferred 52% reduction in uACR from baseline, reflecting a 32% greater reduction compared to empagliflozin monotherapy and 29% greater reduction in finerenone monotherapy. In the STOP DIABETES study (n=1,860), as presented yesterday, triple therapy of metformin, pioglitazone, and GLP-1 RA in addition to lifestyle management prevented diabetes progression in all participants (n=81) at risk of diabetes after five to seven years. Dr. Handelsman said, “diabetes does not have to be a progressive disease” if glucotoxicity was controlled early before it damages beta cell function. For most people, an ideal A1c to preserve beta cells is below 5% for both people with and without diabetes. Similarly, in cardiovascular care, combining aldosterone synthase inhibitors with RAAS inhibitors like ACEi and ARBs suggest synergistic effects for blood pressure, kidney protection, and heart failure. Ultimately, Dr. Handelsman emphasized the importance of maximal CV risk reduction via early and intensive treatments.
- After years of stagnation, the AHA published a new guideline on its prevention, detection, and management of hypertension. Dr. Handelsman said that the new guideline aimed to reflect shifting clinical targets and new therapies. Notably, the new target for systolic blood pressure has decreased from 130 mmHg to 120 mmHg for at-risk populations, including those with diabetes, chronic kidney disease, or prior stroke. New therapeutic modalities include: (i) renal denervation, which applies energy to nerves around renal arteries to disrupt hypertensive signals; (ii) aldosterone synthase inhibitors, which block aldosterone production rather than receptors; and (iii) endothelin receptor antagonists like Tryvio (aprocitentan) for resistant hypertension.
- Finally, Dr. Handelsman highlighted that hypercortisolism could be an underlying cause of hypertension and difficult-to-manage diabetes.In Part 1 of the CATALYST trial (n=1,113), nearly one-quarter of individuals with difficult-to-manage T2D had underlying hypercortisolism, far exceeding the prediction. 33% of this study population had resistant hypertension and 30% had established CVD, suggesting that hypercortisolism may be an underrecognized contributor to metabolic and blood pressure dysregulation.
--by Kayla Mathieu, Elizabeth Rose, Esther Min, Kat Moon, Monica Oxenreiter, and Kelly Close