ATTD 2026 Day #2 Highlights –
Executive Highlights
- The 19th International Conference on Advanced Technologies & Treatments for Diabetes (ATTD) continued to buzz with excitement today in sunny Barcelona, Spain. From“Hot from the Oven” sessions to oral presentations, clinicians and scientists came together to discuss new study results on CGMs, the benefits of early initiation of incretin-based therapies, and a novel therapy for T1D. Experts also shared insights into the challenges of fully closed-loop systems and strategies to promote T1D screening. We were inspired by conversations about diabetes extending beyond the session rooms, such as in crowded exhibit halls and trams across the city.
- In tech, key sessions highlighted new study results and challenged the field to expand the role of diabetes technology. In a morning symposium, Dr. Emma Wilmot (University of Nottingham, UK) presented results from Abbott’s FreeDM2 trial (n=303), which compared FreeStyle Libre 3 with traditional BGM care in people with T2D using basal insulin alongside either SGLT-2 inhibitors or incretin-based therapy. FreeStyle Libre conferred significantly greater glycemic improvements at eight months, with A1c falling from 8.8% to 7.8% with FreeStyle Libre 3 and 8.3% with control.
- On AID systems for T2D, Dr. Heman Shakeri (University of Virginia) highlighted their potential role as a tool to accelerate insulin titration. Under current standards of care, clinicians are advised to begin basal insulin conservatively and increase doses gradually during clinic visits. However, this titration process is slow and can often stall, resulting in nonoptimized glycemic outcomes. The AID-BIT RCT showed that AID systems significantly accelerate the titration and improve TIR during the intervention by 20 percentage points. Based on these results, Dr. Shakeri suggested a shift from stepwise dose adjustments to a brief AID use to determine a patient’s insulin requirement.
- On CGM for prediabetes, Dr. Viral Shah (Indiana University) discussed various roles CGM metrics can play for people with prediabetes. First, it can identify six major stages of diabetes: (i) normoglycemia; (ii) Stage 1 prediabetes; (iii) Stage 2a prediabetes (slow progressors); (iv) Stage 2b prediabetes (fast progressors); (v) Stage 3a diabetes (non-insulin-requiring); and (vi) Stage 3b diabetes (insulin-requiring). It can also estimate the speed of progression and measure the “latest spike time” correlated with weight loss in people with obesity.
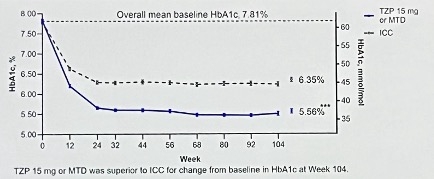
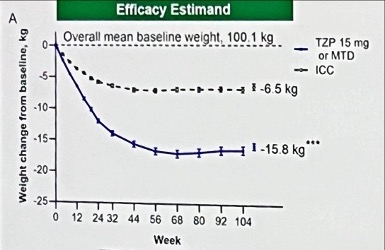
- In therapy, sessions focused on early initiation of tirzepatide, a new gene therapy for T1D, and the safety profile of once-weekly insulin efsitora alfa. In the morning session, Prof. Stefano Del Prato (University of Pisa, Italy) presented results from the ongoing phase 4 SURPASS-EARLY trial (n=794), which evaluates long-term outcomes of early initiation of tirzepatide vs. conventional care – comprising GLP-1 RAs, SGLT-2 inhibitors, DPP-4 inhibitors, and more – in people with T2D. At two years, tirzepatide conferred a superior reduction in A1c, resulting in 5.6% (vs. 6.4% with intensified conventional care) from the baseline of 7.8%. Moreover, the tirzepatide group conferred greater weight loss, CV risk reduction, and higher insulin sensitivity.
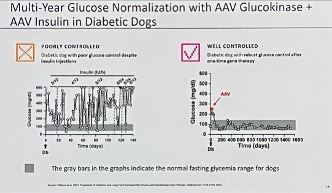
- In another thrilling morning session, Dr. Jeremy Pettus (UCSD) introduced KRIYA-839, a novel gene therapy for T1D. KRIYA-839 is an adeno-associated virus (AAV) gene therapy that delivers insulin and glucokinase genes into patients’ muscles through one-time administration. Insulin expression allows cells to absorb glucose, while glucokinase expression promotes glucose metabolism in the cells. Preclinical studies in rodents and dogs demonstrated glycemic normalization with the administration of AAV glucokinase and AAV insulin. The first-in-human phase 1/2 study for KRIYA-839 will launch in 2026.
- On another exciting front, Prof. Thomas Danne (Breakthrough T1D) introduced two new Breakthrough T1D initiatives aimed at redefining T1D care as an interventional discipline: (i) US certificate program in interventional diabetology; and (ii) BT1D-ATTD Course: Interventional Endocrinology in T1D. Applications for the latter are open until April 30. T1D screening was of high interest across multiple talks, as well. One panel discussion highlighted screening and treatment options for T1D, including Tzield, while another shared strategies to address the gap between population screening and the implementation of immunotherapy.
Table of Contents
-
Technology Highlights
- 1. FreeDM2 trial: FreeStyle Libre 3 improves A1c and TIR compared to BGM in adults with T2D on basal insulin and SGLT-2 inhibitors or incretins
- 2. Using AID to overcome clinical inertia in basal insulin dosing for T2D
- 3. Dr. Viral Shah on CGM for prediabetes: Staging, diagnosis, and potential therapeutic options
- 4. Fully closed-loop AID: Dr. Rayhan Lal discusses future challenges and considerations
- 5. CGM use in people without diabetes: New metrics for phenotyping, Time in Tight Range, and foundation models for glucose
- 6. Real-world performance of the Instinct sensor with the MiniMed 780G AID system
- 7. From hybrid to fully closed-loop: Dr. Marc Breton discusses UVA’s AIDANET AI-driven AID system and early trial results
- 8. dQ&A presents data on DKA awareness and ketone testing behavior of adults with T1D
- 9. Dexcom unveils Smart Basal dosing, extended high glucose alerts, and a new sensor patch in dynamic symposium
- 10. Toward hands-off diabetes care: MiniMed unveils the Vivera fully closed-loop algorithm
- 11. *NEW* Continuous insulin guidance with the DreaMed app: Proof-of-concept outcomes
-
Therapy Highlights
- 12. SURPASS-EARLY: Early initiation of tirzepatide for T2D improves glycemic and cardiovascular health
- 13. Dr. Jeremy Pettus introduces a novel gene therapy for T1D, KRIYA-839, which will enter the first-in-human phase 1/2 trial in 2026
- 14. Post-hoc analysis of the QWINT program finds comparable hypoglycemia duration between once-weekly efsitora alfa and daily basal insulin
-
Big Picture Highlights
- 15. ATTD 2026 exhibit hall brings together 80+ companies highlighting the latest in diabetes technologies and therapies
- 16. Breakthrough T1D to train interventional diabetologists and endocrinologists through US certificate program and joint course with ATTD
- 17. Delaying the onset of T1D: Screening and treatment options
- 18. Bridging the gap between population screening and initiation of immunotherapy
- 19. Exercise and T1D: Physiological differences, clinical trials, real-world evidence, and continuous lactate monitoring
- 20. *NEW* Helmsley Charitable Trust Symposium: Protein intake before exercise can prevent hypoglycemia in people with T1D
- 21. *NEW* Older adults and AID (automated insulin delivery): Choosing (and receiving!) the right technology at the right time for far better care
- 22. *NEW* Dr. Anna Kahkoska on aging and menopause for patients with T1D
Technology Highlights
1. FreeDM2 trial: FreeStyle Libre 3 improves A1c and TIR compared to BGM in adults with T2D on basal insulin and SGLT-2 inhibitors or incretins
Dr Emma Wilmot (Associate Professor, University of Nottingham, UK) presented results from Abbott’s FreeDM2 trial (n=303). The UK-based study compared FreeStyle Libre 3 with traditional BGM care in people with T2D using basal insulin alongside either SGLT-2 inhibitors or incretin-based therapy. Dr Wilmot. Wilmot stressed that although combination therapy with basal insulin is increasingly common, many patients still do not meet recommended glycemic targets, and clinicians have limited understanding of the glycemic and behavioral effects of CGM when added to these regimens. The study therefore aimed to determine whether FreeStyle Libre 3 could improve A1c compared with BGM, and ultimately demonstrated significantly greater improvements in A1c and TIR at four and eight months.
- Participants were randomized 2:1 to FreeStyle Libre 3 (n=198) or BGM (n=105) with usual care for 16 weeks. During this initial 16-week phase, participants could self-titrate insulin and implement lifestyle changes. Those not meeting glycemic targets at the end of this period could then receive clinician support to introduce additional therapies during a second 16-week phase. Participants initially randomized to usual care were also eligible to enroll in an optional 16-week extension phase and switch to FreeStyle Libre 3.
- Baseline characteristics. Participants had a mean age of 61 years and a mean diabetes duration of 17 years. Most (67%) were men, with a mean BMI of 31 kg/m². Baseline glycemia was suboptimal, with a mean A1c of 8.8% and Time in Range (TIR) of 40%. Dr. Wilmot said approximately one-third of participants were from the UK’s most socioeconomically deprived areas, and 84% were white. Many had diabetes-related complications at baseline: more than half had ocular complications, and about one in five had renal or cardiovascular complications. Participants performed an average of two finger-stick tests per day.
- Most were prescribed SGLT-2 inhibitors or metformin at baseline (87% and 86%, respectively), followed by sulfonylureas (33%) and GLP-1 RAs or dual GIP/GLP-1 RAs (26%). Nearly 20% were taking both an SGLT-2 inhibitor and a GIP/GLP-1 RA prior to enrollment.
- At four months, participants using FreeStyle Libre experienced a significantly greater reduction in A1c (-0.6%) compared with those using BGM. Specifically, A1c declined from 8.8% to 8.1% vs. 8.6%, respectively. By eight months, glycemic outcomes improved further, with A1c falling to 7.8% in the FreeStyle Libre 3 group and 8.3% in the control group. Nearly twice as many participants achieved A1c <8% at four months with CGM use (59% vs. 35%), though the difference narrowed slightly at eight months (62% vs. 48%). Similarly, about twice as many participants achieved an A1c reduction of ≥1% at four months with CGM (41% vs. 19%), and by eight months, roughly half of the participants in the FreeStyle Libre 3 group achieved this level of improvement.
- Participants using FreeStyle Libre 3 also saw a 10% greater increase in TIR (~approximately 2.5 hours) compared with BGM. TIR increased from 40% to 54% in the CGM group, versus an increase from 42% to 45% with BGM. By eight months, the mean TIR reached 60% with CGM compared with 50% in the control group. Improvements were observed throughout the day, though Dr. Wilmot highlighted particularly notable gains overnight.
- Medication changes were similar between groups. There were no significant between-group differences in insulin dose at four or eight months. Few participants initiated new medications at four months; introductions increased during the second, clinician-directed phase, but occurred at similar rates across both groups.
- The study also identified notable trends in lifestyle behaviors among CGM users. During the first phase of the trial, participants using CGM were more likely to choose healthier food options than those in the control group, though this difference was no longer significant by eight months. A similar pattern was observed for physical activity: CGM users’ accelerometer data showed greater overall activity and 12 additional minutes of light physical activity per day compared with the control group, but this difference also disappeared by eight months.
2. Using AID to overcome clinical inertia in basal insulin dosing for T2D
Dr. Heman Shakeri (University of Virginia) presented work exploring how AID systems could be used as a tool to accelerate insulin titration in individuals with T2D. He referred to this approach as AID for basal insulin titration (AID for BIT), which proposes using an AID system temporarily to determine an individualized insulin dose before transitioning patients back onto injection therapy. The work builds on prior real-world evidence showing that AID algorithms can help identify optimal insulin dosing in people with T2D, raising the possibility that the technology could help overcome the clinical inertia that slows insulin titration under standard care.
- Dr. Shakeri began by outlining the “titration gap” that exists when initiating basal insulin therapy in T2D. Under current standards of care, clinicians are advised to begin basal insulin conservatively and increase doses gradually based on intermittent glucose data collected during clinic visits. Because these decision points occur only every few days or weeks, the titration process is slow and can often stall. Even when following recommended protocols, reaching an effective insulin dose can take about 16 weeks, leaving many patients on less effective insulin levels for long periods. This delay reflects multiple structural barriers, including limited clinician bandwidth to review frequent adjustments and patients’ fear of hypoglycemia. As Dr. Shakeri said, the result is that many individuals with T2D never reach the optimal insulin dose needed to meaningfully improve glycemic outcomes.
- Retrospective real-world data suggest AID systems may significantly accelerate this process by continuously adjusting insulin delivery in response to glucose patterns. Dr. Shakeri reviewed a study which analyzed individuals with T2D using AID systems (n=796). The analysis showed that AID algorithms rapidly and safely increased insulin delivery for individuals with poorer baseline glycemic management. In some cases, the system identified an optimal insulin dose within seven days, producing reductions in hyperglycemia while keeping Time below Range (TBR) minimal and largely unchanged.
- These findings motivated the AID-BIT RCT, which tested whether short-term AID use could serve as a rapid basal insulin titration tool. The trial consisted of adults with T2D on basal insulin (n=16) and tested whether a brief period of AID use could identify an optimal basal insulin dose before transitioning patients back to injections. To ensure the system focused specifically on basal insulin titration, Dr. Shakeri said all meal-related pathways in the algorithm were discontinued so that the system could only adjust basal insulin delivery. This effectively turned the AID system into a “quick titration engine” with continuous adjustments based on CGM data.
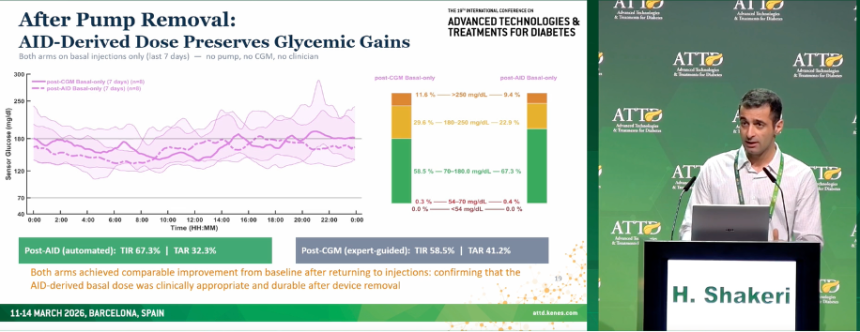
- Results suggest that short-term AID use can substantially improve glycemic outcomes while quickly identifying an optimal insulin dose. During the AID intervention phase, TIR increased by ~20 percentage points to 67%, largely driven by reductions in hyperglycemia. Importantly, TBR was unchanged, indicating that the algorithm increased insulin use without increasing hypoglycemia risk. After the AID system was removed and participants transitioned back to basal injections using the algorithm-derived dose, glycemic outcomes remained stable, suggesting that the system had successfully identified a patient’s appropriate basal insulin dose. The CGM-guided titration arm was used as a control, representing an accelerated and continuous data-driven approach to traditional titration efforts, achieved similar improvements after returning to injections, indicating that the AID-derived basal dose was clinically appropriate and durable even after device removal.
- Dr. Shakeri concluded that short-term AID use could be an effective tool for people with T2D starting basal insulin therapy. Instead of relying on months of stepwise dose adjustments, clinicians could use AID for a brief period to determine a patient’s basal insulin requirement, then translate that dose to injection therapy. If validated in larger studies, this strategy could help close the “titration gap” in T2D and allow clinicians to achieve effective insulin dosing more quickly than current approaches.
3. Dr. Viral Shah on CGM for prediabetes: Staging, diagnosis, and potential therapeutic options
Dr. Viral Shah (Indiana University) delivered an impressive presentation demonstrating advancements in the use of CGM for prediabetes. He discussed the use of CGM metrics in prediabetes staging, the estimated speed of progression, and the potential therapeutic use of CGM for the future.
- Dr. Shah discussed the need for prediabetes staging to identify patients most likely to progress to T2D and the role that CGM plays in this initiative. He suggested six major groups to consider, as published in The Lancet: (i) normoglycemia; (ii) Stage 1 prediabetes; (iii) Stage 2a prediabetes (slow progressors); (iv) Stage 2b prediabetes (fast progressors); (v) Stage 3a diabetes (non-insulin-requiring); and (vi) Stage 3b diabetes (insulin-requiring). Classifications consider fasting plasma glucose levels, OGTT results, A1c values, and Time in Tight Range (TITR). Dr. Shah said that the latter metric is essential for expanding understanding of T2D staging and truly implementing it. He pinpointed a TITR of 90-95% as indicative of Stage 1 prediabetes, 80-90% for Stage 2, and <80% for Stage 3.
- Beyond the three major categories of prediabetes progression, CGM metrics can also be used to estimate the speed of progression to diabetes. This varies greatly between individuals and has traditionally been difficult to predict clinically. Static blood glucose measurements may capture moments of dysglycemia, but do not capture important information such as the rate of change or the amplitude of glucose spikes. CGM enables the collection of 1.5 million data points every five minutes, in the words of Dr. Boris Kovatchev (University of Virginia), which can be harnessed for insight.
- Dr. Shah highlighted a novel glucose metric, “Latest Spike Time,” (LST) that has been correlated with weight loss in people with obesity. In patients using the Signos CGM, abnormal spike patterns that were at least eight times the normal variation seen in CGM were analyzed. Dr. William Dixon et al. (Signos) found that an LST before 5 pm was associated with significant weight loss over time. As OTC CGMs like Abbott’s Lingo and Dexcom’s Stelo expand in popularity, Dr. Shah called upon all providers to familiarize themselves with the systems and the insight they can provide clinicians, sometimes in an unexpected manner.
- The entropy of glycemic measurements can also provide insight into diabetes progression. Dr. Shah cited a study by Dr. Eslam Montaser (Indiana University) et al. that analyzed 5,754 daily CGM profiles across people with normoglycemia, T1D, or T2D. The authors found that plotting the probability of different glycemic states revealed insights into the likelihood of progression. For individuals with low entropy, signaling closely clustered, predictable glucose values, progression to diabetes was less likely. In contrast, those with more variable glucose values and higher entropy were more likely to progress to diabetes.
- Moving beyond diagnostics to CGM as a therapeutic tool requires more evidence. Dr. Shah has explored this topic with coauthors Dr. Salwa Zahalka (University of Colorado) et al., finding no existing data across 12 studies that CGM can be used to change prediabetes outcomes. However, based on his clinical experience and the quantity of data that CGM offers, Dr. Shah believes that such efficacy will eventually be demonstrated. He called for prospective studies on the use of CGM for prediabetes toward T2D prevention, which must address certain limitations before they can be fully implemented. For example, CGMs that are accurate within about 15 mg/dL are perfectly sufficient for PWD, however, for people with prediabetes or normoglycemia, the difference between 85 mg/dL and 100 mg/dL is striking and clinically significant. Dr. Shah’s talk was devoted to nuance throughout – in data analysis and clinical care. Such attention to detail will make all the difference in tackling prediabetes on a large scale.
4. Fully closed-loop AID: Dr. Rayhan Lal discusses future challenges and considerations
In a well-attended afternoon session, Dr. Rayhan Lal (Stanford University) described the global, interdisciplinary challenges that remain for fully closed-loop AID systems. He began by describing his personal journey with T1D, which he has lived with for several decades. He has innovated with his own management over time, and with the use of a GLP-1 RA and the AndroidAPS open-source AID algorithm, he has achieved 82% Time in Range (TIR) without meal boluses for the past three to four years. While a true, fully closed-loop system must also account for exercise, emotional, and hormonal changes that can affect glycemia, meal boluses are an important step towards this. Dr. Lal laid out three main lessons that the field must consider as it moves towards fully closed-loop AID.
- Lesson one: Pricing dynamics limit access to life-saving technology for PWD. Dr. Lal presented the stark differences in manufacturing costs versus out-of-pocket prices for key diabetes technologies. For example, Omnipod DASH and Libre 2 both cost manufacturers about $10 to produce, yet are sold at $60 and $70, respectively. However, in Australia, Omnipod DASH is sold for $15 due to the nation’s system of guaranteed healthcare. Dr. Lal said that the setup of the US healthcare system has prioritized the profits of the wealthy at the expense of everyday people with chronic diseases. Similarly, adjunctive therapies for T1D and disease-modifying therapies like pleconaril and teplizumab are sold for $86,400 and $194,000 per one-month supply, respectively, while their manufacturing costs are $15 and $6. Diabetes technology manufacturers have limited the compatibility of certain devices, such as CGMs and insulin pumps, or have been slow to expand this compatibility, affecting patients’ choices for their diabetes management. Dr. Lal said that the costs associated with a fully closed-loop system are a top concern as he considers the future of the field.
- Lesson two: PWDs do not have full access to their own health data. Dr. Lal said that real-time data access is dictated by the device manufacturer, so a corporate partner often has broader access rights to diabetes data than the patients themselves. Often, patients interested in optimizing their own care may be unable to see the full range of their own health data, while it is instead used for corporate development. Dr. Lal emphasized that open-source AID developers have played a key role in the development of the field as a whole, yet restrictions around data access are limiting innovation and research.
- Lesson three: Combining a CGM and an insulin pump into one device is already a possibility. Dr. Lal pointed to a paper by Tschaikner et al. published in 2020 that demonstrated that a CGM and insulin infusion set can be combined with just a 6-millimeter gap between the sensor and cannula opening. The demonstrated accuracy was similar to a sensor worn on another part of the body. Other options for insulin delivery, including intradermal, intramuscular, intravenous, and intraperitoneal, have other challenges, yet have also demonstrated efficacy. Dr. Lal said that the logistics of a fully closed-loop system have already been proven, yet the field has been slow to adopt them.
- Dr.Lal said that exercise remains the greatest challenge for a true, fully closed-loop system. Truly detecting exercise is imperfect using methods such as accelerometers in CGMs and may not capture the intensity of exercise fully. Dr. Lal also said that activity does not change blood glucose targets; it changes glucose utilization and sensitivity. Aerobic and anaerobic exercise also affect levels differently. While meal announcements may represent a soon-to-be-solved problem, exercise remains a challenge for the future of a fully closed-loop system, alongside the equity issues that Dr. Lal so expertly described.
5. CGM use in people without diabetes: New metrics for phenotyping, Time in Tight Range, and foundation models for glucose
In a recorded presentation, Dr. Smadar Shilo (Tel Aviv University, Israel) presented a range of results of CGM metrics in people without diabetes. Much of the data came from biobanks, including the “Human Phenotype Project” in Israel, which already has two years of longitudinal data on over 14,000 people. To start, Dr. Shilo talked through some results from the “CGMap” project, which evaluated CGM metrics in over 7,000 individuals without diabetes. That study identified several clinical parameters that were associated with CGM metrics, even in people without diabetes. For example, the fractal dimension, a measure of the structure of the retinal vascular tree obtained from fundus imaging, showed correlations with CGM-estimated A1c and CGM J-index. This suggests that fundus imaging can be used for early detection of dysglycemia, even in healthy individuals.
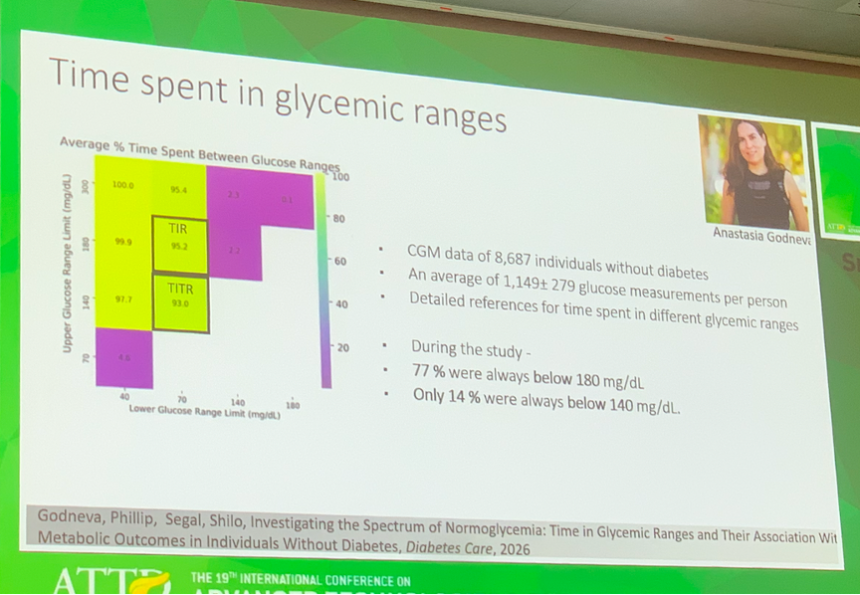
- Dr. Shilo also touched on recent data that showed differences between Time in Range (TIR; 70-180 mg/dL) and Time in Tight Range (TITR; 70-140 mg/dL) in healthy individuals. CGM data from 8,687 individuals without diabetes showed that the average person spends 95% of Time in Range and 93% of Time in Tight Range. More notably, 77% of individuals never went above 180 mg/dL during sensor wear but 86% of individuals did go above 140 mg/dL. On this, Dr. Shilo remarked that as CGMs are more commonly used in people without diabetes, education would be needed to reinforce that glucose levels occasionally rising above 140 mg/dL is quite common in healthy individuals.
- In the same dataset, Dr. Shilo noted that TIR was weakly correlated with A1c while TITR showed no correlation. However, a lesser proportion of Time <140 mg/dL, was associated with higher adiposity, a more atherogenic lipid profile, increase in hepatic-steatosis markers, worse sleep-breathing indices, and an increased risk of incident metabolic disease at follow-up. These correlations were stronger by looking at Time <140 mg/dL compared to Time <180 mg/dL, suggesting this may be a more valuable metric for people without diabetes.
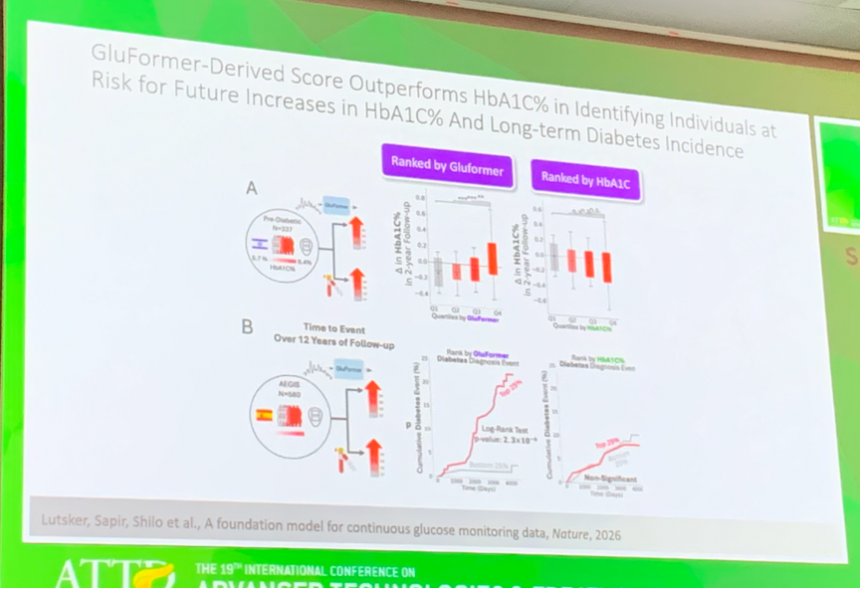
- Finally, Dr. Shilo talked about “GluFormer,” a generative foundation model for glucose in people without diabetes. The model, recently published in Nature, was trained on CGM data from about 11,000 adults without diabetes. The model is able to predict glucose values and was tested for some downstream prediction tasks in a set of individuals across multiple countries, including people with diabetes. Perhaps most impressively, in a cohort of 580 adults, GluFormer was able to predict risk of diabetes and cardiovascular mortality at follow-up (average 11 years) more effectively than A1c. With GluFormer, 66% of incident diabetes cases and 69% of cardiovascular deaths occurred in the top risk quartile, compared with 7% and 0%, respectively, in the bottom quartile. By contrast, with A1c, there was almost no separation between initial quartiles in terms of diabetes incidence at follow-up.
6. Real-world performance of the Instinct sensor with the MiniMed 780G AID system
Dr. Viral Shah (Indiana University) presented a real-world analysis of the performance of MiniMed’s Abbott-partnered Instinct sensor with the MiniMed 780G. The study aimed to assess: (i) the effectiveness of Instinct during real-world MiniMed 780G use; and (ii) the potential impact of switching from Guardian 4 to Instinct on patient outcomes. The analysis used CareLink data with a minimum of 30 days and a maximum of 90 days of data per participant. Overall, most users achieved target glycemia using the Instinct sensor as part of the AID system. Among those who switched sensors, modest improvements in glycemia were observed, largely driven by increased time spent in automated mode. Overall, Dr. Shah said the findings support the idea that the AID algorithm may influence clinical outcomes more than the sensor itself.
- Participants using Instinct with MiniMed 780G (n=13,967) achieved a mean Time in Range (TIR) of 76% and Time in Tight Range (TITR) of 52%. Overall, 72% achieved target TIR of >70%, and nearly all (96%) achieved target Time below Range (TBR; <70 mg/dL) of <4%. As seen with typical MiniMed 780G use, those using MiniMed 780G’s optimal settings[1] achieved higher outcomes, including 80% TIR and 57% TITR. Among these participants, 84% achieved TIR targets and 97% achieved TBR targets. Adults performed better than children and adolescents. Specifically, adult users achieved 75% TIR and 51% TITR, while children and adolescent users saw slightly lower mean TIR of 67% and TITR of 57% with Instinct use.
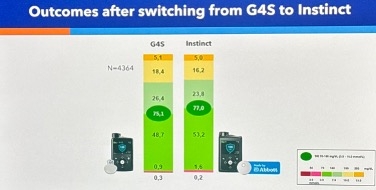
- Participants who switched from Guardian 4 to Instinct (n=4,364) experienced modest increases in TIR (75% to 77%) and TITR (49% to 53%). Dr. Shah attributed these improvements to greater sensor use (91% vs. 98%) and increased time spent in automated mode (90% vs. 96%), translating to nearly 1.5 more hours per day. Correspondingly, the number of daily automated boluses increased with Instinct use. Dr. Shah noted that there was no increase in the proportion of users adopting optimal settings, total basal insulin as a percentage of total daily dose, or the number of user-initiated boluses.
7. From hybrid to fully closed-loop: Dr. Marc Breton discusses UVA’s AIDANET AI-driven AID system and early trial results
In a forward-looking session, Dr. Marc Breton (University of Virginia) presented ongoing work on a fully closed-loop (FCL) insulin delivery system harnessing artificial intelligence, describing how data-driven algorithms may eliminate the need for user-initiated meal boluses. Dr. Breton began by noting that current commercially available, hybrid closed-loop (HCL) AID systems account for nearly all of AID users worldwide, with MiniMed, Insulet, and Tandem systems capturing 94% of the share. While these systems perform best when users announce meals, they have also all demonstrated safety and improved glycemic management even when meal announcements are omitted.
- Dr. Breton explained that moving from HCL to FCL remains challenging primarily due to physiological limitations. The central issue is the mismatch between the rapid rise in glucose following meals and the slower action profile of insulin, which leads to postprandial hyperglycemia even when boluses are delivered at mealtime. To address this challenge, Dr. Breton outlined several possible solutions. More advanced control algorithms could behave differently at the beginning versus later phases of a postprandial excursion, delivering insulin more aggressively early while slowing delivery later as glucose peaks. He said using adjunct therapies, including amylin, GLP-1 RAs, or SGLT-2 inhibitors, may also help soften the intensity of postprandial spikes.
- To overcome these limitations, Dr. Breton described the University of Virginia’s Automated Insulin delivery as an Adaptive NETwork (AIDANET) system. The platform incorporates data-driven modules designed to improve automated management of postprandial glycemia. Importantly, he emphasized that the system retains core safety protections from existing AID algorithms while allowing both hybrid and fully automated use, depending on how individuals choose to interact with the system. The system consists of the following:
- A neural network embedded within the control algorithm that analyzes recent glucose data and informs dosing decisions;
- A meal-pattern detection module that identifies glycemic patterns that resemble meals and delivers automated insulin doses; and
- An adaptation module that evaluates system performance over time and adjusts dosing behavior based on each user’s recent glucose responses.
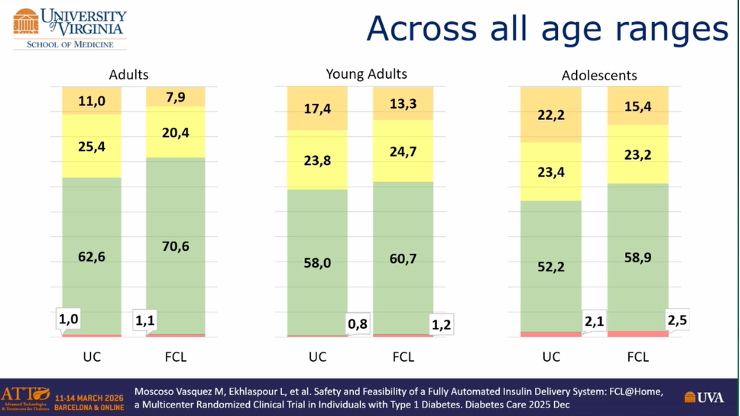
- In the multicenter study FCL@Home, the AIDANET system demonstrated non-inferior glycemic outcomes compared with current hybrid AID therapy, even without meal boluses. The trial included adult, young adult, and adolescent participants across three sites (n=34) and compared one week of FCL therapy against one week of usual care with HCL AID, following a supervised five-day hotel training phase. The primary endpoint, mean CGM glucose tested for non-inferiority with a 10 mg/dL margin, was successfully met, demonstrating that fully automated control could achieve glycemic outcomes comparable to current systems.
- Results were especially encouraging in individuals with poorer baseline glycemic management. Participants with baseline A1c levels ≥8% showed the largest improvements, with meaningful gains in TIR compared with their usual care. Across age groups, the system demonstrated consistent performance, with adult cohorts improving from ~53% to ~76% TIR in some analyses.
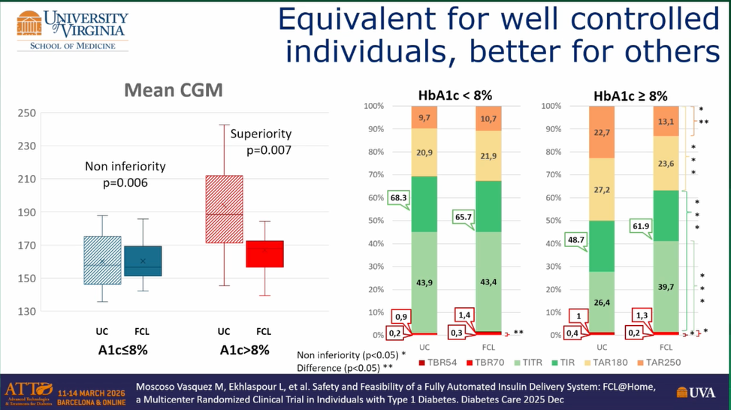
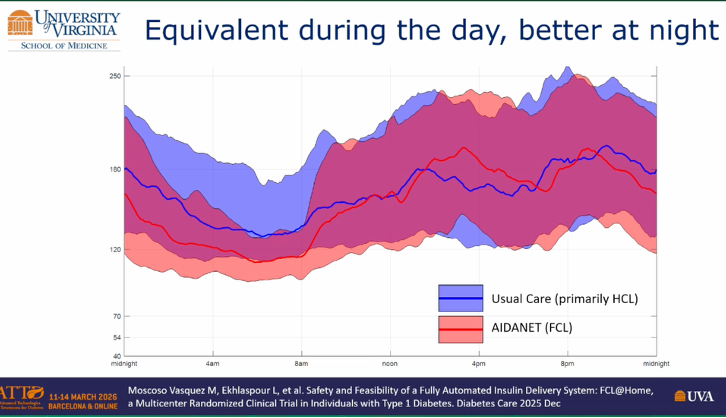
- Performance also varied by time of day. While daytime management was broadly comparable between systems, the FCL system demonstrated improved overnight glycemic regulation relative to current HCL systems.
- While FCL systems aim to reduce daily management burden, Dr. Breton said that optimal outcomes will likely still depend on user engagement. Although the system can safely maintain glycemic outcomes without meal announcements, individuals who choose to bolus or estimate carbohydrates generally achieve better postprandial outcomes.
- Additional testing suggests the technology may also be well suited for pediatric populations. In a study of 36 children divided equally into two cohorts, AIDANET was implemented on the iDiAs platform connected to Dexcom G6 and G7 and the Tandem Mobi pump. Preliminary analysis showed similar glycemic outcomes to those observed in adult cohorts, with comparable daytime management and improved overnight management relative to usual therapy.
- Dr. Breton concluded by highlighting emerging work using transformer-based AID models to further automate insulin dosing. These models analyze historical glucose and insulin time-series data, transforming data streams in to structured sequences that allow AI systems to generate automated insulin dosing decisions. Dr. Breton also previewed the ongoing AIDANET@Home study (n=22), which is evaluating glycemic management with the AIDANET algorithm across three modes: (i) AIDANET-FCL; (ii) AIDANET-HCL; and (iii) AIDANET with a mix between FCL and HCL. The study aims to better understand how individuals interact with varying levels of automation and whether different use patterns influence glycemic outcomes.
8. dQ&A presents data on DKA awareness and ketone testing behavior of adults with T1D
Ms. Philly De Piante (dQ&A) presented an e-Poster in the Exhibit Hall today examining how patient confidence in ketone interpretation relates to testing behavior and DKA awareness in adults with T1D. Ms. De Piante began by explaining that in many cases, numbers around rates of ketone testing in this population are not enough to explain the lived experience of T1D and the associated concerns around DKA. In this patient survey (n=1,419), US adults who own ketone testing kits were asked about: (i) their understanding of ketone testing results; (ii) which situations would prompt ketone testing; and (iii) whether their providers have discussed DKA risk and signs with them. They were then categorized as “confident” or “not confident” in their ability to interpret test results.
- Results showed that 19% of those surveyed were found to lack confidence in understanding ketone levels. These participants were more likely to express uncertainty about previous DKA events (17% vs. 8%), were half as likely to test ketones in all situations that could indicate DKA, and overall expressed more concern about the possibility of experiencing another DKA event (9% vs. 6%). Ms. De Piante concluded that there is a clear need to improve provider communication regarding DKA and education for people with T1D about when to test ketones and how to interpret those results.
9. Dexcom unveils Smart Basal dosing, extended high glucose alerts, and a new sensor patch in dynamic symposium
Dr. Jay Skyler (University of Miami), Prof. Chantal Mathieu (KU Leuven, Belgium), Dr. Keri Leone (Dexcom), and Mr. Girish Naganathan (Dexcom) sat for an afternoon panel discussion in ATTD’s busy auditorium. Dr. Leone and Mr. Naganathan introduced several exciting updates that will be coming soon to Dexcom’s product portfolio, including a new sensor patch, an extended high glucose alert, a Smart Bolus tool, and updates to the Stelo app. Dr. Skyler and Prof. Mathieu interjected regularly to offer their insights into the clinical utility of these features and additional areas for future exploration.
- Mr. Naganathan introduced a new sensor patchthat aims to increase sensor survivability. He cited internal data showing that 82% of G7 15 Day sensors lasts the full 15 days with the patch, with 89% of sensors lasting 14 days. Dr. Leone said that this does not come at the expense of skin safety, with no increase in skin irritation from the previous patch observed so far. Dexcom plans to roll out for Dexcom G7 15 Day users in the US in late 2Q26 or early 3Q26, followed by the rollout for G7 internationally in 3Q26 and for the 10-day G7 in the US in 4Q26. Prof. Mathieu noted that having a sensor active for longer is always an advantage but emphasized the need to monitor potential allergies and site reactions to the patch. Dr. Skyler joked that the longer wear time with the G7 15 Day meant he no longer needed to pack an extra sensor for trips like this, and that the adhesive on his sensor has already improved enough that he personally no longer uses an overlay patch.
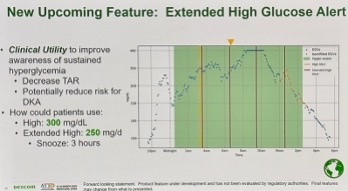
- Dr. Leone also introduced an upcoming feature: an extended high glucose alert designed to enable a more proactive response to sustained hyperglycemia. For example, she said users can set a standard high alert at 300 mg/dL and/or an extended high alert at 250 mg/dL, with the ultimate goal of increasing hyperglycemia awareness, reducing Time above Range, and lowering risk of DKA. Prof. Mathieu commented that it is beneficial that sustained high alerts will be customizable and suggested that future developments around sensor alerts could focus on allowing low alarms to be switched off. In response, Dr. Leone clarified that while the 55 mg/dL urgent low alert cannot be disabled users can modify how the alert is delivered for greater discretion.
- Dexcom also introduced Smart Bolus, which aims to help patients on MDI deliver accurate fast-acting insulin doses titrated over time without increasing fear of hypoglycemia. The feature will provide personal dose guidance by incorporating user-entered carbohydrates, meal timing and type, current glucose levels and trends, and insulin history. Patients are set up with provider-defined parameters, and the calculation follows the same equation typically taught in diabetes education[2]. By reducing the amount of math and decision-making required by patients, Dexcom hopes to improve therapy adherence and patient outcomes.
- Smart Bolus complements Smart Basal, part of Dexcom’s broader effort to simplify insulin optimization for people with diabetes. Dr. Leone suggested this is particularly useful in primary care, where most insulin starts in the US occur but both clinicians and patients often hesitate to initiate therapy. Smart Basal, now available with the G7 15 Day in the US and expected to expand to other products over time, is designed to reduce the need for frequent in-office titration visits. The feature currently supports only glargine U-100, with Dexcom pursuing additions including degludec and U-300. Across trials, no increase in hypoglycemia has been observed. Qualitative research suggests patients feel more confident adjusting eating behaviors, and providers have reported that the data help them titrate basal insulin more quickly and safely. Dr. Skyler noted that reminders to adjust insulin doses can help more people reach the correct dose.
- Dexcom also highlighted recent updates to the Stelo app, which is becoming increasingly designed to support daily experimentation, long-term tracking, and coaching. New features have included advanced food logging that assesses meal composition across carbohydrates, protein, and fat, either from manual entries or photos that are translated into these macronutrient estimates. Dr. Leone emphasized that the model was trained on culturally and ethnically diverse foods. The system can also show users how they have historically responded to that food, focusing on educating them on four aspects of glucose response: rate of rise, magnitude of rise, total glycemic exposure, and recovery toward pre-prandial levels. A built-in AI-based coach was designed to provide further educational insights and suggestions, which Mr. Naganathan described as a “nudge, not judge” approach. Dr. Skyler commented that the coaching responses could be particularly valuable in helping users gain deeper insights into their glycemic responses to different lifestyle habits, while Prof. Mathieu described it as having an educator “sitting on the patient’s shoulder.”

- Dexcom briefly addressed progress in EHR integration as well. About 160 clinics are currently or soon-to-be connected through the MyChart ecosystem, and Dexcom expects the upcoming 21st Century CURES Act requirement mandating HL7-based interoperability by 2028 to accelerate broader connectivity. Similar trends are emerging in European and UK digital health systems. Dexcom explained that through the Clarity One Click feature within Epic, providers and clinics can analyze patient cohorts through population tagging and visualize clinic-level data in a population health dashboard to support risk stratification. EHR connectivity is already established in the US, Canada, the UK, and the Netherlands, with further expansion planned. Both Dr. Skyler and Prof. Mathieu emphasized the importance of going beyond Epic, noting that many hospitals use different systems and that clinicians would benefit from flexibility in customizing how much data appears in reports.
- Finally, Dexcom reviewed its next-generation sensors, which are being developed with a multi-analyte approach capable of measuring both glucose and ketones. Dexcom G8 is expected to be roughly 50% smaller while maintaining the G7 15 Day’s wear time. The company is targeting a MARD <8%, improved Day 1 accuracy, and a warmup time of less than 30 minutes. As G8 development continues, Dexcom will also continue to invest in better adhesive technology, connectivity improvements, and shorter timelines for future partnerships, while also integrating generative AI in more of its products to deliver more personal insights. Dr. Leone also noted that the company wants to expand the technology into additional areas including GDM, prediabetes and metabolic disease, and inpatient care – the last of which Dr. Skyler said is crucial and should be pushed aggressively.
10. Toward hands-off diabetes care: MiniMed unveils the Vivera fully closed-loop algorithm
In one of the most popular sessions of the day, Dr. Goran Petrovski (MiniMed), Dr. Benyamin Grosman (Medtronic), Dr. Amir Tirosh (Tel Aviv University, Israel), Prof. Ben Wheeler (University of Otago, New Zealand), and Prof. Tadej Battelino (University of Ljubljana, Slovenia) presented details on MiniMed’s upcoming fully closed-loop algorithm Vivera to a packed auditorium. The system detects unannounced meals to automatically deliver safe boluses, allowing users to shift between traditional hybrid closed-loop (HCL) and fully closed-loop (FCL) operation. Early feasibility data suggest that the approach can maintain strong glycemic outcomes seen with MiniMed 780G with far fewer meal announcements, highlighting the potential for this next-generation algorithm to simplify diabetes care while preserving TIR.
- Dr. Grosman presented details of the Vivera algorithm, calling the next-generation system the culmination of years of closed‑loop evolution. He emphasized that Vivera is built to minimize user and provider interaction, with bolusing for meals becoming optional. Its most notable breakthrough is its ability to detect unannounced or late-announced meals and deliver safe auto‑boluses that prevent postprandial spikes while not increasing hypoglycemia. During wear, the algorithm will detect unannounced meals and estimate carbohydrates that have not yet been covered by insulin. Each bolus is adjusted using a four-hour glucose prediction model, identifying the largest meal bolus that keeps the prediction about the glucose setpoint. However, users will still have the choice of entering user-initiated meal announcements and boluses, allowing for them to elect the degree to which they engage with the system on a daily basis. The next-gen algorithm will adapt continuously based on patient outcomes during wear, adjusting its corrections based on a user’s persistent hypoglycemic or hyperglycemic events.
- Beyond this ability to transition between HCL-like and FCL use, the next-generation algorithm features several additional new features. Dr. Grosman said that by entering one’s total daily dose, a patient can bypass the traditional 48-hour warmup period. MiniMed will also introduce three new glucose targets with the algorithm: 90, 130, and 140 mg/dL (previously, MiniMed 780G offered 100, 110, and 120 mg/dL glucose targets), as well as a redesigned 150 mg/dL temporary target. Furthermore, active insulin time will no longer influence AID performance, a notable departure from this setting being one of MiniMed 780G’s two settings influencing optimal outcomes[3].
- MiniMed also previewed two different form factors for insulin pumps that will host the Vivera FCL algorithm. During the presentation, MiniMed termed these form factors Novel Medtronic Experimental (NMX) pumps. The first, which features a traditional screen (NMX7), was used in both the adult and pediatric studies assessing the algorithm (see below). The second features MiniMed’s next generation screenless insulin pump, termed NMX8.

- Dr. Tirosh presented first insights from the feasibility study in adults, and Prof. Wheeler presented results from the adolescent study. Participants in both studies underwent a four-week run-in period with Simplera Sync with MiniMed 780G, followed by nine weeks with the NMX7 AID system. This phase was split equally into three periods. First, the NMX7 system was used in HCL-style with announcements for all meals. It was then used as a pure FCL system lacking all meal announcements. Finally, participants could elect the degree to which they engaged with the pump. In the adult study, the final phase evaluated Medtronic’s NMX8 pump, in which participants could announce meals at will.
- In the adult study (n=14), participants had a mean age of 42 years and diabetes duration of 25 years. Mean A1c was low at 6.5%, and participants had a mean total daily dose (TDD) of 46 units, though Dr. Tirosh noted the range varied widely. Participants announced a similar number of daily meals during the meal announcement period as in run-in (approximately four), equating to a mean of ~150 grams of carbohydrates daily. When given the choice, participants elected to initiate boluses less than half of that time, averaging ~two boluses per day.
- There were no serious device-related adverse events, including severe hypoglycemia or DKA, throughout the study. When announcing all meals with NMX7, glycemic outcomes were very similar to the run-in period with MiniMed 780G (TIR of 83% and 84%, respectively). TIR targets were still met when adult users stopped announcing meals with NMX7, though it dropped to 74%. However, during this period TIR and TITR metrics improved over the course of the three weeks, demonstrating the algorithm’s ability to adapt to the user over time. These glycemic outcomes improved slightly when users elected which meals to announce, increasing to 78% TIR, suggesting patients still benefit from some user-initiated boluses even when using a FCL algorithm. Outcomes were similar between the two form factors: among those who used NMX7 and NMX8 with at-will meal announcements (n=10), TIR was 79% and 77%, respectively.
- The featured adolescent study (n=13) included children aged 8-17 years, with a mean age of 13 years and diabetes duration of seven years. Mean A1c was higher than adults at 7.6%, ranging from 6.4% to 9.1%. Participants announced an average of nearly five meals per day, also accounting for ~150 grams of carbohydrates daily. When given the choice to elect announcements, this dropped to approximately one bolus per day, accounting for ~40 grams of carbohydrate intake. One person missed the unannounced phase of the study, therefore data analyzed included 12 participants.
- As with the adults, there were no serious device-related adverse events during the study. TIR improved slightly when switching from MiniMed 780G to NMX7, from 68% to 74%. TIR fell to 65% when participants fully stopped announcing meals and increased slightly to 68% when announcing at will.
- In the adult study (n=14), participants had a mean age of 42 years and diabetes duration of 25 years. Mean A1c was low at 6.5%, and participants had a mean total daily dose (TDD) of 46 units, though Dr. Tirosh noted the range varied widely. Participants announced a similar number of daily meals during the meal announcement period as in run-in (approximately four), equating to a mean of ~150 grams of carbohydrates daily. When given the choice, participants elected to initiate boluses less than half of that time, averaging ~two boluses per day.
- Dr. Petrovski emphasized that Vivera is building on already strong clinical and real-world outcomes with MiniMed 780G. He highlighted real‑world MiniMed 780G performance showing approximately 76% TIR for all users, with those using optimal settings reaching over 80% TIR. Notably, the transition from use of the Guardian 4 sensor to Instinct, as presented by Dr. Viral Shah today at ATTD, revealed that improved outcomes were driven not by sensor technology alone, but by the algorithm’s enhanced automation capabilities. Dr. Petrovski underscored the potential for this new FCL system to reduce complexity for healthcare providers and users alike with its streamlined user experience.
- Prof. Battelino closed the session by discussing how glucose targets shape outcomes. He stressed that even mild elevations in glucose can impair brain function, with studies demonstrating acute declines in spatial working memory and long‑term differences in brain structure linked to Time above Range rather than A1c. Prof. Battelino also highlighted real‑world data showing that 44% of MiniMed 780G users reach target TITR of ≥50% on general settings while 81% reach it with optimal settings, suggesting that advancements to modern technology can meaningfully protect the brain and reduce long‑term risks such as dementia by reducing time in hyperglycemia. He emphasized that better outcomes are not only possible but already happening, and the next step is ensuring these gains come with less burden and more support for people living with diabetes.
11. *NEW* Continuous insulin guidance with the DreaMed app: Proof-of-concept outcomes
Prof. Andrej Janež (Medical University Ljubljana, Slovenia) spoke at ATTD Day #2 on the need for a “paradigm shift from episodic visits to continual intelligence” with the DreaMed app, an insulin dose guidance system for people with diabetes. The talk was titled “Evaluation of CGM-based insulin dose guidance system in people with type 1 and type 2 diabetes: Single arm feasibility study” and was from the “Hot from the Oven” symposium. The app, designed for both patients and clinicians, includes a bolus calculator, patient diary, and individualized insulin treatment plan. It integrates glucose monitoring data from patient devices to provide: (i) daily recommendations when needed; and (ii) weekly titration guidance, including an updated treatment plan, personal behavioral tips, and data visualizations for context.
- Prof. Janež presented results from a prospective, single-arm proof-of-concept study (n=45) with the app. Participants were evenly divided into three groups: (i) people with T1D using MDI; (ii) people with T2D using MDI; and (iii) people with T2D using basal insulin only. After a two- to four-week run-in period, participants received weekly insulin dose recommendations for 10 weeks. During the run-in, baseline metrics included: (i) Time below Range (TBR) of 3.7%; (ii) Time <54 mg/dL of 0.5%; (iii) Time >250 mg/dL of 5.3% (this is lower than we often see); and (iv) weekly averages of 0.5 severe hypoglycemia events and 1.2 prolonged hyperglycemia events.
- By the end of the study, TBR dropped by one percentage point to 2.7% from 3.7%, a drop of nearly 30%, and Time <54 mg/dL improved slightly to 0.4% (from ~55 minutes to ~40 minutes). Participants with T2D on basal-only insulin saw the greatest benefit, with TBR decreasing from 3.8% to 1.5% and Time <54 mg/dL from 0.8% to 0.3%. Those using MDI experienced more modest improvements, with TBR decreasing from 3.7% to 3.2% and no change in Time <54 mg/dL. The mean number of severe hypoglycemia events remained unchanged. Time >250 mg/dL improved overall to 4.6%, though this was driven by MDI users (from 6.8% to 5.5%), while those on basal-only insulin saw a slight increase (from 2.4% to 2.9%).
- Participants with higher baseline A1c experienced the greatest reductions after 10 weeks. Those starting between 7% and 8% saw A1c decrease from 7.5% to 7.2%, while those with A1c ≥8% dropped nearly one percentage point, from 8.8% to 7.9%. Participants with baseline A1c <7% remained stable (6.3% to 6.4%).
- Meaningful glycemic improvements were observed among participants who did not meet the consensus TIR target (≥70%) at baseline (n=21). TIR increased from 58% to 65%, primarily driven by a reduction in Time above Range (TAR) from 39% to 32%. Time >250 mg/dL, TBR, and Time <54 mg/dL also improved, though these changes did not reach statistical significance.
- Adherence to the app’s recommendations was generally high. Among those on basal-only insulin, fewer than 20% overrode more than 20% of recommendations, and about 10% logged at least 70% of their doses. Among MDI users, nearly one-third overrode fewer than 20% of recommendations, and 16% logged at least 70% of doses. Participants also reported high satisfaction with the app experience. Prof. Janež concluded that frequent algorithm-driven insulin titration recommendations can feasibly and safely improve glycemic management among people with diabetes on injection therapy.
Therapy Highlights
12. SURPASS-EARLY: Early initiation of tirzepatide for T2D improves glycemic and cardiovascular health
Italy) presented results from the ongoing phase 4 SURPASS-EARLY trial (n=794), which evaluates long-term outcomes of early initiation of tirzepatide vs. conventional care in people with T2D. The UK Prospective Diabetes Study (UKPDS) and STENO-2 studies found a “legacy effect,” in which achievement of early glycemic control following the diagnosis of T2D translates into long-term risk reduction of key diabetes complications1,2,3. Given that tirzepatide has been shown to improve glycemia, weight, CV risk factors, and insulin sensitivity in people with T2D, the SURPASS-EARLY trial aimed to understand “where tirzepatide will be placed in this picture” of early treatment initiation and its legacy effect.
- Study design and baseline characteristics. SURPASS-EARLY is a four-year, open-label phase 4 study conducted in 10 countries, including the US, Canada, the UK, Italy, and Germany. Adults diagnosed with T2D within four years and on metformin background therapy were randomized to receive tirzepatide or intensified conventional care (sulfonylurea, TZD, DPP-4 inhibitor, SGLT-2 inhibitor, GLP-1 RA, and insulin) based on local guidelines and aiming at achieving optimal glycemic control (within a non-diabetic range).
- The primary endpoint is a noninferior change in A1c from baseline at two years. Secondary endpoints include superior changes in A1c, weight, and waist circumference, as well as CV risk factors and insulin sensitivity and beta-cell function.
- At baseline, participants were 54 years old, with 49% being female. On average, participants had a mean A1c of 7.8%, a weight of 100 kg (221 lbs), a BMI of 35.4 kg/m2, a waist circumference of 114 cm (45 in), and a T2D duration of 2.6 years.
- In the tirzepatide group, 84% of participants reached the highest dose (15 mg). In the intensified conventional care group, 88% had one glucose lowering agent on top of background metformin therapy, 10% had two, and 1.2% had three. By drug classes, a vast majority (85%) was on GLP-1 RAs, including injectable semaglutide (56%), oral semaglutide (18%), and dulaglutide (12%). 17% were on SGLT-2 inhibitors, 3% on sulfonylureas, 3% on insulin, and 2% on DPP-4 inhibitors.
- Results. At two years, tirzepatide conferred a superior reduction in A1c, resulting in 5.6% (vs. 6.4% with intensified conventional care) from the baseline of 7.8%. Likewise, a greater proportion of participants achieved A1c targets; notably, 91% (vs. 66%) and 69% (vs. 27%) had A1c ≤6.5% and <5.7%, respectively. Tirzepatide also led to significantly greater weight loss of 16% compared to 6% from a baseline of 100 kg (221 lbs).
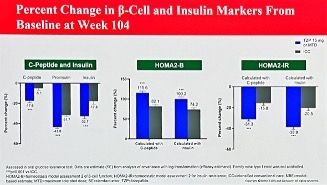
- On risk factors, tirzepatide led to significant improvements in HDL cholesterol (+7.7 percentage points difference), VLDL cholesterol (-18.6 percentage points), and triglycerides (-18.9 percentage points), as well as systolic blood pressure (-3.8 mmHg). Interestingly, tirzepatide also led to lower fasting plasma insulin levels but better improvement in basal insulin function (HPMA-B) and higher insulin sensitivity (HOMA-IR).
- Safety. Overall, tirzepatide had higher adverse event rates (75% vs. 69%) and treatment discontinuation from adverse events (4.5% vs. 0.3%).
- Ultimately, these results support the early initiation of tirzepatide to optimize health outcomes by helping to fulfill a more holistic approach as recommended by current guidelines.
13. Dr. Jeremy Pettus introduces a novel gene therapy for T1D, KRIYA-839, which will enter the first-in-human phase 1/2 trial in 2026
In a fascinating and well-attended symposium, Dr. Jeremy Pettus (UCSD) introduced KRIYA-839, a novel gene therapy for T1D. Dr. Pettus began the talk by highlighting the unmet needs in T1D despite continued innovations. In the US, over 70% of patients have A1c >7.0%, and one in 20 is admitted to hospitals each year for diabetic ketoacidosis (DKA). Moreover, people with well-managed T1D still have a two-to-four-fold higher risk of CVD, warranting additional approaches to address T1D. Reflecting on the T1D treatment landscape, Dr. Pettus shared an analogy that, if insulin were a train, technology a truck, and immuno- or cell therapies cars, gene therapies would be a “fancy fast car” that has not entered clinical development but has the potential to be a significant, quick-to-develop cure.
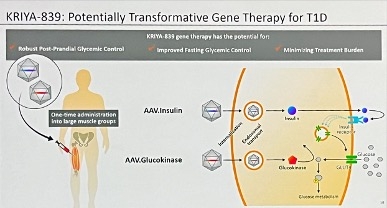
- KRIYA-839 is an adeno-associated virus (AAV) gene therapy that delivers insulin and glucokinase genes into patients’ muscles. As shown in the figure below,insulin expression allows cells to absorb glucose, while glucokinase expression promotes glucose metabolism in the cells.
- KRIYA-839 is designed to be administered once in large leg muscles. Patients will undergo a brief peri-dosing immunomodulation to support transgene expression. Then, in an outpatient clinic, the therapy will be administered with an ultrasound to guide precise and reproducible intramuscular delivery. Patients can be discharged the same day, increasing treatment accessibility and reducing burden.
- As background, AAV gene therapy uses non-pathogenic viruses as a vehicle to transport genes into patients’ cells to edit genes. AAV gene therapies offer durable clinical benefit and simple administration without the need for chronic immunosuppression or strict patient eligibility. While first in T1D, AAV gene therapies have previously been approved for other conditions, such as lipoprotein lipase deficiency (Glybera, alipogene tiparvovec), spinal muscular atrophy (Zolgensma, onasemnogene abeparvovec), and hemophilia A (Roctavian, valoctocogene roxaparvovec).
- Long-term preclinical studies in rodents and dogs demonstrated glycemic normalization with the administration of AAV glucokinase and AAV insulin. As shown in the figure below, four years after one-time gene therapy, diabetic dogs continued to have robust glycemic management with minimal fluctuations.
- The first-in-human study for KRIYA-839 is on track to launch in 2026. Adults with T1D and baseline A1c >7.0% on an AID system will be recruited. The trial will consist of Part 1 (dose escalation) and Part 2 (dose expansion), as well as 52-week post-treatment follow-up and long-term follow-up studies. Primary endpoints are the safety profile and the change in blood glucose and A1c from baseline. Key secondary endpoints include other measures of glycemic health, change in weight, and quality of life.
14. Post-hoc analysis of the QWINT program finds comparable hypoglycemia duration between once-weekly efsitora alfa and daily basal insulin
In this oral presentation, Dr. Natalie Bellini (University Hospitals) presented a post-hoc analysis of the QWINT 2-4 trials, evaluating once-weekly insulin efsitora alfa in adults with T2D. Across the phase 3 QWINT program, efsitora alfa showed glycemic efficacy comparable to once‑daily basal insulins with low rates of hypoglycemia. Because dosing frequency and pharmacokinetic characteristics may influence the pattern and duration of hypoglycemic events, this exploratory post-hoc analysis examined masked CGM and SMBG data from QWINT‑2, ‑3, and ‑4 to further characterize hypoglycemia duration, treatment patterns, and persistent‑recurrent hypoglycemia in adults with T2D.
- Study design. The analysis included participants from three phase 3 trials spanning populations who are insulin‑naïve or on basal‑switch or basal‑plus‑mealtime therapy. Each trial compared efsitora alfa with a once‑daily basal insulin (insulin degludec in QWINT‑2 and ‑3; insulin glargine U100 in QWINT‑4). Masked CGM sessions were conducted at prespecified intervals and were not used for dose titration. Hypoglycemic events were defined using standardized CGM‑derived thresholds: (i) combined level 1 and 2 events required ≥15 minutes <70 mg/dL with ≥15 minutes of recovery; and (ii) level 2 events required ≥15 minutes <54 mg/dL with ≥15 minutes of recovery. Persistent‑recurrent hypoglycemia was assessed using a prespecified SMBG algorithm. Investigator‑identified events were also captured.
- Results. Across all three trials, efsitora alfa and once‑daily basal insulins demonstrated a similar duration of CGM‑derived hypoglycemia. Median durations of combined level 1 and 2 events ranged from 40 to 42.5 minutes with efsitora alfa versus 40 minutes with comparators, while level 2 events ranged from 35 to 40 minutes with efsitora alfa versus 35 minutes with comparators. Most level 2 events were managed with oral carbohydrates or required no intervention. Level 3 events requiring IV glucose or glucagon were infrequent in both groups. Persistent‑recurrent hypoglycemia was rare in QWINT‑2 and ‑3, with slightly higher event counts in QWINT‑4 (19 participants with efsitora alfa vs. 9 with insulin glargine), though investigator‑identified events remained low across all arms. Together, these findings reinforce that once‑weekly efsitora alfa does not prolong hypoglycemia and maintains a safety profile consistent with daily basal insulin therapy in people with T2D.
Big Picture Highlights
15. ATTD 2026 exhibit hall brings together 80+ companies highlighting the latest in diabetes technologies and therapies
The exhibit hall at ATTD 2026 was buzzing with activity, with over 80 companies showcasing their latest innovations in diabetes technology and therapy. Throughout the day, the floor remained lively as attendees moved between booths, networking with colleagues and engaging with exhibitors between sessions. The space was filled with colorful displays, interactive demonstrations, and welcoming company representatives eager to discuss new innovations and answer questions. In addition to exploring new products, many attendees were treated to the delicious food and refreshments offered throughout the hall, making the exhibit area an environment to recharge and continue conversations sparked during scientific sessions.
- Beyond product demonstrations, several exhibitors also offered health-focused experiences directly on the exhibit floor, which proved particularly popular with attendees. iCare’s booth provided free AI-based retinal screening, giving participants the opportunity to quickly assess eye health using advanced imaging technology. A Lilly-sponsored health check screening station offered convenient on-site testing for LDL cholesterol, A1c, and lipoprotein(a) levels, adding a practical and engaging aspect to the exhibit experience. The Close Concerns team was especially excited to see these opportunities, and we look forward to exploring them further during the remainder of the conference!
- Eye-catching installations also helped create memorable moments throughout the hall, including the striking domes, which attracted steady interest from attendees who were curious to learn more about various companies presenting their products. Exhibit hall’s stable – coffee stations – and knowledgeable representatives across the booths contributed to the welcoming atmosphere, making the exhibit hall a vibrant extension of the conference’s collaborative and forward-looking spirit.

16. Breakthrough T1D to train interventional diabetologists and endocrinologists through US certificate program and joint course with ATTD
To a full room, Prof. Thomas Danne (Breakthrough T1D) introduced two new Breakthrough T1D initiatives aimed at redefining T1D care as an interventional discipline. Highlighting the shortage of endocrinologists in the US, Prof. Danne explained that endocrinology likely attracts less interest than specialties like cardiology and radiology due to fewer procedural interventions, hence lower reimbursement. With the current availability of the disease-modifying therapy Tzield (teplizumab) and potential cell therapies in the future, Breakthrough T1D is gearing up to approach T1D care from an interventional perspective, analogous to medical subspecialties such as interventional radiology and interventional cardiology.
- US certificate program in interventional diabetology. Breakthrough T1D and the American College of Diabetology are currently soliciting interest among US diabetes specialists for a certificate program in interventional diabetology. The aim of the program is to build clinical expertise in disease-modifying and islet cell replacement therapies to bridge immune science with real-world care. The program will have a hybrid structure, starting with a three-month virtual preparatory phase (readings, guideline reviews, pre-recorded lectures), followed by a three-day in-person phase at Breakthrough T1D’s headquarters in New York City (plenary sessions; case discussions; expert and peer engagement).
- BT1D-ATTD Course: Interventional Endocrinology in T1D. Breakthrough T1D and ATTD are also collaborating on an interventional endocrinology course for T1D. While not yet finalized, the course will recruit up to 30 pediatric and adult endocrinologists who are early in their careers for its inaugural class. Its core framework is based on four therapeutic components across the disease continuum, including: (i) immune interception (stages 1-2 T1D); (ii) precision monitoring; (iii) advanced management (stage 3 T1D); and (iv) future interception & cure strategies. The course will also feature an ATTD plenary, webinar series, and a two-day intensive course in Europe. Applications are open until April 30.
17. Delaying the onset of T1D: Screening and treatment options
In a packed afternoon session, panelists spotlighted screening and treatment options for T1D, especially given the well-known benefits of Tzield (teplizumab), the first and only FDA-approved for T1D delay. Dr. Michael Haller (University of Florida) started the session with an overview of T1D screening programs in the US, and Dr. Boris Kovatchev (University of Virginia) discussed whether CGMs could replace antibody screening. Dr. Desmond Schatz (University of Florida) then provided insights on screening recommendations for the general population, and Dr. Shweta Mital (University of Manitoba, Canada) concluded the session with cost-benefit analyses of screening and immune interventions.
- Dr. Haller on T1D screening programs in the US. Dr. Haller emphasized that practical outcomes drive screening programs, including fewer DKA at diagnosis, preparedness among patients and their caregivers, earlier access to disease-modifying treatments like Tzield, and meeting inclusion criteria for prevention studies. Screening programs in the US include three common archetypes, including: (i) relatives of people with T1D; (ii) population-based pediatric populations; and (iii) clinic-enabled diffusion. The common denominator across these programs includes a method for confirmatory testing, staged monitoring, and ultimately, the “what to do next” steps. Dr. Haller then highlighted protocols of major screening efforts across TrialNet, ASK, CASCADE, and PLEDGE. He also elaborated on Breakthrough T1D’s Early Detection Pilot Clinic Program, which aims to demonstrate the efficacy of T1D screening and monitoring in the real world. To date, nearly 4,600 individuals have been screened with 29 pilot clinic partnerships. Reflecting on the ongoing efforts in this space, Dr. Haller reminded that screening is no longer only for research and encouraged HCPs to standardize confirmatory testing, monitoring, and interventions through a shared decision-making process.
- Dr. Kovatchev on whether CGMs could replace antibody screening. Before turning the presentation slide, Dr. Kovatchev said the short answer to this question is “yes and no.” Antibody screening often misses 85-90% of future cases and is often limited to those with a family history. As an alternative, CGMs could be used for initial detection of dysglycemia, followed by differential diagnosis of T1D based on antibodies, with a potential opportunity for data integration across CGM metrics, antibody status, and demographics. Dr. Kovatchev referred to a 2014 study, which showed that CGMs could detect early hypoglycemia in children with positive autoantibodies at high risk of progressing to T1D. He also cited a 2025 study that studied whether CGMs could identify stage 3 T1D. Results showed that CGM metrics can accurately predict disease progression and classify an individual’s risk of developing T1D diagnosis along with other factors. As well, Dr. Kovatchev elaborated on a 2023 study, which concluded that CGMs could help identify people likely to progress to T1D, including those with a normal OGTT. Finally, given the plethora of evidence and emerging advances of AI, Dr. Kovatchev encouraged combining CGM and AI for the management of prediabetes.
- Dr. Schatz on recommendations for screening in the general population. Sharing key points from the 2026 ADA Standards of Care, Dr. Schatz reminded the audience of screening recommendations for children, adults, and those at high risk for T1D. He then questioned the field’s preparedness for public health screening, which includes the following criteria: (i) identification of a health challenge that’s recognizable in its early stage; (ii) a valid, reliable, and affordable test for determining eligibility for intervention; and (iii) availability of a cost-effective diagnosis and treatment. Given the increasing prevalence of T1D and its associated complications, Dr. Schatz emphasized the importance of screening more than ever before. Yet, Dr. Schatz also raised challenges, including false positives, inconvenient access, lack of intervention, and other factors among individuals. Dr. Schatz concluded with a firm statement that screening should be performed in relatives and those with a high genetic risk. For population screening, he said the wide-scale effort should begin with confirmation across cost-benefit analyses.
- Dr. Mital on cost effectiveness of screening and immune interventions. Dr. Mital presented findings from a 2026 cost-effective analysis on general population screening for T1D. General population screening at age four incurred an additional cost of $404,534 but led to the detection of 35 additional cases (per 10,000 children), yielding an incremental cost-effectiveness ratio of $11,383/case detected. General population screening at ages two and six increased the cost to $462,679, but it detected 18 more cases (per 10,000 children) at an incremental cost of $25,923/case detected. Findings showed that general population screening detects more children at risk of T1D, but it also incurs higher costs. Incremental costs per case detected were comparable to other screening initiatives in the pediatric population. Dr. Mital also shared results from a 2025 cost-effective analysis of immune therapies in delaying the initiation of AID systems in T1D. Among the strategies considered, ATG therapy followed by AID was the most cost-effective, with lifetime costs of $394,250 and approximately 19 QALYs – these costs were lower, and QALY gains were higher than strategies without immune therapy or AID. Tzield therapy followed by AID led to 0.25 additional QALYs compared with ATG therapy followed by AID, at an additional cost of $153,670. Overall, Dr. Mital concluded that the optimal strategy depends on payers’ ability to negotiate prices for Tzield and additional results on the efficacy of ATG in T1D prevention.
18. Bridging the gap between population screening and initiation of immunotherapy
In a late-afternoon session, Dr. David Maahs (Stanford) delivered a presentation on ways to address the gap between population screening and the implementation of immunotherapy. Dr. Maahs focused on how the field has advanced in translating T1D research into improved clinical care and emphasized that population screening and research on immunomodulation have advanced rapidly. With such progression, the question remains: How do we bridge from screening to immunomodulation? Furthermore, what are the gaps and needs? Dr. Maahs focused his presentation on explaining how to monitor individuals who screen positive and ensure they receive immunotherapy as soon as they need it with a stage 2 T1D diagnosis.
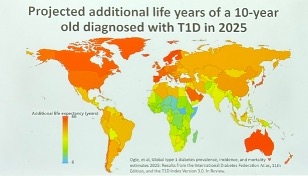
- The importance of T1D diagnosis. Dr. Maahs said that in 2025, an estimated 174,000 people died prematurely from T1D. Within this population, 46,000 are estimated to be <25 years old. Furthermore, 30,000 of the deaths in those under 25 years are estimated to include populations without a T1D diagnosis. The IDF and T1D Atlas estimate that the additional life expectancy of a 10-year-old child diagnosed with T1D varies across countries from six to 66 years. He said that these statistics underscore the need for greater awareness of early detection and diagnosis to improve health outcomes worldwide.
- The needs across HCPs, medical education, and clinical workflow. Dr. Maahs presented a list of needs to be addressed, including those of patients and their caregivers, as well as HCPs. Among primary care providers, he encouraged greater education and awareness about the signs and symptoms of T1D, complications, screening, and overall diabetes management. In the medical system, Dr. Maahs emphasized increased awareness of screening, as well as the use of OGTT and CGMs. For clinical workflows, Dr. Maahs suggested early detection through potential population screening, ongoing follow-ups, and timely initiation of immunomodulation treatment. Finally, he mentioned that national registries and care coordination that support clinical models will be critical for tracking at-risk populations, accelerating research, and ensuring appropriate guidance and treatment. Dr. Maahs also focused on the following needs of people with stage 1 or stage 2 T1D and their families: (i) reliable information; (ii) support from primary care physicians; (iii) T1D education; (iv) psychosocial and dietary support; and (v) access to T1D specialty care.
- Insights from the 4T study. As background, the 4T study integrated CGM data and telemedicine to improve T1D management, allowing HCPs to remotely monitor patients’ data for review and follow-up. In 2023, one-year results from the study showed that the integration conferred a 0.5% reduction in A1c, improved quality of life, and family and HCP satisfaction. Following these results, in 2024, a study prospectively assessed the impact of a systematic, equitable digital-healthcare team program with tighter glucose targets, early use of technology, and remote patient monitoring in young people with newly diagnosed T1D. The participants in the 4T study showed a mean A1c of 6.6%, and 64% of the population reached an A1c <7.0%. Additionally, the mean TIR was 68% at one year after T1D diagnosis. Given these results, Dr. Maahs encouraged the development of systems and processes for earlier screening and the implementation of treatments for people with stage 1 and 2 T1D.
19. Exercise and T1D: Physiological differences, clinical trials, real-world evidence, and continuous lactate monitoring
Drs. Michael Riddell (York University, Canada), Dessi Zaharieva (Stanford University), and Klemen Dovc (University of Ljubljana, Slovenia) tackled the complexities of exercise with T1D. Setting the stage, Dr. Riddell highlighted multiple physiological differences during exercise in people with T1D compared to healthy controls. For example, people with T1D have, on average, a 15% lower aerobic capacity/VO2 max, a 30% slower motor unit conduction velocity (i.e., slower reaction times), and a 20% lower muscle capillarization recruitment (i.e., muscles are being fueled with less oxygen). Despite these differences, Dr. Riddell emphasized that people with T1D can perform equally to those without diabetes, particularly when they maintain glycemic control and engage in higher levels of physical activity. At the same time, glycemic management during exercise in people with T1D remains a significant challenge due to differences in glucose metabolism. Specifically, sensitivity to insulin on board increases during exercise for people with T1D, which Dr. Riddell said is a real Achilles’ heel for closed loop algorithms. Additionally, glucagon levels increase during exercise in individuals without diabetes yet remain flat in those with T1D.
- Dr. Zaharieva reviewed findings from clinical trials and real-world studies for exercise and T1D, concluding that there are insights to be gleaned from both types of research. Exercise conditions, meal timing, insulin on board, environmental factors, and behavioral factors (e.g., stress, sleep, illness) are more controlled in clinical trials, allowing for higher quality data quality and a better mechanistic understanding of how exercise affects glucose levels. Meanwhile, real-world studies are much larger in sample size and more generalizable.
- Clinical trials have revealed insights such as the benefits of using an AID system’s activity feature compared to its automated mode. They have also shown that supporting resistance training with a mobile health app is safe and feasible, as well as reduce insulin requirements.
- Real-world studies such as the T1DEXI have shown that hypoglycemia risk is higher in conditions including longer exercise duration and higher insulin on board at exercise initiation. Other studies have shown that providing structured exercise education in youth with new-onset T1D is associated with better glucose outcomes.
- There are even studies with both controlled and real-world components, such as one that compared the accuracy of three CGMs during exercise.
- Dr. Dovc emphasized the importance of exercise for reducing morbidity and mortality. As background, cardiorespiratory fitness is the best predictor of morbidity and mortality. It can be measured during cardiopulmonary exercise tests, which assess the maximum rate of oxygen the body can consume during intense exercise (i.e., VO2 max). Studies have shown that even five minutes of moderate-to-vigorous physical activity a day can prevent death by 6-10%, and reducing sedentary times by 30 minutes a day can prevent death by 3-10%. Another study found that engaging in a variety of physical activity types (e.g., walking, cycling, swimming, yoga) can also reduce mortality. In Slovenia, there is also a national surveillance system for physical and motor development in youth called SLOfit.
- Dr. Riddell discussed lactate metabolism and potential benefits of continuous lactate monitoring during exercise. Prior knowledge of lactate suggested that it is a waste product that causes muscular fatigue and soreness. A newer theory suggests that lactate serves as both a signaling molecule in muscles for angiogenesis and memory formation, as well as a fuel source for muscle, heart, and brain cells. Additionally, lactate is now also known to be produced continuously – not just during intense exercise or other anaerobic conditions – and used in glucose production/blood sugar balance via the Cori cycle. A key metric that elite athletes have used to enhance performance is the lactate threshold. This corresponds to the point during a progressive exercise test where lactate concentration starts increasing more rapidly. A continuous lactate monitor would allow individuals to improve their capacity to burn fat, increase the mitochondrial function of skeletal muscle, and promote better glucose control by enhancing lactate transport between muscle fibers and the liver (i.e., the Cori cycle).
20. *NEW* Helmsley Charitable Trust Symposium: Protein intake before exercise can prevent hypoglycemia in people with T1D
In the first-ever Helmsley Charitable Trust session at ATTD, Ms. Deniz Dalton, Program Officer of Helmsley’s T1D Program, cogently introduced the Type 1 Diabetes and Exercise Initiative (T1DEXI), aimed at understanding how individuals with T1D can better manage glucose levels during exercise. The initiative took off in 2016, when Helmsley convened a think tank meeting to address this critical gap: although physical activity is a critical cornerstone of health, current technologies like AID systems do not handle exercise well, and the scientific evidence was limited to a few small, short clinical trials. Helmsley launched T1DEXI (n=750) to generate real-world data on a wide variety of exercises (e.g., high-intensity interval, resistance, aerobic, running, walking, gardening) in adults and children with T1D and shared them with researchers around the globe. In a series of talks, experts shared strategies to manage glucose during exercise in T1D.
- Dr. Dale Morrison (University of Melbourne, Australia) advocated for protein intake as an “untapped, practical tool” to prevent hypoglycemia during exercise in T1D. In people with T1D, glucagon secretion via beta cell signaling is impaired, leading to a higher risk of hypoglycemia during exercise. Encouragingly, protein ingestion directly stimulates glucagon secretion via alpha cells and indirectly through gut-derived incretins (see figure below). Indeed, in a study (n=12), whey protein ingestion increased plasma glucagon and glucose, with glycemic elevation sustained for over three hours with higher doses (0.5-0.75 g/kg).
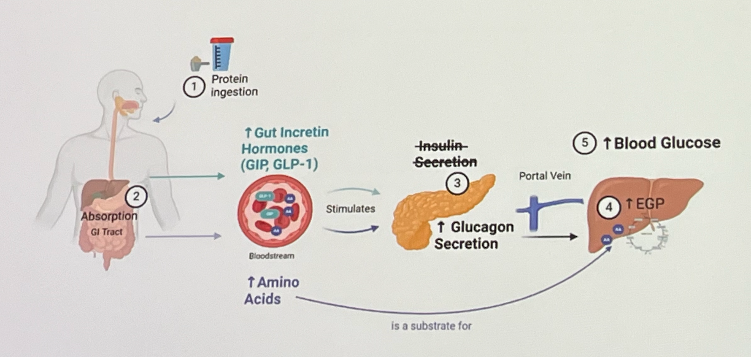
- In another study (n=29), adults using MiniMed 780G experienced fewer hypoglycemic events during a 60-min moderate-intensity cycling if they had a regular meal four hours before and a protein (0.5 g/kg) drink 30 minutes before the exercise. As shown in the figures below, glycemic level remained more stable during and after exercise in the protein group, compared to the control. The finding that protein intake reduces hypoglycemia was consistent across other scenarios, too, including: (i) high-risk conditions (n=21) when people had a meal two hours before exercise and had high insulin-on-board; and (ii) prolonged fasting during Ramadan (n=41).
- Dr. Morrison cited a survey, which found that 56% of people with T1D do not use protein in close proximity to exercise or going to the gym. Among those who do, the majority take protein after exercise (57% vs. 29% taking before) and reported that the primary purpose is to improve muscle building (46%) rather than managing glucose levels (20%). Thus, he emphasized that protein is a low-hanging fruit that is underused and can be implemented “now” to manage exercise in T1D.
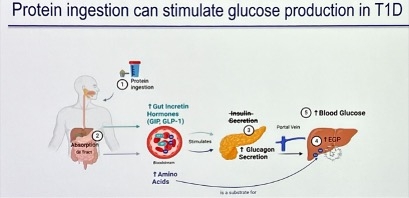
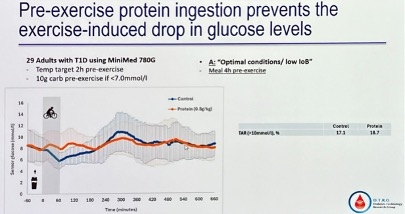
21. *NEW* Older adults and AID (automated insulin delivery): Choosing (and receiving!) the right technology at the right time for far better care
Drs. Yogish Kudva (Mayo Clinic) and Medha Munshi (Harvard University) offered perspectives on the use of AID for reshaping safe and effective diabetes care in older adults with T1D. The highly-regarded clinician/researchers agreed that AID can dramatically improve outcomes for older adults with T1D, and they also emphasized that adoption is best with intentional design around choice, tailored workflows for best teaching, and what they called “geriatric-informed” implementation. As people with T1D live longer and the population of older adults with T1D grows, the field will do well to pair strong efficacy data with equally strong strategies to ensure that older people with T1D can “win” and do very well with AID. There are risks, of course, that older people with T1D may not even be prescribed AID – this is tragic, of course, since AID so dramatically reduces the risk of severe hypoglycemia.
- Dr. Kudva presented growing evidence demonstrating that AID is not only feasible but also highly effective for older adults. Early trials based in the UK and Australia, as well as the US AIDE randomized crossover study (n=82), consistently showed that AID and predictive low-glucose (PLGS) systems substantially reduce hypoglycemia compared to sensor‑augmented pump therapy while also improving Time in Range (TIR), glycemic variability, and A1c.
- In the study, older adults >65 years of age achieved an A1c of 6.9% with fewer hypoglycemic incidents, a result that challenges the long‑standing ADA Standards of Care that includes a higher glycemic target of 7.5% in this population. In addition, 90% of participants chose to continue the use of AID in the extension phase, underscoring both its safety and uptake. We are curious, in fact, who the 10% are who did not choose this. He also highlighted new evidence from a trial (n=319) published in the New England Journal of Medicine in insulin‑treated people with T2D where AID reduced A1c by an additional 0.6 percentage points and increased TIR by 14 percentage points compared to CGM alone. This reinforces the expanding role of AID beyond T1D. As AID expands into T2D, Dr. Kudva emphasized the need for trials specifically to evaluate its use in older adults with T2D.
- Dr. Munshi discussed aging with T1D, grounding her perspective in the heterogeneity of older adults and the practical barriers that shape technology use. She illustrated how aging‑related changes directly affect patients’ ability to manage insulin pumps and AID systems. Real‑world challenges, such as remembering multi‑step infusion‑set changes, pressing small buttons, seeing alerts, hearing alarms, and managing supplies compound these risks. She gave several examples of patient cases that underscored this variability. Some older adults thrive with AID and value its flexibility, while others struggle with repeated errors, anxiety around decision‑making, or a lack of support. Dr. Munshi emphasized that these barriers are not simply individual shortcomings but predictable consequences of aging physiology and care environment complexity.
- Dr. Munshi said that the adoption of technology must be aligned with patient health status. Robust older adults may benefit from AID, while those with intermediate health or mild cognitive impairment may require simplified workflows, caregiver involvement, or CGM‑first strategies. She also stressed the need for the structured assessment of technological readiness, ongoing reassessment as health status changes, and intentional design choices like reduced manual bolus demands, accessibility‑focused interfaces, and clear caregiver pathways to support safe and equitable AID use.
22. *NEW* Dr. Anna Kahkoska on aging and menopause for patients with T1D
In a well-attended Thursday afternoon session, Dr. Anna Kahkoska (University of North Carolina, Chapel Hill) spoke on the challenges of growing older as a female with T1D. As treatments have improved dramatically, the average lifespan for people with T1D continues to increase. 16% of the global population with T1D is now estimated to be over the age of 65. Notably, women bear a higher burden of incident T1D cases compared to men in adult years, peaking in women aged 70-79 at 65.1 cases per 100,000 persons. With the global prevalence of T1D in women over 65 totaling an estimated 2 million (compared to 1.7 million in males), and a differential impact of CVD risk factors by sex despite more favorable cardiometabolic risk factor profiles (see figure below), studying mid- and later-life health outcomes for women with T1D is imperative for ensuring effective care.
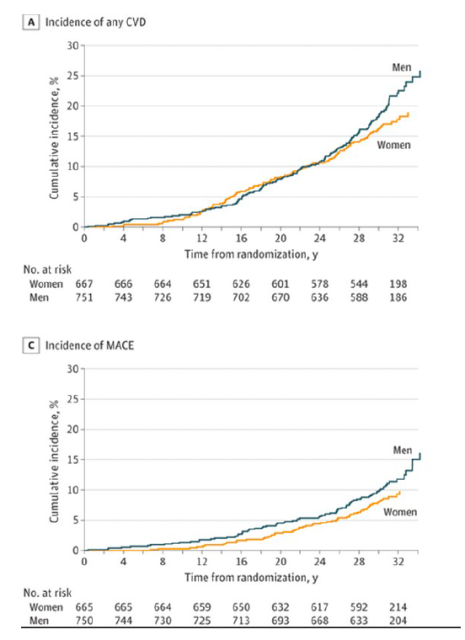
Adapted from "Cardiometabolic Risk Factors and Incident Cardiovascular Disease in Women vs Men With Type 1 Diabetes"
- Interestingly, menopause introduces an underreported level of complexity in T1D care. Across different studies, Dr. Kahkoska noted, women with T1D – and particularly those who were diagnosed at a young age or who have microvascular complications – appear to experience an earlier onset of menopause. In addition, perimenopause, the biological phase leading up to menopause, is characterized by cycle irregularity, fluctuating estrogen, and adverse metabolic changes, including: (i) changes in insulin resistance; (ii) development of dyslipidemia; (iii) increases in central and visceral adiposity; and (iv) endothelial dysfunction. Estrogen has been shown to improve insulin sensitivity, while progesterone can contribute to insulin resistance. The challenge of perimenopause for people with diabetes, Dr. Kahkoska explained, is that both estrogen and progesterone fluctuate without a clear pattern, leading to erratic and unpredictable glucose levels. Additionally, an overall decline in estrogen levels during menopause contributes to insulin resistance, further complicating clinical care.
- All the same, there is currently very limited evidence to guide optimal management of diabetes during menopause. As a result, clinical discussions around the phase of life are lacking. In a UK study, 30% of women reported that menopause was not addressed during their diabetes consultations, said Dr. Kahkoska. Therefore, she called on her peers to address gaps in the literature, which include: (i) focused studies to assess diabetes technology in perimenopause; (ii) longitudinal studies to characterize risk factors for early-onset menopause and trajectories of CVD risk factors through the menopause transition; (iii) large cohort studies to better characterize hormone fluctuations and implications for management; (iv) toolkits for clinician training and patient education; and (v) more evidence to optimize psychosocial T1D management during menopause.
-- by Riya Chatterjee, Kayla Mathieu, Elizabeth Rose, Paul Moon, Jeremy Alkire, Nour Khachemoune, Kat Moon, Esther Min, Elaine Young, Albert Cai, Monica Oxenreiter, and Kelly Close
[1] 100 mg/dL glucose target and active insulin time of two hours.
[2] Dexcom Smart Bolus’s core equation is: Total dose = carbohydrate coverage + correction + trend adjustment – insulin on board.
[3] Optimal settings for MiniMed 780G are: (i) glucose target of 100 mg/dL; and (ii) active insulin time of two hours.