ATTD 2026 Day #3 Highlights –
Executive Highlights
- Attendees continued to gather at the 19th International Conference on Advanced Technologies & Treatments for Diabetes (ATTD), where new data and clinical insights kept the momentum high. A standout session was the 17th ATTD Yearbook, which drew a packed auditorium for 18 rapid-fire talks highlighting key themes and notable studies — from CGM and AID in special populations to emerging therapies for T1D.
- In tech, Dr. Ahmad Haider (McGill University, Canada) presented intriguing data on continuous ketone monitoring in people with T1D taking empagliflozin. Based on a small dataset of 24 participants, his team proposed preliminary targets for time spent in ketosis: <3% for level 1 ketosis (>1 mM) and <1% for level 2 ketosis (>1.5 mM). He emphasized that these thresholds are empirical rather than definitive, but they offer an early framework as continuous ketone monitoring becomes more widely available.
- In therapy, Dr. Satish Garg (University of Colorado) previewed guidance from an upcoming consensus report on adjunctive incretin use in people with T1D and obesity, slated for publication in the June issue of DT&T. Currently, pramlintide — an amylin analogue — is the only FDA-approved therapy for T1D with potential weight-loss benefits. Yet prescriptions for GLP-1 RAs have surged in the US, prompting the need for clearer guidance. At the University of Colorado’s Barbara Davis Center alone, more than 700 people with T1D have been prescribed semaglutide or tirzepatide.
- Screening and early detection was also a focus at an IDF Europe lunch symposium dedicated to “turning vision into reality.” Prof. Tadej Battelino (University of Ljubljana, Slovenia) opened the session by highlighting the timeliness of advances in early-stage T1D. Dr. Sufyan Hussain (King’s College London, UK) presented a newly published international consensus on screening and monitoring early-stage T1D. Ms. Marissa Hitchcock Town (Children with Diabetes) addressed diabetes stigma and practical considerations for population screening, followed by Prof. Tsvetalina Tankova (University of Sofia, Bulgaria) on cardiovascular prevention in dysglycemia and diabetes, and Prof. Sanja Klobucar (University of Rijeka, Croatia) on CGM use in people with obesity, intermediate hyperglycemia, or T2D.
- Dr. Viswanathan Mohan (Dr. Mohan’s Diabetes Specialities Centre) explored lifestyle approaches to preventing T2D, focusing on three metabolic subtypes of prediabetes: isolated impaired fasting glucose (IFG), isolated impaired glucose tolerance (IGT), and combined IFG/IGT. In South Asian populations, he noted, even modest weight loss can significantly reduce progression to diabetes. He also highlighted the under-discussed concept of prediabetes remission. New analyses from the D-CLIP study suggest that regression to normoglycemia is both possible and predictable, and is more common among younger individuals with lower baseline A1c, less insulin resistance, and better preserved beta-cell function.
Table of Contents
-
2026 Yearbook – 18 insightful presentations to a packed crowd!
- 1. Continuous and intermittent glucose monitoring
- 2. Insulin delivery hardware: Pumps and pens
- 3. New insulins, biosimilars, and insulin therapy
- 4. Closed-loop, decision support, and AI
- 5. Using digital health technology to prevent and treat diabetes
- 6. Technology and pregnancy
- 7. Diabetes technology and therapy in the pediatric age group
- 8. Advances in exercise and nutrition as therapy in diabetes
- 9. Primary care and diabetes technologies and treatments
- 10. Use of technologies at the advanced age
- 11. The Real “Real World”: Overcoming practical barriers and disparities in diabetes technology
- 12. Diabetes technology in the hospital
- 13. Impact of diabetes technologies on psychosocial outcomes
- 14. Immune intervention and beta cell replacement therapies in T1D
- 15. Obesity and diabetes
- 16. Emerging trends in MASLD and MASH
- 17. Virtual clinics for diabetes care
- 18. New medications for the treatment of diabetes
-
Technology Highlights
- 1. Debate: Should A1c or CGM be the gold standard for glycemic management?
- 2. mylife Diabetes Care: Evidence and clinical pearls for personalization AID with CamAPS FX
- 3. CGM metrics as predictors of vascular risk: Insights from Virtual DCCT and real‑world evidence
- 4. Dr. Ahmad Haider takes a first pass at recommendations for continuous ketone level targets for people with T1D on SGLT-2 inhibitors
- 5. A preview of continuous ketone monitoring data from Abbott; Drs. Ketan Dhatariya and Rich Bergenstal highlight much to be learned
- 6. From prediabetes to basal insulin: Early CGM use to transform T2D care
- 7. Integrating wearable technology into adult diabetes care
- 8. *NEW* Data integration into EHRs and improving diabetes technology interoperability
-
Therapy Highlights
- 9. Dr. Viswanathan Mohan on the distinction between IFG and IGT in diabetes prevention
- 10. Adjust T1D study of GLP-1 RA use in adults with T1D and obesity shows significant reductions in cardiovascular outcomes and disease risk
- 11. Real-world evidence of reclassification to T1D following misdiagnosis
- 12. Dr. Satish Garg on the adjunctive use of incretins in T1D and obesity: Recommendations from an upcoming consensus report
- 13. Interim results for Diamyd’s phase 3 DIAGNODE-3 results for retogatein in stage 3 T1D expected by end of month
- 14. Clinical pearls on once-weekly insulin use in insulin-naïve and insulin-experienced people with T2D
- 15. T1D screening and monitoring: IDF Europe’s international consensus on for early-stage T1D now published
- 16. Lilly symposium: SURPASS‑EARLY trial underscores the potential to alter T2D progression with early tirzepatide treatment
- 17. Eight years of normoglycemia in preclinical T1D models of KRIYA-839; one administration designed to last a patient’s lifetime
- 18. Immediate, intensive glycemic management for T2D: An argument for early insulin initiation
- 19. *NEW* Updated results from Eledon Pharmaceutical’s tegoprubart (anti-CD40L antibody) as an immunosuppressant for people with T1D
-
Big Picture Highlights
- 19. IDF Europe symposium focuses on diabetes detection, treatments, and cures
- 20. Beyond glycemia: Addressing overweight and obesity in T1D
- 21. Early-onset T2D in pregnancy: Prof. Helen Murphy highlights rising prevalence and urgent need for stronger preconception care
- 22. *NEW* Dr. Nicole Glaser offers a sneak peek at ISPAD’s 2026 updates to Pediatric DKA Guidance
- 23. *NEW* Dr. Ananta Addala on discrimination as the ‘elephant in the room’ shaping diabetes technology uptake
- 23. *NEW* Risk of diabetic retinopathy during pregnancy: New registry data challenge historical concerns around progression risk
2026 Yearbook – 18 insightful presentations to a packed crowd!
An important part of the ATTD framework is the yearly publication of the ATTD Yearbook in DT&T. The authors of each section presented a short digest across 18 short presentations, in a tightly orchestrated session that was attended by a large audience in the largest hall at ATTD.
This year, among the highly curated insights, there were noteworthy contributions in pregnancy, liver health, inpatient CGM, and the steady rise of AI. New therapies and the future of technology were also addressed.
1. Continuous and intermittent glucose monitoring
- Dr. Jennifer Sherr (Yale University) opened the 2026 ATTD Yearbook session by highlighting three studies in the clinical literature on CGM spanning early disease prediction, beta cell function assessment, and inpatient diabetes management.
- First, Dr. Sherr highlighted a pooled analysis evaluating whether CGM metrics could predict progression to stage 3 T1D among individuals with islet autoantibodies (AAb) (Calhoun et al. 2025). The dataset included 218 participants with T1D and ≥1 positive AAb type across five studies: (i) ASK (n=79); (ii) BDR (n=22); (iii) DAISY (n=18); (iv) DIPP (n=8); and (v) the TrialNet Pathway to Prevention (n=91). Nearly 30% of participants developed stage 3 T1D, and by using a model with CGM-derived metrics combined with clinical factors they were able to accurately predict progression. The data suggest that CGM could play an important role in monitoring individuals identified through expanded screening programs and potentially enable home-based tracking of disease progression.
- Dr. Sherr also cited an analysis from the Closed-Loop/Verapamil (CLVer) study examining the association of CGM metrics with stimulated C-peptide measures in youth with recent-onset T1D (Neyman et al. 2025). Across 103 children followed for up to 52 weeks after diagnosis, CGM metrics were correlated with mixed-meal tolerance test-derived C-peptide measures, but the strength of this correlation was not sufficient to replace direct C-peptide testing obtained by conducting mixed meal tolerance test.
- Dr. Sherr concluded by highlighting the DIATEC trial evaluating CGM use in hospitalized individuals with T2D (Olsen et al. 2025). Non-intensive care unit patients (n=166) were randomized to either point-of-care (POC) glucose testing or CGM use. Participants using CGM achieved 15 percentage points higher TIR (+3 hours/day) compared to those monitored with standard POC testing. According to Dr. Sherr, these findings support the growing evidence base for CGM use in hospital settings. However, she said that the full benefits of inpatient CGM will likely depend on integrating sensor data with automated alerts and implementation of insulin titration algorithms, like what was leveraged in the DIATEC study, to guide clinical decision-making.
2. Insulin delivery hardware: Pumps and pens
- Dr. Rayhan Lal (Stanford University) continued his usual coverage of insulin delivery hardware in this year’s edition of the ATTD Yearbook.
- Smart insulin pens:
- Dr. Lal discussed an important use of smart insulin pens for reducing Time Below Range (TBR) in underserved populations (Gomez-Peralta et al. 2024).
- A post hoc analysis created two algorithms to detect glucose excursions, or spikes, from smart pens and correlate them to identify suboptimal bolusing (Wolpert et al. 2025).
- Insulin infusion:
- A systematic review demonstrated persistent gaps in the study of lipohypertrophy, a common complication of insulin infusion (Mader et al. 2025).
- An observational study also found that glycemic management deteriorated from Day 2 to Day 4 of infusion set use, as assessed by CGM metrics (Yoshimura et al. 2025).
- The authors included the pivotal trial for the Tandem seven-day extended wear infusion set, Steadiset, which was completed in 2025 (n=260), observing a mild increase in Time Above Range (TAR) between Day 4 and Day 7 (Lal et al. 2025). Dr. Lal again used his famous Achilles Heel metaphor to highlight the challenges of insulin infusion in diabetes.
- Technology safety and usability:
- During flight takeoff, insulin pumps over-deliver 0.6 units, and under-deliver 0.51 units during landing – Dr. Lal said that these figures may not impact adults yet may be critical for insulin-sensitive children (Garden et al. 2025).
- A study also found that rates of DKA in the DCCT/EDIC cohort have decreased over 34 years, attributed to insulin occlusion alerts, CGM, education, and experience (Budhram et al. 2025).
- Pump initiation and teaching time have become faster over time (Gordon et al. 2025), and deep learning algorithms provide promise for detecting pump faults (Idi et al. 2025).
- Insulin pumps for T1D:
- Dr. Lal called attention to persistent disparities in pump uptake even in areas with universal pump programs (Soliman et al. 2024).
- He noted that insulin sensitivity is acutely enhanced with motion, encouraging patients to frequently stand (Larsen et al. 2025).
- Finally, an analysis of 34,248 adults in the TriNetX database found that pump use was associated with decreased mortality, foot ulcers, DKA, and MI compared to MDI, but also with a higher risk of ischemic heart disease and retinopathy (Haughton et al. 2025).
3. New insulins, biosimilars, and insulin therapy
- Dr. Torben Biester (Auf der Bult Center, Germany) highlighted two studies of the 27 articles chosen across biosimilars, long-acting insulin, and new short-acting and new formulations. Dr. Biester discussed a secondary analysis (n=51) from two trials, comparing faster-acting insulin aspart (Fiasp) to insulin aspart and ultra-rapid insulin lispro (Lyumjev) to insulin lispro using the CamAPS FX hybrid closed-loop algorithm (Haliloglu et al., 2024). The study found that insulin lispro was superior with the use of the CamAPS FX closed-loop system, and faster-acting insulin aspart was not superior to insulin aspart. Dr. Biester added that it is refreshing to see a real comparison of two substances. He also highlighted a randomized controlled trial (n=123) of inhaled insulin plus degludec compared with usual care of MDI, CSII, or AID (Hirsch et al., 2024). The study included adults with an A1c of 5.4-10.5%, with T1D duration >6 months. Results showed that inhaled insulin was non-inferior to usual care, predominantly consisting of AID (48%) or MDI (44%). Specifically, 21% of inhaled insulin users achieved an A1c reduction of greater than 0.5% compared with 5% of the usual care group, and 26% of inhaled insulin users saw a greater than 0.5% increase in A1c compared with 3% in the usual care group. Dr. Biester added that inhaled insulin is superior to total usual care, most notably for non-AID users. Dr. Biester emphasized that insulin continues to be relevant in diabetes care, especially as novel formulations emerge.
4. Closed-loop, decision support, and AI
- Dr. Mark Clements (Glooko) reviewed recent data on AID, decision support systems, and AI. Beginning with closed-loop AID systems, his chapter identified 300 manuscripts published between July 1, 2024, and June 30, 2025. Dr. Clements identified several major themes, including long-term real-world observations and AID in T2D and very young children. More rare were studies on conceptually new technology, such as human-machine co-adaption and replay simulation, as well as early feasibility studies from fully closed-loop systems. Dr. Clements highlighted four studies in particular (Battelino et al. 2025; Elbarbary et al. 2024; Kovatchev et al. 2025; Kudva et al. 2025) and specifically called out the last of the four, a 13-week RCT comparing Control-IQ+ to CGM alone that demonstrated significantly greater improvements to A1c and TIR.
- On decision support, Dr. Clements pointed to what he believed was the first study on an AI-powered insulin titration system for people with T2D (Ying et al. 2025), which showed that the ML system was noninferior for TIR outcomes compared to physician led groups.
- Dr. Clements predicted that novel applications of AI and LLMs would be the fastest growing section of diabetes literature in the next five years. The chapter identified more than 1,500 publications on the topic, ranging from glucose, hospitalization, complications, and progression prediction to adaptive interventions. He highlighted one in particular (Metwally et al. 2025), which he said offers a “volume of data” on phenotypes for muscle and hepatic insulin resistance that can be used to inform the development of future therapies.
5. Using digital health technology to prevent and treat diabetes
- The esteemed Dr. Neal Kaufman (Canary Health) explored key progress, proof-of-concept, and critical areas of improvement in digital health interventions at ATTD 2026. Echoing his sentiment from ATTD 2025, Dr. Kaufman stressed the impact on patient behavior that personalized digital health interventions can have, but warned that certain limitations will continue to limit efficacy and access to such benefits until rectified.
- To underscore the value of digital health interventions, Dr. Kaufman first explored the DIAMANTE study (n=168) – a 24-week RCT with a control, random, and adaptive arm. Adaptive intervention, which included receiving a daily text selected by a reinforcement learning algorithm, conferred a substantial increase (19% increase in daily step count) in physical activity compared to control or random conditions (+4% and +2%, respectively). Dr. Kaufman concluded that the DIAMANTE study supports the use of reinforcement learning algorithms in personalizing digital health interventions to increase physical activities in diverse populations.
- Nevertheless, Dr. Kaufman stressed that further emphasis on personalized access is required. Specifically, he discussed: (i) precision recruitment and engagement; (ii) personalization as critical to increasing engagement and efficacy; (iii) considering the complexity of the lived experience of diabetes in program design; and (iv) availability in multiple languages.
- Dr. Kaufman also reviewed papers on the potential for family caregivers support during his time at the podium (Setyoadi et al. 2024; Kim et al. 2023; Amed et al. 2025).
- To underscore the value of digital health interventions, Dr. Kaufman first explored the DIAMANTE study (n=168) – a 24-week RCT with a control, random, and adaptive arm. Adaptive intervention, which included receiving a daily text selected by a reinforcement learning algorithm, conferred a substantial increase (19% increase in daily step count) in physical activity compared to control or random conditions (+4% and +2%, respectively). Dr. Kaufman concluded that the DIAMANTE study supports the use of reinforcement learning algorithms in personalizing digital health interventions to increase physical activities in diverse populations.
6. Technology and pregnancy
- Dr. Jennifer Yamamoto (University of Manitoba, Canada) reviewed the recent literature on diabetes technology use during pregnancy, highlighting two studies among eight selected papers.
- She began with a prospective cohort study comparing CGM profiles in pregnancies with and without GDM (Durnwald et al. 2024). Participants (n=768) used CGM prior to 17 weeks’ gestation and conventional GDM screening later in pregnancy. While GDM is typically diagnosed at ~24-28 weeks, this CGM data revealed clear differences in glucose profiles between those who did (n=58) and did not develop GDM. Retrospective examination of earlier CGM data showed that glycemic differences were already detectable as early as the second trimester, highlighting the potential role of CGM in earlier identification (and treatment) of dysglycemia during pregnancy.
- Dr. Yamamoto also discussed a large retrospective cohort study examining the safety of GLP-1 RA use during the preconception period (Imbroane et al. 2025). Given the rapidly increasing use of GLP-1 RAs among younger adults, many of whom are women of reproductive age, the study evaluated pregnancy outcomes among individuals exposed to GLP-1 RAs prior to conception. Results suggested that GLP-1 RA use during this period was not associated with increased risk, but rather was linked to lower rates of several adverse obstetric outcomes, including lower rates of GDM, preterm delivery, hypertensive disorders of pregnancy, and Cesarean delivery. Dr. Yamamoto cautioned that these findings should be interpreted carefully given the limitations inherent to retrospective database studies and called for more prospective studies to better define the safety and potential benefits of GLP-1 RA use in pre-pregnancy care.
7. Diabetes technology and therapy in the pediatric age group
- Dr. David Maahs (Stanford University) again brought his expertise in pediatric endocrinology to highlight a diverse set of publications. In an analysis of nine international registries and over 100,000 children with T1D, each registry demonstrated an increase in the use of CGM, insulin pumps, and AID in parallel to decreases in A1c and a reduction in severe hypoglycemic events (Zimmerman et al. 2025). In another study of over 4,000 children with T1D, beginning CGM use less than six months after diagnosis led to lower A1c levels three years post-diagnosis, underscoring the need to remove barriers to CGM (Mann et al. 2025). Turning to the early use of AID, in children aged 10-17 newly diagnosed with T1D had no changes to C-peptide levels over 48 months, but had 12% higher TIR and 0.9% lower A1c values (Ware et al. 2024). Even in children aged 1-7 years, a 0.4% improvement to A1c values and 8% to Time in Range (TIR) was shown over 18 months, highlighting the long-term safety and benefit of AID for youth (Ware et al. 2024). In a study of over 9,000 children in nine countries, DKA at diagnosis was associated with higher A1c values, neurocognitive damage, and higher BMI after two years. Early AID uptake mitigated some of this association (Dovc et al. 2025).
8. Advances in exercise and nutrition as therapy in diabetes
- Dr. Michael Riddell (York University, Canada) discussed the robust volume of research related to exercise and nutrition in diabetes, with 3,075 titles related to exercise and diabetes and 8,767 related to nutrition and diabetes published between July 1, 2024, and June 30, 2025. Of these, he highlighted 10 papers that he found to be particularly novel and impactful.
- On nutrition, Dr. Riddell explained that consumption of meat, especially processed and red meat, was correlated with elevated risk for developing T2D (Li et al. 2024). With a humorous jab at hotdogs, he showed research demonstrating that ultra-processed foods were correlated with elevated T2D risk (Vitale et al. 2024; Dicken et al. 2024), while whole foods and plant-based diets were shown to be correlated with a reduced need for diabetes-related medications (Hanick et al. 2024).
- Dr. Riddell also shared research on sweetened beverages that showed consuming over two servings of sugar- or artificially-sweetened drinks daily was correlated with a 41% and 11% greater risk of developing T2D, respectively (Pacheco et al. 2025). Consuming two per week without following proper exercise guidelines was also linked with elevated risk.
- Touching briefly on exercise, Dr. Riddell shared that resistance training improves body composition with GLP-1 RA use, yoga has been shown to be beneficial for youth with T1D, and mobile health biometrics enhances exercise adherence.
- Finally, joking that doctors like him may be replaced in the future, he discussed research that indicated that generative AI can be useful for providing accurate and helpful instructions regarding exercise for patients with T2D, though he warned that one must be careful before rashly accepting advice from AI (Chung and Chang, 2024).
9. Primary care and diabetes technologies and treatments
- Dr. Gregg Simonson (International Diabetes Center) presented about primary care, where much of T2D management occurs. This year, 12 studies – five on diabetes therapy, three on technology, and four on care models – were selected among 361 articles. In therapy, Dr. Simonson highlighted the SOUL trial (n=9,650), published in NEJM (McGuire et al., 2025), which investigated the use of oral semaglutide for MACE in T2D. The study found 3.1 events per 100 person-years in the oral semaglutide group compared with 3.7 in the placebo. Dr. Simonson highlighted that nonfatal MI had the largest risk difference between oral semaglutide and placebo. In technology, Dr. Simonson highlighted a retrospective cohort analysis (Garg et al., 2024) of CGM use in people with T2D on one of three treatment regimens: (i) non-insulin; (ii) basal insulin; and (iii) prandial insulin therapy. The results showed a significant reduction in hospitalizations and ER visits across all three treatment groups. In addition, a pre-specified subgroup analysis found that three-month A1c reductions were maintained throughout the post-index period. Dr. Simonson concluded that for primary care providers, this data shows that CGM use results in fewer hospital and ER visits, along with improved glucose management. On care models, Dr. Simonson highlighted the International Geriatric Diabetes Society’s Deprescribing Consensus Initiative (Munshi et al., 2025), examining the unique challenges older adults face, such as multimorbidity, cognitive or functional decline, and difficulty managing complex regimens. The publication proposes a structured 4S Pathway to guide clinicians in reassessing goals through shared decision‑making and implementing safer, more manageable treatment strategies.
10. Use of technologies at the advanced age
- Dr. Anna Kahkoska (University of North Carolina Chapel Hill) and her co-authors selected 13 articles (from over 300) to include in the chapter. She highlighted three articles covering CGM and AID use in older adults, as well as diabetes care in long-term care facilities.
- Research on CGM use found that the average CGM education time for older adults is longer and more variable compared to younger adults (Weinstock et al. 2024).
- In a 10-day blinded CGM study (n=65, mean A1c = 7.2%) in eight nursing homes in the US, over one in four residents had ≥1% time below 70 mg/dL and over half of residents spent >10% of time above 250 mg/dL, with the highest burden seen, interestingly, among insulin users (Munshi et al. 2025).
- In a 36-week, multicenter, randomized, crossover trial (n=82) of people with T1D ages 65 to 86 years old, a comparison of sensor-augmented pump (SAP) to hybrid closed loop (HCL) found that HCL more effectively decreases hypoglycemia and improves glycemia (Kudva et al. 2025). In the 12-week extension phase 91% of the participants chose to continue using HCL (Kudva et al. 2025).
11. The Real “Real World”: Overcoming practical barriers and disparities in diabetes technology
- Stanford’s Dr. Ananta Addala presented the real-world data section of this year’s ATTD yearbook section, with a focus on the barriers and disparities in diabetes technology use. Of the 387 articles identified, up significantly from the 2025 session, 14 were included in this year’s chapter. She categorized them into five themes: (i) early frontiers of AI in diabetes care; (ii) diabetes technology in higher-risk situations; (iii) continuous barriers to diabetes technology use; (iv) how we affect our diabetes technology; and (v) tracing inequities to transform diabetes care. Dr. Addala highlighted two studies she though best represented the third and fifth theme:
- The SKIN-PEDIC study (Berg et al. 2025) was a thorough global exploration of the skin problems children and adolescents face with devices. Across the diverse pediatric population with various skin conditions and devices used, eczema, skin infections, wounds, and scarring were common, and the study identified several associated factors, including longer pump and CGM wear and use of certain devices.
- Dr. Addala also highlighted an interventional RCT in the US (Agarwal et al. 2024) that aimed to support young adults with diabetes, all of whom had A1c ≥9% at baseline and concerning rates of DKA. With weekly clinics, flexible scheduling, screenings for social needs, and enhanced access to diabetes tech, participants saw improvements to A1c, incidence of hospitalization, and diabetes technology uptake.
12. Diabetes technology in the hospital
- Dr. Tim Hropot (University Medical Centre Ljubljana, Slovenia) discussed the continual challenges of diabetes technology in the hospital. The DIATEC study compared CGM with point-of-care (POC) glucose monitoring in 166 non-ICU patients with T2D. In-hospital CGM use increased TIR by 15% (77.6% vs. 62.7%, p<0.001), mainly by reducing TAR. CGM also lowered TBR, glycemic variability, prolonged hypoglycemic events, insulin usage, and in-hospital complications (Olsen et al. 2025). In the US, the TIGHT study studied 110 adults with T2D at six academic hospitals. Participants were randomized to either standard therapy with a glucose target of 140-180 mg/dL or intensive therapy with a glucose target 90-130 mg/dL guided by CGM. No difference was seen in mean glucose values and only 7% of the intensive group achieved the target range. Participants with lower baseline A1c values (<7.5%) achieved substantially higher TIR with CGM (77% vs. 62%) (Hirsch et al. 2025).
13. Impact of diabetes technologies on psychosocial outcomes
- Dr. Alon Liberman (Children’s Medical Center) shared insights from two studies that highlighted the impact that diabetes technology has on psychosocial outcomes, particularly in youth.
- The first study assessed the psychosocial implications of messaging from clinicians and CGM devices and apps. Dr. Liberman explained that youth often felt as if their TIR numbers were being judged or graded as if it were a school test (Tanenbaum et al. 2024). Due to the pressure and stress associated with this perception, youth and their families were more likely to create their own non-consensus target ranges to cope and regain their sense of control. Colors commonly used in CGM apps, such as green, yellow, and red also often negatively impacted patient-reported stress. These concerns worsened when considering TITR, with many viewing the metric as an additional pressure, though Dr. Liberman clarified that this sentiment was not universal and some felt motivated by the metric.
- In the second study, Dr. Liberman discussed executive function challenges in teens with T1D, especially around emotional regulation, and how A1c was impacted by the use of insulin pumps. In the study, while teens without executive functioning challenges demonstrated insignificant differences in A1c values with or without insulin pumps, teens with challenges saw a significant reduction from baseline A1c (Vitale et al. 2025). Dr. Liberman noted that there was little additional risk from the technology and concluded that diabetes technologies can improve equity by overcoming certain psychosocial barriers.
14. Immune intervention and beta cell replacement therapies in T1D
- Dr. Desmond Schatz (University of Florida) two selections of articles relevant to immune intervention and restorative therapies: (i) a study on Tzield (teplizumab) maintaining insulin secretion in “rapid progressors” in stage 2 T1D (Galderisi et al., 2025); and (ii) a study on Vertex’s zimislecel, a stem cell-derived islet therapy (Reichman et al., 2025).
- The first study analyzed the TN10 trial using oral minimal model (OMM)-derived indices to characterize the history of stage 2 T1D in placebo and Tzield-treated individuals. As background, OMM represents a differential equation-based model of meal-stimulated glucose and insulin dynamics. Results showed that individuals considered “rapid progressors” treated with Tzield transitioned from stage 2 to stage 3 T1D within two years, but still showed improved insulin secretion compared to those identified as “rapid progressors” treated with placebo. Curiously, rapid or slow progression to T1D did not correlate with changes in CD8 T cell exhaustion.
- The second study, previously presented at ADA 2025, demonstrated positive results in follow-up data from the FORWARD study (n=12). All participants achieved A1c <7.0% and Time in Range (TIR) >70%, and TIR continued to increase to 93% at one year. 10 of 12 participants eliminated insulin use, and insulin use was reduced in the two participants who did not achieve insulin independence. There were no severe hypoglycemic events for any of the participants.
15. Obesity and diabetes
- Dr. Viral Shah (Indiana University) highlighted five studies among 223 clinical trials published between July 2024 and June 2025. The review focused on three themes: (i) GLP-1 RA beyond diabetes and obesity; (ii) T2D prevention; and (iii) use in T1D.
- First, Dr. Shah highlighted an analysis of the SELECT trial (n=17,604), which found that while semaglutide did not reduce incident COVID-19, it lowered serious adverse event or mortality rates among those who were infected.
- The NutrIMM study (n=112) offers a potential mechanism for the anti-inflammatory effects of GLP-1 RAs: people with obesity have more inflammatory markers and reduced immune response, and weight loss through GLP-1 RA can improve immune function.
- Next, Dr. Shah spotlighted clinical trial analyses demonstrating that semaglutide and tirzepatide were effective in preventing T2D in people with prediabetes. He added that it is time to change the term “prediabetes” into “stage 2 T2D” to create regulatory pathways for T2D prevention.
- Lastly, Dr. Shah pointed to the ADJUST-T1D trial (n=115), in which GLP-1 RA significantly improved CGM metrics in people with T1D, compared to AID systems alone.
16. Emerging trends in MASLD and MASH
- To close out the ATTD Yearbook, Dr. Satish Garg (University of Colorado) offered insights on MASLD and MASH. Dr. Garg shared a striking statistic that individuals with lean MASLD have a 1.6-fold increase in mortality. The global prevalence of lean MASLD is estimated to be 5% in the general population and makes up 19% of all MASLD cases. The global prevalence of MASLD is estimated to be nearly 40%. After decades of limited therapeutic options, Dr. Garg spotlighted a new generation of FDA-approved treatments for MASLD and MASH: Rezdiffra’s resmetirom (MAESTRO-NASH study) and Novo Nordisk’s semaglutide (ESSENCE study). Moreover, three separate therapies remain under investigation for both diseases, including: (i) FGF-21 (Noureddin et al. 2025); (ii) dual/triple agonists (Loomba et al. 2024); and (iii) survodutide for MASH and MASLD (Sanyal et al. 2024).
17. Virtual clinics for diabetes care
- As with last year’s ATTD Yearbook Dr. Satish Garg (University of Colorado) shared the latest DT&T metrics. Now in its 27th year, DT&T’s global readership covers 170 countries. Manuscript submission have increased by 20% in 2025 (compared to 8% in 2024). The publication remains highly selective with an ~82% rejection rate (~85% in 2024). In 2025, there were >575,000 full-text downloads (+15%), including 22,000+ downloads for ATTD and ATTD-Asia abstracts and 18,500+ for the ATTD Yearbook.
- On virtual clinics for diabetes care, Dr. Garg kept things short and sweet with a single slide highlighting four key articles, which showed improved patient-reported outcomes with CGM-aided virtual diabetes care (Hood et al. 2025), lowered A1c following a pharmacist-led hybrid care diabetes clinic (Smith et al. 2025), improved patient satisfaction and glycemia with a hybrid gestational diabetes care model (Axelrod et al. 2025), and feasibility of remote CGM use training in older adults (also referenced in the “Use of Technologies at the Advanced Age” chapter of this year’s Yearbook) (Weinstock et al. 2024).
18. New medications for the treatment of diabetes
- Dr. Satish Garg (University of Colorado) highlighted multiple studies of new medications for the treatment of diabetes.
- The first study (Linong et al., 2025) involved the phase 3 GLORY-1 trial of once-weekly mazdutide in Chinese adults with obesity or overweight. At baseline, the mean body weight was 87.2 kg (181 lbs) and the mean BMI was 31.1 kg/m². At Week 32, the mean percentage change in body weight from baseline decreased by 10%, 13%, and 0.45% in the mazdutide 4 mg, 6 mg, and placebo groups, respectively. Furthermore, at Week 48, the mean percentage change in body weight was 11%, 14%, and 0.3% in the mazdutide 4 mg, 6 mg, and placebo groups, respectively.
- Dr. Garg also highlighted another study (McGuire et al., 2025) of the phase 3 SOUL trial, which assessed oral semaglutide in people with T2D and high CV risk. Primary outcome events (MACE) occurred in 12% of the oral semaglutide group, compared with 14% in the placebo group (hazard ratio, 0.86), indicating that oral semaglutide was associated with a significantly lower risk of major adverse CV events than placebo.
- Finally, Dr. Garg presented his study (Garg et al., 2025) on cardiovascular and renal biomarkers in people with T1D and overweight or obesity, who had been treated with tirzepatide. The retrospective study found that long-term use of tirzepatide in the population led to more than 23% weight loss and sustained improvement in glucose management. Additionally, irrespective of changes in weight or A1c levels, the study showed significant improvements in cardiovascular biomarkers and preservation of kidney function. Dr. Garg said these findings are quite notable, as GLP-1 RAs are not yet approved for people with T1D, yet studies have shown an increasing trend in the prescribing of incretin treatments for this population. A long term randomized controlled trial would be valuable.
Technology Highlights
1. Debate: Should A1c or CGM be the gold standard for glycemic management?
Dr. Richard Bergenstal (International Diabetes Center) and Dr. Elizabeth Selvin (Johns Hopkins University) hosted a lively debate seeking a gold standard for glycemic management. Dr. Selvin strongly advocated for A1c to remain the gold standard, while Dr. Bergenstal said that the time has come for CGM metrics to replace A1c.
- Pro: A1c should remain the standard of care for evaluating glucose control, said Dr. Selvin. First, Dr. Selvin discussed availability, which is necessary to establish a metric as a truly global standard of care. Unlike CGM, A1c is low cost, requires basic lab infrastructure, and is widely available around the globe and covered by insurance. She also highlighted A1c’s alignment with the likelihood of developing long-term complications, as demonstrated by the landmark DCCT. Glycation in the blood leads to complications, said Dr. Selvin, and A1c directly reflects this, unlike CGM metrics. While work is ongoing to evaluate CGM metrics for predicting long-term outcomes, there have been limited long-term outcome studies completed to date. Metrics also vary between devices, while A1c has been highly standardized around the world by the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC). Dr. Selvin recognized the value of CGM for preventing hypoglycemia and providing a window into daily glucose fluctuations but believes that CGM must complement the use of A1c and is not a total replacement. She advocates for the use of A1c as a long-term control and risk metric and for CGM as a short-term management tool.
- Con: Dr. Bergenstal said that the time has come to cross the bridge from A1c to CGM metrics. Dr. Bergenstal said that glycemic control remains inadequate in most countries despite the ubiquity of A1c testing and its establishment in the standards of care for diabetes treatment. In the US, from 1999-2018, only 60% of people with T2D have an A1c value <8.0% if on insulin, and only 30% have an A1c less than 7.0%. He said that the field is clearly searching for better management strategies, and proposed CGM to fill this gap. He noted that the 2026 ADA Standards of Care first suggest the use of A1c for glycemic management and only suggest the use of CGM and diabetes education after three to four steps if management is inadequate. He instead believes that CGM should come before A1c because of the wealth of daily data it provides. He cited three patients from his own practice, all with A1c values of 6.7%, and showed how different their CGM data were, with 83%, 69%, and 51% Time in Range (TIR). This demonstrates how A1c values cannot capture all the nuance of diabetes care that can impact long-term complications. He then acknowledged challenges with the Glucose Management Indicator (GMI) metric, which is meant to estimate A1c values from CGM data yet has highly variable results in practice. He recently led a study to update GMI to more closely reflect A1c values, which will be published shortly and may address some of the major concerns with CGM alone. Dr. Bergenstal said that only CGM metrics can effectively guide glycemic, metabolic & quality of life improvements through personalized care.
- Rebuttal: Limitations remain unaddressed for CGM, said Dr. Selvin. She said that RCTs continue to use A1c as the standardized outcome because it is more robust than CGM metrics. At the population level, she said, problems in glycemic management should not be attributed to A1c, but rather to other systemic failures. She said that gold standards should only be replaced with a superior metric.
- Rebuttal: Dr. Bergenstal said that CGM enables a new goal for long term diabetes management: a safe life with reduced overall risk, not just survival. The audience applauded loudly for both Dr. Selvin and Dr. Bergenstal, with a slight preference for the CGM perspective.
2. mylife Diabetes Care: Evidence and clinical pearls for personalization AID with CamAPS FX
In a mylife Diabetes Care (formerly Ypsomed Diabetes Care)-sponsored session, Prof. Roman Hovorka (University of Cambridge, UK), Dr. Marco Marigliano (University of Verona, Italy), and Dr. Carmen Quirós (University Hospital Mutua de Terrassa, Spain) explained how the CamAPS FX AID system can be personalized using personal glucose targets (PGT) to improve outcomes across different age groups. They emphasized that personalizing glucose targets allows clinicians to balance glycemic outcomes with hypoglycemia risk depending on patient characteristics and daily circumstances.
- Prof. Hovorka described how adjustable PGT allows CamAPS FX to personalize glycemic outcomes and balance safety considerations across age groups. He showed that the system demonstrates a primarily linear relationship between the glucose target selected and the resulting mean glucose outcomes. Lower targets generally produce lower average glucose and higher Time in Range (TIR), whereas higher targets lead to more protection from hypoglycemia. However, outcomes with CamAPS FX use vary across population. Older adults tend to achieve the highest TIR and very young children often achieve lower TIR due to greater glycemic variability and a greater emphasis on hypoglycemia prevention within the algorithm. Prof. Hovorka also highlighted the importance of overnight management, noting that nighttime glucose tends to be more stable and therefore represents an opportunity to tighten glycemic targets rather than relax them.
- In pregnancy, the AIDAPT trial used CamAPS FX to successfully set lower targets, such as ~99 mg/dL during the first trimester of pregnancy and even lower targets later, demonstrating the system’s ability to safely support tighter glycemic management.
- When managing hypoglycemia risk, Prof. Hovorka recommended adjusting system parameters, such as the insulin-to-carbohydrate ratios, before immediately increasing glucose targets, since temporary hypoglycemia risk may reflect short-term physiological changes rather than inappropriate algorithm settings.
- Dr. Marigliano presented real-world evidence demonstrating how PGT can help personalize AID therapy in very young children, a population with unique glucose management challenges. He said that several studies have demonstrated meaningful glycemic improvements with AID use in children under six years old, with TIR typically reaching ~64-67% after improvements of ~11 percentage points, which is sustained over long-term follow-up. He referenced a multicenter real-world analysis of preschool-aged children using CamAPS FX presented at ISPAD 2025, which demonstrated significant glycemic improvements. However, he emphasized that managing diabetes in young children is still difficult due to: (i) insulin needs changing rapidly; (ii) meals being irregular due to snacking or food refusal; and (iii) spontaneous activity levels.
- Despite these improvements, the youngest cohort still experiences lower TIR than older age groups, reflecting their greater physiologic variability and the algorithm’s prioritization of hypoglycemia prevention. Dr. Marigliano said that careful personalization, specifically through PGT adjustments, can help address this challenge. For instance, clinicians may set slightly higher glucose targets during late morning hours when hypoglycemia risk is elevated and tighten targets overnight, as demonstrated by a real-world analysis from 2025. In addition to target selection, he stressed the importance of practical management strategies. One such strategy was optimizing bolus timing, which should be ideally 5-15 minutes before meals. He also suggested avoiding overly aggressive or overly weak carbohydrate ratios. Data from his center in Verona showed encouraging outcomes among very young children using CamAPS FX (n=40), with mean A1c levels decreasing from ~7.5% to ~6.9% over one year and TIR improving by ~15 percentage points, demonstrating that careful personalization and family education can substantially improve outcomes even in this challenging age group.
- To close the symposium, Dr. Quirós discussed how similar strategies apply in adulthood, where adjusting PGT can help clinicians optimize glycemic outcomes while maintaining safety. She reviewed a study demonstrating the clinical impact of using PGT and how target selection differed across age groups and individuals. Her key clinical takeaway was that tighter glycose targets are not necessarily beneficial for every person, and targets should always be individualized based on each person’s circumstances and preferences. Optimal targets depend on factors such as hypoglycemia risk, daily routines, and patient preferences. Dr. Quirós said that clinicians should adjust targets incrementally and work closely with individuals to build confidence in the system and ultimately optimize outcomes.
3. CGM metrics as predictors of vascular risk: Insights from Virtual DCCT and real‑world evidence
In this session, Dr. William Horton (University of Virginia) presented findings from a study that explored whether CGM metrics can serve as reliable predictors of cardiovascular (CV) outcomes in people with T1D, using an impressive reconstruction of CGM data from the DCCT (n=1,441). Because the DCCT predated modern CGM, his team used machine learning to populate individualized virtual CGM traces for all the participants in both the intensive and control groups, based on the A1c and seven point blood glucose data from the original trial. From this point, the team calculated ‘CGM metrics’ such as Time in Range (TIR), Time in Tight Range (TITR), mean glucose, and hyperglycemia exposure. These metrics were then compared against CV outcomes defined in two ways: the original broad composite definition that included a wide range of CV events, and a modern stricter definition limited to the most clinically severe outcomes.
- Dr. Horton showed that it was possible to replicate the original adjusted hazard ratios for CV events for A1c, with virtual CMG metrics - TIR, TITR, mean glucose, and hyperglycemia exposure. It turns out that individuals in the DCCT who did not experience CV events had slightly lower mean A1c (8.2% vs. 8.4%) and therefore spent more TIR (50% vs. 47%), while those with events had modest but consistent reductions in both TIR and TITR and higher mean glucose (190 mg/dL vs. 197 mg/dL). The original DCCT adjusted hazard ratio for the CV outcome measure was 1.29 for a 1.44% increase in A1c. This was almost identical for a TIR reduction of 18%, and a TITR reduction of 15%. These results reinforce the concept that CGM data should serve as clinically meaningful endpoints for long‑term outcomes, especially as clinicians seek metrics that better reflect day‑to‑day glycemic patterns.
- On limitations, Dr. Horton emphasized that while the DCCT provides a rich dataset, it is not the ideal population for evaluating hypoglycemia‑related CV risk, given its younger age and lower baseline CV burden. Dr. Horton highlighted the need for prospective studies in older, higher‑risk populations and pointed to the large‑scale FACULTY study (n=70,000) in France as a major step toward answering these questions using real‑world CGM data. The study is underway, and links real-world CGM data with national health claims records to examine how CGM metrics relate to future macrovascular and microvascular complications.
- In a related session, Prof. Chiara Fabris (also from the University of Virginia) presented multiple real‑world and longitudinal datasets showing that lower TIR and TITR track with higher microvascular risk. In one study of adults with T1D (n=808), individuals with microvascular complications had statistically significantly lower TIR (50% vs. 54%) and TITR (32% vs. 36%), and the odds of retinopathy rose steadily across lower TIR/TITR quartiles. Her key takeaway was that CGM‑derived metrics, especially TIR and TITR, are consistently linked to both the prevalence and incidence of microvascular complications, particularly retinopathy, and therefore should be used to assess glycemic management, track disease progression, and guide therapy adjustments alongside or even beyond A1c.
- Dr. Horton closed by discussing the U‑shaped relationship between glycemia and CV mortality, noting that both chronic hyperglycemia and frequent hypoglycemia appear to elevate risk. He did not expect that the U-shaped relationship would hold with TIR, and asserted that it would be important to determine the ideal TIR target for CV health to add to our guidelines. Initial work in China suggests that truly CV-protective TIR thresholds may be in the range of 85% which, if true, raises the question of how we will be able to hit those targets..
4. Dr. Ahmad Haider takes a first pass at recommendations for continuous ketone level targets for people with T1D on SGLT-2 inhibitors
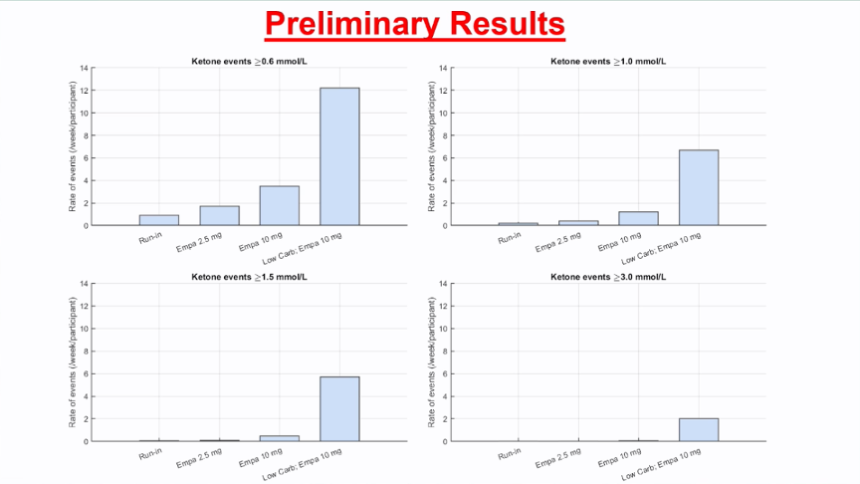
During a quiet afternoon session, Dr. Ahmad Haider (McGill University, Canada) presented fascinating data using continuous ketone monitoring data in people with T1D on empagliflozin. Using the data, Dr. Haider defined some targets for ketone levels for this particular population, though he made clear that these targets were not “really scientific,” but just drawn up empirically from their small dataset.
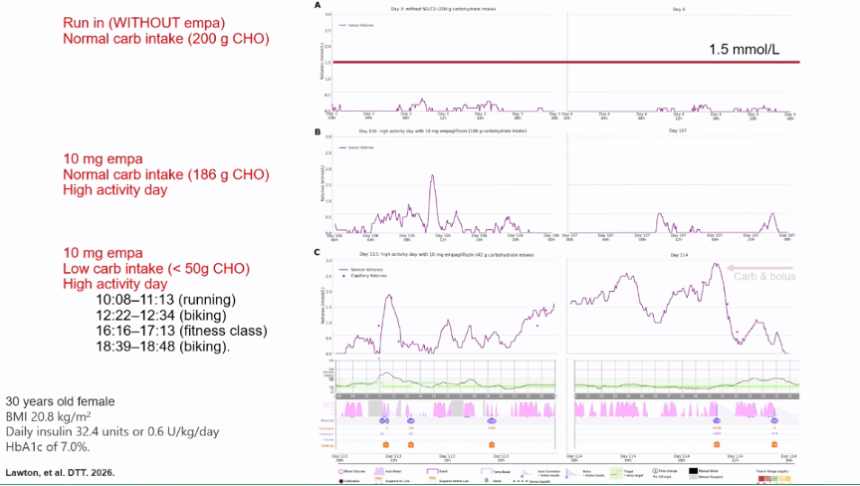
- In the study, 24 adults were given continuous ketone monitors (from Sibionics) and empagliflozin. Participants started with four weeks of run-in with no empagliflozin, four weeks with 2.5 mg empagliflozin, eight weeks at 10 mg, and finally – to really push the limits – one week with 10 mg of empagliflozin and a low carbohydrate diet (<50 g carbs per day). The ketone traces with increased empagliflozin doses show an obvious trend with increased ketone levels as empagliflozin dose increased. However, increased ketone levels are not necessarily bad if they do not lead to DKA, and, as Dr. Haider noted, they may even be cardioprotective.
- In one participant, the highest empagliflozin dose and low carbohydrate diet, combined with high activity, led to extremely high ketone levels and a protocol deviation. Ketone levels rose extremely high, as seen in the first chart below, the participant became symptomatic, and they had to eat some carbohydrates and dose insulin to bring ketone levels back down. However, for another participant, ketone levels rose to similar levels and even higher with the 10 mg empagliflozin and low carbohydrate diet. Despite this, the participant never became symptomatic and continued the study, highlighting heterogeneity across individuals.
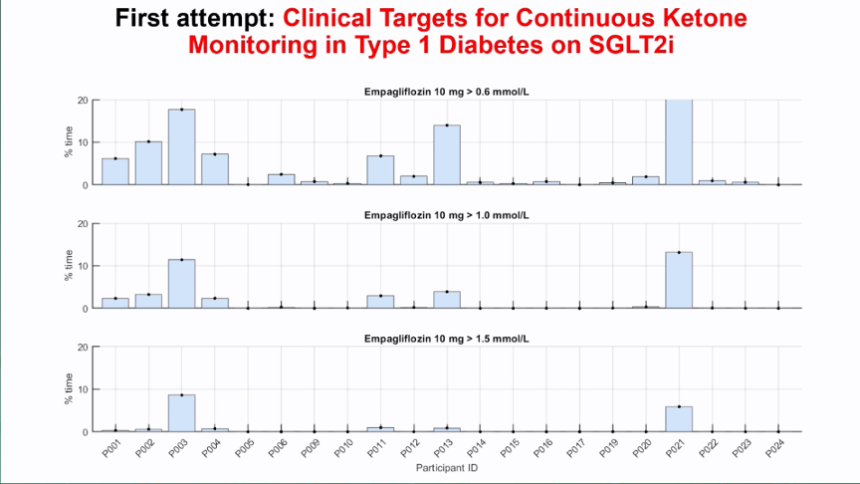
- Despite the varying individual responses to ketone levels, Dr. Haider proposed the first attempt at targets: <3% for level 1 ketosis (>1 mM) and <1% for level 2 ketosis (>1.5 mM). These targets were drawn up entirely empirically based on the 24 participants in the study but serve as a conversation starter as continuous ketone monitors become more available.
5. A preview of continuous ketone monitoring data from Abbott; Drs. Ketan Dhatariya and Rich Bergenstal highlight much to be learned
In the cavernous auditorium in Barcelona’s CCIB, Drs. Ketan Dhatariya (Norfolk and Norwich University Hospitals, UK) and Rich Bergenstal (International Diabetes Center) emphasized that there is still much to learn about continuous ketone monitoring data during an Abbott-sponsored symposium. Dr. Dhatariya kicked things off by reviewing what is currently known about ketone levels in the body. In particular, Dr. Dhatariya emphasized that high ketone levels themselves are not necessarily a bad thing, saying, “We’re all designed to starve.” In fact, Dr. Dhatariya showed results from a study in which humans fasted and beta-hydroxybutyrate levels were sustained at 6 mM for nearly a month. However, because these ketone levels rose gradually, the body was naturally able to compensate. Instead, Dr. Dhatariya noted, the change and rate of change in ketone levels may be more relevant when it comes to managing and preventing ketoacidosis.
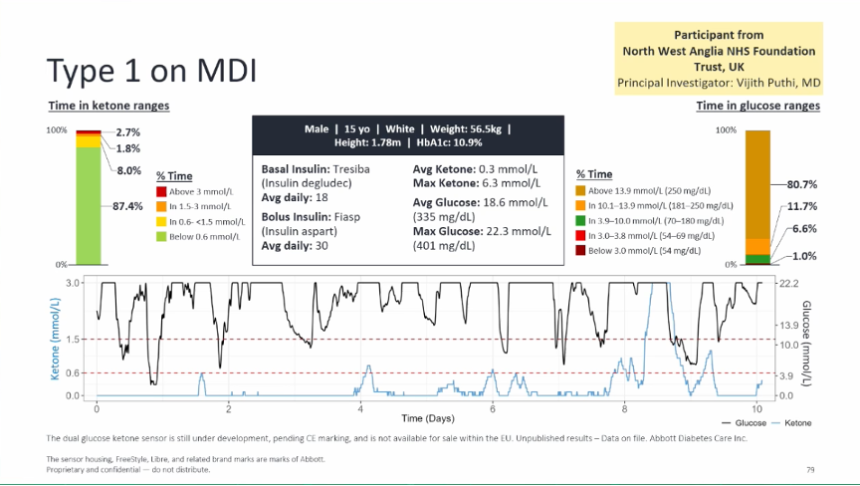
Following on, Dr. Bergenstal presented our first look at real-world data from 1,400+ participants wearing blinded dual glucose ketone sensors. While aggregate study data is still being analyzed, Dr. Bergenstal provided a few example sensor traces, highlighting the richness of the data from the sensors, as well as how much was still not understood on the relationship between glucose and ketone levels.
- In the first case, Dr. Bergenstal showed a person with T1D with consistently high glucose levels. This individual spent nearly all of their time above range, and in fact spent much of their time with glucose at the highest levels measurable by the sensor (i.e., >400 mg/dL). However, their ketone levels generally stayed low throughout wear with the exception of one major ketone spike on Day 6. For this, Dr. Bergenstal noted that it’s difficult to know what the cause of that ketone spike was, whether it was due to illness, missing an insulin dose, or something else.
- In another case, Dr. Bergenstal showed sensor traces for a person with T1D on an insulin pump. In this case, glucose was also consistently high, but ketone spikes also occurred with regularity. With a blinded sensor, it’s difficult to know what was causing these ketone spikes, but the two examples show heterogeneity in how glucose and ketone levels are associated with each other.
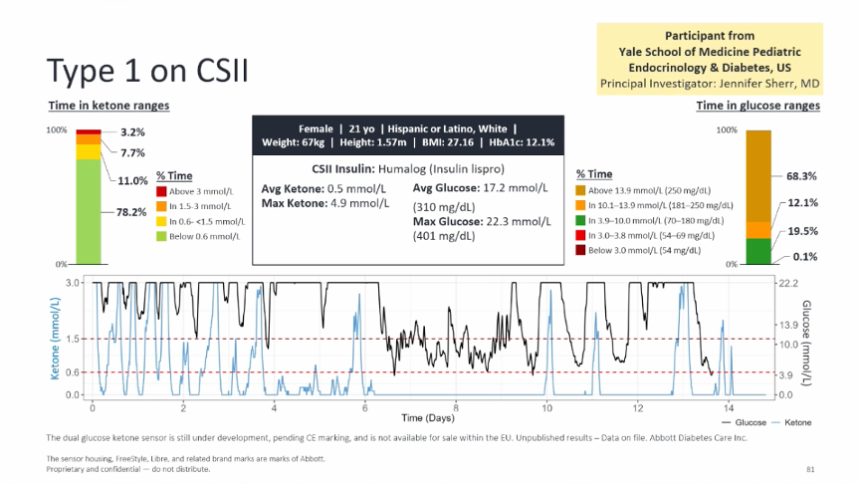
- Dr. Bergenstal highlighted the diversity in the dataset that was collected with the blinded glucose ketone sensor. The study enrolled over 1,400 participants across the US, UK, Austria, Germany, and Australia, and included people with T1D and T2D. It included people using MDI, pumps, hybrid closed loop, basal insulin only, or SGLT-2s. Additionally, pregnant participants and participants with CKD and CVD were included in the dataset. In all, the data will be collected to analyze typical ranges for ketone levels across various diabetes types and comorbidities which will become especially important as continuous ketone sensors become available.
6. From prediabetes to basal insulin: Early CGM use to transform T2D care
In a busy morning Dexcom symposium, Dr. Viral Shah (Indiana University), Dr. Thomas Martens (International Diabetes Center), and Dr. Sean Oser (University of Colorado Anschutz) stressed the value of early initiation of CGM to optimize therapy and encourage early behavior change. Together, they described how CGM can guide interventions in prediabetes (or stage 2 T2D) to supporting patients initiating basal insulin.
- Dr. Shah opened by proposing a staging framework for T2D similar to that used for T1D. He argued that the term “prediabetes” should be eliminated because it minimizes the condition’s links to serious complications by framing it merely as a risk factor for T2D. Instead, individuals with dysglycemia (but without overt diabetes) should be classified as having stage 2 T2D. Just as CGM can help patients reach therapeutic targets regardless of insulin use among people with T2D, CGM can help prompt and inform behavior change to begin improving glycemia. Dr. Shah also called for updated guidance that emphasizes CGM-based glycemic optimization, as well as greater collaboration with industry and regulators to expand access to therapies such as modern incretins to help prevent progression from stage 2 to stage 3 T2D.
- Dr. Martens highlighted data from the Dexcom Global Registry, which includes CGM-naïve adults with T2D managed in primary care. Participants in this analysis (n=318) represented a diverse population with varied education and insurance status and were typically taking one to three medications; about one-third used GLP-1 RAs and one-third used SGLT-2 inhibitors at enrollment. Real-world CGM adherence was high, with 75% wearing CGM on at least 70% of days – similar to adherence seen in the MOBILE trial. CGM use led to a rapid A1c reduction of 0.5 percentage points from a baseline of 7.4%, reaching a ~0.7 percentage point reduction at one year. Benefits were consistent across age groups, and participants already using GLP-1 RAs experienced greater improvements, suggesting complementary effects between the therapies. At one year, participants also reported an average 2.4 kg (~5 lbs) weight loss, lower diabetes distress, and improvements in eating and exercise habits. Dr. Martens concluded that CGM can meaningfully improve glycemic management in real-world primary care settings, with benefits sustained over a year.
- Finally, Dr. Oser discussed Dexcom’s CGM-powered Smart Basal feature, designed to address clinical inertia in basal insulin titration. He noted that nearly three-in-four new basal insulin users fail to reach glycemic targets within one year of initiation. Smart Basal, available in the US with Dexcom G7 15 Day and insulin glargine U-100, uses an algorithm to calculate a patient’s recommended basal dose each day within provider-defined limits (for example, maximum daily dose increases). The system aims to identify the optimal dose within 90 days, though Dr. Oser noted that in practice it can often occur in about a third of that time. Patients receive the recommended daily dose in their app and are prompted to log administration. Dr. Oser said faster titration to optimal basal dose can significantly improve TIR, reduce Time above Range, and lower GMI.
7. Integrating wearable technology into adult diabetes care
Dr. Jane Jeffrie Seley (Weill Cornell Medicine) gave an insightful presentation on best practices to better integrate wearable technology into adult diabetes care. With a special focus on AID systems, she introduced the ICC framework, which helps guide patients and providers toward the right technology, configure the device to make it more tailored to the user, and facilitation patient-provider collaboration through a data-driven lens to improve access and promote equitable care. As the insulin delivery ecosystem continues to rapidly move towards insulin pumps and away from MDI, Dr. Jeffrie Seley proceeded to explain the optimal process a provider should take when selecting a wearable technology. Specifically, decisions should consider the patient’s lifestyle, history, and historic and current glycemic outcomes, taking into account specific pump features, CGM types and compatibility, level of desired engagement with the device, and more. Dr. Jeffrie Seley concluded that providers should strive to become an expert on all AID systems available in their region and educate other players in the diabetes care ecosystem to learn more as well – this is the only way to appropriately prescribe the right devices to patients.
8. *NEW* Data integration into EHRs and improving diabetes technology interoperability
Dr. Peter Adolfsson (University of Gothenburg, Sweden) shared his perspective on how data is being integrated into EHRs in this popular morning session. First explaining the type of data being integrated into EHRs, which include clinical data, patient-generated data, genomic data, and demographic data including social determinants of health, he laid out the current methods and standards for integration. These include facilitating messages between healthcare systems, using application program interfaces (APIs) as bridges, following DICOM (the international standard for medical images), and adhering to the clinical document architecture (a standard defining the structure and semantics of clinical documents). Diving deeper, Dr. Adolfsson discussed the Integration of Continuous Glucose Monitoring Data into the Electronic Health Record (iCoDE), an initiative of the Diabetes Technology Society aimed at creating standards for importing CGM data directly to EHR systems. Specifically, these standards call for high levels of interoperability and cooperation between the government, diabetes technology companies, and hospital systems. The challenges of such a project include ensuring that the data uploaded is high quality, accessible, and HIPAA compliant. Notably, Dr. Adolfsson said that these implementation goals starts with the US, which has more established EHRs and data systems, claiming that Europe is “at least two years behind.”
Therapy Highlights
9. Dr. Viswanathan Mohan on the distinction between IFG and IGT in diabetes prevention
In this morning session, Dr. Viswanathan Mohan (Dr. Mohan’s Diabetes Specialities Centre) discussed the critical topic of prevention of T2D through lifestyle changes. He explored the differences between three different metabolic subtypes of prediabetes: (i) people with isolated impaired fasting glucose (IFG); (ii) those with isolated impaired glucose tolerance (IGT); and (iii) those with both IFG and IGT. In South Asian populations, a relatively modest weight loss can prevent progression to diabetes in many people. He advocated that prediabetes remission should be an important goal of health systems.
- Dr. Mohan explained that isolated IFG (plasma glucose of >100 mg/dl and <126 mg/dL) is driven primarily by hepatic insulin resistance, whereas IGT (>140 and <200 mg/dL, two hours after a 75g OGTT) reflects insulin resistance in muscle. While many regions report higher rates of IGT, one study found that Southeast Asia stands out with the opposite pattern, with IFG being far more common than IGT (10% vs. 3%). This phenotype, Dr. Mohan noted, has implications for prevention strategies.
- Dr. Mohan addressed the question of whether diabetes can be prevented in people with prediabetes, leaning on IFG and IGT subtypes to answer the question. Drawing on landmark trials from the US, Finland, China, and India, he highlighted that lifestyle interventions, such as the National Diabetes Prevention Program (DPP) consistently reduce diabetes incidence, up to 58% in Western cohorts, but somewhat lower in China and India, likely due to lower baseline obesity. But the real nuance emerged when he dissected outcomes by prediabetes subtype. The D‑CLIP trial showed that individuals with isolated IGT or combined IFG + IGT responded well to lifestyle change, with nearly half avoiding progression to diabetes. In contrast, those with isolated IFG showed minimal benefit, with only about 3% achieving prevention. A recent meta‑analysis reinforced this pattern, confirming that isolated IFG is far more resistant to conventional lifestyle interventions.
- Dr. Mohan also addressed the possibility of prediabetes remission. While remission of T2D is now widely discussed, Dr. Mohan noted that remission of prediabetes has received far less attention. Presenting new analyses from the D‑CLIP study, including a paper submitted earlier this year, he showed that regression to normoglycemia is not only possible but predictable, with clear patterns across phenotypes. Those who achieved remission tended to be younger, had lower baseline A1c, were less insulin resistant, and had better preserved beta‑cell function. In addition, isolated IFG or isolated IGT were more common among regressors, whereas combined IFG + IGT dominated among non‑regressors. Notably, even modest weight loss (just 2.5 to 5 kg, on average) significantly increased the likelihood of remission in South Asians - a population that requires far smaller weight reduction than white Europeans to achieve a metabolic benefit. Dr. Mohan emphasized that glycemic remission should be a goal of prevention in people with prediabetes and those at high risk for T2D.
10. Adjust T1D study of GLP-1 RA use in adults with T1D and obesity shows significant reductions in cardiovascular outcomes and disease risk
Dr. Viral Shah (Indiana University) and Dr. Janet Snell-Bergeon (University of Colorado Anschutz) presented glycemic and cardiovascular results from the ADJUST T1D RCT, which evaluated the safety and efficacy of semaglutide in adults with T1D and obesity. Glycemic outcomes were previously published in Diabetes Care in June 2025. Because cardiovascular risk remains elevated in this population — approximately three to four times higher than in people without diabetes — the study also assessed semaglutide’s impact on cardiovascular risk factors, recognizing that improved glycemic management alone may not sufficiently reduce cardiovascular risk.
- Dr. Snell-Bergeon presented cardiovascular secondary outcomes. Using the trial data, investigators estimated participants’ five- and 10-year cardiovascular disease (CVD) event risk. The semaglutide group experienced an approximately 20% reduction in both five- and 10-year predicted CVD risk, with risk declining steadily over the 26-week study period. In contrast, the placebo group showed no meaningful change from baseline to Week 26.
- The study found significant improvements in several lipid measures. Total cholesterol declined by about 23 mg/dL compared with placebo, and LDL cholesterol showed a between-group difference of 18.4 mg/dL. HDL cholesterol initially decreased in the semaglutide group by eight weeks, though this effect resolved and was no longer significant by Week 26. Triglyceride levels declined in both groups, with no significant between-group difference at the end of the study.
- Semaglutide treatment was associated with a significant reduction in systolic blood pressure of 6.2 mmHg, while no change was observed in the placebo group. A significant between-group difference in diastolic blood pressure emerged only at Week 26, with the semaglutide group showing a modest 2 mmHg decrease from a baseline of 124 mmHg. Dr. Snell-Bergeon suggested that a longer study duration might reveal a larger difference. The trial also identified improvements in central blood pressure and arterial stiffness at Week 26, including significant reductions in central systolic blood pressure, mean arterial pressure, and pulse pressure with semaglutide compared with placebo. Central diastolic blood pressure did not change significantly. In addition, brachial artery distensibility, a measure of vascular stiffness, improved significantly with semaglutide treatment.
- Although participants began the trial with generally good kidney health, the investigators observed a significant between-group difference in urinary albumin-to-creatinine ratio (UACR): levels declined slightly with semaglutide and increased slightly in the placebo group. Estimated glomerular filtration rate (eGFR) remained stable in both cohorts from a baseline of approximately 100 mL/min/1.73 m2.
- Dr. Shah also reviewed the ADJUST T1D study’s glycemic outcomes. More than one-third of participants receiving semaglutide met all three key endpoints: (i) TIR >70%; (ii) Time below Range <4%; and (iii) weight loss >5%. No participants in the placebo group met all three criteria. A1c decreased from 7.8% at baseline to 7.1% at 26 weeks in the semaglutide group, corresponding to an adjusted between-group difference of 0.3%. CGM metrics also improved. TIR increased from 56% to 67%, with most of the improvement reflecting greater TITR. Participants receiving semaglutide lost approximately 9 kg from a baseline weight of about 100 kg, equivalent to roughly 9% weight loss. Importantly, weight loss had not plateaued by 26 weeks, suggesting that a longer trial could produce further reductions, even though A1c levels had stabilized by that point.
- Dr. Shah also noted that most reductions in insulin use occurred in postprandial dosing rather than basal insulin. However, he emphasized that many participants were using AID systems, which selectively modulate basal insulin. While the precise contribution of weight loss to insulin reduction remains uncertain, Dr. Shah said the data suggest that semaglutide’s glycemic benefits are not entirely dependent on weight reduction. Regarding safety, no cases of DKA were reported. Rates of severe hypoglycemia were similar between groups, while gastrointestinal adverse events occurred approximately twice as often in the semaglutide group.
11. Real-world evidence of reclassification to T1D following misdiagnosis
In a morning oral session, Dr. Jeremy Pettus (UCSD) presented results from the RECLASS-T1D study (n=6,759,145), which estimated the proportion of individuals diagnosed with prediabetes or T2D who were later reclassified as having T1D. Other objectives of the study included time to reclassification and healthcare utilization following reclassification. The study used EHR data from TrialNetX and included participants with prediabetes or T2D diagnosis from July 2016 to October 2024. Overall, 2.2% of individuals diagnosed with prediabetes or T2D were ultimately reclassified to T1D. People who were later reclassified with T1D were more likely to be younger and had higher A1c. Interestingly, BMI was not a distinguishing factor for reclassification.
- The overlap between T1D and T2D. Dr. Pettus explained that T1D and T2D share multiple overlapping characteristics, leading to misclassification among patients. The risk of misdiagnosis increases with age, with rates of 14% in ages 13-17 and 55% in ages ≥50. People with adult-onset T1D are especially at risk of misclassification, leading to clinical and emotional challenges.
- Current criteria used to distinguish T1D from T2D. Dr. Pettus presented the AABBCC framework (age, autoimmunity, BMI, background, control, comorbidities) currently used to differentiate the two types of diabetes. For example, those who are younger and those who have other autoimmune diseases (e.g., celiac or hyperthyroidism) are likely to have T1D. However, Dr. Pettus noted that while such factors are important to consider, they don’t help distinguish all cases of diabetes diagnosis. He encouraged focusing on people in the “middle” – those with unclear features of either T1D or T2D.
- Reclassification of prediabetes and T2D into T1D. Among the total population initially diagnosed with prediabetes or T2D, 2.2% were reclassified with T1D. While 2.2% may seem like a low proportion of individuals with reclassification, Dr. Pettus said that the true number of people (n=147,419) creates a different perspective. Considering only people with a T2D diagnosis, the reclassification rate was nearly 4%.
- Features of those reclassified with T1D. The study found that reclassification rates were higher in individuals <18 years than in those 18-35 years (7% vs. 4.4%). There was no notable difference in reclassification rate across gender and race/ethnicity. While underweight individuals had slightly higher reclassification rates (2.5%), overall, BMI was not found to be a reliable predictor of reclassification. Furthermore, individuals with renal disease had higher reclassification rates (2.8%), as well as those with Addison’s disease (2.9%) and celiac disease (2.4%).
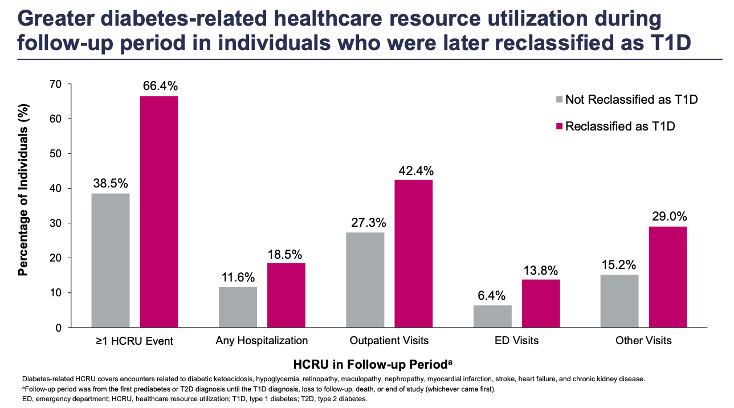
- Timing of reclassification and utilization of healthcare resources. The study also found that most reclassifications (81%) to T1D occurred within three years of initial diagnosis with prediabetes or T2D. Dr. Pettus commented that this timeline seems “relatively soon.” On the other hand, 19% were reclassified after three years, highlighting the proportion of individuals who likely had unmet needs in their diabetes management. Study results also pointed toward greater use of diabetes-related healthcare resources during the follow-up period in people later reclassified as T1D. In response to this finding, Dr. Pettus said that people with misclassification likely had suboptimal disease management. While the field has recommendations and guidance in place, Dr. Pettus pushed for greater efforts toward distinguishing between T1D and T2D to provide the sufficient care people need.
12. Dr. Satish Garg on the adjunctive use of incretins in T1D and obesity: Recommendations from an upcoming consensus report
Dr. Satish Garg (University of Colorado) shared guidelines from an upcoming consensus report for the adjunctive use of incretins in people with T1D and obesity. Drawing on much of his research from the last decade, Dr. Garg reviewed findings from multiple studies that are referenced in the upcoming report, which will be published in the June edition of DT&T. As background, pramlintide, an amylin analogue, is the only FDA-approved therapy for T1D that has potential weight loss benefits. Despite this, there has been an exponential increase in prescriptions for GLP-1 RAs in the US, warranting a consensus report and guidelines on their safe use in T1D. Dr. Garg shared that there are over 700 patients with T1D at University of Colorado’s Barbara Davis Center for Diabetes who have been prescribed semaglutide or tirzepatide.
Key takeaways from the report include:
- Start slow, adjust dosage gradually, and individualize treatment. Dr. Garg said that the full dose is usually not necessary to achieve the full benefits of these therapies in this population. The majority of his patients, for example, only need to go up to the 7.5 mg and 10 mg doses of tirzepatide. He also emphasized the need to titrate insulin doses carefully, particularly prandial insulin. He shared a case study in which a 20% reduction in a patient’s total daily dose was insufficient, resulting in an ER visit for a hypoglycemic event. In another case study, a patient decided to reduce their basal insulin by 60% instead of the advised 20%, running the risk of ketosis. For some patients, it may also be necessary to adjust the dosages of their other medications (e.g., T4, statins, and blood pressure medications). Once the desired weight is reached, the consensus recommends considering a dosage reduction to achieve a maintenance dose.
- Dr. Garg also emphasized the importance of managing nutrition to prevent sarcopenia, mitigating GI side effects, and ensuring patients have ketone strips and glucagon.
- Baseline labs and annual eye exams. The consensus report recommends lab tests for TSH, uric acid, albumin excretion rate (AER), albumin-to-creatine (A/C) ratio, eGFR, and more. Annual eye exams are also advised given reports of incident or worsening diabetic retinopathy resulting from rapid A1c correction. Dr. Garg emphasized that in a real-world study with tirzepatide, there was no difference in risk compared to controls except when individuals had a high baseline A1c.
13. Interim results for Diamyd’s phase 3 DIAGNODE-3 results for retogatein in stage 3 T1D expected by end of month
During the exhibit hall tech fair presentations, Diamyd Medical’s Chief Scientific Officer Mr. Anton Lindqvist gave an overview of the company’s T1D precision medicine work and shared updates about study recruitment and upcoming results. As background, the company’s key candidate retogatein is an antigen-specific immunomodulatory therapy targeting individuals carrying the HLA DR3-DQ2 haplotype (approximately 40% of individuals with T1D). Retogatein is administered as an intralymphatic injection. Mr. Lindqvist highlighted that the company has been in the clinical development phase of T1D treatments for over 20 years, having dosed now over 1,000 patients. The company’s early studies led to the discovery that individuals with the HLA DR3-DQ2 haplotype were particularly responsive to retogatein, prompting the company to focus on this population.
- Phase 3 DIAGNODE-3 trial for stage 3 T1D. As shared in the company’s F1Q26 call, the DIAGNODE-3 trial for retogatein has completed participant screening, enrollment, and randomization. Interim results are expected in March 2026, and this readout will be based on approximately 170 of the 310-320 individuals who, by that time, will have completed their 15-month visit. The company will also present these interim results in a symposium at ADA 2026 in June. The full primary readout is not expected until 3Q27.
- Of those screened in DIAGNODE-3, around 52% had the DR3/X or DR3/DR4 genotype, retogatein’s target population. About 37% had the DR4/X genotype, which may benefit from proinsulin treatment – a potential future direction for the company. The remaining 11% are not carriers of the DR3 or DR4 allele.
- DiAPREV-IT and DiaPrecise for early-stage T1D. Diamyd Medical is also in the process of publishing results from its DiAPREV-IT study for retogatein, which found a significant delay in progression to stage 3 T1D in 50 children positive for ≥2 islet autoantibodies. DiaPrecise is an ongoing phase 2 trial (n=16) in children and adolescents with stage 1 or 2 T1D estimated to complete in December 2026.
14. Clinical pearls on once-weekly insulin use in insulin-naïve and insulin-experienced people with T2D
In this PeerView and Lilly-sponsored educational symposium, Prof. Chantal Mathieu (KU Leuven, Belgium), Dr. Harpreet Bajaj (LMC Healthcare, Canada), and Dr. Athena Philis-Tsimikas (Scripps Health) shared clinical recommendations on using once-weekly insulin in people with T2D. Prof. Mathieu said that basal insulin is a critical treatment for people with T2D who are not at glycemic goal despite noninsulin agents or cannot tolerate other medications. However, due to the complexity of the insulin regimen, fear of hypoglycemia, and poor adherence, many patients face challenges in intensifying insulin treatment. Indeed, studies show that nearly one in five patients misses at least one basal insulin dose over 14 days. In the US and Europe, adherence rates range from 42-56%. Prof. Mathieu said that once-weekly basal insulin, like Novo Nordisk’s insulin icodec (U-700) and Lilly’s efsitora alfa (U-500), can lower treatment burden and address these challenges. The symposium focused specifically on their use in insulin-naïve and insulin-experienced people with T2D. See PeerView’s guide for clinicians on insulin icodec and efsitora alfa use.
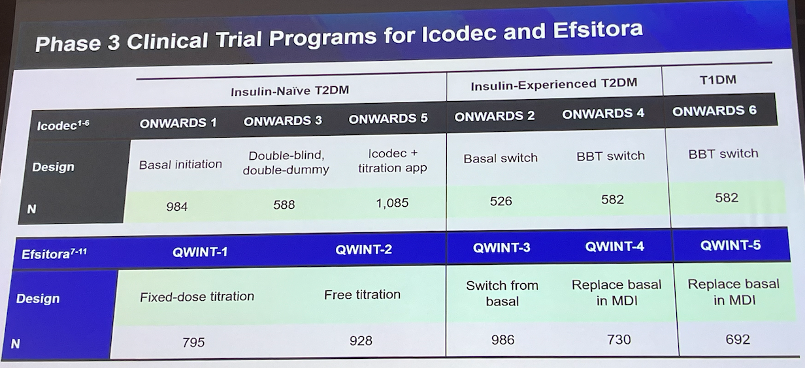
- Dr. Bajaj said that insulin-naïve patients with T2D were probably the “easiest” patient profile to consider once-weekly insulin. In the ONWARDS-1, 3, and 5 trials, insulin icodec demonstrated superior A1c reduction (1.55-1.68 vs. 1.31-1.36 percentage points) compared to insulin glargine or degludec. In the QWINT-1 and 2 trials, insulin efsitora alfa showed noninferior A1c reductions (1.19-1.34 vs. 1.16-1.26 percentage points). Moreover, hypoglycemia incidence and duration were similar between once-weekly and once-daily insulins, although weight gain was numerically greater with once-weekly insulins. Dr. Bajaj further explained titration protocols: insulin efsitora alfa begins with 100U and is up-titrated every four weeks based on glycemic level, while insulin icodec’s doses are adjusted by 20U (10U if at high risk of hypoglycemia) based on three pre-breakfast glucose levels. Finally, he said that more studies are needed to assess its use in children, pregnant or lactating women, individuals with hypoglycemia unawareness, or those newly diagnosed with T1D. See the table below for key clinical takeaways for using two once-weekly insulins.
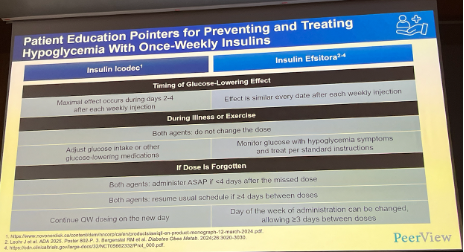
- For insulin-experienced people with T2D, Dr. Tsimikas reviewed ONWARDS-2, 4, QWINT-3, and 4 studies, in which insulin icodec and efsitora alfa demonstrated comparable efficacy in A1c reduction as insulin degludec or glargine. Hypoglycemia incidence was similar for both once-weekly and once-daily insulins; weight gain was comparable, as well, except in the ONWARDS-2 trial, in which insulin icodec conferred a 1.7 kg (3.4 lbs) increase in body weight compared to insulin degludec. Next, Dr. Tsimikas addressed several common questions about once-weekly insulin use in insulin-experienced people with T2D.
- First, what happens when a patient misses a once-weekly insulin dose? Encouragingly, in a randomized crossover trial (n=85), double or triple doses of insulin icodec had similar rates of clinically significant hypoglycemia as insulin glargine. In another study, a missed or doubled dose had minimal effects on Time in Range (see figure below).
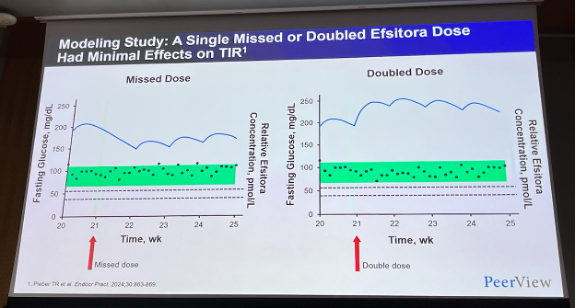
- How do the efficacy and safety of once-weekly insulin differ depending on baseline GLP-1 RA use? According to a subgroup analysis of the ONWARDS program, GLP-1 RA use did not affect the safety or efficacy of insulin icodec. In addition, the COMBINE-1, 2, and 3 studies found that insulin icodec combined with semaglutide was superior to insulin icodec or semaglutide monotherapies and noninferior to basal-bolus therapy.
- How should patients on once-weekly insulin prepare for perioperative settings? Dr. Tsimikas said that once-weekly insulins should be discontinued weeks ahead of the operation (four weeks for insulin icodec; eight weeks for efsitora alfa) if patients have reduced caloric intake for over 24 hours after a procedure or a liquid diet for over two days before a procedure. In an emergency situation, no dose adjustment is needed for once-weekly insulin, and hyper- and hypoglycemia should be managed with usual protocols.
15. T1D screening and monitoring: IDF Europe’s international consensus on for early-stage T1D now published
Prof. Sufyan Hussain (King’s College London, UK) gave an overview of the rationale and contents of IDF Europe’s international consensus on screening and monitoring for early-stage T1D, which was published today in Diabetes, Obesity, and Metabolism. Prof. Hussain noted that this consensus is not so much a source of clinical recommendations for screening and monitoring (see the Breakthrough T1D-led consensus document for more on this) but rather a document making a case for screening and monitoring to the policy front.
- The document presents a nine-step national implementation roadmap: (i) create a mandate for islet autoantibody general population screening; (ii) build advocacy by engaging and educating stakeholders, especially PCPs; (iii) broadcast the news by creating awareness campaigns, which have shown to reduce DKA at T1D onset by up to 65.5%; (iv) promote public health participation; (v) start screening upon establishing necessary infrastructure; (vi) support people with early-stage T1D with monitoring programs, educational content, and psychological counseling; (vii) build registries for islet autoantibody screening; (viii) evaluate and improve processes; and (ix) determine value through cost-benefit analyses at local, national, and pan-European levels.
- On the rationale for this consensus, Prof. Hussain highlighted that roughly 0.3-0.6% of the population in Europe, or ~2.8 million people, has T1D. This figure is projected to rise to 3.9 million by 2040. The frequency of DKA at diagnosis in Europe is 40-42% and as high as two in three cases in Romania, for example. The annual cost burden across Europe is 17 billion euros, and each DKA event avoided saves an estimated 4,700 euros. Screening and monitoring can reduce DKA at T1D onset by up to 80%, and Prof. Hussain highlighted that public attitudes toward screening are largely positive – over 93% of individuals who participated in screening reported that they would do so again. Capillary fingerpick sampling and at-home dried blood spot kits appear to be the most preferred (90%) sampling method. Still there remains a significant knowledge gap, with 51-76% of parents and first-degree relatives reporting little to no knowledge about islet autoantibodies.
16. Lilly symposium: SURPASS‑EARLY trial underscores the potential to alter T2D progression with early tirzepatide treatment
In this Lilly‑sponsored symposium, Dr. Alice Cheng (University of Toronto, Canada) presented results from the ongoing SURPASS‑EARLY trial (n=794), a long‑term, phase 4 randomized study that evaluates whether early initiation of tirzepatide can shift the metabolic trajectory of T2D. This follows the full readout from Day #2 of ATTD and provides additional context on clinical impact. Adults diagnosed with T2D in the last four years were randomized to tirzepatide (titrated to 15 mg or maximum tolerated dose) plus metformin, or to intensified conventional care (ICC) with metformin and stepwise addition of guideline‑directed therapies. Over 104 weeks, the study assessed glycemic management, weight, waist circumference, and cardiometabolic markers to determine whether early, potent pharmacologic intervention could deliver greater and more durable metabolic improvements.
- Results. Compared with ICC, tirzepatide produced consistently superior outcomes across all major endpoints. Participants receiving tirzepatide achieved a greater reduction in A1c (2.24% compared to 1.45%) and substantially more weight loss (16% compared to 6%). Tirzepatide also led to improvements in HDL cholesterol, VLDL cholesterol, and triglycerides. Importantly, a significantly higher proportion of participants reached A1c targets, with 91% (vs. 66%) and 69% (vs. 27%) having A1c ≤6.5% and <5.7%, respectively.
- Clinical implications. Dr. Cheng was joined by Dr. Sufyan Hussain (King's College London, UK), Dr. Santiago Tofe (The University of the Balearic Islands, Spain), and Dr. Jonathan Rachman (University of Oxford, England), who emphasized that these results reinforce a broader shift toward early, comprehensive metabolic intervention. The combination of substantial weight loss, improved insulin sensitivity, and reduced beta cell stress aligns with the concept of modifying disease trajectory rather than simply managing hyperglycemia. They also highlighted how modern pharmacotherapy challenges traditional definitions of remission, as many individuals can now safely achieve near‑normoglycemia while on treatment. At the same time, sustained lifestyle support remains essential to prevent weight regain and metabolic deterioration. The panel emphasized the practical clinical relevance of early tirzepatide use. Many individuals may maintain excellent glycemic and weight outcomes with one additional therapy (tirzepatide + metformin), whereas ICC often requires multiple agents to achieve similar targets. The upcoming four‑year data will be critical for understanding durability and beta cell function trajectory.
17. Eight years of normoglycemia in preclinical T1D models of KRIYA-839; one administration designed to last a patient’s lifetime
In a captivating Friday evening symposium, representatives of North Carolina-based Kriya Therapeutics expanded on yesterday’s presentation of KRIYA-839, a novel gene therapy for T1D. CEO and Co-Founder of Kriya Therapeutics, Dr. Shankar Ramaswamy, joined Dr. Fraser Wright (Kriya Therapeutics), Prof. Fatima Bosch (Universitat Autònomia de Barcelona, Spain), and Dr. Jeremy Pettus (UCSD) to explore the potential of KRIYA-839 in humans as it moves to a first-in-human trial later this year.
- As background, KRIYA-839 is an adeno-associated virus (AAV) gene therapy that delivers insulin and glucokinase genes into patients’ muscles. Muscle cells, Dr. Jeremy Pettus (UCSF) noted today, do not typically regenerate. Modifications to muscle cells stand to last a lifetime, making KRIYA-839 a potential “one-and-done type of procedure.” Based on preclinical data, Dr. Pettus shared today that the genetic modifications are expected to “set” around three months after treatment.
- KRIYA-839 will be injected into the quadriceps muscles in both legs to “spread out” the therapy after a brief peri-dosing immunomodulation to support transgene expression. In initial trials, the therapy will be administered in an outpatient clinic with an ultrasound to guide precise and reproducible intramuscular delivery. Consistent with comments made on Day #2 of ATTD, patients can be discharged the same day as the procedure.
- In long-term preclinical studies in rodents and dogs this afternoon, glycemic control was maintained for at least eight years after a one-time dose of KRIYA-839 in preclinical models (see below). Notably, none of the preclinical models developed secondary complications. Sharing her excitement with the audience, Prof. Bosch notes that the preclinical species had “recovered completely from the diabetes” – including glycemic control, body weight, and energy (as evident in a video shared with the audience).
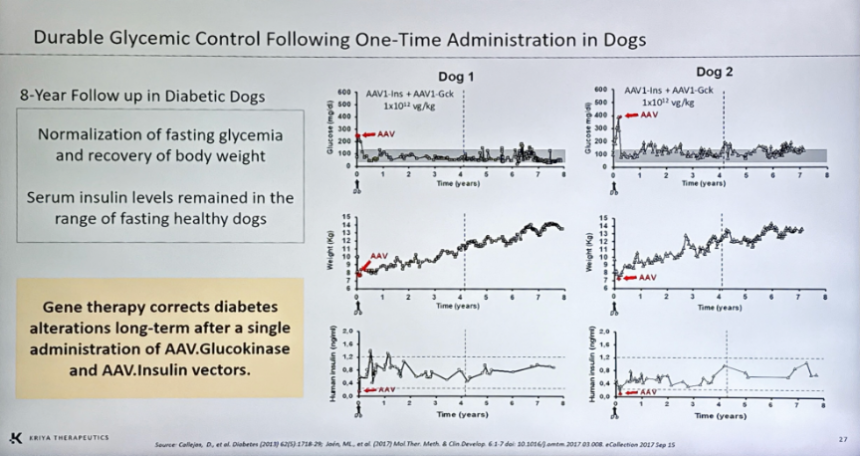
- Moreover, preclinical data support self-adjustment by treated muscle cells, maintaining appropriate glucose control for metabolic changes associated with aging without increased incidence of hypoglycemia. As shown in the photo below, an OGTT administered eight years after treatment demonstrated that both treated dogs had normal glucose tolerance. Furthermore, a post-mortem analysis of the preclinical models revealed that only a marginal number of ß cells remained in the pancreas among the dogs with induced T1D. Therefore, glycemic control was determined not to be from islet regeneration, but from the genetically engineered muscle.
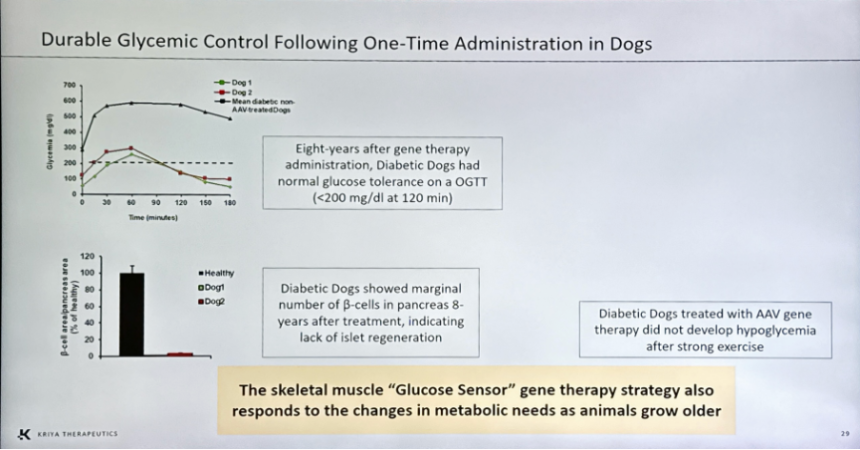
- A first-in-human study for KRIYA-839 remains on track to launch in 2026, and a potential for launch in clinics was shared to be as early as 2030. Adults with T1D and baseline A1c >7.0% on an AID system will be recruited. The trial will consist of Part 1 (dose escalation) and Part 2 (dose expansion), as well as 52-week post-treatment follow-up and long-term follow-up studies.
- Today’s speakers repeatedly framed KRIYA-839 as a response to persistent unmet needs in T1D, even in the hybrid-closed loop era. Specifically, they argued that current and future treatments, while mimicking physiologic insulin secretion, leave patients with a high disease burden, glycemic variability, and long-term complication risk. KRIYA-839 seeks to relieve the need for exogenous insulin by engineering skeletal muscle as a “glucose sensor” that co-expresses low-level insulin and glucokinase.
18. Immediate, intensive glycemic management for T2D: An argument for early insulin initiation
In this engaging morning symposium, Prof. Tadej Battelino (UMC Ljubljana, Slovenia), Dr. Illana Halperin (University of Toronto, Canada), Dr. Alice Cheng (University of Toronto, Canada), and Prof. Othmar Moser (University of Graz, Austria) offered clinical insight into insulin use for patients with T2D.
- Dr. Halperin advocated for the need for timely treatment intensification, drawing a parallel between early GLP-1 RA use in prediabetes and earlier insulin initiation in T2D. For GLP-1 RAs, patients who receive their first injectable therapy earlier in the diabetes disease course are more likely to achieve and maintain glycemic targets. Citing the UKPDS 44-year follow-up study (n=600), Dr. Halperin showed that early, intensive blood glucose management (an A1c target of <7.0%) confers a durable “glycemic legacy”: sustained risk reductions for microvascular complications, myocardial infarction, and all-cause mortality beyond a decade after trial completion. Accordingly, Dr. Halperin stressed that the T2D community must overcome therapeutic inertia. Timely intervention, she added, is critical to reduce risk of T2D complications – particularly for a population that develops T2D at a younger age than ever before, lengthening disease duration.
- Dr. Alice Cheng built on Prof. Halperin’s argument, reviewing the BEGIN and EDITION programs, which compared first- and second-generation insulins, as well as the head-to-head BRIGHT and CONCLUDE studies, which compared two second-generation analogs. Across these data, Dr. Cheng noted that second-generation basal insulin provides similar glucose-lowering effects with less hypoglycemia compared to first-generation agents. Further, she argued that when incretin-based treatments alone are insufficient for glycemic management in T2D, adding a basal insulin could be an effective next step. Fixed-ratio combinations (FRCs) of basal insulin and GLP-1 RA might also further simplify insulin administration while improving A1c, limiting weight gain, and reducing hypoglycemia compared to a premix or basal-bolus regimen. While an FRC may not be appropriate for every person with T2D, she concluded, the option could reduce injection burden.
- Prof. Moser closed the session by highlighting the potential for technology to support insulin use, including: (i) digital diabetes education; (ii) app-based titration algorithms; (iii) connected insulin pens; and (iv) integrated data platforms that combine CGM, dosing, and lifestyle information into a single ecosystem for HPCs and PWD. He said that such tools could accelerate insulin titration, improve A1c and Time in Range, and decrease clinician workload while helping patients manage the “mental math” and burden of insulin self-management.
19. *NEW* Updated results from Eledon Pharmaceutical’s tegoprubart (anti-CD40L antibody) as an immunosuppressant for people with T1D
In an evening session, Dr. Piotr Witkowski (University of Chicago) presented updated results from the investigator-led pilot trial of Eledon Pharmaceutical’s tegoprubart (anti-CD40L antibody) in people with T1D – results were also announced in a press release. These results include data from 12 participants, providing an update to results from six participants announced in November 2025 and presented at the Rachmiel Levine-Arthur Riggs Diabetes Research Symposium 2025. As background, tegoprubart targets the CD40L pathway to block immune cell activation, offering a safer and more effective immunosuppressant than traditional treatments. Immunosuppressants like tacrolimus, primarily used for transplantation, increase toxicity, including direct harm to islets.
- Trial background and baseline characteristics. The investigator-led pilot study enrolled 12 adults with T1D who received allogeneic islet transplantation at the University of Chicago Medicine. Participants had a median duration of T1D for approximately 33 years and a mean A1c of 8.0% before transplantation. All participants received tegoprubart at the time of their pancreatic islet transplantation. Enrollment criteria included participants 18-65 years of age, with a diagnosis of T1D ≥five years with onset of disease at <40 years of age.
- Preliminary results. Preliminary results from the pilot study demonstrated the safety and effectiveness of tegoprubart in protecting islet grafts post-transplantation. All 12 participants showed improvements in blood glucose management after the first islet transplantation. To date, 10 participants remain insulin independent, including six after one transplantation and four after two transplantations. The remaining two participants in the trial are on the same trajectory. Of the 10 participants who achieved insulin independence, all reached an A1c level <6.0%, with a mean of 5.4%.
- Safety results. Immunosuppression with tegoprubart was well tolerated, with adverse events related to post-transplant immunosuppression treated by lowering the mycophenolic acid dose. No participants showed rejections or development of donor-specific HLA antibodies. Participants also showed no signs of nephrotoxicity, neurotoxicity, or hypertension, which are commonly associated with tacrolimus-based immunosuppression.
- Future outlooks. Dr. Witkowski expressed gratitude for the trial, as well as for extending the study to evaluate tegoprubart in people with T1D and CKD undergoing islet cell transplantation. Positive results from this trial would position tegoprubart as an alternative to tacrolimus, which is generally unsuitable for people with CKD due to risks of kidney toxicity.
Big Picture Highlights
19. IDF Europe symposium focuses on diabetes detection, treatments, and cures
In the afternoon, IDF Europe hosted a lunch symposium focused on diabetes detection, treatment, and cure. Introducing the session theme, “Turning vision into reality,” Prof. Tadej Battelino (University of Ljubljana, Slovenia) welcomed the attendees and emphasized how timely this topic is in light of emerging development in the field. Dr. Sufyan Hussain (King’s College London, UK) started the session, highlighting an international consensus on screening and monitoring early-stage T1D, published today. Then, Ms. Marissa Hitchcock Town (Children with Diabetes) focused on diabetes stigma and practical approaches for population screening for T1D. Prof. Tsvetalina Tankova (University of Sofia, Bulgaria) followed this presentation with a presentation on CVD prevention for people with dysglycemia and diabetes, and Prof. Sanja Klobucar (University of Rijeka, Croatia) spoke on the use of CGM in people living with obesity, intermediate hyperglycemia, or T2D.
- Dr. Hussain on the newly published international consensus on screening and monitoring T1D. Just this morning, Diabetes, Obesity, and Metabolismpublished an international consensus on screening and monitoring early-stage T1D. From a European perspective, the article outlines key components of implementing general population screening for early-stage T1D. Dr. Hussain highlighted key takeaways from the statement, including the need for screening, as the frequency of DKA at T1D onset remains high at 20-40%, with associated risks of cognitive dysfunction, diminished beta cell function, acute kidney injury, and other complications. The consensus emphasizes that screening and monitoring could reduce the incidence of DKA at T1D onset by up to 80%, and that early detection could be further associated with reduced symptom severity at T1D onset, reduced long-term microvascular and cardiovascular disease, and overall improved quality of life. Dr. Hussain also highlighted that the consensus provides critical policy recommendations, including: (i) equity, making screening accessible for all populations regardless of socioeconomic status, ethnicity, or location; (ii) registries, allowing monitoring programs before screening; (iii) HCP education for T1D management, especially in primary care; (iv) participation with psychological support and clear communication for everyone who tests positive; and (v) evaluation of outcomes, including cost-benefit analyses. With the approval of a disease-modifying treatment, emerging screening criteria, and compelling evidence, Dr. Hussain stressed, “The moment for action is now.”
- Ms. Town addresses diabetes stigma, especially to encourage population screening for T1D. Taking the stage, Ms. Town shared that she has used “PWD” as her first credential to highlight her journey of living with T1D for 36 years. She even presented screenshots of her TIR data and a QR code for the audience to view her glucose data to emphasize how she has difficulty managing her condition. She highlighted how despite decades of living with T1D, in addition to professional certifications and working in the diabetes field, she still will experience time out of range. Ms. Town encouraged the importance of using appropriate and cognizant language with people with diabetes, avoiding labels like “diabetic,” “control,” and “compliance.” Especially among people being encouraged for T1D and early detection, Ms. Town said HCPs should: (i) use clear and simple language; (ii) provide context on risks and diagnosis at early stages; (iii) use caution with timeline estimates in diabetes progression; and (iv) provide actionable steps with glucose monitoring and advice on medical assistance.
- Prof. Tankova on CVD prevention for people with dysglycemia and diabetes. Prof. Tankova explained that prediabetes not only increases the risk of developing T2D but also CVD and other diabetes complications. Therefore, the management of prediabetes also affects the impact on micro- and macrovascular diseases. For example, a 2010 meta-analysis found an 18% increased risk of CVD in people with impaired fasting glucose and 20% increased risk of CVD in people with impaired glucose tolerance. Furthermore, a 2021 systematic review found that impaired glucose tolerance was associated with 19% increased risk of all-cause mortality, and impaired fasting glucose was associated with a 17% increased risk of all-cause mortality. Following these results, a 2025 study clarified the relationship between prediabetes and cardiovascular risk, finding that the progression of diabetes accounts for <25% of CVD risk. Therefore, prediabetes has an association with an increased CVD risk even without diabetes progression.
- Prof. Tankova explained that altogether, these results highlight that the field must adopt a new approach, focusing on remission of prediabetes (i.e., transition from prediabetes to normoglycemia), rather than “just” stopping progression from prediabetes to diabetes. She referred to studies like the DPPOS study, which has shown the effectiveness of intensive lifestyle intervention on remission of prediabetes and CVD, as well as a 2024 study on GLP-1 RAs and lifestyle modification showing a 76% increased incidence of prediabetes reversion to normoglycemia. Prof. Tankova reminded, “We have strong tools in our hands,” encouraging the possibilities of prediabetes remission and ultimately, reduction of CVD.
- Prof. Klobucar on the use of CGM in people living with obesity, intermediate hyperglycemia, or T2D. Prof. Klobucar noted that CGM remains underappreciated in this population, despite emerging benefits. Establishing the relationship between obesity, intermediate hyperglycemia, and T2D, Prof. Klobucar said early detection of dysglycemia and timely intervention could break the chain of metabolic dysregulation. Referring to the studies demonstrating how standard diagnostic criteria (e.g., fasting glucose, oral glucose tolerance test, and A1c) often fail to detect or misclassify dysglycemia and new patterns of glucose dysregulation, Prof. Klobucar called for the use of CGM as an “educational and motivational tool.” With real-time biofeedback on the effects of diet and physical activity on glycemic levels, people could implement behavioral changes focused on obesity and T2D. Interestingly, a 2022 study found that the use of CGM has supported 67% of study participants experiencing diabetes remission at a three-month follow up. Importantly, Prof. Klobucar encouraged considering ways to reduce global disparities through the widespread adoption of CGM and the simplification of AI-driven data interpretation.
20. Beyond glycemia: Addressing overweight and obesity in T1D
Prof. Lia Bally (University of Bern, Switzerland) discussed the physiology behind overweight and obesity in T1D and its whole-body implications. Obesity is rapidly increasing in prevalence worldwide and among people with T1D as well. However, Prof. Bally urged the audience not to think of this trend as “simply obesity happening on top of T1D,” but rather to understand the fundamental physiology that contributes to the increased prevalence. She provided a detailed mechanistic exploration of overweight and obesity in T1D, three major ways to combat the rising prevalence, and related comorbidities that remain overlooked.
- The delivery of life-saving insulin for people with T1D has effects on weight gain and insulin resistance. In patients without diabetes, the pancreas secretes insulin into the portal vein, leading the portal vein to have a two-to-three-fold higher insulin concentration compared to peripheral insulin concentration in circulation. However, in T1D, the injection of subcutaneous insulin means that insulin concentration is higher in circulation, deemed peripheral overinsulinization. This contributes to insulin resistance and weight gain. In an analysis of specific organs, insulin sensitivity was lower in muscle and adipose tissue for people with T1D, while hepatic insulin sensitivity was similar across groups. Even in people with T1D with a normal weight and strong management, insulin sensitivity is lower than in matched controls, reflecting the consequences of peripheral insulin exposure. Prof. Bally said that once adipose tissue begins to accumulate with weight gain, this insulin resistance is only further amplified. She suggested three major approaches that may minimize excess insulin exposure: glucose-responsive AID systems, a restoration of the portal-peripheral insulin gradient, and improving insulin sensitivity via lifestyle intervention, adjunctive pharmacotherapy, or bariatric surgery.
- Prof. Bally discussed the benefits and drawbacks of three major classes of adjunctive therapies for T1D. GLP-1 RAs provide A1c reduction, weight loss, an increase in insulin sensitivity, and reduce total daily insulin dose, yet cause GI symptoms, ketosis, and biliopancreatic complications. SGLT-2 inhibitors also lower A1c values, contribute slight weight loss, reduce total daily dose, and improve kidney function. They also carry a risk of urinary tract infections, hypoglycemia, and euglycemic DKA. Finally, metformin lends a slight A1c value improvement, an improvement to insulin sensitivity, and a reduction in total daily dose, yet causes GI symptoms, hypoglycemia, and lactic acidosis in some cases. Prof. Bally identified GLP-1 RAs as the most promising weight-loss strategy that has been studied in T1D to date, as they can confer 20-35% reductions to insulin requirements, improve Time in Range (TIR) without increased hypoglycemia, and improve cardiometabolic health. She called for further mechanistic insight into the role of glucagon, gastric emptying, and insulin sensitivity, and said that individualized dosing and proactive insulin adjustment are essential. The use of GLP-1 RAs for T1D remains off-label, and there are specific safety concerns of euglycemic DKA and hypoglycemia that must be carefully navigated. Prof. Bally also said that the therapies lend a sixfold increase to hip fracture risk and recommended serial DXA scans and functional tests for patients using the therapies.
- Comorbidities must be given appropriate attention and mechanistic understanding for people with T1D. Prof. Bally said that T1D confers cardiovascular (CVD) risk independent of glucose control – even with an A1c value of 6.9% or less, CVD death is twice as prevalent compared to people without diabetes. This is driven by inflammation, insulin resistance, and oxidative stress. Additionally, she identified a female-specific vulnerability to CVD in T1D. In the general population, women are less likely to have CVD than men, but this protective effect is not seen in people with T1D. Polycystic ovary syndrome (PCOS) has about 20-40% prevalence in women with T1D, as well as excessive gestational weight gain and postpartum weight retention. In perimenopause, increased weight gain has been observed, along with an increase to cardiometabolic risk. All of these factors lead Prof. Bally to call for more aggressive CVD risk management.
21. Early-onset T2D in pregnancy: Prof. Helen Murphy highlights rising prevalence and urgent need for stronger preconception care
Prof. Helen Murphy (University of East Anglia, UK) examined pregnancy outcomes in women with early-onset T2D, emphasizing that the growing prevalence of T2D in women under age 40 represents a major and under-addressed clinical challenge. Drawing on national audit data and emerging CGM studies, she argued that improving outcomes for these pregnancies will require more than technology alone, highlighting the importance of preconception care, contraception access, and broader social support alongside glycemic management.
- Prof. Murphy began by highlighting the rapidly rising prevalence and high complication burden associated with early-onset T2D, specifically among socially underserved populations. Globally, early-onset T2D disproportionately affects women from ethnic minority groups and individuals living in areas of social deprivation. It is also often accompanied by clustered cardiometabolic risk factors. Among women diagnosed before age 30, ~80% develop at least one microvascular complication by age 26, and life expectancy is reduced by ~16 years compared with later-onset disease. Using data from the UK’s mandatory National Pregnancy and Diabetes Audit, Prof. Murphy showed that pregnancies complicated by early-onset T2D now exceed those with T1D. Between 2022-2024, the UK recorded over 9,000 pregnancies with T2D versus ~6,000 with T1D, meaning roughly 60% of diabetes pregnancies now occur in women with early-onset T2D. Alarmingly, rates of serious adverse pregnancy outcomes, including congenital anomalies, stillbirth, and neonatal death, are now higher in early-onset T2D pregnancies than in T1D pregnancies, reflecting persistent disparities in care.
- Prof. Murphy said that the most impactful intervention for improving pregnancy outcomes in this population is not technology, but better preconception care and pregnancy planning. She showed that women living in the most deprived communities are both least likely to plan pregnancies and most likely to develop early-onset T2D. Achieving optimal glycemic outcomes before and during pregnancy remains critical. Maternal A1c above target after 24 weeks gestation is strongly associated with increased risk of stillbirth and neonatal death, even after adjusting for early pregnancy glycemia. However, while progress has been made in improving early pregnancy glycemic outcomes among women with T1D, the data suggests little improvement, and potentially worsening trends, in early-onset T2D pregnancies, underscoring the need for targeted clinical interventions.
- Turning to technology, Prof. Murphy discussed the potential and current limitations of CGM use in pregnancies complicated by early-onset T2D. In the UK, ~90% of women with T1D enter pregnancy already using CGM and ~97.5% are using CGM by 24 weeks, demonstrating near-universal adoption. In contrast, only ~16% of women with T2D enter pregnancy using CGM and only about half are offered the technology early in pregnancy, despite strong patient preference for it. While RCTs and real-world data have shown that CGM improves glycemic outcomes in T1D pregnancies, she noted that evidence in T2D pregnancies remains limited. Key unanswered questions include optimal CGM targets and how CGM metrics relate to neonatal outcomes in this population. Prof. Murphy highlighted an ongoing UK trial, the PROTECT RCT, where her team is actively recruiting 422 pregnant women across 20 NHS sites. The study aims to determine the clinical benefits and cost-effectiveness of CGM in women with T2D. Ultimately, she concluded that improving outcomes will require an integrated care strategy that combines glycemic optimization with contraception access and broader social care, instead of relying on technology alone.
22. *NEW* Dr. Nicole Glaser offers a sneak peek at ISPAD’s 2026 updates to Pediatric DKA Guidance
In an engaging Friday afternoon address, Dr. Nicole Glaser (University of California Davis) offered a first look at ISPAD’s 2026 updates to pediatric DKA guidelines. Dr. Glaser stressed that the 2026 guidelines remain a work in progress. Therefore, recommendations she shared in today’s presentation may change before the official 2026 guidelines are published later this year, but should provide good insight into the discussions behind the upcoming guidelines.
- ISPAD’s 2026 guidelines will emphasize the adjunctive use of CGM for glucose monitoring during DKA treatment. In recent studies, CGMs were found to offer similar accuracy during cases of DKA compared to non-DKA cases. While this evidence is insufficient to recommend replacing point of care (POC) glucose testing, ISPAD plans to recommend the adjunctive use of CGM during pediatric treatment for DKA.
- ISPAD will expand options for DKA treatment based on the biochemical features of DKA and local capabilities. The guidelines, Dr. Glaser said, will be broken down into cases of mild DKA, moderate-severe DKA, and hyperosmolar DKA.
- In mild DKA, which was defined as well-appearing and hemodynamically stable patients without hyperosmolarity or vomiting, ISPAD will recommend a subcutaneous insulin protocol. The protocol, Dr. Glaser explained, is designed to be less labor-intensive and to be managed on a general pediatric ward – addressing a common challenge of limited intensive care and specialized diabetes ward capacity. Recommendations for mild DKA treatment were drafted based on group consensus. Dr. Glaser emphasized that such recommendations can be modified according to local capabilities and resources.
- Basal insulin infusion (0.3 units/kg for new-onset diabetes or a patient’s usual dose for known diabetes) is now recommended at the time of mild DKA presentation.
- Rapid-acting insulin (0.15 units/kg every 3-4 hours) is also advised for mild DKA. The rapid-acting dose should be adjusted to patient response: dose reduction is recommended if blood glucose falls >5 mmol/L/hour and an increase is recommended if the BOHB/anion gap does not improve.
- Fluids can be taken orally if well-tolerated, with an aim to replace 5% dehydration. If unsuccessful, IV rehydration with a 10 mL/kg 0.9% saline bolus and, later, 0.45-0.9% saline and 20 mmol/L KCL is recommended to replace 5% dehydration.
- Monitoring of vital signs and POC glucose testing is recommended every 1-2 hours for the first 3-4 hours after presentation. Subsequently, monitoring vitals, POC glucose, BOHB, and electrolytes is recommended every 3-4 hours.
- In hyperosmolar DKA (defined as serum glucose >600 mg/dL and serum osmolarity >320 mOsm/kg), Dr. Glaser characterized fluid and electrolyte deficits and risk of ketosis/acidosis to be substantially greater than mild-moderate DKA.
- Monitoring was described as “the key” to treatment of patients presenting with hyperosmolar DKA. Frequent electrolyte monitoring is now recommended, including: (i) basic electrolytes (e.g. K) every 2-3 hours; (ii) Phos, Ca, and Mg every 3-4 hours; and (iii) frequent reassessment (initially hourly) of I/O balance and circulatory status. Hourly monitoring of each, Dr. Glaser noted, may be required.
- In mild DKA, which was defined as well-appearing and hemodynamically stable patients without hyperosmolarity or vomiting, ISPAD will recommend a subcutaneous insulin protocol. The protocol, Dr. Glaser explained, is designed to be less labor-intensive and to be managed on a general pediatric ward – addressing a common challenge of limited intensive care and specialized diabetes ward capacity. Recommendations for mild DKA treatment were drafted based on group consensus. Dr. Glaser emphasized that such recommendations can be modified according to local capabilities and resources.
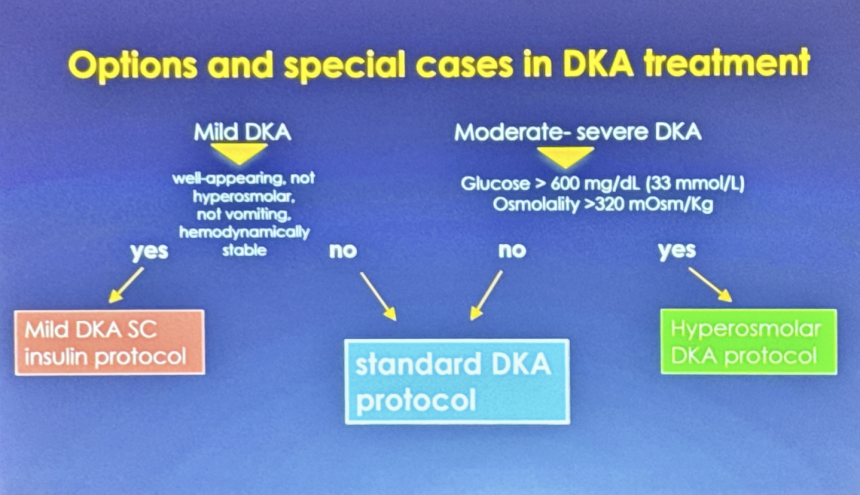
- The 2026 updates expand guideline discussion of hyperinflammatory states caused by DKA and their potential role in DKA complications. A hyperinflammatory state has been well characterized to contribute to insulin resistance before and during DKA episodes. Moreover, clinical inflammatory indexes (e.g. systemic immune-inflammation index) have been shown to correlate with DKA severity. Thus, updated guidelines suggest that inflammation may play a role in DKA complications, including sub-clinical cerebral edema, myocardial injury markers, and acute kidney injury (AKI).
- AKI occurs in 43-64% of all pediatric DKA cases and is highly predictive of AKI at subsequent DKA episodes. Patients with AKI during a prior DKA incidence, Dr. Glaser continued, have an “8-9x” higher rate of AKI for a subsequent DKA episode. A prior case of AKI, notably, also increases the rate of development of albuminuria later in life.
- While life-threatening cerebral edema and injury is rare (0.3-0.9%) in DKA, sub-clinical cerebral edema and injury are common. Further, children who suffer from a DKA episode also have evidence of subtle, lasting neurological injuries. This concern, Dr. Glaser added, becomes far more substantial in children who experience recurrent DKA episodes.
- Technology use and basal insulin to prevent recurrent DKA are emphasized in the 2026 updates. Dr. Glaser noted that the use of CGM alone confers a 40-50% lower rate of DKA. Use of insulin pumps with AID, however, confers higher rates of recurrent DKA. Per 100 patient years, children who used AID experienced 1.74 DKA events compared to 0.96 in children who did not use AID. In youth with an A1c value >8.5%, this trend was exacerbated: 5.25 incidences of DKA were reported per 100 patient-years in AID users compared to 1.53 in non-users. The administration of basal insulin by school personnel was highlighted for its 30% reduction in readmission for DKA, prompting a recommendation for the use of injected basal insulin in addition to insulin pump use in children with recurrent DKA. Notably, combining basal insulin injections with an insulin pump reduced DKA frequency from 25% to 9%.
23. *NEW* Dr. Ananta Addala on discrimination as the ‘elephant in the room’ shaping diabetes technology uptake
In this impactful session, Dr. Ananta Addala (Stanford University) discussed how discrimination – often the “elephant in the room” – shapes diabetes disparities, emotional burden, and technology readiness for underrepresented youth and families. Dr. Addala said that people often struggle to talk about discrimination because we are operating under a “fundamental logical fallacy,” treating race as if it were the same as ancestry. She said that while race is defined differently across country, regional, and even federal standards, most only ever look at pieces of the problem when trying to understand what drives disparities.
- Dr. Addala presented evidence showing that discrimination is measurable. Among caregivers, everyday discrimination correlated strongly with community discrimination (r=0.74; p<0.001) and lifetime discrimination (r=0.68, p<0.001). Discrimination also affects diabetes outcomes, with some studies finding that it is tied to lower diabetes‑technology acceptance (r=-0.38, p=0.05). Furthermore, Dr. Addala said that explicit racism is not only experienced individually but shared across generations. For example, explicit racism scores among youth and their parents are highly correlated, showing that discriminatory experiences are often mutually experienced among family members. She also said that parental reports of explicit racism were strongly linked to whether youth reported greater CGM burden and diabetes distress. She explained that these findings underscore that it’s not only the youth’s experience that shapes technology readiness, but the caregiver’s as well. These patterns generally mirror what is seen in generational trauma.
- While qualitative findings show that many marginalized families describe CGM as a necessity, pumps are viewed as optional or difficult to pursue because of insurance instability, fear of losing coverage, or lack of knowledge from providers. Families said that maintaining consistent access to CGM felt essential, whereas pursuing a pump often felt as if they were seeking a technology without certainty that its use would be sustainable. Dr. Addala closed by emphasizing that addressing discrimination in diabetes care requires coordinated action across every level of the system. She highlighted concrete steps that span policy, community representation, institutional practices, interpersonal interactions, and individual education that can be taken. Together, these actions outline a path toward more equitable access to diabetes technologies and more equitable outcomes for youth and families.
23. *NEW* Risk of diabetic retinopathy during pregnancy: New registry data challenge historical concerns around progression risk
Ms. Janni Larsson (Zealand University Hospital Roskilde, Denmark) spoke about diabetic retinopathy (DR) in pregnancy, including a clinical overview of the disease contextualized within nationwide evidence from a Danish registry. While pregnancy has historically been associated with worsening DR due to increased rates of circulating VEGF in the body, her group’s findings suggest that pregnancy may not independently increase the risk of progression with improved glycemic management and structured screening.
- Ms. Larsson contextualized DR as a leading cause of visual impairment globally and emphasized the importance of early detection but noted that progression rates have fallen dramatically over time. She reviewed the pathophysiology of DR, from early microaneurysms to proliferative disease with neovascularization and tractional retinal detachment. She also highlighted screening as critical to enabling timely treatment before vision loss occurs. Notably, historical data showed a marked decline in progression rates over several decades (from ~8% to <1% five-year risk), reflecting advances in diabetes management.
- Turning to new data, she presented findings from The Danish Registry of Diabetic Retinopathy (DiaBase), which suggest that pregnancy itself may not increase the risk of DR progression compared to non-pregnant women with T1D. In a cohort of pregnant women with T1D (n=1,041) matched to non-pregnant controls, there were no significant differences in: (i) progression to proliferative DR; (ii) development of diabetic macular edema; or (iii) need for treatment, such as laser or anti- VEGF injections, before, during, or after pregnancy. She noted that rates of treatment were low overall, and no excess risk was observed across pregnancy or postpartum periods. According to Ms. Larsson and her team, pregnancy was not identified as an independent driver of worsening retinopathy.
- Consistent with historical findings, baseline disease severity was found to be the primary determinant of risk, reinforcing the importance of individual screening strategies for DR before and during pregnancy. Within the pregnancy cohort, factors such as higher baseline DR level and longer diabetes duration were associated with progression. Notably, only ~2% of women with no or mild DR required laser treatment, compared to ~11% among those with more advanced disease, representing over a five-fold difference in treatment risk by baseline severity. This suggests that risk stratification may guide more efficient screening approaches.
- To close, she said these findings have already influenced clinical practice in Denmark, supporting a differentiated screening approach during pregnancy. National guidelines now recommend a single first-trimester screening for all women, with no additional screening during pregnancy for those without signs of retinopathy, followed by regular postpartum follow-up. Taken together, Ms. Larsson highlighted how advances in diabetes care are reshaping assumptions about pregnancy-related risk.
-- by Jeremy Alkire, Riya Chatterjee, Albert Cai, Nour Khachemoune, Kayla Mathieu, Esther Min, Kat Moon, Paul Moon, Elizabeth Rose, Elaine Young, Monica Oxenreiter, and Kelly Close