ADCES Diabetes Technology Conference 2025 Day #1 Highlights –
Executive Highlights
- The Association of Diabetes Care and Education Specialists’ (ADCES) fifth annual Diabetes Technology Conference (DTC) kicked off in the heart of the Windy City at the Fairmont Chicago Millennium Park. From opening remarks to product theaters and hands-on sessions, we felt the warm energy from both speakers and attendees, all aiming to improve diabetes care and management for each patient. See here for what’s to come tomorrow!
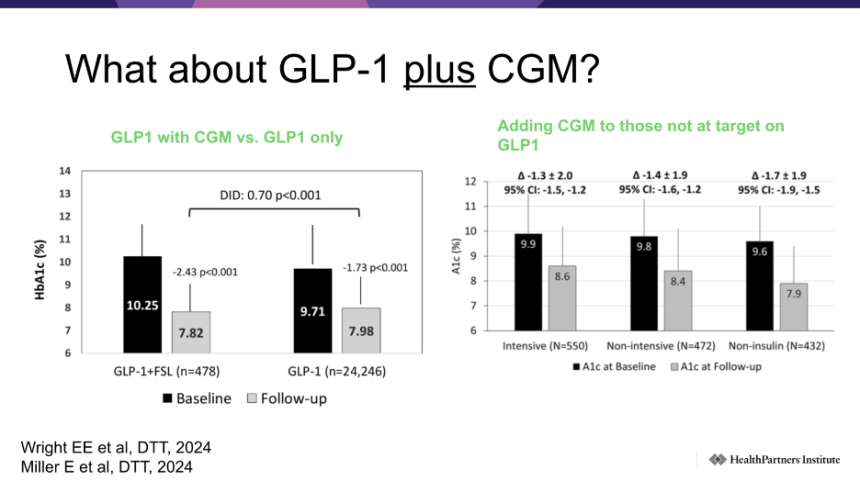
- Dr. Anders Carlson (International Diabetes Center) started the conference with a review of the current state and future of diabetes technology. On CGM, Dr. Carlson noted that technological advancements are enabling many people with diabetes on intensive insulin therapy to not only hit their TIR goals (70-180 mg/dL) but also aim for the even more stringent TITR. He also noted early success with CGM in people not using insulin, highlighting data from DT&T showing that CGM delivered an extra 0.6% A1c benefit in people with T2D already taking GLP-1 RAs. Looking at the future, Dr. Carlson highlighted three areas that were really interesting to him: (i) dual glucose and ketone monitoring devices (DGK); (ii) CGM in pregnancy; and (iii) CGM in prediabetes.
- CGM implementation and interdisciplinary team engagement were key focuses of the day. Ms. Caitlin Nass (University of Maryland Medical System) offered practical guidance on integrating CGM into clinical workflows, an area of major importance. She emphasized the need for consistent, basic CGM literacy across the care team, as simple as understanding how CGM differs from BGM. Dr. Morgan Stewart (UT Austin College of Pharmacy) drew on her experience as a pharmacist in an interdisciplinary diabetes care team to discuss how health systems can better integrate care responsibilities, including her perspective on who should “own” specific aspects of care while maintaining a multidisciplinary model.
- Several diabetes technology companies – Medtronic, Sequel, Insulet – hosted product theaters, each detailing the intricacies of their systems and optimal implementation strategies.
- Ms. Heather Lackey (Medtronic) led Medtronic’s afternoon product theaters, highlighting a range of system features and new sensor innovations. She reviewed the differences between Instinct and Simplera Sync, and examined recent real-world evidence from a global MiniMed 780G database, demonstrating that the strongest glycemic outcomes occur with its optimal settings.
- Sequel’s afternoon workshop was packed with almost double the number of attendees as chairs, with ADCES attendees eager to get hands-on experience with the twiist AID system. Led by Ms. Stephanie Taff (Sequel Associate Director of Medical Education) and Ms. Mary Harris (Sequel Medical Science Liaison), attendees learned how to adjust pump and app settings, review alert options, and tailor features to meet individual needs with twiist.
- Insulet hosted a dinner product theater highlighting the use of Omnipod 5 in adults with T2D. Dr. Katelyn O’Brien (Boston Medical Center) reviewed the clinical need for AID in people with T2D on insulin therapy, with 85% of those with T2D on MDI having an A1c >7.0% and nearly 60% have an A1c >8.0%, positive findings from the SECURE-T2D trial (which Dr. O’Brien said closely mirror her clinical experience), and the glycemic benefits of using Omnipod 5’s optimal settings.
Chicago remains the backdrop to ADCES’s winter technology conference.
Conference Website | Agenda | Registration
Table of Contents
-
Top Highlights
- 1. Dr. Anders Carlson reviews successes, challenges, and the future of diabetes technologies
- 2. MiniMed 780G product theaters spotlight new Simplera Sync and Instinct CGM options, real-world evidence supporting optimized settings use
- 3. Insights from Omnipod 5 and SECURE-T2D: Expanding access to AID
- 4. Clinical overview of AID systems, including practical approaches with the PANTHER program and CARES framework
- 5. Practical guidance on making CGM implementation work in the real world
- 6. Building efficient diabetes technology workflows across the care team
- 7. Sequel offers a hands-on workshop to demonstrate the differentiating features of the twiist AID system
- 8. Back to school: A step-by-step guide on interpreting AID reports
Top Highlights
1. Dr. Anders Carlson reviews successes, challenges, and the future of diabetes technologies
Kicking things off on Friday morning, Dr. Anders Carlson (International Diabetes Center) set the stage for the rest of the conference with a review of the current state and future of diabetes technology. To kick things off, Dr. Carlson noted that the state of the art diabetes technology changes quickly, and his slides, which he updated just a couple of weeks ago, were already outdated with last week’s release of the latest 2026 ADA Standards of Care.
- Recent successes in diabetes technology have come from AID and CGM, as the two technologies have enabled large improvements in both glycemic and psychosocial outcomes, especially in T1D. Dr. Carlson also highlighted the early but growing evidence base surrounding the use of AID systems in T2D, sharing data from Insulet, Tandem, and Medtronic.
- On the CGM side, Dr. Carlson discussed similar themes, starting with the profound impact that CGM has had on people on intensive insulin therapy. With the power of CGM, Dr. Carlson urged providers and educators to help their patients go from “possible to physiologic,” noting that these technology advancements are allowing people with diabetes to not only hit their Time in Range goals (70-180 mg/dL) but aim for Time in Tight Range (TITR; 70-140 mg/dL), glucose levels which are closer to those of people without diabetes. Dr. Carlson also noted early success with CGM in people not using insulin, highlighting data from DT&T showing that CGM delivered an extra 0.6% A1c benefit in people with T2D already taking GLP-1 RAs. Finally, Dr. Carlson even expressed excitement about new over-the-counter CGMs (Abbott’s Lingo and Dexcom’s Stelo), though he also shared a gentle warning that the release of these devices into the broader market would require some meaningful education education. Dr. Carlson shared an anecdote about a healthy patient who had tried an over-the-counter CGM and been scared into thinking they had diabetes when their glucose levels fluctuated slightly after eating, a story which drew some understanding laughs from the audience.
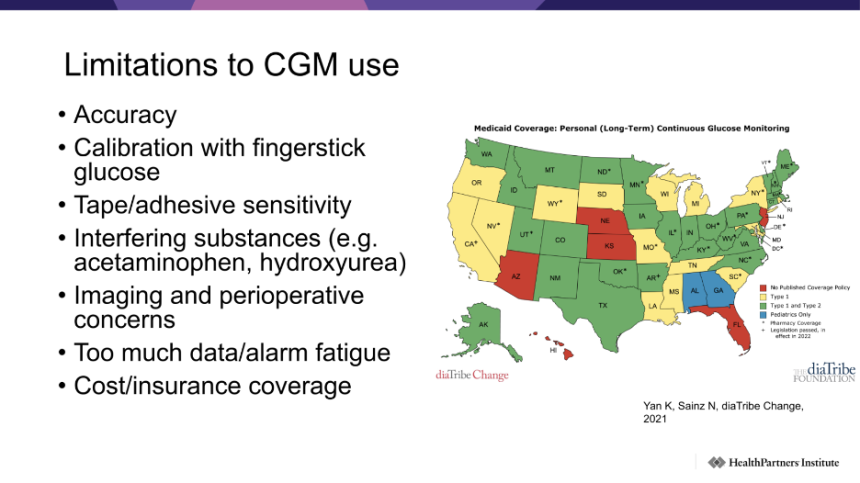
- On the challenges side, Dr. Carlson noted that disparities in adoption and access issues remain critical barriers. For example, Dr. Carlson expressed his frustration that, as a provider with patients in both Minnesota and Wisconsin, differences in state-to-state Medicaid coverage meant that he cannot offer his Wisconsin patients the same tools and devices that he could to his Minnesota patients. On the adoption side, Dr. Carlson highlighted some of the unique challenges to CGM adoption faced by older adults (well-synthesized in a 2023 paper by Dr. Medha Munshi), including dexterity to insert sensors every 10-14 days, visual and hearing impairment, and data overload.
- Looking at the future, Dr. Carlson highlighted three areas of keen interest (i) dual glucose and ketone monitoring devices (DGK); (ii) CGM in pregnancy; and (iii) CGM in prediabetes. On the ketone monitoring side, Dr. Carlson noted that many people have been waiting to use SGLT-2 inhibitors in people with T1D in the US for a long time (SGLT-2 inhibitors have been approved for use in people with T1D in Europe since 2019), something that could be unlocked with a reliable continuous ketone monitoring device that could mitigate DKA. Ultimately, Dr. Carlson encouraged multiple new use cases for CGM, highlighting the recent consensus statement from EASD 2025 and the potential for CGM to provide a better understanding of and treatment for prediabetes, a metabolic state that continues to be plagued with murky guidelines and definitions.
2. MiniMed 780G product theaters spotlight new Simplera Sync and Instinct CGM options, real-world evidence supporting optimized settings use
Ms. Heather Lackey (Medtronic) led Medtronic’s MiniMed 780G product theaters this afternoon, reviewing its product features, sensor updates, and body of clinical and real-world evidence, with particular emphasis on use with optimized settings.
- A breadth of clinical evidence supports outcomes using the system. In pivotal trials, such as that of Simplera Sync with an extended infusion set in adults aged 18-80 years, users of MiniMed 780G saw an overall 14% increase in TIR. In children aged 7-17 years, users of MiniMed 780G experienced an overall 17% increase in TIR. MiniMed 780G has also demonstrated efficacy in the T2D population, with clinically significant improvements in A1c, TIR, and TAR, and no increase in hypoglycemia. Among study participants, 63% had no prior pump or CGM experience, suggesting a smooth transition to MiniMed without prior technology experiences. Importantly, benefits were observed without significant changes in weight or BMI.
- Real-world evidence reinforces consistent outcomes across MiniMed 780G users, particularly those using optimized settings. The latest real-world study featuring nearly 440,000 users found mean 72% TIR across all users, including 47% TITR and an average GMI of 7.0%. Among those using the recommended settings (100 mg/dL glucose target[1] and 2-hour active insulin time [AIT]; n>73,000), however, TIR jumped to 78%, driven by an increase to TITR (53%), and GMI was 6.8%. US-specific data showed very similar outcomes, with 72% TIR and 78% TITR with the recommended settings. Why isn’t everyone using these settings then? Ms. Lackey suggested many don’t because of fear of hypoglycemia with the two-hour insulin target, though such fears are not supported by the data. She recommended showing individuals like this that Time below Range with the two-hour target is actually lower than that with longer active insulin times. Ms. Lackey said that all patient settings can be checked in CareLink reports, under “Device Settings Report” or “Assessment and Progress Report.”
- In 2024, additional real-world data showed that MiniMed 780G users achieved a 91% TIR overnight and an additional 36 minutes per night without alarms and alerts. These results demonstrate how the MiniMed 780G enables users to experience fewer interruptions during sleep and facilitates better glycemic management through autocorrections. Decreased sleep interruptions can help reduce the nighttime burden, especially since children with T1D often experience shorter sleep durations, and adults with T1D report poorer sleep quality.
- Ms. Lackey highlighted recent sensor innovation from Medtronic, with Guardian 4 being succeeded by (though the sensor remains available) the Simplera Sync and Instinct sensors. She reviewed both sensors’ details:
- Simplera Sync, about the size of a quarter, has launched in the US with a seven-day wear time. It features a two-hour warmup period and is recommended to be worn anywhere on the body. The sensor can be linked directly to the pump.
- Instinct, which is made by Abbott for exclusive use with MiniMed 780G, has been cleared by the FDA and entered full commercial launch in the US at the beginning of this month. It is about the size of a penny, has a 15-day wear time, a one-hour warmup period, and is recommended to be worn on the same side of the body as the insulin pump (not necessarily the infusion site). The pairing for Instinct is done with a smartphone, and if a user doesn’t have a compatible device, a “locked-down” one will be provided for users to be able to access the app. Sample Instinct sensors were made available for attendees to practice insertion on a Lenny stuffed animal, the same process used by Simplera Sync featuring a simple “press and release” functionality.

- Ms. Lackey also reviewed Medtronic’s extended one-week infusion set that can be used with MiniMed 780G’s extended reservoir. After years of telling patients that they must change infusion site once every three days, she recalled being pleasantly shocked upon seeing the data that the site did not “burn” after a week of wear. She explained that the infusion set’s design has been key to success. This includes: (i) extended wear connector/cap that improves insulin stability and infusion set site performance; (ii) extended wear tubing that improves insulin preservative retention and stability; and (iii) extended wear adhesive patch that improves adherence to skin.
3. Insights from Omnipod 5 and SECURE-T2D: Expanding access to AID
Dr. Katelyn O’Brien (Boston Medical Center) hosted Insulet’s product theater on Omnipod 5 use in T2D. She was joined by an engaged audience, about half of whom were first-time ADCES DTC attendees, though most reported some familiarity with Omnipod 5. She recalled that attending her first DTC helped her become a “diabetes technology champion,” and noted that attendees were on a similar trajectory for their own clinical practices.
- There is a clear need for AID in people with T2D. Dr. O’Brien highlighted that many people with T2D on MDI are not meeting glycemic targets: 85% have an A1c >7.0% and nearly 60% have an A1c >8.0%. The ADA has recently strengthened its support for insulin pump technology in the latest Standards of Care, now recommending AID as the preferred insulin delivery method for T1D and adults with T2D and adding a new level B recommendation to consider AID for adults with T2D on basal insulin who are not meeting goals. Anecdotally, she shared that she started a patient on basal-only insulin on AID just one week ago, and already their total daily dose has decreased and TIR has improved. The goal, ultimately, is to transition more patients onto this technology that improves outcomes.
- Dr. O’Brien reviewed findings from the SECURE-T2D trial (n=305), which closely mirror her clinical experience. Nearly half of participants were Hispanic or Black, many had high baseline A1c, one-third had a high total daily insulin dose (≥100 units/day), more than half were on incretin therapy, and perhaps most compelling, 84% did not carbohydrate count prior to the study. Importantly, these baseline characteristics did not limit system success:
- A1c reduction: Participants with baseline A1c ≤6.9% had similar mean A1c at study end, but she emphasized that this does not mean the system should not be offered to them. Those with the highest baseline A1c experienced the greatest improvement, with reductions exceeding 2%;
- Mean total daily insulin dose decreased by 29%, from 80 units to 57 units, with minimal weight gain (+0.8 kg from a baseline of 99.7 kg). Reductions in insulin dose were sustained throughout the study; and
- TIR increased from 45% to 66%, with improvements maintained over time.
- Dr. O’Brien emphasized use of Insulet’s optimal settings, which include the 110 mg/dL glucose target. In real-world use, lowering glucose targets from 150 mg/dL to 110 mg/dL showed TIR improvements by 10%, and even lowering from 120 mg/dL to 110 mg/dL improved TIR by 3%. Additional real-world evidence showed that even users with fewer than one bolus per day achieved 62% TIR at the 110 mg/dL target; however, carbohydrate counting remained beneficial, with those delivering more than four boluses per day achieving 74% TIR, underscoring the continued importance of behavioral interventions. Simplified carbohydrate entries (clinician-entered custom foods that simplify carbohydrate input by meal or portion size) also nearly achieved glycemic targets, with mean TIR reaching 69%.
- Dr. O’Brien concluded by outlining how to initiate pump therapy using the Omnipod 5 order form, an online tool requiring only two inputs: patient weight and current total daily dose. The form automatically generates recommended settings, including insulin-to-carbohydrate ratio (using the 400 rule) and correction factor (using the 1700 rule), and Dr. O’Brien recommended aligning the “correct above” feature with tiered glucose target (e.g. 110 mg/dL for the 110 mg/dL target). She also recommended considering turning reverse correction off. At follow-up, she advised clinicians to adjust settings as needed, including modifying the insulin-to-carbohydrate ratio to the 350 rule or the correction factor to the 1,500 rule.
4. Clinical overview of AID systems, including practical approaches with the PANTHER program and CARES framework
Ms. Cari Berget (University of Colorado) took the stage this morning to present a clinical overview of AID systems, along with a practical approach with the PANTHER program. Across diabetes care and education specialists, Ms. Berget has led the PANTHER program, based at the Barbara Davis Center for Diabetes, to provide educational resources for diabetes management. This program continues to evolve with essential tools to guide clinicians working with diabetes technology. The PANTHER program simplifies: (i) information about AID devices; (ii) data interpretation and optimization; and (iii) education for people with diabetes. Ms. Berget took a deep dive into each of these approaches by reviewing the clinical considerations of AID systems, the CARES framework, and finally, underscoring data interpretation for educational purposes.
- An overview of AID systems across clinical evidence. Ms. Berget called AID a “huge advancement,” emphasizing the technology’s ability to predict future glucose levels based on various factors. Presenting a slide with pivotal trials of AID systems widely used in T1D, Ms. Berget said the goal is not to compare different algorithms. Rather, she highlighted the similar outcomes in TIR and A1c levels in both children and adults. Given that the degree of TIR improvement represents relative changes, depending on age, baseline TIR and A1c levels, and behaviors (e.g., percent time in automation and bolusing), Ms. Berget encouraged the focus on individual experiences to understand glycemic outcomes. For example, individuals with a higher baseline TIR are likely to experience a higher TIR after AID use, but less relative improvement; those with a lower baseline TIR are likely to experience a lower TIR after AID use, but more relative improvement.
- The importance of personalization in device selection. Building on the point about relative outcomes, Ms. Berget addressed the act of balancing benefits and burdens when selecting a device. She said, “The best AID system is the one the person wants to use.” Patients will sustain the use of the device if the benefits outweigh the burdens, and therefore, the ease of use is as important, if not more important, than the algorithm itself. Other features to consider in device selection include device type (e.g., cell phone, CGM preference, remote data sharing options), form factor (e.g., size and shape of the pump), customizability (e.g., inputs), and practicality (e.g., cost, insurance coverage, insulin cartridge size).
- The PANTHER program approach integrates the CARES framework. Ms. Berget discussed leveraging the PANTHER program’s CARES framework to help clinicians streamline adjustment of AID systems with: (i) calculating insulin delivery; (ii) adjusting settings for pumps; (iii) reverting automated to manual mode; (iv) educating patients and caregivers; and (v) sharing remote data and determining compatible sensors. She also shared an AID comparison chart available online, which uses the CARES framework and summarizes key clinical information about AID devices. PANTHERTOOLS also includes detailed overviews of individual devices, as well as education for users and clinicians, to help optimize diabetes outcomes. Finally, Ms. Berget shared educational handouts for skin solutions, which provide tips on device placement and strategies to prevent skin irritation from specific devices.
5. Practical guidance on making CGM implementation work in the real world
Ms. Caitlin Nass (University of Maryland Medical System) offered practical guidance on integrating CGM into clinical workflows. She emphasized the need for consistent, basic CGM literacy across the care team, as simple as understanding how CGM differs from BGM. She noted that while patients can manage CGM independently, they shouldn’t be expected to; clinics need dedicated time and clear responsibility for CGM education. The benefits of CGM are broad-based and its use by all people with diabetes has been supported with increasing recommendations in the ADA’s Standards of Care.
- Real-world evidence on CGM use has shown reductions in all-cause and diabetes-related hospitalizations in the six months before vs. 12 months after CGM prescription. For example, Ms. Nass reviewed a study in which all insulin-using groups experienced significant decreases in acute healthcare utilization, with the greatest benefit in intensive insulin users. She said that these findings align with expectations that more information and safety alerts would both save lives and reduce healthcare costs.
- When discussing remote sharing options for providers, Ms. Nass explained that free options are cost-effective and provide the same data but require more training, which can be challenging for busy clinics with high turnover. Subscription platforms (such as Glooko or Tidepool) may or may not be worthwhile depending on the number of patients seen using CGM and insulin pumps. On a clinic’s overall CGM implementation plan, she said clinicians must define their own strategy for accessing and sharing CGM data. She asked the audience to consider their business case for CGM: are you seeking to expand access for GDM, improve HEDIS measures, or generate revenue? Keeping desired outcomes clear, she said, helps cultivate new “diabetes enthusiasts” and ultimately moves forward your collective mission.
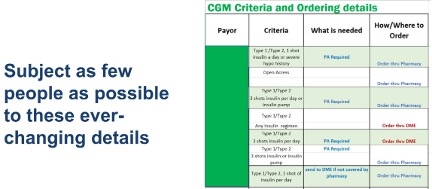
- Coverage is complex but essential to understand when initiating CGM prescribing. As Medicare varies by state, Medicaid orders through DME, and most commercial plans use pharmacy benefits, she noted that it makes sense CGM coverage remains difficult to navigate for those outside endocrinology. She showed a spreadsheet she often uses in her Maryland practice outlining CGM criteria and ordering requirements (see figure below), which she said is constantly changing but crucial for at least one person to track and understand. She added that she still prescribes through DME for many patients and recommended Parachute Health, an integrated ordering platform that simplifies documentation and interfaces with most DME suppliers, to ease that ordering practice.
- Ms. Nass was also an advocate for the use of professional CGM. She said she routinely used 14-day professional sensors to engage patients new to the technology and said she would return to them if free samples became scarce. While the ADA Standards of Care contain less robust data on professional CGM compared to real-time CGM, she said she remains “a believer” in its efficacy.
- She reassured clinicians that AGP reports are easier to review with patients than they may expect; patients intuitively understand the color-coding and TIR logic. As some still argue over the best target range for patients, she encouraged clinicians to tailor the consensus-driven 70-180 mg/dL range — for example, she does not recommend certain patients go <100 mg/dL — and incorporate individual recommendations into patient education. She also stressed the importance of looking beyond the summary view to specific trends in highs and lows. Although patients generally have low-glucose alarms, very low TBR may indicate that they are catching and treating lows quickly. Identifying whether these patterns relate to meals, exercise, or medications is key, and she encouraged clinicians to engage patients in documenting their insulin, carbohydrates, and activities to enhance these insights.
- Ms. Nass noted persistent disparities in CGM access rooted in broader social and healthcare structures and highlighted the impact of simple interventions like CGM samples. She described a pediatric team at Hopkins that conducted the IMPACT study, in which after trial CGM use, 85% of participants reported wanting personal CGM, and at three to six months follow-up 76% had obtained one and 43% were using a personal CGM. She also cited the CUT-DM study in a Spanish-language diabetes education program, where half of the participants also received CGM. All participants saw A1c reductions at 12 weeks – as nature of the diabetes education – with CGM users experiencing substantially greater improvement (1.3% with education alone vs. 2.5% with CGM as well).
6. Building efficient diabetes technology workflows across the care team
Dr. Morgan Stewart (UT Austin College of Pharmacy) drew on her experience as a pharmacist in an interdisciplinary diabetes care team to discuss how health systems can better integrate care responsibilities. She emphasized that when team members lean on one another, efficiency increases and both care quality and patient outcomes improve. Depending on resource constraints, teams may or may not have access to all roles, and the comfort level with diabetes technology varies across settings (e.g., endocrinology vs. primary care). Training should reflect these differences. In her clinic, for example, front-desk staff receive additional training so they can effectively communicate patient questions on pump or sensor questions to the prescriber — for example, being able to clarify what device a patient was discussing on the phone with them rather than referring to it as a “glucose thingy.” Once these integrated teams are in place, she noted, clinics often see increased CGM adoption and corresponding A1c improvements as they can better harness the “data galore” offered by CGM technology.
- She highlighted that the ADA Standards of Care align with this approach. Recommendation 4.2 underscores the importance of coordinated interprofessional teams to support diabetes technology implementation. This includes medical assistants, care managers, community health workers, pharmacy technicians, and IT personnel. The Standards also emphasize ensuring that patients, particularly those on intensive insulin therapy, have access to HCPs with diabetes technology expertise. Additionally, the ADCES ICC (Identify, Configure, Collaborate) framework provides a strong structure to optimize technology-enabled care through: (i) identifying appropriate candidates; (ii) engaging them in preference-based conversations; and (iii) integrating the full care team in follow-through.
- Dr. Stewart also offered her perspective on who should “own” specific aspects of care while maintaining a multidisciplinary model, while still promoting the multidisciplinary model of diabetes care itself.
- Identifying candidates: A shared responsibility across the team, though typically led by the prescriber;
- Submitting orders: Prescribers and pharmacists with prescribing authority. For PCPs unfamiliar with device ordering, smart sets can ensure they request all necessary components;
- Ensuring payer coverage: While medical assistants and nurses are also involved, Dr. Stewart spotlighted the critical and often undervalued role of pharmacy technicians. She described how her clinic’s technician independently identified more than 200 patients denied CGM coverage and secured the correct documentation so they could receive their sensors;
- Patient education: Beyond education being provided by prescribers, pharmacists, dietitians, and nurses, she identified local CGM representatives as additional resources to support device-specific training;
- Downloading data: Medical assistants, nurses, dietitians, and pharmacists;
- Data interpretation: Although often assumed to be the prescriber’s role, clear clinic protocols can empower CDCES nurses and dietitians to review data and adjust therapy between visits;
- Troubleshooting and addressing barriers: Well-suited for community health workers, social and behavioral health workers, and company representatives;
- Ensuring consistent follow-up: Shared across the team, but typically led by care coordinators, front-desk staff, and medical assistants; and
- Optimizing workflow: Coders and IT personnel can help ensure appropriate reimbursement.
- Dr. Stewart also facilitated table discussions where attendees shared interdisciplinary care strategies from their clinics. Participants highlighted team members they already rely on, such as technology coordinators who help clinicians understand devices or pharmacist-CDCES integrated teams where CDCESs identify candidates, pharmacists sign orders, and CDCESs provide education. Several attendees praised the ordering software Parachute for making DME CGM ordering “as easy as Amazon.” Others identified new roles they plan to engage more deeply, such as pharmacy technicians who can flag patients struggling to pick up CGM prescriptions between visits.
- Ultimately, Dr. Stewart advocated for simple solutions that maximize workflow efficiency rather than those that reinvent the wheel. This may mean brief team huddles at the start of the day or reviewing patient lists the day before. As with any workflow change, she emphasized the importance of monitoring progress and outcomes to understand what works.
7. Sequel offers a hands-on workshop to demonstrate the differentiating features of the twiist AID system
Sequel’s afternoon workshop was packed with almost double the number of attendees as chairs, with folks eager to get hands-on experience with the twiist AID system. Ms. Stephanie Taff (Sequel Associate Director of Medical Education) and Ms. Mary Harris (Sequel Medical Science Liaison) introduced the session with an informative video on the unique features of twiist that help personalize diabetes management with flexibility. Based on the PANTHER program’s CARES framework, twiist provides: (i) calculation and adjustment of basal rates every five minutes based on a six-hour predicted CGM glucose, with a wide correction range set between 87-180 mg/dL; (ii) adjustment of pre-meal preset to lower correction range up to one hour before meals and workout pre-set to raise correction target for exercise; (iii) reversion to programmed basal rates when twiist loses connection with CGM for more than 15 minutes; (iv) selection of carb absorption emoji that best fits meal for pre-bolus and bolus meals for missed meals; and (v) integration with CGM data across FreeStyle Libre 3 Plus and Eversense 365, along with an application for remote data sharing.
- Hands-on experience to adjust pump and app settings, review alert options, and tailor features to meet individual needs. Attendees were able to experience various features of twiist at each table, which had three sets of an iPhone, iPad, and Apple Watch, along with twiist. Ms. Taff and Ms. Harris presented a case study of a 36-year-old woman who has been living with a 15-year-old woman and using an AID system for four years. With engaging scenarios, like the patient preparing for her lunch and other meals throughout the day, attendees were able to receive training on how twiist supports daily management of insulin delivery. Specific topics that were covered include the pre-meal preset, which reduces post-meal glucose spikes, and the carb entry bolus, which uses different emojis categorized by fast, medium, and long duration food absorption. Finally, attendees gained experience with retrospective carb entry, one of the major aspects of twiist that helps people with diabetes provide more accurate information to adjust their basal rate and aim for the correction range.

8. Back to school: A step-by-step guide on interpreting AID reports
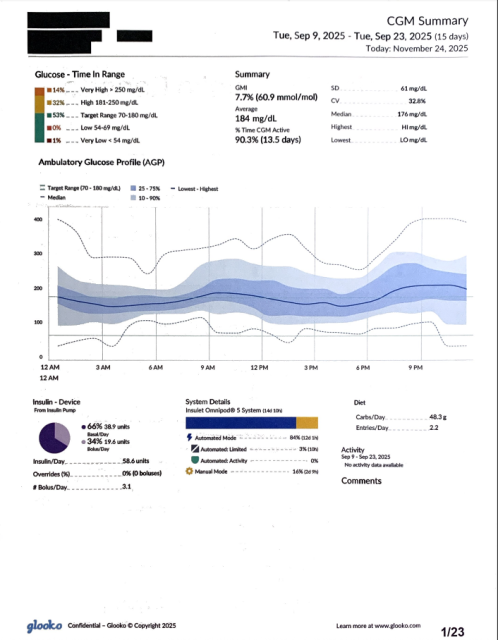
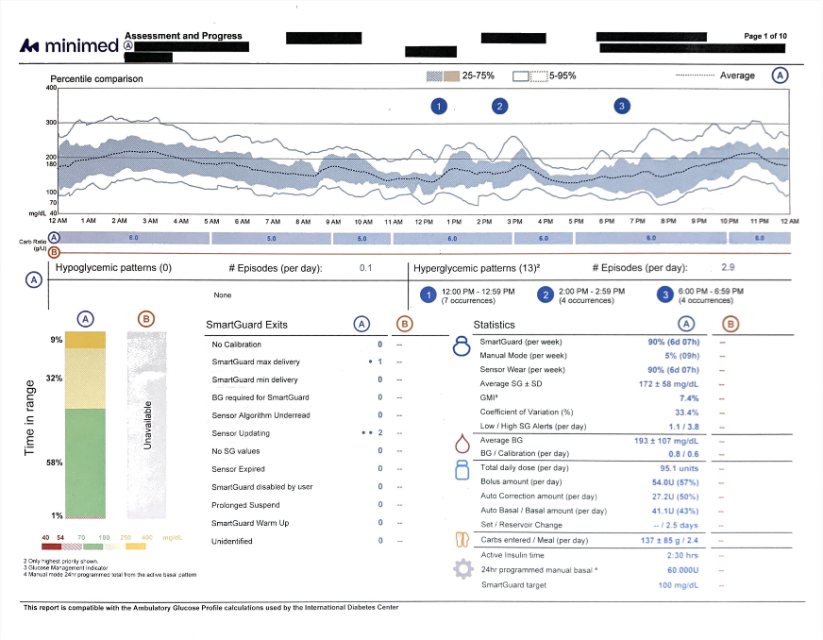
To close out Friday’s sessions, Ms. Cari Berget (Barbara Davis Center), Dr. Diana Isaacs (Cleveland Clinic), and Ms. Emily Boranian (Barbara Davis Center) walked attendees through an interactive session on reviewing AID reports from all the major AID systems available in the US. The instructors taught audience members to analyze downloaded reports from real-world users of each system, starting with the “Big Picture,” then the “Small Picture,” and finally the “Plan.” For each report, audience members were given two minutes to start with the “Big Picture,” considering the percentage of time the AID system was in closed loop, as well as primary glycemic metrics (e.g., TIR), and glucose patterns. Then, audience members assessed the “Small Picture,” considering the glycemic patterns identified in the more detailed weekly reports, and finally the “Plan,” creating specific points for adjusting insulin pump settings or providing education to patients.
- During the sessions, we were struck by the differences between the AID reports. As the session was aptly titled, “AID Speed Dating,” attendees were asked to rapidly go between different systems’ AID reports (Medtronic 780G, Insulet/Glooko Omnipod 5, Tandem Control-IQ, Sequel twiist, and Beta Bionics iLet). Small differences between the various manufacturers’ reports meant that it took some time to determine details such as the average number of meal boluses delivered per day, as they were located in different parts of the page and described using different language. While CGM manufacturers have broadly adopted the standardized ambulatory glucose profile (AGP) for reporting CGM data, AID systems have not reached the same level of standardization. To that end, we are reminded of Drs. Viral Shah and Satish Garg, who proposed a standard “artificial pancreas dashboard” back in 2020.
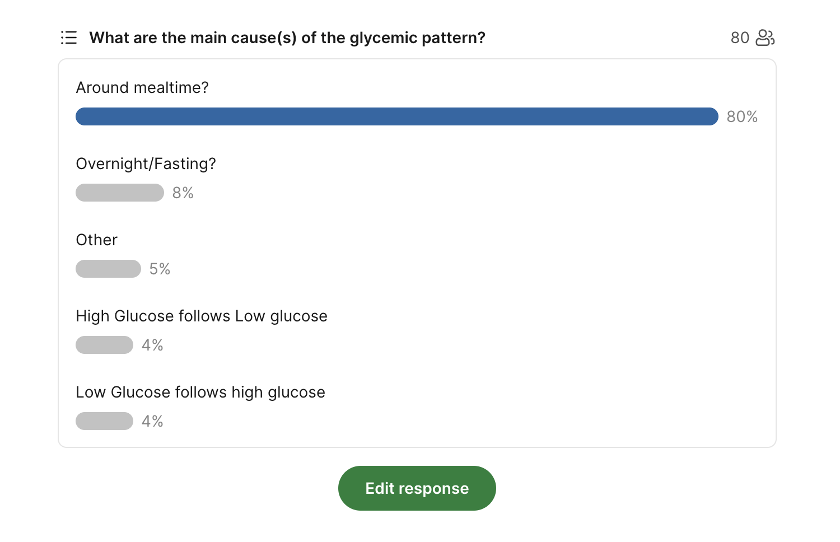
- Despite the heterogeneity in the reports, audience members were largely in agreement with their assessment of the AID data. For example, in the case study of an Insulet Omnipod 5 user, 80% of audience members agreed that mealtime hyperglycemia was the primary driver of suboptimal glycemic management. Of course, attendees of the conference are likely to be more engaged in diabetes technology than the typical diabetes educator; nonetheless, we were impressed by their ability to navigate the differing reports and quickly (in a “speed dating” fashion) identify consistent patterns for improvement and education.
-- by Jeremy Alkire, Esther Min, Albert Cai, Monica Oxenreiter, and Kelly Close
[1] For patients 7-15 years old, it is recommended to start at 110 mg/dL, and move down to 100 mg/dL when the prescriber feels there is low risk of hypoglycemia.