EASD 2025 Full Report –
Executive Highlights
- We were grateful to have the opportunity to gather in Vienna, Austria’s Congress & Convention Center alongside over 13,500 other participants excited to learn about the latest breakthroughs and engage in inspiring discussions in the diabetes field. There were more than 1,300 general abstracts, 96 late-breaking abstracts, and 50 lectures. We applaud EASD on organizing such invigorating discussion and reflections on data, therapeutic and technological innovations, and social determinants of health, and we’re already looking forward to attending next year’s conference in Milan, Italy, from September 28-October 2.
- On T1D cures and management, EASD 2025 was packed with insights on disease‑modification and comorbidity risk reduction in people with T1D. In an overcrowded spotlight session highlighting benefits of GLP-1 RAs in T1D, Dr. Petter Bjornstad (University of Colorado) explained that in the ADJUST‑T1D trial A1c dropped 0.7% with semaglutide (vs. 0.3% with placebo), and Dr. Jennifer Snaith (Garvan Institute of Medical Research) reported that ≥5% and ≥10% weight loss was achieved in all and 45% participants on tirzepatide, respectively, in the TIRTLE‑1 trial of tirzepatide in T1D. On modifying the progression of T1D, Dr. Michaela Waibel (St. Vincent’s Institute of Medical Research, Australia) presented two-year outcomes from the phase 2 BANDIT trial, which found that baricitinib 4 mg/day significantly preserved mixed‑meal‑stimulated C‑peptide at Week 48 versus placebo (p=0.001) with accompanying reductions in insulin requirement and early improvements in TIR.
- The cardiovascular benefits of incretin-based therapies took the spotlight at EASD 2025. The long-anticipated phase 3 SURPASS-CVOT (n=13,165) readout drew thousands of attendees in person and online, showing that tirzepatide significantly reduced the all-cause death by 16% and significantly reduced the risk of composite kidney endpoint by 19% overall and 22% in the high-risk population. Novo Nordisk shared results of the REACH real-world study (n=58,336), which found that semaglutide was associated with 23% reduced risk of three-point MACE (ischemic stroke, MI, and all-cause death), compared to dulaglutide (p<0.001). Furthermore, full results of the phase 3 ATTAIN-1 trial showed that orforglipron 36 mg, 12 mg, and 6 mg conferred 12%, 9%, and 8% weight loss, compared to 0.9% with placebo, in people with overweight or obesity. Positive weight loss results from Jiangsu Hengrui Pharmaceuticals’ dual GLP-1/GIP RA HRS9531, Zealand’s once-weekly dual GLP-1/GLP-2 RA dapiglutide, and the long-acting amylin analog cagrilintide were also presented at the conference.
- In T2D prevention and management, advances in T2D therapies continued their momentum at EASD 2025, where sessions included trial readouts on tirzepatide in pediatric populations with T2D and a secondary CGM-based analysis of the REDEFINE 2 trial of CagriSema (fixed combination of cagrilintide 2.4 mg and semaglutide 2.4 mg) in people with T2D. Furthermore, several sessions highlighted the benefits and clinical considerations for SGLT-2 inhibitor combination therapy for kidney protection and finerenone combination therapy for additive renal benefits on UACR levels.
- In glucose monitoring, new data supported its value in inpatient care, pregnancy, and T2D. A standout session led by Dexcom COO Mr. Jake Leach included Prof. Sufyan Hussain (King’s College London, UK), Dr. Keri Leone (Dexcom), and Dr. Halis Akturk (University of Colorado Anschutz), who spotlighted CGM’s impact on reducing complications, including DR, CV risk markers, and hospitalizations and ER visits. Clinical evidence on the safety of inpatient CGM use strengthened, with Prof. Mikkel Olsen (Steno Diabetes Center Copenhagen) sharing data in T2D inpatients (n=166) showing a nearly 15-point TIR gain (63 to 78%) and 24% fewer complications. Finally, speakers touted recent findings on the benefits of CGM in pregnancy and T2D.
- In insulin delivery, EASD 2025 featured real-world and clinical study data reinforcing the safety and efficacy of AID systems across T1D and T2D. As we await a “fully” closed loop system, a growing body of evidence has demonstrated the impact of AID on folks who do not regularly bolus, with positive data from Control-IQ and MiniMed 780G presented in Vienna. Both Tandem and Medtronic also presented two- and three-year data from the real-world use of their AID systems; Medtronic also presented data on MiniMed 780G use in: (i) pediatrics; (ii) T2D; (iii) pregnancy; and (iv) advanced CKD.
- In CGM metrics, several sessions suggested complementing A1c with metrics like TIR. Interestingly, we saw more CGM-derived metrics being used to enable new categorization frameworks - Dr. Anuj Maheshwari (Hind Institute of Medical Sciences, India) and Dr. Shubashree Patil (Diabetes and Wellness Clinic, India) presented an observational study (n=527) identifying five novel diabetes subgroups based on CGM variability profiles: (i) stable hyperglycemia; (ii) postprandial spike; (iii) brittle hypoglycemia; (iv) dawn phenomenon; and (v) erratic fluctuates, with each subgroup corresponding to distinct therapeutic strategies.
In this report, we provide our full coverage of EASD 2025. Our sections include:
- Themes
- GLP-1 Receptor Agonists
- SGLT Inhibitors
- Insulin Therapy
- Type 1 “Cures,” Prevention, Delay, and Adjunctive Therapies
- Diabetes Complications
- T2D Treatment and Remission
- Obesity
- Award Lectures
- Big Picture of Diabetes Therapy
- Glucose Monitoring – BGM and CGM
- Automated Insulin Delivery, Pumps, and Pens
- Big Picture of Diabetes Technology
- Big Picture and Additional Topics
- The diaTribe Foundation 18th Annual Diabetes Forum
- Exhibit Hall
Table of Contents
-
Themes
- Tech
-
Therapy
- 1. Incretin-based therapies in the heart: SURPASS-CVOT trial and additional analyses show CV benefits of semaglutide and tirzepatide
- 2. Updates on obesity care: From oral GLP-1 RA to quadruple agonists
- 3. Rise of T2D therapies: SGLT-2 inhibitors, GLP-1 RAs, finerenone, and more
- 4. Updates on T1D disease-modifying therapies and adjunctive therapies
- 5. Microvascular complications: Emerging therapies to manage diabetic retinopathy, neuropathic pain, and renal impairment
- 6. The development of liver complications takes focus through an EASD-EASL joint symposium and hypotheses around fructose consumption
-
Big Picture
- 1. Award and special lectures highlight innovative research, public health champions, and the future of personalized care
- 2. T1D screening efforts highlight a need for attention to adult populations and avoiding complications at the time of diagnosis
- 3. Broadening the view of diabetes: From emotional burden to environmental drivers
-
GLP-1 Receptor Agonists
- Amgen’s symposium highlights the roles of GIP receptor agonism/antagonism and once-monthly MariTide in metabolic diseases; Dr. Donna Ryan: a “golden age” of obesity development
- Post-hoc analysis of SOUL trial finds CV benefits of Rybelsus (oral semaglutide) regardless of baseline A1c or BMI
- Full phase 2 results of dual GLP-1/GIP RA HRS9531 for overweight or obesity without T2D
- The role of incretin-based treatments in T1D management
- Full results of phase 3 ATTAIN-1 trial: Lilly’s once-daily GLP-1 orforglipron demonstrates 11% weight loss in people with obesity
- Phase 3 REDEFINE 2 trial: CagriSema significantly increases Time in Range in people with obesity and T2D, per secondary analysis
- TIRTLE1 T1D trial shows that Lilly’s once-weekly GLP-1/GIP tirzepatide reduces weight (9%) and insulin dose (33%) and improves body composition
- Incretin-associated sarcopenia: Does it matter which treatment?
- Phase 2b COURAGE trial: Regeneron’s trevogrumab help preserve 50-80% of lean mass lost with semaglutide alone
- Amycretin demonstrates favorable pharmacokinetics, safety, and tolerability in people with renal impairment
- Pooled analysis of SOUL, FLOW, and STRIDE: Semaglutide reduces major adverse limb events by 30% compared to placebo
- Real-world study finds semaglutide is associated with 23% reduced MACE compared to dulaglutide in people with T2D and CVD
- Zealand’s once-weekly dual GLP-1/GLP-2 RA dapiglutide confers up to 8% weight loss at Week 13
- Full results of SURPASS-CVOT: Tirzepatide reduces MACE numerically by 8%
- Additional results of SURPASS-CVOT: Tirzepatide significantly reduces weight and glycemic outcomes
- SURPASS-PEDS: Tirzepatide dropped A1c by 2.3 percentage points from undisclosed baseline; first GLP-1 RA to demonstrate clinically meaningful weight loss (-9.1%) in youth with T2D
- STEP UP post-hoc studies reveal positive effects on body composition, proximal muscle strength, and control of eating with semaglutide 7.2 mg
- GLP-1 RA-based therapies and impact fertility, pregnancy, and early-onset T2D in women
- Pre-specified analysis of SOUL trial: Oral semaglutide reduces hospitalization burden in people with T2D and ASCVD or CKD
- Pre-specified analysis of SOUL trial finds reduction in major adverse limb events with Rybelsus (oral semaglutide) in people with and without PAD
-
SGLT-2 Inhibitors
- Profs. Heerspink, Roden, and Bozkurt highlight the potential for SGLT-2 inhibitor and GLP-1 RA combination therapy for cardiorenal protection
- Trends of SGLT-2 inhibitor use in T2D in the UK: Up to 90% with T2D and CKD eligible, but uptake not yet optimal
- Prespecified analysis of phase 2 CONFIDENCE trial: simultaneous use of finerenone (Bayer’s Karendia) and empagliflozin (BI/Lilly’s Jardiance) prompted far better outcomes while addition of GLP-1 yielded nothing additional
- New paths for old friends: Potential new roles for GLP-1 RAs and SGLT-2 inhibitors
- Do we need really need a large outcome trial to prove the cardiorenal benefits of SGLT-2 inhibitor and GLP-1 RA combination use?
- Insulin Therapy
-
Type 1 “Cures,” Prevention, Delay, and Adjunctive Therapies
- INNODIA’s phase 2 MELD-ATG trial finds low-dose ATG significantly preserves C-peptide levels in young individuals with new-onset T1D
- In Ver-A-T1D trial, verapamil confers non-statistically significant preservation in C-peptide in new-onset T1D
- “There's no insulin like your own”: Two-year outcomes of the BANDIT trial demonstrate JAK inhibitor baricitinib preserves C-peptide
- Fr1da study shows insights into single islet antibody prevalence and progression in children
- “The era of diagnosis”: Survival rates for T1D increased over decades
-
Diabetes Complications
- CKD and T1D: Profs. Heerspink and Rossing argue status quo must change
- Revolutionizing cardiometabolic health: Novo Nordisk’s industry symposium focuses on the kidney, liver, and weight management
- Fructose consumption may play a key role in the development of MASLD
- Precision medicine in T2D: Targeting GLP-1 RAs and SGLT-2 inhibitor combination treatment for kidney protection
- Phase 2b PROGRESS trial results show AAK1 inhibitor pilavapadin (LX9211) reduces pain in DPN; findings support phase 3 trial for 10 mg dose
- EASD-EASL joint symposium: Bridging the gap with improved screening and the use of combination therapies
- Hyperglycemic crises: Q&A offers insight into best practice guidelines on DKA management
- EASD-CEDA Joint Symposium: Diabetic complications in the era of precision medicine
- Significant increases in dementia-related mortality in people with diabetes compared to those without
- New insights into persistent and increasing burdens of diabetes morbidity
- Benefits and challenges of AI-assisted screening for diabetic retinopathy and an overview of the eye health treatment landscape
- Pooled analysis demonstrates the safety and efficacy of semaglutide among people with CKD also on dialysis
- Fenofibrate lessens the progression of diabetic retinopathy and maculopathy in people with T2D
- Diabetic peripheral neuropathy is associated with an increased risk of stroke in individuals with T1D
-
T2D Treatment and Remission
- Lilly symposium highlights the evolving and crucial role of CVOTs in T2D management
- Phase 3 study finds A1c reduction and potential cardiorenal protection with berberine ursodeoxycholate
- Dr. Steven Kahn and Prof. Roy Taylor on new-age incretin therapies as a path to T2D remission
- GIP infusion alone or in addition to semaglutide shows no improvement in glucose levels or body weight in T2D
-
Obesity
- Post-hoc analysis of phase 3 REDEFINE-1 trial: Long-acting amylin analog cagrilintide confers greater weight loss (12%) than placebo (2.3%)
- Oral quadruple agonist NA-831 for obesity: Topline phase 2 results suggest weight loss without muscle loss and GI-related side effects
- Oral GLP‑1 RGT‑075 demonstrates clinically meaningful weight loss and blood pressure reduction in people with obesity
- Once‑weekly amylin agonist eloralintide conferred up to 11% weight loss at Week 12 in people with obesity
-
Award Lectures + Additional Topics
- 57th Claude Bernard Lecture by the esteemed Professor Andrew Hattersley focuses on “precision diabetes”: Learning from the rare and applying to the common
- Prof. Mikael Rydén receives the Camillo Golgi Prize for expanding knowledge of white adipose tissue and its role in diabetes
- 19th Albert Renold Lecture: Prof. Raphael Scharfmann on pancreatic development as a key to discover unexpected treatments of diabetes
- 60th Minkowski Lecture: Dr. Teresa Mezza on prioritizing the pancreas in T2D
- EASD Diabetes Global Impact Prize Lecture
-
Big Picture of Diabetes Therapy
- Additional CATALYST trial insights and perspectives on the current hypercortisolism diagnostic cutoff from UNC’s Dr. John Buse
- C-peptide measurements to improve classifications of diabetes in routine clinical practice
- ELSA study shows acceptability and feasibility of general population screening for pre-symptomatic T1D among children in the UK
- Discussion with Dr. Alice Cheng, Prof. Francesco Giorgino, and Prof. Ezio Bonifacio on population-wide, age-indiscriminate screening for T1D
- An early look into the Breakthrough T1D-led early-stage T1D screening consensus document: Recommendations on who, what, when, where, how
-
Glucose Monitoring – BGM, CGM, and CKM
- CGM and DGK: Dr. Bergenstal highlights technology-enabled improvements in T1D and T2D management
- Dexcom COO Mr. Jake Leach spotlights CGM as a tool for reducing diabetes complications and enhancing therapy optimization
- Roche’s Accu-Chek SmartGuide CGM: Real-world data (n=249) shows significant reduction (20%) in nocturnal hypoglycemic events with Night Low Predict feature
- Safety and accuracy of CGM for inpatient DKA management compared to hourly POC testing
- International RCT finds CGM reduces risk of large-for-gestational-age infants in women with GDM
- CGM use in hospitals: Clinical benefits and implementation challenges
- Evidence supports benefit of CGM for reduction of severe, recurrent hypoglycemia
- Trust as the cornerstone: CGM, AID, and AI in the next era of diabetes care
- Diabetes technology for pregnancy: Bridging gaps between evidence and guidelines
- GRACE and DipGluMo show the huge power of CGM’s role in GDM management
- MiniMed 780G vs. Control-IQ: Handling unannounced meal in adolescents with T1D
- CGM as a routine for T2D: Evidence from RCTs, real-world data, and case studies
- CGM use in hospitals: Clinical benefits and implementation challenges
-
Insulin Delivery: AID, Pumps, and Pens
- Three years of MiniMed 780G: Durable glycemic outcomes, reduced burden, and strengthened patient confidence
- Glycemic improvements with Tandem’s Control-IQ at 12 months maintained at 24 months
- Automation in complexity: MiniMed 780G shows strength in T2D and other populations
- Control-IQ in focus: A review of clinical strategies and 2025 OUS software updates
- Medtronic shares clinical pearls for using smart MDI: Improving outcomes and simplifying decision making
- Exercise and AID: Insights from the RAPPID study on hypoglycemia risk
- Nationwide French data highlight durability and glycemic gains associated with AID use
- CamAPS FX and Control-IQ improve glycemia and neonatal outcomes vs. MiniMed 780G in pregnant women with T1D; strong outcomes across all systems
- Insulet-sponsored symposium emphasizes scalable onboarding strategies and real-world outcomes with Omnipod 5 in T1D
- INLOOP study: One-year real-world outcomes with Diabeloop DBLG1 show durable glycemic and quality-of-life benefits
- RADIANT adult sub-analysis (n=79): Omnipod 5 drives significant A1c and TIR gains vs. MDI with CGM, with A1c reaching 7.2% and an extra five-plus hours time “in range”
-
Big Picture of Diabetes Technology
- Novel diabetes subgroup classifications and optimized treatment plans based on glucose variability patterns from CGM data
- A look to the FDA’s iCGM requirements: Evolving the minimum expectations for CGM market authorization in the EU
- Defining provider roles in diabetes technology: The University of Leicester’s four-level competency framework
- EASD Expert Session with Prof. Sabine Hofer and Dr. Amit Gupta: Education, reimbursement, and safety remain central to diabetes technology adoption across global settings
- The diaTribe Foundation 19th Annual Diabetes Forum
-
Big Picture and Additional Topics
- Vienna welcomes nearly 11,500 participants with diabetes posters spotted in airport, buildings, and subways
- Prof. Chantal Mathieu delivers most-valuable EASD Presidential Address, extolling vision for personalized, global diabetes care
- Under promise and over deliver: Dr. Dan Drucker on his philosophy for scientific research
- EASD draft guidelines aim to bring diabetes distress assessment and management into routine care
- Global analysis finds that diabetes is the largest contributor to sugar-sweetened beverage-related deaths
- Risk factors for severe hypoglycemia in older adults: Insights from the iNPHORM study
- Systematic analysis of the Global Burden of Disease reports major large-scale findings on prediabetes prevalence from 1990 to 2023
- Rethinking A1c: Genetics, aging, and CGM differences challenge the “one-size-fits-all”
- New insights in glycemic management: Sleep duration, pregnancy, and a head-to-head comparison of three CGMs during exercise
- Exercise boosts TIR in CGM analysis of adolescents with T1D (n=3,069)
- Diabetologia Symposium: Ancestry, access, and inequality shape the global diabetes landscape
- Fewer than 40% of Danish women with prior GDM undergo postpartum diabetes screening within seven years
- Higher A1c thresholds required to predict T1D progression in adults compared to children with positive islet autoantibody
- Exhibit Hall
Themes
Tech
1. CGM shows value across the continuum of care, reinforced by data on T2D, inpatient care, and pregnancy
EASD 2025 showcased how CGM continues to rapidly evolve beyond just outpatient use, with new data supporting its value in inpatient care, pregnancy, and T2D. Across sessions, speakers highlighted CGM’s role in enhancing safety, optimizing therapy, and improving outcomes across the diabetes continuum.
- CGM’s growing role in complication prevention and therapy optimization was a central focus. A standout session led by Dexcom COO Mr. Jake Leach included Prof. Sufyan Hussain (King’s College London, UK), Dr. Keri Leone (Dexcom), and Dr. Halis Akturk (University of Colorado Anschutz), who spotlighted CGM’s impact on reducing complications and tailoring treatment. Dr. Leone presented a 2024 cohort study linking CGM initiation in T1D (n=550) to a 47% lower likelihood of diabetic retinopathy, alongside data (n=47) showing improved CV risk markers with Dexcom G6 use. Dr. Akturk shared results from a large T2D cohort (n=74,679) showing reduced hospitalizations and ER visits. Dr. Hans DeVries (Academic Medical Center, the Netherlands) also reviewed real-world data that showed ER visits for hypoglycemia dropped 5% to 2% after CGM initiation, with greatest benefit among people with impaired hypoglycemia awareness.
- Clinical evidence on the safety of inpatient CGM use strengthened. Prof. Mikkel Olsen (Steno Diabetes Center Copenhagen) shared DIETEC trial data in T2D inpatients (n=166) showing a nearly 15-point TIR gain (63 to 78%) and 24% fewer complications. Separately, Dr. Magdalene Bogun (Columbia University) presented an inpatient DKA study (n=163) showing that Dexcom G6 readings correlated with hourly point-of-care (POC) tests (MARD 17.4% and 19.8% after DKA resolution) and allowed clinicians to reduce testing burden without compromising safety.
- The evidence of improved pregnancy outcomes with CGM continues to build. Prof. Tina Linder (Medical University of Vienna, Austria) showed that CGM use in GDM lowered rates of large-for-gestational-age (LGA) infants (2.5% vs. 10.3% with BGM) and improved glycemic outcomes late in pregnancy in the international GRACE RCT. Prof. Helen Murphy (University of East Anglia, UK) echoed these results, highlighting CGM’s potential to detect dysglycemia and GDM earlier in pregnancy.
- Real-world evidence highlighted CGM as a routine component of T2D care. In an Abbott-sponsored symposium, Profs. Emma Wilmot (University of Nottingham, UK) and Virginia Bellido (Hospital Universitario Virgen del Rocío, Spain) reviewed evidence from FreeStyle Libre trials MOBILE (n=175), IMMEDIATE (n=116), and PDF (n=126), which all showed consistent A1c reductions (0.4-0.5%) and TIR increases across both insulin- and non-insulin-treated T2D cohorts when a CGM was incorporated into treatment plans. Both called for policy alignment with this evidence, arguing that CGM’s ability to provide insights into food, exercise, and medication impact makes it an essential feedback tool across the T2D population.
2. Real-world and clinical evidence supporting the use of AID continues to grow
EASD 2025 featured data reinforcing the safety and efficacy of AID systems across diverse populations, with growing evidence from both real-world and clinical studies in T1D and T2D.
- As we await a “fully” closed loop system, we have been interested in the growing body of evidence showing the impact of AID on folks who do not regularly bolus. Dr. Laurel Messer (Tandem) focused much of Tandem’s symposium on Control-IQ’s AutoBolus feature, designed to support users who frequently miss manual boluses. In a 12-month single-center study, participants relying on AutoBolus for >90% of doses saw a 19% TIR increase and a 1.6% A1c reduction from undisclosed baselines. Elsewhere, Dr. Salvatore Scirè Calabrisotto (University of Catania, Italy) compared MiniMed 780G and Control-IQ in a randomized crossover study (n=20) assessing unannounced meals; both systems converged glucose profiles within four hours, though proportional-integral-derivative-based algorithms (MiniMed 780G) slightly outperformed model predictive control-based systems (Control-IQ) in this context, while reinforcing the importance of meal bolusing for optimal control for lower and later spikes.
- Medtronic presented data across a range of populations. Early in the conference Dr. Jennifer McVean (Medtronic) presented three-year real-world evidence (n=1,145) from MiniMed 780G users (≥16 years old) across Europe, the Middle East, and Africa, showing sustained glycemic improvement: TIR rose from “upper-60%” at baseline to 79% and remained stable over 36 months. Additional findings highlighted MiniMed 780G use in key groups:
- Pediatrics: Prof. Battelino reviewed results from the LENNY trial supporting the use of MiniMed 780G in children age two and older;
- T2D: Prof. Nørgaard presented data supporting MiniMed 780G’s efficacy, durability, and cost-effectiveness in T2D;
- Advanced CKD, including those on dialysis: Prof. Nørgaard also reported improved TIR (from ~55%-66% at baseline to 71%-77%) in short-term studies of patients with severe CKD or on dialysis with MiniMed 780G use, without increased hypoglycemia; and
- Pregnancy: Dr. Cukierman-Yaffe emphasized opportunities and challenges of MiniMed 780G use during pregnancy in women with T1D. Dr. Carmen Quiros (Hospital Universitari Mútua Terrassa, Spain) also presented results from a Spanish multicenter observational trial in which those using MiniMed 780G achieved mean TIR ≥70% and A1c of 6.2% by the third trimester, though Control-IQ and CamAPS FX users reached significantly lower median A1c and risk of large-for-gestational-age neonates.
- Additional data on Control-IQ was also presented. Prof. Jolien De Meuleeester (KU Leuven, Belgium) shared two-year INRANGE study data showing durable benefits: TIR rose from 59% at baseline to 71% at 12 and 24 months, and the share of users achieving target TIR >70% more than doubled – from 25% at baseline to 58% at 12 months and 56% at 24 months.
Across presentations, the message was clear: AID systems are demonstrating consistent, sustained glycemic benefits in increasingly diverse and complex patient populations.
3. Beyond A1c: Looking at the value of TIR and other CGM-derived metrics for personal care
While A1c continues to be considered the “gold-standard” metric for tracking diabetes management, several sessions suggested complementing A1c with metrics like TIR. Collectively, speakers underscored that A1c levels alone cannot capture a patient’s glycemic variability, nor can it fully account for genetic, physiologic, or behavioral factors that influence outcomes. Studies reaffirmed that the future of diabetes management should ideally integrate TIR, glycemic variability, and patient context alongside A1c. As technology advances and standardization efforts move forward, CGM-derived metrics will likely redefine diagnostic criteria and personal treatment pathways.
- Speakers cautioned against overreliance on A1c alone. Prof. Inês Barroso (University of Exeter Medical School, UK) showed that genetic variants such as G6PD can significantly alter A1c independent of true glycemia, delaying diagnosis by years in specific ethnic groups and compounding disparities in complication risk. She cautioned that overreliance on A1c alone could systematically lead to underdiagnosis and undertreatment in affected populations. Prof. Astrid Petersmann (University Medicine Oldenburg, Germany) and Dr. Guido Freckmann (Institute of Diabetes Technology GmbH, Germany) agreed with this statement, discussing how age-related increases in A1c in people with diabetes may lead to inaccurate diagnostic cut-offs and saying that CGM integration with A1c measures must be standardized.
- CGM-derived metrics are enabling new categorization frameworks to personalize treatment beyond A1c. Dr. Anuj Maheshwari (Hind Institute of Medical Sciences, India) and Dr. Shubashree Patil (Diabetes and Wellness Clinic, India) presented an observational study (n=527) identifying five novel diabetes subgroups based on CGM variability profiles: (i) stable hyperglycemia; (ii) postprandial spike; (iii) brittle hypoglycemia; (iv) dawn phenomenon; and (v) erratic fluctuates. Each subgroup corresponded to distinct therapeutic strategies.
Therapy
1. Incretin-based therapies in the heart: SURPASS-CVOT trial and additional analyses show CV benefits of semaglutide and tirzepatide
Incretin-based therapies and their cardiovascular benefits took the spotlight at EASD 2025. The long-anticipated phase 3 SURPASS-CVOT (n=13,165) readout specifically drew thousands of attendees in person and online despite an early morning session. As background, the phase 3 trial is a head-to-head cardiovascular outcomes trial (CVOT) comparing Mounjaro (tirzepatide) to Trulicity (dulaglutide) in people with T2D and established cardiovascular disease (CVD). At four years, tirzepatide numerically reduced the risk of three-point MACE (CV death, myocardial infarction [MI], stroke; CI: 0.83-1.01, p=0.086) by 8% compared to dulaglutide. Strikingly, tirzepatide significantly reduced the all-cause death by 16%. Compared to a placebo, tirzepatide had 28% reduction in three-point MACE and 39% reduction in all-cause death. Additional analyses confirmed renal and metabolic benefits of tirzepatide. Specifically, tirzepatide significantly reduced the risk of composite kidney endpoint by 19% overall and 22% in the high-risk population, compared to placebo.
- Meanwhile, Novo Nordisk shared results of the REACH real-world study (n=58,336), which compared semaglutide to dulaglutide on the risk of major adverse cardiovascular events (MACE) among people with T2D and atherosclerotic cardiovascular disease (ASCVD). In this trial emulation using Medicaid claims data from 2006-2022, semaglutide was associated with 23% reduced risk of three-point MACE (ischemic stroke, MI, and all-cause death), compared to dulaglutide (p<0.001). Likewise, semaglutide had 25% lower risk of five-point MACE (ischemic stroke, MI, unstable angina, heart failure, and all-cause death), compared to dulaglutide (p<0.001). By individual MACE events, semaglutide was statistically significantly associated with 35% reduction of ischemic stroke and 26% reduction of all-cause death than with dulaglutide. While the presenter Dr. Xi Tan (Novo Nordisk) emphasized that CV benefits of semaglutide are molecule-specific and cannot be assumed across the total GLP-1 RA class, it is important to note that REACH is a real-world study that has intrinsic differences from RCTs. Direct comparison of CV benefits between semaglutide and tirzepatide warrants a head-to-head trial.
- On oral therapies, Dr. Silvio Inzucchi (Yale University) presented post-hoc analysis of the SOUL trial, evaluating cardiovascular benefits of Rybelsus (oral semaglutide) by baseline A1c and BMI in people with T2D and ASCVD or chronic kidney disease (CKD). As a reminder, the phase 3b SOUL trial (n=9,650) demonstrated a statistically significant and superior 14% major adverse cardiovascular events (MACE) reduction with oral semaglutide. This analysis confirmed that CV benefits of oral semaglutide were consistent across baseline BMI but more pronounced with higher baseline A1c.
2. Updates on obesity care: From oral GLP-1 RA to quadruple agonists
Obesity treatments were of high interest at EASD 2025, with several trial readouts across multiple incretin-based therapies. Notably, full results of the phase 3 ATTAIN-1 trial showed that orforglipron 36 mg, 12 mg, and 6 mg conferred 12%, 9%, and 8% weight loss, compared to 0.9% with placebo, in people with overweight or obesity. Moreover, orforglipron led to significant improvements in cardiometabolic markers, including waist circumference (11 cm vs. 2 cm with placebo), total fat mass (20% vs. 2% with placebo) systolic blood pressure (6.7 mmHg vs. 1 mmHg), triglycerides (16.4% vs. 5%), and A1c (0.4 percentage-points vs. no change). Other oral agents included oral quadruple GLP-1, GIP, glucagon, and IGF-1 RA NA-831, which conferred 13.8% weight loss (13.8 kg from a baseline of 99.8 kg) in people with obesity in a phase 2 trial (n=125). Across all NA-931 groups, seven participants (7.3%) experienced mild nausea, compared to three participants in the placebo group (10.3%).
- Several injectable dual agonists have also shown benefits in weight loss. Notably, in a phase 2 trial (n=61), Jiangsu Hengrui Pharmaceuticals’ dual GLP-1/GIP RA HRS9531 conferred a mean weight loss of 23% compared to 1.7% weight loss for those on placebo. Moreover, HRS9531 reduced waist circumference (18 cm vs. 3 cm with placebo), BMI (7.1 kg/m2 vs. 0.7 kg/m2), SBP (14.3 mmHg vs. 5.2 mmHg), A1c (0.4 vs. 0.1 percentage points), and triglyceride levels (41% vs. increase by 45%) at Week 36. Safety findings were generally consistent with incretin-based therapies. Zealand’s once-weekly dual GLP-1/GLP-2 RA dapiglutideconferred up to 8% weight loss at Week 13 in a phase 1b multiple ascending dose trial (n=54). Moreover, mean systolic blood pressure decreased by ~5 mmHg compared to baseline.
- Several post-hoc analyses revealed new insights on candidates like amylin analog or high-dose semaglutide. A post-hoc analysis of the phase 3 REDEFINE-1 trial (n=3,417) found that long-acting amylin analog cagrilintide conferred an average weight loss of 11.8% (12.5 kg or 28 lbs) at Week 68, compared to 2.3% (2.5 kg or 5.5 lbs) with placebo. Notably, 31.6% of participants reached ≥15% weight loss versus 4.7% in the placebo group. Cagrilintide also reduced mean waist circumference by 10.6 cm versus 4 cm with placebo, suggesting therapeutic benefits of cagrilintide separately from CagriSema. A prespecified post-hoc analysis of the STEP-UP trial found that semaglutide 7.2 mg improved body composition, proximal muscle strength, and control of eating.
- Finally, many sessions at EASD 2025 discussed the clinical significance of weight loss quality. In one debate, Prof. Gabriele Riccardi (Federico II University, Italy) and Prof. Martin Haluzík (Diabetes Center of the Institute, Czech Republic) discussed whether incretin treatments (i.e., semaglutide vs. tirzepatide) impact sarcopenia differently. Both agreed that the loss of fat free mass with incretin treatment is an expected outcome, representing the mechanism of body composition. Prof. Riccardi referenced the relationship between weight reduction and loss of lean body mass in the context of different strategies (e.g., diet and bariatric surgery). Like what’s seen with incretin treatments, weight loss with various interventions all lead to a reduction in lean body mass because of a compensatory mechanism. However, the degree to which incretin treatment impacts body composition is not clear and has raised concerns about whether the type of treatment for weight loss matters.
- Separately, Regeneron Pharmaceuticals presented full results of the ongoing phase 2b COURAGE trial (n=1,005), which evaluates the effects of trevogrumab (anti-GDF8/anti-myostatin) with or without garetosmab (anti-activin A) on weight loss quality in people with obesity, when combined with semaglutide. Combination therapy helps preserve 50-80% of lean mass lost with semaglutide alone. Moreover, the triple combination therapy conferred greatest fat mass loss (27%), compared to semaglutide with trevogrumab (19%) and semaglutide alone (16%). Likewise, triple combination therapy achieved greatest weight loss (13%), followed by semaglutide with trevogrumab (11%) and semaglutide alone (10%). By weight loss quality, 7% of total weight loss was from lean mass in the triple therapy group, compared to 18% from semaglutide with trevogrumab and 33% from semaglutide alone.
3. Rise of T2D therapies: SGLT-2 inhibitors, GLP-1 RAs, finerenone, and more
Advances in T2D therapies continued their momentum at EASD 2025, where we heard about SGLT-2 inhibitors, finerenone, GLP-1 RAs, and first-in-class candidates. Sessions included trial readouts on tirzepatide in pediatric populations with T2D, as well as a secondary CGM-based analysis of the REDEFINE 2 trial of CagriSema (fixed combination of cagrilintide 2.4 mg and semaglutide 2.4 mg) in people with T2D. Other discussions included potential of empagliflozin (BI/Lilly’s Jardiance) and finerenone (Bayer’s Kerendia) as a combination therapy and a potential new diagnostic threshold for hypercortisolism.
- On incretin-based therapies, tirzepatide demonstrated clinically meaningful weight loss (9.1%) and A1c reduction by 2.3 percentage-points among youth with T2D in the phase 3 SURPASS-PEDS trial (n=99). Moreover, 79% of participants taking either tirzepatide 5 mg or 10 mg had an A1c below 6.5%, compared to 29% of those taking placebo. Given that young population have greater cardiometabolic risk with earlier diagnosis of obesity and diabetes, the therapy could offer significant benefits.
- Another session shared CGM results of the phase 3 REDEFINE 2 trial (n=1,206), which found that CagriSema, a fixed combination of cagrilintide 2.4 mg and semaglutide 2.4 mg, doubled Time in Range (TIR) from 44% at baseline to 89% at Week 68. This reflects 10 hours and 55 minutes more spent in TIR each day in people with overweight or obesity and T2D. Improvements in CGM metrics were more prominent among those with greater weight loss. This follows full trial readout at ADA 2025, in which CagriSema conferred 15.7% weight loss (vs. 3.1% with placebo) and 2.1% reduction in A1c (vs. no change).
- Several sessions highlighted benefits and clinical considerations for combination therapies. One study based on EHR data from a UK primary care database supports GLP-1 RA and SGLT-2 inhibitor combination therapy for kidney protection. Specifically, the incidence of kidney disease progression was lowest with people receiving both treatments (incidence rate of 2.8 per 1000 patient-years), followed by SGLT-2 inhibitors only (3.2 per 1,000 patient-years), GLP-1 RAs only (4.7 per 1,000 patient-years), and DPP-4 inhibitors or sulfonylureas (5.5 per 1,000 patient-years). Another session focused on combination therapies using finerenone, a nonsteroidal mineralocorticoid receptor antagonist. In a prespecified analysis of the phase 2 CONFIDENCE trial (n=800), simultaneous use of finerenone and empagliflozin conferred additive renal benefits on UACR levels, while GLP-1 RA did not add further benefit. Overall, the analysis found that GLP-1 RA use at baseline does not compromise efficacy or safety, supporting the use of triple therapy in appropriate patients.
- On novel therapies, Dr. John Buse (UNC School of Medicine) shared additional insights on clinical characteristics of CATALYST trial participants when stratified by cortisol levels measured with post-dexamethasone suppression test (DST). As background, the CATALYST trial (Part 1 and Part 2) found that 24% of people with difficult-to-treat T2D have hypercortisolism (Part 1, n=1,057) and that Korlym (mifepristone) is an effective therapeutic intervention (Part 2, n=252). The analysis found that participants with cortisol in the 1.2-1.8 µg/dL range share more similarities – such as medication use and presence of cardiac disorders – with those in the >1.8 µg/dL group than the <1.2 µg/dL group. Dr. Buse thus proposed a lower cutoff for cortisol levels, given that that the current diagnostic cutoff of >1.8 µg/dL does not accurately reflect cardiometabolic risk that exists along a continuum.
4. Updates on T1D disease-modifying therapies and adjunctive therapies
EASD 2025 was packed with insights on disease‑modification and comorbidity risk reduction in people with T1D. Specifically, sessions focused on immune‑modulating agents that aim to preserve endogenous C‑peptide and incretin‑based therapies that can reduce weight, insulin needs, and cardiorenal risks. Overall, there was a strong emphasis on the need to prove durability and safety of therapies, expand trial participant diversity, and identify responder phenotypes.
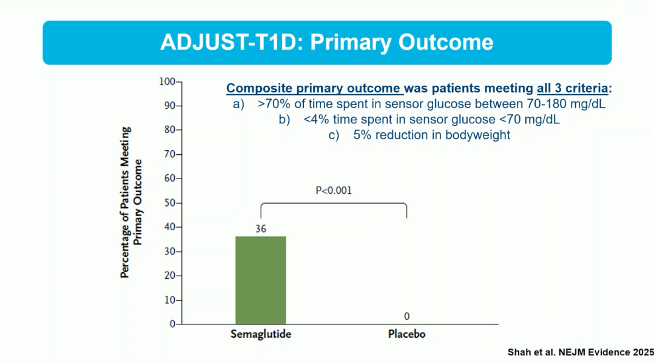
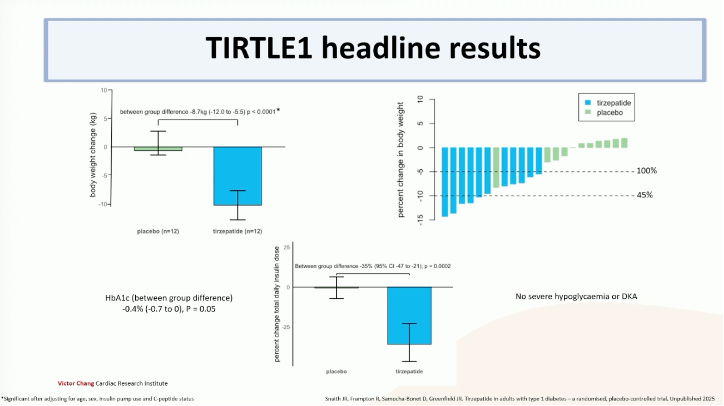
- Incretin-based therapies for T1D: An overcrowded spotlight session highlighted benefits of GLP-1 RAs shown in T1D across various trials. Dr. Petter Bjornstad (University of Colorado) shared findings from the ADJUST‑T1D trial, in which A1c dropped 0.7% with semaglutide (vs. 0.3% with placebo) and the composite outcome (TIR >70%, TBR <4%, ≥5% weight loss) was achieved in 36% of participants receiving semaglutide (vs. none with placebo). Dr. Jennifer Snaith (Garvan Institute of Medical Research) reported results of the TIRTLE‑1 trial of tirzepatide, which found that ≥5% and ≥10% weight loss was achieved in all and 45% participants on tirzepatide, respectively. Tirzepatide also led to a mean A1c reduction of 0.4% with no severe hypoglycemia or DKA. Prof. Riitta Veijola (University of Oulu, Finland) urged larger pediatric trials to define safety and efficacy in children. These findings underscore the growing momentum behind incretin therapies as adjuncts in T1D.
- Preservation of C-peptide: Several sessions highlighted trial results of candidates, anti-thymocyte globulin (ATG), verapamil, and baricitinib, on modifying the progression of T1D. Prof. Chantal Mathieu (KU Leuven, Belgium) presented full results of the MELD‑ATG trial, in which ATG preserved stimulated C‑peptide AUC by 0.102 nmol/L/min versus placebo (p=0.014) in younger people recently diagnosed with T1D. Safety signals included infusion‑related CRS in 33% of the 2.5 mg/kg group and 24% of the 0.5 mg/kg group (none in placebo) and serum sickness in 81.8% and 33% of participants respectively, while CGM metrics remained stable with ATG versus declines in placebo.
- Prof. Thomas Pieber (Medical University Graz, Austria) presented results from Ver-A-T1D trial of verapamil 360 mg daily, which did not meet its primary endpoint for C‑peptide preservation versus placebo. Still, verapamil lowered A1c by 0.3-0.5 percentage points with significance through six months (p=0.001), had a favorable safety profile overall, and will be evaluated further in longer‑term and combination studies.
- Dr. Michaela Waibel (St. Vincent’s Institute of Medical Research, Australia) drove home the point that “there’s no insulin like your own” in her presentation of two-year out comes from the phase 2 BANDIT trial. The study found that baricitinib 4 mg/day significantly preserved mixed‑meal‑stimulated C‑peptide at Week 48 versus placebo (p=0.001) with accompanying reductions in insulin requirement and early improvements in TIR, but the C‑peptide and insulin benefits lost statistical significance by Week 96. Subgroup and responder analyses suggested larger effects in adults (18-30 years) and in participants with BMI ≥30 kg/m2 or ≥80% adherence.
5. Microvascular complications: Emerging therapies to manage diabetic retinopathy, neuropathic pain, and renal impairment
EASD 2025 spotlighted microvascular complications of diabetes, such as diabetic retinopathy, neuropathic pain, and renal impairment. A key session of interest was the full readout of phase 2b PROGRESS trial (n=496), which evaluated AAK1 inhibitor pilavapadin (LX9211) for pain reduction in patients with DPN. In the PROGRESS study, the 10 mg daily dose conferred a 1.7-point reduction, 20/10mg daily dose a 1.8-point reduction, 20 mg daily dose a 1.4-point reduction, and placebo a 1.3-point reduction. Dr. Rodica Pop-Busui (Oregon Health & Science University) explained that the nonlinear dosing effect seen across both PROGRESS and RELIEF-DPN may be due to tolerability issues at higher doses which likely deterred patient adherence. Ultimately, the trial results support phase 3 advancement of pilavapadin 10 mg.
- On major adverse limb events, semaglutide was associated with 30% reduced major adverse limb events (MALE) compared to placebo in a pooled analysis (n=13,975) of the SOUL, FLOW, and STRIDE trials. Semaglutide also consistently reduced the composite endpoints of MALE or all-cause death (HR=0.85), MALE or CV death (HR=0.82), and MALE or MACE (HR=0.83). Semaglutide is the first pharmacotherapy to reduce limb events in people with T2D, regardless of PAD at baseline.
- On eye health, lipid-lowering fenofibrate was found to reduce the progression of diabetic retinopathy in people with both T1D and T2D in the LENS trial (n=1,151). After a median follow-up of four years, just under 23% of participants treated with fenofibrate met the primary endpoint (referable disease or treatment), compared to 29% participants who received placebo, reflecting a 27% risk reduction (p=0.006). The Breakthrough T1D-funded FAME-1 Eye trial and Jaeb Center for Health Research-funded Protocol AF trial are underway to study the effects of fenofibrate for adults with T1D and both T1D and T2D, respectively. On the therapeutic landscape for diabetic macular edema and diabetic retinopathy, SGLT-2 inhibitors and GLP-1 RAs have also shown potential protective effects against disease progression.
- AI-assisted screening for diabetic retinopathy offers high sensitivity and specificity for detecting the disease. Further, AI-assisted screening can positively impact screening uptake by improving patient satisfaction, such as in children. Yet, challenges remain a barrier to AI-assisted screening implementation, including image quality issues, generalizability across populations and devices, reimbursement, and implementation into clinic workflows.
- On kidney health, a phase 2b trial (n=125) on amycretin showed that the therapy demonstrated favorable pharmacokinetics, safety, and tolerability in people with renal impairment.Overall, amycretin was well-tolerated across all groups with similar safety profile as other GLP-1 and amylin RAs. Treatment-emergent adverse events were described to range from 57-86%, with mild renal impairment experiencing lowest and end-stage kidney disease experiencing highest rates. As background, amycretin is evaluated for its weight loss efficacy and has previously conferred 9.7%, 16%, and 22% weight loss after a 12-week maintenance period with the 1.25 mg, 5 mg, and 20 mg doses, respectively.
6. The development of liver complications takes focus through an EASD-EASL joint symposium and hypotheses around fructose consumption
At EASD 2025, the management of liver health was viewed as a key part of holistic diabetes care. The field is rapidly undergoing change in the liver health arena, promoting targeted metabolic therapies for hepatic health and emphasizing the importance of screening in broad populations. On the mechanistic front, research has recently explored the role of glucagon dysfunction and fructose-associated gene expression changes in the development of MASLD and MASH. Understanding the precise causes of these diseases will allow for more effective treatment including the use of GLP-1 RAs and beyond.
- Prof. Laurent Castera (University Beaujon Hospital, France) and Prof. Philip Newsome (King's College London, UK) highlighted a paradigm shift toward earlier detection and more targeted metabolic therapies for liver health in T2D. Barriers to diagnosing MASLD persist, including limited histopathology and lack of awareness of best diagnosis practices. The QUID-NASH program aims to develop a virtual liver biopsy for the diagnosis and staging of MASH in people with T2D. 58% of people with T2D and MASLD also had MASH, emphasizing the importance of screening. Best practices for non-invasive tests (NITs), including FIB-4 and ELF were also a cornerstone of this discussion.
- Glucagon dysfunction may also play a key role in MASH. In MASH, combined agonism of GLP-1, GIPR, and GCGR suppresses appetite, boosts insulin secretion, and drives mitochondrial turnover, fatty-acid oxidation, lipolysis, and thermogenesis. This incretin/glucagon combination reduces hepatic steatosis, inflammation, and fibrosis while improving glucose homeostasis. GLP-1 RAs may play a key role in addressing this: the phase 3 ESSENCE trial showed that semaglutide drove a 63% resolution of steatohepatitis without fibrosis worsening versus 34% in placebo and a 37% fibrosis improvement without steatohepatitis worsening versus 22% in placebo.
- Dr. Florine Westerbeke (Amsterdam University, the Netherlands) suggested a potential new physiological pathway for the development of metabolic dysfunction-associated steatotic liver disease (MASLD). RNA sequencing has identified fructose-associated gene expression changes related to MASLD: fasting fructose levels were found to be higher in patients with MASLD, independent of fasting glucose levels, with a strong dietary component suggested for this effect. This distinction was then used in the different gene expression analysis to determine that 3,969 genes were differentially expressed in the liver in patients with MASLD, with the majority being downregulated. These levels have also been linked to mitochondrial dysfunction in patients with obesity. Fructose-associated toxicity related to the gut microbiome may also play a key role in MASLD pathogenesis.
- Fasting peripheral fructose concentrations correlate with postprandial ethanol production, a sign of gut dysbiosis that can lead to lipogenesis and MASLD. In particular, these levels were associated with Streptococcus parasanguinis, which has previously associated with gut dysbiosis. This can result in impaired digestion and metabolism, and a decreased quality of life overall. In all, fasting fructose levels based on diet increase mitochondrial dysfunction and gut dysbiosis, which may represent a yet-underexplored pathway in the development of MASLD.
Big Picture
1. Award and special lectures highlight innovative research, public health champions, and the future of personalized care
EASD 2025 showcased a slate of awards and special lectures recognizing early‑career innovators and lifetime leaders whose work shapes diabetes science and care. Together, these presentations covered mechanistic discovery and population health, highlighting advances in precision diagnostics, pancreas‑focused biology, pharmacologic remission, adipose biology, and scalable delivery models that promise real-world impact.
- Professor Andrew Hattersley (University of Exeter, UK) received the Claude Bernard Lecture prize and discussed “precision diabetes.” He showed how genetic and clinical subtyping of rare forms of the condition such as neonatal diabetes and MODY can guide targeted treatments and correct widespread misdiagnosis. In interventions, he highlighted neonatal diabetes, which can respond to sulfonylureas, and the University of Exeter’s global testing program. He also described T2D stratification work, including a new five‑drug predictive model that improves mean A1c values by about 0.5%.
- Dr. Teresa Mezza (Università Cattolica e Fondazione Gemelli, Italy) received the Minkowski Prize for using human experimental models to reframe T2D. She showed that insulin resistance provokes early compensatory beta-cell functional changes, ductal trans differentiation, and increased intra-islet GLP-1. These changes ultimately fail, driving disease progression. She concluded that beta cell quality, rather than mass loss, is the earliest, most predictive defect in T2D and called for re-centering the pancreas and intervening before hyperglycemia sets in.
- Dr. Steven Kahn (University of Washington) and Prof. Roy Taylor (Newcastle University, UK) highlighted next‑generation GLP‑1 RAs and dual agonists like tirzepatide as powerful tools for achieving T2D remission. These therapies have shown dramatic reductions in disease progression as well as sustained glycemic improvements in trials such as SELECT and SURMOUNT‑1. Prof. Taylor emphasized that remission via substantial weight loss can restore pancreatic volume and beta‑cell function, arguing that remission is achievable but should not be termed a “cure.” He also noted that many benefits require ongoing therapy or sustained weight loss.
- Dr. Viswanathan Mohan received the EASD Diabetes Global Impact Prize for decades of transformative work building scalable diabetes care, research, education, and charity programs in India. His programs have screened millions of people, trained tens of thousands of clinicians, and delivered free lifelong care to thousands of people in resource‑limited settings. His integrated model includes digital tools, representative epidemiology revealing the South Asian phenotype, rural telediabetology, and massive distance‑learning initiatives and has improved outcomes at the population level, setting a global example for diabetes care delivery.
- In a presidential address, Prof. Chantal Mathieu (UZ Leuven, Belgium) framed diabetes as a spectrum of disease and championed precision, individual care. She announced the launch of education and global initiatives, including lab talks, an expanded Early Career Academy, an immunology course, and a new open‑access journal, Metabologia. She stressed translating research into practice (including a forthcoming guideline on diabetes distress), thanked colleagues as she closed her presidency, and announced Prof. Francesco Giorgino (University of Bari Aldo Moro, Italy) as her 2026 successor.
- As he received the Albert Renold Prize, Prof. Raphael Scharfmann (Cochin Institute, France) showcased human-focused pancreatic development models. These models have revealed the earlier and simultaneous emergence of insulin, glucagon, and somatostatin cells and enabled the generation of functional human beta cells. He highlighted translational tools like EndoC-beta lines and urged refining beta, alpha, and delta cell models to discover unexpected diabetes treatments.
- Prof. Mikael Rydén (Karolinska Institute, Sweden) received the Camillo Golgi Prize for highlighting white adipose tissue plasticity, showing how altered lipid turnover, adipocyte hypertrophy versus hyperplasia, and an “obesity memory” drive metabolic risk and diabetes. He called for open, accessible data to accelerate research and to better prevent and treat obesity‑related diabetes.
2. T1D screening efforts highlight a need for attention to adult populations and avoiding complications at the time of diagnosis
Across all sessions, presenters agreed that the misdiagnosis of T1D in adults remains a serious issue, often with dire consequences for care. The efficacy of screening individuals who have a first-degree relative with T1D was demonstrated in the large-scale ELSA study, encouraging broader scale use of this method and public support for such efforts. Pragmatic concerns around the management of DKA were also discussed, with speakers arguing that lower-grade DKA may not require hospitalization, and that dual glucose-ketone sensing must establish benchmarks for normalcy before it is widely adopted.
- Prof. Parth Narendran (University of Birmingham, UK) presented updated findings from the ELSA study (n=25,165), focusing on the feasibility and acceptability of general population screening for pre-symptomatic T1D among children in the UK. Overall, results showed that the screening model was feasible, with 91% of families completing confirmatory testing, 95% completing staging processes, and 84% attending follow-up education programming. The study identified 56 single-antibody and 125 multiple-antibody children. 85% of these individuals then completed education and support for diabetes management. Prof. Narendran concluded that first-degree relatives are an effective target population for T1D screening – they were more engaged on average and more likely to screen positive with a 3.7% diagnosis rate, compared to 2.2% for those with any relatives with T1D and 0.25% in the general population.
- Dr. Alice Cheng (University of Toronto), Prof. Francesco Giorgino (University of Bari Aldo Moro, Italy) and Prof. Ezio Bonifacio (University of Dresden, Germany) discussed the evolving landscape of T1D screening. Beginning with diagnosis challenges, a July 2025 study published in Diabetes Care, “Contrasting Adult and Pediatric Populations in a Cohort of At-Risk Relatives in The T1D TrialNet Pathway to Prevention,” showed that adults with stage 2 T1D progress to stage 3 at similar rates as children (5-year risk: 78% for both groups), challenging assumptions about disease trajectory and pacing.
- On misdiagnosis, of the 39% of T1D diagnoses that are missed in adults, 77% are misdiagnosed with T2D. Prof. Giorgino discussed the AABBCC approach (age, autoimmunity, body habitus, background, C-peptide, and comorbidities) as a practical framework, with a need for continued work on improving screening for T1D. Ultimately, speakers emphasized that only ~10% of people with T1D have a first-degree relative with the disease, and thus identifying the remaining 90% requires robust systems and multi-test strategies at a population level.
- In preparation for an upcoming consensus statement on population-level screening for early-stage T1D, Breakthrough T1D’s Dr. Anastasia Albanese-O’Neill, Dr. Marian Rewers (University of Colorado), Prof. Anette-Gabriele Ziegler (Helmholtz Zentrum Munich, Germany), and Prof. Chantal Mathieu (UZ Leuven, Belgium) discussed the benefits and challenges of T1D screening. Prior to clinical diagnosis, T1D screening may provide the opportunity to receive disease-modifying therapy, namely Tzield (teplizumab), or participate in clinical trials to stop or slow disease progression.
- However, awareness of early-stage T1D can also induce anxiety, and receiving an early-stage T1D diagnosis can also be stigmatizing. To this, Dr. Rewers emphasized the need for informative monitoring programs and community education to raise awareness and reduce stigma. Prof. Ziegler also stressed the importance of rescreening for children if they are islet-autoantibody-negative, drawing from findings in the BabyDiab, TEDDY, Fr1da, and T1DI studies. If islet autoantibodies are not detected, providers should recommend rescreening in the future and emphasize that it is still possible to develop T1D even though results are currently negative.
- Recent consensus guidelines on hyperglycemic crises were discussed by Prof. Jan Gojda (Charles University, Czech Republic), Dr. Shivani Misra (Imperial College London, UK), and Dr. Rodolfo Galindo (University of Miami Miller School of Medicine). Dr. Galindo stressed that mild DKA should not automatically require ICU admission, as such treatment escalation may increase the risk of hospital-related complications, and instead endorsed protocols using short-acting subcutaneous insulin administered every one to two hours. Both Dr. Misra and Dr. Galindo also pointed to the need for further research into ketone physiology before DGK is widely implemented. More broadly, the panel highlighted that this consensus guidance is not purely scientific but also pragmatic, considering nursing workflows, institutional resources, and the need for multiple tiers of care to ensure global applicability.
3. Broadening the view of diabetes: From emotional burden to environmental drivers
Several other big-picture themes in diabetes care and morbidity rose to prominence at EASD 2025.
- Diabetes distress. Closing out the third day of EASD 2025, an impassioned panel discussed EASD’s draft clinical practice guidance on assessing and managing diabetes distress (the emotional burden of living with diabetes) in T1D and T2D. The draft guidelines aim to ensure diabetes distress is no longer overlooked, offering clarity on how to recognize and manage it in routine practice. The draft guidance includes eight Good Practice Statements during clinical assessments and nine specific GRADE recommendations each for T1D and T2D. The guidelines are expected to be published early 2026.
- Diabetes risk factors. Environmental and lifestyle influences on T2D were a recurring focus. Dr. Yvonne Xu (University of Washington) presented new Global Burden of Disease data showing a 14% global prevalence of prediabetes — affecting roughly 674 million people — rising to 27% by ADA criteria. Prevalence peaks in those aged 50–59 and is highest in Puerto Rico (31%) and lowest in Rwanda (3%). The largest national burdens were seen in China, India, and the US. Meanwhile, analysis of sugar-sweetened beverage (SSB)-related mortality revealed an astonishing 174% increase from 1990-2021, driven primarily by diabetes. Death rates were highest in the Caribbean and Central America and growing fastest in the Middle East and Southeast Asia.
- Diabetes morbidity. In a closing session, Prof. Edward Gregg (RCSI, Ireland) highlighted persistent multimorbidity in diabetes, urging a shift beyond single-complication research. Diabetes confers a two- to threefold increase in long-term conditions, including dementia. Complementing this, Prof. Kanika Mehta (Baker Heart and Diabetes Institute, Australia) shared population-based findings showing rising dementia-related mortality among people with diabetes, especially in older adults across several high-income countries.
GLP-1 Receptor Agonists
Amgen’s symposium highlights the roles of GIP receptor agonism/antagonism and once-monthly MariTide in metabolic diseases; Dr. Donna Ryan: a “golden age” of obesity development
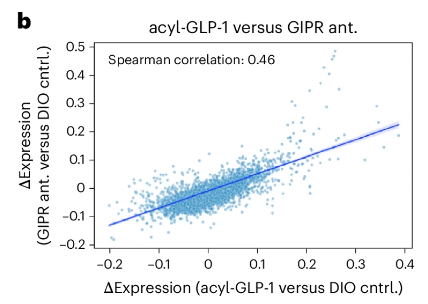
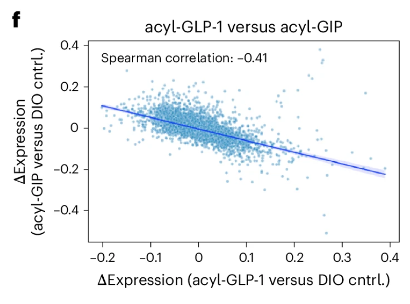
In a fascinating afternoon symposium, Prof. Timo Mueller (Ludwig-Maximilians-University Munich, Germany) and Dr. Donna Ryan (Pennington Biomedical Research Center) discussed the mechanisms of GIP receptor (GIPR) agonism and antagonism and the therapeutic potential of once-monthly MariTide (GLP-1 RA and GIP antagonist) in diabetes and obesity. In opening remarks, Dr. Abd Tahrani (Amgen) emphasized that obesity is a chronic disease that should be treated like hypertension or dyslipidemia. However, several challenges exist, including: (i) treatment adherence, with >50% discontinuing GLP-1 RAs after one year; (ii) weight regain after discontinuation; (iii) unequal access to pharmacotherapy; and (iv) treatment heterogeneity. Thus, Dr. Tahrani argued for new approaches to cardiometabolic management, which are imperative to addressing these challenges.
- Prof. Mueller reviewed the role of GLP-1 and GIP in metabolic health. Incretin hormones GLP-1 and GIP are secreted from the gut and stimulate insulin. These incretins also drive other effects: GLP-1 slows gastric emptying, suppresses glucagon secretion, and induces satiety. GIP has been shown to distinctly act on the brain to induce satiety and decrease body weight. Like a “good cop… mak[ing] sure the car doesn’t leave on the left or right-hand side,” GIP also acts in glucose-dependent manner, regulating glucagon release from alpha cells and lipogenesis (fat formation) or lipolysis (fat breakdown) in adipose tissues.
- Prof. Mueller further explained that GIPR agonism and antagonism induce metabolic benefits via distinct mechanisms, demystifying the apparent irony between the two approaches. Preclinical studies found that GIP agonism decreases body weight via GABAergic (inhibitory neurotransmitter) GIPR neurons, with superior weight loss found in GLP-1/GIP RA in mice with these neurons preserved but not in mice with the neurons knocked-out. On the other hand, GIP antagonism does not rely on GABAergic or glutamatergic (excitatory neurotransmitter) GIPR neurons, suggesting distinct mechanisms. Transcriptomics further showed that GIPR agonism and antagonism induce opposite gene expression patterns, with antagonism but not agonism mimicking that of GLP-1 RA in hindbrain neurons. These findings suggest that GIPR antagonists may strengthen GLP-1 RA effects, while GIPR agonism may provide complementary mechanisms. During Q&A, Dr. Mueller further suggested that weight loss from GIPR antagonism may be mediated by non-neuronal cells like oligodendrocytes, as well.
- Dr. Ryan highlighted the ongoing phase 3 MARITIME program, which is evaluating once-monthly GLP-1 RA/GIPR antagonism MariTide in several trials. As a reminder, 52-week phase 2 results were announced at ADA 2025, demonstrating up to 20% weight loss (vs. 2.6% with placebo) in people with obesity without T2D and 17% weight loss (vs. 1.4% with placebo) in people with T2D. However, discontinuation rates (14-29% in non-dose escalation arms) due to GI-related adverse events like nausea and vomiting were very high in both cohorts. Dr. Ryan highlighted that the weight loss was greater than expected, with improvements in A1c, blood pressure, and hs-CRP. High rates of adverse events emphasize the importance of careful dose-escalation refinements as guided by the Modified Index of Nausea, Vomiting, and Retching (M-INVR) index. Currently, five phase 3 trials are ongoing, including: (i) MARITIME-1 (n=3,501) for adults without T2D; (ii) MARITIME-2 (n=999) for adults with T2D; (iii) Maritime 3-J (n=272) for Japanese participants; (iv) MARITIME-CV (n=12,800) for adults with established ASCVD; and (v) MARITIME-HF (n=5,056) for people with obesity and heart failure (HF) with preserved or mildly reduced ejection fraction. Dr. Ryan called the current generation as the “golden age” of obesity drug development, with oral formulations, three different candidates using GIPR antagonism, and multi-incretin treatments being evaluated.
Post-hoc analysis of SOUL trial finds CV benefits of Rybelsus (oral semaglutide) regardless of baseline A1c or BMI
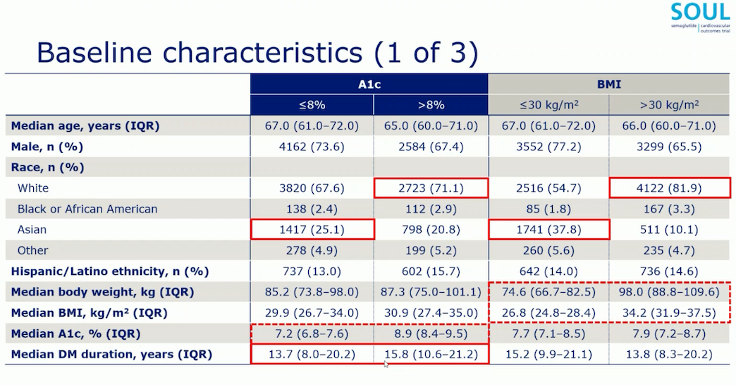
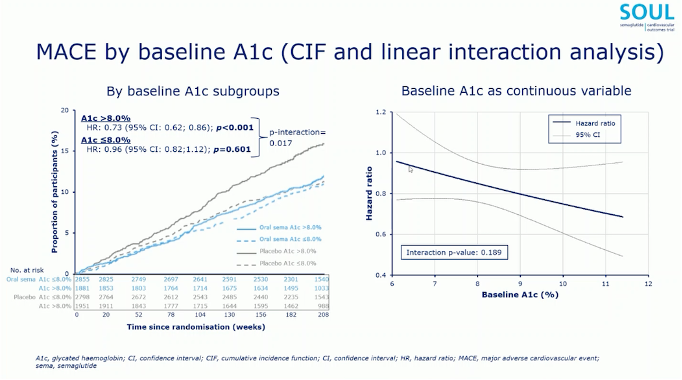
In this crowded morning session, Dr. Silvio Inzucchi (Yale University) presented post-hoc analysis of the SOUL trial, evaluating cardiovascular benefits of Rybelsus (oral semaglutide) by baseline A1c and BMI in people with T2D and atherosclerotic cardiovascular disease (ASCVD) or chronic kidney disease (CKD). As a reminder, the phase 3b SOUL trial (n=9,650) demonstrated a statistically significant and superior 14% major adverse cardiovascular events (MACE) reduction with oral semaglutide.
- Baseline characteristics. Participants were divided by A1c (≤8% or >8%) and BMI (≤30 kg/m2 or >30 kg/m2). Baseline age on average was similar across all groups, but low A1c and BMI groups had greater percentage of males (74% and 77%, respectively) than higher A1c and BMI groups (67% and 66%, respectively). By demographics, as shown in the figure below, Dr. Inzucchi noted that Asians were more likely to have lower A1c and BMI, while White people were more likely to have higher A1c and BMI. Clinically, higher A1c group was more likely to have longer duration of diabetes (16 vs. 14 years in lower A1c group) and on insulin treatment (64% vs. 42% in lower A1c group), which are expected.
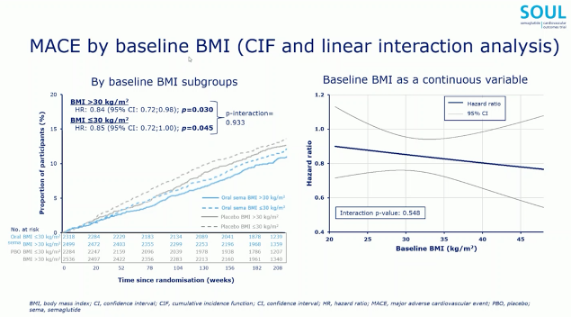
- CV benefits of oral semaglutide were consistent across baseline BMI but more pronounced with higher baseline A1c. By baseline A1c, oral semaglutide conferred 4% and 27% MACE reduction in lower (≤8%) and higher A1c (>8%) group, respectively (p=0.017). Linear interaction analysis, which treats baseline A1c as a continuous variable rather than categorical, found numerically greater MACE risk reduction at higher A1c (p=0.189). By baseline BMI, oral semaglutide conferred similar MACE reduction by 15% and 16% for lower and higher BMI groups (p=0.933). CV benefits of oral semaglutide were not influenced by baseline body weight (p=0.733) or baseline BMI as a continuous variable (p=0.548). Further exploratory analysis found that the change in A1c (p=0.502), BMI (p=0.257), and body weight (p=0.332) during the trial did not influence CV benefits of oral semaglutide.
Full phase 2 results of dual GLP-1/GIP RA HRS9531 for overweight or obesity without T2D
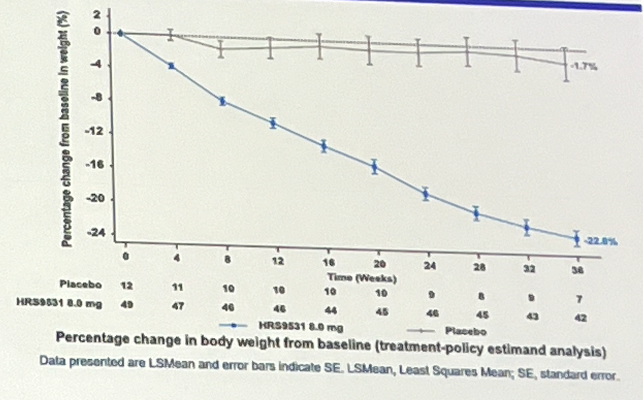
In a packed symposium, Dr. Kun He (Shandong First Medical University, China) presented full results of the phase 2 trial (n=61), evaluating dual GLP-1/GIP receptor agonist HRS9531 from Jiangsu Hengrui Pharmaceuticals in Chinese adults with overweight or obesity but not diabetes. This follows topline results that we reported on when announced in January 2025 that found that HRS9531 conferred a mean weight loss of 23% vs. under 2% weight loss in placebo at Week 36. HRS9531 is also evaluated in phase 3 trials for obesity and T2D. In July 2025, the company announced topline results of the phase 3 trial (n=567) for obesity, in which HRS9531 conferred placebo-adjusted mean weight loss of 16% from baseline of 93 kg (205 lbs) at Week 48. The company shared plans to submit New Drug Application (NDA) in China.
- Trial design and baseline characteristics. Chinese adults with obesity (BMI ≥28 kg/m2) or overweight with a weight-related comorbidity (BMI ≥24 kg/m2) were randomized to receive once-weekly subcutaneous injections of HRS9531 8 mg (n=49) or placebo (n=12). The primary endpoint was the change in body weight from baseline to Week 36. At baseline, participants were on average 33 years old, with ~70% being female. Clinically, participants had average baseline weight of 85 kg (187 lbs), BMI 31 kg/m2, A1c 5.4%, waist circumference 101 cm, and systolic blood pressure (SBP) 120 mmHg.
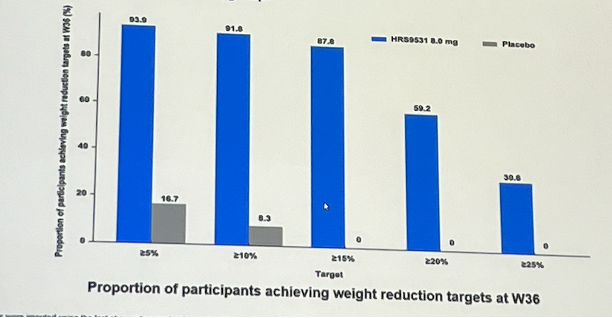
- Results. At Week 36, HRS9531 conferred a mean weight loss of 23% compared to virtually no weight loss, specifically just 1.7% weight loss, for those on placebo. Significantly higher percentage of participants achieved weight loss thresholds, as shown in the figure below. Notably, 88%, 60%, and 31% of HRS9531-treated participants achieved ≥15%, ≥20%, and ≥25% weight loss, respectively, compared to none in the placebo group. Moreover, HRS9531 reduced waist circumference (18 cm vs. 3 cm with placebo), BMI (7.1 kg/m2 vs. 0.7 kg/m2), SBP (14.3 mmHg vs. 5.2 mmHg), A1c (0.4 vs. 0.1 percentage points), and triglyceride levels (41% vs. increase by 45%) at Week 36. Safety findings were generally consistent with incretin-based therapies, with majority of treatment-emergent adverse events being mild and GI-related. Most common GI events included diarrhea (27% vs. none), nausea (25% vs. none), and vomiting (20% vs. none). Notably, no participants permanently discontinued treatment due to treatment-emergent adverse events. While the difference in A1c is not as large as differences in weight loss, we are sure patients who had the 0.4 drop were much more pleased than those who experienced just a 0.1 drop (though something is better than nothing, whether or not the 0.1 is even “accurate” would be a question). Yet again, CGM metrics would be extremely helpful to have with this trial.
The role of incretin-based treatments in T1D management
In a spotlight session so crowded that attendees sat on the floor, panelists explored the science and clinical evidence of where incretin therapies fit in the T1D treatment paradigm. Prof. Riitta Veijola (University of Oulu, Finland) elaborated on the use of GLP-1 RAs in children with T1D, while Dr. Petter Bjornstad (University of Colorado) focused on the adult population. Prof. Jerry Greenfield (St. Vincent’s Hospital, Australia) discussed how GIP agonism enhances the effects of GLP-1 RAs in T1D, along with sharing unpublished data from the TIRTLE 1 trial of tirzepatide in adults with T1D and obesity. The panelists all encouraged the need for GLP-1 RAs as an adjunctive therapy for T1D, especially given the challenges of meeting target A1c levels and addressing complications with insulin alone. Given what we know about hypoglycemia concerns, even for those fortunate enough to have CGM, we are still very wary about regulatory assessment by the FDA. We hope that CGM data can be reviewed in order to reinforce the degree to which glycemic improvement can be seen with GLP-1 (even in the midst of more hypoglycemia, which is manageable) – we are curious if there is dQ&A or other data showing the perceived and actual benefit / risk profiles.
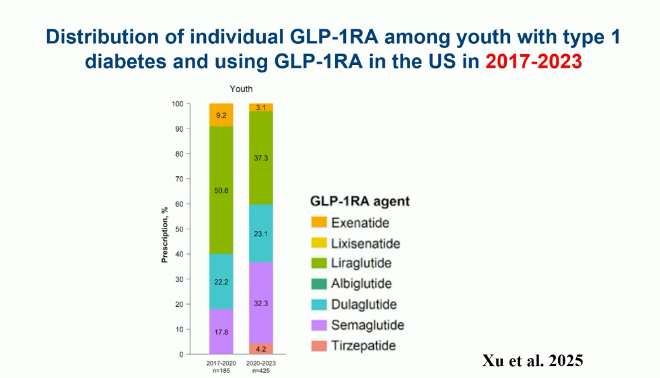
- Prof. Veijola on the use of GLP-1 RAs in children with T1D. GLP-1 RAs are currently approved for children with T2D ≥10 years and approved for children with obesity ≥6 years. While GLP-1 RAs are not approved for T1D, a 2025 study (“Trends in obesity and glucagon-like peptide-1 receptor agonist prescriptions in T1D in the US” by Jung-Im Shin, et. al. in Diabetes, Obesity, and Metabolism) showed that in the last 15 years, the prescriptions of GLP-1 RAs have significantly increased across all BMI categories among both youth and adults with T1D. When looking at the distribution of GLP-1 RA use among youth with T1D, liraglutide (Novo Nordisk’s Victoza) was the most prescribed treatment between 2017 and 2020, followed by dulaglutide (Lilly’s Trulicity), semaglutide (Novo Nordisk’s Ozempic), and exenatide (AZ’s Bydureon and/or Byetta). Although liraglutide remained the most prescribed treatment between 2020 and 2023, the distribution narrowed with increasing treatment of semaglutide and emerging numbers for tirzepatide. We wonder if this is the most popular because there is a perceived flatting of appetite by day when it is taken, which is some of what we hear from some people with T1D who are on it – they seem to appreciate the ability to turn this “on” or “off” from what we hear, though this is anecdotal.
- Beyond the use of GLP-1 RAs in children with T1D, Prof. Veijola also spoke on children with early-stage T1D. She referenced a 2021 study that showed the combination of anti-IL21 and liraglutide preserves beta cell function in adults newly diagnosed with T1D. Furthermore, she elaborated on a 2023 study (“Semaglutide in Early Type 1 Diabetes” by the esteemed Dr. Paresh Dandona, et. al., published in the NEJM in which Ozempic, started within three months of T1D diagnosis in adults, led to the elimination of prandial insulin in all patients and basal insulin in 70% of the study population! These findings highlight that GLP-1 RAs could also potentially help preserve beta cell function in children, alone or in combination with other treatments. Considering the limited evidence in children with T1D, Prof. Veijola encouraged large trials at various stages of T1D to determine the safety and efficacy of GLP-1 RAs in this population.
- Dr. Bjornstad on the use of GLP-1 RAs in adults with T1D. Dr. Bjornstad listed several reasons for needing GLP-1 RA treatment in T1D management, including: (i) inherent limitations of insulin with risks of hypoglycemia, fluctuations in glucose levels, and weight gain; (ii) gaps in glycemic management with most people with T1D unable to achieve A1c or TIR targets, even with AID systems; (iii) increasing metabolic complications like obesity, insulin resistance, and hyperinsulinemia; and (iv) proven CKM protection of GLP-1 RAs showing clear benefits in CV and kidney health. As he advocated for GLP-1 RAs, Dr. Bjornstad clarified that GLP-1 RAs would not compete with insulin or technology interventions but rather act as a synergistic treatment to help mitigate CKM in T1D.
- To further illustrate the need for GLP-1 RAs, Dr. Bjornstad overviewed clinical trial data in T1D, including the most recently published results from the ADJUST-T1D trial presented at ADA 2025. As background, the trial evaluated the use of semaglutide as an adjunct to insulin in adults with T1D and obesity using AID. The composite primary outcome (achieving TIR >70%, TBR <4%, and ≥5% weight loss) was met by 36% of participants in the semaglutide group versus zero in the placebo group. Furthermore, A1c decreased by 0.7% from 7.8% at baseline to 7.1% in the semaglutide group compared to 0.3% from 7.7% at baseline to 7.4% in the placebo group.
- Dr. Bjornstad also outlined other trials investigating the use of GLP-1 RAs in T1D, including: (i) RESET1 of semaglutide in heart health; (ii) T1-DISCO of semaglutide in CV outcomes; (iii) REMODEL-T1D of semaglutide in kidney oxygenation and function; and (iv) OBES1TY of semaglutide in body weight, insulin dose requirements, and glucose levels.
- Prof. Greenfield on GIP/GLP-1 RA in T1D. In light of the emerging evidence of incretin-based treatments, Prof. Greenfield focused on the combination of GIP/GIP-1 RAs. Studies have shown that GLP-1 RAs reduce glucagon and increase C-peptide levels, while GIP RAs have no effect during hyperglycemia. In comparison, GIP RAs increase glucagon levels during hypoglycemia, serving as an ideal molecule for people with T1D. Turning to neurological effects, Prof. Greenfield shared data that shows how GIP RAs inhibit food intake and nausea in the central nervous system. Therefore, Prof. Greenfield emphasized that GIP RAs help blunt nauseating side effects of GLP-1 RAs in humans, explaining the greater tolerability of tirzepatide at doses higher than semaglutide.
- Looking forward, several trials are underway to study the use of tirzepatide in T1D. Prof. Greenfield shared unpublished data of the TIRTLE 1 trial, which focused on the effect of tirzepatide on weight and metabolism in adults with T1D. Headline results showed that all trial participants saw ≥5% weight loss, and 45% of participants saw ≥10% weight loss. Furthermore, the mean A1c reduction was 4% with no severe hypoglycemia or DKA. Reflecting on these findings, Prof. Greenfield encouraged further trials on the effects of low-dose tirzepatide in people with T1D and without obesity, as well as tirzepatide on CV risk reduction.
Full results of phase 3 ATTAIN-1 trial: Lilly’s once-daily GLP-1 orforglipron demonstrates 11% weight loss in people with obesity
A standing-room only symposium, Drs. Sean Wharton (Wharton Medical Clinic, Canada) and Nasreen Alfaris (King Fahad Medical City, Saudi Arabia) presented full results of the phase 3 ATTAIN-1 trial (n=3,127), which evaluated orforglipron, the first once-daily oral small molecule GLP-1 RA, in people with obesity and without T2D. Results were simultaneously published in NEJM and announced in Lilly’s press release. These results follow topline results announced in Lilly’s 2Q25 earnings call, which found weight loss of 12%, 9%, and 8% with orforglipron 36 mg, 12 mg, and 6 mg, respectively, compared to 1% in the placebo group. At the highest dose, approximately 60% of participants achieved body weight reductions of ≥10%. Discontinuation rates due to adverse events were 10%, 8%, and 5% for orforglipron 36 mg, 12 mg, and 6 mg, respectively.
- Study design. The 72-week global[1] trial enrolled 3,127 adults with obesity (BMI ≥30 kg/m2) or overweight (BMI 27-30 kg/m2) with at least one weight-related comorbidity. Individuals with T2D were excluded from the trial. Participants were randomized to placebo, orforglipron 6 mg, 12 mg, or 36 mg, with slower titration compared to phase 2 trial. Participants also underwent lifestyle program but were not mandated to follow a 500-calorie deficit to reflect real-world practice. The primary endpoint was the change in body weight at Week 72. Key secondary endpoints included percentage of participants achieving weight loss threshold (≥5%, ≥10%, ≥15%, ≥20%), waist circumference, blood pressure, non-HDL cholesterol, triglycerides, and other metabolic markers. Analyses used both an efficacy estimand – assuming full adherence – and treatment-regimen estimand.
- Baseline characteristics. On average, participants were 45 years old at baseline, with 64% being women. Clinically, mean body weight was 103 kg (227 lbs), mean BMI of 37 kg/m2, waist circumference of 112 cm (44 inches), and A1c of 5.6%. By BMI category, obesity Class I (BMI 30-35 kg/m2) was most common (36.8%), while overweight (BMI <30 kg/m2) with comorbidities least common (9%). 36% had prediabetes at baseline.
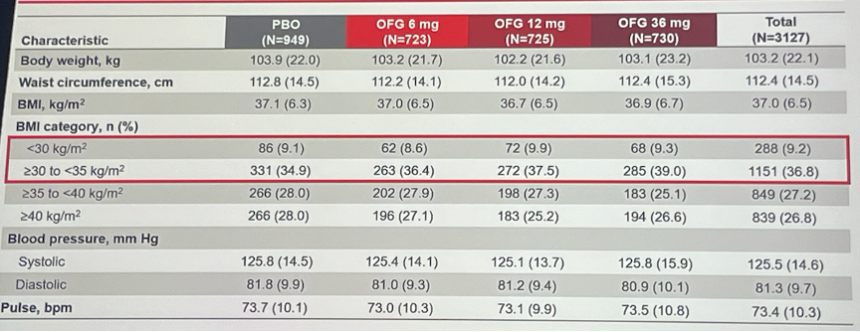
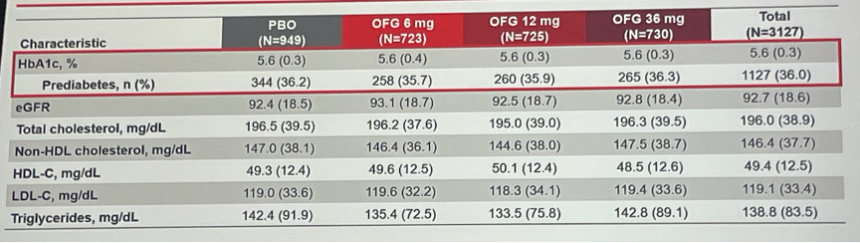
- Results. By the efficacy estimand, orforglipron 36 mg, 12 mg, and 6 mg conferred 12%, 9%, and 8% weight loss, compared to placebo which conferred 0.9% loss (see figure below). By categorical weight loss, 77%, 60%, 40%, and 20% of participants on orforglipron 36 mg conferred ≥5%, ≥10%, ≥15%, and ≥20% weight loss. Orforglipron 36 mg also reduced waist circumference by 11 cm (vs. 2 cm with placebo) from a baseline of 112 cm. Body composition, as measured by DXA, found that orforglipron 36 mg led to 20% reduction of total fat mass (vs. 2% with placebo) and 6.6% reduction of lean mass (vs. no change), with the latter contributing 27% of the total loss from the drug. Visceral fat mass was reduced by 28% (vs. 7% increase). Finally, orforglipron 36 mg significantly improved cardiometabolic markers, lowering systolic blood pressure by 6.7 mmHg (vs. 1 mmHg), diastolic blood pressure by 2.6 mmHg (vs. 1 mmHg), triglycerides by 16.4% (vs. 5%), non-HDL cholesterol by 7.6% (vs. 1%), A1c by 0.4 percentage-points (vs. no change), and an inflammation marker hsCRP by 47.7% (vs. 12.7%). See baseline levels in the table above.
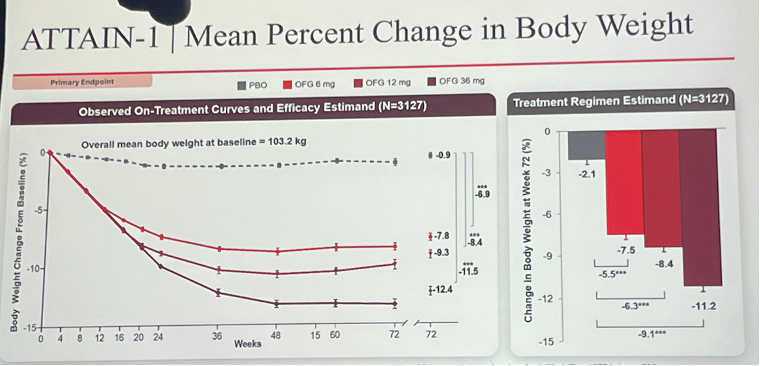
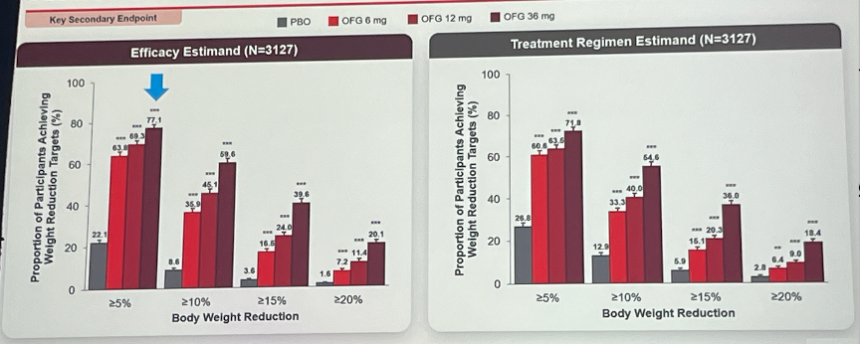
- Safety. Overall, adverse events occurred mainly during dose escalation period and were mostly mild-to-moderate. Adverse events were more frequent with orforglipron than placebo. Most common events included nausea (29-36% vs. 10% with placebo), constipation (22-30% vs. 9%), diarrhea (21-23% vs. 10%), and vomiting (13-24% vs. 4%). Discontinuations due to GI events were higher with increasing dose: 10%, 8%, 5%, and 3%, respectively. There were three deaths in placebo and treatment groups due to pulmonary embolism, cardiac death, and ovarian cancer, all deemed unrelated. Finally, investigators found no liver safety signals. Overall, the safety profile was consistent to the GLP-1 RA class.
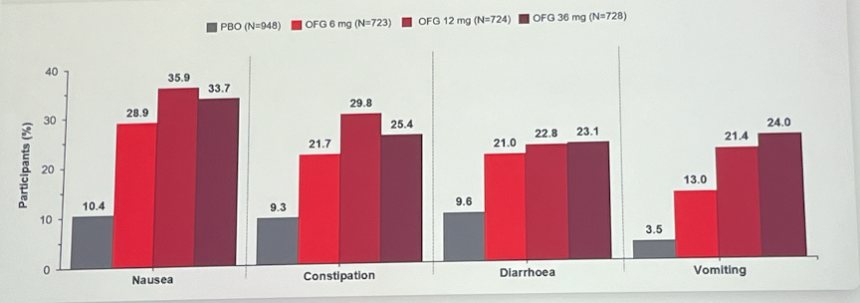
- Dr. Vanita Aroda (Brigham and Women’s Hospital) shared an independent commentary, emphasizing the importance of patient-centered care. Dr. Aroda reviewed two decades of progress in incretin-based therapies, from exenatide in 2005 to semaglutide in 2017, oral semaglutide in 2019, and tirzepatide in 2022, which have gradually improved on efficacy and cardiorenal protection. She positioned orforglipron to be the next marker of the timeline as the first oral small molecule GLP-1 RA, which are easy to take with fewer intake restrictions. She also pointed out that the ATTAIN-1 trial enrolled a broadly representative population, with an average age in the 40s and gender and racial diversity, and offered structured lifestyle counseling for all arms, as evident in placebo group losing 0.9% of body weight.
- Dr. Aroda underscored that the trial could have been more patient-oriented with patient-reported outcomes and more flexible titration scheme or maintenance dosage. She walked the audience through trial participants’ journeys during the ATTAIN-1, noting how participants in the placebo group would have had to refrain from getting additional therapies during a year and half of the study, while those in the treatment group might have been pushed to get unnecessarily higher dosage, leading to high GI event and discontinuation rates. She pointed out that there have been significant media attention with numerous headlines about weight loss expectations and investment but said that the only headline should be, “It’s about the Patient.”
- During Q&A, panelists suggested future studies to capture patient-reported outcomes, use active comparators or long-term extensions, and explore lower BMI cut-offs for non-white populations so that effective therapies reach those at risk earlier.
Phase 3 REDEFINE 2 trial: CagriSema significantly increases Time in Range in people with obesity and T2D, per secondary analysis
In this packed session, Dr. Richard Pratley (AdventHealth) presented secondary analysis (n=199) of the phase 3 REDEFINE 2 trial (n=1,206) about glycemic trends as measured by CGM. As background, the REDEFINE 2 trial evaluated CagriSema (fixed combination of cagrilintide 2.4 mg and semaglutide 2.4 mg) in people with overweight or obesity and T2D, compared to placebo alone. As announced at ADA 2025, CagriSema conferred 15.7% weight loss (vs. 3.1% with placebo) and 2.1% reduction in A1c (vs. no change) in trial product estimand, which assumes CagriSema was taken as intended. The secondary analysis investigated how CagriSema affected CGM metrics in the subgroup who underwent CGM.
- Study design and baseline characteristics. ~200 participants were selected from US sites as a CGM subgroup. These participants had 20-day double-blind glycemia readings with Dexcom G6 Pro for three 20-day periods at Weeks 0, 24, and 68 (see figure below). Change in CGM metrics – including TIR (70-180 mg/dL), Time above Range (TAR; level 1 >180 mg/dL, level 2 >250 mg/dL), Time below Range (TBR; level 1 <70 mg/dL or level 2 <54 mg/dL), and Time in Tight Range (TITR; 70-140 mg/dL), as well as within-day glucose variability and achievement of composite endpoint (>70% TIR and <4% TBR) – were analyzed between those taking CagriSema (n=149) or placebo (n=50).
- At baseline, CagriSema and placebo group were well-balanced. Participants were 60 years old, with 47% being female and 80% white, 13% Black, and 3% Asian. Clinically, participants had average A1c of 8%, mean diabetes duration of 10 years, and body weight of 104 kg (229 lbs). Approximately 22% were on sulfonylureas and 23% on SGLT-2 inhibitors.
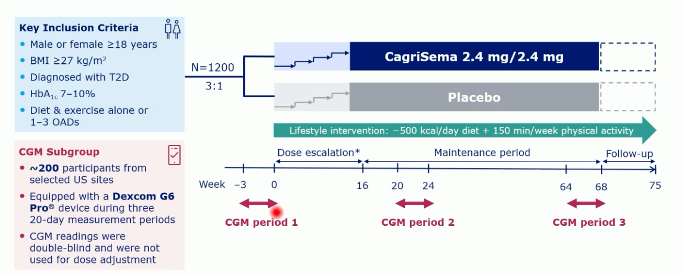
- Results. CagriSema doubled TIR from 44% at baseline to 89% at Week 68, reflecting 10 hours and 55 minutes more spent in TIR each day (see figure below). This compares to placebo, which increased TIR from 41% to 53%, up two hours and 48 minutes per day. CagriSema increased TITR over four-fold from 15% to 65%, up 12 hour per day with CagriSema, compared to placebo, which increased by one hour and 39 minutes per day. CagriSema drastically reduced TAR while keeping TBR <1%. Dr. Pratley said that this suggests a favorable safety profile. Despite large glycemic improvements on a background of sulfonylureas in 22% of participants, hypoglycemia events were minimal. During Q&A, he clarified that earlier phase 2 data suggest both cagrilintide and semaglutide produced glycemic improvements individually, with cagrilintide thought to mitigate postprandial hyperglycemia and reduce glucose variability.
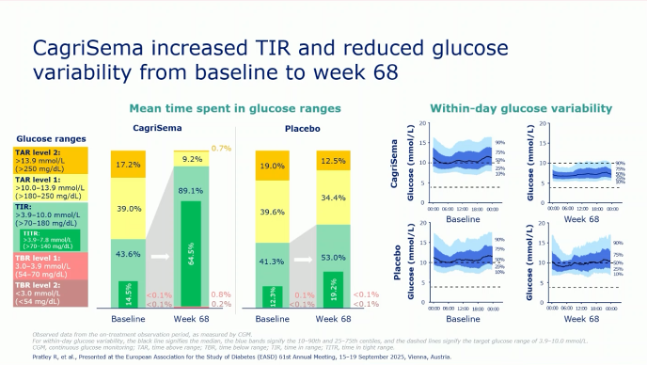
- When stratified by weight loss (<10%, 10-15%, 15-20%, and ≥20%), improvements in TIR, TITR, and within-day glucose variability were more prominent among those with greater weight loss (see figure below). Finally, 84-92% of participants on CagriSema achieved the composite endpoint (≥70% TIR and <4% TBR) across all weight loss categories, as shown in the figure below. Percentage was highest (92%) in the 10-15% weight loss group and lowest (82%) in the <10% weight loss group.
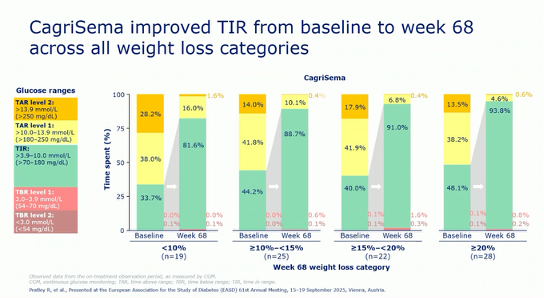
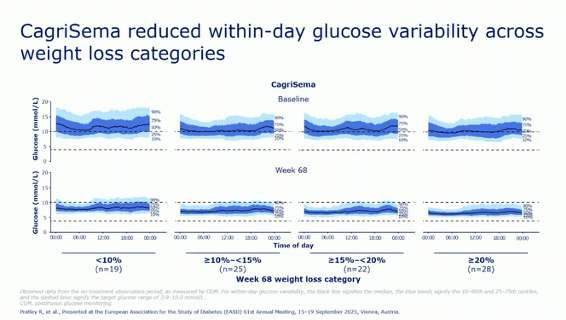
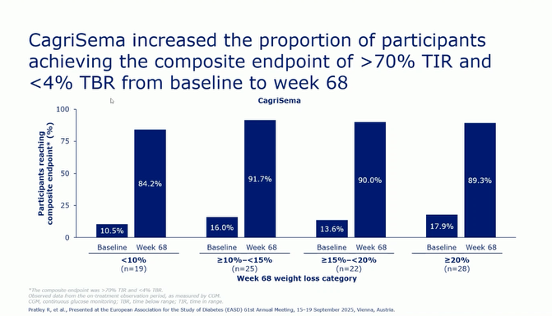
TIRTLE1 T1D trial shows that Lilly’s once-weekly GLP-1/GIP tirzepatide reduces weight (9%) and insulin dose (33%) and improves body composition
In a morning oral session, Dr. Jennifer Snaith (Garvan Institute of Medical Research, Australia) presented results from the phase 2 TIRTLE1 trial (n=24) of tirzepatide in adults with T1D. Two-thirds of adults with T1D live with overweight or obesity, facing increased risks of CVD and mortality. While insulin is currently the only treatment approved for T1D, studies like DCCT-EDIC have shown that insulin leads to increased metabolic syndrome and weight gain, which blunts the CV benefits of glycemic management. Treatments like tirzepatide have shown efficacy in T2D, improving weight management and reducing insulin resistance. Although tirzepatide is not yet approved in T1D, there’s been increasing off-label use in this population. Therefore, the TIRTLE1 trial studied the impact of low-dose tirzepatide on body weight in adults with T1D and obesity. Overall results showed that even at low doses, tirzepatide supports weight management in adults with T1D and obesity. The ongoing phase 3 SURPASS-T1D (n=905) will further build on these results with a longer duration of study.
- Study design. The trial included adults who had a T1D diagnosis for more than two years and a BMI of at least 30 kg/m2. They were randomized 1:1 to receive weekly subcutaneous tirzepatide (2.5 mg for four weeks; 5 mg after or maximum tolerated dose) or placebo for 12 weeks. Interventions were provided with phone support, helping with insulin titration based on glucose level response. The primary endpoint was the change in body weight; secondary outcomes included change in insulin dose, A1c levels, diet features, and body composition.
- Baseline characteristics. Trial participants had a mean age of 41 years, BMI of 34 kg/m2, A1c 7.3%, and TIR 65%. The median total daily dose of insulin was 69 units/day. Additionally, 42% of participants were female, 13 were on an insulin pump, and 11 administered multiple daily injections.
- Weight loss. After 12 weeks, tirzepatide demonstrated a significant body weight reduction of 10 kg (23 lbs), compared to 0.7 kg (1.5 lbs) with placebo (mean difference of 8.7 kg [19 lbs]; p<0.001). Overall, tirzepatide conferred an 8.8% weight loss, with all participants achieving ≥5% weight loss and 45% achieving ≥10% weight loss.
- Dr. Snaith said these results are comparable to other trials, including: (i) SURMOUNT-1 (n=2,539) of tirzepatide in people with obesity, in which 85% of participants achieved ≥5% weight loss and 69% achieved ≥10% weight loss; and (ii) SURPASS-5 (n=475) of tirzepatide in people with T2D treated with insulin, in which 56% of participants achieved ≥5% weight loss and 24% achieved ≥10% weight loss.
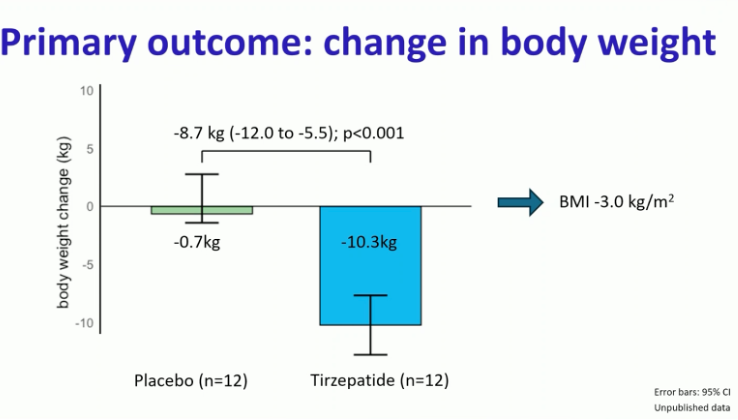
- Body composition. Tirzepatide significantly reduced 7.2 kg (19 lbs) more fat mass compared to placebo (p=0.0002). Tirzepatide also numerically reduced 1.8 kg (4 lbs) more fat-free mass compared to placebo (p=0.06). Overall, fat mass loss accounted for 80% of total mass loss, while fat free mass accounted for 20%.
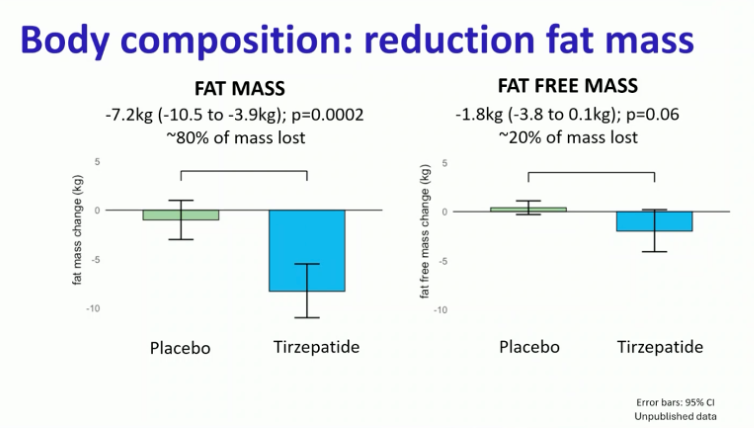
- Glycemic levels. The mean A1c change from baseline for tirzepatide was 0.5% A1c, compared to 0.2% for placebo (mean difference of 0.4%; p=0.05). The mean improvement in TIR from baseline was 3.2% for tirzepatide, compared to 2.6% for placebo (mean difference of 8.4%; p=0.17). The mean improvement in TBR was 1.6% for tirzepatide and a reduction of 0.3% for placebo (mean difference of 1.8%; p=0.17).
- Insulin dose. Dr. Snaith emphasized that the degree of reduction in insulin doses was quite surprising. Tirzepatide demonstrated a 25% reduction in basal insulin dose (p=0.002) and 49% reduction in bolus insulin dose (p=0.008), compared to placebo. Importantly, an exploratory analysis of pump users showed that acute changes in insulin dose appeared early in the trial, before weight loss was seen. The change in total daily insulin dose was significant at Week 6 and sustained at Week 12. Reflecting on these results, Dr. Snaith suggested that the effect of tirzepatide on insulin doses may hint at the treatment effects on insulin sensitivity in T1D with potential weight-independent mechanisms.
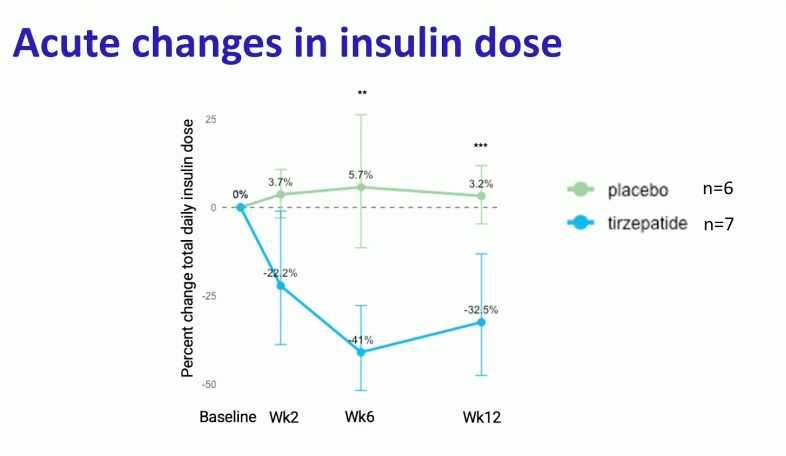
- Adverse events. Participants in neither the tirzepatide nor the placebo group experienced serious adverse events. However, 75% of participants in the tirzepatide group and 8% in the placebo group experienced non-serious adverse events that were mostly related to GI effects, aligning with the overall profile of GLP-1 RAs.
- Patient-reported outcomes. Dr. Snaith was eager to share that all participants on tirzepatide noted that the treatment helped them address their diabetes management, compared to 37% in the placebo group. The difference in treatment satisfaction score between the tirzepatide and placebo group was: (i) 2.1 for preventing weight gain; (ii) 1.8 for preventing high glucose levels; (iii) 1.5 for reducing units of insulin needed per day; and (iv) 1.6 for improving mental fatigue and emotional distress.
Incretin-associated sarcopenia: Does it matter which treatment?
In an engaging debate, Prof. Gabriele Riccardi (Federico II University, Italy) and Prof. Martin Haluzík (Diabetes Center of the Institute for Clinical and Experimental Medicine, Czech Republic) discussed whether incretin treatments (i.e., GLP-1 RA semaglutide or GIP/GLP-1 RA tirzepatide) impact sarcopenia differently. Throughout the debate, both Prof. Riccardi and Prof. Haluzík agreed that the loss of fat free mass with incretin treatment is an expected outcome, representing the mechanism of body composition. Prof. Riccardi referenced the relationship between weight reduction and loss of lean body mass in the context of different strategies (e.g., diet and bariatric surgery). Like what’s seen with incretin treatments, weight loss with various interventions all lead to a reduction in lean body mass because of a compensatory mechanism. However, the degree to which incretin treatment impacts body composition is not clear and has raised concerns about whether the type of treatment for weight loss matters. To address this question, Prof. Riccardi argued that sarcopenia doesn’t depend on the treatment but rather the degree of weight loss, and Prof. Haluzík argued that it is a dependent relationship.
- Prof. Riccardi explained that sarcopenia doesn’t depend on the treatment and instead, depends on the degree of weight loss. Comparing separate trials, Prof. Riccardi showed that tirzepatide confers a greater degree of weight loss than semaglutide (average of 5 kg [11 lbs] difference). However, aside from this difference, the lean mass loss amounts to 24% of body weight reduction for semaglutide, which is comparable to the results seen with tirzepatide. In a trial directly comparing tirzepatide and semaglutide, the percentage of muscle loss was found to be similar between the two groups (32% vs. 35%).
- Additionally, Prof. Riccardi emphasized that body weight reduction does not always indicate a reduction in function. In fact, the SURMOUNT-1 trial of tirzepatide showed that people not only experienced weight loss but also demonstrated greater scores in physical function. Prof. Riccardi attributed this improvement to the fact that weight reduction eliminates fat, which also improves insulin resistance and metabolic profiles.
- Considering these results, Prof. Riccardi argued that the risk of sarcopenia depends on the degree of weight loss and not on the type of incretin treatment, especially in elderly people without overweight or obesity. He also reminded the audience that muscle mass loss is an indirect marker of muscle strength.
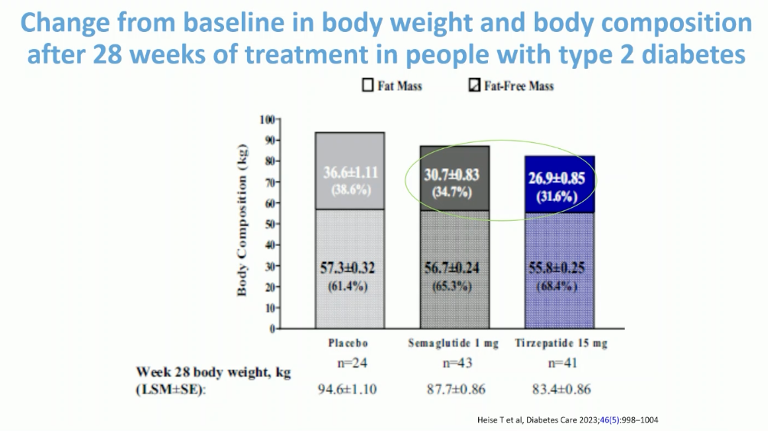
- Prof. Haluzík argued that sarcopenia depends on the type of incretin treatment. Contrasting the mechanisms of GLP-1 and GIP receptor agonism, Prof. Haluzík highlighted an important distinction that GIP RAs are only present in subcutaneous white adipose tissue. This difference may explain the greater degree of weight loss seen with tirzepatide compared to semaglutide, as the GIP component of tirzepatide acts more potently on skeletal mechanisms. Furthermore, Prof. Haluzík returned to the same trial Prof. Riccardi previously referenced, which showed similar muscle loss between tirzepatide and semaglutide. Prof. Haluzík interpreted the results differently and explained that because tirzepatide achieves greater total weight and fat loss, tirzepatide relatively has more effective preservation of lean mass. He also claimed that the mechanistic differences could help tirzepatide selectively target fat tissue.
Phase 2b COURAGE trial: Regeneron’s trevogrumab help preserve 50-80% of lean mass lost with semaglutide alone
Regeneron Pharmaceuticals’ Dr. Ofri Mosenzon (Senior Medical Director) presented primary analysis of the ongoing phase 2b COURAGE trial (n=1,005), which evaluates the effects of trevogrumab (anti-GDF8/anti-myostatin) with or without garetosmab (anti-activin A) on weight loss quality in people with obesity, when combined with Novo Nordisk’s semaglutide (GLP-1 RA). Topline results for the interim 26-week period were announced in June 2025, demonstrating that the combination therapy help preserve 50-80% of lean mass lost with semaglutide alone.
As background, myostatin and activin A are key ligands for the ActRIIa/b receptor (see figure below) that negatively regulates muscle mass. Trevogrumab and garetosmab are monoclonal antibodies against myostatin and activin A, respectively. These candidates aim to preserve lean body mass, which has been shown to account for 15-45% of total weight loss from incretin-based therapies like semaglutide, liraglutide, or tirzepatide.
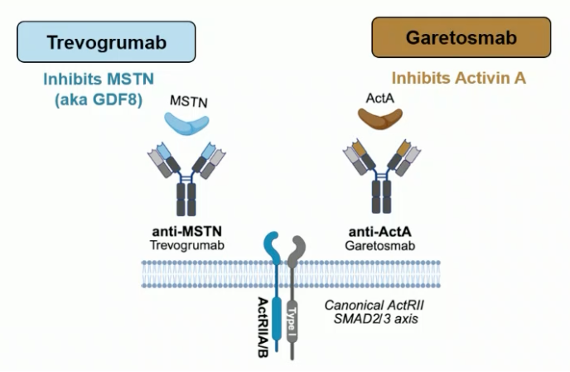
- Trial design and baseline characteristics. The trial is organized in two parts across multiple combinations of therapies and placebo: (i) weight loss phase; and (ii) weight maintenance phase. Participants (n=605) were randomized to receive semaglutide alone or in combination with two different doses of trevogrumab (100 mg or 200 mg), with or without garetosmab 10 mg/kg. Primary endpoints include change in total lean and fat mass, as measured by DXA, and total weight loss from baseline to Week 26. Secondary and exploratory endpoints included change in waist circumference, blood pressure, lipid levels, and safety profile. At baseline, participants were 49 years old, with 68% being female, 73% white, and 20% Black. Clinically, participants had average weight of 102 kg (225 lbs), BMI 36.7 kg/m2, waist circumference of 113 cm (44 inches), and A1c of 5.7%. Total fat and lean mass were 45 kg (99 lbs) and 53 kg (117 lbs), respectively.
- Results. Trevogrumab, with or without garetosmab, significantly preserved lean mass loss and increased fat mass loss. As shown in the figures below, the triple combination therapy preserved the lean mass loss the most, resulting in 2% reduction from baseline (vs. 3% with dual combination therapy and 7% with semaglutide alone). Similarly, the triple combination therapy conferred greatest fat mass loss (27%), compared to semaglutide with trevogrumab (19%) and semaglutide alone (16%). Likewise, triple combination therapy achieved greatest weight loss (13%), followed by semaglutide with trevogrumab (11%) and semaglutide alone (10%). By weight loss quality, 7% of total weight loss was from lean mass in the triple therapy group, compared to 18% from semaglutide with trevogrumab and 33% from semaglutide alone.
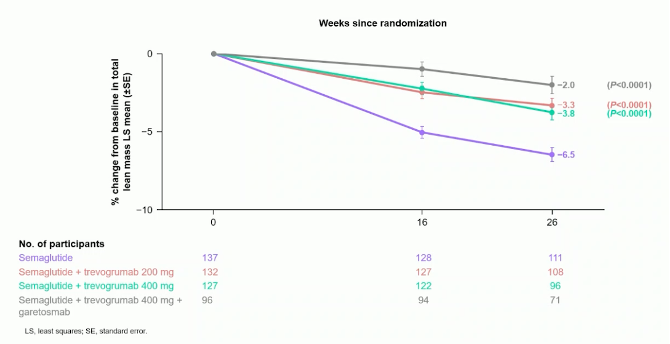
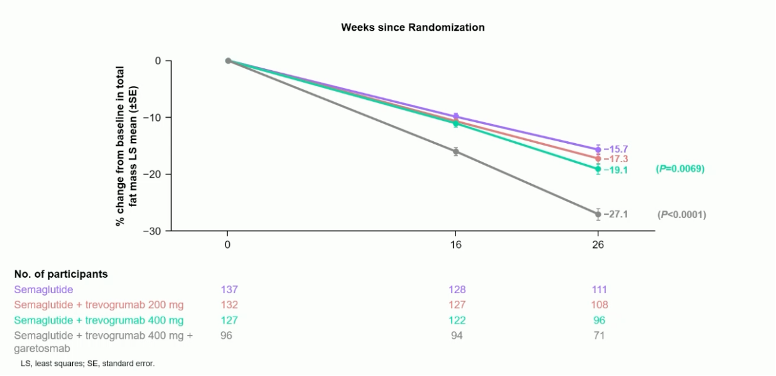
- Mono and combination therapies improved cardiometabolic biomarkers. Mono, dual, and triple therapies reduced waist circumference (10, 11, and 12 cm in, respectively), hsCRP (38%, 44%, and 52%), systolic blood pressure (6.2, 6.3, and 5.6 mmHg), A1c (0.34, 0.35, and 0.42), total cholesterol (13%, 12%, and 10%), and LDL cholesterol (17%, 15%, and 9%). While most reductions were statistically insignificant across groups, A1c reduction was significantly greater in triple combination therapy compared to monotherapy (p=0.003). On the other hand, LDL cholesterol reduction was significantly higher in the monotherapy group (p=0.003).
- Safety. Overall, trevogrumab, with or without garetosmab, added to semaglutide, was generally well-tolerated (see figure below). Dr. Mosenzon pointed out that severe adverse events were highest in the triple combination group (9%), compared to dual (1%) or monotherapy (1%). Similarly, treatment discontinuation was highest among the triple combination group (31%), compared to dual (11%) and monotherapies (5%). Muscle spasms were most common in the triple therapy group (41%), compared to dual (9%) and monotherapies (5%). GI-side effects were second-most common and was consistent across groups. See more details in the figure below.
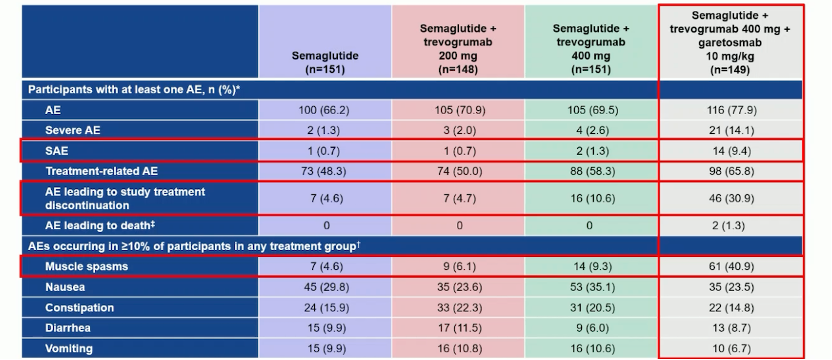
Amycretin demonstrates favorable pharmacokinetics, safety, and tolerability in people with renal impairment
In a popular afternoon session, Novo Nordisk’s Dr. Sine Haugaard (Principal Clinical Pharmacology Specialist) presented how renal impairment affects pharmacokinetic, safety, and tolerability of amycretin. As background, amycretin is Novo Nordisk’s once-weekly subcutaneous GLP-1/amylin RA investigated for obesity, T2D, and comorbidities. The phase 2b trial (n=125), presented at ADA 2025, found that amycretin conferred 9.7%, 16%, and 22% weight loss after a 12-week maintenance period with the 1.25 mg, 5 mg, and 20 mg doses, respectively. In the multiple ascending dose part of the trial, people on the 60 mg amycretin dose achieved a weight loss of 24% at 36 weeks. This interventional single-center, open-label, single-dose study (n=42) assessed amycretin in people with varying renal function.
- Trial design and baseline characteristics. Participants with normal (n=14; eGFR ≥90 mL/min), mild (n=7; eGFR 60-89 mL/min), moderate (n=7; eGFR 30-59 mL/min), severe renal impairment (n=7; eGFR <30 mL/min), and end-stage kidney disease (n=7; dialysis) received a single injection of subcutaneous amycretin 0.3 mg and were followed until Day 28. At baseline, participants were between 47-62 years old on average across the groups. Mean body weight ranged from 81-94 kg (179-207 lbs), and mean BMI ranged from 27-31 kg/m2. See more details on baseline characteristics below.
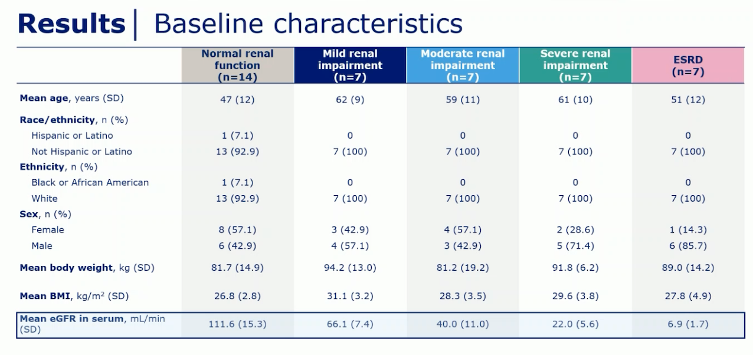
- Results. Half-life tended to be slightly longer with higher degrees of renal impairment (88, 94, 111, 113, and 110 hours, respectively). Other pharmacokinetic parameters were unimpacted by the degree of renal impairment. Dr. Haugaard said this suggests that dose adjustment is not required for people with advanced stages of kidney disease. Overall, amycretin was well-tolerated across all groups with similar safety profile as other GLP-1 and amylin RAs. More specifically, treatment-emergent adverse events ranged from 57-86%, with mild renal impairment experiencing lowest and end-stage kidney disease experiencing highest rates. Most adverse events were mild-to-moderate in severity and resolved by the end of study.
Pooled analysis of SOUL, FLOW, and STRIDE: Semaglutide reduces major adverse limb events by 30% compared to placebo
In a crowded morning symposium, Dr. Subodh Verma (University of Toronto, Canada) presented a pooled analysis (n=13,975) of the SOUL, FLOW, and STRIDE trials[2], evaluating the impact of semaglutide on major adverse limb events (MALE) compared to placebo. Dr. Verma began that peripheral artery disease (PAD) is common in diabetes, affecting ~200 million individuals globally, and increases risks of comorbidities, such as ulcers, amputations, cardiovascular (CV) events, and functional decline, including frailty, social isolation, and depression. However, in the last 25 years, there were no durable diabetes therapy to reduce limb events. In each of the three trials included in the analysis, investigators noticed trends that semaglutide reduced MALE by 29%-46% regardless of PAD history. Hence, the study aimed to assess the effects of semaglutide on MALE, as well as composites of MALE and CV events, in people with T2D.
- Study design and baseline characteristics. MALE was defined by an independent committee based on prespecified criteria for hospitalization for acute or chronic limb ischemia requiring revascularization, amputation, or pharmacotherapy. At baseline, participants were 67 years old, with 71% being male. Clinically, mean A1c was 7.7%, BMI 30 kg/m2, eGFR 67 mL/min/1.73 m2, and LDL-cholesterol 2 mmol/L. The vast majority (92%) had hypertension, and 61% had coronary artery disease. 6% had lower extremity revascularization. The majority of participants were on lipid-lowering therapies (86%), ACEi/ARB (83%), and antiplatelets (70%). 25% were on SGLT-2 inhibitors.
- Results. Semaglutide was associated with 30% relative risk reduction (p=0.0072), with a total of 132 events in the placebo group and 93 events in the semaglutide group. Hazard ratio for time to first hospitalizations for chronic limb ischemia was 0.72 (p=0.019), suggesting semaglutide’s benefits in lowering hospitalizations. Participants with baseline PAD experienced greater MACE than those without, which is expected. Semaglutide reduced MALE regardless of baseline PAD by 31%, although absolute risk reduction was greater in those with baseline PAD. Finally, for composite endpoints, semaglutide consistently achieved significant risk reduction in MALE or all-cause death (HR=0.85), MALE or CV death (HR=0.82), MALE or major adverse cardiovascular outcomes (MACE; HR=0.83).
- Ultimately, Dr. Verma highlighted that semaglutide is the first pharmacotherapy to reduce limb events in people with T2D, regardless of PAD at baseline, and supplements the STRIDE trial results, which found improved functional capacity, maximum walking distance, with semaglutide. Dr. Verma further clarified that these benefits do not appear to be mediated solely by glycemic or weight changes. STRIDE enrolled patients who were not necessarily overweight, and benefits on ankle-brachial index were observed early before significant A1c or weight reductions, suggesting that semaglutide may have independent vascular-protective or microvascular perfusion effects. More detailed results around amputation types and other causes will be presented at AHA 2025.
Real-world study finds semaglutide is associated with 23% reduced MACE compared to dulaglutide in people with T2D and CVD
In this packed symposium, Dr. Xi Tan (Novo Nordisk) presented results of the REACH real-world study (n=58,336), which compared semaglutide to dulaglutide on the risk of major adverse cardiovascular events (MACE) among people with T2D and atherosclerotic cardiovascular disease (ASCVD).The results were also announced in Novo Nordisk’s simultaneous press release.
- Study design and baseline characteristics. The observational cohort study used Medicaid claims data from 2006-2022 to conduct a target trial emulation. Adults 66 years or older with T2D and ASCVD who initiated semaglutide or dulaglutide between the study period were 1:1 propensity score matched. At baseline, participants were 73 years old, with 61% being male, 89% white, 5% Black, and 1% Asian. Clinically, participants had T2D for an average of seven years and ASCVD for six years. While investigators did not restrict the analysis by dosing, Dr. Tan noted that dosage were likely limited by the coverage plans. Specifically, less than 5% of the semaglutide group were treated with 2 mg, with most reaching 1 mg dose. For the dulaglutide group, 15% were on higher dose (3 mg and 4.5 mg), while 85% were on lower dose (1.5 mg or less).
- Results. Semaglutide was associated with associated with 23% reduced risk of three-point MACE (ischemic stroke, myocardial infarction [MI], and all-cause death), compared to dulaglutide (p<0.001). Likewise, semaglutide had 25% lower risk of five-point MACE (ischemic stroke, MI, unstable angina, heart failure, and all-cause death), compared to dulaglutide (p<0.001). By individual MACE events, semaglutide was statistically significantly associated with 35% reduction of ischemic stroke and 26% reduction of all-cause death than dulaglutide. The risks of myocardial infarction were not statistically significant. Investigators found consistent results with US commercial insurance and Medicare Advantage population when adjusting for A1c and BMI. Ultimately, Dr. Tan emphasized that CV benefits of semaglutide is molecule-specific and cannot be assumed across the total GLP-1 RA class. She shared that these results could inform clinicians and policy decisions amid rising GLP-1 RA use and ongoing Medicare price negotiations. During Q&A, when asked about SURPASS-CVOT, which demonstrated noninferior CV benefits of tirzepatide to dulaglutide, Dr. Tan said REACH is a real-world study which has intrinsic differences from RCTs; direct comparison of CV benefits between semaglutide and tirzepatide warrants a head-to-head trial.
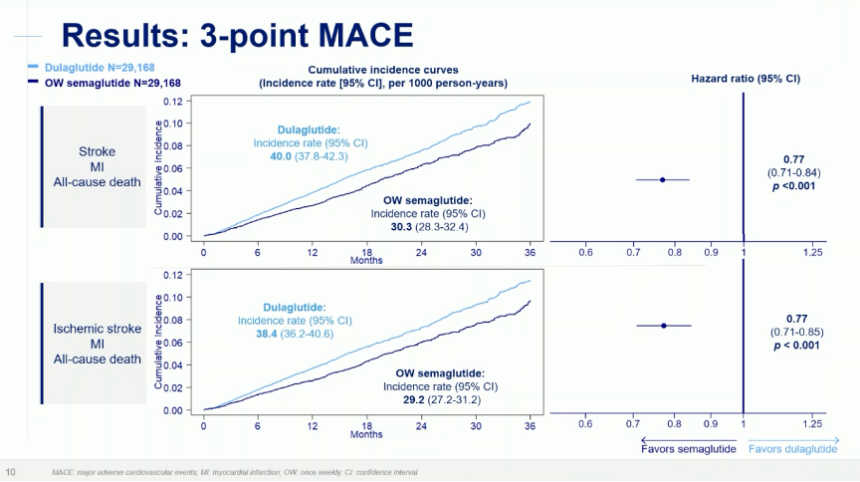
Zealand’s once-weekly dual GLP-1/GLP-2 RA dapiglutide confers up to 8% weight loss at Week 13
Zealand’s Mr. Mark Krogh Hvistendahl (Clinical Pharmacology Scientist) presented results of the 13-week phase 1b multiple ascending dose trial (n=54) of once-weekly dual GLP-1/GLP-2 RA dapiglutide. The results follow topline results presented in September 2024, which found placebo-adjusted weight loss of up to 8.3% with dapiglutide. Furthermore, dapiglutide, with doses up to 13 mg, was considered safe and well-tolerated with GI adverse events consistent with other incretin-based therapies. As background, dapiglutide is derived from a GLP-2 peptide backbone with GLP-1 activity added via amino acid substitutions. He explained that the GLP-1 component reduces body weight, while GLP-2 is designed to improve intestinal barriers and provide additional anti-inflammatory effects to address obesity and low-grade inflammation-derived comorbidities.
- Trial design. The Part 1 of the trial, involving dose escalation every two weeks, enrolled 55 adults with overweight or obesity but not diabetes. Within three dose cohorts (target maintenance doses of 7.5 mg, 10 mg, and 13 mg weekly), participants were randomized to placebo or dapiglutide. Because the trial involved 13 weeks of follow up, participants receiving higher doses remained on the maintenance dose for shorter periods. While the presentation was only about Part 1 of the trial, Part 2 is evaluating a slower escalation scheme every four weeks and higher doses up to 26 mg for 28 weeks. At baseline, participants were 46 years old, with 85% male. Clinically, participants had a relatively low body weight of 95 kg (209 lbs) and a BMI of 30 kg/m2.
- Results. All doses of dapiglutide conferred weight loss, compared to placebo. Specifically, dapiglutide 10 mg resulted in 8.3% weight loss compared to 2% increase in placebo at Week 13. Investigators did not observe changes in anti-inflammatory biomarkers (hsCRP, LPS-binding protein) because participants had low baseline levels. However, Mr. Hvistendahl shared that future studies will recruit individuals with higher inflammation to test this hypothesis. Mean systolic blood pressure decreased by ~5 mmHg compared to baseline. Finally, pharmacokinetics confirmed once-weekly dosing as optimal.
- Safety. Dapiglutide showed a dose-dependent increase in treatment-emergent adverse events (primary endpoint of the trial), with most being mild. There was only one serious adverse event – a miscarriage in the 10 mg group – deemed unrelated to study drug. Most events were GI-related (86% in 13 mg group vs. 42% in placebo), including nausea (71% vs. 8%), vomiting (43% vs. none), and diarrhea (43% vs. none), consistent with incretin-based therapies. Decreased appetite reported as an adverse event (71% vs. none) reflects on-target efficacy.
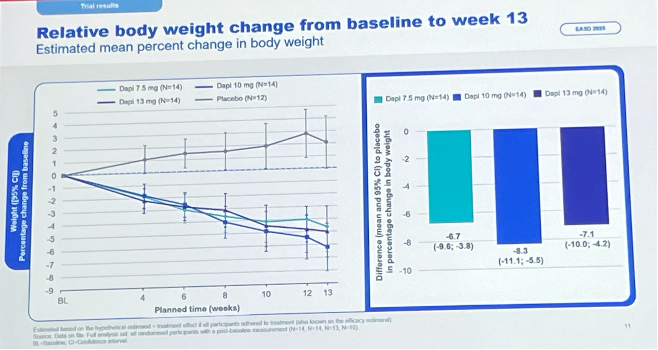
Full results of SURPASS-CVOT: Tirzepatide reduces MACE numerically by 8%
In a jam-packed symposium full of excitement (in addition to thousands of online viewers), the long-anticipated phase 3 SURPASS-CVOT (n=13,299) results were delivered. The phase 3 SURPASS-CVOT is a head-to-head cardiovascular outcomes trial (CVOT) comparing Mounjaro (tirzepatide) to Trulicity (dulaglutide) in people with T2D and established cardiovascular disease (CVD). Topline results from July 2025 showed that tirzepatide was noninferior to dulaglutide in reducing the risk of major adverse cardiovascular events (MACE-3; composite of CV death, heart attack, or stroke). Drs. Stephen Nicholls (Monash University, Australia), David D’Alessio (Duke University), and Sophia Zoungas (Monash University, Australia) presented cardiovascular (CV), glycemic, and renal outcomes, respectively, followed by Dr. Hertzel Gerstein (McMaster University, Canada), who shared an independent commentary.
At three years, tirzepatide numerically reduced MACE-3 risk (CI: 0.83-1.01, p=0.086) by 8% compared to dulaglutide. When further analyzed with phase 3 REWIND CVOT (n=9,901), in which dulaglutide demonstrated a 12% MACE reduction (CI: 0.89-0.99, p=0.026) and numeric 10% reduction in all-cause mortality (CI:0.80-1.01, p=0.067), tirzepatide conferred significant risk reductions of MACE-3 by 28% and all-cause mortality by 39% compared to putative placebo. Tirzepatide conferred significantly greater improvements in A1c (1.7 vs. 0.9 percentage points from 8.4% at baseline), body weight (12% vs. 5% from 92.6 kg or 204 lbs), triglycerides (24% vs. 10% from 166 mg/dL), and systolic blood pressure (6.5 vs. 4.2 mmHg), compared to dulaglutide. On the primary renal outcome, tirzepatide significantly reduced 19% in overall and 22% in high-risk population, compared to dulaglutide.
- Study design. The primary object of this four-year, global, head-to-head comparison trial was to assess whether tirzepatide was noninferior to dulaglutide in reducing cardiovascular risks. The trial included 13,299 adults with over 40 years of T2D diagnosis, established CVD, and BMI ≥25 kg/m2, who were randomized to take dulaglutide 1.5 mg (reflecting REWIND trial design) or tirzepatide (15 mg or maximum tolerated dose). Noninferiority threshold for tirzepatide to dulaglutide was defined as HR with an upper bound of <1.05 for the 95.3% confidence interval to ensure tirzepatide’s superiority to a putative placebo.
- Baseline characteristics. At baseline, participants were an average 64 years old, with 29% being female, 81% white, 9% Asian, and 30% Hispanic or Latino. Clinically, participants had a mean body weight of 93 kg (205 lbs), BMI of 32.6 kg/m2, and A1c of 8.4% (see more in the table below). For baseline medication use, the vast majority was on a statin (86%) and metformin (81%); 40% were on an ACEi/ARB, 30% on SGLT-2 inhibitors, 22% on sulfonylureas, 6% on DPP-4 inhibitors, and 49% on insulin.
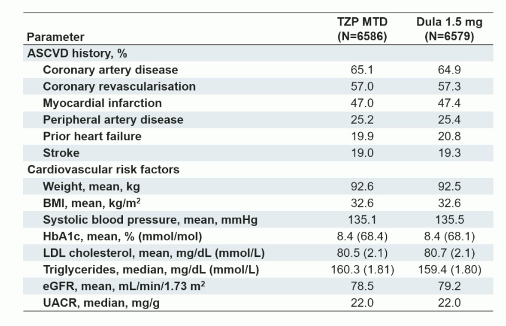
- Cardiovascular outcomes. Tirzepatide was statistically noninferior to dulaglutide, numerically reducing the risk of primary endpoint by 8%. (HR=0.92; p=0.003). P-value for the superiority was 0.086, which did not meet the prespecified threshold. Strikingly, tirzepatide significantly reduced the all-cause death by 16% among other key secondary endpoints (see table below). Dr. Nicholls noted that tirzepatide led to reduction of non-CV deaths, as well, predominantly related to infection. The benefits were consistent across sex, age, BMI, A1c, duration of T2D, CVD history, and SGLT-2 inhibitor use.
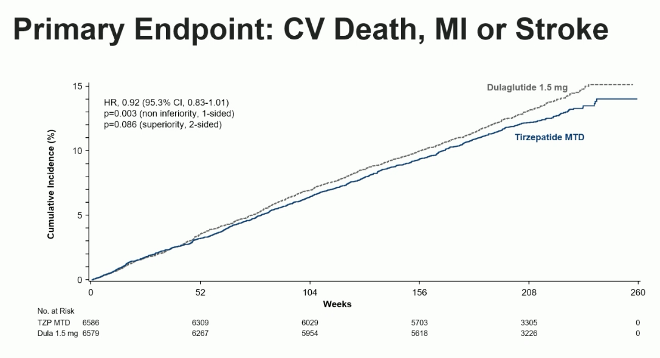
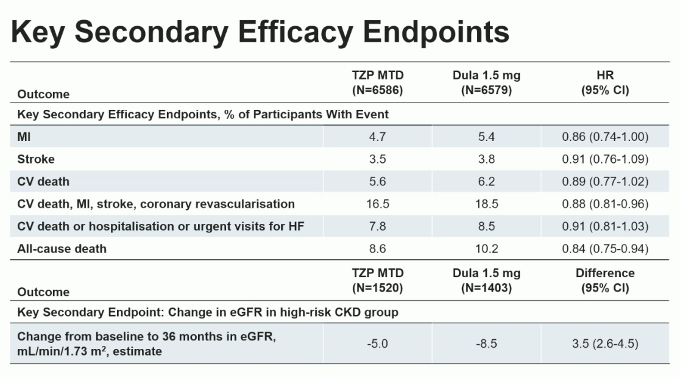
- Compared to a putative placebo, tirzepatide had 28% reduction in three-point MACE (CV death, MI, stroke) and 39% reduction in all-cause death. Using these results, investigators conducted a pre-specified indirect estimate of tirzepatide’s CV benefits over placebo, based on the phase 3 REWIND CVOT (n=9,901), in which dulaglutide demonstrated a 12% MACE reduction compared to placebo. In this analysis, only a subgroup of the REWIND trial that meet the trial eligibility criteria of SURPASS-CVOT was included. Tirzepatide confirmed cardioprotective effects – see full results below.
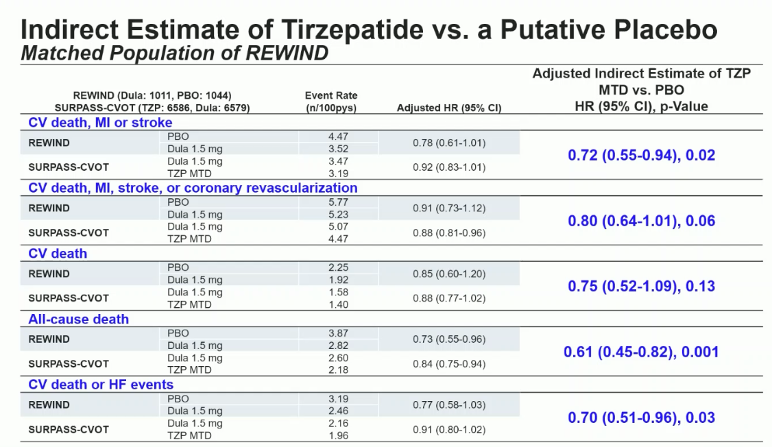
- Safety. Overall, rates of treatment-emergent adverse events were similar across the two treatments. Tirzepatide had moderately higher rates of GI events, including nausea (25% vs. 22%), diarrhea (25% vs. 19%), and decreased appetite (17% vs. 9%).
Additional results of SURPASS-CVOT: Tirzepatide significantly reduces weight and glycemic outcomes
Continuing the discussion, Drs. David D’Alessio (Duke) and Sophia Zoungas (Monash University, Australia) presented glycemic, metabolic, and renal outcomes.
- Glycemic and metabolic outcomes. Tirzepatide conferred significantly greater improvements in A1c, body weight, lipids, and blood pressure, compared to dulaglutide. Specifically, at Week 260, tirzepatide reduced A1c by 1.7 percentage points (vs. 0.9 percentage points with dulaglutide) from baseline of 8.4%. Tirzepatide group achieved 12% reduction in body weight (vs. 5%) from baseline of 92.6 kg (204 lbs). Significantly greater proportion of participants achieved A1c and weight loss targets (see figure below): for example, 82% on tirzepatide (vs. 45%) achieved A1c <7.0%, and 60% of tirzepatide group (vs. 11%) achieved weight loss ≥10%. Subgroup analysis confirmed that tirzepatide consistently reduced A1c and body weight regardless of sex, age, T2D duration, baseline A1c, BMI, or SGLT-2 inhibitor use.
- Hypoglycemia. Consistent with other incretin-based therapies, both tirzepatide and dulaglutide groups experienced slight increase in hypoglycemia in the first year of the trial but abated over time. Dr. D’Alessio said that this was due to adjustments in titration for sulfonylurea or insulin; participants without baseline use of these medications experienced minimal hypoglycemia rates.
- Lipid and blood pressure. Finally, both tirzepatide and dulaglutide improved lipid levels and blood pressure. Specifically, tirzepatide conferred significantly greater reduction in triglycerides by 24% (vs. 10%) from baseline of 166 mg/dL. LDL cholesterol decreased modestly in both groups but was not statistically different (1.7% vs. 2.5% from baseline of 72 mg/dL). Reductions in systolic (6.5 vs. 4.2 mmHg from baseline of 135 mmHg) and diastolic blood pressures (2.7 vs. increase of 0.3 mmHg from baseline of 78 mmHg) were greater in tirzepatide, as well.
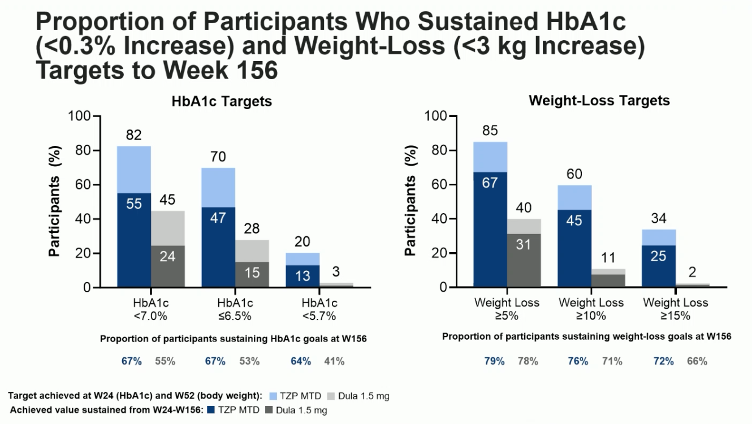
- Renal outcomes. Dr. Zoungas reviewed the effects of tirzepatide compared with dulaglutide on kidney outcomes and safety in participants in T2D with established CVD and high risk for chronic kidney disease (CKD). “High risk” included “high risk” (orange) and “very high risk” (red) categories defined according to KDIGO guideline. Primary endpoint was time to first occurrence of composite kidney endpoint (persistent macroalbuminuria, persistent ≥50% reduction in eGFR, end-stage kidney disease, or death from kidney disease). Secondary endpoints included time to composite kidney endpoints and change in eGFR and UACR at 36 months.
- Baseline characteristics of high-risk CKD subgroup. As shown in the table below, participants were slightly older (67 years) and had longer duration (18 years) than the overall cohort. Similar to the overall population, participants had high use of statins and ACEi/ARBs. Higher proportion of the CKD subgroup was on insulin (63% vs. 49% of overall group). High risk CKD population had slightly more treatment discontinuation (26.2% and 25.5% for tirzepatide and dulaglutide), compared to the overall population (21.6% and 19.8%, respectively).
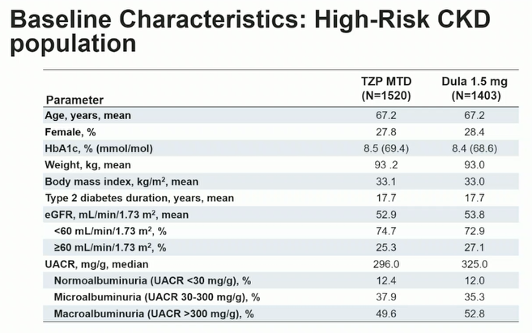
- Tirzepatide significantly reduced 19% in overall and 22% in the high -risk population, compared to placebo. Renal benefits for components and composite kidney endpoints were consistent between overall and high-risk population – notably, high-risk CKD population experienced 31% reduction in the composite kidney endpoint that includes CV death. Tirzepatide significantly slowed eGFR decline from baseline for both the overall (6.9 vs. 8.0 mL/min/1.73 m2) and high-risk population (5.0 vs. 8.5 mL/min/1.73 m2). Similarly, tirzepatide conferred 22 and 26 percentage point decrease in UACR compared to dulaglutide. Finally, the safety profile was similar between tirzepatide and dulaglutide in this population.
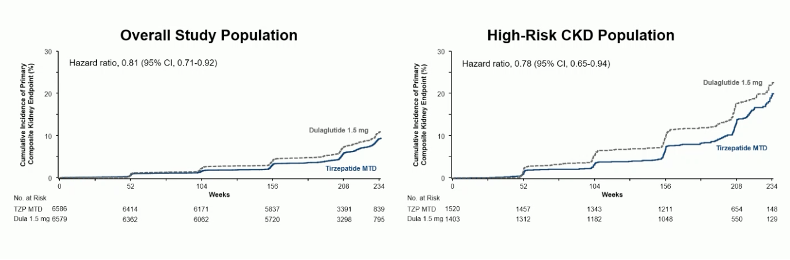
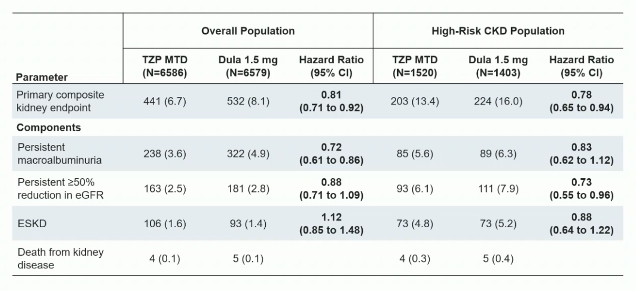
- Prof. Hertzel Gerstein (McMaster University, Canada) provided a most valuable independent commentary, praising the trial design and execution, such as the accrual of 1,663 primary events and balanced background use of SGLT-2 inhibitors. He further contextualized the SURPASS-CVOT against prior general GLP-1 RA class. He cited a meta-analysis of GLP-1 RAs that found 15% risk reduction in people with prior CVD – the p-value for interaction was 0.59, suggesting that GLP-1 RAs have generally similar cardioprotective effects. When he estimated tirzepatide’s efficacy against a “putative placebo” by multiplying the HR of tirzepatide to dulaglutide (representing all GLP-1 RAs) and the HR of GLP-1 RAs to placebo, tirzepatide conferred a 21% risk reduction in MACE, 23% reduction in CV death, and 26% reduction in all-cause death (see table below). While these mathematical exercises have limitations, he suggested that tirzepatide likely is more potent (“quantitative”) than the GLP-1 RAs at the doses tested and are likely similar in terms of “qualitative” efficacy.
- To estimate a “putative placebo” effect for tirzepatide, the SURPASS investigators prespecified a model multiplying tirzepatide’s risk reduction vs. dulaglutide by dulaglutide’s REWIND effect vs. placebo, applied to a REWIND subgroup most similar to SURPASS participants. This, he said, is a mathematical exercise—helpful but with inherent limitations. It allows exploration of whether dual GIP/GLP-1 agonism confers a qualitative advantage over GLP-1 RAs or mainly a quantitative (dose-potency) difference.
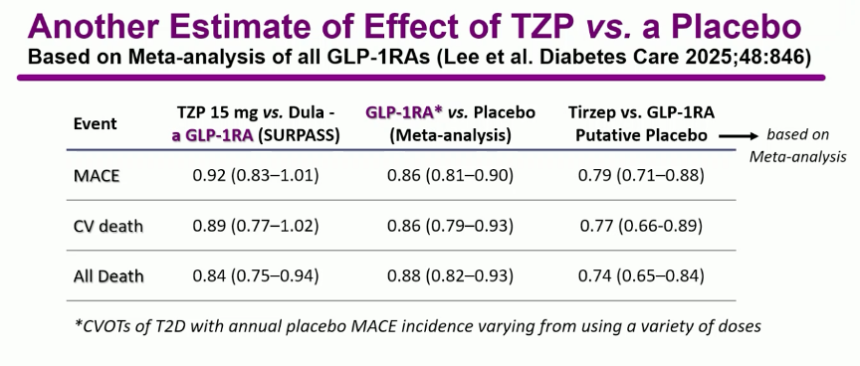
SURPASS-PEDS: Tirzepatide dropped A1c by 2.3 percentage points from undisclosed baseline; first GLP-1 RA to demonstrate clinically meaningful weight loss (-9.1%) in youth with T2D
In a late afternoon session, Dr. Tamara Hannon (Indiana University School of Medicine) presented findings from the SURPASS-PEDS trial. Full results were published yesterday in the Lancet. As background, SURPASS-PEDS investigated the use of tirzepatide in youth with T2D. Currently, treatment options for this population are limited to metformin, insulin, three GLP-1 RAs (liraglutide, exenatide, dulaglutide), and two SGLT-2 inhibitors (dapagliflozin, empagliflozin). Dr. Hannon noted that these therapies often have less glycemic efficacy and higher treatment failure rates in pediatrics compared to adults. Additionally, none of these therapies have demonstrated clinically meaningful weight loss compared to placebo.
- Study design. A total of 99 youth with T2D aged 10 to 17 years old were randomized 1:1:1 to received tirzepatide 5 mg, tirzepatide 10 mg, or placebo once-weekly. Participants had inadequate glycemic control (A1c >6.5% and ≤11%) and were being treated with metformin, basal insulin, or both. The primary endpoint was change in A1c at 30 weeks from baseline. Results for both tirzepatide groups were pooled in the analysis. Secondary outcomes included change in body weight and BMI. There was an additional 22-week open-label extension in which participants on placebo received tirzepatide 5 mg.
- Baseline characteristics. Mean age was 14.7 years old, with 44% of participants ranging in the ages of ≥10 and ≤14 years, and 56% in the ages of ≥15 to <18. Notably, two-thirds of participants were of Hispanic or Latino ethnicity, and 20% of participants were American Indian or Alaska Native. Mean A1c was 8.0%. Most participants were treated with metformin (68.7%), and some were treated with basal insulin (8.1%) or both (23.2%). Mean body weight and BMI were 96.6 kg (213 lbs) and 35.4 kg/m2, respectively.
- Results: Change in A1c. At 30 weeks, A1c decreased by 2.3 percentage points among all participants taking tirzepatide. Specifically, placebo-adjusted change in A1c was -2.4 percentage points for the tirzepatide 10 mg group and -2.2 percentage points for tirzepatide 5 mg. Notably, 79% of participants taking either tirzepatide 5 mg or 10 mg had an A1c below 6.5% (the threshold for diabetes), compared to 29% of those taking placebo. Additionally, 53% of participants on tirzepatide had an A1c below 5.7% (the threshold for prediabetes), compared to 14% on placebo.
- At 52 weeks (i.e., following the open-label extension), mean A1c for participants on tirzepatide was 5.8% (5.9% and 5.7% for tirzepatide 10 mg and 5 mg, respectively). The placebo group, which switched to tirzepatide 5 mg at Week 30, had a mean A1c of 6.6%.
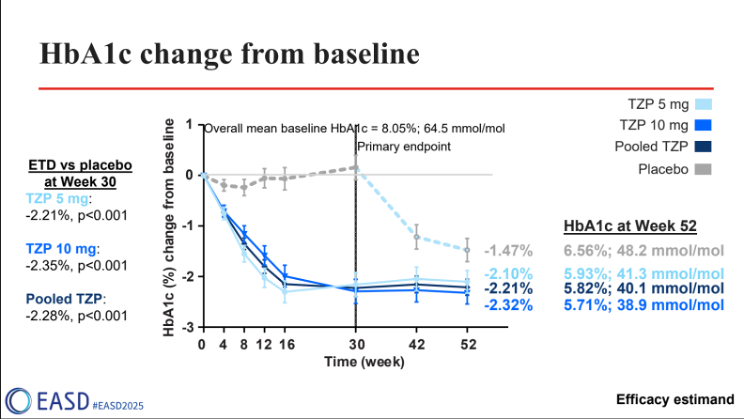
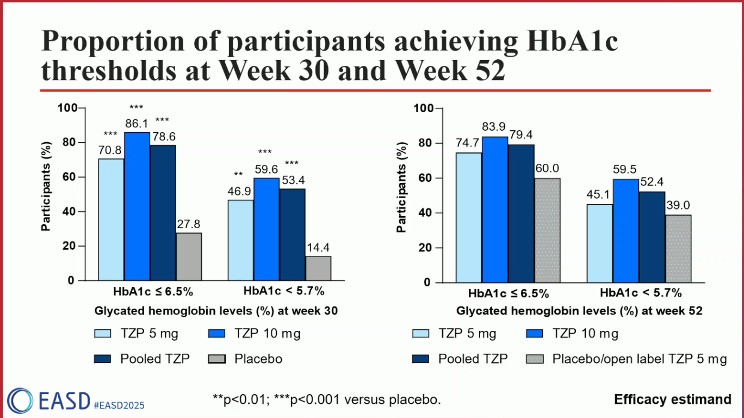
- Results: Change in body weight and BMI. At 30 weeks, body weight in the tirzepatide groups decreased by 9.1% (10.9% and 7.2% for tirzepatide 10 mg and 5 mg, respectively). Among participants taking tirzepatide, BMI decreased by 9.3 units from 35.6 to 26.3 kg/m2, compared to a 0.4 unit decrease in placebo (34.7 to 34.3 kg/m2).
- At 52 weeks, body weight had decreased by 10.9% in the tirzepatide groups, with the 10 mg group achieving 13.8% weight loss for a mean body weight of 82.2 kg (181 lbs)—that’s 14.4 kg (32 lbs) of weight loss.
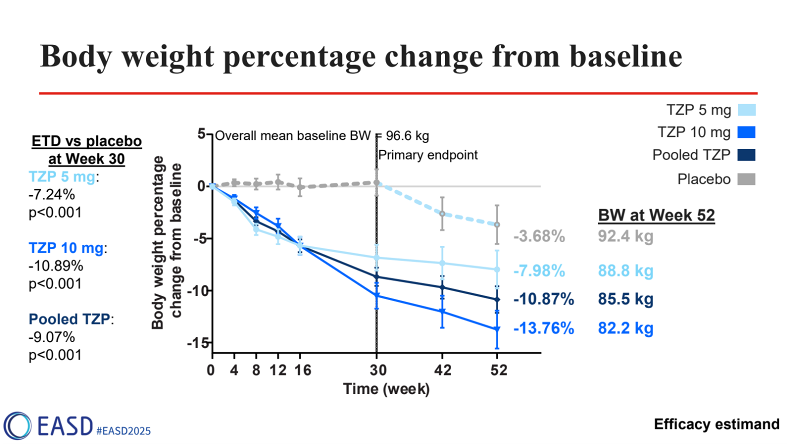
- Safety. Adverse events were reported in 44 of 65 participants (68%) in the tirzepatide groups, compared to 15 of 34 participants (44%) in placebo. Two patients in the tirzepatide 5 mg group had adverse events — nausea and suicidal ideation — that led to treatment discontinuation. Serious adverse events were reported in one participant on tirzepatide 5 mg (appendicitis), one participant on tirzepatide 10 mg (mastoiditis), and one participant in placebo (borderline personality disorder, suicidal ideation and attempt). GI-related side effects were more common in the tirzepatide groups. All events were mild or moderate in severity.
STEP UP post-hoc studies reveal positive effects on body composition, proximal muscle strength, and control of eating with semaglutide 7.2 mg
In a fiery morning session, Profs. Jøran Hjelmesæth (Vestfold Hospital Trust, Norway) and Michelle Dalton (Leeds Trinity University, UK) presented compelling prespecified post-hoc analyses of the STEP UP trial. In the phase 3b RCT, adults with BMI ≥30 kg/m2 without T2D were randomized 5:1:1 to once-weekly semaglutide 7.2 mg, semaglutide 2.4 mg, or placebo as an adjunct to a lifestyle intervention for 72 weeks. This higher dose of semaglutide was demonstrated to have improved weight loss effects compared to the 2.4 mg dose, inspiring further investigation into the benefits of the therapy beyond weight loss.
- Prof. Hjelmesæth demonstrated significant adipose tissue reduction with the use of semaglutide 7.2 mg, alongside the preservation of muscle mass and function. He began by asking those who believed that the preservation of muscle mass during weight loss to stand – almost every audience member rose. To explore this concern, body composition was measured using MRI for a subgroup of STEP UP participants (n=55), evaluating volume of total adipose tissue, visceral adipose tissue, and lean tissue. Total adipose tissue volume decreased by 25% from baseline in the treatment group compared to a 1% decrease in placebo (p <0.0001). Visceral adipose tissue volume was reduced by 31% in the intervention group compared to a 6% decrease in placebo (p=0.040). On the other hand, total lean tissue volume was reduced by 7% for semaglutide compared to a near-zero change in placebo (p=0.138), muscle volume was reduced by 10% compared to 1% in placebo (p=0.060), and muscle fat was reduced by 6% compared to a 4% increase in placebo (p=0.001). The proportion of weight loss from thoracic vertebra 9 (mid abdomen) to the knee was 84% adipose tissue mass loss and 16% lean mass loss. When the change in number of sit-to-stand repetitions were assessed from baseline to Week 72, no significant difference was observed between the treatment group and placebo (1.7 versus 1.8, respectively, p=0.966).
- Participants treated with semaglutide had significantly greater reductions in total adipose tissue volume (estimated treatment difference (ETD): -24%) and visceral adipose tissue volume (ETD: -25%) compared with those receiving placebo. The changes in total lean tissue volume and muscle volume did not differ significantly between treatment groups. However, Prof. Hjelmesæth noted that the small study size limits statistical power and therefore warrants further investigation with a larger cohort. Muscle fat was also significantly reduced following treatment with semaglutide (ETD: -10%). Importantly, muscle function was preserved with semaglutide treatment as measured by the sit-to-stand test.
- Prof. Dalton drew upon her background in psychology to explore changes to cravings and eating behaviors with the use of semaglutide 7.2 mg. Semaglutide 2.4 mg has demonstrated improvements to control of eating, but the effects of higher doses remain unknown. Disordered eating patterns are well-known to be linked to weight gain and obesity. Changes were assessed using the Control of Eating Questionnaire to assess cravings (CoEQ) and Three-Factor-Eating Questionnaire to assess behaviors (TFEQ-R18v2).
- Changes to all four CoEQ domains were statistically significant at Week 72 compared to placebo (p=0.03, p=0.08, p=0.49, and p=0.07, respectively). A positive effect was seen as early as Week 24, showing a meaningful and enduring impact on cravings and behaviors. A particular reduction to cravings for fruit/fruit juice and salty/spicy food was noticed, which may warrant further investigation into effects on certain foods.
- TFEQ-R18v2 scale scores demonstrated improvement as well. Cognitive restraint may have been improved compared to placebo, while emotional eating and uncontrolled eating had stronger improvement effects compared to placebo at 72 weeks. Despite the greater weight reduction observed with semaglutide 7.2 mg compared to 2.4 mg, no significant differences to these behavioral scales were observed at higher doses in this work. Prof. Dalton said that this may suggest intriguing alternate mechanisms that contribute to greater weight reduction with higher doses.
GLP-1 RA-based therapies and impact fertility, pregnancy, and early-onset T2D in women
Dr. Charlotte Moffett (Ulster University, UK) and Prof. Helen Murphy (University of East Anglia, UK) presented complementary perspectives on the intersection of GLP-1 RA-based therapies, diabetes, and reproductive health. Prof. Murphy contextualized the rapid increase in obesity and early-onset T2D among women of reproductive age and examined the implications for GLP-1 RA use in pregnancy, while Prof. Moffett approached the topic from a basic science perspective, highlighting the links between gut hormones and ovarian function.
- Dr. Moffett spoke first, emphasizing the high burden of infertility in people with diabetes and metabolic disease. Globally, she said, one in seven couples in the UK are affected by infertility, and, in fact, strong correlations have been observed between infertility and T2D, according to Dr. Moffett. She also said up to 40% of women with T1D also have polycystic ovary syndrome (PCOS), and 50-80% of people with PCOS exhibit some degree of insulin resistance. She also highlighted gut hormones as a mechanistic link between metabolic and reproductive dysfunction and referenced preclinical models showing how GLP-1 plays a role in regulating follicle development.
- Prof. Murphy then shifted the focus to the clinical landscape, warning of the rapid rise of early-onset T2D among women of reproductive age. In the US, 57% of pregnancies impacted diabetes are now those who had T2D prior to pregnancy, with the burden, Prof. Murphy said, falling disproportionately on minority and socioeconomically challenged women.
- Separately,she shared another striking statistic from this population: women diagnosed with T2D before the age of 30 lose an estimated 16 years of life expectancy. Against this backdrop, GLP-1 RA use has surged among women aged 18-25, increasing by nearly 600% in recent years. This has led to real-world fertility consequences, with Prof. Murphy warning that tirzepatide (Mounjaro) reduces oral contraceptive absorption to ~66%, underscoring the importance of counseling on barrier or IUD use.
- Ultimately, both speakers highlighted the need for more research and clinical guidance on the intersection of diabetes, obesity, and reproductive health. They called for mandatory pregnancy registries and more inclusive clinical trials to clarify the role of GLP-1 RAs in women of reproductive age. While early data shows promise, particularly for preconception use, Dr. Moffett and Prof. Murphy both warned that careful management is warranted and is of the upmost importance
Pre-specified analysis of SOUL trial: Oral semaglutide reduces hospitalization burden in people with T2D and ASCVD or CKD
In a packed afternoon session, Dr. John Buse (University of North Carolina) presented a pre-specified secondary analysis of the phase 3 SOUL trial (n=9,650) on treatment with Rybelsus (oral semaglutide) in adults with T2D and ASCVD or CKD. In the trial, oral semaglutide demonstrated a statistically significant and superior 14% major adverse cardiovascular events (MACE) reduction.
- Trial design and baseline characteristics. In the trial, severe adverse events (SAEs) were reported, including hospitalizations. This prespecified analysis assessed the incidence of hospitalization in people taking oral semaglutide vs. placebo. Baseline characteristics were the following: (i) average participant age was 66 years; (ii) 29% were women; and (iii) most participants had a history of CVD and 43% had a history of CKD.
- Results. Compared to those on placebo, participants who were treated with oral semaglutide had:
- 8% reduced incidence of first hospitalizations (14 events vs. 15 events per 1oo patient-years; p=0.004);
- 9% fewer total hospitalizations (22 vs. 24 per 1oo patient-years; p=0.005);
- 10% fewer hospitalizations for ≥three days or ending in death (18 vs. 21 per 1oo patient-years; p=0.004); and
- 16% days hospitalized (243 vs. 291; p=0.001).
Subgroup analysis showed consistent benefits on the first incidence of SAE-related hospitalizations across sex, age, BMI categories, SGLT-2 inhibitor use, and medical history. Dr. Buse noted that the protective effects are more pronounced in those with baseline A1c >8% (p<0.01) or eGFR <60 mL/min/1.73 m² (p=0.02). That’s interesting to us since that is a “healthier” A1c level, in which protective effects are happening, but a “less healthy” kidney function. Notably, further analysis demonstrated that oral semaglutide significantly reduced hospitalizations for cardiac disorders by 14%, infections by 11%, and injuries by 28%. The “injuries” was higher than we might have anticipated and we plan to investigate further into this.
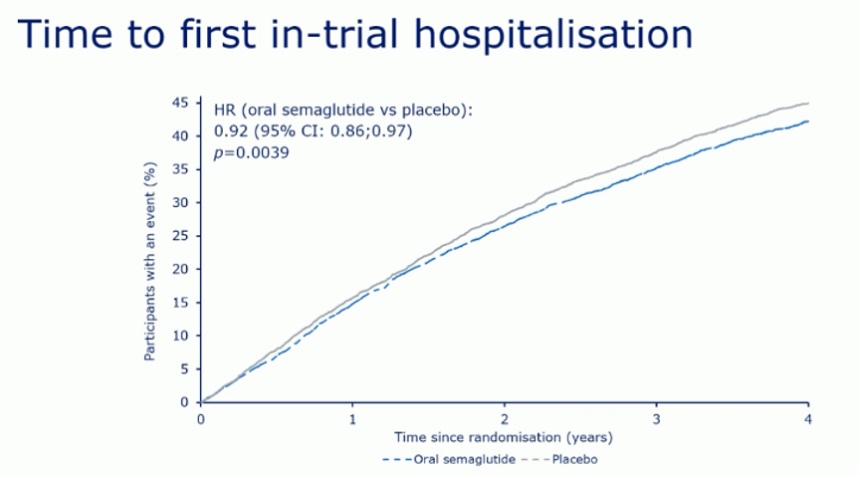
Pre-specified analysis of SOUL trial finds reduction in major adverse limb events with Rybelsus (oral semaglutide) in people with and without PAD
In this crowded morning session, Dr. Matt Cavender (University of North Carolina Chapel Hill) presented a new prespecified subgroup analysis of the SOUL trial, evaluating the effect of Rybelsus (oral semaglutide) on major adverse limb events (MALE) in people with T2D and peripheral artery disease (PAD). PAD is a common yet often overlooked comorbidity, estimated to affect 30% of people with T2D >50 years of age, which is also associated with increased risks of CV and limb events. As a reminder, the phase 3b SOUL trial (n=9,650) demonstrated that oral semaglutide significantly reduced major adverse cardiovascular events (MACE) by 14%.
- Baseline characteristics. In the SOUL trial, 17.5% of participants (n=1,515) had PAD at baseline. This subgroup was predominantly male (71%) with a mean age of 67 years, BMI of 31 kg/m2, and A1c of 8.0%. Comorbidities were frequently experienced by the subgroup, including coronary heart disease (64%), cerebrovascular disease (30%), chronic heart failure (34%), and CKD (25%). Most participants with PAD received background therapies, including lipid-lowering agents (87%), antiplatelet therapy (82%), and ACE/ARB/ARNI (82%), which underscores the significant disease burden in this population.
- CV and limb outcomes were consistent, regardless of PAD. Across CV endpoints, semaglutide conferred benefits irrespective of the severity of baseline CVD – from subgroups with no known ASCVD to those with an isolated vascular disease; or multiple CV events. Compared to placebo, semaglutide significantly reduced CV death, MI, or stroke in patients without PAD by 18% (HR=0.82) and in those with PAD by 3% (HR=0.97). A nonsignificant interaction (p-int=0.22) between the groups indicates that semaglutide’s benefits do not differ by PAD status. For expanded ischemic outcomes (CV death, MI, stroke, hospitalization, and revascularization), results were similarly consistent (p-int=0.67). Importantly, semaglutide significantly reduced MALE events, with comparable risk reductions (see below) in both PAD (HR=0.70) and non-PAD (HR=0.69) subgroups. In all, findings suggest that oral semaglutide’s effects on MALE are unaffected by PAD status.
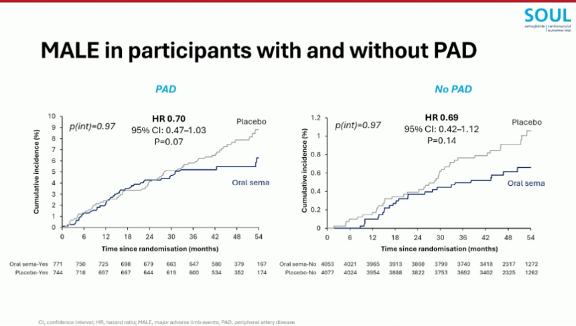
- Still, Dr. Ildiko Lingvay (University of Texas Southwestern) cautioned that the findings, while encouraging, are exploratory and requires more dedicated trials. While it is promising to observe significant reduction in MALE with oral semaglutide, the SOUL trial’s hierarchical testing sequence was not preserved beyond the first two confirmatory secondary outcomes, which were not statistically significant. Therefore, all subsequent outcomes are technically exploratory. She cautioned that this applies across the board, including heart failure composite outcomes, interaction analyses with baseline SGLT-2 inhibitor use, and subgroup analyses by baseline PAD status. These analyses all fall into what she described as “subtypes of subtypes” – incremental slices of the overall trial population that are statistically underpowered. All exploratory findings, Dr. Lingvay argued, are intriguing and directionally consistent with growing evidence for GLP-1 RA benefits but should not be over-interpreted or cited with patients without confirmation from future dedicated trials.
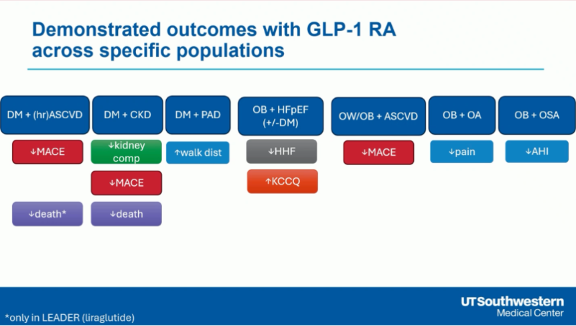
SGLT-2 Inhibitors
Profs. Heerspink, Roden, and Bozkurt highlight the potential for SGLT-2 inhibitor and GLP-1 RA combination therapy for cardiorenal protection
In this afternoon symposium sponsored by AstraZeneca, Prof. Dr. Hiddo Heerspink (University of Groningen, the Netherlands), Prof. Michael Roden (Heinrich-Heine University Düsseldorf, Germany), and Dr. Biykem Bozkurt (Baylor University) explored the synergistic potential of SGLT-2 inhibitors and GLP-1 RAs for multi-organ protection in people with T2D. The symposium provided an overview of how each class has distinct, yet complementary benefits for cardio-renal-metabolic management.
- Prof. Roden reviewed physiological mechanisms of both therapies, noting their roots in naturally occurring pathways. He described how SGLT-2 inhibitors promote natriuresis (which is when elevated pressure causes the kidneys to inaccurately work to reduce fluid and sodium levels, decreasing reabsorption and increasing water excretion), cardiac fuel shifts, and renal energy loss – reducing inflammation and improving endothelial function. Meanwhile, GLP-1 RAs enhance insulin and gut hormone signaling, reduce oxidative stress, and improve cardiac metabolism. Together, these distinct mechanisms may act complementarily to protect cardiac and renal health in people with T2D.
- Prof. Heerspink presented clinical evidence for kidney protection with the use of SGLT-2 inhibitors and GLP-1 RAS. He highlighted the CREDENCE, DAPA-CKD, and EMPA-KIDNEY trials to demonstrate the reductions in the risk of composite kidney outcomes with SGLT-2 inhibitor use. Prof. Heerspink also highlighted data from the FLOW trial, in which semaglutide slowed eGFR decline compared to placebo, regardless of baseline SGLT-2 inhibitor use. He then shared results from a SMART-C meta-analysis, which showed that SGLT-2 inhibitors provided kidney protection regardless of baseline GLP-1 RA use, suggesting independent and additive mechanisms.
- Dr. Bozkurt discussed the cardioprotective effects of combining the two therapies, emphasizing that obesity, CKD, and hyperglycemia have overtaken traditional risk factors as dominant drivers of cardiovascular disease. With this shift in risk profiles, understanding the cardiovascular benefits of weight- and glucose-lowering therapies is crucial in managing CVD. She reviewed how SGLT-2 inhibitors consistently reduced heart failure hospitalizations by 35% across trials like EMPA-REG. Additionally, she showed that both SGLT-2 inhibitors and GLP-1 RAs reduce MACE, but through distinct mechanisms, as outlined by Prof. Roden. Dr. Bozkurt concluded by highlighting the complementary effects of both therapies – lowering blood pressure, weight, albuminuria, inflammation, and oxidative stress – and proposed that the combined use may offer a new standard for reducing CV mortality and heart failure.
Trends of SGLT-2 inhibitor use in T2D in the UK: Up to 90% with T2D and CKD eligible, but uptake not yet optimal
In a striking afternoon oral symposium, Dr. Martha Dinsdale (University of Exeter, UK) highlighted trends in the use of SGLT-2 inhibitors across age and frailty subgroups in people with T2D. SGLT-2 inhibitors have demonstrated encouraging results beyond glycemic management, improving weight management, reducing CVD risks, and offering kidney protection. Recognizing the benefits of this treatment class, guidelines like those of EASD have recommended SGLT-2 inhibitors as a second-line therapy for people with established/high-risk CVD or CKD. While the guidance applies to 90% of people in the UK with T2D and CKD/CVD, paradoxically, these high-risk populations are less likely to receive SGLT-2 inhibitors compared to those without comorbidities. Therefore, a study (n=117,046) aimed to describe how second-line treatment prescriptions in the UK have changed across age and frailty groups between 2019 and 2024. The study also evaluated whether these changes were associated with improvement in short-term clinical outcomes.
- The study was based on UK primary care and hospital records. The study used data from Clinical Practice Research Datalink (CPRD), including electronic health records, from 2019 to 2024. The study participants included adults initiating second-line therapy after metformin. Once researchers gathered their electronic frailty index, they were divided into the following groups: (i) age ≤70 years (n=84,589); (ii) age >70 years without frailty (n=18,933); and (iii) age >70 years with frailty (n=13,542).
- SGLT-2 inhibitors were the most prescribed second-line treatment. Across all age and frailty groups, SGLT-2 inhibitors were the most prescribed treatment after metformin. These trends were consistent across sex, ethnicity, and in adults with or without CVD/CKD. The greatest increase was seen in adults >70 years with frailty, from 10% in 2019 to 60% in 2024.
- Increased SGLT-2 inhibitor prescription trends were associated with short-term outcomes. The study further investigated whether the increased prescriptions of SGLT-2 inhibitors were related to improvements in short-term outcomes at the population level from 2019 to 2024. 12-month data on A1c responses and weight changes showed modest improvements across age and frailty groups with SGLT-2 inhibitor treatment. Furthermore, treatment discontinuation within the 12 months was consistent.
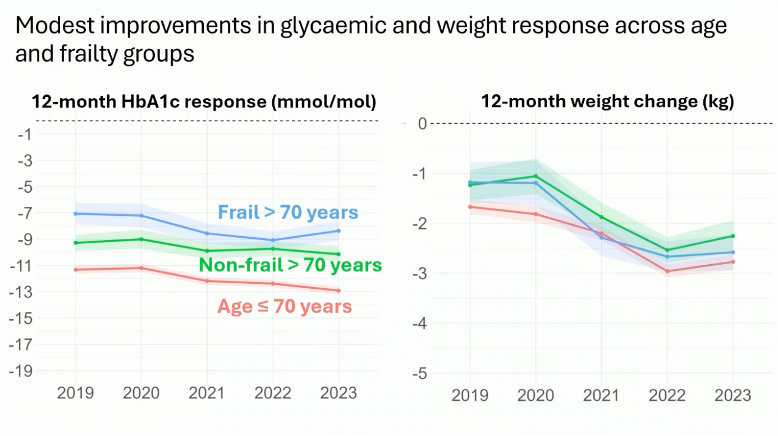
- Despite increased prescriptions of SGLT-2 inhibitors, results showed no improvements in complication rates – though none may have been expected for this population. The study didn’t show a reduction in age-related diabetes complications, heart failure, and kidney failure across the period of increased SGLT-2 inhibitor uptake. Dr. Dinsdale suggested several reasons for this observation, including speculations that the study included a low-risk population, so the benefit of SGLT-2 inhibitors was not demonstrated within the study duration.
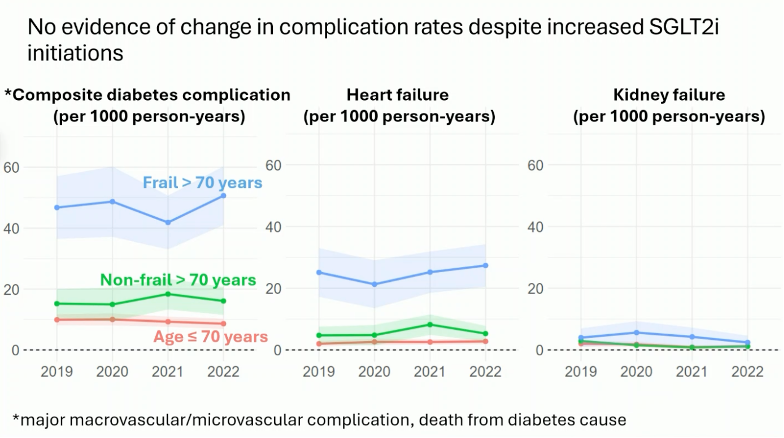
- Dr. Dinsdale called for individualized treatment to improve population-level glycemic responses. While this study showed increased prescriptions of SGLT-2 inhibitors, Dr. Dinsdale noted that “one size doesn’t fit all.” She referenced the newly developed five-drug model for optimal treatment model, which was outlined in a Lancet publication earlier this year. This model uses clinical data (e.g., age, sex, diabetes duration, A1c, BMI, eGFR, cholesterol) to determine optimal glucose-lowering treatments for people with T2D. The study applied this model across the patient cohort and found that the predicted optimal treatment could improve A1c responses by 5 mmol/mol. Furthermore, the analysis showed that not all groups benefit most from SGLT-2 inhibitors, predicting that the treatment is most optimal for ages ≤70 years and GLP-1 RAs for ages >70 years with and without frailty.
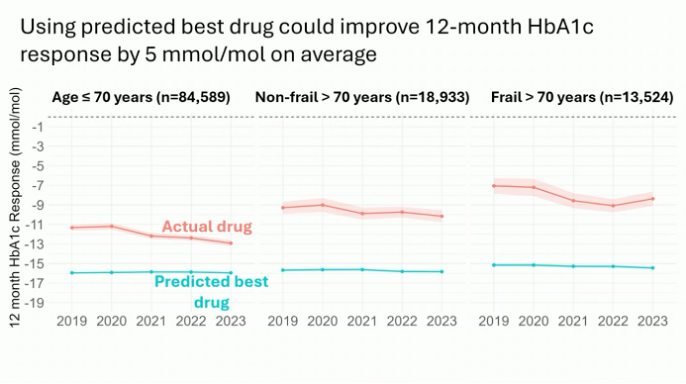
Prespecified analysis of phase 2 CONFIDENCE trial: simultaneous use of finerenone (Bayer’s Karendia) and empagliflozin (BI/Lilly’s Jardiance) prompted far better outcomes while addition of GLP-1 yielded nothing additional
In this morning session, Dr. Rajiv Agarwal (Indiana University) presented results from a post-hoc analysis (n=182) of the CONFIDENCE trial (n=800). The results were simultaneously published today in Diabetes Care. As a reminder, the trial found that simultaneous use of finerenone and empagliflozin reduced urinary albumin-to-creatinine ratio (UACR) by 52% at Day 180, conferring 29% and 32% greater relative reductions in UACR, compared to finerenone or empagliflozin alone, respectively – this is fantastic!. This prespecified analysis investigated whether the efficacy and safety of the combination therapy were affected by baseline GLP-1 RA use. We were a bit surprised about this – yet and still, we certainly think there is at least a bit of complexity with the better-known classes, specifically incretins. Titration, for example, continues to be extremely challenging for GLP-1 and for some (but at least they know it right away!) So perhaps it is better that better outcomes were not seen, since adding a third agent may have been very complicated. On a positive note, while SGLT-2 inhibitors are a bit hard to take due to emergence of UTIs, patients taking them understand very well where things are headed. By contrast, the side effect profile for Kerendia appears positively benign – so, getting to combination therapy with BI/Lilly’s Jardiance shouldn’t be hard at all and it yields a far better results. We love that this is an “oral combo” as well – yet another reason to prove to people how positive it is to be very proactive to look out for kidneys. Ultimately, we hear so many positives about how easy it is to both prescribe and take and we feel that the more people with diabetes at high risk of kidney disease will be over the moon at how easy it is to be proactive. Ultimately, we will say that so many negatives often pop up with titration with GLP-1 that we wouldn’t mind seeing clear assessment of how easy titration actually was. All this is our understanding seeing only a bit of the data and we look very forward to learning more from the scholars.
- Baseline characteristics. The analysis included 182 participants who were on a GLP-1 RAs at baseline. Dr. Agarwal highlighted the differences across baseline characteristics, with GLP-1 RA users having higher BMI compared to nonusers (32 kg versus 27 kg), higher insulin use (59% versus 34%), higher statin use (87% versus 71%), and lower DPP-4 inhibitor use (4% versus 41%).
- Results. At Day 180, in the combination therapy group, UACR in patients on GLP-1 RAs was reduced by 51% compared to 57% in those not using GLP-1 RAs. For participants receiving finerenone monotherapy, there was a 35 % reduction in GLP-1 RAs users versus 37% in nonusers. For participants using empagliflozin alone, GLP-1 RA users had 36% reduction in UACR versus 33% in nonusers. eGFR changes were consistent across groups, as well. In safety results, the incidence rate of hyperkalemia was 9% in GLP-1 RA users and 9.5% in nonusers. Overall, the analysis found that GLP-1 RA use at baseline does not compromise efficacy or safety, supporting the use of triple therapy in appropriate patients. Ultimately, this was a fairly small trial and we do wonder what might be seen in a far bigger group – we know, of course, from Novo Nordisk’s very exciting FLOW trial that GLP-1 solo did very well in this trial! That said, given tolerability and ease of use – while we imagine most patients would go with two orals any day compared to an incretin, Richard Wood’s dQ&A group is really the one to answer that! dQ&A has thousands of paitents in the US, Canada, and in seven European countries and they sure can give you their opinions – some of them have answered every single quarterly survey sent to them since 2009!
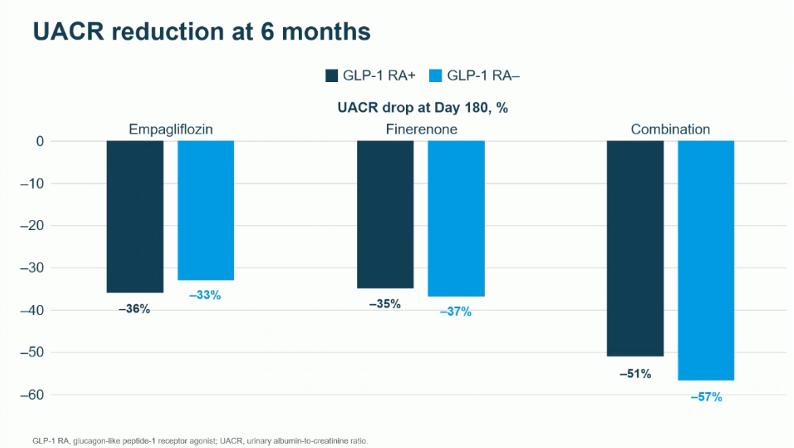
New paths for old friends: Potential new roles for GLP-1 RAs and SGLT-2 inhibitors
The final day of EASD 2025 featured an innovative, forward-looking symposium on potential new uses for GLP-1 RAs and SGLT-2 inhibitors. Dr. Mehdi Farokhnia (Johns Hopkins University) and Prof. Martin Heni (University Hospital Ulm, Germany) focused on one therapy each, offering evidence for the complex neurological benefits of these therapies. We heard more about some of the most exciting possibilities we could imagine, such as the fact that SGLT-2 inhibitors have demonstrated promise for restoring insulin sensitivity specifically to the brain, while GLP-1 RAs may be the next frontier for the treatment of alcohol use disorder (AUD).
- Prof. Heni began by encouraging the audience to dive deeper into the idea of “mind over metabolism” and its relevance for SGLT-2 inhibitors. It is known that these therapies function by interfering with the sodium-glucose transport process in the kidneys, resulting in glucose being excreted from the body in urine. With this caloric loss comes weight loss. He cited a number of studies that have demonstrated weight loss with the use of SGLT-2 inhibitors until approximately 28 weeks of treatment, when weight plateaus.
- Prof. Heni raised the question of why this occurs and explored the hypothesis that the brain may be involved in this process. As demonstrated by Sawada et al., the effect of SGLT-2 inhibition on weight loss is partly mediated by liver-brain-adipose neurocircuitry, and 2022 studies by Ruiten et al. were the first to show that dapagliflozin specifically causes an increase in activity in the right amygdala and right caudate nucleus, areas of the brain that are important for metabolism, eating behaviors, and cognitive function. These areas are also insulin sensitive. Prof. Heni then explored if SGLT-2 inhibitors may act on these areas of the brain to improve insulin sensitivity.
- While SGLT-2 inhibitors did not have an effect on whole-body insulin sensitivity, the therapeutic class has demonstrated improvements to insulin responsiveness in the brain. A 2022 study demonstrated no difference in whole body insulin sensitivity between patients taking empagliflozin versus placebo (p=0.8). However, in a study using intranasal insulin to affect the brain directly (n=40), empagliflozin has been found to restore hypothalamic insulin responsiveness in prediabetes with eight weeks of treatment (absolute change in CBF mL/100 g/min, p=0.04 for empagliflozin before and after treatment versus 0.2 for placebo). As this budding area of research continues to develop, Prof. Heni posits that SGLT-2 inhibitors may be used in the future to restore brain hypothalamic insulin sensitivity and improve systemic metabolism. Future work will continue to explore this therapeutic area, as well as promising work suggesting benefits of SGLT-2 inhibitors for protection against dementia.
- Dr. Farokhnia’s presentation, “No longer stuck on you: GLP-1 RAs for addiction,” was compelling. The primary focus of addiction studies with these therapies has been AUD, which is characterized by impaired ability to control alcohol use despite adverse social, occupational, and health consequences. The condition may cause lasting changes in the brain, making patients vulnerable to relapse. Psychosocial treatments and pharmacological treatments including acamprosate and naltrexone are available, however, innovation has seemingly stagnated over the past 20 years, while AUD rates remain high. During addiction, neurocircuits, synaptic systems, and molecules within the brain can be affected, leading to long-term changes. GLP-1 is known to regulate blood glucose and food intake, and is also a neuropeptide, leading to its study for AUD.
- GLP-1 RAs have demonstrated benefit for AUD in both human and rodent studies. The Veterans Aging Cohort Study draws upon health data from 13.5 million veterans who received medical treatment. New initiators of GLP-1 RAs who received two or more doses over ≥60 consecutive days (washout: ≥180 days) and who had nonzero alcohol use tendencies at baseline assessed by AUDIT-C score were included in a study. The use of GLP-1 RAs was associated with a decrease to alcohol use based on AUDIT-C score compared to those who did not take GLP-1 RAs. This effect was especially pronounced in participants with AUD and hazardous alcohol use. In contrast, the use of DPP-4 inhibitors had no demonstrated effect on AUDIT-C score compared to those unexposed to therapy, and GLP-1 RAs demonstrated a decreased in AUDIT-C score when compared directly with DPP-4 inhibitors as well. In closing, Dr. Farokhnia pointed to ongoing work through studies such as Semaglutide Therapy for Alcohol Reduction (STAR) and several ongoing RCTs evaluating GLP-1 RAs for AUD as well as addiction to other compounds. In sum, GLP-1 RAs may soon present a new frontier for AUD treatment in the next two decades and beyond.
Do we need really need a large outcome trial to prove the cardiorenal benefits of SGLT-2 inhibitor and GLP-1 RA combination use?
In this morning session, the highly-admired Dr. Hertzel Gernstein (McMaster University & Hamilton Health Sciences, Canada) reviewed meta-analyses of cardiovascular (CV) outcome trials to make a compelling case for SLGT-2 inhibitors and GLP-1 RA combination therapy. SGLT-2 inhibitors and GLP-1 RAs confer substantial CV and kidney benefits, but no outcomes trial has directly investigated the benefit of using both therapies in combination, in comparison to either therapy alone. Rather than proposing an additional large outcomes trial, Dr. Gerstein leveraged background SGLT-2 inhibitor use in GLP-1 RA trials in existing CV meta-analyses, and vice versa, to support the combination use in high-risk patients.
- Dr. Gerstein advocated for filling in clinical context with existing evidence. GLP-1 RAs and SGLT-2 inhibitors are examples where randomized outcomes trials revealed clinical benefits beyond the trial’s original focus. These therapies, developed initially for diabetes management, demonstrated substantial and unexpected CV benefits. Therefore, Dr. Gerstein highlighted that such large studies not only confirm safety and efficacy of the trials’ focus but may also offer findings that confer unexpected advantages. Existing outcomes trials, which include the use of background GLP-1 RA use in SGLT-2 inhibitor outcomes trials (and vice versa), can help inform clinical decisions on whether combination therapy is appropriate for high-risk patients.
- Although the exact mechanisms of GLP-1 RAs and SGLT-2 inhibitors are debated, their benefits are well established. Both drug classes reduce CV and kidney 0utcomes in people with and without T2D, with no evidence suggesting differential effects base on diabetes status. Similarly, on intermediate measures including weight, A1c, blood pressure (BP), eGFR, and albuminuria, the effect of these drugs appears to be independent. Moreover, according to Dr. Gerstein’s analysis of recent outcomes trials, no meaningful interaction between the two occurred – indicating that combination therapy offers the additive benefits of both.
- “Explanations are evanescent. Observations are robust.” Debates on the mechanism of these therapies might go on forever, Dr. Gernstein added. However, individual benefits of GLP-1 RAs and SGLT-2 inhibitors are clear. Given the evidence of non-interaction between the two, Dr. Gernstein advocated for high-risk patients to receive the benefits of both and urged clinicians to apply existing data to their practice, rather than awaiting a designated SGLT-2 inhibitor/GLP-1 RA combination outcomes trial.
- Furthermore, Dr. Gerstein questioned if we need a large outcome trial to prove the added benefits of SGLT-2 inhibitor and GLP-1 RA combination use. Depriving high-risk patients of the “profound” potential additive benefits (decreased NNTs, MACE, HF, and kidney decline) would be hard to ethically justify, he argued. He is sure persuasive, Dr. Gerstein is.
Insulin Therapy
Insulin therapy and cardiorenal outcomes in T2D: A pooled analysis of CANVAS and CREDENCE
Using data from the CANVAS and CREDENCE trials, originally presented at ADA in 2017, Dr. Martina Chiriacò (University of Pisa, Italy) presented findings from an analysis assessing whether background insulin monotherapy has an impact on cardiorenal outcomes in people with T2D. As background, insulin therapy has been shown in some observational studies to increase the risk of cardiovascular disease. On the other hand, the ORIGIN study (n=12,537) found that insulin has a neutral effect on cardiovascular outcomes. Similarly, the effects of insulin therapy on renal outcomes and microvascular complications are unclear. In this analysis, pooled data from the CANVAS and CREDENCE trials investigating the SGLT-2 inhibitor canagliflozin were used to further assess the impact of insulin therapy on cardiorenal outcomes. Whereas CANVAS investigated cardiovascular outcomes for canagliflozin in adults with T2D and high CV risk, CREDENCE looked at renal outcomes for canagliflozin in adults T2D and CKD.
- Methods and baseline characteristics. Participants (n=14,530) were divided into three groups: (i) insulin monotherapy (n=2,766); (ii) metformin monotherapy (n=2,127); and (iii) other therapies (n=9,637). The cardiovascular outcomes assessed were heart failure/CV death, MACE, all-cause death, and renal outcomes. At baseline, the insulin monotherapy group had a less favorable cardiovascular profile. Participants in this group were older and had had diabetes for a longer duration. They also had higher A1c levels, higher blood pressures, greater history of heart failure and CVD, greater albuminuria, and lower eGFRs.
- Results. As shown below, univariate analyses (i.e., prior to adjusting for confounding variables) revealed that participants on insulin monotherapy, in comparison to all other participants, had significantly increased risk across all four outcomes assessed. That said, adjusted hazard ratios revealed no significant difference in risk for all-cause death and renal outcomes. Heart failure/CV death and MACE risk were also lower, though still significantly increased compared to participants on metformin monotherapy or other therapies. Importantly (and perhaps even more importantly hearing this again today, as we did back in 2017), J&J’s Invokana significantly reduced the risk of all four outcomes except all-cause death.
- Adjusted hazard ratios for participants in the metformin monotherapy group reinforced, in case there are lingering questions about the value of metformin, that metformin does not have a protective effect again cardiorenal outcomes. By contrast, canagliflozin reduced the risk of all cardiorenal outcomes assessed besides all-cause death.
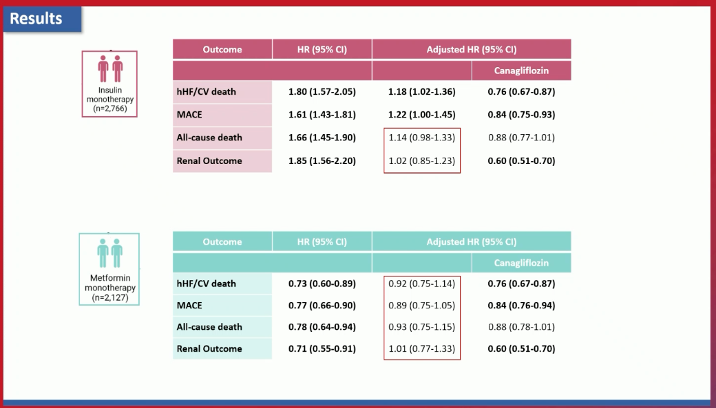
Type 1 “Cures,” Prevention, Delay, and Adjunctive Therapies
INNODIA’s phase 2 MELD-ATG trial finds low-dose ATG significantly preserves C-peptide levels in young individuals with new-onset T1D
In this early morning session, Prof. Chantal Mathieu (KU Leuven, Belgium) presented full results of the phase 2 MELD-ATG trial (n=117), which evaluated anti-thymocyte globulin (ATG) on beta cell preservation in young people (5-25 years) newly diagnosed with stage 1 T1D. The results were simultaneously published in The Lancet. As background, ATG suppress immune T cells and are a potent immunosuppressant used for organ transplantation since the 1960s. TrialNet’s previous phase 2 study (n=89) found that low dose of ATG (~2.5 mg/kg vs. 9-12 mg/kg used for transplantation) may slow beta cell loss in new-onset T1D but also produced cytokine release syndrome (CRS; 48% vs. none) and serum sickness (72% vs. none) in participants. The MELT-ATG study aimed to answer if an even lower dose (0.5 mg/kg) may retain efficacy with an improved safety profile. Ultimately, the study confirmed the efficacy of ATG on beta cell function preservation and established an effective minimum low dose (0.5 mg/kg) in a pediatric and young adult European cohort.
For context, the MELD-ATG trial is one of six studies (Diagnode-3, FABULINUS, Ver-A-T1D, MELD-ATG, Impact, and CFZ533) by Innodia, the largest European Network led by Prof. Mathieu. These studies have aligned trial design, such as inclusion criteria and biomarker analysis, to accelerate development of T1D prevention therapies and cures.
- Trial design. The MELD-ATG study recruited young individuals between 5-25 years newly diagnosed with T1D within six weeks. Participants were randomized to receive intravenous ATG (0.1, 0.5, 1.5, and 2.5 mg/kg) or placebo over two consecutive days. The trial adopted an adaptive dosing scheme; an independent unblinded Dose-Determining Committee regularly reviewed immune, metabolic, and safety data and adjusted doses as deemed necessary. The primary endpoint was change in stimulated C-peptide area under curve (AUC) at 12 months. Secondary endpoints included A1c, insulin dose, and CGM metrics, and immune biomarkers.
- At baseline, participants consisted of 18% children (5-9 years), 65% adolescents (10-17 years), and 17% young adults (18-25 years). Clinically, mean A1c was 7.8% and median of mixed-meal stimulated C-peptide level was 0.8 nmol/L/min.
- Results. The trial met its primary endpoint, with ATG 2.5 mg/kg conferring significant C-peptide preservation over placebo by 0.124 nmol/L/min (p=0.003). Moreover, investigators identified 0.5 mg/kg as the minimum effective low dose, which significant preserved C-peptide AUC by 0.102 nmol/L/min (p=0.014). The efficacy was more pronounced in ages 5-17 and less in ages 18-25 (p-interaction=0.42). A1c remained low in both treatment groups (0.5 and 2.5 mg/kg), with the low dose achieving significant reduction compared to placebo group (0.5 percentage points; p=0.024). Insulin dose transiently increased in first month, which Prof. Mathieu attributed to serum sickness rescued by steroid therapy. Excitingly, ATG improved CGM metrics, measured at Months 3, 6, and 12 with blinded Dexcom G6. As shown in the figure below, Time in Range (TIR; 70-180 mg/dL) and Time in Tight Range (TITR; 70-140 mg/dL) remained stable in the 2.5 mg/kg arm at 63% and 38%, respectively, while placebo group experienced a decline from 65% to 58% and 41% to 34%, respectively.
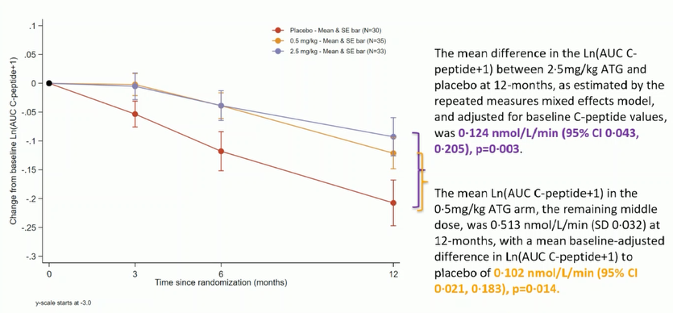

- Safety. Low-dose ATG was generally well-tolerated even in young children. Two Grade 4, life-threatening events (severe hypoglycemia) occurred, one in placebo and another in the 0.5 mg/kg arm. Expected adverse events included cytokine release syndrome (CRS) during infusion and serum sickness approximately 10-15 days later. In the trial, CRS occurred in 33% of 2.5 mg/kg arm (n=11) and 24% of 0.5 mg/kg arm (n=8), compared to none in placebo. Nonsteroidal anti-inflammatory drugs (e.g., ibuprofen or aspirin), antiemetics, and one-time steroid mitigated the symptoms. Serum sickness was more prevalent, with 81.8% in 2.5 mg/kg and 33% in 0.5 mg/kg experiencing for 3-5 days, compared to none in placebo.
In Ver-A-T1D trial, verapamil confers non-statistically significant preservation in C-peptide in new-onset T1D
In an early morning session, Prof. Thomas Pieber (Medical University Graz, Austria) delivered full results of the year-long Ver-A-T1D trial (n=136), evaluating verapamil on beta cell function preservation in adults with new-onset stage 3 T1D. As background, verapamil is a calcium channel blocker used as an antihypertensive agent for over 40 years. Verapamil also lowers beta cell TXNIP (thioredoxin-interacting molecule), a stress molecule that promotes beta cell apoptosis. Human studies in 2018 and 2023 have also suggested preserved C-peptide in individuals newly diagnosed with T1D. Hence, this RCT aimed to assess the effect of verapamil 360 mg vs. placebo on the preservation of beta cell function in people with new-onset stage 3 T1D.
- Study design and baseline characteristics. 136 participants recently diagnosed with T1D were randomized 2:1 to once-daily oral verapamil or placebo treatment for 12 months. At baseline, participants were an average of 29 years old, with 68% being male. Clinically, participants had A1c of 7.9%, BMI of 24 kg/m2, total daily insulin dose of 0.32 U/day, and C-peptide AUC of 0.86 mmol/L.
- Results. The trial did not meet the primary endpoint, as the change in C-peptide AUC from baseline did not differ significantly between verapamil and placebo (p=0.063). Nonetheless, as shown in the figure below, the intention-to-treat analysis showed verapamil numerically maintained C-peptide, while placebo declined modestly. Prof. Pieber explained that C-peptide decline in the placebo group was smaller than anticipated (experiencing ~10% loss) compared to prior studies, which likely made the threshold for clinically meaningful difference of 0.18 nmol/L/min “not appropriate” for the study. Per-protocol analysis, excluding withdrawals (n=13), discontinuations (n=7), and administrative or dispensing errors (n=2), found that verapamil significantly reduced C-peptide AUC (p=0.034).
- Secondary endpoints. Verapamil consistently lowered A1c by 0.3 to 0.5 percentage points compared to placebo – the difference of which was statistically significant for the first six months (p=0.001) but not at the numerically by 12 months (p=0.128). There was no significant difference in the insulin dose. Similarly, there were no significant differences in CGM metrics (TIR and TITR) at 1, 3, 6, 9, and 12 months between verapamil and placebo groups.
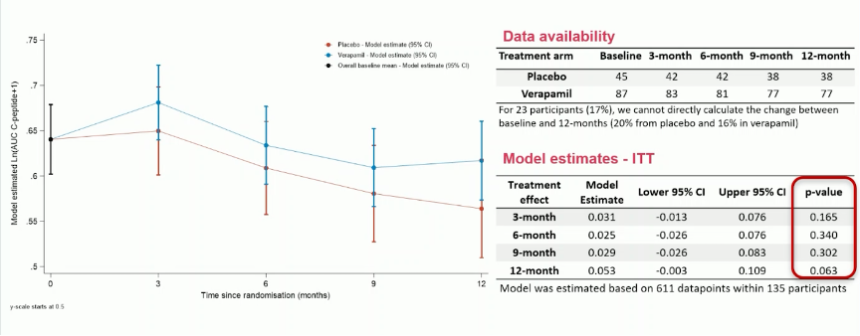
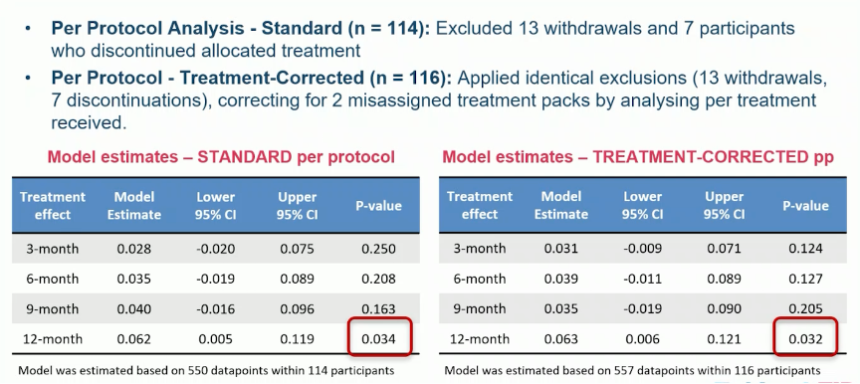
- Safety. Overall, verapamil was safe and generally well-tolerated in adults with no unexpected adverse events. Adverse events occurred at similar rates (97% vs. 94% in placebo), and serious adverse events were more prevalent in the placebo group (11%) than verapamil (7%). Two life-threatening events happened in the verapamil group — one severe hypoglycemia from accidental insulin overdose and one suicide attempt — which were deemed unrelated to the drug. Verapamil also caused expected side effects, including constipation (14% vs. 2%) and diarrhea (7% vs. 2%), mild first-degree atrioventricular (AV) block (20% vs. none), bradycardia (14% vs. 4%), and palpitations (4% vs. 4%). Neither second- or third-degree AV blocks nor hypotension occurred. All CV events were mild and reversible with dose reduction and did not lead to drug discontinuation.
- Verapamil may be an ideal candidate for combination therapies with other immune-modulating agents, given the favorable safety profile and the direct beta cell protection, Prof. Pieber said. Going forward, longer-term effects of verapamil (over three years of treatment) continue to be assessed in the open-label extension Ver-A-Long trial. Investigators also hope to conduct the T1DPlus to test possible drug combinations with verapamil.
“There's no insulin like your own”: Two-year outcomes of the BANDIT trial demonstrate JAK inhibitor baricitinib preserves C-peptide
Dr. Michaela Waibel (St. Vincent’s Institute of Medical Research, Australia) delivered two-year outcomes of the phase 2 BANDIT trial (n=91), which evaluates JAK 1/2 inhibitor baricitinib in individuals with new-onset T1D. As background, certain immune cells require JAK-associated intracellular signaling molecules, so JAK1 and JAK2 inhibitors may be able to impair immune function to prevent the death of beta cells. This drug class is indicated for autoimmune diseases, such as rheumatoid arthritis and alopecia areata. In 2023, the BANDIT trial showed that baricitinib significantly preserved mixed-meal-stimulated mean C-peptide level compared to the placebo group (p=0.001) at Week 48. The presentation shared results of the two-year follow up of this study.
In addition to baricitinib, several JAK inhibitors are being assessed in T1D, such as JAK1 inhibitor abrocitinib and JAK3/TEC inhibitor ritlecitinib in the JAKPOT T1D trial.
- Trial design and baseline characteristics. 91 participants diagnosed with T1D within the past 100 days aged 10-30 years were randomized 2:1 to baricitinib (4 mg per day) or placebo. 89 participants were followed for 96 weeks. At baseline, the mean age was 18 years old, with vast majority being white. A1c across both treatment arms ranged from 7% to 7.5%, and the baseline median of the mixed-meal–stimulated mean C-peptide level at screening ranged from 0.6 to 0.67 nmol/L/min. See more details about baseline characteristics here.
- Results. Baricitinib significantly preserved C-peptide during the treatment but not beyond, as the difference lost the statistical significance at Week 96. Insulin requirement was similarly reduced during the treatment period but did not last beyond Week 48 (see figure below). A1c was not significantly different across all time points. While TIR was significantly improved for baricitinib group early treatment period, the effect diminished over time. Subgroup analysis further suggested that the benefits of baricitinib on C-peptide preservation and A1c reduction may be greater among adults (18-30 years) than children (10-17), though the study was not powered to detect differences. The treatment is well-tolerated and safe.
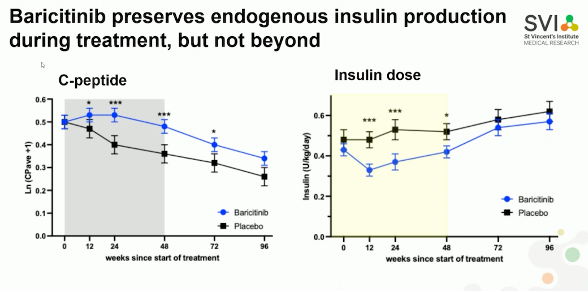
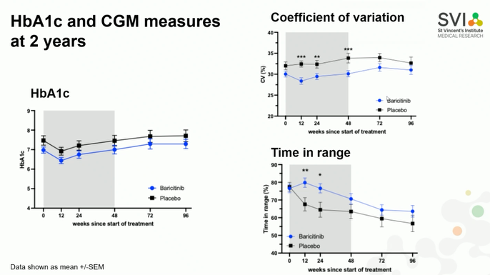
- Additional analyses. Pharmacological studies confirmed that the JAK-STAT pathway inhibition with baricitinib is reversible, as there is no difference in STAT3 phosphorylation 24 hours after a dose. By age groups, there was no difference in STAT3 phosphorylation or inhibition from baricitinib. These results were consistent with STAT1 and STAT5 phosphorylation. In another analysis evaluating potential effects on alpha cell function, baricitinib group seemed to experience slight decline in glucose response across the study. Further analysis by responders (n=48) and non-responders (n=12) to baricitinib had statistically significant differences in C-peptide preservation (p<0.001), A1c (p=0.004), and insulin dose (p=0.001). Dr. Waibel reported that BMI ≥30 kg/m2 and adherence rate ≥80% numerically predicts the response. As we do, she looks forward to larger phase 3 trials.
Fr1da study shows insights into single islet antibody prevalence and progression in children
In an oral session, Prof. Sarah Schill (Technical University Munich, Germany) presented findings from the Fr1da study, which was extended in October 2019 to include the detection and follow-up of single islet autoantibody positivity. Given the importance of early intervention and treatment, the field has focused on improving public awareness and screening initiatives to diagnose T1D, defined as the presence of two or more confirmed positive islet autoantibodies. The current study assessed the prevalence, persistence, and outcomes of single islet autoantibody positivity and progression to early-stage or diagnosis of T1D.
- Methods. The study screened for autoantibodies using ELISA and LIPS assays, followed by confirmatory testing with radio-binding assays. The detection of a single autoantibody was determined using three to six times higher cut-off values than those used for multiple autoantibody positivity. The study recommended at least three years of annual follow-up for children who tested positive for a single islet autoantibody; three to four years of rescreening was recommended for children who tested negative.
- Results. Between October 2019 and March 2025, the study enrolled 104,276 children. Nearly the entire study population had sufficient blood samples for screening. 0.25% of children were diagnosed with early-stage T1D, and 22% of this population progressed to clinical diabetes. During a follow-up period, 9% of children no longer showed positive detection of autoantibody positivity, 12% developed early-stage T1D, and 79% remained positive for single autoantibody detection. After a median of two years, four children within the population who maintained single autoantibody positivity developed clinical diabetes. When 11,181 children who tested negative for autoantibodies in the first screening round were retested at a later age, 0.1% were positive for one autoantibody and 0.21% were diagnosed with early-stage T1D.
- Discussion. Reflecting on these results, Prof. Schill highlighted the importance of screening and follow-up among children with single islet autoantibodies to help detect clinical T1D diagnosis. Furthermore, Prof. Schill encouraged rescreening efforts to routinely follow children with single and multiple autoantibodies in the first screening.
“The era of diagnosis”: Survival rates for T1D increased over decades
In an engaging afternoon address, Dr. Astrid Lavens (Sciensano, Belgium) explored the “impact of the era of diagnosis” on T1D mortality trends. Ultimately, it was great to see in this presentation data on survival rates for those with T1D increasing. Although mortality rates for people living with T1D have markedly declined over the past two decades, age-standardized mortality rates for people with T1D remain two-to-five times that of people without diabetes, and up to 8.5 times higher for children and adolescents with T1D. This cross-sectional, real-world observational study sought to analyze mortality rates between 15- and 25-years post diagnosis among people living with T1D in Belgium diagnosed between (i) 1985-1998 (group A; n=345) and (ii) 1998-2009 (group B; n=948).
- Study design. Using a nationwide register, researchers collected data on adults diagnosed with T1D before age 30 in Belgium between 2001-2022. A baseline profile on clinical, demographic, treatment, and complication data was collected 15 years after diagnosis for each participant. At 25 years post-diagnosis, investigators collected data on vital status and year of death.
- At baseline, group B (participants diagnosed between 1998-2009) had higher rates of obesity and were more likely to be on lipid-lowering therapy, compared to group A (those diagnosed between 1985-1998) (p<0.05; p<0.05). However, group B were less likely to be on antihypertensive therapies (p<0.01). Notably, group A had a significantly higher average A1c of 8.3 compared to group B, whose mean A1c was 8.1 (p<0.05). There was no difference in the rates of complications like diabetic retinopathy and albuminuria.
- Survival rates 25 years after diagnosis were far better for those diagnosed in the “later era” (1998-2009). Specifically, group A conferred a significantly higher incidence of mortality 25 years post-diagnosis compared to group B (see below; p<0.0079). Standardized mortality rates (SMR), calculated by dividing observed deaths by expected deaths, also significantly differed between the two groups, with group A conferring an SMR of 4.14, while group B demonstrated an SMR of 2.28 at 25 years post-diagnosis. Interestingly, a higher A1c (HR 1.08; p=0.0087) and age (HR 1.49; p=0.0019) 15 years post-diagnosis were associated with an increased risk for all-cause mortality 25 years post-diagnosis.
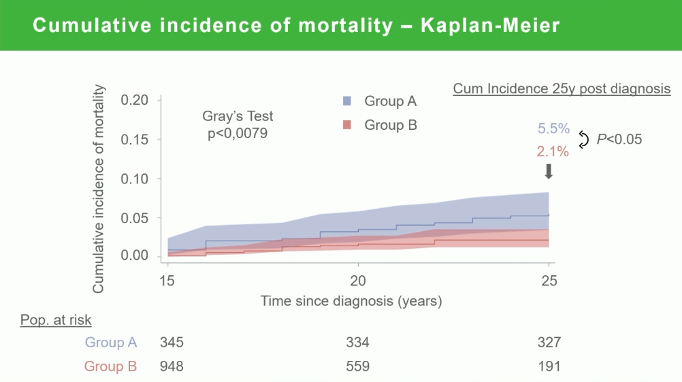
Diabetes Complications
CKD and T1D: Profs. Heerspink and Rossing argue status quo must change
In this afternoon symposium sponsored by Bayer, Prof. Per Henrik Groop (University of Helsinki, Finland) chaired a session on T1D and chronic kidney disease (CKD), featuring panelists Dr. Hiddo Heerspink (University of Groningen, the Netherlands), Prof. Peter Rossing (University of Copenhagen, Denmark), and diabetes advocate and person with T1D Mr. Uros Bogdanovic (KrAn Studio, Serbia). All four speakers highlighted how little management of CKD has changed for people with T1D in the last few decades, despite the fact that nearly one-third of people with T1D will develop CKD in their lifetimes. Bayer’s Kerendia (finerenone) was referenced throughout the conversation as a potential management tool for T1D and CKD.
- Dr. Heerspink emphasized the need to close the treatment gap for people with T1D and CKD. Although T1D and T2D differ in etiology, they share similar downstream mechanisms of hyperglycemia-driven inflammation and tissue damage, making albuminuria (uACR) a key bridging biomarker for clinical trials. He explained that early reductions in albuminuria strongly predict slower CKD progression, as demonstrated by finerenone’s effects in the FIDELIO-DKD and FIGARO-DKD trials where 87% of kidney outcome benefits were explained by albuminuria reduction. Importantly, he noted that the FINE-ONE trial, a global phase 3 study evaluating finerenone in CKD associated with T1D, is now complete. He also cited a just-published article (at the time of the presentation, it had not yet been published!) that will provide pivotal data using albuminuria as a surrogate endpoint to accelerate evidence translation without requiring prohibitively large, long-term outcome studies. With the projected rise in T1D prevalence by up to 107% by 2040, studies like FINE-ONE represent a crucial step toward expanding evidence-based treatment options for this underserved population.
- Prof. Rossing stressed the importance of initiating treatment for CKD as early as possible, noting that preserving kidney function from the outset leads to better long-term outcomes and extended life expectancy. However, he acknowledged that current healthcare resources and the lack of definitive data prevent the initiation of preventative therapy at the point of T1D diagnosis. He highlighted the need for clear biomarkers that can identify high-risk individuals before albuminuria becomes elevated, allowing for earlier and more targeted intervention. Prof. Rossing linked this approach to the rationale behind the CONFIDENCE study, which focuses on albuminuria reduction as a proxy for kidney protection and improved cardiovascular outcomes. He addressed the critical role of regular screening in enabling earlier detection and advocated for therapies such as finerenone to be administered as early as possible to delay or prevent CKD progression in people with T1D.
- Mr. Bogdanovic discussed how people with T1D are often told they can manage their condition well to avoid complications. When people then go on to develop complications, he added that they face a psychosocial burden of “failure” to prevent this progression, based on messaging patients previously received. He noted that although patients are generally aware of complications as a broad concept, there is insufficient education about the risk factors, progression, and treatment of CKD and that CKD is often conflated with dialysis. Mr. Bogdanovic highlighted the need for earlier and more individualized discussions about complications, as current conversations typically occur only once problems emerge, and for healthcare providers to go beyond a narrow focus on blood glucose management to consider patients’ emotional and psychological well-being. He stressed the importance of peer-to-peer support as a vital component of education and emotional resilience. Importantly, he agreed with other panelists that while diabetes technology has advanced rapidly, many medications for diabetes complications are designed and tested for T2D rather than T1D, leaving a status quo for complication management that is suboptimal.
- Dr. Heerspink echoed his concerns that there have been no new therapies for T1D-related CKD in decades and highlighted the CURE-CKD US patient registry showing that 27.1% of people with T1D have CKD. Nearly four out of five of this population were prescribed RAS inhibitors, which are the only guideline-recommended therapy currently available for this cohort.
Revolutionizing cardiometabolic health: Novo Nordisk’s industry symposium focuses on the kidney, liver, and weight management
Featuring a grand entrance with a hologram, Novo Nordisk’s industry symposium held insightful sessions on revolutionizing cardiometabolic health. Dr. Alice Cheng (University of Toronto, Canada) and Prof. Mikael Ryden (Karolinska Institute, Sweden) chaired the session focused on the expanding spectrum of cardiometabolic phenotypes. A select group of faculty members focused on the broad range of cardiometabolic health, including Prof. Christoph Wanner (University Hospital of Würzburg, Germany) on the kidney with approaches on CKD and Prof. Laurent Castera (Université Paris-Cité, France) on the liver with emerging research that expands optimal clinical outcomes. Prof. Antje Koerner (University of Leipzig, Germany) concluded the session by focusing on the pediatric population with obesity, encouraging new strategies for weight management.
- Prof. Wanner on the kidney with synergistic strategies across cardiometabolic diseases. Prof. Wanner started by highlighting alarming statistics that characterize CKD as a growing global challenge, with an increase in mortality rates associated with risk factors. He emphasized that CKD serves as a potent risk amplifier, as: (i) more than 50% of people with CKD have obesity; (ii) 40% of people with diabetes have CKD; (iii) 35-40% of people with CKD have CVD; and (iv) 35-45% of people with heart failure have CKD. Despite these statistics, he’s been encouraged by the pillar approach to treat CKD and diabetes, which now includes RAAS blockade, SGLT-2 inhibitors, finerenone, and semaglutide.
- Prof. Wanner reviewed the pivotal FLOW trial (n=3,533), in which semaglutide demonstrated a 24% reduction in the risk of kidney events. In this trial, kidney and CV components of the primary composite endpoint contributed to the risk reduction. As well, in the SELECT trial (n=17,604), semaglutide reduced the risk of kidney events by 22% compared to placebo in people living with overweight or obesity and CVD, with macroalbuminuria and onset of persistent eGFR components contributing to risk reduction. Furthermore, in the SMART trial (n=125), semaglutide showed improvements in albuminuria compared to placebo in people living with obesity and CKD. Reflecting on the abundant number of trial outcomes, Prof. Wanner pointed to the multifactorial benefits of semaglutide in kidney function with both direct (e.g., natriuresis, hemodynamic effects, endothelial function, anti-inflammation, inhibition of RAAS) and indirect effects (e.g., glycemic management, blood pressure, weight loss).
- Prof. Castera on MASH with integrating emerging data into clinical pathways. As a hepatologist, Prof. Castera clarified that while liver disease has long been attributed to alcohol-related conditions, the risk of MASLD increases with the number of coexisting cardiometabolic comorbidities. He emphasized the unmet need, especially among people with obesity or T2D who are at an increased risk of developing MASH. Globally, up to 66% of people with T2D and MASLD have MASH, and up to 34% of people with obesity have MASH. Many patients are unaware of their diagnosis, further leading to severe complications, CV events, and increased mortality. In fact, MASH-driven fibrosis and cirrhosis can cause 16x higher risk of liver-related mortality, 4x higher risk of all-cause mortality, and 4x higher risk of CV events.
- While it’s important for diagnosis and early screening, Prof. Castera emphasized that biopsy is impractical with many limitations (e.g., invasive, associated morbidity and mortality, sampling variability, expense). There’s also a limited number of hepatologists and pathologists. Therefore, Prof. Castera proposed that non-invasive tests can help stratify people for liver fibrosis in different clinical settings, including blood tests that include FIB-4 as a widely available option and ELF as a direct serum measurement of hepatic fibrosis. He also explained the advantages of imaging with VCTE, which measures liver stiffness as a surrogate for fibrosis and cirrhosis. Given the importance of non-invasive tests, the EASL-EASD-EASO 2024 guideline reflects sequential testing of MASLD.
- Turning to treatment options, Prof. Castera explained that long-term improvement in MASH can be achieved by targeting cardiometabolic and hepatic mechanisms with semaglutide. As a reminder, semaglutide is now approved for MASH based on the phase 3 ESSENCE trial (n=1,200).
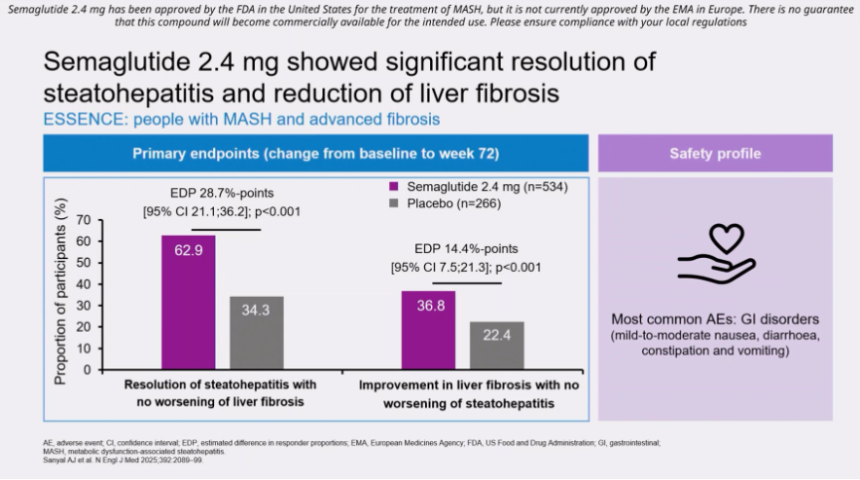
- Prof. Koerner on focusing on childhood with new paths in obesity management.The global prevalence of childhood obesity has remained a challenge and will only continue to grow. Global estimates show that there were 11 million children with obesity in 1975, compared to 175 million in 2020. In 2035, the prevalence is expected to double, with 380 million estimated in 2035. Early childhood serves as a critical period for the manifestation of childhood obesity, and 90% of childhood obesity persists into adulthood. Without addressing obesity, children will face serious complications seen in adult obesity. Specifically, childhood obesity has a strong association with 5x increased risk of obesity, 4x increased risk of T2D, 3x increased risk of CV mortality, and 1.3x increased risk of cancer. Therefore, early childhood serves as a “critical window” for intervention, especially for the remission of CV risk factors.
- Currently, semaglutide is approved for ages ≥12 years based on the results of the STEP TEENS trial (n=201), in which semaglutide conferred a significant 18% body weight reduction, and almost half of the trial participants treated with semaglutide achieved a BMI below the obesity threshold. However, while treatment options remain, Prof. Koerner urged even earlier stages of intervention. Focusing on ages ≥6 years, the STEP Young trial (n=210) is studying two-year semaglutide treatment in children; this trial is expected to complete by the end of next year. Additionally, the STEP Teens Weight Maintenance trial (n=500) is focusing on weight loss maintenance; this trial is expected to be completed in 2031.
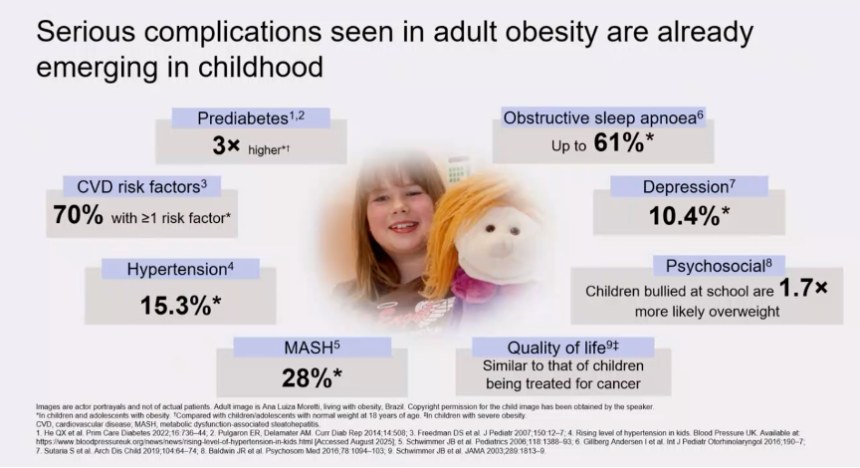
Fructose consumption may play a key role in the development of MASLD
Interest was high in this very “basic science”-heavy oral presentation by Dr. Florine Westerbeke (Amsterdam University, the Netherlands), whose work suggested a potential new physiological pathway for the development of metabolic dysfunction-associated steatotic liver disease (MASLD). Dr. Westerbeke began by emphasizing, as we have heard time and again, about MASLD’s worldwide prevalence, with the condition affecting approximately one-third (!) of the global population and expected to rise to 55% by 2040. Genetic factors such as the PNPLA3 and TM6SF2 genes have been linked to the development of the condition, as well as related conditions like diabetes, obesity, and cardiovascular disease (CVD), and environmental factors including diet and the gut microbiota. In this work, Dr. Westerbeke and colleagues focused on the latter two factors, using RNA sequencing to identify fructose-associated gene expression changes related to MASLD. Fasting fructose levels were found to be higher in patients with MASLD, independent of fasting glucose levels, with a strong dietary component suggested for this effect. These levels have also been linked to mitochondrial dysfunction in patients with obesity. Fructose-associated toxicity related to the gut microbiome may also play a key role in MASLD pathogenesis.
- In the study, RNA sequencing was performed on liver, jejunum, and visceral adipose tissue (VAT) biopsies obtained during surgery that occurred during the BARIA study (n=304), a prospective bariatric surgery cohort. Plasma fructose levels were also measured in 39 subjects when fasting and two hours post-meal in a preoperative mixed meal test (MMT), as well as intraoperatively in peripheral and portal vein blood in 38 subjects. Differential gene expression analysis was performed for each tissue using DESeq2 to identify significant differences in the genes expressed in the tissues and gene expression changes associated with MASLD. The mean age was 48 years, 77% of participants were female, 24% had T2D, and 62% were found to have MASLD.
- Fructose metabolism by the liver leads to lipogenesis, alongside fermentation by the gut microbiota, which may play a key role in MASLD. Classically, the metabolism of fructose is known to create fatty acids in the body, known as lipogenesis. However, in the liver, this metabolic process is considered unregulated, as it bypasses the rate-limiting steps seen in glycolysis. With rapid hepatic fructose metabolism, the ChREBP/SREBP-1c genes are activated, leading to an upregulation of lipogenic enzymes. In the gut, excessive fructose can lead to its fermentation by the gut microbiota, leading to the production of ethanol and acetate, two toxic metabolites, and lipogenesis causing MASLD. The gut dysbiosis caused by these metabolites can have harmful systemic effects.
- MASLD is associated with higher fasting fructose levels, independent of glucose levels. This distinction was then used in the differential gene expression analysis to determine that 3,969 genes were differentially expressed in the liver in patients with MASLD, with the majority being downregulated.
- Using “functional enrichment” analysis[1],” the authors determined that increased fasting fructose levels are linked to mitochondrial dysfunction in patients with obesity. Downregulation of genes involved in all complexes of the electron transport chain in the process of oxidative phosphorylation was demonstrated, highlighting impaired energy metabolism in these individuals. Mechanistically, the key PPARGC1A gene, a master regulator of mitochondrial biogenesis, was identified as a link between increased fasting fructose levels and MASLD.
- Fasting peripheral fructose concentrations correlate with postprandial ethanol production, a sign of gut dysbiosis that can lead to lipogenesis and MASLD. In particular, these levels were associated with Streptococcus parasanguinis, which has previously associated with gut dysbiosis. This can result in impaired digestion and metabolism, and a decreased quality of life overall. In all, fasting fructose levels based on diet increase mitochondrial dysfunction and gut dysbiosis, which may represent a yet-underexplored pathway in the development of MASLD.
Precision medicine in T2D: Targeting GLP-1 RAs and SGLT-2 inhibitor combination treatment for kidney protection
Dr. Thijs Jansz (University of Exeter, UK) presented compelling data supporting combination therapy of GLP-1 RAs and SGLT-2 inhibitors for the prevention of kidney disease in T2D. Dr. Jansz began with a compelling analogy: if one were to find themselves in an apartment with no heat in the winter, should one get an electric blanket or a space heater? He explained that each have different benefits, but one might reasonably conclude that using both would provide the greatest benefit. In the same vein, Dr. Jansz set out to quantify the additive effects of taking GLP-1 RAs in combination with SGLT-2 inhibitors. SGLT-2 inhibitors have demonstrated renal-protective effects in people with T2D, and recent trials have also demonstrated that GLP-1 RAs reduce the risk of kidney failure. However, studies have yet to evaluate the benefit of GLP-1 RAs for patients already taking SGLT-2 inhibitors, leading to this work. Dr. Jansz and colleagues evaluated whether the benefits of these therapies are applicable to all patient subgroups, and if combination therapy has an additive effect. Positive results were found for both research questions.
- Methods. Clinical Practice Research Datalink EHR data from 2013-2023, a UK primary care database, was used to identify adults with T2D and healthy kidney function (eGFR ≥60mL/min/1.73m2) who started a GLP-1 RA (n=40,112), SGLT-2 inhibitor (n=122,343), both a GLP-1 RA and an SGLT-2 inhibitor (n=21,223), or the comparator drugs DPP-4 inhibitors or sulfonylureas (n=143,392). Treatment effects on kidney disease progression were evaluated over three years using Cox proportional hazards models with ≥50% eGFR decline, end-stage kidney disease, or kidney-related death as endpoints. The CKD Prognosis Consortium (CKD-PC) risk score for kidney disease progression was used to identify those with greatest benefit from GLP-1 RA and SGLT-2 inhibitor combination treatment. Patients taking GLP-1 RAs were more likely to be female, white, and have a higher BMI compared to the other treatment groups.
- The incidence of kidney disease progression was lowest with GLP-1 RA and SGLT-2 inhibitor combination treatment (incidence rate of 2.8 per 1000 patient-years), followed by SGLT-2 inhibitors only (3.2 per 1000 patient-years), GLP-1 RAs only (4.7 per 1000 patient-years), and DPP-4 inhibitors or sulfonylureas (5.5 per 1000 patient-years). SGLT-2 inhibitors were found to have the broadest benefit across all patient populations. GLP-1 RA and SGLT-2 inhibitor combination treatment was associated with a 55% lower risk of kidney disease progression compared to DPP-4 inhibitors or sulfonylureas (HR 0.45). This was greater than the relative risk reductions with GLP-1 RA use alone (HR 0.69) or SGLT-2 inhibitor use only (HR 0.57) compared to DPP-4 inhibitors or sulfonylureas. Compared to SGLT-2 inhibitor use only, GLP-1 RA and SGLT-2 inhibitor combination treatment was associated with a further 21% risk reduction (HR 0.79). To confirm the additive effect of combination therapy, an interaction term for GLP-1 RAs and SGLT-2 inhibitors was non-significant, suggesting that GLP-1 RAs provide added renal benefit on top of SGLT-2 inhibitor treatment.
- A risk score may be useful for targeting the use of combination therapy. Dr. Jansz demonstrated that the top 10% of patients at greatest risk of kidney disease as calculated by the CKD-PC risk score would have a three-year NNT of 169 for combination therapy compared to SGLT-2 inhibitor use alone. This is compared to a NNT of 2005 for the bottom 10% of patients at lower risk of kidney disease.
- This strong performance demonstrates that GLP-1 RAs have particular benefit in addition to SGLT-2 inhibitors for patients at highest risk of kidney disease – the use of the CKD-PC risk score may provide a pathway to precision medicine. “When winter comes for the kidneys,” Dr. Jansz said, you should first reach for an SGLT-2 inhibitor. If it gets really cold, you might consider using the CKD-PC risk calculator to add on a GLP-1 RA as well.
Phase 2b PROGRESS trial results show AAK1 inhibitor pilavapadin (LX9211) reduces pain in DPN; findings support phase 3 trial for 10 mg dose
In a well-attended afternoon oral session, Dr. Rodica Pop-Busui (Oregon Health & Science University) presented results from the phase 2b PROGRESS dose optimization trial (n=496), investigating oral, non-opioid AAK1 inhibitor of pilavapadin (LX9211) in adults with moderate to severe diabetic peripheral neuropathic pain (DPNP). As a reminder, the PROGRESS trial follows FDA feedback in May 2023 and phase 2 results from the RELIEF-DPN-1 and RELIEF-PHN-1 study. The key goal of this study was to improve pilavapadin’s tolerability and optimize its dosing scheme. Lexicon simultaneously announced the results today in a press release, following initial topline results from 4Q24.
- Trial design and baseline characteristics. Adults with T1D or T2D were randomized to one of four treatment arms: (i) placebo; (ii) pilavapadin 10 mg; (iii) pilavapadin 20 mg for seven days followed by 10 mg thereafter (20/10 mg); and (iv) pilavapadin 20 mg. At baseline, participants’ mean average daily pain score (ADPS), where a higher score indicates greater pain intensity, was 6.9. Participants received treatment for eight weeks, followed by a four-week, single-blind placebo safety period and were allowed up to three grams of acetaminophen per day as rescue medication for DPNP. As previously announced from Lexicon’s 4Q24 topline results, most participants had moderate pain at baseline, defined as an ADPS score of 5-7 (77%; n=246), while the remainder of participants were classified as having severe pain (i.e., ADPS score of 8-9). Average duration of DPN was 6.6 years.
- All doses, including placebo, significantly reduced ADPS from baseline to Week 8 (p<0.001). In the PROGRESS study, the 10 mg daily dose conferred a 1.7-point reduction, 20/10mg daily dose a 1.8-point reduction, 20 mg daily dose a 1.4-point reduction, and placebo a 1.3-point reduction – with similar results seen in the RELIEF-DPN study (see below). Given statistical analysis was powered for dose-dependent reduction, the study did not reach statistical significance with its primary endpoint (p=0.11). However, a post-hoc analysis excluding the 20 mg arm did indicate primary endpoint significance (p<0.04), showing an early separation from placebo that persisted throughout the study.
- On the nonlinear dosing effect seen in the 20 mg dose in both PROGRESS and RELIEF-DPN (see below), Dr. Pop-Busui hypothesized that tolerability issues may have deterred patient adherence. Future trials will focus on the more tolerable 10 mg dose.
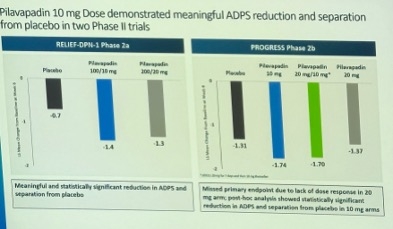
- PROGRESS demonstrated a more favorable tolerability profile than RELIEF-DPN – which used a 100 mg and 200 mg loading dose on Day 1 before subsequent daily administration of 10 mg and 20 mg, respectively. Most adverse events in all treatment arms were mild-to-moderate, with dizziness and nausea being most frequent. Adverse events were more frequent in the pilavapadin 20 mg group (n=61) than in the 10 mg group (n=44).
- In a discussion with the CC team at EASD, CMO Dr. Craig Granowitz shared that participants did not experience a rebound effect after initiating the four-week placebo safety period. Rather, participants who received pilavapadin gradually returned to baseline levels of ADPS. Treatment groups did not exhibit liking behavior during the safety period.
- PROGRESS results support advancement of pilavapadin 10 mg into phase 3 trials as a promising non-opioid treatment for DPNP. While Dr. Pop-Busui refrained from commenting on next steps at EASD, Dr. Granowitz shared in 4Q24 that there will likely be two two-armed pivotal trials, each with 300-400 participants, examining pilavapadin 10 mg. The primary endpoint will likely be a placebo-adjusted 0.6-point drop in ADPS, following the PROGRESS trial’s design. Other endpoints, according to the same Lexicon’s 4Q24 pipeline update, will include changes in sleep interruption, burning pain, and acetaminophen use. The phase 3 program will also consider demographics of participants, as PROGRESS included twice as many African American participants compared to RELEIF-DPN-1.
- As the first nonopioid treatment in DPN in two decades, pilavapadin could fill a need for nine million people in the US with progressive DPN. Among this population, 60% have tried multiple treatments, as most therapies do not provide sufficient relief, and a third have resorted to opioid treatments for short-term pain relief, which can increase the risk of opioid addiction.
EASD-EASL joint symposium: Bridging the gap with improved screening and the use of combination therapies
In a packed morning joint symposium, Prof. Laurent Castera (University Beaujon Hospital, France) and Prof. Philip Newsome (King's College London, UK) discussed advancements in awareness, screening, and therapies for liver complications that are prevalent in people with T2D. With metabolic dysfunction-associated steatotic liver disease (MASLD) now affecting an estimated 65% of the global T2D population, their insights underscored a paradigm shift toward earlier detection and more targeted metabolic therapies for liver health in T2D.
- Prof. Castera opened the session by addressing the many barriers to diagnosing MASLD, including limited histopathology and lack of awareness of best diagnosis practices. The QUID-NASH program aims to develop a virtual liver biopsy for the diagnosis and staging of MASH in people with T2D. He highlighted a study (n=330) conducted by the program which showed that 58% of people with T2D and MASLD also had MASH, emphasizing the importance of screening. Importantly, he discussed best practices for non-invasive tests (NITs), including FIB-4 and ELF. Prof. Castera also emphasized the utility of liver stiffness measurements (LSM) in predicting clinical outcomes. One study (n=10,920) found that an LSM increase of >30% was a strong predictor of subsequent liver-related events in patients with MASLD. He called for a broader consensus around guidelines for clinically-relevant LSM increases.
- Prof. Newsome then provided an overview of the role of glucagon dysfunction in MASH, with a focus on emerging GLP-1 RA combination therapies that address the dysfunction. In MASH, combined agonism of GLP-1, GIPR, and GCGR suppresses appetite, boosts insulin secretion, and drives mitochondrial turnover, fatty-acid oxidation, lipolysis, and thermogenesis. This incretin/glucagon combination reduces hepatic steatosis, inflammation, and fibrosis while improving glucose homeostasis. Prof. Newsome reviewed results from the phase 3 ESSENCE trial which showed that semaglutide drove a 63% resolution of steatohepatitis without fibrosis worsening versus 34% in placebo and a 37% fibrosis improvement without steatohepatitis worsening versus 22% in placebo.
- In a phase 2b trial (n=834), adults with overweight or obesity and T2D were treated with cotadutide (GLP-1/ glucagon RA) and liraglutide (GLP-1 RA). Participants on cotadutide demonstrated dose-dependent weight loss up to 6 kg (~13 pounds) and ALT reductions up to 14%, significantly outperforming liraglutide (3 kg weight loss, 6.24% ALT reduction) and placebo (1 kg weight loss, 1% ALT reduction). These findings underscore the added benefit for liver health when a glucagon RA is added into treatment. Similar benefits were observed with survodutide (GLP-1/ glucagon RA) and retatrutide (GLP-1/GIP/GCGR receptors). Prof. Newsome urged the audience to consider that the significant hepatic benefits observed with incretin/glucagon combination therapies support their consideration as first-line treatments for improving liver health in patients with metabolic dysfunction disorders.
Hyperglycemic crises: Q&A offers insight into best practice guidelines on DKA management
In an innovative session style, Prof. Jan Gojda (Charles University, Czech Republic) led Dr. Shivani Misra (Imperial College London, the UK) and Dr. Rodolfo Galindo (Emory School of Medicine) in a Q&A presentation designed to address the recent consensus guidelines on hyperglycemic crises. Dr. Galindo encouraged participation by noting, “You all showed up to ask questions of us! So, ask!” The session focused on translating consensus guidelines into clinical practice, particularly on determining appropriate levels of care for diabetic ketoacidosis (DKA).
- To engage attendees, the panel first polled the audience on their current use of blood, serum, and urine ketone testing, using this feedback to highlight regional variations in practice and to emphasize that new diagnostic tools should only be developed when there is clear clinical utility. Dr. Galindo stressed that mild DKA should not automatically require ICU admission, as such treatment escalation may increase the risk of hospital-related complications, and instead endorsed protocols using short-acting subcutaneous insulin administered every one to two hours in lower-acuity settings.
- On the role of CGM and CKM as wellness devices, Dr. Misra cautioned the audience that CGM as a wearable for a healthy population has a lot of great use cases, but the research and clinical communities have not yet established appropriate targets for a population without diabetes. She said, “We have not defined the parameters of normalcy [in analyte sensing] in the general, healthy population.” Both Dr. Misra and Dr. Galindo pointed to the need for further research into ketone physiology before CKM is widely implemented.
- The discussion also addressed CGM’s role in DKA management, with Dr. Galindo cautioning that its maximum reading is 400 mg/dL and that there is lag time, concluding, “I do not recommend CGM for the treatment of DKA. CGM is great for outpatient use to prevent DKA, but it is not valid for the treatment once the crisis has started.” More broadly, the panel highlighted that this consensus guidance is not purely scientific but also pragmatic, taking into account nursing workflows, institutional resources, and the need for multiple tiers of care to ensure global applicability.
EASD-CEDA Joint Symposium: Diabetic complications in the era of precision medicine
This well-attended session was hosted by the EASD alongside CEDA – the European Center for Diabetes - which the chairs described as “the second diabetes association in Europe.” Its goal was to “put neuropathy on the map of current diabetes challenges” and its focus was progress in basic neuropathy research – both in distal sensorimotor polyneuropathy (DSPN) and cardiovascular autonomic neuropathy (CAN). The speakers, including Dr. Julia Szendroedi (University Hospital Heidelberg, Germany), Dr. Péter Kempler (Semmelweis University, Hungary), and Dr. Christian Herder (German Diabetes Center, Germany), presented data which reviewed the field, attempted to understand more of the underlying mechanisms, stratified risk, and pointed the way towards more precision treatment.
- Dr. Szendroedi noted that screening studies of people with prediabetes for DSPN has yielded a wide variation of results (between <5% and 70%), because of heterogenous testing methods, study definitions and techniques, and time windows. However, gathering a range of variables (such as insulin resistance, skin AGEs, OGTT, etc.) results in risk models with predictive power. Phenotypic sub-types of prediabetes and diabetes have been developed that show different risks of developing DSPN - which Dr. Szendroedi suggested could be used at the time of diagnosis to prioritize education and treatment. Dr. Szendroedi described detailed research work to describe nerve fiber changes in DSPN. She concluded that prediabetic DPN is a mosaic of different mechanisms across patients, which therefore requires early screening.
- Dr. Kempler revealed that CAN is a strong driver of cardiovascular mortality in people with diabetes. He demonstrated that CAN results from hyperglycemia - which induces micro- and macro-vascular endothelial cell damage. He reviewed a variety of studies asserting that CAN was associated with 1.5x to 5x higher mortality. Excess mortality in the intensively managed group of the ACCORD trial (which Dr. Kempler provocatively called “not a very well-planned study”), turned out to be strongly associated with a history of neuropathy, particularly in female members of the intensive therapy group. He noted, “The lesson to be learned from the ACCORD study is that somatic and autonomic dysfunction are significant risk factors in cardiovascular disease.” Dr. Kempler finished by discussing a potential treatment - pathogenetically oriented alpha-linoleic acid (ALA) - which in his early studies has driven an impressive 45% reduction in all-cause mortality and a ~30% reduction in MI, stroke and heart failure.
- In a lightning-speed presentation, Dr. Herder presented a wealth of data connecting inflammation and DSPN. He has identified multiple new inflammation-related biomarkers that predict DSPN (based on the KORA population study in Southern Germany). This proteomics work measured 71 biomarkers and associated 26 with DSPN. Dr. Herder et al. selected six that had a meaningful correlation and gave clues to the mechanisms linking inflammation and DSPN. Dr. Herder also came back to the (pre)diabetes phenotype clusters mentioned by Dr. Szendroedi; he was able to connect the biomarkers and inflammation to these sub-types and predicted which sub-types would be at highest and lowest risk for DSPN. Importantly, these biomarkers suggested upstream drug targets (including TNF-alpha and IL-1beta). He was very excited about the ongoing INTERCEPT‑T2D trial of NLRP3 inflammasome inhibition (with dapansutrile) – which should impact IL-1beta. Secondary endpoints of the trial include biomarkers for neuropathy, though it will be a couple of years before we see the results.
Significant increases in dementia-related mortality in people with diabetes compared to those without
In a session focused on the intersection of cognitive dysfunction and diabetes, Prof. Kanika Mehta (Baker Heart and Diabetes Institute, Australia) presented findings from a population-based analysis on age-specific trends in mortality from dementia among people with and without diabetes. Alongside the increasing prevalence of diabetes and related complications, there has also been the emergence of dementia and mortality rates. In fact, some countries with high dementia rates among people with diabetes compared to those without have reported an increase in diabetes-associated mortality rates. To further investigate the relationship between dementia and diabetes, a study focused on whether mortality rates from diabetes-associated dementia differ by age and sex. Overall findings showed that dementia has generally increased at older ages, with a more significant rise among people with diabetes.
- Methods. The study used mortality data from registries from seven jurisdictions, including Australia, Denmark, Finland, France, Scotland, and Alberta and Ontario from Canada. The follow-up period was approximately 20 years. Data included mortality rates and ratios for women and men aged 60-90 years, with dementia as the underlying cause of death.
- Results. The study analyzed a total of 114,559 and 589,706 deaths related to dementia for people with and without diabetes, respectively. The trends in mortality from dementia varied across age groups but were relatively consistent for both men and women. Among ages 60 and 70, up to three jurisdictions showed increasing rates of mortality related to dementia, while others demonstrated unclear trends. At ages 80 and 90, up to six jurisdictions showed an increase in mortality rates for both people with and without diabetes, but the rates were more pronounced in those with diabetes. In Scotland, particularly, dementia in people with diabetes consistently increased, from 36% to 51% for women and 38% to 46% for men.
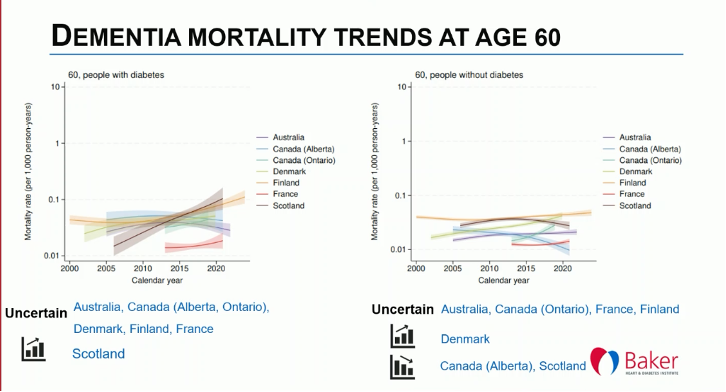
New insights into persistent and increasing burdens of diabetes morbidity
In the final session of EASD 2025, Prof. Edward Gregg (RCSI University of Medicine and Health Sciences, Ireland) outlined the changing landscape of diabetes complications, showing how multimorbidity persists and highlighting the need to move beyond single-complication research. Professor Gregg was previously at CDC in the US and we were absolutely thrilled that attendees could hear him speak.
- Prof. Gregg began that diabetes confers a two-to-three times higher risks of multiple long-term conditions. These include traditional high-risk complications including chronic kidney disease and coronary heart disease (and also easier to manage ones, like hypertension), as well as more common lower-risk conditions that involve metabolic, vascular, respiratory, aging or fragility, and mental health. While CVD mortality has sharply fallen through the decades, mortality rates from other causes have not. He also pointed out that older adults have experienced disproportionately high mortality reductions, while younger individuals have face sharper increases in rising obesity, earlier onset T2D, and increasing complications – contributing to the persistence or increase of multimorbidity. Dr. Gregg’s analysis underscores the need for new metrics which account for multimorbidity, rather than considering complications as an isolated incident.
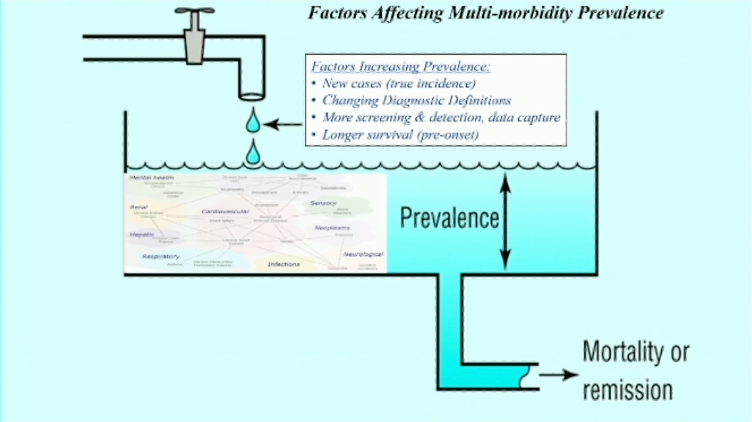
Benefits and challenges of AI-assisted screening for diabetic retinopathy and an overview of the eye health treatment landscape
In a morning session dedicated to diabetic retinopathy, Dr. Maria Cicinelli (IRCCS San Raffaele Scientific Institute, Italy), Prof. Alicia Jenkins (Baker Heart and Diabetes Institute, Australia), and Dr. Inês Pereira Marques (AIBILI, Portugal) discussed screening and the therapeutic landscape.
- Dr. Cicinelli highlighted the benefits and challenges of AI-assisted screening. As background, screening for diabetic retinopathy is typically performed via a dilated fundus exam, which can cause temporary light sensitivity and blurred vision for hours afterwards. In contrast, non-mydriatic fundus photography is now available and eliminated the need for dilation. Additionally, these pictures can be analyzed using platforms such as ARIAS (Automated Retinal Image Analysis Software), which is AI-powered and offers high sensitivity and specificity for detecting diabetic retinopathy. In addition to accuracy, Dr. Cicinelli emphasized that AI-assisted screening can positively impact screening uptake by improving patient satisfaction, such as in children. Challenges that remain include image quality issues, generalizability across populations and devices, reimbursement, and implementation into clinic workflows.
- Prof. Jenkins gave an overview of clinical trials for the lipid-lowering drug fenofibrate, which is currently under further investigation for diabetic retinopathy. In diabetes, leaky retinal vasculature can cause lipids to accumulate in the retina. Crystalline cholesterol deposits have also been observed in the retinas of people with diabetes. These conditions lead to inflammation and oxidative damage due to altered metabolism. Fenofibrate, an oral medication used to treat high cholesterol and triglyceride levels, has been investigated in the LENS trial (n=1,151), which found that fenofibrate can reduce the progression of diabetic retinopathy in people with both T1D and T2D. Currently, the Breakthrough T1D-funded FAME-1 Eye trial is underway for adults with T1D and expected to complete in 2026. There is also the Protocol AF (Fenofibrate for Prevention of DR Worsening) trial for people with T1D and T2D, which is sponsored by the Jaeb Center for Health Research.
- Dr. Pereira Marques reviewed the landscape of treatments for diabetic macular edema (DME) and diabetic retinopathy. For DME, current treatment options in the landscape and pipeline include macular laser photocoagulation, anti-inflammatory therapies (e.g., steroids, IL-6 inhibitors), anti-VEGF therapies, and gene therapies. These options are limited by factors such as variable response rates, side effects (e.g., increase intraocular pressure, cataracts), high costs, adherence, and the need for intravitreal injections (which are invasive, painful, and must be administered by a specialist). Specific therapies under investigation include the intravitreal implant ILUVIEN (see NEW DAY study), Vabysmo (faricimab) (see YOSEMITE/RHINE and RHONE-X studies), and Eylea (aflibercept) (see PHOTON study). For diabetic retinopathy, treatments options that are available or under investigation include pan-retinal photocoagulation, anti-VEGF therapies, fenofibrate, SGLT-2 inhibitors, and GLP-1 RAs, neuroprotective therapies, and gene therapies. Specific examples include ranibizumab (see PAVILION trial), phase 3 candidates APX3330 and OCS-01, and DPP-4 inhibitor sitagliptin (in the form of eye drops).
Pooled analysis demonstrates the safety and efficacy of semaglutide among people with CKD also on dialysis
In a session spotlighting the latest developments with GLP-1 RAs, Dr. Klara Klein (University of North Carolina) presented findings from a pooled analysis (n=34,064) of the SUSTAIN-6, SELECT, FLOW, and SOUL trials that studied semaglutide in people treated with dialysis. Diabetes is the leading cause of CKD, with approximately one in three adults with diabetes having CKD. The prevalence of kidney failure will only increase, as estimates project that 14.5 million people will need kidney replacement therapy by 2030, compared to just under 10 million required in 2010. Furthermore, the mortality rates of dialysis-dependent kidney failure demonstrate a staggering 60% reduction in survival rates over five years. Of note, cardiovascular complications account for more than 50% of mortality rates in kidney dialysis. Given the high unmet needs in people with dialysis treatment, this pooled analysis looked at whether semaglutide could serve as a potential intervention, given its efficacious results across CVD and CKD. We were pleased to see this descriptive study find that semaglutide was safe and demonstrated efficacy in this study’s non-randomized trial population. However, these findings also make us wonder the degree to which the placebo effect contributed to the results in some or all of these trials, as nearly 60% of those on placebo in these trials reported adverse events, compared to 25% fewer reported by those on semaglutide.
- The absence of trials establishing the safety and efficacy of GLP-1 RAs in dialysis. To date, only one trial has studied GLP-1 RAs in an outpatient dialysis setting, as far as we know. The 12-week pharmacokinetic study included 24 people treated with dialysis; 14 people were randomized to liraglutide and 10 randomized to placebo. Safety concerns of liraglutide treatment included increased rates of hypoglycemic, especially for those on insulin or SUs (approximately 20-25% of people in these trials were on insulin, tending to be on the higher end of the range for the placebo group), and GI side effects, experienced by many people on this therapy. The pooled analysis compared adverse events across four cardiovascular or kidney outcomes trials (SUSTAIN-6, SELECT, FLOW, and SOUL) in participants originally randomized to semaglutide or placebo and who initiated dialysis during follow-up. People in all trials except SELECT had T2D.
- Participant characteristics between groups that received semaglutide and placebo were similar[2]. Of note, more participants in the placebo group were treated with insulin (20% in the semaglutide group vs. 25% in the placebo group). The mean duration of follow-up was around one year in both groups. Among participants who initiated dialysis, 71 and 94 participants in the semaglutide and placebo groups continued treatment, respectively.
- Similar adverse events occurred between the semaglutide and placebo groups. A high percentage of people in all of the treated arms experienced side effects, underscoring the degree of illness in this often difficult-to-treat population. The proportion of participants experiencing severe adverse events were similar between the semaglutide (45%) and placebo group (57%). In terms of cardiovascular events, however, researchers noticed that the event rate of severe adverse events for semaglutide originally looked higher in the semaglutide group (162 events/100 person years) compared to the placebo (111 events/100 person years), when one participant serving as an outlier – contributing 43 severe adverse events to the semaglutide group – was excluded this patient, the analysis should show similar event rates for semaglutide (105 events/100 person years) and placebo groups (111 events/100 person years).
- The proportion of heart attacks and all-cause mortality events is lower in the semaglutide group. The analysis also showed that the proportion of MACE was numerically lower in the semaglutide group (10%), compared to placebo (17%). As well, the proportion of all-cause mortality was lower for semaglutide (14%) compared to placebo (19%).
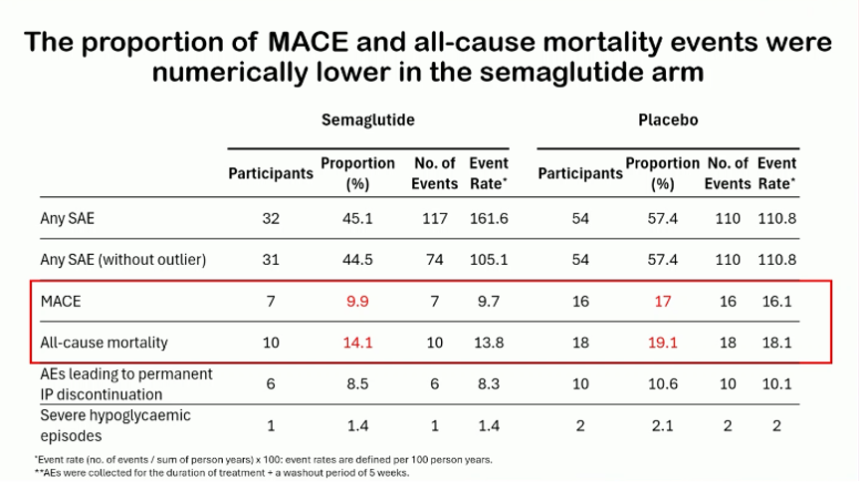
- Dr. Klein discussed strengths and limitations of the study. She explained that the results from the pooled analysis represent the largest prospective cohort of patients treated with GLP-1 RA and dialysis. The results highlight long-term outcomes, with over one year of follow-up after dialysis initiation. Furthermore, specific adverse events were systematically collected for comprehensive comparison across treatment groups. However, some of the limitations of the study include the lack of randomization in the population receiving dialysis, which may have biased the cohort with semaglutide treatment.
Fenofibrate lessens the progression of diabetic retinopathy and maculopathy in people with T2D
In this afternoon session, Dr. Vanessa Silva (Oxford University, UK) shared results from the LENS trial (n=1,151), which investigated the effect of lipid-lowering fenofibrate on the progression of diabetic retinopathy (DR). As background, fenofibrate is a peroxisome proliferator-activated receptor (PPAR) alpha agonist that regulates lipid metabolism by lowering triglycerides, reducing ApoB, and increasing HDL cholesterol. Nearly 80% of individuals with T2D have high cholesterol, and nearly a quarter of people with diabetes develop DR. Hence, investigators assessed whether fenofibrate – an oral medication typically used for high cholesterol and triglycerides – provides benefit for DR progression, particularly in the context of background statin use and varying eye disease severity. Importantly, evidence suggests that fenofibrate may also act directly within the eye.
- Trial design and baseline characteristics. Adults with non-referable (early stage) DR or maculopathy were recruited in Scotland using the Diabetic Eye Screening (DES) program. Participants were randomized to receive fenofibrate 145 mg tablets (n=576) or placebo (n=575). 74% of participants were concurrently treated with statin therapy, and 11% had moderate baseline retinopathy or maculopathy while the remainder had bilateral mild disease.. The LENS trial’s primary outcome was a composite of developing referable diabetic retinopathy or maculopathy – defined by the DES grading scheme – and treatment for retinopathy or maculopathy (intravitreal injection, laser, or vitrectomy).
- Results. After a median follow-up of four years, just under 23% of participants treated with fenofibrate met the primary endpoint (referable disease or treatment), compared to 29% participants who received placebo – reflecting a 27% risk reduction (p=0.006). The benefits of fenofibrate therapy were consistent regardless of the use of statin therapy (p-heterogeneity=0.66). The proportional benefit was also similar regardless of the severity of eye disease at baseline (p-heterogeneity=0.25). Therefore, participants with moderate disease, who are at higher risk of progression, derived greater benefit than those with mild disease in absolute terms.
Diabetic peripheral neuropathy is associated with an increased risk of stroke in individuals with T1D
In a morning session, Ms. Sara Itkonen (Folkhälsan Research Center, Finland) explored diabetic peripheral neuropathy (DPN) as an independent risk factor for stroke in people with T1D. T1D increases the risk of stroke by up to six times, lowers the median age of stroke incidence by 20 years, and is associated with worse prognosis. Moreover, the risk of stroke in T1D has previously been associated with diabetic kidney disease, proliferative diabetic retinopathy, hypertension, higher A1c, and smoking. This study sought to determine whether DPN is also associated a greater risk of stroke in people with T1D, independent of other diabetic vascular complications. Notably, DPN affects around 30% of all individuals with diabetes. Using the nationwide Finnish Diabetic Nephropathy Study (FinnDiane), researchers identified 3,005 patients with T1D, stroke status, and a minimum follow-up time of one year. Each participant also completed the FinnDiane Neuropathy Questionnaire (FDN-Q), which was converted into a Michigan Neuropathy Screening Instrument questionnaire (MNSI-Q) score, and were followed up for a median ten-year period. Stroke events were identified via national registries and confirmed from medical records through the end of 2020. MNSI-Q cutoffs for DPN diagnosis were set to ≥7 and ≥4, with higher scores indicating more symptoms of DPN. Stroke events, which occurred in 123 of 3,005 participants, were more common among older individuals, males, those with longer diabetes durations, and those with DPN diagnosis (≥ 4 MNSI-Q score). Notably, participants who suffered a stroke had a an almost two-fold increase in diabetes complications, including the history of kidney replacement therapy (p<0.001), cardiovascular disease (p<0.001), peripheral vascular disease (p<0.001), and proliferative retinopathy (p<0.001). Both MNSI-Q score ≥7 and ≥4 led to a two-to-three-fold increased risk for stroke. Furthermore, cumulative stroke incidence increased independently with DPN diagnosis (see figure below), with the MNSI-Q ≥7 and no history of a curve trending similarly with an MNSI-Q ≤ 7 with kidney replacement therapy.
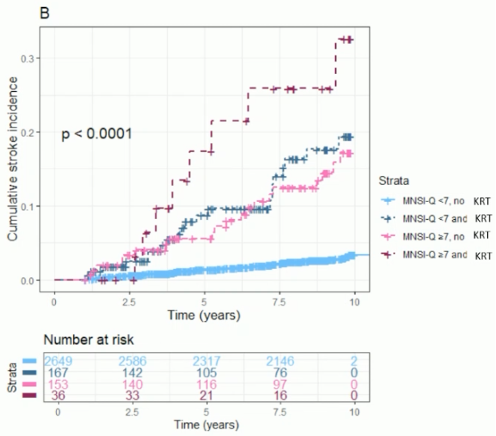
T2D Treatment and Remission
Lilly symposium highlights the evolving and crucial role of CVOTs in T2D management
In this packed lunchtime symposium sponsored by Lilly, Prof. Oliver Schnell (Ludwig Maximilian University, Munich, Germany), Prof. Melanie Davies (University of Leicester, UK), and Dr. Pam Taub (UCSD) discussed the revolutionary nature of CVOTs in T2D management. Prof. Schnell provided important epidemiological context, emphasizing that one-third of people with T2D have CVD, with heart disease responsible for up to 50% of diabetes related mortality. He argued that glucose-lowering agents should be evaluated not only on their efficacy with glycemic reduction but also on potential cardiovascular benefits.
- Prof. Davies reviewed the evolution of CVOTs, showcasing the numerous advancements that have expanded knowledge on the indirect effects of d therapies. Early studies like the UGDP and UKPDS 33 evaluated cardiovascular safety signals for sulfonylureas. In 2008, a new era of CVOTs began with the FDA’s guideline, which included expectations that all new T2D therapies demonstrate no increased risk for cardiovascular events. She spotlighted the EMPA-REG CVOT, published a decade ago, as a turning point, demonstrating that an SGLT-2 inhibitor empagliflozin not only did not increase risk, but reduced major adverse CV events. Subsequent trials like LEADER, REWIND, and more cemented GLP-1 RAs as a cardioprotective therapy, as well. Looking ahead, Prof. Davies, like many others, is anticipating results from the SURPASS CVOT, comparing cardiovascular benefits of dual GLP-1/GIP RA tirzepatide and GLP-1 RA dulaglutide, to be presented on Thursday at this meeting. She also expressed excitement about the use of in silico patient modeling to accelerate future CVOTs and therapy development.
- Dr. Taub dived into how next generation diabetes therapies leverage pleiotropic mechanisms to improve cardiovascular function and glycemic management simultaneously. She compared SGLT-2 inhibitors, GLP-1 RAs, and GIP/GLP-1 RA, with all three classes reducing inflammation, improving endothelial function, and positively influencing cardiac remodeling. Dr. Taub described the mechanisms by which GIP and GLP-1 may independently impact cardiovascular function, with: (i) GIP driving tissue-specific vasodilation and mediation of arthrosclerosis; and (ii) GLP-1 driving endothelial cell proliferation and improved cardiac function. When combined, the therapies provide synergistic cardiovascular benefits, reducing inflammation, inhibiting angiotensin II-induced cardiac hypertrophy and fibrosis, and enhancing left ventricular ejection fraction. She was also enthusiastic about other combination therapies, highlighting that pairing GLP-1 RAs with amylin or glucagon can increase overall metabolic benefit. She ultimately urged cardiologists and endocrinologists to collaborate to best serve their patients with T2D, choosing agents for both glucose-lowering and proven cardiac protection.
Phase 3 study finds A1c reduction and potential cardiorenal protection with berberine ursodeoxycholate
In an overcrowded session, Dr. Linong Ji (Peking University) presented results of a phase 3 Symphony 2 trial (n=549) evaluating berberine ursodeoxycholate (HTD1801) in people with T2D. HTD1801 is a first-in-class anti-inflammatory metabolic modulator that activates AMP-activated protein kinase (AMPK; regulates cellular energy homeostasis) and inhibits the NLRP3 inflammasome. Designed to improve insulin resistance, glucose metabolism, and reduce liver fat and inflammation, this investigational drug is studied for metabolic diseases like T2D and metabolic dysfunction-association steatohepatitis (MASH). Previously, the Symphony 1 trial demonstrated significant A1c reduction (1.3 percentage points) with HTD1801 versus diet and exercise alone. The Symphony 2 trial aimed to evaluate the efficacy and safety of HTD1801 compared to placebo in people with T2D inadequately managed with metformin.
As background, berberine is used in traditional Chinese medicine and taken as a supplement to lower A1c and weight. However, as session chairs Dr. Athena Philis-Tsimikas (Scripps Whittier Diabetes Institute) and Dr. Aaron Novikoff (Helmholtz Zentrum Munich, Germany) mentioned, few robust trials have investigated the efficacy and safety of berberine until now.
- Trial design and baseline characteristics. Conducted across 64 sites in China, the study randomized participants with A1c between 7.0-10.5% with stable metformin use to HTD1801 1000 mg twice a day (n=365) or placebo (n=184). The primary endpoint was change in A1c from baseline to Week 24, while secondary endpoints included change in fasting glucose, lipid levels, and inflammation markers. At baseline, participants were 56 years old, with 47% being female. Clinically, participants had average weight of 70 kg (154 lbs), six years of diabetes duration, and A1c of 8.5% despite metformin use.
- Results. The trial met its primary endpoint, with HTD1801 conferring A1c reduction of 1.21 percentage points (vs. 0.68 percentage points with placebo; p<0.0001) at Week 24. Moreover, 33% of participants (vs. 11% in placebo group; p<0.0001) achieved A1c <7.0% at Week 24. HTD1801 also improved postprandial glucose and insulin levels, reduced LDL-cholesterol (0.35 mmol/L vs. increase of 0.01 mmol/L with placebo; p<0.0001), and lowered inflammation marker hs-CRP (p<0.01). Interestingly, Dr. Ji suggested that HTD1801 may offer renal protective benefits, as eGFR remained stable in the overall population and increased in patients with mild renal impairment (see figure below).
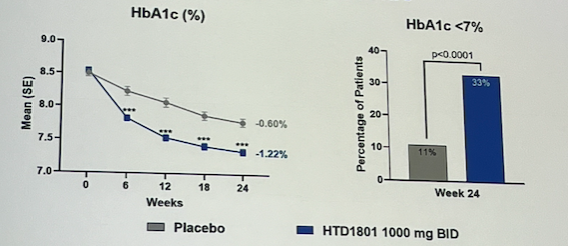
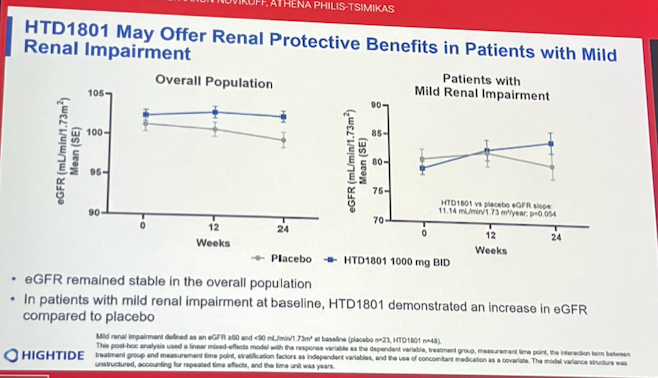
- Safety. Adverse events occurred in 75% of HTD1801 treatment group (vs. 68% in placebo group), while serious adverse events occurred in 4% (vs. 6%). Most common adverse events were diarrhea (23% vs. 1%). Low-grade hypoglycemia occurred in four participants receiving HTD1801 (vs. one in placebo).
Dr. Steven Kahn and Prof. Roy Taylor on new-age incretin therapies as a path to T2D remission
In a packed afternoon spotlight session, Dr. Steven Kahn (University of Washington) and Prof. Roy Taylor (Newcastle University, UK) highlighted the T2D remission capabilities of GLP-1 RAs. The session underscored how next-generation GLP-1 RAs and dual agonists like tirzepatide are reshaping the T2D remission landscape, with data from GRADE, SELECT, and SURMOUNT-1 showing dramatic reductions in diabetes progression and improvements in glycemia. Prof. Taylor complemented this with insights from the DiRECT trial, demonstrating that remission through weight loss can lead to near-complete recovery of pancreatic volume. Presenters framed remission as an achievable goal for people living with T2D.
- Dr. Kahn offered an overview of how GLP-1 RAs and dual agonists have evolved from primarily glucose-lowering agents into powerful tools for diabetes remission, backed by landmark trials.
- In the GRADE trial, individuals with existing T2D (n=4,801) treated with insulin glargine, glimepiride, liraglutide, or sitagliptin achieved A1c lowering from a baseline of 7.5% to below 7.0%. However, A1c levels did increase after five years. Dr. Kahn highlighted that liraglutide was the best of the four therapies for sustained A1c lowering.
- In the SELECT trial (n=17,604), individuals with preexisting cardiovascular disease, overweight, or obesity, and without diabetes treated with semaglutide experienced slowed diabetes progression, with 70% of participants on semaglutide achieving normoglycemia versus just 36% taking placebo after three years. He highlighted that the preventive impact was strongest in individuals with higher baseline A1c values (≥6.0%).
- In the SURMOUNT-1 trial (n=2,539), Dr. Kahn demonstrated similar effects for tirzepatide, where diabetes progression was reduced by 94% in adults with prediabetes and overweight or obesity. After treatment discontinuation at Week 72, participants experienced a mean weight regain of 7%, and 16% reverted from normoglycemia to prediabetes. 1.2% developed diabetes. Dr. Kahn emphasized need for lifelong use of these therapies to preserve metabolic gains.
- Prof. Taylor then turned to a discussion on defining reversal, remission, and cures for T2D, ultimately advocating against the use of the term “cure.” He provided an overview of the 2021 consensus definitions, where reversal and remission are each contingent on the cessation of therapy. He proposed an amendment to this definition to exclude appetite suppressants based on the transformative effects of weight loss on A1c lowering and more.
- Prof. Taylor reminded attendees of a post-hoc analysis of the DiRECT trial which showed that people with T2D who achieve remission through weight loss can experience a gradual recovery of beta cell function and pancreatic volume that approach normal levels over two years. Dr. Taylor emphasized the idea that beta cells in people with T2D are metabolically suppressed rather than irreversibly damaged and can be reactivated with sustained lifestyle or therapeutic intervention.
- Importantly, the intervention group experienced fewer serious adverse events than controls, reinforcing the long-term safety and public health benefits of structured weight loss programs. We look forward to hearing results of the NHS T2D Path to Remission Program next year.
GIP infusion alone or in addition to semaglutide shows no improvement in glucose levels or body weight in T2D
In a morning oral session, Dr. Mads Helsted (University of Copenhagen, Denmark) presented interventional studyfindings (n=61) on the efficacy of GIP infusion alone versus combination therapy with semaglutide in people with T2D. Clinical treatments, like Lilly’s tirzepatide (dual GLP-1/GIP RA), have demonstrated promising metabolic benefits of GIP agonism, especially when added to GLP-1 RAs. Hence, investigators hypothesized that adding GIP to semaglutide would enhance glycemic management. Surprisingly, study results showed that GIP infusion didn’t affect glucose levels or body weight in people with T2D.
- Methods. This trial involved 61 participants with T2D who had a mean age of 63.9 years, BMI of 31.6 kg/m2, and a median A1c of 7.1%. Participants were first randomized 1:1 to eight weeks of once weekly semaglutide (0.25 mg during the first four weeks and then 0.5 mg) or placebo. They were then randomized 1:1 to receive a six-week continuous infusion of GIP or placebo via an infusion pump as an add-on to 0.5 mg semaglutide once-weekly or placebo. The primary endpoint was the change in mean glucose levels from baseline to the end of treatment, measured by CGM metrics.
- Results. As expected, CGM metrics showed a significant difference between groups that received semaglutide compared to those that receive placebo. However, when GIP was added, results did not show further differences between the two groups. Within baseline placebo groups, the difference in glucose change was 0.80 mmol/L between groups with placebo and GIP as added treatment (p=0.90). Within baseline semaglutide groups, the difference in glucose change was 0.05 mmol/L between groups with placebo and GIP as added treatment (p=0.90). GIP infusion also showed no differences in mean body weight change and diastolic blood pressure. Additionally, GIP did not change oral glucose tolerance outcomes nor did C-peptide levels that indicate insulin secretion.
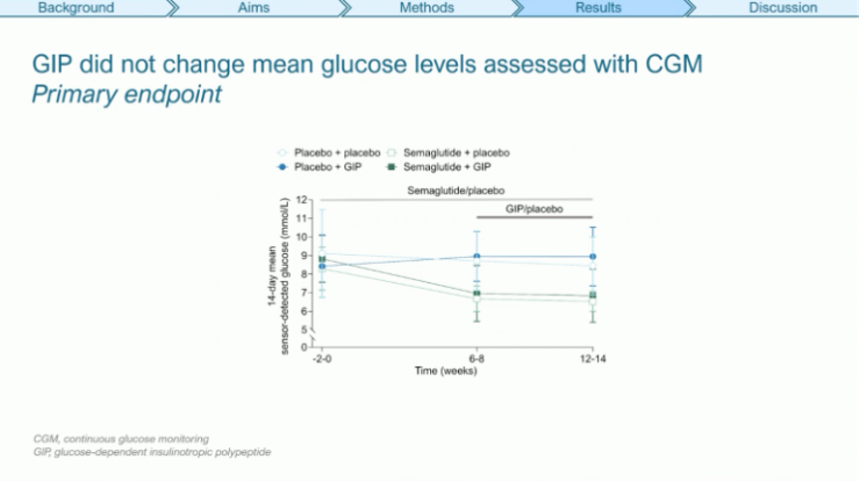
- Discussion. During Q&A, Dr. Helsted addressed questions on why results from this study differ from that of other trials of tirzepatide, a dual GIP/GLP-1 RA. He noted limiting factors of the trial, including the small population size. Additionally, he suggested that while the GIP dose used in the trial was the highest possible dose due to difficulties with administration in an insulin pump, it may not have been high enough to see similar effects as tirzepatide.
Obesity
Post-hoc analysis of phase 3 REDEFINE-1 trial: Long-acting amylin analog cagrilintide confers greater weight loss (12%) than placebo (2.3%)
A poster by Dr. Timothy Garvey (University of Alabama at Birmingham) presented a post-hoc analysis of the phase 3 REDEFINE-1 trial (n=3,417), demonstrating that once-weekly long-acting amylin analog cagrilintide 2.4 mg was both safe and effective in treating adults with obesity or weight-related comorbidities. Results were simultaneously announced in Novo Nordisk’s press release. As a reminder, full results of the REDEFINE-1 trial were presented at ADA 2025, demonstrating that CagriSema (a fixed combination of cagrilintide 2.4 mg and semaglutide 2.4 mg) conferred 20% weight loss, compared to 15% with semaglutide alone, 12% with cagrilintide alone, and 3% with placebo. This post-hoc analysis marks the first phase 3 trial data for cagrilintide monotherapy for obesity. Dr. Garvey highlighted that cagrilintide may serve as an alternative for those who do not tolerate incretin-based therapies. Novo Nordisk will advance cagrilintide into the dedicated phase 3 RENEW program, expected to begin in 4Q25.
- Study design and baseline characteristics. The post-hoc analysis included 302 participants with obesity who received cagrilintide, with a mean age of 47 years, BMI of 38 kg/m², and body weight of 107 kg (236 lbs). Of the participants who received cagrilintide, 66% were female and 71% were white. To be eligible, participants were required to have a BMI ≥30 kg/m² or ≥27 kg/m² with at least one weight-related comorbidity. Individuals with diabetes were excluded.
- Results. Participants receiving cagrilintide achieved average weight loss of 11.8% (12.5 kg or 28 lbs), compared to 2.3% (2.5 kg or 5.5 lbs) with placebo at Week 68. Notably, 31.6% of participants reached ≥15% weight loss versus 4.7% in the placebo group. Cagrilintide also reduced mean waist circumference by 10.6 cm versus 4 cm with placebo. Most common adverse events were mild-to-moderate and gastrointestinal (GI) events, which were more frequent in the cagrilintide group (54%) than the placebo group (40%). GI events included nausea (24% vs. 13%), vomiting (21% vs. 12%), diarrhea (15% vs. 12%), and constipation (7% vs. 4%). By discontinuation rates, only 1% of participants discontinued due to nausea, compared with 0.1% in placebo and 6% with CagriSema, suggesting improved tolerability.
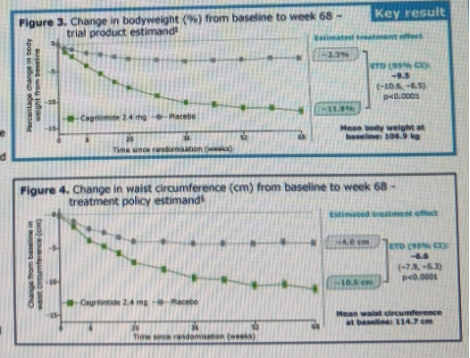
Oral quadruple agonist NA-831 for obesity: Topline phase 2 results suggest weight loss without muscle loss and GI-related side effects
Dr. Lloyd Tran (Biomed Industries) presented phase 2 results for NA-931, an oral, once-daily quadruple agonist for obesity. NA-931 is a GLP-1, GIP, glucagon, and IGF-1 receptor agonist and shows biased signaling at the GIP and IGF-1 receptors. In its phase 1 study, NA-931 conferred weight loss of up to 6.8% at 28 days from a baseline of 99.3 kg (219 lbs) in people with obesity, with or without T2D. Notably, there were virtually no GI-related adverse events. Two out of 54 participants experienced mild nausea, and one experienced diarrhea. In the placebo group, two out of 20 experienced mild nausea, one experienced vomiting, and one experienced diarrhea. Dr. Tran said that the side effects were likely mitigated by the IGF-1 RA component of NA-931. As background, IGF-1, or insulin-like growth factor-1, has been shown to have positive effects on the gastrointestinal system.
- Study design. Participants in this multicenter, randomized, double-blind 13-week study had obesity or overweight with at least one weight-related comorbidity. They were randomized into one of four NA-931 treatment cohorts (60 mg, 90 mg, 120 mg, or 150 mg) or placebo.
- Baseline characteristics. There were a total of 125 participants, with 24 in each treatment cohort and 29 in placebo. Mean age across the four cohorts and placebo group ranged from 42.7 to 46.7 years old, and around two-thirds of participants were female. Mean weight ranged from 96.2 to 100 kg (212 to 220 lbs), and mean A1c ranged from 4.9 to 5.4%.
- Results. At 13 weeks, 150 mg NA-931 conferred 13.8% weight loss (13.8 kg from a baseline of 99.8 kg). In comparison, the placebo group showed a 1.9% weight loss (2.3 kg from a baseline of 96.2 kg). Dr. Tran noted that this study showed preliminary results that NA-931 does not cause muscle mass loss.
- Safety. Across all NA-931 groups, seven participants (7.3%) experienced mild nausea, compared to three participants in the placebo group (10.3%). No participants experienced moderate or severe nausea. Vomiting, diarrhea, and constipation were reported in five, six, and two participants in the treatment groups (5.2%, 6.3%, and 2.1%), respectively, compared to two, two, and zero participants in placebo (6.9%, 6.9%, 0%).
Oral GLP‑1 RGT‑075 demonstrates clinically meaningful weight loss and blood pressure reduction in people with obesity
In this afternoon oral presentation, Dr. Julio Rosenstock (Velocity Clinical Research) presented results from Regor Pharmaceutical’s phase 2a proof-of-concept RCT on a once-daily, oral small molecule GLP-1 RA, RGT-075. RGT-075 conferred robust short-term weight loss and clinically meaningful reductions in blood pressure (BP) in people with obesity without T2D. The safety profile aligns with the GLP-1 RA class, with predictable GI tolerability that appears manageable with titration. RGT-075 merits further clinical development given its oral formulation and potential cardiometabolic benefits shown in this trial. In terms of the study design and baseline characteristics, this phase 2a study (n=73) assessed 125 mg dose of once-daily RGT-075 over 12 weeks. Participants included adults with obesity (BMI ≥ 30 kg/m²) or overweight (BMI ≥ 27 kg/m²) and at least one obesity-related comorbidity. People with T2D (A1c≥6.5%) were excluded from the trial. At baseline, the median age of participants was 50 years, with a mean weight of 104 kg (229 lbs), mean BMI of nearly 37 kg/m², and an average baseline A1c of 5.6-5.7%. Ultimately, RGT-075 was associated with a 5.4% mean reduction in body weight with RGT-075 compared to 0.5% with placebo, with no plateau by Week 12. Although RGT-075 conferred only a negligible placebo‑adjusted A1c reduction of 0.21 (p=0.054) compared to placebo, the baseline was so low (normal!) that this was unsurprising (we were actually surprised to see it this high, though accuracy constraints prevent final assessments). The most impressive part of the results were findings on blood pressure - systolic blood pressure dropped by 12 mmHg on RGT-075, versus 3 mmHg on placebo, while RGT-075 prompted a placebo‑adjusted diastolic blood pressure reduction of 5.5 mmHg. This was an impressive result, even with a side effect profile in which nausea of nearly 40% was experienced by those on RGT-075, compared to 4% on placebo.
Once‑weekly amylin agonist eloralintide conferred up to 11% weight loss at Week 12 in people with obesity
In this afternoon symposium, Dr. Edward Pratt (Eli Lilly), presented a phase 1 proof-of-concept study (n=6) for eloralintide, a long-acting amylin RA in people with obesity. The single‑center, 12‑week, multi‑ascending‑dose phase 1 study evaluated safety, tolerability, pharmacokinetics, and preliminary efficacy across multiple dose cohorts. Eloralintide conferred dose‑dependent, clinically meaningful weight loss at 12 weeks. Safety profile was favorable, with most events being mild (rather than mild to moderate!) and GI-related. This phase 1 study (n=36) evaluated safety and tolerability of once-weekly subcutaneous eloralintide. The trial included adults with a BMI of 27-40 kg/m² who had stable weight for 3 months (<5% body weight change). Exclusion criteria included: (i) people with diabetes (A1c ≥6.5%); (ii) people with a prior or planned surgical treatment for obesity; (iii) people who were on weight-loss promoting therapies within three months of screening were excluded; and (iv) eGFR <30.0 mL/min/1.73 m². At Week 12, eloralintide demonstrated clinically meaningful and dose‑dependent weight loss. Mean percent reduction from baseline was 8.9% for 3 mg, 8.5% for 6 mg, and 11.3% for 12 mg. No meaningful weight loss was demonstrated in the placebo group. Overall incidence of treatment‑emergent adverse events (TEAEs) was similar across groups, with 63%, 67%, 79%, and 60% of the 1.2 mg, 3 mg, 6 mg, and 12 mg cohorts reporting at least one TEAE, respectively, compared to 56% in the placebo group. Treatment‑related AEs were higher in the treatment group, affecting 13%, 17%, 44%, and 44%, in the 1.2 mg, 3 mg, 6 mg, and 12 mg cohorts, respectively, compared to 7.4% in the placebo arm. Serious AEs occurred in 2% of all participants. AEs leading to discontinuation were uncommon. Most AEs were mild, gastrointestinal events, with a decline in appetite most common.
Award Lectures + Additional Topics
57th Claude Bernard Lecture by the esteemed Professor Andrew Hattersley focuses on “precision diabetes”: Learning from the rare and applying to the common
Prof. Andrew Hattersley (University of Exeter, UK), was awarded the Claude Benard Lecture prize in recognition of his innovative leadership and lifetime achievements in diabetes research. This year’s award at EASD was handsomely underwritten by Sanofi, and the presentation began with a wonderful video of Prof. Hattersley at his lab in Exeter, reminiscing about his work there that began thirty years ago, starting in 1995! Prof. Hattersley received an extremely warm round of applause, to which he said, “Having been in the audience at EASD for 34 years and having watched my heroes give this lecture, it feels like a dream to be here on stage …” (and, he allowed, “also absolutely terrifying”). Prof. Hattersley’s lecture focused on the development of “precision diabetes” – methods of identifying diabetes subtypes that result in practical treatment differences and differentiated outcomes. He discussed neonatal diabetes – monogenic diabetes diagnosed within the first six months of life, MODY (Maturity-Onset Diabetes of the Young), non-autoimmune insulin deficient diabetes seen in African populations, adults who were diagnosed with T2D and later found to have T1D, and even the promising future of precision therapeutics. For many years now, we’ve regarded Dr. Hattersley as a major diabetes hero – and attended literaly dozens of his presentations that we have documented in our Close Concerns KnowledgeBase – so seeing this prize awarded felt incredibly exciting to us, as well as very inspirational.
- “Precision diabetes” was first explored with respect to neonatal diabetes - monogenic diabetes diagnosed within the first six months of life. Neonatal diabetes is about 2-3% of all pediatric diabetes. It was discovered that 50% of neonatal diabetes results from potassium channel mutations and can be treated very successfully with a high dose sulfonylurea. 90% of these patients eventually stop taking insulin and even discontinue blood glucose monitoring. After pioneering work by Prof. Hattersley’s team, today there are 453 known sub-types of neonatal diabetes that can be identified by genetic sequencing, resulting in the selection of the most appropriate treatment in each case. The University of Exeter offers free testing globally, having tested 3,569 patients from 114 countries to date.
- In a similar vein, testing for MODY can reveal genetic sub-types with the appropriate treatment options, and this approach has become the standard of care. MODY is commonly misdiagnosed – as 97-99% of people with a diabetes diagnosis do not have monogenic diabetes, it remains difficult to rationalize universal testing for MODY. Some presentations are well-known, such as diabetes with a renal development disease or neural deafness. For other cases, Prof. Hattersley has developed standards. For example, “T1D” patients that are three-antibody-negative have a 12% chance of having MODY. This rises to 33% if they have an A1c <7.5% or a parent with diabetes. There is also a MODY calculator for people with a T2D diagnosis – the probability of MODY rises with younger age at diagnosis and lower BMI.
- Certain subtypes of T1D are rarer and do not have differentiated treatment options. Prof. Hattersley explained that certain pancreatic endotypes have different C-peptide levels. There is also non-autoimmune insulin deficient diabetes that presents very similarly to “regular” T1D in slim young people. Prof. Hattersley discussed “YODA” – a trial of Young-Onset Diabetes in sub-Saharan African children who had T1D, where, strikingly, 65% of the participants had no islet autoantibodies. The investigators ruled out T2D, monogenic diabetes, ketosis, and malnutrition and also noted that this subtype was present in 16% of Black people with T1D in the USA.
- Getting the correct diagnosis is key – adults are often diagnosed with T2D, but in fact have T1D. For example, former UK Prime Minister Theresa May was diagnosed at 56. It may be difficult to correct this problem since T1D is such a rarity in older age groups, despite the fact that 50% of people with T1D develop it as adults. Studies show that within three years, almost everyone in this class is being treated correctly with insulin, although the diagnosis may still be incorrect.
- On the other hand, there are people diagnosed as “adult T1D” that actually have T2D. An antibody test can help clarify, and will distinguish patients that may have T2D or MODY. This is why Prof. Hattersley commented: “If you think it’s T1D, do the antibodies.” He also recommended that all longstanding “T1D” adults and insulin-treated people with “T2D” deserve a C-peptide test – just to make sure the diagnosis is correct and insulin is required.
- Finally, Prof. Hattersley turned to T2D – arguably the most challenging since it is well-known to be polygenic. There are diverse presentations and treatment regimens present in T2D – but Prof. Hattersley continues to wonder if they are optimal. Years of work developing subtypes based on genetic and clinical factors were not successful in predicting treatment outcomes, but this year, Dr. John Dennis (University of Exeter, UK) developed a five drug model drawing upon his actuarial background (recently expanded to include semaglutide) that takes routine data such as age at diagnosis, sex, BMI, duration of diabetes, baseline A1c, eGFR, HDL and ALT and predicts the response of five treatments (DPP-4 inhibitors, SGLT-2 inhibitors, sulfonylureas, TZDs, and GLP-1 RAs) ‑ see chart below. The model has been tested with data from clinical trials and delivers a ~0.5% mean improvement in A1c compared to non-optimal glucose lowering, equivalent to a 2.5-year delay in treatment intensification. The model also delivered a reduction in five-year complications.
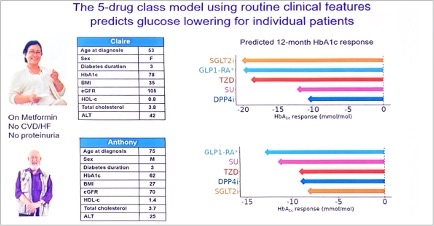
- The model had some surprising findings – for example, it predicts that GLP-1 RAs lower A1c the most compared to other therapies for 70% of females, but only 10% of males. How fascinating! GLP-1 RAs also tend to be less effective for those with higher BMI or lower age at diagnosis. What’s next, in terms of creating impact from these findings? As we understand it from Professor Hattersley, the next steps are to validate a software decision aid to be used in clinical practice. A test version can be found here. For the first time, this is practical precision diabetes for T2D. As we have seen for some years now, and reinforced mightily in Professor Hattersley’s lecture, it sure seems like “precision diabetes” has a promising future.
Prof. Mikael Rydén receives the Camillo Golgi Prize for expanding knowledge of white adipose tissue and its role in diabetes
Prof. Mikael Rydén (Karolinska Institute, Sweden) received the Camillo Golgi Prize for his staggering contributions to understanding of adipose tissue and how it relates to diabetes, delivering an engaging lecture to a full room. The Camillo Golgi Prize recognizes outstanding contributions in the field of histopathology, pathogenesis, prevention, and treatment of the complications and comorbidities of diabetes mellitus. Prof. Rydén’s “love of fat” was inspired by two of his mentors, Profs. Jan Bolinder and Peter Arner, inspiring an illustrious career. With no hesitation and high enthusiasm, he began his award lecture focusing on the role of white adipose tissue (WAT) in diabetes and other cardiometabolic complications. WAT is very plastic – more than almost any other organ – and can grow very large or also shrink, said Prof. Rydén. Healthy adipose tissue growth has stable lipid turnover, inflammation, insulin resistance, and fibrosis, while in pathological fat growth low lipid turnover, increased adipocyte hypertrophy, inflammation, fibrosis, and hypoxia are observed (see figure below).
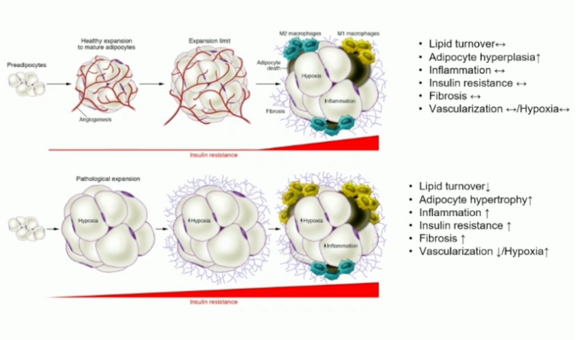
- Obesity is strongly linked to the development of T2D and develops through two major lipid growth pathways. The primarily relevant fat depots in the body are subcutaneous abdominal adipose tissue and visceral omental abdominal fat. Excess fat is of course vilified as unhealthy in popular understanding, but many people with obesity have healthy biomarkers as well, which raises the question of whether healthy forms of obesity exist. Prof. Rydén acknowledged the wide range of biomarkers possible with obesity yet also noted that meta-analyses of longitudinal studies of people with healthy obesity demonstrated a fourfold higher incidence of T2D compared to normal weight individuals. Therefore, the implications of weight gain and obesity motivate analysis into their origins and potential prevention. Prof. Rydén said that excess metabolic energy is stored as lipids in adipocytes which have a large capacity to expand. When storage capacity is attenuated, such as by insulin resistance, this leads to ectopic lipid deposition. The two major causes of this relatively facile growth are changes to lipid turnover and changes to adipocyte size and number.
- Changes to lipid turnover rate lead to obesity with systemic metabolic effects. Prof. Rydén explained that lipid turnover in human adipocytes is regulated by hormones – circulating insulin stimulates lipogenesis, leading to the production and storage of fat in the body. Through the use of carbon-14 dating, Prof. Rydén and colleagues determined that the average age of lipids stored in the body is approximately 1.2 years. In people who are overweight, lipolysis is reduced while lipogenesis is maintained, leading to a stagnation of lipid storage and an average stored lipid age of 1.5 years. In obesity, a massive increase in lipid storage leads to an average stored age of 1.8 years in the body. Altered lipid turnover rates have previously been shown to explain variations in circulating cholesterol and triglycerides. With a balance of lipid uptake and removal, people generally remain lean, said Prof. Rydén. However, with a disruption to the balance between these two states, the growth of WAT and weight gain develop. It is likely that this physiology developed as an evolutionary advantage in the human past when periods of starvation were much more common – fat storage could be life-saving in these cases. The increase in weight gain, overweight, and obesity thus represents a uniquely modern problem with severe consequences all the same.
- Changes to adipocyte size and number have long-lasting consequences. Prof. Rydén said that there are two major forms of adipose tissue regardless of body type: hypertrophy and hyperplasia. Hypertrophic cells are large and are associated with risk of T2D and a strong hereditary basis for T2D. However, hyperplastic cells are much smaller in size but greater in number, which has protective effects against metabolic conditions. Keeping these baseline cell types in mind, it has also been demonstrated that numbers of fat cells are maintained over long periods of time – studies have demonstrated that people who had obesity beginning in childhood may have twice the number of fat cells as those who were lean even after reaching adulthood. Carbon-14 dating has also demonstrated that adipocytes are constantly produced in adult humans with an average life span of 10 years, however, fat cell number is constant after weight loss. Through years of study, Prof. Rydén has concluded that fat cell number can increase but not decrease. Once they have been formed, a new set-point is created. This “memory” found in WAT has also been associated with hypoleptinemia after weight loss, which Prof. Rydén characterized as small and "hungry" fat cells that possibly facilitate future weight regain.
- In all, Prof. Rydén, a self-proclaimed “fat nerd,” summarized his work with a few striking points. He has demonstrated support for the idea of an “obesity memory,” where obesity induces irreversible changes in WAT gene expression, cytoarchitecture, and function which may contribute to increased risk of weight gain after weight loss. There are also large interindividual variations in the proportions of insulin-responding adipocytes and weight loss – causal links are currently being assessed in model systems as well as prospective clinical studies. Alongside his passion for the study of fat, Prof. Rydén is almost equally as passionate about easily accessible data. He closed by calling for all researchers in the room to make their data available and searchable to promote scientific advancement worldwide.
19th Albert Renold Lecture: Prof. Raphael Scharfmann on pancreatic development as a key to discover unexpected treatments of diabetes
To open the third day of the conference, Prof. Raphael Scharfmann (Cochin Institute, France) received the 19th annual Albert Renold Prize, awarded each year in honor of Prof. Albert Renold, a pioneer in the diabetes abnormalities research. Prof. Scharfmann was recognized for his groundbreaking contributions, including his lab’s 2014 success in generating functional human pancreatic beta cells. In his lecture, Prof. Scharfmann reflected on his scientific journey beginning in 1999 with the Minkowski prize and his guiding philosophy to “do differently from others.”
- Prof. Scharfmann detailed his early work culturing fetal rodent pancreatic explants, which demonstrated that endocrine cells differentiate through a default pathway. While many labs in the 2000s focused on pancreas development in mice, his team pivoted to human models, creating dynamic platforms like in vitro organoid-like systems and in vivo transplantation into severe combined immunodeficient (SCID) mice. These models enabled a deep descriptive analysis of human embryonic pancreatic development and revealed that insulin-producing (INS⁺) cells appear earlier than previously believed (around the fifth week post-conception). His lab also showed that endocrine cells, including glucagon (GCG⁺) and somatostatin (SST⁺) producers, emerge simultaneously with INS⁺ cells and align centrally within the pancreas, suggesting islet formation through clustering.
- As his group transitioned to the development of translational models, Prof. Scharfmann described the creation of the EndoC-β series of human beta cell lines via gene transfer into pancreatic progenitors. He highlighted the transcription factor MNX1 – mutated in neonatal diabetes – as a critical regulator of beta cell identity. Prof. Scharfmann described the comparison of functional metrics between primary human beta cells and EndoC-βH1 cells to illustrate both the utility and limitations of these models in diabetes research.
- Prof. Scharfmann closed by asking “What’s next?” He outlined future goals focused on refining human beta cell models for imaging, targeting, and protection, while expanding focus beyond beta cells to include alpha and delta cells. To young scientists, he advised to “sail between islands,” embrace scientific freedom, and dare to do things differently, reminding them that such boldness may one day be rewarded with the Albert Renold Award.
60th Minkowski Lecture: Dr. Teresa Mezza on prioritizing the pancreas in T2D
Dr. Teresa Mezza (Università Cattolica e Fondazione Gemelli, Italy) was awarded the Minkowski Prize for her outstanding research as an early career scientist. She has significantly contributed to the advancement of the understanding of diabetes and was recognized for her application of human experimental models. These models have provided crucial insight into the roles of insulin resistance and islet adaptation in shaping disease progression and therapeutic responses. During the 60th annual Minkowski lecture, Dr. Mezza presented a series of studies that she has conducted throughout her career, collectively reframing our understanding of beta-cell dysfunction and recentering the pancreas in T2D research.
- Dr. Mezza showed that in individuals without diabetes, insulin resistance drives compensatory increases in beta-cell mass and changes in islet morphology long before hyperglycemia appears. Her work using hyperglycemic and arginine-stimulated clamps revealed that insulin secretion increases in insulin-resistant individuals. This response is not sustained, pointing to early functional defects.
- She also highlighted evidence of ductal transdifferentiation (the conversion of one cell type to another), where insulin-positive cells emerge within pancreatic ducts. This is more prominent in insulin-resistant subjects, suggesting that the pancreas attempts to regenerate beta-cell mass under metabolic stress. She further highlighted her perspective study on beta-cell plasticity, which synthesizes evidence for islet transdifferentiation and dedifferentiation in humans. Early functional adaptation and eventual maladaptation underlies the transition from insulin resistance to diabetes. In parallel, her work has demonstrated that intra-islet GLP-1 production rises in insulin resistance, correlating with changes in glucose sensitivity and beta-cell function.
- Dr. Mezza emphasized that beta-cell dysfunction, rather than mass loss, is the earliest and most predictive marker of diabetes onset. Using longitudinal data from pancreatectomy patients, she showed that individuals with impaired glucose sensitivity before surgery were more likely to develop diabetes postoperatively regardless of the extent of beta-cell mass reduction. Together, these studies deliver a single message: the earliest defects in T2D lie in beta-cell quality rather than quantity. To change the future of diabetes, we must re-center the pancreas and act before hyperglycemia predominates, said Dr. Mezza in a call to action.
EASD Diabetes Global Impact Prize Lecture
The EASD Diabetes Global Impact Prize was today awarded to Dr. Viswanathan Mohan or “Mohan” for his “outstanding contribution to diabetes research and prevention, and his transformation of medical practice, not only in India but worldwide.” It is awarded to individuals who have made contributions to clinical or translational work on a global scale, impacting the lives of people with diabetes in resource constrained settings. There could hardly be a more fitting first recipient than Dr. Mohan, who was specifically cited for his efforts to “gain more knowledge on the etiology of diabetes that occur in populations worldwide.” The prize is supported by Lilly.
It was a great privilege to attend the award lecture by Dr. Mohan, who is a visionary and entrepreneur who has helped thousands of clinicians and millions of people with diabetes, starting in his home country of India. Dr. Mohan has published over 1,700 papers and has nearly 250,000 citations – one of the most cited diabetes researchers ever. He also has well over a million followers on social media. And, he will always slow down to be in touch with those who want to understand diabetes btter.
At Close Concerns, we’ve had the privilege of visiting Dr. Mohan in India multiple times over the last 20 years and have been incredibly impressed by how his team of health workers has achieved A1cs similar to the United States at scale in remote rural villages that possess minimal resources. While Time in Range is not measured for poor patients, we suspect they are doing far better than many people in the US, one of the highest-resourced countries.
Standing ovation! Dr. Mohan spoke for nearly an hour and only had time to begin to touch on some the highlights of his life’s work. At the conclusion of his lecture, there was not a single person seated in the large Paris Halle that we could see.
- Dr. Mohan started by describing how, as a young man, he followed in his father’s footsteps as a doctor, beginning to research diabetes in the garage of his father’s practice, while still a medical student. Between 1971 and 1991, he helped his father build the first diabetes hospital and diabetes research center in India.
- In 1991, with his late wife, Dr. Rema Mohan, he established a specialist diabetes hospital, ‘Dr. Mohan’s Diabetes Specialities Centre” (DMDSC) which was the foundation of his enormous impact and legacy. Today, DMDSC has 50 branches in 32 cities, a staff of >1,400 with over 130 diabetes doctors and serves 700,000 registered people with diabetes. The concept is ‘total diabetes care’ – every test or treatment that might be needed is available in the building and all check-ups can be completed within six hours.

Today, his current group of diabetes institutions can be described into four key parts – clinical care, research, education and training and charity. Each have had tremendous impact in India (and abroad), and he described them all during the course of this inspirational lecture, which we recommend reviewing in full.
Here are some of the (many) highlights:
- Digital Diabetes Delivery: Dr. Mohan’s team have created three applications: (i) “DIA”, an AI chatbot to help patients with diabetes questions; (ii) “DiaLA”, a super-useful mobile app to help with appointments, health tracking, prescriptions, medical records, CGM data; and (iii) “DiaNA”, a precision medicine tool to predict risk, classify T2D subgroups and recommend treatments.
- Epidemiology: Starting in Chennai with a urban population study (CUPS, n=1,399), Dr. Mohan and his team expanded to an urban/rural study (n=26,000) and then to a pan-India study (n=121,081), which was painstakingly sampled to be totally representative of the country. These incredible studies screened for diabetes, developed risk scores, published the first data on prevalence of complications, obtained data on metabolic markers, profiled diet and physical activity, and developed numerous interventions and recommendations. One important insight was the development of the “South Asian Phenotype,” which describes a person with propensity to develop T2D at a much younger age and lower BMI than White Europeans. Although genetic differences are important, a high carb diet (>65% of calories) was associated with risk. Dr. Mohan stated “[A high carb intake] is why we have a diabetes epidemic in India.”
- Education: Dr. Mohan’s Diabetes Education Academy has trained over 500 doctors in diabetes, that have collectively treated over 1.5 million people with diabetes. To scale faster, he created a distance learning program that has now trained over 19,000 doctors, who have benefitted 18.8 million people with diabetes. The program is now being offered free to neighboring countries. There is a similar program for diabetes educators, with nearly 29,000 trained to date.
- Rural Practices: 65% of India’s population lives in poor rural areas, whereas 74% of doctors practice in urban areas. In addition to poverty, rural areas have low literacy rates, low awareness of diabetes, and problems with access. Starting in one village, Chunampet, in 2006, Dr. Mohan created a model for rural care. He trained local villagers as health workers who could screen the entire population. Those with diabetes were treated in a mobile ‘telediabetology’ van (with a huge satellite dish bolted to the roof!). In three years, they screened 23,380 people, treated 1,138 people with diabetes, and achieved good control with low-cost drugs. This served as a model for expansion. Dr. Mohan cited the ‘snowball effect’ for his success: “Start small, never start big, expand whatever works well.”
- Charity: In India, only people below the poverty line receive any government healthcare funding. 70% of Indians therefore pay out of pocket for medical care. Often they can’t even afford insulin. Dr. Mohan’s charity, DIRECT, currently provides lifelong free treatment for >15,000 patients. The charity also supports free diabetes clinics and mobile hospitals, free diabetes camps (25,000 to date), free screening for diabetes (5m screened to date) and large public awareness programs.
Dr. Mohan closed by quoting an Indian scientist, Prof. J. C. Bose, who said, “When one dedicates himself (herself) wholly for a great object (cause), the closed doors shall open and the seemingly impossible will become possible for him (her).” He thanked his doctors, saying, “While I am standing here giving my talk, these people are doing the work, seeing patients six days a week .. it’s not easy…so this is for them.” Bravo.
Big Picture of Diabetes Therapy
Additional CATALYST trial insights and perspectives on the current hypercortisolism diagnostic cutoff from UNC’s Dr. John Buse
Dr. John Buse (UNC School of Medicine) compared the characteristics of CATALYST trial participants when stratified by post-dexamethasone suppression test (DST) cortisol levels. As background, the CATALYST trial (Part 1 and Part 2) evaluated the prevalence of hypercortisolism in people with difficult-to-treat T2D (Part 1, n=1,057) and the efficacy of Korlym (mifepristone) as a therapeutic intervention (Part 2, n=252). Hypercortisolism, also known as Cushing’s syndrome, is characterized by excess cortisol in the body, and signs and symptoms include hypertension, diabetes, and rapid weight gain in the face, abdomen, and back of the neck. A dexamethasone suppression test assesses whether cortisol production can be suppressed using dexamethasone, a steroid known to decrease cortisol levels. Following the test, cortisol levels >1.8 µg/dL may indicate hypercortisolism. In the present analysis, CATALYST trial participants were stratified into three groups based on post-DST cortisol levels (<1.2 µg/dL, 1.2-1.8 µg/dL, and >1.8 µg/dL).
- Use of antihyperglycemic medications. GLP-1 RA and SGLT-2 inhibitor use was more common in both the >1.8 µg/dL and 1.2-1.8 µg/dL groups compared to the <1.2 µg/dL group (GLP-1 RAs: 62% vs. 61% vs. 53% of participants; SGLT-2 inhibitors: 62% vs. 57% vs. 45%). This was also true for combination therapy involving insulin, GLP-1 RAs, and/or SGLT-2 inhibitors. For both mono and combination therapy, there were no significant differences between the >1.8 µg/dL and 1.2-1.8 µg/dL groups. Use of insulin, sulfonylureas, and pioglitazone monotherapy was not significantly different across all three groups.
- Use of antihypertensive, cardiovascular, analgesic, and psychiatric medications. Hypertensive use was significantly more common with each increasing post-DST level group. Use of lipid-modifying agents was more common in both the >1.8 µg/dL and 1.2-1.8 µg/dL groups compared to the <1.2 µg/dL group, though there were no significant differences between the >1.8 µg/dL and 1.2-1.8 µg/dL groups. This was also true for other CV medications, analgesics, and psychiatric medications
- Prevalence of cardiac comorbidities. Cardiac disorders (e.g., coronary artery disease, atrial fibrillation, congestive heart failure) were more common in both the >1.8 µg/dL and 1.2-1.8 µg/dL groups compared to the <1.2 µg/dL group. There were no significant differences between the >1.8 µg/dL and 1.2-1.8 µg/dL groups.
- Discussion. Findings from this analysis show that participants in the 1.2-1.8 µg/dL range share more similarities with those in the >1.8 µg/dL group than the <1.2 µg/dL group. Dr. Buse proposed that that while current guidelines recommend a hypercortisolism diagnostic cutoff of >1.8 µg/dL, cardiometabolic risk appears to exist along a continuum. He called for more research to elucidate whether a lower cutoff is warranted.
C-peptide measurements to improve classifications of diabetes in routine clinical practice
Closing out one of the last sessions of EASD, Prof. Andy Jones (University of Exeter, UK) and Prof. Mark Strachan (Western General Hospital, UK) spoke on classifications of diabetes in adults in routine clinical practice. Both panelists highlighted the challenges of diabetes classification and the risks that come with misdiagnosis. They emphasized the importance of integrating better criteria for diagnosis, including C-peptide levels.
- Prof. Jones on overcoming diagnostic challenges of T1D and T2D. Differences in glycemic treatment requirements depend on endogenous insulin production, as T1D refers to absolute insulin deficiency and T2D relates to relative insulin deficiency. However, clinical features like onset of diabetes, ketone levels, and BMI do not clearly discriminate between T1D and T2D at diagnosis. Among many characteristics, the age of diagnosis serves as the strongest clinical indicator of diabetes subtype. Prof. Jones explained that the strong association between age and T2D risk indicates that the vast majority of new-onset diabetes in older adults is T2D. T1D diagnosis in older adults remains challenging because 95% of T1D cases include an onset at the age of 15, with any associated features and predictive value >96%. On the other hand, 1% of T1D cases have an onset at the age of 65 with no single feature that makes T1D diagnosis likely, along with a predictive value >7%.
- Prof. Jones reminded that islet autoantibodies provide the most utility to diabetes diagnosis and serve as a reliable predictor of future progress or decline in endogenous insulin. In comparison, C-peptide levels show most utility in longstanding diabetes but remain a poor predictor of future diagnosis. Therefore, islet autoantibodies have a weak relationship to current treatment requirements, while C-peptide levels are better for clinical use in diabetes management and intervention.
- Due to challenges in diabetes diagnosis, patients face misclassification of diabetes in older adults. In a study, 58% of adults in the UK with T1D who tested negative for autoantibodies were confirmed to have T2D through C-peptide and genetic testing. Furthermore, studies have shown that the presence of positive islet autoantibodies does not always confirm a diabetes diagnosis. Therefore, Prof. Jones encouraged the implementation of international guidelines that advise routine testing, especially among adults with suspected T1D. Furthermore, he urged the audience to consider other diagnostic criteria, as negative islet autoantibodies do not exclude T1D.
- Prof. Strachan on routine biomarker assessments in diabetes management. Prof. Strachan and his team have implemented a diagnostic algorithm to help increase the classification and diagnosis of T1D. The algorithm included three components, including: (i) C-peptide levels; (ii) autoantibody testing; and (iii) genetic testing. By integrating the structured algorithm into clinical care, the study detected 114 patients with C-peptide levels >200 pmol/L, among 859 participants tested. Additionally, 54 patients met the criteria for T1D diagnosis. Furthermore, 58 people were reclassified, including 44 people as T2D and 14 with monogenic diabetes. Prof. Strachan commented that a 7% reclassification rate reflects the challenges of diagnostic criteria and encouraged the use of C-peptide levels for better diagnosis and cost efficiency.
- Prof. Strachan highlighted the national program of diagnostic biomarker testing in T1D in Scotland. In 2021, Scotland became the first country to offer C-peptide blood tests to improve diagnostic accuracy. Scotland currently has 37,124 people with T1D diagnosis, and about 45% of this population has had a C-peptide measurement. However, Prof. Strachan commented that the implementation of this biomarker testing has significant geographic variation, especially as it depends on individual decision of HCPs. Therefore, he encouraged HCPs to increase awareness and uptake of C-peptide measurements.
ELSA study shows acceptability and feasibility of general population screening for pre-symptomatic T1D among children in the UK
During an oral session, Prof. Parth Narendran (University of Birmingham, UK) presented updated findings from the ELSA study (n=25,165) that was published in a preprint article in The Lancet last week. This study focused on the feasibility and acceptability of general population screening for pre-symptomatic T1D among children in the UK. Overall, results showed that the screening model was feasible with 91% of families completing confirmatory testing, 95% completing staging processes, and 84% attending follow-up education programming. Almost all families rated the experience positively. As the UK’s largest pediatric trial for population screening, the ELSA study provides insightful considerations for shaping future screening programs in the UK and international regions.
- Methods. Children across the UK were offered screening for autoantibodies with dried blood spot samples (DBS) in various settings that included: (i) schools; (ii) primary care physicians; (iii) social media; (iv) hospitals; and (v) community centers. Following positive DBS results, children were followed with a venous confirmation test for specific autoantibodies. Children who showed multiple positive autoantibodies received metabolic staging with an oral glucose tolerance test. The study defined feasibility based on the type of recruitment, uptake of screening, and demographic factors; acceptability was assessed through qualitative interviews with families following the study.
- Trial Results. Between November 2022 and 2024, the study enrolled 25,165 children. The median age was eight years, 52% were male, and 37% of families had a history of T1D. Recruitment worked well across schools, primary care settings, and social media platforms. In community settings, non-White ethnicities showed higher rates of participation; Black and South Asian populations had under-recruitment.
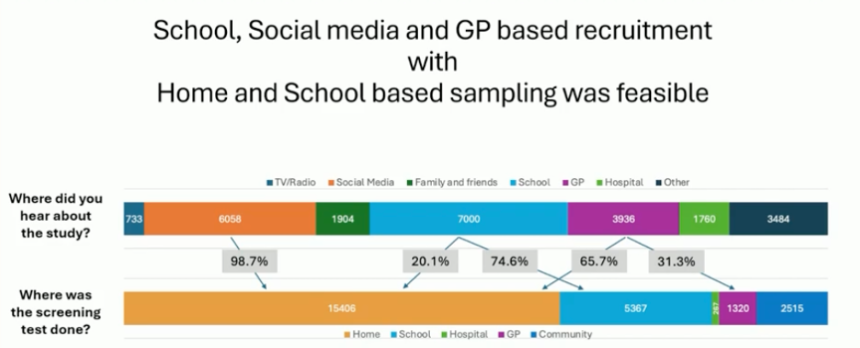
- Clinical Results. In the study, 98% of children screened DBS negative and 2% positive. 95% of children who screened positive received venous confirmation and metabolic staging. The study identified 56 single-antibody and 125 multiple-antibody children, and 85% completed education and support for diabetes management. Furthermore, 98% of the population found the screening acceptable, with a positive experience and willingness to recommend it to others. Some families particularly highlighted the overall convenient process of screening and the opportunity to become informed about a child’s risk status.
- Future outlooks. Reflecting on these findings, Prof. Narendran reminded that first-degree relatives are an effective target population for screening, especially as they were more engaged (i.e., 37% of ELSA participants) and showed greater participation for returning diagnosis kits. Furthermore, he emphasized that first-degree relatives are more likely to screen positive with a 3.7% diagnosis rate, compared to 2.2% for those with any relatives with T1D and 0.25% in the general population.
Discussion with Dr. Alice Cheng, Prof. Francesco Giorgino, and Prof. Ezio Bonifacio on population-wide, age-indiscriminate screening for T1D
In this standing-room-only afternoon symposium sponsored by Sanofi and chaired by Dr. Alice Cheng (University of Toronto), Prof. Francesco Giorgino (University of Bari Aldo Moro, Italy) and Prof. Ezio Bonifacio (University of Dresden, Germany) discussed the evolving landscape of T1D screening. Speakers urged attendees to think about moving beyond family history and pediatric models to encourage a more inclusive and data-driven approach to T1D screening.
- Dr. Cheng cited that more than half of new T1D cases occur in adults, yet screening efforts and diagnostic algorithms remain largely pediatric-focused. The panel highlighted findings from the Diabetes Care paper published in July 2025, “Contrasting Adult and Pediatric Populations in a Cohort of At-Risk Relatives in The T1D TrialNet Pathway to Prevention,” which showed that adults with stage 2 T1D[1] progress to stage 3 at similar rates as children (5-year risk: 78% for both groups), challenging assumptions about disease trajectory and pacing.
- On misdiagnosis, Prof. Giorgino pointed to the prediabetes space and the need for better sensitivity in tools, while acknowledging that no perfect algorithm exists. Dr. Cheng further cited that of the 39% of T1D diagnosis that are missed in adults, 77% are misdiagnosed with T2D. Prof. Giorgino discussed the AABBCC approach (age, autoimmunity, body habitus, background, C-peptide, and comorbidities) as a practical framework, with a need for continued work on improving screening for T1D.
- Dr. Cheng then directed the focus to understanding population-wide screening protocols in Italy and Germany. Prof. Giorgino highlighted Italy’s 2023 mandate for universal pediatric screening for T1D and celiac disease. He emphasized that providing concrete incentives for population-level screening, such as significant DKA reduction, is imperative in making legislative progress. Prof. Bonifacio highlighted Germany’s success with its Fr1da study, which began in 2015 and screens for children in Bavaria and other regions for T1D. Studies like this serve as a model to evaluate the feasibility of population-wide screening for T1D in children. Despite the progress, Prof. Bonifacio acknowledged that there needs to be more widespread coverage for diabetes care in general in Germany. Ultimately, speakers emphasized that only ~10% of people with T1D have a first-degree relative with the disease, and thus identifying the remaining 90% requires robust systems and multi-test strategies at a population level.
- Dr. Cheng called for advocacy and engagement, highlighting programs like TrialNet in North America that allow individuals to enroll in research and risk monitoring. She emphasized the role of clinicians and researchers in mobilizing at-risk populations and influencing policy to expand access to screening. Drawing on the successes of Italy, highlighted by Profs. Giorgino and Bonifacio, Dr. Cheng emphasized the need for legislators to hear from those directly affected by T1D.
An early look into the Breakthrough T1D-led early-stage T1D screening consensus document: Recommendations on who, what, when, where, how
In a well-attended afternoon session chaired by Breakthrough T1D’s Dr. Anastasia Albanese-O’Neill, Dr. Marian Rewers (University of Colorado), Prof. Anette-Gabriele Ziegler (Helmholtz Zentrum Munich, Germany), and Prof. Chantal Mathieu (UZ Leuven, Belgium) shared insights and recommendations on population-level screening for early-stage T1D from an upcoming consensus document. As background, there currently is a consensus monitoring guidance document for early-stage T1D, which was unveiled at ADA 2024. The draft consensus document under discussion focuses on an even earlier step: screening individuals before they have developed early-stage T1D. Currently, the document is undergoing peer review, after which it will be open to public comment and endorsement from global diabetes societies and organizations prior to publication.
- Dr. Rewers discussed the benefits and challenges of T1D screening. Prior to clinical diagnosis, T1D screening can give patients and their families a “soft landing,” affording them time to plan, prepare, and receive education. They may also have the opportunity to receive disease-modifying therapy, namely Tzield (teplizumab), or participate in clinical trials that may stop or slow disease progression. Screening can also prevent DKA and hospitalization at diagnosis, and early detection and glycemic control can improve long-term outcomes and decrease complication risk.
- On potential challenges and solutions, Dr. Rewers recognized that blood sampling can be painful and fear-inducing and recommended topical anesthetics. Awareness of early-stage T1D can also induce anxiety, and receiving an early-stage T1D diagnosis can also be stigmatizing. To this, Dr. Rewers emphasized the importance of keeping patients and their families engaged in informative monitoring programs and offering community education to raise awareness and reduce stigma. False-positive test results can be minimized by using highly sensitive assays (e.g., radiobinding assay, ELISA, ECL, ADAP, LIPS), and false reassurance following a negative result can be mitigated by offering clear guidance and information on next steps.
- Prof. Ziegler reviewed recommendations on populations to be screened and the age and cadence of screening. Prof. Ziegler advocated for general population screening. She highlighted the Fr1da study, which offered population-level screening in Bavaria, Germany, from 2015 to 2019, and revealed that progression rates from islet autoantibody positivity to T1D are similar in people with and without relatives with T1D. Fr1da also showed a 93% reduction in DKA (2.5% of participants vs. 36.7% in the general population) and 44% reduction in mean A1c at diagnosis (6.8% among participants vs. 10.5% in the general population). To facilitate population screening, Prof. Ziegler emphasized the need for infrastructure that can confirm positive results and monitor individuals who test positive.
- On when and how often to screen, Prof. Ziegler stressed the importance of rescreening for children if they are islet-autoantibody-negative. Specifically, drawing from findings in the BabyDiab, TEDDY, Fr1da, and T1DI studies, screening is recommended at two to four years old, and rescreening is recommended at six to eight years old, and 10-15 years old. There is not as much research around screening for individuals older than 15 years old. In this population, the recommendations propose a one-time screening in addition to following established public health activities.
- Prof. Mathieu gave an overview of the recommendations for where screening should take place and how to effectively communicate results. Barriers to participation can be minimized by integrating screening into established public health activities such as vaccination clinics. It is also important for providers to be knowledgeable on the entire screening process, from before screening takes place to next steps following screening (e.g., delivery of results and referrals). On communicating results, Prof. Mathieu highlighted the importance of using clear and neutral terminology. If islet autoantibodies are not detected, providers should recommend rescreening in the future and emphasize that it is still possible to develop T1D even though results are currently negative.
- On gaps in understanding, Prof. Mathieu highlighted that more research is needed to understand whether adults should be screened for early-stage T1D. She also noted that early-stage T1D and T1D disease progression is not as well studied in non-white populations. Further, there are many opportunities on the precision medicine front that can enable personalized approaches to monitoring and treatment.
Glucose Monitoring – BGM, CGM, and CKM
CGM and DGK: Dr. Bergenstal highlights technology-enabled improvements in T1D and T2D management
Dr. Richard Bergenstal (International Diabetes Center), Prof. Monika Kellerer (Marienhospital Suttgart, Germany), and Prof. Ramzi Ajjan (University of Leeds, UK) highlighted the evolving role of continuous monitoring and technology in diabetes care. Dr. Bergenstal framed dual glucose-ketone (DGK) monitoring as an “evolutionary step,” emphasizing its potential to reduce DKA by providing real-time ketone data, integrating alerts, and supporting early intervention. Prof. Kellerer focused on CGM in T2D not on insulin, presenting evidence that CGM improves A1c and Time in Range (TIR) and reduces both all-cause and diabetes-related hospitalizations. Prof. Ajjan underscored how CGM supports therapy adherence and lifestyle modification, demonstrating that structured CGM use alongside education and exercise guidance can meaningfully improve glycemic outcomes, while also highlighting the limitations of current metrics like GMI and the ongoing issue of therapeutic inertia in T2D management. Together, the session emphasized that continuous monitoring of all kinds can drive both clinical and behavioral improvements across the diabetes spectrum.
- Dr. Bergenstal opened the session with a forward-looking discussion on DGK monitoring. He first contextualized DGK within the historical trajectory of diabetes management: as attention to hypoglycemia grew, the DCCT/EDIC cohort saw progressively lower A1c levels, driven by the advent of CGM, AGP standardization, and AID innovation. Seeing glycemic data in real time allowed patients to link meals with glucose excursions, while clinicians could work panel-by-panel in the AGP to identify actionable problem areas. However, he said that DKA has not received a comparable degree of focus despite being the leading cause of death for children and adults with diabetes. While CGM use reduces DKA risk – the RELIEF study reported a ~50% reduction – it remains the most common acute event in both T1D and T2D. DCCT follow-up data, for example, documented over 400 DKA cases across 34 years of cohort data, with certain populations (pump users, women, individuals with cardiovascular disease, and those with diabetes-related foot complications) more likely to experience DKA. Intriguingly, those with CKD did not show higher risk, a finding Dr. Bergenstal noted warrants further study.
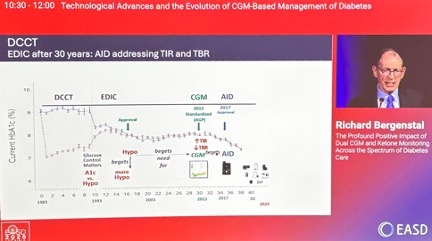
- Meanwhile, evidence continues to mount for the value of integrating ketone monitoring.Data suggest that patients with T1D using an SGLT-2 inhibitor with ≥0.8 mmol/L ketones face a 3.2x higher risk of ketoacidosis the following month. Despite this, most people with diabetes do not regularly test ketones: urine testing remains common, though less reliable, than blood measurement, and many rely on persistent, CGM-detected hyperglycemia alone to trigger ketone checks. Furthermore, an alarming proportion of patients with diabetes remain unaware of DKA symptoms and are unprepared for emergencies consistent with guidelines.
- Dr. Bergenstal argued that DGK will fill this gap by providing insight into the variability of ketone rises across individuals – variability that cannot be predicted from glucose trends alone. Citing Abbott’s glucose pump suspension studies, he underscored that ketone response was not dependent on baseline glucose or glucose rate of change, reinforcing the need for direct ketone measurement. For DGK to succeed, Dr. Bergenstal outlined three essential characteristics:
- Easy: Ideally, the same filament should measure both glucose and ketones;
- Accurate: Infusion suspension studies have shown promising agreement between continuous ketone monitoring and lab values; and
- Integrated: DGK should follow the iCGM pathway, evolving into “iCKM.” Bergenstal noted that four companies have confirmed that it will integrate with Abbott’s DGK once available (Sequel’s twiist, Tandem’s t:slim X2 and Mobi with Control-IQ+, Beta Bionics’ iLet, and Ypsomed’s mylife Loop), with Insulet also signaling its intent to integrate the sensor with Omnipod 5.
- He also advocated for standardized ketone thresholds, a “ketone range bar” in reports, and optional alerts for high ketone levels. Integration into the AGP report, alongside education for patients (like wallet cards for those on SGLT-2 inhibitors) and protocols for HCPs (including incorporating STOP DKA Protocol), will be critical for meaningful proactive action on rising ketones.
- To conclude, Dr. Bergenstal highlighted a recent case report from Australia involving a clinical trial participant randomized to either dapagliflozin or placebo. During the warmup period of his CGM, he received an early ketone alert at 1.5 mmol/L, which ultimately revealed a dislodged pump cannula. While he did not follow instructions precisely (delivering correction insulin via pump rather than pen), the DGK warning enabled earlier recognition and intervention, likely preventing severe DKA. He reviewed a checklist of steps needed for successful DGK implementation (see below), stressing that all are achievable within the next several years. In his words, “If you want to know what ketones will do in response to glucose levels, you have to measure ketones as well.”
- Dr. Bergenstal argued that DGK will fill this gap by providing insight into the variability of ketone rises across individuals – variability that cannot be predicted from glucose trends alone. Citing Abbott’s glucose pump suspension studies, he underscored that ketone response was not dependent on baseline glucose or glucose rate of change, reinforcing the need for direct ketone measurement. For DGK to succeed, Dr. Bergenstal outlined three essential characteristics:
- Prof. Kellerer delivered a comprehensive overview of the growing evidence supporting CGM use in people with T2D who are not on insulin therapy. While both EASD and ADA guidelines already acknowledge the value of CGM in this population, she emphasized that CGM should be seen as a part of and contributing to a holistic care plan. She reviewed several publications supporting this position. A recent meta-analysis found that in people with T2D not on insulin, CGM users achieved greater A1c reductions, more TIR, and less Time below Range (TBR) compared to BGM users. Transitioning from BGM to CGM lowered A1c was also found to improve glycemic outcomes regardless of insulin use, and among those not on insulin, CGM use reduced hospitalizations by 11% for all-cause and 30% for diabetes-related events compared to pre-index periods. This finding was corroborated by a study published earlier this year, which found 18% fewer all-cause and 60% fewer diabetes-related hospitalizations in people not on insulin with 12 months of CGM use. Finally, highlighting a late-breaking abstract to be presented at EASD this year, Prof. Kellerer said that an economic modeling study from a Medicaid perspective showed that if CGM were reimbursed for all with T2D, it could prevent ~143,000 hospitalizations over three years and save ~$1.7 billion.
- Prof. Kellerer also highlighted its potential to reduce the need for therapeutic escalation in some patients. She highlighted a study that found that initiating CGM six months after starting a GLP-1 RA led to a 1.7% A1c drop (from 9.6%), comparable to reductions typically seen in insulin users. Additionally, in adults with T2D and A1c >8%, those treated with GLP-1 RA + FreeStyle Libre achieved an additional 0.4% A1c reduction vs. GLP-1 RA alone (-2.4% and -2.0%, respectively) when matched at baseline A1c (10.2%).
- She concluded with a review of CGM’s adherence and behavioral benefits. A French national claims late-breaker to be presented at EASD showed that patients with T2D have a higher risk of micro- and macrovascular complications compared to those without diabetes, concluding that CGM access could reduce treatment inertial contributing to these disparate outcomes. People with T2D not on insulin therapy with consistent FreeStyle Libre use, for example, has been shown to have a greater probability of treatment progression than those using BGM. CGM also increases self-care behaviors compared to BGM in T2D not on insulin, and patients have reported healthier choices in diet, activity, and overall diabetes self-care driven by CGM data.
- Prof. Ajjan continued the focus on T2D, emphasizing how CGM not only informs glycemic management but also supports lifestyle modification and therapy adherence. He cited the PDF trial, in which people with T2D on antihyperglycemic agents or basal insulin using CGM with structured education significantly reduced A1c and highlighted how CGM data can drive exercise-based treatment adjustments with subsequently TIR improvements. Prof. Ajjan emphasized that gentle, regular activity had greater long-term benefits than intense but infrequent exercise. Echoing the conclusion of Prof. Kellerer’s remarks, Prof. Ajjan underscored the broader challenge of therapeutic inertia in T2D management: despite CGM and other tools, medication intensification often lags behind, contributing to persistent hospital admissions for both microvascular and macrovascular complications.
Dexcom COO Mr. Jake Leach spotlights CGM as a tool for reducing diabetes complications and enhancing therapy optimization
A well-attended afternoon symposium sponsored by Dexcom provided strong support for considering CGM to be a direct tool for the treatment of diabetes. Prof. Sufyan Hussain (King’s College London, England), Dr. Keri Leone (Senior Director of Global Medical Affairs, Dexcom), Dr. Halis Akturk (University of Colorado Anschutz), and Mr. Jake Leach (President and COO, Dexcom) discussed a breadth of uses for CGM, emphasizing that it should be considered an intervention rather than simply a monitoring device. CGM has demonstrated benefits for vascular complications, improving hospitalization rates and outcomes, and many other benefits independent of insulin delivery. With the introduction of Dexcom’s Smart Basal feature for calculating a personalized recommended dose of basal insulin, the benefits of CGM may continue to expand even further.
- Dr. Leone presented compelling evidence supporting the use of CGM to reduce micro- and macrovascular complications. A 2024 cohort study including 550 individuals with T1D who had not previously used CGM, initiation of CGM was associated with a lower risk of developing diabetic retinopathy (DR). During the eight-year study period, 22% of participants progressed to DR. CGM use was associated with a 47% lower likelihood of developing DR. Interestingly, insulin pump use alone had no positive or negative relationship with the development of DR. Use of insulin pumps and CGM together was associated with 40% lower odds of proliferative DR compared to patients using neither device. Turning to macrovascular complications, Dr. Leone also discussed the use of CGM for reducing cardiovascular disease risk. In a study of 47 participants using the Dexcom G6 CGM, there were significant reductions to A1c, BMI, triglycerides, blood pressure, total cholesterol, diabetes distress and 10-year predicted risk for atherosclerotic cardiovascular disease (ASCVD). In all, Dr. Leone strongly recommends the use of CGM as a behavioral tool to improve glycemic management and reduce the likelihood of complications.
- Dr. Akturk positioned CGM as an active tool for advancing outcomes along the care journey. A 2024 real-world study of 74,679 adults with T2D demonstrated significant reductions in all-cause hospitalizations, acute diabetes-related hospitalizations and acute diabetes-related emergency room visits. When CGM is provided to patients in need who may be struggling with glycemic management, such as through the Dexcom Community Glucose Monitoring Project, significant improvements to A1c are noted (9.4% at baseline compared to 7.1% at 12 months), with 86% of patients meeting an A1c target less than 8.0% by 12 months. Structured interviews with PWD have also demonstrated that CGM improves both attitudes and behaviors with positive daily impacts.
- Finally, Mr. Leach emphasized how Dexcom aims to continually drive innovation in diabetes management with the announcement of Dexcom Smart Basal, an integrated titration module. He turned to Dexcom’s basal therapy optimization software that is designed to power precise insulin initiation and adjustments. When initiated by a healthcare provider in Dexcom Clarity, users will log insulin doses and CGM measurements to calculate a personalized recommended dose of basal insulin under the Smart Basal feature. The module is currently under review for approval from the FDA and CE-Marking, said Mr. Leach. Above all, he emphasized that this feature supports safety by avoiding insulin stacking and hypoglycemia risk. In closing, Mr. Leach said that Dexcom hopes to focus on significantly reducing hypoglycemia and DKA events in both adults and pediatrics as a guiding principle.
Roche’s Accu-Chek SmartGuide CGM: Real-world data (n=249) shows significant reduction (20%) in nocturnal hypoglycemic events with Night Low Predict feature
Roche’s afternoon symposium centered around its AI-powered Accu-Chek SmartGuide CGM, featuring new real-world data presented by Dr. Timothy Bailey (University of California, San Diego), clinical perspectives from Prof. Julia Mader (University of Graz, Austria), and a patient perspective from Ms. Michelle Schmidt (Diability, Germany). As background, Accu-Chek SmartGuide is differentiated by its three AI-enabled predictive algorithms: (i) Glucose Predict; (ii) Low Glucose Predict; and (iii) Night Low Predict. The CGM was unveiled at ATTD 2024, and performance study results (n=48) showed a 90.5% 20/20% agreement rate[1] and MARD of 9.2%. The CGM lasts for 14-days and requires one hour of warmup and one-time calibration on the first day of wear. It is currently only indicated for adults.
- Dr. Bailey presented a real-world analysis (n=249) on the CGM’s Night Low Predict feature. The analysis assessed the likelihood of three conditions with vs. without use of the Night Low Predict feature:
- One or more nocturnal hypoglycemic event (of any severity and, more specifically, level 2 hypoglycemia [<54 mg/dL])
- Nocturnal Time below Range (<70 mg/dL)
- One or more nocturnal hyperglycemic event (of any severity and, more specifically, >180 mg/dL)
- Inclusion criteria. Data used in the analysis came from users who had at least 15 days of sensor usage, including days with ≥70% sensor coverage. Users also had to have had at least one nighttime hypoglycemic event and received at least one prediction.
- Demographics and clinical characteristics. Study participants were mostly from Germany (n=214, 86%), with others from the Netherlands (n=20, 8%) and Switzerland (n=15, 6%). As background, Accu-Chek SmartGuide has only been launched in select European countries. The mean participant age was 52 years old, and the age range was 20-84 years old. There was a mix of participants with T2D (n=112, 45.5%) and T1D (n=89, 34%), with the remainder being unknown.
- Data availability. Of the 249 users, the median number of days of data availability was 32 days/user (range: 15-141 days). Users received predictions on 6,063 of 8,158 nights (74%), and hypoglycemic events were detected in 36% of nights.
- Results. With the Night Low Predict feature, significant improvements were seen for nocturnal hypoglycemic events and Time Below range, but not for nocturnal hyperglycemic events.
- Night Low Predict reduced the likelihood of one or more nocturnal hypoglycemic event of any severity by 20% and of a level 2 hypoglycemic event by 31%.
- Night Low Predict reduced the likelihood of any nocturnal time <70 mg/dL by 31% and Time <54 mg/dL by 39%.
- Night Low Predict did not have significant changes in the likelihood of nocturnal hyperglycemic events.
- Prof. Mader discussed the clinical benefits of predictive glucose technologies. She highlighted their ability to enable more proactive, rather than reactive, care. They also have the potential to reduce hypoglycemia, as demonstrated in Dr. Bailey’s presentation, improve sleep quality, reduce diabetes burden, and facilitate therapy adjustments. With Accu-Chek SmartGuide, only one data of user data is needed to begin using the Night Low Predict feature, and only a few hours of data are needed for the Glucose Predict feature, which has a prediction horizon of two hours.
- Ms. Schmidt shared a poignant personal experience with nocturnal hypoglycemia and highlighted the potential for predictive technologies to improve quality of life for people with diabetes and their loved ones. At the age of six, Ms. Schmidt experienced a severe nocturnal hypoglycemic event. She recalled waking up not to a CGM alarm, as those were not yet available at the time, but rather to her own body’s symptoms. She was unable to call out to her parents and had difficulty opening the glucose tablet packaging, eventually ingesting the tablets with the packaging. She described nocturnal hypoglycemia as one of the worst feelings a person can have, sometimes making her feel as if she were close to dying.
- Ms. Schmidt emphasized how predictive technologies can reduce fear. Since her experience with nocturnal hypoglycemia, Ms. Schmidt said her parents became especially fearful and would keep her glucose high at night to prevent lows. Predictive technologies, she believes, can be helpful in reducing that fear and worry. While these technologies still require user knowledge and are unable to think for patients, Ms. Schmidt felt that can still be helpful by thinking with patients.
Safety and accuracy of CGM for inpatient DKA management compared to hourly POC testing
Dr. Magdalena Bogun (Columbia University) presented a single-center observational study (n=163) evaluating the safety and accuracy of inpatient CGM for DKA management with IV insulin infusion compared to standard hourly point-of-care (POC) testing. Conducted at the height of the COVID-19 pandemic, the study included 44 patients monitored with Dexcom G6 CGM in an ED stepdown unit and 119 patients monitored with hourly POC testing in the ED or ICU. CGM was initiated at what was characterized as “provider discretion”. A smartphone receiver was placed on the IV pole, and both clinicians and nurses carried smartphone receivers to access real-time CGM data. Providers were instructed to confirm CGM values >350 mg/dL with POC testing, and CGM was primarily used for treatment adjustments between 100–350 mg/dL (unlike “real life” given that patients were on IV drips, glucose levels under 100 mg/dL weren’t seen). Addressing concerns expressed during Q&A about the expected accuracy of Dexcom G6 use during DKA and severe hyperglycemia, Dr. Bogun said that CGM was typically inserted after glucose levels had fallen below 350 mg/dL, allowing clinicians to track fluctuations during IV insulin therapy until discharge.
- Baseline characteristics: Adult participants had a mean age of 49 years with a fantastic mix of both T1D (40%) and T2D (60%). A little over half, 54%, were male. Admission labs and labs at DKA resolution did not differ between groups. Overall, 36% of participants required ICU admission — 50% in the SOC group vs. none in the CGM group.
- CGM accuracy: While Dexcom G6 sensors showed a MARD of 17.4% during IV insulin treatment and 19.8% after DKA resolution, above the widely-accepted threshold of 10% for most commercially available CGMs in outpatient use, it would be great to know a little more about how the comparisons were created. Clarke Error Grid analysis found 99% of paired values in Zones A/B during treatment and 96% post-resolution.
- Clinical outcomes. Time to DKA resolution was similar between groups (12.8 hours with CGM vs. 12.0 with SOC). Median hospital length of stay was comparable and said not to be statistically different though the difference, 120 hours vs. 99 hours, is one that patients may perceive as different – a full day! Median ICU stay in the SOC group was 28.5 hours. As expected, CGM patients required significantly fewer POC tests (median of five vs. 12; p<0.0001). Notably, hypoglycemic events were rare and not significantly different (0% vs. 3%), due to the insulin drip. Dr. Bogun emphasized that these findings demonstrate the safety of remote monitoring in hospital settings among people with diabetes admitted in DKA. She further hypothesized that the reduction in ICU admissions with CGM monitoring could lower system costs by reducing the time taken to conduct hourly POC glucose measurements (a dreaded task by many nurses as we understand it) without compromising outcomes. Presumably a benefit would be to nursing productivity.
International RCT finds CGM reduces risk of large-for-gestational-age infants in women with GDM
Prof. Tina Linder (Medical University of Vienna, Austria) presented results from the GRACE trial, a large multicenter randomized controlled trial (RCT) evaluating the impact of CGM usage versus self-monitoring of blood glucose (SMBG) on obstetric outcomes in women with gestational diabetes (GDM). We can’t begin to believe how much better CGM use must be for women with diabetes, especially new diabetes – gestational diabetes!
- Study design. The open-label trial enrolled women with GDM (n=375) across four sites in Austria, Germany, and Switzerland. Participants were randomized 1:1 to either Dexcom G6 CGM (n=190) or SMBG (n=185). Women in the SMBG group also wore a blinded CGM for 10 days after randomization and again at 36-38 weeks’ gestation, while those in the intervention group used CGM continuously until delivery. The primary endpoint was the proportion of large-for-gestational-age (LGA) infants, with secondary endpoints including maternal/neonatal outcomes, insulin use, CGM metrics, and safety. We are interested in learning more about short-term differences in cost, which wasn’t discussed, so that appropriate investment can be considered.
- Results. LGA occurred in 3.5% of infants in the CGM group versus 10.3% with SMBG, representing a whopping, statistically significant reduction that persisted after adjustment for baseline characteristics and study site (to say nothing of, we’re sure better health will likely also persist, but of course, that is unknown and hardly measurable unless a longer-term trial could be designed). Mean newborn weight percentiles were also lower in the CGM group. As would be expected, women using CGM demonstrated better TITR (70-140 mg/dL) between 36-38 weeks of gestation compared to baseline.
- Conclusion. Researchers concluded that CGM use lowers the risk of LGA infants in women with GDM and can help identify those who need intensified insulin therapy – to say nothing of, presumably, monitoring and taking care to prevent T2D. Prof. Linder emphasized that these findings, together with improved glycemic management, support CGM as a valuable tool and the standard of care in the management of GDM.
CGM use in hospitals: Clinical benefits and implementation challenges
Prof. Mikkel Olsen (Steno Diabetes Center Copenhagen, Denmark) and Dr. Elias Spanakis (University of Maryland School of Medicine) discussed the role of CGM in hospital management. Both speakers stressed that dysglycemia during hospitalization, which is common, costly, and often preventable, remains largely unaddressed in today’s care continuum.
- Prof. Olsen presented compelling data showing that CGM can improve both glycemic and other clinical outcomes in hospitals. In the DIETEC trial (n=166), inpatient CGM use among those with T2D increased TIR by nearly 15 percentage points (from 63% to 78%) when combined with structured insulin titration and inpatient diabetes teams. Day-to-day analyses showed patients on CGM steadily improved to 80-90% TIR by discharge, while those monitored by BGM plateaued at approximately 60%. It isn’t known if any participants were using CGM at baseline. Prof. Olsen acknowledged that accuracy is strongest in non-ICU settings and more variable in ICU patients, reinforcing the need that many in the ICU may need more attention to glycemic health. Glycemic gains for those with CGM were also associated with an impressive 24% drop in hospital complications, particularly infections. Looking ahead, he called for a consensus framework to define patient selection and glycemic targets, as well as for integration of CGM data into EHRs, striking an optimistic tone on the future of CGM use in hospitals.
- Dr. Spanakis emphasized both the promise and practical challenges of inpatient diabetes technology use. He cited the multicenter TIGHT trial (n=120), where even with intensive CGM use, one-third of hospitalized patients with T2D had mean glucose levels over 180 mg/dL, highlighting the difficulty of meeting targets within a four to five day hospital stay. He advocated for remote CGM telemetry, comparing it to cardiac monitoring, so nurses could oversee multiple patients and act on alarms in real time. On AID, while early studies of inpatient AID use have reported TIR levels of over 65-70%, Dr. Spanakis cautioned that scaling this technology will require algorithmic adaptation to “dynamic hospital environments” and extensive staff training and education – see another session at EASD on the University of Leicester’s new four-level diabetes technology competency framework for providers for more thoughts on how to tackle this issue. He also pointed to the emerging role of electronic glucose management systems (eGMS) – computerized insulin dosing algorithms – in improving inpatient outcomes. While he noted that most evidence remains retrospective, that is perhaps not surprising at the present time.
Evidence supports benefit of CGM for reduction of severe, recurrent hypoglycemia
Prof. Hans DeVries (Academic Medical Center, the Netherlands) reviewed evidence on the role of CGM and AID in reducing severe hypoglycemia, incorporating both clinical trial evidence and real-world data. His talk underscored how far the field has progressed since the early 2010s but also made clear that impaired hypoglycemia awareness remains the strongest driver of risk.
- RCTs show the clear benefit of CGM for high-risk groups, but not full protection. Early studies and meta-analyses did not demonstrate a reduction in severe hypoglycemia with CGM, largely due to poor sensor accuracy and the exclusion of patients with impaired awareness. Later trials targeting high-risk groups changed this picture, with crossover RCTs showing a reduction in severe events requiring external assistance. The HypoDE study (n=149) similarly demonstrated fewer events needing outside assistance, though effects on grade 4 events (such as seizures and hospitalizations) were limited.
- Real-world data confirm reduced hospitalizations with CGM. Prof. DeVries referenced an analysis of over 3,000 CGM initiators, with results showing that emergency visits or hospitalizations for hypoglycemia dropped from 5% to 2% in the year after CGM initiation, compared to no meaningful changes among non-initiators. Large pediatric registries (n=100,000) also show declines in severe hypoglycemia incidence over time, but rates remain at approximately 1.7 events per 100 patient-years.
- Impaired hypoglycemia awareness remains the dominant risk factor, more so than high absolute Time below Range (TBR) values. Prof. DeVries noted that around 20-25% of people with diabetes fall into this category, and their risk of a severe hypoglycemic event rises steeply, even with less overall exposure to hypoglycemia. In a study comparing CGM with structured psychological training, both reduced severe events, but CGM provided a more pronounced and durable effect. This effect was particularly pronounced when it was incorporated after behavioral training had failed.
- Looking ahead, Prof. Hans emphasized the potential of closed-loop systems for hypoglycemia prevention. Systems that suspend insulin delivery in response to early warning signs already prevent many events, but because subcutaneous insulin has a residual effect, complete protection still requires additional work. He pointed to bihormonal systems combining insulin and glucagon as a promising solution to eliminate the severe hypoglycemia and mentioned that such devices are currently being tested in promising pivotal trials.
Trust as the cornerstone: CGM, AID, and AI in the next era of diabetes care
This afternoon session on EASD’s Spotlight Stage explored the intersection of CGM, AID, and AI in diabetes care, with faculty emphasizing trust, safety, and patient-centered innovation as guiding principles. Prof. Stefano Del Prato (Sant’Anna School of Advanced Studies, Italy) warned that rapid expansion of CGM without robust reliability standards could erode clinician and patient trust, while Prof. Eric Renard (CHU Montpellier, France) highlighted the promise of AI-driven registries and digital twins in advancing AID and Prof. Sabine Hofer (Medical University of Innsbruck, Austria) shared her goals for diabetes care in 2045. Across the discussion, speakers agreed that technology must remain transparent, reliable, and supportive of human-centered care.
- On current and future applications of AI. Prof. Del Prato highlighted that AI is already present in care: AI-enabled fundoscopy analysis is used to determine diabetic retinopathy (DR) severity, and exploratory studies are testing applications from X-rays predicting diabetes risk to facial texture and tongue features identifying prediabetes. AI holds strong potential for specific applications such as optimizing insulin doses without increasing hypoglycemia.
- On CGM. Prof. Del Prato spotlighted the widening use of CGM when building his case that the most important factor in expanded diabetes technology adoption is patient and clinician trust in safety. He reiterated his call from the Spotlight Stage yesterday for stricter authorization requirements in the EU, with standards for reliability and safety comparable to those in the US, Canada, and Japan. Prof. Hofer added that this is particularly important for children and adolescents, the group most likely to use diabetes technology. Trust in accuracy, she emphasized, is essential to driving down population-level A1c and severe adverse events, while registries tailored to pediatric populations are key to informing future interventions.
- On AID. Prof. Renard said that Europe’s extensive patient registries offer strong potential for accelerating AI implementation in AID, enabling international data standardization for applications such as: (i) PCP-led phenotype identification for risk and treatment optimization; and (ii) digital twin technology to support individualized treatment decisions. On the latter, he noted that digital twins could be powerful tools for optimizing AID system settings.
- On fully closed-loop (FCL) systems, Prof. Renard remarked that “we are not far.” He predicted that within 10 years, algorithms built on neural networks could fundamentally reshape AID, with the potential to reach 100% TIR or even TITR. While not mentioned in the session, see the AIDANET neural network FCL AID system in development. Prof. Hofer added that eliminating the need for accurate carbohydrate counting would free providers to focus on patients’ lives rather than glucose excursions.
- On concerns with AI. Prof. Hofer emphasized that trust remains the biggest barrier, as clinicians often cannot explain to patients where their data is going or how it will be protected. Prof. Del Prato added that privacy, regulation, and cost-effectiveness must all be addressed, along with clear guidelines and proper educational support for stakeholders.
- On the future of diabetes care. Profs. Del Prato, Renard, and Hofer agreed that diabetes care in 2045 should be more patient-centered, with providers able to devote more time to listening to patients’ primary concerns. By streamlining routine tasks, Prof. Renard argued, AI will ultimately “make a more human medicine.”
- On the EUDF consensus statements. Prof. Del Prato previewed the forthcoming EUDF consensus roadmap, “Artificial intelligence driven clinical decision-support systems to assist healthcare professionals and people with diabetes at the point of care: a Delphi-based consensus roadmap,” soon to be published in Diabetologia. He summarized its key recommendations: AI should: (i) facilitate patient-centered care; (ii) empower HCPs; (iii) include robust regulation and privacy safeguards; (iv) optimize clinical data capture; and (v) encourage data standardization and sharing.
Diabetes technology for pregnancy: Bridging gaps between evidence and guidelines
Prof. Latife Bozkurt (Vienna Health Care Group, Austria), Prof. Christian Göbl (Medical University of Vienna, Austria), and Prof. Katrien Benhalima (UZ Leuven, Belgium) offered complementary perspectives on how CGM and AID systems have the potential to reshape care for pregnant women with T1D, T2D, and gestational diabetes. Collectively, their talks underscored how technology is reshaping maternal-fetal care while also exposing gaps in global guidance and equity.
- Prof. Bozkurt emphasized how CGM and hybrid closed-loop (HCL) systems are transforming glycemic management in T1D pregnancies, shifting from reactive, manual approaches to data-driven and partially automated care. Data from the CONCEPTT RCT (n=108) and an observational cohort study (n=186) show that modest TIR improvements (approximately 7%) translate into meaningful reductions in neonatal complications, including a 46% reduction in large-for-gestational-age (LGA) infants. Approved AID systems such as CamAPS FX (AiDAPT trial: n=57, +15% TIR) and MiniMed 780G[2] (CRISTAL trial: n=95, higher overnight TIR) show promise, though adaptations for pregnancy physiology remain essential. Open questions include when to initiate AID during pregnancy, how to best adapt algorithms, and how to manage systems postpartum.
- Prof. Göbl presented results from the GRACE study, the largest RCT of CGM in women with GDM to date (n=375). Women randomized to CGM had: (i) fewer LGA infants (3.5% in the CGM group vs. 10.3% in the BGM group); (ii) lower birth weight percentiles; (iii) modest TIR gains (95% in the CGM group versus 93% in the BGM group); and (iv) fewer NICU admissions – all achieved without increased severe hypoglycemia. Prof. Göbl contextualized these findings with prior evidence: the CONCEPTT trial demonstrated clear benefits in T1D, while DipGluMo (n=330) showed neutral results for CGM use in GDM, highlighting heterogeneity across different populations and the need for tailored guidance.
- Prof. Benhalima unveiled a new international consensus statement on diabetes technology in pregnancy, convened by the diaTribe Foundation with multidisciplinary input from global experts and patient representatives. The statement is currently in review, and we very much look forward to further updates.
GRACE and DipGluMo show the huge power of CGM’s role in GDM management
Gestational diabetes mellitus (GDM) was a major focus on the final day of EASD 2025 in this Dexcom-sponsored symposium. Prof. Tina Linder (Medical University of Vienna, Austria), Prof. Christian Göbl (Medical University of Vienna, Austria), and Prof. Helen Murphy (University of East Anglia, the UK) explored recent data on CGM use in gestational diabetes, comparing findings from the GRACE and DipGluMo studies to explore the potential for CGM to improve both maternal glycemic management and neonatal outcomes. All over the floor today, we kept hearing, “did you see the GOBL data?” … which initially sounded like a trial, but really reflects the name Göbl, for Professor Göbl, of course!
- As a reminder, the GRACE study results were first presented on Tuesday by Prof. Linder (Medical University of Vienna, Austria). The open-label trial enrolled women with GDM (n=375) across four sites in Austria, Germany, and Switzerland. Participants were randomized 1:1 to either Dexcom G6 CGM (n=190) or BGM (n=185). Women in the BGM group also wore a blinded CGM for 10 days after randomization and again at 36-38 weeks’ gestation. LGA occurred in 3.5% of infants in the CGM group versus 10.3% with BGM. Mean newborn weight percentiles were also lower in the CGM group. As expected, women using CGM demonstrated more Time in Pregnancy Range (TIPR, 65-140 mg/dL) between 36-38 weeks of gestation compared to baseline. Prof. Linder added that it is clear that there is high patient acceptance for CGM, with glycemic benefits from continuous monitoring seen even among those who traditionally don’t adhere to regular BGM testing. However, she identified the ongoing need to identify optimal TIR and glucose ranges for patients with GDM, as well as if there is a need for variable TIR by GDM phenotype.
- Prof. Göbl then reviewed findings from the Swiss DipGluMo study (n=299), which closely mirrored GRACE in design but yielded strikingly different results: LGA rates were identical between CGM and BGM groups (10% each). He suggested several possible explanations, including slightly younger age (33 vs. 34 years) and lower BMI (26 vs. 27 kg/m²) in DipGluMo suggesting a better-managed study population, as well as looser treatment targets, fewer recommended BGM checks, and more conservative insulin algorithms. As a result, rapid-acting insulin use was far lower in DipGluMo (4-5%) than in GRACE (30-41%). Prof. Murphy seized on these differences, warning against unrealistic expectations for LGA outcomes in GDM. She argued that since ~10% of infants in the general population are above the 90th percentile, this should remain the threshold for GDM care, rather than aiming for even lower rates. “We shouldn’t expect women with GDM to have smaller babies than they would if they didn’t have diabetes,” she concluded, stressing that focus should instead be on minimizing excess postnatal growth.
- Looking ahead. Prof. Murphy also pointed to CGM’s promise for detecting dysglycemia and GDM early in pregnancy, enabling earlier interventions and potentially lowering LGA risk. She expressed optimism about forthcoming results from the MAGiC study and its collaboration with GLAM, which she hopes will show that abnormal glucose patterns are already detectable in the first trimester.
MiniMed 780G vs. Control-IQ: Handling unannounced meal in adolescents with T1D
Dr. Salvatore Scirè Calabrisotto (University of Catania, Italy) presented a randomized crossoverstudy (n=20) evaluating the response of two hybrid closed-loop AID systems – Medtronic MiniMed 780G and Tandem Control-IQ – to unannounced meals. Unannounced meals remain a major challenge for AID systems, especially in adolescents, where missed or delayed boluses are common. MiniMed 780G’s Auto Correction bolus and Control-IQ’s (and Control-IQ+’s) AutoBolus features work to correct the associated rapid glucose excursions with unannounced meals, and both have been shown in separate studies to maintain positive glycemic outcomes even in those who frequently forget to bolus.
- Study design. The researchers employed a randomized crossover design. Participants consumed either a carbohydrate-only (CHO) breakfast (bread and jam, 31 g carbohydrates) or a mixed breakfast (30 g carbohydrates + 15 g protein). Group A (n=10) began with six meals (three CHO, three mixed) with meal announcements, followed by a seven-day washout and then six unannounced meals. Group B followed the opposite order. All participants were instructed to bolus 10 minutes before the announced meals.
- Baseline characteristics. Participants were adolescents with T1D (ages 11–18 years) who had been using AID for at least three months and had a diabetes duration at least one year. Mean age was 15 years, 35% were female, mean A1c was 6.9%, and mean TIR was 76%. Half the cohort used MiniMed 780G, which runs on a proportional-integral-derivative (PID) algorithm, while the other half used Control-IQ, which employs a model predictive control (MPC) algorithm.
- Results. Across both systems and meal types, glucose profiles converged within four hours. As expected, mixed meals produced a slightly delayed and higher peak due to protein metabolism. Unannounced meals led to earlier, sharper glucose excursions compared to announced meals (see figure below).
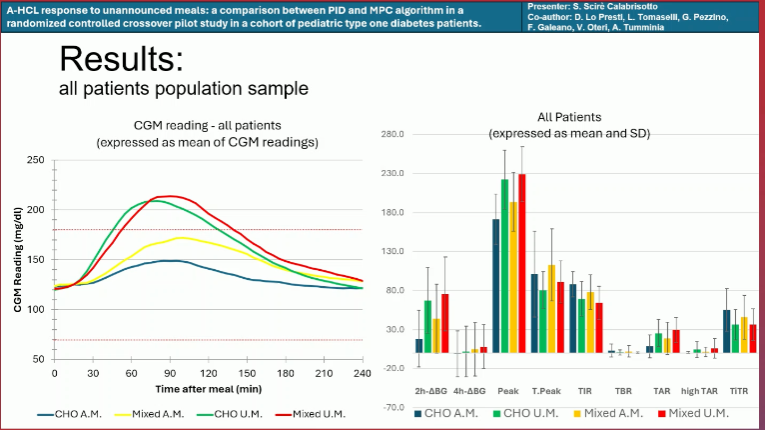
- MiniMed 780G vs. Control-IQ responding to CHO meals. With announced CHO meals, both systems produced nearly identical profiles, rising from ~120 mg/dL to ~150 mg/dL at ~90 minutes (see figure below). With unannounced meals, peaks were higher, but MiniMed 780G users had a lower mean peak (~200 mg/dL) than Control-IQ users (~220 mg/dL). Both systems achieved comparable TIR and Time in Tight Range (TITR; 70-140 mg/dL) with announced meals, though MiniMed 780G maintained slightly higher values with unannounced meals.
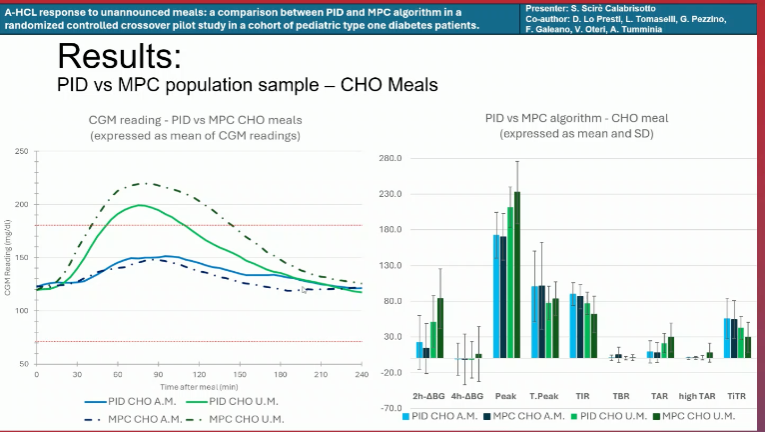
- MiniMed 780G vs. Control-IQ responding to mixed meals. With announced mixed meals, MiniMed 780G peaked at ~160 mg/dL and Control-IQ at ~180 mg/dL, both at ~90 minutes. With unannounced mixed meals, differences widened: MiniMed 780G peaked earlier and lower (~200 mg/dL) than Control-IQ (~230 mg/dL). Unlike with CHO meals, MiniMed 780G users achieved higher mean TIR with announced meals than Control-IQ users, which achieved a similar TIR to MiniMed 780G use with unannounced meals.
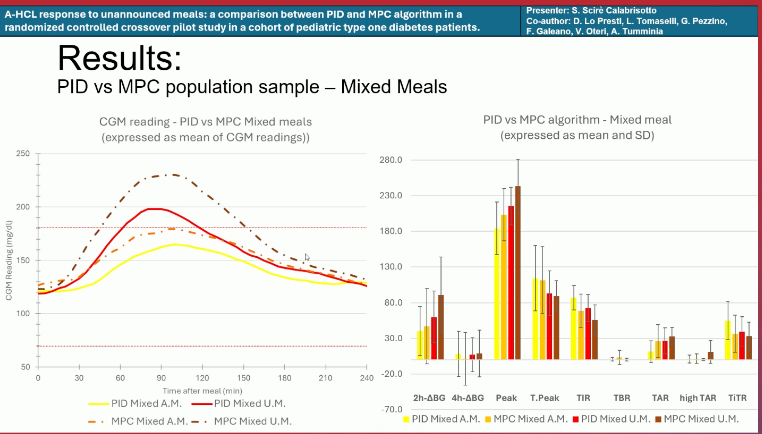
- Dr. Calabrisotto concluded that PID-based algorithms (MiniMed 780G) appear to handle unannounced meals slightly better than MPC-based algorithms (Control-IQ), regardless of meal type. However, both systems perform best when meals are announced, underscoring the importance of bolusing and meal disclosure even with advanced AID.
CGM as a routine for T2D: Evidence from RCTs, real-world data, and case studies
In an Abbott-sponsored symposium chaired by Prof. Stefano Del Prato (University of Pisa School, Italy), Prof. Emma Wilmot (University of Nottingham, UK) and Prof. Virginia Bellido (Hospital Universitario Virgen del Rocío, Spain) discussed why CGM should be considered part of a routine for people with T2D. Across RCTs, real-world data, and case studies, the session highlighted the consistent glycemic and behavioral benefits of CGM and called for policy alignment with existing evidence.
- RCTs and systematic reviews confirm that CGM improves outcomes in both insulin and non-insulin-treated T2D. Building on presentations at ADA 2025, speakers suggested using CGM for diabetes management for insulin-treated individuals. Data from FreeStyle Libre trials demonstrated 0.5% A1c reductions with improved treatment satisfaction. Furthermore, the MOBILE study (n=175) demonstrated a 0.4% A1c reduction in basal insulin users with CGM, and the IMMEDIATE study (n=116) confirmed benefits in those on non-insulin therapy. Another umbrella review further reinforced consistent A1c reductions, as well as TIR and TAR improvements, with findings invariant across CGM modality, study funding, and prior insulin use.
- Pairing CGM with structured education enhances engagement and behavior change. Prof. Wilmot highlighted that CGM is most impactful when paired with simple, tailored education. The PDF study, a 12-week RCT (n=126), showed that adding intermittently scanned CGM (isCGM) to lifestyle counseling significantly improved glycemic outcomes in adults with T2D. Prof. Bellido further detailed several case studies illustrating how CGM revealed post-meal hyperglycemia and nocturnal lows, driving adjustments in diet, insulin timing, and lifestyle. Notably, through both RCTs and case studies, FreeStyle Libre 3 use was associated with improved patient confidence, awareness, and adherence, suggesting that behavior modification is another benefit of CGM use.
- Policy and access remain misaligned with evidence despite consistent benefits across populations. The symposium closed with a call for healthcare systems to align reimbursement with evidence showing the benefits of CGM use in people with T2D, both with and without insulin treatment. Both Prof. Wilmot and Prof. Bellido stressed that CGM provides fundamental insights empowering both patients and HCPs to act earlier and more effectively. They also noted that impactful data should be leveraged to expand access, as every individual with diabetes has the potential to benefit from CGMs across diverse settings
CGM use in hospitals: Clinical benefits and implementation challenges
Prof. Mikkel Olsen (Steno Diabetes Center Copenhagen, Denmark) and Dr. Elias Spanakis (University of Maryland School of Medicine) discussed the role of CGM in hospital management. Both speakers stressed that dysglycemia during hospitalization, which is common, costly, and often preventable, remains largely unaddressed in today’s care continuum.
- Prof. Olsen presented compelling data showing that CGM can improve both glycemic and other clinical outcomes in hospitals. In the DIETEC trial (n=166), inpatient CGM use among those with T2D increased TIR by nearly 15 percentage points (from 63% to 78%) when combined with structured insulin titration and inpatient diabetes teams. Day-to-day analyses showed patients on CGM steadily improved to 80-90% TIR by discharge, while those monitored by BGM plateaued at approximately 60%. It isn’t known if any participants were using CGM at baseline. Prof. Olsen acknowledged that accuracy is strongest in non-ICU settings and more variable in ICU patients, reinforcing the need that many in the ICU may need more attention to glycemic health. Glycemic gains for those with CGM were also associated with an impressive 24% drop in hospital complications, particularly infections. Looking ahead, he called for a consensus framework to define patient selection and glycemic targets, as well as for integration of CGM data into EHRs, striking an optimistic tone on the future of CGM use in hospitals.
- Dr. Spanakis emphasized both the promise and practical challenges of inpatient diabetes technology use. He cited the multicenter TIGHT trial (n=120), where even with intensive CGM use, one-third of hospitalized patients with T2D had mean glucose levels over 180 mg/dL, highlighting the difficulty of meeting targets within a four to five day hospital stay. He advocated for remote CGM telemetry, comparing it to cardiac monitoring, so nurses could oversee multiple patients and act on alarms in real time. On AID, while early studies of inpatient AID use have reported TIR levels of over 65-70%, Dr. Spanakis cautioned that scaling this technology will require algorithmic adaptation to “dynamic hospital environments” and extensive staff training and education – see another session at EASD on the University of Leicester’s new four-level diabetes technology competency framework for providers for more thoughts on how to tackle this issue. He also pointed to the emerging role of electronic glucose management systems (eGMS) – computerized insulin dosing algorithms – in improving inpatient outcomes. While he noted that most evidence remains retrospective, that is perhaps not surprising at the present time.
Insulin Delivery: AID, Pumps, and Pens
At Medtronic’s Monday afternoon industry symposium, experts showcased growing evidence base supporting expanded labeling of MiniMed 780G. Prof. Tadej Battelino (University of Ljubljana, Slovenia), Dr. Tali Cukierman-Yaffe (Tel Aviv University, Israel), Prof. Kirsten Nørgaard (University of Copenhagen, Denmark), and Prof. Jurgen Vercauteren (KU Leuven, Belgium) presented data supporting the use of MiniMed 780G in children as young as two years of age, during pregnancy, and in insulin-requiring T2D populations. These findings were used to support the July 2025 CE-Mark announcement which authorized MiniMed 780G for these patient populations in the EU. The session concluded with a discussion on EDENT1FI, a large-scale European screening initiative for early-stage T1D, underscoring how earlier detection and CGM adoption have the potential to reshape care pathways. Together, the speakers reinforced Medtronic’s positioning of MiniMed 780G as a broadly applicable tool across the full spectrum of diabetes.
- Prof. Battelino reviewed results from the LENNY trial supporting the use of MiniMed 780G in children aged two and older. Young children with T1D often face high glycemic variability and neurocognitive vulnerability. Prof. Battelino cited recently published results (n=101) showing that MiniMed 780G improved Time in Range (TIR) by ~10 percentage points (68% in auto mode versus 58% in manual mode and during run-in) and lowered A1c levels by approximately 0.6% (average A1c of 7.0% in auto mode vs. 7.6% in manual mode; 7.5% during run-in) without new safety signals. Parents also reported improved sleep and reduced fear of hypoglycemia with use of the system. Based upon these positive results, the system recently received CE-Mark for children ages two and up. This aligns with growing guideline support (ISPAD, NICE, Germany) and national rollouts that prioritize pediatrics.
- Dr. Cukierman-Yaffe discussed the use of MiniMed 780G during pregnancy in women with T1D, emphasizing both opportunities and challenges. She presented cases across all trimesters, noting that open-loop and SmartGuard modes often require adjustment based on maternal needs. For example, in the first trimester, loosening the carb ratio and fine-tuning SmartGuard settings helped a patient with hypoglycemia unawareness maintain TIR without severe lows. In later trimesters, SmartGuard has proven valuable for controlling postprandial hyperglycemia, particularly when paired with “assisted carbs” (adding 20-50% carb equivalents to meals) to improve outcomes when dealing with increased insulin resistance associated with pregnancy. Dr. Cukierman-Yaffe concluded that while AID tools such as the MiniMed 780G system show strong promise in pregnancy, clinical oversight remains essential to balance maternal and neonatal outcomes.
- Prof. Nørgaard presented a comprehensive look at the use of MiniMed 780G in T2D, emphasizing efficacy, durability, and cost-effectiveness. Drawing on data from Denmark’s extensive registries, she noted that fewer than 20% of insulin-treated patients with T2D in this population achieve target A1c. In the IMPACT 2 study (n=95), switching from MDI or conventional pumps to MiniMed 780G improved TIR from ~72% to ~80% and lowered A1c by ~0.7% (7.9% to 7.2%). Real-world data (n=18,466) showed similar benefits, with optimal system settings (including a 100 mg/dL glucose target and two-hour active insulin time) proving critical even in those with high insulin requirements. Importantly, outcomes were sustained up to across 12 months of use. A cost-effectiveness analysis across Scandinavian countries demonstrated QALY gains and reduced complication risks, with adoption remaining well below willingness-to-pay thresholds in patients with baseline A1c ≥8.0%. Prof. Nørgaard concluded that MiniMed 780G is both clinically beneficial and economically justified for patients with insulin-treated T2D, particularly those with baseline glycemic challenges or renal complications.
- Prof. Vercauteren closed with insights from EDENT1FI, a European initiative that aims to screen 20,000 children for early-stage T1D. He emphasized how CGM, particularly use of the Simplera Sync sensor, is reshaping staging by providing child-friendly, real-world glucose data that is superior to traditional OGTTs. The consortium spans 27 partners across 13 countries and is evaluating: (i) medical; (ii) psychosocial; and (iii) economic outcomes of early screening. Prof. Vercauteren, who has T1D himself, stressed that access disparities remain a barrier. He called for parents to have the option to use CGM for monitoring at-risk children. In his view, early detection will only succeed if it is feasible, acceptable, and has equitable access.
Three years of MiniMed 780G: Durable glycemic outcomes, reduced burden, and strengthened patient confidence
Dr. Jennifer McVean (Medtronic) presented three-year real-world results (n=1,145) from MiniMed 780G users (≥16 years old) across Europe, the Middle East, and Africa (EMEA). Participants had “at least” 10 days of CGM use prior to starting MiniMed 780G automated mode, and ≥10 days of CGM data per month. Results at 36 months demonstrated strong early glycemic improvements sustained throughout three years of MiniMed 780G use, achieving reductions in user burden with fewer user-initiated boluses and greater trust in the system. Dr. McVean characterized these findings are especially important as we approach the fully closed-loop AID era, in that systems must be able to deliver the expected outcomes while building patient trust and reliance upon the systems.
- Early glycemic improvements across the board were sustained at 36 months of MiniMed 780G use. TIR increased rapidly from the “upper 60s%” at baseline to nearly 80% (79%, to be exact) and stayed stable throughout 36 months. TITR followed a similar pattern, increasing to 54% from a baseline of just over 40% and remaining ≥50% for 36 months. Time below Range (<70 mg/dL) dropped from 2.5% at baseline to 2.0% at one month and fell further to 1.8% at 36 months. Impressively, >75% of participants achieved target TIR >70%, and over half achieved target TITR of >50%. What impressive results!
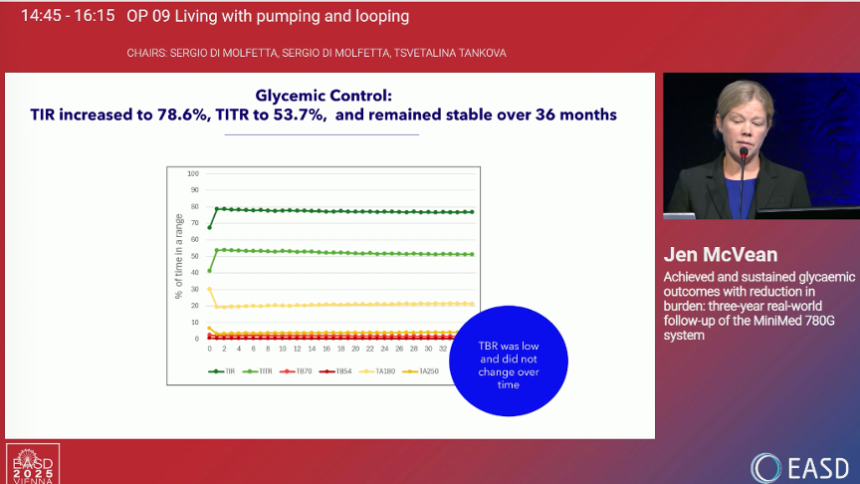
- Dr. McVean highlighted that these glycemic improvements occurred in the context of reduction burden. The percent of user-delivered insulin as a share of total delivered insulin fell from 52% to 42% at 36 months – first a rapid reduction, with a continual, gradual subsequent decrease. The amount of bolus insulin delivered automatically increased rapidly from none at baseline to 12% at one month and continued to increase over the course of the 36 months. Relatedly, user-initiated boluses fell from 5.6 per day at baseline to 4.8 per day, remaining relatively consistent over 36 months.
- User trust in the MiniMed 780G system also strengthened over the course of 36 months. The amount of time spent in automated mode, for example, remained in the mid- to upper-90% after its initial sharp rise after system initiation. At one month of use, ~40% of users were using the recommended glucose target of 100 mg/dL, reaching nearly 60% at 36 months. The recommended active insulin time of two hours had increased to 30% at one month, increasing to the mid-50% by study end.
Glycemic improvements with Tandem’s Control-IQ at 12 months maintained at 24 months
Prof. Jolien De Meuleeester (KU Leuven, Belgium) presented results from the INRANGE study, sharing two-year outcomes data on Tandem’s Control-IQ algorithm. Adults with T1D who started pump therapy using Control-IQ between October 2021 and December 2022 across 13 centers in Belgium were included in the study (n=473); 93% (n=442) had continued using Control-IQ at 24 months.
- Baseline characteristics. Over half (57%) of participants were men, with a mean age of 39 years and diabetes duration of 20 years. 47% were on MDI at baseline, and 53% had been on another AID system. Participants had a baseline A1c of 7.4% and TIR of ~59%.
- Results. Glycemic outcomes were consistent at 12 months and 24 months.
Metric | Baseline | 12 months | 24 months |
TIR | 59% | 71% | 71% |
TITR | 37% | 45% | 46% |
Time <70 mg/dL | 4.2% | 1.9% | 2.1% |
Time <54 mg/dL | 1.0% | 0.4% | 0.5% |
Time >180 mg/dL | 37% | 27% | 27% |
Time >250 mg/dL | 13% | 7% | 8% |
A1c | 7.4% | 6.7% | 6.7% |
- TIR. TIR increased from 59% at baseline to 71% at 12 and 24 months. The proportion of participants achieving target TIR >70% more than doubled – from 25% at baseline to 58% at 12 months and 56% at 24 months.
- TITR. A similar glycemic trend was observed with TITR, which increased from 37% at baseline to 45% at 12 months and 46% at 24 months. The proportion of participants achieving target TITR >50% nearly doubled, increasing from 18% at baseline to 30% at 12 months and 32% at 24 months.
- A1c. A1c fell from 7.4% at baseline to 6.7% at 12 months, which was maintained at 24 months. The proportion of participants achieving target A1c <7.0% nearly doubled, rising from 34% at baseline to 66% at 12 months and 64% at 24 months.
- Improvements to self-reported quality of life (QoL) at 12 months were also maintained at 24 months. Specifically, Control-IQ users reported significant improvements to physical and general health, as well as social function at 12 months. Significant improvements to physical health and social functioning were maintained at 24 months. Improvements to diabetes-specific QoL factors (see figure below) were all sustained at 24 months.
- Improvements in self-reported severe hypoglycemic events (SHE) and work absenteeism at 12 months were also sustained at 24 months. Self-detection of SHE had increased from four to 16 annual events at 12 months of use, and 15 annual events during the second year of Control-IQ use – a simply outstanding result. Similarly, the number of absentee days at work also nearly halved after 12 months of use – from 126 days to 73 days – and further fell to 69 days per year at 24 months. The confluence of these outcomes led to a maintanence of the composite heptagon – consisting of TIR, TITR, A1c, TBR, work absenteeism days, hypoglycemia fear survey worry score, and satisfaction score – at both 12 and 24 months of use (see figures below).
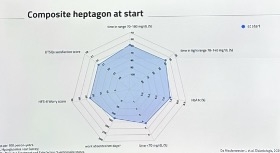
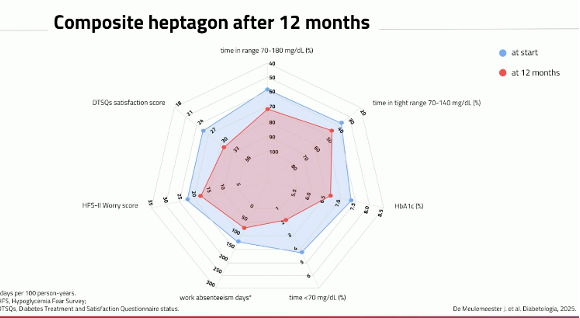
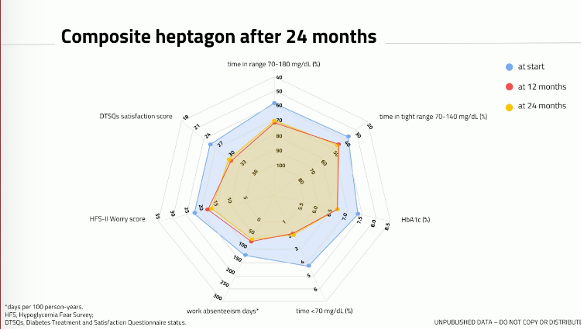
Automation in complexity: MiniMed 780G shows strength in T2D and other populations
At a packed symposium in the 360° Arena, Prof. Ohad Cohen (Medtronic) and Prof. Kirsten Nørgaard (Steno Diabetes Center Copenhagen, Denmark) discussed the expanding role of the MiniMed 780G system in insulin-using T2D with a focus on complex subgroups including chronic kidney disease (CKD) and dialysis. Both presented evidence that automation can deliver substantial glycemic improvements with low hypoglycemia risk, even in highly complex patients.
- Prof. Cohen reviewed both clinical trial and real-world evidence supporting MiniMed 780G use in T2D. In the IMPACT 2 study (n=95), participants saw an 8% improvement in Time in Range (TIR), from 72% to nearly 80%, and reached 51% Time in Tight Range (TITR) with minimal hypoglycemia. Automation from MiniMed 780G provided the majority of insulin corrections (~70%), reducing patient burden. Notably, results were consistent in those also on GLP-1 RAs, suggesting synergistic benefits rather than conflict between the two approaches. Real-world data from over 26,000 users further demonstrated strong glycemic benefits regardless of the phenotype: (i) T2D with high insulin requirements; (ii) T2D with low insulin requirements; and (iii) insulin-resistant T1D. In all cohorts, mean TIR exceed 70% with low rates of hypoglycemia.
- Prof. Nørgaard addressed whether AID systems can help people with T1D or T2D and severe CKD, including those on dialysis. She emphasized the dual challenge in this group: increased insulin resistance drives hyperglycemia while impaired counter-regulation increases a patient’s risk of hypoglycemia. She cited a short-term crossover study of advanced CKD patients in Denmark and Australia, in which TIR increased from ~55%-66% at baseline to 71%-77% with MiniMed 780G use, without a significant increase in hypoglycemia. Prof. Nørgaard also detailed case studies demonstrating the system’s utility across: (i) peritoneal dialysis: auto-corrections helped offset the glucose load from dialysis solutions; (ii) hemodialysis: temporary targets reduced glycemic variability around sessions; and (iii) both T1D and T2D with severe CKD: MiniMed 780G improved glycemic variability while preserving safety, consistently increasing TIR to 70%-75% in these highly complex scenarios.
- Together, the panelists reinforced MiniMed 780G’s potential to significantly improve glycemic outcomes in insulin-using T2D, with evidence from both clinical trials and real-world studies suggesting that the system is feasible, safe, and effective across diverse T2D phenotypes. While broader validation and guidance will be necessary, findings presented in today’s symposium strengthened the case for incorporating 780G use into the management of complex diabetes populations.
Control-IQ in focus: A review of clinical strategies and 2025 OUS software updates
At a Tandem-sponsored presentation in EASD’s “Arena,” Dr. Laurel Messer (Tandem) reviewed the benefits of the Control-IQ algorithm. She focused on the AutoBolus feature, which delivers insulin for predicted or actual hyperglycemia up to once an hour. AutoBolus particularly benefits patients who frequently miss user-initiated boluses, such as adolescents and young adults (ages 14–24, where 51% of boluses are delivered automatically) and those with higher baseline A1cs (≥8.0%, where an average of ≥50% of bolus insulin comes via AutoBolus). Dr. Messer emphasized that glycemic control can improve even with minimal changes to patient behavior when supported by automatically initiated intervention. She also highlighted a single-center, 12-month study of Control-IQ users relying almost entirely on AutoBolus (>90%), which showed a 19% increase in TIR and 1.6% A1c reduction from an undisclosed baseline.
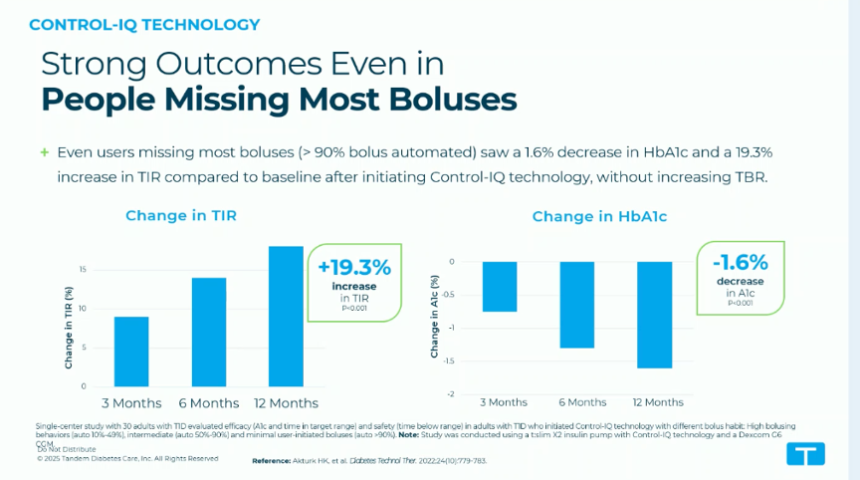
- Targeting clinical application and optimization of the Control-IQ algorithm, Dr. Messer noted that adjusting the correction factor affects basal delivery, user-initiated boluses, and AutoBolus. A retrospective analysis (n=~22,000) showed the most aggressive correction factors were linked to 79% TIR, 14 percentage points higher than with those using the most conservative settings (65%), with no significant difference in hypoglycemia.
- Dr. Messer also highlighted software updates available in 2025 (that vary in timing by market). The t:connect mobile app offers greater discretion by enabling management from a smartphone – the app for iPhone and Android smartphones most recently received Health Canada authorization earlier this month, with launch expected later this year. The mobile bolus control feature has been available in the t:connect app to US users since 2022. We’re eager to learn more about the company’s expected timeline for EU rollout. Dr. Messer also discussed Tandem Source, which will support automatic uploads and streamlined analysis across patients and providers. Key features include: (i) an overview report for trends; (ii) a daily therapy timeline; and (iii) settings review. Tandem Source also adds a copy-as-text function to facilitate the transfer of relevant information into EHR systems. The platform was made available to US providers, caregivers, and patients at the end of 2023.
Medtronic shares clinical pearls for using smart MDI: Improving outcomes and simplifying decision making
Prof. Ohad Cohen (Medtronic), Prof. Goran Petrovski (Medtronic), and Prof. Laurent Crenier (Hôpital Erasme, Belgium) took to the Spotlight Stage to present clinical evidence and case examples for smart MDI, positioning it as a practical and effective step forward for injection users. While AID systems often dominate the conversation in diabetes technology, the session highlighted that smart MDI can meaningfully improve glycemic outcomes and simplify provider decision-making for users that continue to prefer MDI.
- Prof. Petrovski shared unpublished real-world data (n=5,597) from users of the InPen smart MDI system. Over 170 days of follow-up, users achieved a mean GMI of 7.5% and Time in Range (TIR) of 58%. Engagement with notifications was the major driver of success: responding to over 75% of missed-bolus alerts was associated with 68% TIR, while responding to correction alerts pushed TIR up to 72%, all without any increase to hypoglycemia. Longitudinal data in 2,600 users demonstrated that even small behavioral adjustments, such as one extra bolus per week, translated into approximately two more hours per day in Range and a 0.3% decrease in GMI. Together, these data suggest that smart MDI’s impact comes from both tracking and adjusting behavior at critical moments.
- Prof. Crenier offered a provider-facing perspective, showing how smart MDI can enhance injection therapy by revealing previously hidden patterns. He presented a patient case where he treated an individual with longstanding T1D, frequent hypoglycemia, and a fear of bolusing. Smart MDI revealed specific issues with both basal insulin dosing and systematic under-bolusing at meals. Features such as long-acting insulin assessment, which filters AGP data to isolate basal effects, and bolus calculator statistics, which track under-dosing and missed meals, enabled constructive patient-provider conversations. Over four months, these insights resulted in a reduction of GMI from 8.3% to 7.0% with fewer missed boluses and reduced variability, which were the patient’s best results in over a decade. To close, he demonstrated the Smart MDI system setup (see figure below). This feature is designed to be straightforward for HCPs and translates into a simple user experience as well, as the patient only needs to select meal type (low, medium, or high carb) while the system calculates appropriate doses in the background.
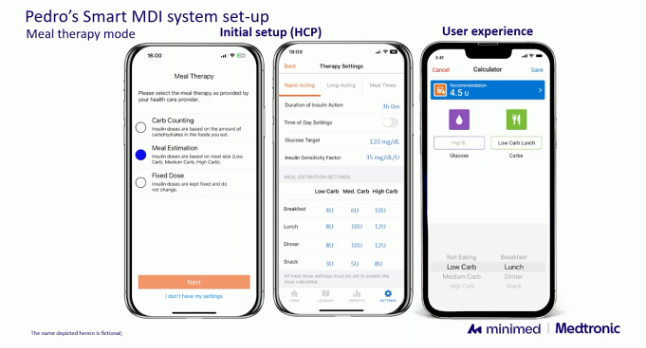
Exercise and AID: Insights from the RAPPID study on hypoglycemia risk
Prof. Bruno Guerci (Lorraine University, France) presented results from the RAPPID study (n=86), which evaluated glycemic management in people with T1D using AID during one month of standard physical activity. Participants were regularly active, engaging in at least two ≥30-minute sessions per week, and had been on AID for at least three months. Researchers advised participants to set a temporary target one hour before activity with hypoglycemia risk and to announce carbohydrates prior to exercise if no temporary target was used. Prof. Guerci said that the RAPPID study has been accepted for open access publication in Diabetes, Obesity, & Metabolism.
- Baseline characteristics. Participants had a mean age of 43 years, diabetes duration of 24 years, and 21% self-reported as athletic. Mean baseline A1c was 6.9%, and mean TIR was 72%, consistent across AID models. Mean AID use duration was 18 months; 45% used MiniMed 780G, 26% used t:slim X2 with Control-IQ, and 26% used mylife YpsoPump.
- Results. A total of 954 physical activity sessions were logged, including 714 with CGM data. Most were aerobic (73%) and endurance-based (75%). Participants averaged 3.2 sessions per week, with a mean session duration of 1.5 hours, totaling 19 hours of physical activity per participant across the study.
- TIR was lowest during exercise and the early recovery period (three hours post-exercise), averaging 69%. These periods also had the greatest Time below Range (TBR; <70 mg/dL), with 4% TBR and 2% Time <54 mg/dL. By the following morning (!), TIR returned to baseline (72%).
- Aerobic activity was associated with greater level 1 hypoglycemia (TBR 5% during and 4% after exercise) and higher level 2 hypoglycemia (Time <54 mg/dL; 2% during and 1% after exercise), compared to no Time <54 mg/dL with anaerobic activity. However, aerobic sessions also achieved higher TIR (71%) than anaerobic sessions (65% during and 68% after exercise). Mixed activity sessions had the highest overall hypoglycemia, largely driven by level 1 hypoglycemia.
- Out of 714 monitored sessions, 281 hypoglycemic values were recorded. Events typically lasted 15-60 minutes, with few exceeding one hour. Nearly 30% of events reached <54 mg/dL and persisted in level 2 hypoglycemia for at least 15 minutes.
Nationwide French data highlight durability and glycemic gains associated with AID use
Dr. Chloe Amouyal (Sorbonne Université, Paris, France) presented results from a real-world French nationwide observatory study evaluating two years of AID use in children and adults who initiated the technology in 2022. All participants had T1D; 28% were children and 56% were female. The mean age was 38 years. Nearly all used either Tandem t:slim X2 with Control-IQ (50%) or MiniMed 780G (49%), the two systems reimbursed nationally at the time of the study.
- Dr. Amouyal described adherence as “excellent,” with 98% still using AID after two years. Most pump discontinuations were temporary, often due to system burden or timing (e.g., summer months might see more pump “vacations” than other seasons). Participants spent a mean 95% of time in automated mode.
- Glycemic outcomes. Mean A1c of 7.7% fell 0.5 percentage points to 7.2% after 24 months. TIR improved from 58% to 69%, up 11 percentage points, driven mainly by a reduction in Time above Range (>180 mg/dL), which fell substantially from 39% to 29%. The proportion of people achieving target TIR >70% more than doubled to 49% from 22%, and those meeting both targets (TIR >70% and <4% Time below Range [<70 mg/dL]) tripled to 42% from 14%. Still, Dr. Amouyal emphasized that fewer than half of participants reached both targets, underscoring the need for greater education on carbohydrate counting and ideally more regular follow-up.
- Complications. Severe hypoglycemic events were also significantly reduced by 24 months, falling from 4% of patients reporting one within the last 12 months to just 1%. DKA incidence remained stable, improving to 0.9% to 1.2% incidence in the previous 12 months.
CamAPS FX and Control-IQ improve glycemia and neonatal outcomes vs. MiniMed 780G in pregnant women with T1D; strong outcomes across all systems
Dr. Carmen Quiros (Hospital Universitari Mútua Terrassa, Spain) presented results from a multicenter observational trial comparing Tandem’s Control-IQ algorithm, Medtronic’s MiniMed 780G system, and CamDiab’s CamAPS FX hybrid closed-loop system in pregnant women with T1D. CamAPS FX had the edge in some glycemic measures and in neonatal outcomes. But the good news is that all three systems delivered A1c <6.5% and TIR above 65% in the third trimester. It seems clear that AID should be the logical choice for pregnancy.
- The trial spanned 27 hospitals in Spain, with AID use starting before 20 weeks of gestation. Participants (n=137) had a mean age of 34 years and diabetes duration of 19 years. Prior to pregnancy, most MiniMed 780G (80%) and Control-IQ (64%) users were already on their respective systems, compared to 37% of CamAPS FX users. In the cohort, n=14 were on Control-IQ systems, n=85 on MiniMed 780G, and n=38 on CamAPS FX.
- Glycemic targets: CamAPS FX users employed lower glucose targets during pregnancy (96 mg/dL, 91 mg/dL, and 87 mg/dL across trimesters) than MiniMed 780G users (103 mg/dL in the first trimester, 100 mg/dL thereafter).
- Control-IQ and CamAPS FX both achieved lower A1c levels than MiniMed 780G in later trimesters; In the second trimester, Control-IQ users had lower median A1c than MiniMed 780G users (~5.4% vs. ~6.2%), while both Control-IQ and CamAPS FX held significantly lower median A1c than MiniMed 780G by the third trimester. Notably, median A1c was <6.5% across all systems and trimesters. Turning to time in range (TIR), the only statistically significant TIR difference between systems occurred in the second trimester, when CamAPS FX users achieved higher TIR than MiniMed 780G (70% vs. 65%). By the third trimester, all systems reached mean TIR ≥70%.
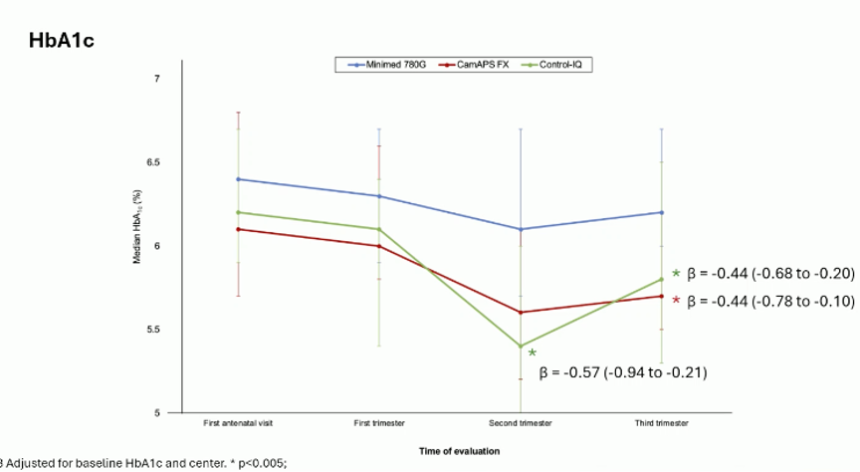
- Maternal and neonatal outcomes: Rates of gestational weight gain, cesarean section, and preeclampsia did not differ by system. Neonatal outcomes, however, favored CamAPS FX: mean birthweight was lower, as were rates of large-for-gestational-age infants (38% vs. 63%), macrosomia (3% vs. 29% and 23% [Control-IQ]), and NICU admission (3% for CamAPS FX and MiniMed 780G vs. 15% with Control-IQ). Adjusted models showed both CamAPS FX and Control-IQ reduced the risk of large-for-gestational-age compared to MiniMed 780G.
Insulet-sponsored symposium emphasizes scalable onboarding strategies and real-world outcomes with Omnipod 5 in T1D
Prof. Pratik Choudhary (University of Leicester, United Kingdom) and Dr. Sandra Schlüter (Hannover Medical School, Germany) shared practical strategies for expanding access to AID systems, drawing on experiences with Omnipod 5 in both group-based and virtual settings. The pair engaged the audience with interactive polling and a case-based discussion, underscoring both the real-world benefits of AID and the logistical challenges of scaling initiation. Speakers repeatedly emphasized one theme throughout the session: given the simplicity of Omnipod 5, healthcare teams can rethink traditional workflows to onboard more patients simultaneously, without compromising safety or outcomes.
- Real-world outcomes mirror trial results, reinforcing Omnipod 5’s impact on both glycemic outcomes and quality of life. Prof. Choudhary and Dr. Schlüter referred to data from the RADIANT trial and compared it to results in their own clinics, showing mean Time in Range (TIR) improvements of >20 percentage points (from ~40% to >60%), with minimal hypoglycemia. They also emphasized the benefits conferred by using Omnipod 5’s optimal settings. In global datasets, patients using lower glucose targets (110 mg/dL) and more aggressive carbohydrate settings achieved median TIR of 74-77%. Prof. Choudhary and Dr. Schlüter also shared patient stories from their own clinics, including an individual with decades of poor management who saw their A1c levels fall from 10% to 6.9% after switching to Omnipod 5, with concurrent and significant quality of life improvements.
- Group-based onboarding approaches have improved access for many patients. In Leicester, the UK, Prof. Choudhary detailed how his team increased annual initiations from ~30 patients to more than 400 by moving sessions out of hospitals and into community centers, starting 20 patients at a time. Additionally, he said that his team was able to successfully scale onboarding by removing several common barriers, including: (i) removing carbohydrate counting; (ii) streamlining settings set-up; and (iii) harnessing cloud-based care to provide “light touch” follow-up support. In a similar vein, Dr. Schlüter said that she implemented smaller-group (four to six patients) sessions paired with structured safety training, peer-to-peer learning, and immediate system start-up. She noticed that peer support has been a powerful driver of sustained success, with some cohorts forming their own WhatsApp groups that continue long after onboarding. While audience polling suggested that only ~20-25% of patients in many European clinics are currently using an AID system, both speakers agreed that systems like Omnipod 5 should be available to all, challenging healthcare providers to now shift their attention to scaling adoption.
INLOOP study: One-year real-world outcomes with Diabeloop DBLG1 show durable glycemic and quality-of-life benefits
Prof. Maria Lytrivi (Université libre de Bruxelles, Belgium) presented results from the prospective INLOOP study that assessed real-world outcomes with Diabeloop’s DBLG1 AID system. The French-based system evaluated in the study consisted of Diabeloop’s DBLG1 algorithm, Roche’s Accu-Chek Insight pump, and the Dexcom G6 CGM. Roche’s Accu-Chek Insight pump uses pre-filled NovoRapid PumpCart cartridges and allows users to set “very low” basal rates (down to 0.2 U/hour). While the AID market in Europe is increasingly competitive, the Diabeloop algorithm – housed in a locked-down handset – has predictive low-glucose suspend, basal rate adjustment automation, automatic correction bolus features, and activity modes for quick adjustments, including ZENmode to temporarily raise target glucose (and ensure no lows). We are curious to see how these positive outcomes with the DBLG1 system will translate to the launch of the next-generation DBLG2 algorithm slated for next year, as well as any potential differences in real-world outcomes for DBLG1 users with ViCentra’s Kaleido patch pump – which is slightly smaller (5 cm x 3.5 cm x 1.25 cm and weighing 15 grams) than Insulet’s Omnipod 5 (5.2 cm x 3.9 cm x 1.45 cm and weighs 26 grams).
- The study enrolled 167 adults with T1D across 12 Belgian centers between May 2022 and September 2023. Participants had a mean age of 44 years, mean diabetes duration of 26 years, and mean BMI of 26 kg/m². In the study, 62% of the participants were female, 96% were CGM users at baseline, and 41% reported microvascular complications.
- Glycemic outcomes significantly improved at four months and were sustained at 12 months. Improvements in TIR were greatest in individuals with lower baseline TIR, higher baseline A1c, pump-naïve status, and higher automated mode use (see figure below).
- TIR improved from 57% at baseline to 70% at four months and was sustained at 69% at one year. The proportion of participants achieving TIR >70% more than doubled over that period, from 18% to 47%.
- Time in Tight Range (TITR; 70-140 mg/dL) rose in line increased meaningfully, though far less than TIR (not surprising given tighter targets), moving from 35% to 42% at one year, or seven percentage points compared to 29 percentage points for TIR, about 4x greater a move.
- Time below Range (TBR; <70 mg/dL) dropped from 3.7% to 1.4%, with 92% achieving the <4% target vs. 52% at baseline. The rate at which hypoglycemia and severe hypoglycemia have diminished in recent years is so gratifying for the field – next is working out how a far higher percentage of people with T1D (and T2D) can have access to AID.
- A1c dropped from 7.6% to 7%, 0.6 percentage points, and, strikingly, the proportion achieving A1c of <7% doubled, from 27% to 54%.
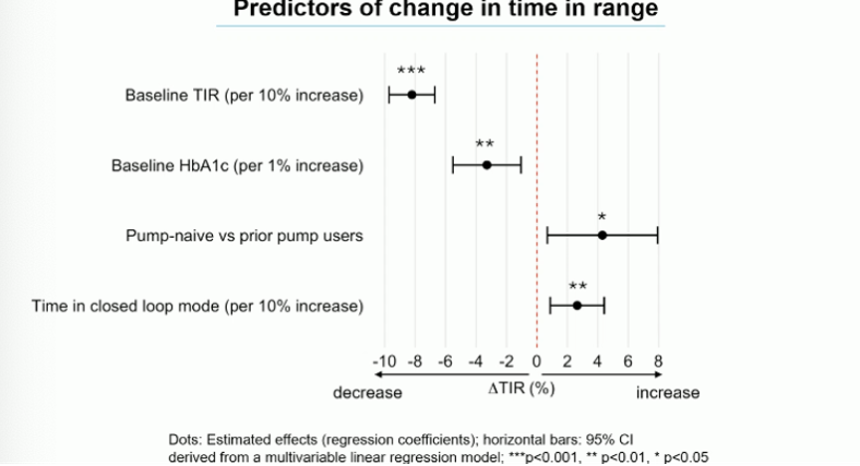
- Quality of life. After one year, participants reported moderate improvements in fear of hypoglycemia, treatment satisfaction, and diabetes impact, alongside small-to-moderate gains in overall problem areas and device satisfaction.
- Safety and discontinuation. Severe hypoglycemia fell markedly, with the proportion of participants affected dropping from 10% to 1% and the event rate declining from 116 to 8.6 per 100 patient-years. Most discontinuations occurred in the first four months (53%), mainly due to technical issues, system complexity, or alarm fatigue.
RADIANT adult sub-analysis (n=79): Omnipod 5 drives significant A1c and TIR gains vs. MDI with CGM, with A1c reaching 7.2% and an extra five-plus hours time “in range”
Prof. Bruno Guerci (University of Lorraine, France) presented an adult sub-analysis of the RADIANT study (n=79), which compared Omnipod 5 to MDI with FreeStyle Libre 2 CGM in people with T1D. The RADIANT trial originally enrolled 188 participants (children and adults) across 19 sites in Belgium, France, and the UK. All participants had ≥one year of T1D diagnosis and ≥three months of MDI with CGM use. After two weeks of baseline data collection, participants were randomized 2:1 to Omnipod 5 (n=125) or MDI with CGM (n=63) for just over three months (13 weeks). Overall, Omnipod 5 drove a 0.8 percentage point greater A1c reduction vs. MDI with CGM (falling from 8.1% to 7.2%; p<0.0001).
- Adult demographics. Adults in the study had a mean age of 40-41 years and a diabetes duration of ~20 years. Interestingly, most Omnipod 5 users selected the lowest glycemic target of 110 mg/dL for 57% throughout the study, and spent 99% of their time in automated mode. The groups were nearly evenly split by sex.
- In the new sub-analysis presented, Prof. Guerci highlighted that adults with higher baseline A1c (≥8.0%) saw a 1.1 percentage point greater treatment-adjusted A1c reduction with Omnipod 5 (falling from 8.7% to 7.5%) vs. MDI with CGM (from 8.6% to 8.5%), which had exactly the same drop in A1c of 0.1 percentage points. He also noted that gains in TIR were driven primarily by reduced rates of hyperglycemia: Omnipod 5 users saw a 23-percentage-point treatment-adjusted reduction in TAR (>180 mg/dL), falling from 57% to 33% compared to an increase from 54% to 56% in the MDI with CGM cohort. Furthermore, Omnipod 5 users experienced a 10-percentage-point reduction in Time >300 mg/dL (falling from 13% to 3.4%; reduction of 2.4 hours/day), whereas MDI with CGM users experienced a two-percentage-point increase (rise from 12% to 14%).
- Consistent with the full RADIANT population, no significant group differences were seen in TBR <70 mg/dL (2% with Omnipod 5 vs. 1.4% in adults using MDI with CGM) or Time <54 mg/dL (0.2% vs. 0.1%, respectively). However, Prof. Guerci noted that more Omnipod 5 users achieved target TBR <4% at 13 weeks (92% vs. 82%, respectively)
- Previously, topline results of the RADIANT trial were presented at ATTD 2025. Participants randomized to Omnipod 5 (n=52) achieved an A1c reduction by 0.9 percentage points (falling from 8.3% to 7.3%), compared to a 0.1 percentage point reduction with MDI with CGM (from 8.2% to 8.1%; n=27) – this A1c change is not only far smaller, but also not close to target. At 13 weeks, adults on Omnipod 5 achieved 65% TIR (up from 41% at baseline), while the MDI with CGM group averaged 42% TIR (down from 43%). This result represented a 23% baseline-adjusted difference, reflecting an increase of 5.6 hours/day spent in TIR.
Big Picture of Diabetes Technology
Novel diabetes subgroup classifications and optimized treatment plans based on glucose variability patterns from CGM data
Dr. Anuj Maheshwari (Hind Institute of Medical Sciences, India) and Dr. Shubhashree Patil (Diabetes and Wellness Clinic, India) presented data from a prospective observational study, identifying optimal treatment plans for five novel diabetes subgroups, classified after two weeks of CGM wear (n=527). The study was driven by the need to improve the personalization of diabetes care, with 40% of treatments failing due to inappropriate medication adherence and 60% of patients with similar A1c showing different glucose patterns. Both presenters said that treatment personalization based on CGM phenotype can reduce the trial-and-error associated with many first-line treatments. Most participants (87%) had already been diagnosed with T2D, and the remaining 13% had T1D diagnoses. Participants completed 14 days of CGM wear and a six-month follow-up evaluation. Almost 75% of patients with T2D were on baseline metformin, and the proposed optimal treatment plans below were considered as adjunct therapies.
- Dr. Maheshwari listed processes for clinical practice. Implementation requires: (i) a 14-day CGM assessment; (ii) automated subgroup classification with machine learning; (iii) clinical treatment selection depending on subgroup classification; and (iv) follow-up monitoring by specified subgroup outcomes. Participants in the subgroups were not randomized to different treatment options.
- The five novel diabetes subgroups and their optimized treatment courses included:
- Stable hyperglycemia (31%). This subgroup was characterized by consistently elevated glucose of 200-300 mg/dL and coefficient of variation (CV) <20%. It was often seen in those with advanced T2D. Dr. Maheshwari explained that the study identified primary treatment include long-acting insulin or high-dose metformin with lifestyle modifications focused on consistent carbohydrate intake. Ongoing monitoring should focus on A1c trends rather than daily variability.
- Postprandial spike (22%). This subgroup was characterized by excessive postprandial glucose excursions and delayed returns to baseline fasting glucose and was especially common in those with early T2D. Dr. Maheshwari emphasized that first-line treatment for those in this subgroup should include GLP-1 RAs, with prandial rapid-acting insulin if needed. Dr. Patil said that those who initiated GLP-1 RAs in this subgroup saw a 32% reduction in glycemic variability, significantly greater than the 9% reduction seen in those who initiated GLP-1 RAs classified to other subgroups (p<0.001).
- Brittle hypoglycemia (18%). Participants had frequent hypoglycemic episodes and glucose CV >35%, as well as unpredictable insulin sensitivity. They often had T1D or “advanced” T2D. Dr. Maheshwari said that optimal treatment for this subgroup should include hybrid closed loop (HCL) pump options. For regions or populations for which the technology is not available or affordable, CGM-guided insulin adjustments with hypoglycemia-aware algorithms should be used. Dr. Patil explained that participants in this subgroup using AID saw a 76% reduction in the number of hypoglycemic events compared to a 34% reduction in events with MDI (p<0.001). She also reported that those on AID had higher mean TIR and self-reported quality of life scores. As a sidenote, we are surprised that “brittle” continues to be used as a term to characterize even a “type” of complication of diabetes, though it is certainly better than characterizing diabetes this way or worse as a noun or as a “type” of diabetes that someone has! (It’s great not to see reference, for example, to “a brittle diabetic” or even “she has brittle diabetes” – etc!)
- Dawn phenomenon (16%). Dr. Maheshwari emphasized that participants with pronounced dawn phenomenon often go unrecognized in clinical care without CGM-based evaluation. He said that the participating clinics preferentially prescribed SGLT-2 inhibitors or intermediate-acting insulin for those in this subgroup. Upon SGLT-2 inhibitor initiation, those in this cohort saw a mean 28% greater reduction in morning hypoglycemia compared to baseline. Dr. Patil added that SGLT-2 inhibitor initiators in this subgroup saw a mean reduction in morning glucose of 63 mg/dL, significantly greater than the 18 mg/dL reduction seen in those classified to other subgroups. While the data was not provided, she said that they also saw stronger A1c reductions and greater differential weight loss of over 1 kg compared to other subgroups.
- Erratic fluctuators (13%). These “difficult-to-manage” participants were characterized by unpredictable glucose patterns throughout the day, with high glycemic variability without clear triggers. Dr. Maheshwari’s comprehensive treatment plan for those in this subgroup included: (i) rt-CGM (which is the only type of CGM used in most geographies, to our knowledge); (ii) combination therapy with “flexible dosing”; (iii) self-management education (presumably many have had this already); and (iv) endocrinologist-directed treatment co-management (presumably many already have this as well).
- Dr. Patil said that the CGM-based classification system by glycemic patterns predicted hospitalization risk significantly higher rates than traditional predictors including A1c, disease duration, and known risk factors (AUC ROC 0.83 vs. 0.67, respectively; p<0.001). Dr. Maheshwari reported a 35% improvement in treatment response rates, 45% reduction in medication changes, and 60% increase in patient treatment satisfaction. Furthermore, she said that treatment adherence increased from 73% to 89% and that the time to optimal therapy reportedly decreased with use of the CGM-based classification system. A multi-center study across 15 countries is currently planned (n=2,500) to validate these findings and help determine if participants may change subgroups with long-term treatment.
A look to the FDA’s iCGM requirements: Evolving the minimum expectations for CGM market authorization in the EU
At a busy afternoon symposium on EASD’s Spotlight Stage, Prof. Concetta Irace (University Magna Graecia, Italy), Prof. Peter Adolfsson (University of Gothenburg, Sweden), and Prof. Stefano Del Prato (Sant’Anna School of Advanced Studies, Italy) called for higher minimum standards for CGM market authorization in Europe. Prof. Irace reviewed the EU’s regulatory landscape under the MDR, Prof. Adolfsson critiqued the overreliance on mean absolute relative difference (MARD) as an accuracy metric, and Prof. Del Prato urged adoption of more rigorous, clinically meaningful performance expectations aligned with other regulatory bodies’ standards and recent recommendations from an expert panel.
- Prof. Irace described the current state of CGM authorization in Europe. She outlined the “profound transformation” from the Medical Device Directive (MDD) to the Medical Device Regulation (MDR). Key changes included: (i) the application of MDR as guidelines across all EU countries, unlike the MDD directive; (ii) the requirement of clinical and preclinical studies; and (iii) obligatory post-market surveillance. She also emphasized MDR’s goals to improve patient safety evaluation, transparency, traceability, and harmonization. CGM authorization in the EU today goes through notified bodies, which audit manufacturers and review technical documentation, clinical evaluations, and post-market plans. Expert panels (including two specialists in endocrinology/diabetes) can issue opinions, though these are nonbinding. Notably, unlike the FDA, EU expert panels do not include patients — something Prof. Tadej Battelino (University Medical Center Ljubljana, Slovenia) noted could help build trust. Technical documentation must now cover device description, risk management, safety/performance data, clinical evidence (which can include published literature on other devices to prove their general role of the device in the patient population), and post-market surveillance/clinical follow-up (PMS/PMCF). However, clinicians still lack access to all device technical details, leading to opacity in these approval pathways.
- Prof. Adolfsson added that EU standards rely too heavily on MARD. He described “CGM-MARD doping,” where companies can manipulate results to show MARD <10.0% by: (i) testing in easier-to-manage populations (T2D or non-diabetes rather than T1D); (ii) selecting favorable sensor batches or days; or (iii) using clamp studies that underestimate real-life glucose variability. He stressed that accuracy cannot be judged on MARD alone; how data are generated matters.
- Prof. Del Prato called for stricter, clinically meaningful requirements, pointing to FDA standards that demand robust accuracy data in the intended population across the full glucose range. He highlighted that the EUDF recently convened experts to develop recommendations, concluding with a strong call to action: Europe must not lag behind global standards and should pursue international harmonization to safeguard patients and maintain trust in CGMs. Ultimately, he endorsed proposals for new requirements in EU CGM market authorization (eCGM) and additional CE-Mark safeguards that were published in March.
Defining provider roles in diabetes technology: The University of Leicester’s four-level competency framework
In a morning session chaired by Ms. Laura Willcocks (Leicester General Hospital, UK), Ms. Erica Richardson (Leicester Diabetes Centre, UK) and Prof. Pratik Choudhary (University of Leicester, UK) presented the University of Leicester’s new diabetes technology competency framework. Designed to clarify “who should know what about technology” in a healthcare system, the framework aims to expand CGM and AID adoption, streamline provider roles, and improve equity and patient experience. It was developed with input from diabetes nurses, clinicians, audits of current knowledge, and patient/advocate feedback. Ms. Richardson emphasized that maintaining competencies requires ongoing education to keep pace with rapid innovation.
- Level 1: Awareness. Any HCP or support worker who may not be primarily working in diabetes but encounters people with diabetes who are using diabetes technologies should have basic awareness of diabetes technology. Given that ~30% of hospitalized patients have diabetes, and an estimated half use technology, Prof. Choudhary stressed the importance of this level. Providers should: (i) be able to recognize insulin pumps and sensors; (ii) distinguish between the two conceptually and visually; (iii) know how to respond to emergencies or device errors; and (iv) identify who might benefit. Ms. Richardson suggested resources such as flyers, posters, short videos, and seminars.
- Level 2: Competence. These providers may be primary care providers, general endocrinologists, nurses/dieticians, or educators who work within diabetes but are not specialized in diabetes technology. They see a broad range of people with diabetes and need to guide patients around their use of technology. Hospital departments can support them through training days, online modules, or facilitating access to industry or academic sessions. According to Prof. Choudhary, those in Level 2 should: (i) be able to differentiate between the CGM and pump system offerings; (ii) understand common causes of low TIR and hypoglycemia and how to address them; and (iii) offer general advice, such as managing exercise-related hypoglycemia.
- Level 3: Expertise. Ms. Richardson explained that those in Level 3 are likely experts in diabetes technology and spend a large proportion of their time seeing people who use diabetes technology, They may support people in their team who are at Level 2, such as doctors or nurses specifically offering insulin pump services. These trainings will often include hands-on components on the specific devices. Prof. Choudhary said that these experts should be able to: (i) onboard patients to pumps; (ii) understand how algorithms function; (iii) adjust system settings; and (iv) manage complex cases (for example, high A1c, frequent hypoglycemia, and complications). Level 3 providers typically take over care from Level 2 for tailored guidance.
- Level 4:Leadership. Prof. Choudhary explained that those in Level 4 are often leads for T1D services or senior diabetes specialists responsible for educational development across the team. Ms. Richardson said that they are not only expected to demonstrate expert levels of knowledge and skills in complex situations to support all team members, but also help identify training resources and engage in national forums and conferences to share new insights.
EASD Expert Session with Prof. Sabine Hofer and Dr. Amit Gupta: Education, reimbursement, and safety remain central to diabetes technology adoption across global settings
At EASD’s Expert Session on Technology, Prof. Sabine Hofer (Medical University of Innsbruck, Austria) and Dr. Amit Gupta (Chair, IDF School of Diabetes and Education Committee) addressed wide-ranging questions in a highly interactive Q&A moderated by Prof. Julia Mader (Medical University of Graz, Austria). Themes spanned technology access barriers, pediatric CGM adoption, device accuracy, challenges of use, and the role of evolving metrics in guiding care.
- Access and reimbursement remain major barriers in low- and middle-income countries (LMICs), while reimbursement enables near-universal uptake in nations such as Austria. Dr. Gupta emphasized that although CGM and AID are available in India, uptake is limited by three persistent barriers: (i) out-of-pocket costs; (ii) lack of reimbursement; and (iii) insufficient provider education. He noted that patients bear the cost of both devices and physician training. By contrast, Prof. Hofer described Austria’s unique position, where reimbursement is provided for nearly all children and adolescents with T1D. This has enabled over 90% CGM uptake and over 70% hybrid closed-loop system (HCL) use. Registry data covering approximately 80-85% of the pediatric population confirming sustained high penetration.
- Education is essential for successful technology adoption, patient safety, and trust. Throughout the session, Dr. Gupta repeatedly returned to the need for robust education for HCPs, patients, and caregivers alike, both to facilitate device onboarding and to prevent distress. He cautioned against blind trust in CGMs, noting that false lows or highs may represent either technical errors or true dysglycemia, and emphasized the need to train providers to cross-check with BGM and look for clinical signs of dysglycemia. Prof. Hofer similarly noted that education must extend to families, schools, and caregivers, particularly in pediatrics. In this population, stigma, screen-time concerns, and restrictions on phone use within schools present unique challenges.
- Metrics are evolving, but panelists believe both A1c and TIR remain complementary and essential. Addressing whether TIR could replace A1c, Dr. Gupta pointed to Dr. Tadej Battelino’s perspective that TIR and Time in Tight Range (TITR) are increasingly important but argued that A1c and TIR capture distinct aspects of glycemia. Prof. Hofer agreed, citing specific limitations of A1c in patients with anemia and hemoglobinopathies and noting that TIR’s intuitive color-coded “traffic-light” system is especially useful in pediatrics. Both panelists underscored the importance of using metrics in complement to one another rather than substitution.
- Complex populations illustrate the limits of current evidence. Both experts discussed nuanced cases where evidence is thin and guidelines are lacking. Prof. Hofer described off-label CGM use in neonates that requires meticulous site preparation and skin protection – further development of best practices remains necessary. She also highlighted the promising potential of continuous ketone monitoring for pediatrics once these devices become available. Dr. Gupta noted accuracy challenges for patients on dialysis and at high altitudes, where a glucose oxidase-based meter may be impacted by decreased oxygen tension. The panel agreed that CGM use in children with obesity or prediabetes remains an open question with insufficient data to define cutoff values for intervention – this, and other aspects of diabetes technology, will continue to evolve.
The diaTribe Foundation 19th Annual Diabetes Forum
Building the future of diabetes care: Prof. Tadej Battelino receives diaTribe Solvable Problems’ Vanguard Leadership Award
diaTribe held its Solvable Problems event at the unique Mirage venue steps away from Vienna’s Messe Wien Congress Center. Prof. Chantal Mathieu (KU Leuven, Belgium) presented the Vanguard Leadership in Diabetes Award to Prof. Tadej Battelino (University of Ljubljana, Slovenia). She explained that the award is given to bold leaders who don’t just imagine a better future, but those who build it – “an award written for Tadej”. Prof. Mathieu characterized Prof. Battelino as a trailblazer in diabetes care globally, combining exceptional clinical and research expertise with an empathy and warmth (and intensity!) that places patients at the center of everything he does. From speaking with children presenting in DKA to supporting the new parents of a child recently diagnosed with T1D, Prof. Battelino is well-known for understanding the human side of this condition as deeply as the scientific. Prof. Mathieu also emphasized his role in advancing novel technologies, first for T1D and now for all people with diabetes. His work on novel CGM metrics has shaped the field — Time in Range, for example, is now a central and intuitive measure for young people thanks in large part to his work, she said. As a clinician, researcher, and friend, Prof. Mathieu presented the Vanguard Award to someone committed to solving problems, proposing solutions, and inspiring those around him.
- In accepting the award, Prof. Battelino reflected on his journey as a testament to dedication, mentorship, and vision. Raised with a strong work ethic and fortunate to learn from exceptional teachers, he credited mentors like Dr. Rich Bergenstal (International Diabetes Center) for shaping his critical thinking in diabetes care, as well as patients themselves for teaching him that the most meaningful progress comes from listening to those living with the condition. Alongside collaborators like Prof. Moshe Phillip (Schneider Children's Medical Center, Israel) and Prof. Thomas Danne (Breakthrough T1D), he has continually dreamed big — believing in the possibility of a cure while working to advance advocacy and regulatory progress in Europe. Whether through advocacy, mentoring colleagues, or celebrating the successes of the community, Prof. Battelino exemplifies visionary, human-centered, and transformative leadership, reminding us that in advancing diabetes care, it doesn’t matter who “wins” — we all win together.
Big Picture and Additional Topics
Vienna welcomes nearly 11,500 participants with diabetes posters spotted in airport, buildings, and subways
We arrived in Vienna along with over ten thousand participants, who will be engaging in clinical and scientific discussions that shape the future of diabetes management. As we were settling in, we were pleasantly surprised to find multiple posters and ads about diabetes pop up across the city. From the baggage claim area at Vienna Airport, we saw Sanofi’s ad raising awareness about T1D screening and Novo Nordisk on obesity as a chronic disease. In the city, the subway trains had Lilly’s ad asking, “Was, wenn der körper selbst das abnehmen verhindert?” (“What if the body itself prevents weight loss” in German). In Stephansplatz, right next to the St. Stephen’s Cathedral, built in 1578 CE, Roche’s wide poster showcases Accu-Chek with a saying, “Glucose High and Lows.” Even apps, like Uber, has ads from diabetes companies, too! We are excited that diabetes therapies and technologies are gaining attention amid EASD 2025.
Prof. Chantal Mathieu delivers most-valuable EASD Presidential Address, extolling vision for personalized, global diabetes care
Opening the 61st EASD Annual Meeting, Prof. Chantal Mathieu (UZ Leuven, Belgium) set the tone for the week with a wide-ranging Presidential Address that both celebrated the growth of EASD and set an ambitious agenda for the future. She welcomed over 13,500 participants and pointed to a record 2,170 abstracts submitted, with 1,354 accepted and over 1,900 presentations scheduled across the next five days. Describing the program as a “feast of science,” she emphasized that the meeting would span topics ranging from disease insights and treatment advances to disease modification, late-breaking clinical trial results, and implementation research.
- “Rethinking diabetes” and an emphasis on precision medicine framed the scientific agenda. Prof. Mathieu urged the field to move beyond the rigid labels of T1D and T2D and instead view diabetes as a spectrum. Citing a recent Diabetologia publication on T1D heterogeneity, she emphasized that variability exists across all forms of diabetes. She highlighted the importance of diagnosing the individual rather than the type, pointing to precision medicine as the future of care. In her vision, the next era of diabetes care will be defined by individualized types and personalized treatment pathways.
- New initiatives reflect EASD’s ongoing investment in education, publishing, and global engagement. Prof. Mathieu introduced innovations such as “lab talks,” offering behind-the-scenes perspectives from leading researchers, and emphasized preparing the next generation through expanding the Early Career Academy. She announced new training opportunities including EASD’s first immunology course and a continuation of the technology school program to equip clinicians for immunology-based disease-modifying therapies. Prof. Mathieu also celebrated Diabetologia’s60th anniversary, while introducing Metabologia, a new open-access sister journal extending into obesity, complications, and immunology. Globally, she discussed the newly established Global Council and the Global Impact Prize, while commending the European Diabetes Forum (EUDF) under Prof. Stefano Del Prato’s (University of Pisa, Italy) leadership for elevating diabetes policy discussions across Europe.
- She underscored that the implementation of findings remains a central challenge for the field. Prof. Mathieu cautioned that research without translation will not demonstrate effective impact over time. She cited the upcoming release of the EASD’s first-ever guideline on diabetes distress as an actionable step toward bridging evidence and clinical practice. Developed in response to clinician input and the voices of people with diabetes, the guideline addresses an overlooked but critical need and hopes to inspire the publication of future implementation-focused guidelines
- Closing her presidency, Prof. Mathieu reflected on her term with gratitude and hope. She thanked colleagues, staff, and the executive board, announcing that Prof. Francesco Giorgino (University of Bari Aldo Moro, Italy) will succeed her as President of EASD in 2026. She finished with a message of hope: wishing the diabetes community not only good health, but also a peaceful world as EASD looks ahead to its next chapter. Prof. Mathieu has long been a trusted and thoughtful voice in the field – one whose commentary we have frequently sought on a range of topics. She will be deeply missed as EASD President, and we look forward to following her continued impact on the field. We also are eager to see what comes next as Prof. Giorgino assumes the role in 2026.
Under promise and over deliver: Dr. Dan Drucker on his philosophy for scientific research
In the first of eight “Lab Talks” at EASD this week, Dr. Dan Drucker (University of Toronto) shared his philosophy on research, emphasizing the importance of reproducibility. As background, Lab Talks are brand new to EASD this year and offer attendees the rare and valuable opportunity to hear esteemed lab heads share their perspectives on research and ask questions. There are two sessions daily — see below and here for the full list of speakers.
- Reproducibility in research: Creating a definition. Dr. Drucker highlighted that there are multiple ways to approach reproducibility in research. While it’s important to see whether other labs can reproduce a study’s findings, Dr. Drucker maintained that it’s more important that the original researcher is able to repeat their own findings. As for methods, Dr. Drucker felt that there is ultimately no “right” or “wrong” way to reproduce results, whether that’s using one of the many types of animal models available, human subjects, or other ways. The key for researchers, he said, is to define what reproducibility means to them. This can vary, which Dr. Drucker highlighted with a hockey analogy. In the Canadian NHL playoffs, the first team to win four of seven games is deemed the winner. Everyone accepts this, and no questions are asked. He then asked the audience whether this would apply to research (i.e., if you conduct an experiment seven times and get it right four of those times, does it work?). He said there is no right or wrong answer, but rather a philosophical issue and a matter of definition. For Dr. Drucker, reproducibility means producing the same findings every single time.
- Addressing the reproducibility crisis through a look within. Dr. Drucker pointed out the enormous pressure researchers and trainees now face to have impressive stories and publications in high profile journals. He said, “Honestly for me, that’s hard to do,” and instead shared that he prefers more “careful, small, and incremental” science, words which he said often appear in reviewer comments when a paper is rejected. The pressure to produce novel and appealing research has created a reproducibility crisis, and Dr. Drucker called on the audience to look internally (i.e., the researchers themselves) for the source of this crisis. Media releases for research studies can sometimes overhype and exaggerate findings, creating false hope and inflated expectations (e.g., “I just read that they’ve cured…”). He said that his lab tries not to feed into the hype, pointing out to audience members that they likely would not be able to find any press releases from the Drucker lab related to its involvement in discovering DPP-4 inhibitors or GLP-1 RAs, among others. His philosophy for scientific research, he said, is to under promise and over deliver.
- “Trust but verify.” Dr. Drucker and his lab have done extensive work on localizing the GLP-1 receptor, and he said that 80-90% of papers that describe attempts to localize the receptor are “flat out wrong” because the researchers did not take the time to validate the reagents used in the study. He said that many reagents (e.g., antibodies) researchers purchase to use in studies are allegedly trustworthy but not truly so, adding that some reagents being used in these localization studies are “useless” and still being used to publish papers in major journals.
- Publications: A tale of the tortoise and the hare. On publishing research in journals, Dr. Drucker said that while it is good to aspire to publish in top journals, at the end of the day, one can get just as far, if not farther, by publishing high-quality papers in “solid” journals. He showed how many of his major papers early on were all published in PNAS (PNAS currently has an impact factor of 9.1, while the Lancet’s is 88.5 and NEJM’s is 78.5).
- Industry funding and relationships. As Dr. Drucker summarized in the slide below, there are advantages and disadvantages to working with industry on research. In his case, he said that the benefits outweighed the risks, especially as government funding for scientific and medical research is less robust in Canada where he is based.
EASD draft guidelines aim to bring diabetes distress assessment and management into routine care
Closing out the third day of EASD 2025, an impassioned panel discussed EASD’s draft clinical practice guidance on assessing and managing diabetes distress in T1D and T2D. Prof. Jane Speight (ACBRD, Australia) explained that diabetes distress — distinct from depression — is the emotional burden of living with diabetes. It is highly prevalent: nearly one-third of people with diabetes experience it at any given time, half will experience it within a 9–18 month timeframe, and ~80% report at least one problem area at any given time. Diabetes distress is linked to lower self-care, reduced quality of life, and poorer glycemic outcomes. The draft guidelines aim to ensure diabetes distress is no longer overlooked, offering clarity on how to recognize and manage it in routine practice. Dr. Richard Holt (University of Southampton, UK) added that the guidelines are expected to be published in 1Q26.
- Setting the tone, Ms. Michelle Law, a person with diabetes, described diabetes distress as “a negative soundtrack in your head that can get very loud.” After years of intensive management to prepare for pregnancy, she hit a wall — “no short-term goals, just the distant threat of complications. Not inspiring, just frightening.” She emphasized that these guidelines could finally create space in clinical care to talk about the challenges of diabetes, space she had previously felt uncomfortable claiming.
- Dr. Thomas Karagiannis (Aristotle University of Thessaloniki, Greece) outlined the guideline development process, which followed EASD’s SOPs for clinical practice guidelines and the GRADE methodology. The guidelines will undergo multi-stage review process and Dr. Holt noted that the public comment period will be open through October 31, 2025. Eight questions on assessment generated eight Good Practice Statements, while six questions on management produced nine GRADE recommendations each for T1D and T2D. Evidence was drawn from realist review syntheses (King’s College London) and a systematic review/meta-analysis (Amsterdam UMC).
- Prof. Jackie Sturt (King’s College London, UK) presented the eight Good Practice Statements for assessment, including:
- Discussing the emotional side of diabetes at every consultation to acknowledge open conversation as an important tool for emotional and physical well-being and prompting reflection of unmet needs to enable early intervention.
- Asking open-ended questions about distress.
- Using validated tools to identify and monitor specific sources of distress to enable the identification of specific experiences and sources of diabetes distress, directing consultations towards issues important to the person, consistency in clinical assessments, and appropriate scoring and clinical interpretation.
- Assessing and monitoring diabetes distress at regular intervals.
- Validating experiences regardless of score to ensure that their experiences and emotional responses are validated and appropriately considered.
- Recording findings in clinical notes.
- Jointly planning next steps when distress is identified.
- Competently offering psychological support to those experiencing diabetes distress and enlisting specialist support when needed.
- Finally, Dr. Karin Kanc (Diabetes&Me, Slovenia) reviewed recommendations for management, stressing that while HCPs focus on medical and technological interventions, they may underestimate the emotional toll of diabetes. Selected recommendations include:
- For T1D: Use psychological interventions in addition to usual care (Recommendation 1.1; GRADE: Low); use CGM rather than BGM to reduce distress, an acceptable alternative despite CGM’s associated alarm fatigue and data overload (Recommendation 1.8; GRADE: Moderate); do not suggest AID use specifically to reduce distress (Recommendation 1.9; GRADE: Moderate). Dr. Kanc clarified that Recommendation 1.9 does not account for the glycemic benefits seen with AID systems and should not be considered a comprehensive view of its risk-benefit profile – rather, providers should encourage AID use when the patient would otherwise be recommended, and not for the management of diabetes burden alone.
- For T2D: Use psychological interventions (Recommendation 2.1; GRADE: Very Low), psychoeducational interventions (Recommendation 2.2; GRADE: Very Low), and educational interventions (Recommendation 2.3; GRADE: Low) in addition to usual care, all associated with small-to-moderate improvements and no harm.
Global analysis finds that diabetes is the largest contributor to sugar-sweetened beverage-related deaths
Prof. Chang Liu (Capital Medical University, China) presented findings from a global analysis assessing the impact of sugar-sweetened beverages on diabetes and cardiovascular disease burden. As background, sugar-sweetened beverage (SSB) intake increased by 16% between 1990 and 2018. High-risk populations include younger adults globally and adults from the Middle East and North Africa. Recent estimates suggest that SSB have contributed to 2.2 million new T2D cases and 1.2 million new CVD cases.
- Methods. Data were sourced from the Global Burden of Disease study, which offers morbidity and mortality data for over 200 countries and territories from 1990 to 2021. The present analysis examined SSB-attributable deaths and disease burden (CKD, diabetes, ischemic heart disease, and stroke) from 1990 to 2021, plus a 30-year projection (2022 to 2051). Findings were additionally stratified by age, sex, and geographic regions, among others. Sugar-sweetened beverages included in the analysis included carbonated and non-carbonated soft drinks, sports drinks, energy drinks, and sweetened waters, but excluded 100% fruit and vegetable juices.
- Results from 1990 to 2021. The number of SSB-attributable deaths increased by 174% from 1990 to 2021 (from 27,286 to 74,657). Additionally, the age-standardized death rate (ASDR) increased from 0.78 to 0.89 per 100,000, and the average annual percent change (AAPC) in deaths was +0.46%. While deaths were more common among females, death rates are now higher in males (AAPC: 0.71% in males vs. 0.22% in females). By age groups, deaths were more common among older populations; however, deaths rates are higher among young and middle-aged adults. By region, deaths rates are highest in the Caribbean and Central America and most rapidly growing in the Middle East and Southeast Asia. Northern Europe has the lowest SSB-attributable death rate.
- By disease, diabetes was the largest contributor to SSB-attributable deaths. From 1990 to 2021, the number of deaths increased by 205% (from 17,652 to 53,898), and ASDR increased from 0.49 to 0.64 per 100,000, for an AAPC of +0.85%. Meanwhile, the analyses revealed declining death rates for SSB-attributable deaths related to ischemic heart disease and stroke. However, when stratified by age groups, the absolute number of deaths increased sharply among younger adults from 1990 to 2021. Indeed, higher death rates were found in younger birth cohorts at the same age. For example, death rates for 25-year-old individuals born in 1965 and 1995 were 0.047 and 0.069 per 100,000, respectively, a 47% increase.
- Projections for 2022 to 2051. The overall ASDR is projected to reach 1.69 per 100,000 by 2051, with the most dramatic increases expected in younger age groups, particularly those aged 25-29. In this age group, SSB-attributable deaths related to strokes are projected to increase by 400%. For CKD, diabetes, and ischemic heart disease, that figure is 169%, 73%, and 62%, respectively.
Risk factors for severe hypoglycemia in older adults: Insights from the iNPHORM study
Dr. Alexandria Ratzki-Leewing (University of Maryland) presented a secondary analysis (n=310) of the iNPHORM study evaluating risk factors in T1D and insulin-treated T2D for level 3 hypoglycemia – severe hypoglycemia requiring intervention. Participants had a mean age of 68 years and a mean diabetes duration of 16 years; most had T2D (91%), and 46% were female. Overall, 20% of participants reported at least one level 3 hypoglycemic event within the previous 12 months, with an incidence rate of one episode per year. Baseline A1c, age, and the number of prior severe events were not predictive. Instead, three risk factors emerged:
- Women were 2.5 times more likely to experience severe hypoglycemia;
- Those with greater numbers of diabetes complications[1] were 2.1 times more likely to experience severe hypoglycemia; and
- Those with at least one year of CGM use were 5.7 times more likely to experience severe hypoglycemia.
Commenting on this interesting finding, Dr. Ratzki-Leewing noted that reverse causality was possible in the elevated risk ratio with long-term CGM use, in that those with CGM would be more likely to document hypoglycemic events. She added that the study was conducted in 2020, when CGM uptake began accelerating. As iNPHORM harnessed real-world data, CGM initiation was not necessarily accompanied by education programs, and she wondered if fear of hyperglycemia among the older adult population and the ability to closely monitor glycemic trends with CGM contributed to the higher risk of hypoglycemia with longer CGM use. Dr. Ratzki-Leewing concluded that level 3 hypoglycemia is common among older adults with diabetes and driven by diverse risk factors, underscoring the need for tailored strategies — particularly improved education — to reduce the burden of severe events.
Systematic analysis of the Global Burden of Disease reports major large-scale findings on prediabetes prevalence from 1990 to 2023
In an oral session, Dr. Yvonne Xu (University of Washington) presented findings from a systematic analysis of the Global Burden of Disease (GBD) study – while this study has been presented many times, such as in 2010, 2017, and beyond, it was first presented in 1993, reporting on the first work on it from 1990. The global consortium of reserachers working on it now extends beyond 12,000. Music to our ears, Dr. Xu emphasized the importance of identifying prediabetes, as it represents a key population at high risk of diabetes progression, CVD, and all-cause mortality. The current global estimate by the IDF found that less than one-third of countries have relevant data on prediabetes. Furthermore, limitations include unstandardized definitions of glucose tests and diagnostic values. While the GBD studies trends for 365 diseases and nearly 100 risk factors (e.g., T1D and T2D), they don’t have an estimate for prediabetes. Therefore, this systematic analysis sought to provide a large-scale analysis to estimate the prevalence of prediabetes by sex, age, and location from 1990 to 2023.
- Fasting plasma glucose (FPG) to model prediabetes prevalence. The systematic analysis estimated the prevalence of prediabetes by modeling the population distribution of FPG. Researchers input data, representing 163 regions of mean and individual FPG levels, to determine parameters for the distribution. FPG distributions were generated for each location by sex, age, and year.
- Prevalence of prediabetes. The study found an estimated 14% global prevalence of prediabetes, which represents 674 million people. The highest prevalence of prediabetes was found in Puerto Rico (31%) and the lowest in Rwanda (3%). The countries with the highest contributing cases of prediabetes included China (177 million), India (114 million), US (36 million), Brazil (31 million), and Japan (23 million). The highest increases in the number of cases were seen in North Africa and the Middle East.
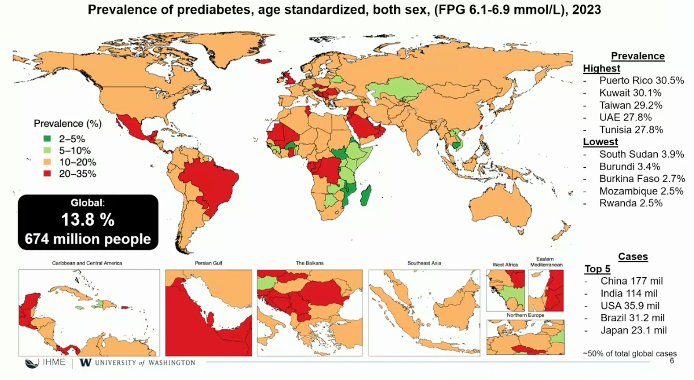
- Global age and sex patterns. The study found a similar prevalence of prediabetes (14%) by sex in 2023, and the distribution by age patterns for both sexes showed the highest prevalence of prediabetes in the age group 50 to 59. Between 1990 and 2023, age-standardized prevalence for both sexes increased by 23%. The highest prevalence of prediabetes was in people under 45, and there were no changes or only small changes from ages 55 to 80. Dr. Xu clarified that this observation indicates the rapid transition from prediabetes to diabetes.
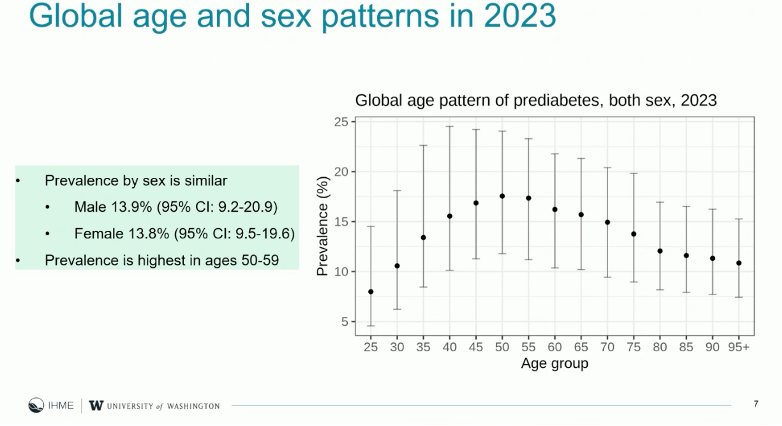
- Global prediabetes based on different FPG ranges. The study looked at age-standardized prevalence for both sexes based on different FPG ranges. The global prevalence of prediabetes was 14% (674 million people) based on the WHO criteria (6.1-6.9 mmol/L) and 27% (1.3 billion people) based on the ADA standard (5.6-6.9 mmol/L).
- Strengths and limitations of the study. Dr. Xu said that the strengths of the study include high data coverage across time, age, and location. As well, she commented on the benefits of estimating prevalence across various FPG ranges, along with the wide range of data and measurements. Some limitations of the study include that the study didn’t account for prediabetes, defined by OGTT or A1c. Furthermore, Dr. Xu raised concern that distributions from population mean FPG values may be sensitive to clusters of high FPG observations from the population from undiagnosed, untreated, and unmanaged diabetes.
- Future implications. Dr. Xu emphasized that this study represents a comprehensive report on the prevalence of prediabetes. The results are significant, especially as the number of cases was found to be similar to global CVD cases in 2023 (627 million), and therefore, represents a public health concern that needs to be addressed. Based on these findings, she encouraged global screening guidelines for the identification of high-risk populations. Furthermore, she urged the audience to consider interventions and policies to ensure populations are equipped with necessary resources, especially in regions with rapid growth of prediabetes.
Rethinking A1c: Genetics, aging, and CGM differences challenge the “one-size-fits-all”
Prof. Inês Barroso (University of Exeter Medical School, UK), Prof. Astrid Petersmann (University Medicine Oldenburg, Germany), and Prof. Guido Freckmann (Institute of Diabetes Technology GmbH, Germany) explored why the field should move beyond A1c levels alone. Their talks highlighted the influence of genetics, age, and emerging CGM metrics, which in conjunction warrant the refinement of current A1c thresholds for more equitable and accurate diagnosis that is applicable to diverse populations.
- Genetic variation can bias A1c readings, delaying diagnosis in high-risk groups. Prof. Barroso showed how non-glycemic factors, including ancestry, sex, and genetic variants, can substantially alter A1c values for a given glucose level. She pointed to G6PD deficiency (prevalent in one-in-seven Black men and 1-in-63 Asian men in the UK), which results in shorter red blood cell lifespan and produces A1c values approximately 10 mmol (~3.1%) lower than expected. Notably, this generates a four-year average delay in diabetes diagnosis in these groups, compounding already elevated risks for T2D and complications. Similar effects were described for PIEZO1 variants in South Asians, which tend to lower A1c levels without improving overall glycemic management. Prof. Barroso cautioned that reliance on A1c metrics alone risks systematic underdiagnosis and undertreatment in these affected populations, with downstream increases in the prevalence of microvascular complications like retinopathy. She proposed the eventual implementation of genotype-adjusted A1c thresholds, though this approach poses practical challenges.
- Age-related increases in A1c may also require revised diagnostic cut-offs. Prof. Petersmann presented evidence from large population studies, including the Framingham Offspring Study (n=2,473), SIGT (n=1,573), and German SHIP cohorts (n=2,973). These showed consistent age-related A1c increases in people without diabetes by approximately 0.07-0.09% per decade. While the analytic precision of A1c measurement has improved significantly in recent decades, she emphasized that the “one-size-fits-all” diagnostic limits fail to account for physiologic age effects. Prof. Petersmann called for robust population-based reference data, stratified by age, that could refine diagnostic cut-offs.
- CGM integration could complement A1c measures but requires standardization. Prof. Freckmann argued that while A1c remains a valuable standardized tool, it fails to determine short-term variability and transient hyperglycemia. With over 80% of people with T1D and a growing number of T2D patients now using CGM, real-world data offer opportunities to complement A1c with metrics such as TIR and GMI. However, he cautioned that CGM is currently designed for therapy, rather than diagnosis, and lacks international standardization, with different devices yielding systematically different results, as shown below. Early consensus efforts by IFCC and EASD working groups are currently underway to establish uniform CGM-derived metrics for potential diagnostic use. Prof. Freckmann concluded that while A1c will remain irreplaceable, pairing it with standardized CGM outputs could potentially provide a more individualized and accurate diagnostic framework.
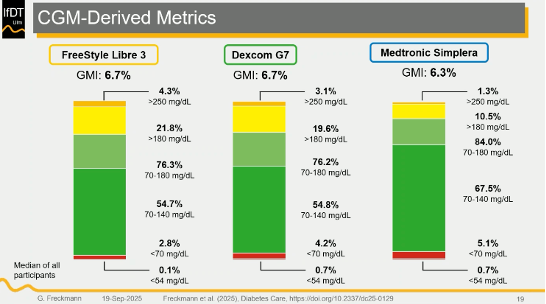
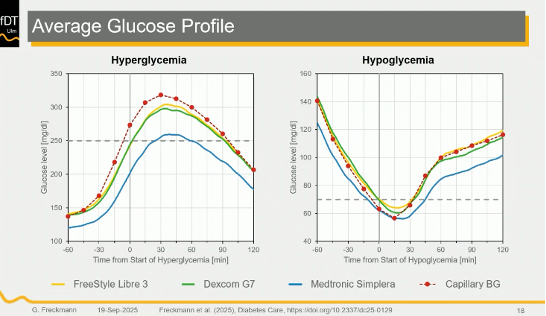
New insights in glycemic management: Sleep duration, pregnancy, and a head-to-head comparison of three CGMs during exercise
Prof. Anna Duda-Sobczak (Poznan University of Medical Sciences, Poland), Dr. Shristi Rawal (Rutgers University), and Prof. Sabrina Sanfilippo (University of Bayreuth, Germany) explored the role of sleep in T1D and pregnancy as well as head-to-head comparisons of different CGM systems during exercise. Collectively, the findings underscored how both lifestyle factors and device performance shape outcomes in T1D and pregnancy.
- Adequate sleep is independently associated with better glycemic stability in adults with T1D. Prof. Duda-Sobczak presented an analysis of CGM data from adults with T1D (n=155), which found that those meeting National Sleep Foundation (NSF) recommendations (between seven and nine hours of sleep) had: (i) significantly lower mean glucose (161 vs. 172-175 mg/dL); (ii) reduced glycemic variability; and (iii) higher TIR (64% vs. 57%) compared to both short (<7 hours) and long sleepers (>9 hours). Logistic regression analysis confirmed that recommended sleep duration predicted lower glycemic variability, highlighting sleep as an overlooked lifestyle factor in T1D management.
- Longer sleep improved glucose profiles in pregnant women with GDM or impaired glucose tolerance (IGT). Dr. Rawal presented a preliminary analysis of CGM data in women with GDM or IGT (n=48) across sites in the US and Nepal. Results showed that while sleep quality was not predictive of glycemic outcomes, longer sleep duration correlated with more favorable CGM-derived glycemic profiles. In the US subgroup, sleeping 6.1-7.9 hours was associated with significantly lower: (i) 24-hour mean glucose; (ii) fasting glucose; and (iii) nocturnal glucose. She said that the absence of these associations in the Nepal subgroup suggested contextual factors such as diet, lifestyle, and healthcare access may shape the sleep-glycemia relationship.
- Turning to exercise, Dexcom G7 and Abbott’s FreeStyle Libre 3 were found to outperform Medtronic’s Simplera during exercise and at-home settings. Prof. Sanfilippo reviewed a prospective head-to-head comparison of the three CGM systems (n=20 adults with T1D) over seven days. Participants simultaneously wore Dexcom G7, Libre 3, and Simplera across a structured three-day exercise protocol and a four-day at-home phase. Median absolute relative difference (MedARD) was 7.5% for Libre 3, 8.4% for Dexcom G7, and 13.8% for Simplera. While no significant differences were observed between Dexcom G7 and Libre 3 across the two study phases, Prof. Sanfilippo remarked that Simplera demonstrated significantly lower accuracy during exercise.
Exercise boosts TIR in CGM analysis of adolescents with T1D (n=3,069)
Dr. Alexander Eckert (University of Ulm, Germany) presented an analysis of CGM patterns in adolescents with T1D (n=3,069), stratified by physical activity level. Data were collected from >500 centers across Germany, Switzerland, and Austria between July 2023 and December 2024, including ~90% of children and adolescents with T1D. Participants were categorized by weekly activity: (i) low (<2 hours); (ii) moderate (3-4 hours); and (iii) high (≥5 hours). Dr. Eckert suggested that the lower-than-expected threshold for “high” weekly physical activity could represent an achievable target for youth with T1D, along with proper education on maintaining glycemic safety during exercise.
- Baseline characteristics. AID use was similar across groups (~two-thirds of participants). The high-activity group included more boys (63% vs. 47% [low] and 53% [moderate]). Mean age was 15 years with a baseline A1c of ~7.3%. Interestingly, baseline TIR rose modestly with more activity (58% low, 59% moderate, and 63% high).
- Higher activity was associated with lower mean glucose throughout the day, particularly in the afternoon and evening, along with higher TIR and TITR (70-140 mg/dL). These improvements were driven by less TAR (>180 mg/dL). Low and moderate activity did not show significant differences
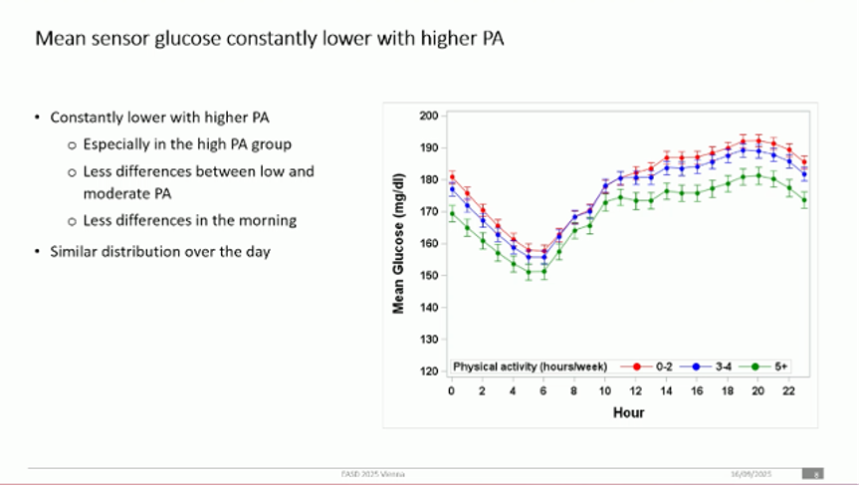
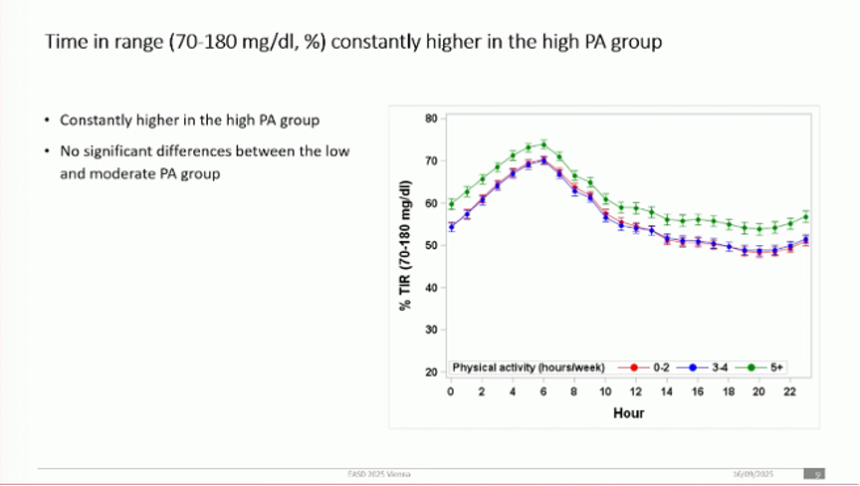
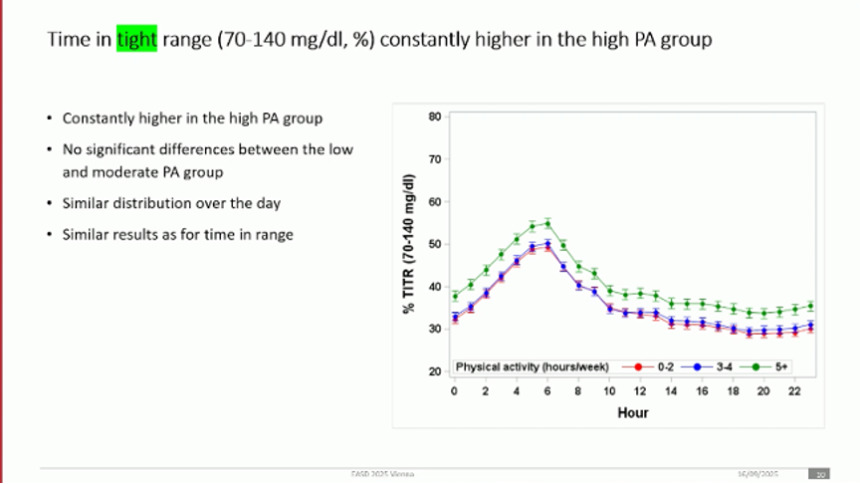
- MDI users showed higher glucose peaks in the afternoon and overnight, with larger differences by activity level.In contrast, AID users had smaller, steadier afternoon peaks and fewer differences across cohorts, reflecting tighter glycemic management (see figure below). A slightly higher risk of afternoon and overnight hypoglycemia with greater activity was noted, mainly in AID users. Still, Dr. Eckert emphasized that for most adolescents with T1D, the glycemic and overall health benefits of physical activity far outweigh the risks.
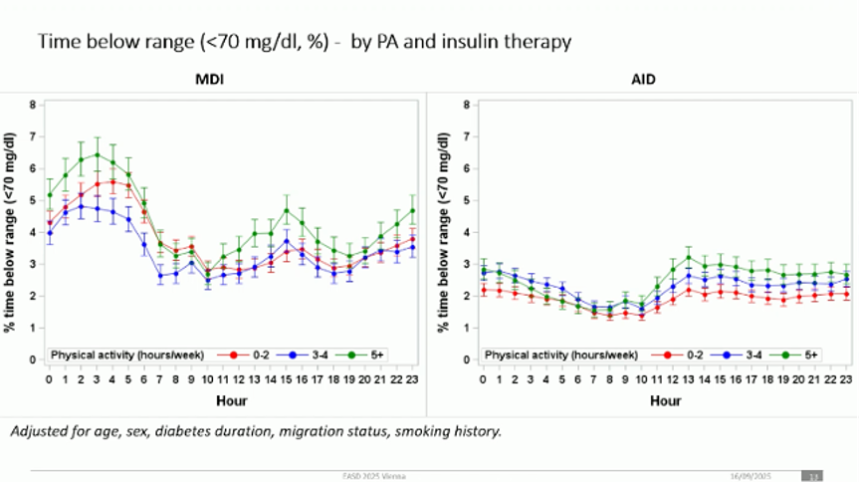
Diabetologia Symposium: Ancestry, access, and inequality shape the global diabetes landscape
At this wide-ranging symposium, Prof. Nish Chaturvedi (University College London, UK), Prof. Richard Oram (University of Exeter, UK), and Prof. Dianna Magliano (Baker Heart and Diabetes Institute, Australia) explored global inequities in diabetes prevalence, care, and outcomes. The session underscored that while scientific progress in technology and therapy continues, (i) social determinants of health; (ii) healthcare access restrictions; and (iii) an individual’s demographic context remain defining drivers of diabetes risk and mortality worldwide.
- Prof. Chaturvedi examined how race, ethnicity, and ancestry intersect to shape diabetes risk and care. She urged clinicians to move beyond biological generalizations and recognize the layered effects of genetics, culture, and socioeconomic positions. Prof. Chaturvedi noted that while ancestry is tightly correlated with geography and genetics, ethnicity reflects shared cultural norms and lived experiences. These dimensions together shape racial experiences, from health behaviors and diet to access to care and environmental stressors. She cited UK data showing that first-generation migrants remain significantly more socioeconomically deprived than Europeans, with second-generation migrants experiencing improved social positioning. Interestingly, these patterns correspond with lower T2D risk in the second generation, largely explained by gains in socioeconomic status and lower obesity rates. Prof. Chaturvedi concluded that the interaction of ancestry, ethnicity, policy, and social opportunity determines risk more than genetics alone.
- Prof. Oram provided a sobering global overview of T1D, discussing extreme variation in incidence, access, and survival. Using the T1D index, Prof. Oram highlighted persistent mortality disparities, with projections of ~175,000 T1D deaths in 2025. Of these, nearly 66% occurred in those under 25 years of age and 30,000 were due to insulin inaccessibility. He also shared date from the YODA study and the Pan African Medical Journal revealing that acute glycemic complications remain the leading cause of death due to lack of insulin and basic supplies in sub-Saharan Africa. His talk echoed Prof. Chaturvedi’s message: while technology and therapies fuel optimism in high-income countries, the upfront cost of survival globally remains considerable.
- Prof. Dianna Magliano closed the session by unpacking the global variation in T2D prevalence. Drawing on international registry and surveillance data, she outlined how prevalence reflects a complex interaction of: (i) demography; (ii) genetics; (iii) healthcare infrastructure; (iv) and lifestyle risk factors. These determinants differ sharply between countries, explaining the uneven burden of T2D across geographies. She noted that T2D prevalence is highest in middle-income countries, including Africa, Asia, and Southeast Asia. In closing, Prof. Magliano called for a stronger integration of health and food policy to address these structural drivers, especially in low- and middle-income countries where urbanization is outpacing prevention efforts.
Fewer than 40% of Danish women with prior GDM undergo postpartum diabetes screening within seven years
Prof. Sofie Haedersdal (Steno Diabetes Center Copenhagen, Denmark) presented an analysis of postpartum diabetes screening adherence among Danish women with prior gestational diabetes (GDM), revealing persistently low follow-up testing rates despite clear national guidelines. Using nationwide registry data spanning from 2015-2022, her team showed that fewer than 40% of women with prior GDM underwent glycemic testing in the seven years following delivery, underscoring the urgent need for better systematic follow-up procedures and care support after delivery.
- Study design. The analysis drew from Denmark’s comprehensive national data, linking the National Patient Register, Birth Register, and Clinical Laboratory Information Register. Women with at least one delivery complicated by GDM (n=19,984; mean age: 32 years) between July 2015 and December 2022 were included, and the study excluded those with an existing diabetes diagnosis. Three types of postpartum glycemic metrics were analyzed: (i) A1c levels; (ii) fasting plasma glucose (FPG) levels; and (iii) 75-g oral glucose tolerance test (OGTT).
- Results. Prof. Haedersdal and her team found that of the eligible women with at least six months of follow-up data, only 12.7% of women were screened within six months postpartum. Cumulative adherence improved slightly over time but remained poor: 15.9% by 14 months, 25.5% by 47 months, and 36.6% by 84 months. Only about 5% of women met the full guidelines criteria of testing within the first postpartum year and again within the subsequent four years. These findings indicate that the vast majority of women with prior GDM in Denmark are not receiving recommended diabetes screening during the highest-risk window for T2D onset.
- Discussion. Prof. Haedersdal emphasized that postpartum glycemic testing represents a critical missed opportunity for early intervention to prevent T2D and related complications. She called for national efforts to improve comprehensive follow-up, highlighting how continuous monitoring of adherence metrics will be essential to ensure that women with prior GDM receive the long-term care they need.
Higher A1c thresholds required to predict T1D progression in adults compared to children with positive islet autoantibody
In an oral session, Prof. Erin Templeman (University of Exeter, UK) shared findings on the comparison of A1c thresholds for predicting T1D progression between children and adults. Prof. Templeman explained that A1c increases with age due to both glycemic and non-glycemic related factors. Some of these factors may influence the predictive value of A1c thresholds for T1D progression, affecting strategies for monitoring and diabetes management among children and adults. Therefore, a study aimed to determine the effects of age on A1c thresholds for predicting the progression of T1D diagnosis among individuals with positive autoantibodies.
- Methods. The study included relatives who screened for autoantibodies in the TrialNet Pathway to Prevention study. Individuals who tested positive for autoantibodies received an oral glucose tolerance test (OGTT) and an A1c measurement among children and adults. Then, a model estimated the risk of T1D within age groups to assess differences between the cohorts.
- Results. There were 6,085 participants (27% adults) who tested positive for islet-autoantibodies. Among this population, 29% developed T1D, of whom 14% were adults. The adults who progressed to diabetes had a higher A1c level at the time of autoantibody detection than children (36 mmol/mol or 5.4% vs. 34 mmol/mol or 5.3%, p<0.001). The study showed an increased risk of developing clinical T1D with increasing A1c levels for both age groups. However, a higher level of A1c was needed to identify adults at equivalent progression risk to children. For example, Prof. Templeman explained that children with A1c of 39 mmol/mol or 5.7%, which is the A1c threshold for stage 2 T1D, had a higher risk of developing T1D within 12 months compared to adults (39% vs. 15%, p<0.001).
- Discussion. While A1c remains a strong predictor for T1D progression, Prof. Templeman emphasized that the impact of age on A1c affects interpretations of risks. Therefore, she encouraged adjusting thresholds to optimize the use of A1c levels when building monitoring and management of autoantibody screening.
Exhibit Hall
EASD 2025’s exhibit hall offered a lively, visually striking experience, with towering booths topped by large (sometimes rotating) overhead signs, bright print posters and digital displays, and many smaller, more intimate booths. Many provided demonstrations of their respective products to attendees and reviewed recent data on patient outcomes, creating valuable learning opportunities for the thousands of clinicians in attendance. The energy from the scientific sessions carried naturally into the hall, where conversations often continued from the many product theaters held throughout the conference. Moreover, many attendees wandered through the space with complimentary coffees and teas in hand, courtesy of generous exhibitors. See specific coverage of nearly 20 companies’ booths below.
Diabetes Technology
Abbott
Stepping into Abbott’s spacious booth near the center of the Exhibit Hall, we were immediately struck by the range of real-world applications highlighted across its various platforms. As expected, representatives were enthusiastic in showcasing both clinical and patient experiences with the FreeStyle Libre system. A steady crowd gathered around the popular “Sensor Wear Experience” table at the heart of the booth, where attendees could get a hands-on feel for sensor size, wear duration, and compatibility with AID systems around the world. Abbott was also actively distributing the third issue of The Sensor Report, a concise, visually engaging brochure that dives into CGM regulatory variation across global markets.
One especially intriguing corner of the booth was dedicated to raising awareness about the dangers of unmonitored ketone levels — a clear nod to Abbott’s upcoming dual glucose-ketone (DGK) sensor, a much-discussed innovation throughout the conference. The display seemed to hint at the company’s broader educational campaign ahead of its DGK launch, emphasizing ketone monitoring as an essential part of comprehensive diabetes care. Finally, a large screen played Abbott’s #AboveTheBias campaign video, originally launched earlier this year in a high-profile New York City event that has since gained viral traction. The campaign’s focus on lived diabetes experiences added an emotional and human-centered dimension to the booth experience. We appreciated how the booth captured the full spectrum of diabetes care, from technical to clinical and emotional.

Ascensia
Consistent with prior conferences and Senseonics’s overall focus on ease of use, Ascensia’s booth continued to emphasize the tagline, “One year. One CGM.” The implantable Eversense 365 sensor has a one-year wear time and a removable transmitter. The sensor requires once-daily calibrations for the first 13 days of use, followed by once-weekly calibrations for the next 50 weeks, spanning nearly a year of continuous use. At EASD 2025, displays and company representatives also focused heavily on the environmental benefits of Eversense 365, saying, “no more wasted CGMs.” Ascensia certainly has environmental advantages, which we imagine can be especially persuasive in the European market of focus at EASD. Ascensia has seen broad interest in the implantable CGM from providers and patients alike – with 250% userbase growth in 3Q25 year over year and almost 40% sequentially. Ascensia expects a doubling of its userbase every year, as well as consistent growth in its prescriber base. In insulin pump partnerships, the planned integration of Eversense 365 with Sequel’s twiist remains on track for the end of 2025, which would mark the first closed-loop pump integration for the 365-day sensor. Representatives said that Senseonics also continues to develop the Bluetooth-enabled Gemini and Freedom sensors, which will function as isCGMs when patients prefer to remove the external transmitter. The company plans to launch these devices in 4Q26 and 4Q27, respectively.

Dexcom
Dexcom’s signature green booth showcased the company’s growing emphasis on individualized treatment from their sensors’ unique features. Large displays throughout the booth highlighted clinical data showing a 72% reduction in hypoglycemic events in people with T1D, underscoring the significant outcomes enabled by Dexcom’s technology. Product demonstrations featured Dexcom G7, Dexcom ONE+, and the Clarity platform, with representatives drawing attention to G7’s smaller form factor, 30-minute warm-up time, and 12-hour grace period, as well as the recent expansion of direct-to-Apple Watch connectivity, augmenting the convenience of data viewing for many users. These key points of discussion were complemented by a Dexcom-sponsored symposium at the start of the conference, where President and COO Mr. Jake Leach previewed Smart Basal as an upcoming feature within Clarity, designed to calculate personalized basal insulin doses (which is currently under FDA and CE-Mark review). Dr. Halis Akturk (University of Colorado Anschutz) presented further real-world findings in adults with T2D (n=74,679) there, showing reductions in hospitalizations and emergency visits. Together, Dexcom’s vibrant booth on the exhibit hall and the company’s symposium reinforced its message: CGM should be viewed as an essential therapeutic tool for optimizing diabetes care and management.

Glooko
Glooko featured a data-driven showcase of its diabetes management platform, including app demonstrations from representatives. Attendees were shown how the Glooko integrates data from CGMs, insulin pumps, smart pens, and wearables into a single platform designed for both patients and providers. The booth emphasized the app’s new AI-powered pattern recognition, customizable alerts for more individualized management, and streamlined user experience, which aim to make data interpretation easier and more actionable. Representatives also highlighted Glooko’s growing global presence, with the app now available in over 30 countries and compatible with more than 95% of diabetes devices. Discussions at the booth positioned the California-based company as bridging the clinical and digital worlds of diabetes management.
Beyond the exhibit hall, our team recently had the opportunity to meet with Glooko’s Mr. Rich Glenn (President, Connected Care), Mr. Mike Alvarez (CEO), and Dr. Mark Clements (CMO) to discuss the company’s acquisition of Monarch Medical Technologies, the developer of the EndoTool Glucose Management System. EndoTool aims to reduce hypoglycemia risk and standardize outcomes across critical care units with patient-specific dosing recommendations through algorithms that consider insulin sensitivity, nutritional intake, and comorbidities. By pairing EndoTool’s dosing algorithms with Glooko’s outpatient diabetes device integrations and remote monitoring platform, the company aims to streamline the transition from hospital to home, reduce readmissions, and better align inpatient care with post-discharge management. This illustrates a clear niche for an integrated inpatient-outpatient dosing algorithm and glycemic management platform.

Insulet
Insulet’s signature Omnipod mango booth drew a steady crowd throughout EASD to explore what’s next for Omnipod 5 AID System. Interactive demonstrations showcased the AID system, and a large display depicted the company’s collaboration with Marvel on Dyasonic: Sound of Strength, the comic aiming to expand chronic disease visibility and subsequently reduce stigma around the disease. Conversations at the booth centered around global expansion with Omnipod 5 compatibility with Dexcom G7, whichlaunched across several new markets including Australia (March), Switzerland (April), and Italy (early September). It’s terrific for patients and clinicians outside the US to see these expansions as well as ones in Denmark, Finland, Norway, Sweden, the Netherlands, Germany, France, and the UK, where Omnipod has launched previously – the international expansion is certainly impressive. On the digital front, the upcoming iOS app rollout in the US also generated excitement, particularly among attendees eager for their patients to have greater platform accessibility. The company’s symposium echoed the representatives’ same theme of accessibility and scalability, where Prof. Pratik Choudhary (University of Leicester, UK), and Prof. Sandra Schlüter (Hannover Medical School, Germany) described how streamlined onboarding models can significantly broaden AID adoption. We were pleased to see the sustained interest in Omnipod 5 throughout the conference and look forward to more of this throughout 2026.

i-SENS
Stepping into i-SENS’ vibrant booth, visitors were immediately drawn to the wide range of glucose monitoring platforms on display. Company representatives were particularly eager to discuss the CareSens Air, the company’s sleek, real-time CGM. A dedicated section of the booth highlighted i-SENS' BGM platform, featuring a variety of blood glucose meters designed for precision and reliability. Attendees were particularly interested in the latest models, which offer faster readings and improved accuracy, crucial for patients looking to stay on top of their glucose levels throughout the day. In another corner, interest in the Sens 365 patient monitoring platform took over. Representatives were eager to demonstrate how this comprehensive system offers continuous monitoring and data analytics, allowing both patients and healthcare providers to track glucose levels and adjust treatments accordingly in real-time. It’s clear that i-SENS intended for visitors leave with a deeper understanding of how it is working to enhance patient care, whether through CGM, BGM, or patient-centered monitoring solutions.

Medtronic
Medtronic’s booth featured the name Medtronic as a sort of guiding beacon at the top, with the ground-level booth squarely dedicated to the name MiniMed. MiniMed is expected to fully split from Medtronic in 2026 and will retain a focus on AID, including the MiniMed 780G system. Medtronic’s booth at EASD focused on the breadth of benefit offered by MiniMed 780G, with the tagline, “superior outcomes with less effort for a wide range of people with diabetes.” Looking ahead, the company highlighted that it expects MiniMed 780G to soon be available for use in children ages two and up, along with pregnant women. In July 2025, Medtronic received CE-Mark for MiniMed 780G in T2D, pregnancy, and for patients with T1D ages two and older. At the time of the announcement, the company signaled that launch for these indications would occur in fall 2025, with no further update provided as of 3Q25. The EASD 2025 booth was accordingly filled with excitement and anticipation for the new indications, with booth representatives discussing benefits of the expanded indications with providers.

SIBIONICS
A short walk from the Exhibit Hall entrance brought us to the striking turquoise glow of the SIBIONICS booth, which was centered around the company’s GS3 CGM system. With product samples on display and demo videos playing on a large central screen, representatives walked visitors through key features of GS3, including its wear duration (14 days), compact sensor size (as thin as one coin), and user-friendly mobile integration. Conversations with representatives frequently touched on the system's real-time data sharing capabilities and benefits of use for “all types of diabetes” – T1D, T2D, and prediabetes. While most of the booth’s attention was focused on the GS3 CGM, reps also hinted at broader ambitions, including ongoing development of niia Signature, an all-in-one patch pump (GS3 CGM + PharmaSens-developed patch pump). As one of the newer players in the European market, SIBIONICS made a distinctive showing, and we will be tracking their progress in achieving their mission statement of “realizing the unimagined” as they consider expansion to the US and other global markets.

Diabetes Therapy
Amgen
Amgen’s presence was hard to miss at EASD with its booth featuring once-monthly MariTide (maridebart cafraglutide), a GLP-1 RA and GIP receptor antagonist, across multiple screens. Our team particularly appreciated learning about MariTide through an interactive augmented reality visual that featured its mechanism of action as a long-acting antibody conjugate that combines GLP-1 agonism and GIP antagonism for obesity. Previously, in a phase 2 trial among participants with obesity or overweight without T2D (n=465), MariTide conferred up to 20% weight loss without plateau compared to 2.6% with placebo at Week 52. In participants with obesity or overweight and T2D (n=127), MariTide showed up to 17% weight loss compared to 1.4% with placebo. As we heard in 2Q25, the following trials are underway: (i) MARITIME-1 in obesity or overweight, without T2D; (ii) MARITIME-2 in obesity or overweight, with T2D; (iii) MARITIME-CV in ASCVD and obesity or overweight; and (iv) MARITIME-HF in heart failure with preserved or mildly reduced ejection fraction and obesity.

AstraZeneca
AstraZeneca’s blue booth emphasized the organs affected by the cardio-renal-metabolic syndrome, as shown in the hanging banner and the featured products and candidates. Next to an aromatic coffee stand, the exhibit was organized into distinct zones including Research & Development, Disease Awareness, Medical Information, and a stand-alone section highlighting Forxiga (dapagliflozin). Interactive kiosks and tablet stations allowed attendees to explore Forxiga’s benefit on outcomes, watch animations about its mechanism of action, and submit inquiries directly through a UK Medical Information form. A large life‑sized screen featuring an animation of a doctor directed attendees to “trace the links” between obesity and cardiometabolic health. These themes echoed the focus of the industry symposium sponsored by AstraZeneca, which explored the synergistic potential of SGLT-2 inhibitors and GLP-1 RAs for multi-organ protection in people with T2D. SGLT-2 inhibitors promote natriuresis (which is when elevated pressure causes the kidneys to inaccurately work to reduce fluid and sodium levels, decreasing reabsorption and increasing water excretion), cardiac fuel shifts, and renal energy loss – reducing inflammation and improving endothelial function. Finally, the Disease Awareness section highlighted statistics on cardiorenal outcomes and the need to implement optimized guideline-directed therapy for chronic kidney disease, in which SGLT-2 inhibitors are one of the four pillars of treatment.

Bayer
Bayer’s booth, set on the periphery of EASD 2025’s massive exhibit hall, showcased Kerendia (finerenone) and its role in slowing chronic kidney disease (CKD) progression in people with T1D. The stand’s red-and-white color palette and prominent tagline, “One move can change the outcome” emphasized Kerendia’s impact on improving cardiorenal health. Interactive displays, educational panels, and appealing visuals attracted attendees to learn more about Kerendia’s mechanism of action and clinical evidence for optimizing CKD and T2D care. Bayer representatives were friendly, informative, and stressed the therapy’s benefit for cardiorenal health in people with T2D. At EASD 2025, Bayer’s industry symposium further emphasized unmet needs in T1D and CKD care. Despite the fact that nearly one-third of people with T1D will develop CKD in their lifetimes, little management of CKD has changed for people with T1D in the last few decades. Bayer’s Kerendia (finerenone) was referenced throughout the conversation as a potential management tool for T1D and CKD. Excitingly, at the American Society of Nephrology 2025, full results of the phase 3 FINE-ONEstudy were presented, in which finerenone demonstrated a statistically significant 25% reduction in UACR (albumin-to-creatinine ratio) compared to placebo at six months in people with T1D and CKD. We are thrilled that finerenone can soon be available to this population!

Daiichi Sankyo
Daiichi Sankyo’s booth focused on two drugs, Nilemdo (bempedoic acid) and Nustendi (ezetimibe and bempedoic acid), which are indicated to lower cholesterol levels in adults with hypercholesterolemia or high-risk atherosclerotic cardiovascular disease (ASCVD). In addition to a tea and coffee station, a large screen highlighting patients who can benefit from Nilemdo or Nustendi drew attendees’ attention. Reps kindly approached us and asked if we had any questions about the products. They highlighted results from the massive CLEAR Outcomes trial (n=13,970), which found significant placebo-adjusted LDL-c reduction by 21 percentage points with bempedoic acid at 6 months and 13% lower incidence of 4-MACE (CV death, nonfatal myocardial infarction, nonfatal stroke, or coronary revascularization) at 41 months. Another trial demonstrated CV benefits of triple therapy with bempedoic acid, ezetimibe, and statin. The rep noted that the drugs were found efficacious in both statin and statin-intolerant patients alike.

Diamyd Medical
Diamyd Medical’s light-blue booth focused on Diamyd (rhGAD65), an antigen-specific immunomodulatory precision therapy for the treatment and prevention of T1D. Specifically, Diamyd is a GAD65 protein-containing molecule for people with detectable GAD65 antibodies and the HLA DR3-DQ2 haplotype, which affects about 40% of people with T1D. Sharing informational handouts and published papers, the reps explained that Diamyd demonstrated C-peptide preservation and partial remission at 15 months in this genetic subgroup in a phase 2b trial (n=109). Diamyd is now evaluated in the ongoing DIAGNODE-3 study at approximately 50 European and 13 US sites. We also congratulated the reps for Diamyd Medical’s patent approvals for insulin-based antigen treatment – another precision therapy candidate that would target people with T1D who carry the HLA DR4-DQ8 genetic marker. The company estimates that the two genetic markers together encompass up to 90% of people with T1D. Reps shared that Diamyd Medical aims to focus on the DIAGNODE-3 trial before advancing a second clinical candidate.

Lilly
Lilly boasted a large, red booth that showcased the company’s expansive cardiometabolic health pipeline. Large television and tablet displays highlighted the mechanisms of action for various incretin-based therapies including retatrutide (triple GLP-1/GIP/glucagon RA) in phase 3, orforglipron (oral GLP-1 RA) in phase 3, and tirzepatide (dual GLP-1/GIP RA) currently approved for diabetes and obesity. In particular, the reps highlighted Mounjaro (tirzepatide for T2D) as “a class of its own” with superior A1c reduction when compared with semaglutide according to the SURPASS trial. Moreover, while not mentioned in the booth, EASD 2025 featured several trial results of tirzepatide and orforglipron. In the phase 3 ATTAIN-1 trial (n=3,127), orforglipron demonstrated up to 12% reduction in body weight compared to 0.9% with placebo in people with obesity and not T2D. In the landmark phase 3 SURPASS-CVOT trial, tirzepatide was noninferior to dulaglutide in reducing the risk of MACE, demonstrating cardiovascular benefits. We’re excited about the continued development of the pipeline, as shown in the table here.
On the opposite side of the booth, we were moved to see a panel about Lilly’s support for Life for a Child, a nonprofit organization supporting children with diabetes in under-resourced communities. Notably, Lilly donated 10.6 million insulin vials for 150,000+ children across 65 countries! The booth achieved a nice balance between Lilly’s R&D and social responsibility that instills confidence in Lilly’s commitment to delivering innovation, while also ensuring accessibility to that innovation.

Madrigal
Madrigal’s large, blue booth was at the center of the exhibit hall, drawing attendees in with an aromatic coffee station and a large display describing stages of MASLD (metabolic dysfunction-associated steatotic liver disease) and MASH (metabolic dysfunction-associated steatohepatitis). The rep greeted us enthusiastically and asked if we had any questions about Rezdiffra (resmetirom), a first-in-class, once-daily oral thyroid hormone receptor-β agonist indicated for MASH with moderate-to-advanced fibrosis (stages F2/F3). He explained that in the phase 3 MAESTRO-NASH trial (n=966), Rezdiffra conferred MASH resolution without worsening of fibrosis in 30% of participants (vs. 10% in placebo), and improved fibrosis by at least one stage without worsening of MASH in 29% of participants (vs. 17% in placebo). He also noted that Rezdiffra can increase liver enzymes ALT and AST in people receiving statin therapy and emphasized the importance of adjusting statin dosage at Rezdiffra initiation. Since the launch in April 2024, Rezdiffra became available in more countries – most recently in Germany at the time of speaking with the rep, following the EU approval in August 2025. The rep also shared that many attendees have asked when the drug will be available at their respective countries, highlighting the growing global interest.

Novo Nordisk
Novo Nordisk’s booth sat front and center in the bustling exhibit hall, beckoning attendees with its vibrant pink heart structures and a photo booth. The company’s leading GLP-1 RA drug portfolio, Ozempic (semaglutide for T2D) and Wegovy (semaglutide for weight loss), were promoted in tandem. Each therapy received its own informative and interactive heart-shaped display in bold hues of red, pink, and blue. At the center of the booth, attendees could find a circular LED display which advertised general uses for Ozempic and Wegovy, as well as a few striking statistics from Novo Nordisk’s clinical trials. For example, in the phase 3 STEP 1 trial (n=1,961), Wegovy demonstrated a 15% weight loss compared to 2% with placebo at Week 68. While not a primary focus of the booth, Rybelsus (oral semaglutide) also demonstrated a significant cardiovascular benefit beyond glycemic reduction. In the phase 3b SOUL trial (n=9,650), Rybelsus demonstrated a 14% MACE reduction compared to placebo, and in its post-hoc analysis presented at EASD 2025, the benefits were significant regardless of baseline A1c or BMI. The booth offered a dynamic, welcoming space for conversation with friendly company representatives. Through education blended with eye-catching, engaging displays, HCPs explored how Ozempic and Wegovy can improve outcomes in metabolic health and how clinicians can use them in day-to-day practice. Novo Nordisk also boasts an extensive insulin portfolio, including Tresiba (insulin degludec), Fiasp (insulin aspart), NovoLog (insulin aspart), and fixed-ratio basal insulin/GLP-1 RA combination Xultophy.

Regeneron
Regeneron’s blue-and-purple ombre booth shared information on body composition as well as weight-loss induced muscle mass loss, in line with the company’s phase 2b COURAGE trial readout at EASD. As background, the 26-week study (n=1,005) evaluated the effects of trevogrumab (anti-GDF8/anti-myostatin) with or without garetosmab (anti-activin A) on weight loss quality in people with obesity when combined with the GLP-1 RA semaglutide. Reps were excited to share its results, which revealed that trevogrumab preserves 50-80% of lean mass lost with semaglutide alone. Specifically, triple combination therapy (i.e., trevogrumab, garetosmab, and semaglutide) preserved lean mass the most compared to dual combination therapy (i.e., trevogrumab and semaglutide) and semaglutide alone (2% reduction vs. 3% vs. 7% from a baseline of 53 kg [117 lbs]).

Sanofi
Sanofi’s booth was certainly a highlight at EASD 2025, featuring a thought-provoking and visually striking theme related to T1D prevention: “Is T1D hiding from you?” The installation (pictured below) spotlighted undiagnosed or misdiagnosed T1D with two covered human silhouettes symbolizing the disease’s often unseen presence in the body until serious complications of T1D such as DKA prompt a diagnosis. The creative concept drew attention to Sanofi’s partnership with br1dge’s T1D screening program – which had its own booth to screen attendees on site for T1D autoantibodies in the back corner of the same hall. Sanofi representatives and promotional materials urged attendees to get tested that same day, drawing attention to the company’s T1D screening expansion efforts alongside its therapeutic offering, Tzield (teplizumab). In all, the booth focused on improving early identification of T1D in both children and adults and emphasized Sanofi’s commitment to Tzield – which is currently the only therapy approved to delay the progression of insulin dependence for individuals with Stage 2, presymptomatic T1D. While it was not a focus at the booth, Sanofi also boasts a broad insulin portfolio, including Toujeo (insulin glargine), Lantus (insulin glargine), and fixed-ratio basal insulin/GLP-1 RA Soliqua (insulin glargine/lixisenatide). We appreciate Sanofi’s dedication to health of people with diabetes.


[1] Complications included foot damage, gastroparesis, hyperosmolar hyperglycemic nonketotic coma, nephropathy, and neuropathy. DKA was not included.
[1] 20/20% agreement assesses the proportion of paired points in which the CGM value falls within ±20 mg/dL (<100 mg/dL) or ±20% (≥100 mg/dL) of paired capillary blood glucose values.
[2]Based on CRISTAL trial results, MiniMed 780G received expanded CE-Mark in July 2025 for pregnancy.
[1] As a reminder, T1D is a progressive disease with several stages: stage 1 T1D refers to people with two or more islet autoantibodies and normal glucose level; stage 2 T1D for those with at least two autoantibodies and dysglycemia; and stage 3 for those with clinical diagnosis of T1D.
[1]As we understand it, this term is sometimes used to refer to “approaches that derive biological / functional meaning from lists of genes” – see “Pathways and gene sets: What is functional enrichment analysis?”
[1]The trial was conducted in nine countries, including Brazil (28%), the USA (27%), Japan (10%), Spain (10%), China (10%), Slovakia (8%), Republic of Korea (3%), Taiwan (3%), and India (2%).
[2] As a reminder, the SOUL trial (n=9,650) found 14% MACE reduction with Rybelsus (oral semaglutide) in people with T2D and ASCVD or CKD. The FLOW trial (n=3,533) found that Ozempic (injectable semaglutide) confers 24% risk reduction in kidney outcomes in people with T2D and CKD. Finally, the STRIDE trial found that Ozempic (injectable semaglutide) increases maximum walking distance by 13% (40 m) in people with T2D and PAD.