AACE 2026 Day #1 Highlights –
Executive Highlights
- The American Association of Clinical Endocrinology (AACE) 2026 kicked off today in lively Las Vegas. AACE President Dr. Dace Trence (University of Washington) opened the conference with a high‑energy session where she highlighted the conference’s more than 2,400 attendees, including over 800 first‑time participants. Program Chair Dr. Rifka Schulman‑Rosenbaum introduced this year’s theme, “Viva Nutrition! Advancing Endocrine Practice from the Inside Out,” emphasizing practical, clinically grounded sessions designed to integrate nutrition into everyday endocrine care.
- In his keynote address, Dr. Jeffrey Mechanick (Icahn School of Medicine at Mount Sinai) reframed nutrition as the interaction between diet and metabolism that underpins every major endocrine condition, highlighting multimorbidity data and calling for longitudinal, systems‑level models that address shared metabolic drivers rather than single‑disease endpoints.
- Global and cardiometabolic sessions highlighted the heterogeneity of diabetes and the convergence of metabolic disease. Speakers from Pakistan, Mexico, and India underscored region‑specific genetics, early‑onset T2D in high‑risk populations, and the disproportionate burden in LMICs. Cardiometabolic and liver-focused sessions reinforced the shift toward adiposity‑centric care, updated dyslipidemia guidance prioritizing ApoB and non‑HDL‑C, and the need for early detection of “at‑risk MASH” supported by modern noninvasive tools and an expanding therapeutic pipeline.
- In diabetes technology, sessions highlighted the rapid expansion of CGM, AI, and emerging CKM. Dexcom showcased earlier CGM use in non‑insulin T2D, real‑world A1c reductions, and its Smart Basal titration platform. In a session on AI, Dr. David Ahn (Mary & Dick Allen Diabetes Center) described the evolution from assistive tools to agentic systems capable of autonomous clinical action.
- Three “Year in Review” sessions highlighted advances across diabetes, nutrition, and cardiometabolic/lipid science. The diabetes review covered updated treatment algorithms, SURPASS‑CVOT, ESSENCE, and progress in oral GLP‑1 RA development, alongside emerging disease‑modifying strategies in T1D such as teplizumab and stem‑cell-derived islet therapies. The nutrition review reinforced nutrition as a metabolic driver across endocrine disease, while the cardiometabolic/lipid review emphasized updated dyslipidemia guidance prioritizing ApoB and non‑HDL‑C and the shift toward integrated, adiposity‑centric risk reduction.
See the conference agenda, registration, and our preview for what to expect in the days ahead.
Table of Contents
-
Top Highlights
- 1. Opening session places nutrition at the center of AACE 2026 Annual Meeting
- 2. Role of AI in diabetes care: Leveraging CGM-driven insights to support agentic recommendations
- 3. Global perspectives from Pakistan, Mexico, and India highlight diabetes heterogeneity and the need for context-specific care across regions
- 4. Interdisciplinary strategies to detect and treat “at‑risk MASH”
- 5. CKM discussion continues: Dr. Rodolfo Galindo emphasizes metabolic complexity and the need for standardized interpretation
- 6. Dexcom product theater showcases CGM portfolio, evidence in non-insulin T2D, and Smart Basal titration platform
- 7. Diabetes Year in Review: Treatment algorithm improvements for better care across T1D and T2D
- 8. Dr. Michelle Look on exercise and nutrition recommendations during GLP-1 RA/GIP therapy for obesity
- 9. Cardiometabolic “Year in Review”: Evolving lipid therapy guidelines and cardiometabolic strategies for long‑term risk reduction
- 10. AACE’s prediabetes algorithm: Case studies to demonstrate efficacy
- 11. Nutrition & Obesity Year in Review: Obesity care moves beyond BMI as pharmacologic options accelerate and nutrition remains foundational
- 12. “Betting on basal”: Casino-themed night focused on how to improve odds for PWDs
Top Highlights
1. Opening session places nutrition at the center of AACE 2026 Annual Meeting
AACE President Dr. Dace Trence (University of Washington) opened the 35th Annual Meeting in Las Vegas with an energetic welcome to more than 2,400 attendees, including over 800 first‑time participants. She reflected on AACE’s 35‑year history advancing endocrine innovation, strengthening clinical practice, and improving community health through education, collaboration, and evidence‑based guidance. Dr. Trence also highlighted major initiatives launching this year, including AACE’s updated consensus statement on T2D management, published earlier this week. She also previewed AACE’s first in‑person MASLD/MASH Strategic Roundtable and the expansion of AACE’s global quality programs, such as the AACE Diabetes Center of Excellence. Program Chair Dr. Rifka Schulman‑Rosenbaum (Long Island Jewish Medical Center) highlighted this year’s theme: “Viva Nutrition! Advancing Endocrine Practice from the Inside Out.” She emphasized nutrition as a cornerstone of chronic endocrine disease management and highlighted the meeting’s diverse formats designed to keep sessions practical, clinically relevant, and connected to everyday endocrine care.
- In his keynote address, Dr. Jeffrey Mechanick (Icahn School of Medicine at Mount Sinai) urged attendees to think about nutrition not as a single‑disease intervention, but as the interaction between diet and metabolism that underpins the chronic endocrine conditions clinicians manage every day. Framing his talk through Joseph Campbell’s “Hero’s Journey,” he traced his own three‑decade arc within AACE, from endocrine fellow in 1988-1990 to AACE/ACE president and now keynote lecturer.
- He defined nutrition as the interaction between diet and metabolism, emphasizing health as a relative state shaped by metrics, symptom burden, and happiness, with a pathophysiologic state defined as persisting for 3-12 months. Dr. Mechanick walked through how nutrition threads through every major endocrine condition, reviewing its role in obesity care, diabetes management, dyslipidemia treatment, bone health, PCOS, and thyroid disorders.
- He highlighted multimorbidity data, including a 1999-2018 analysis showing that most individuals with ASCVD had four or more concurrent chronic diseases, and a more than 30,000-patient dataset in which conditions such as MI (17%), CHF (54%), and COPD (40%) clustered tightly. These findings reinforced his point that patients rarely present with a single diagnosis, and that nutrition, because it intersects with every major endocrine condition, must be approached within the broader context of multimorbidity rather than as a disease‑specific intervention. Together, these data grounded his call for models of endocrine care that address shared drivers of chronic disease rather than isolated endpoints.
- He argued for a shift toward chronic disease models that focus on the upstream processes driving long‑term metabolic risk, integrating lifestyle medicine, systems-level thinking, and preventive infrastructure. He pointed to the rise in chronic disease over the past several decades and noted that trends in smoking, exercise, alcohol use, and healthier eating do not track with that increase, while the steep rise in obesity does.
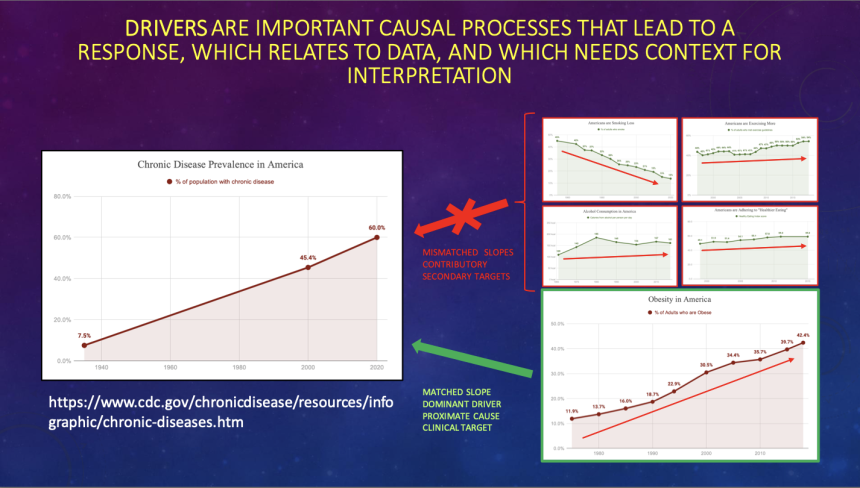
He used this mismatch to show that clinicians need structured, longitudinal approaches that address the dominant metabolic processes shaping disease risk, not episodic, disease‑specific interventions. He highlighted “lifestyle medicine” as a defined set of processes that can be built into routine endocrine care and emphasized the importance of preventive systems that support early risk identification and sustained behavior change. By placing nutrition within this broader framework, he argued that clinicians can more effectively influence long‑term metabolic trajectories across the endocrine spectrum.
2. Role of AI in diabetes care: Leveraging CGM-driven insights to support agentic recommendations
In a highly engaging afternoon session, Dr. David Ahn (Mary & Dick Allen Diabetes Center) presented on the role of AI in diabetes care on behalf of himself and Dr. David Lieb (Eastern Virginia Medical School). The hall was packed, with some attendees sitting on the floor once there were no more seats available. Dr. Ahn started with a comprehensive overview of how AI is reshaping the clinical management of diabetes. He said that AI should be understood not as a replacement for clinicians, but as an additive tool that is rapidly becoming essential for effective practice. While the audience showed some degree of familiarity with AI tools (as evidenced by polling data indicating over half of the audience used AI in their workflows today), the primary focus of the session remained on the clinical and translational implications of AI for diabetes care.
- In 2026, clinicians and people with diabetes are facing an unprecedented scale and complexity of modern diabetes (and broader health) data. Dr. Ahn highlighted the transition from traditional BGM, which yielded only a handful of daily data points, to CGM systems and wearable devices that can generate thousands of data inputs per day. This data proliferation, while rich in potential insight, introduces significant analytical challenges, including (i) inconsistent data capture; (ii) variability in physiological responses; and (iii) difficulty identifying clinically meaningful patterns. Dr. Ahn suggested that AI is uniquely positioned to address these challenges by enabling pattern recognition, predictive modeling, and real-time decision support.
- To organize these diverse applications, Dr. Ahn proposed a framework based on degree of autonomy and methodological complexity, distinguishing between assistive, rule-based tools and more advanced generative or agentic systems. He cited evidence from randomized controlled trials involving over 6,500 participants to substantiate the clinical utility of AI, demonstrating improvements in A1c among individuals with T2D. Dr. Ahn also differentiated the role of AI in T1D vs. T2D: the former offers a data-rich environment with rapid feedback loops conducive to algorithm training, whereas the latter presents challenges of scale, heterogeneity, and delayed therapeutic intensification. While many of the cited data sets did not reach statistical significance in terms of superiority, most AI-led interventions were noninferior to human-led interventions, demonstrating the value of AI-supported decision making in a clinical workflow. Potential use cases included alerts for missed medications, trend analysis, and other interactions that could alter patient behavior to improve outcomes.
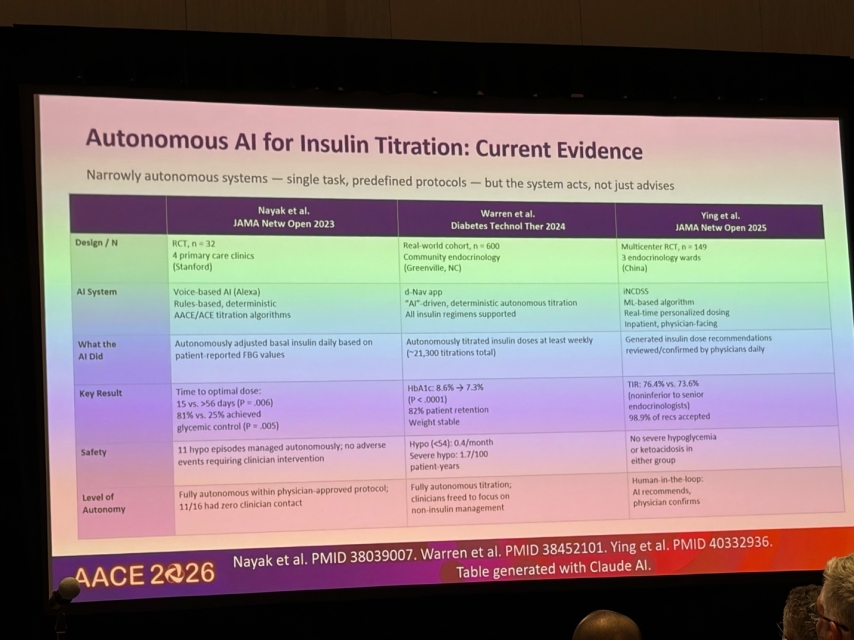
- Finally, incorporating material from Dr. Lieb, Dr. Ahn talked about the emerging role of agentic AI systems capable of autonomous or semi-autonomous clinical action (see above). Examples included AI-driven insulin titration, neural network-based artificial pancreas models, and digital twin simulations that allow clinicians and patients to model potential treatment scenarios prior to implementation. While these innovations offer substantial promise in improving efficiency and personalization of care, there are still important risks to consider, including algorithmic bias, clinician overreliance on automation (and subsequent deskilling), regulatory gaps, and disparities related to the digital divide. The evolving role of the endocrinologist was framed as shifting from direct data interpretation toward oversight of AI systems and management of complex clinical scenarios. In this context, Drs. Ahn and Lieb framed the integration of AI into diabetes not as an optional add-on, but a necessary evolution requiring both technical competency and careful attention to equity and safety.
3. Global perspectives from Pakistan, Mexico, and India highlight diabetes heterogeneity and the need for context-specific care across regions
In this session on global perspectives in diabetes and obesity, Profs. A.H. Aamir (Peshawar General Hospital, Pakistan), Roopa Mehta (National Institute of Medical Sciences and Nutrition, Mexico), and Dr. Subhankar Chowdhury (Manipal Hospital, India) examined how diabetes and obesity vary across regions in epidemiology, pathophysiology, and management. Across presentations, speakers concurred that diabetes is not a uniform disease, and that global care will require more precise phenotyping and culturally tailored interventions, particularly in low- and middle-income (LMIC) countries.
- Prof. Aamir highlighted the rapidly rising global burden for diabetes and obesity, drawing attention to the disproportionate burden in LMICs and the need for region-specific screening and policy action. He said that ~589 million people are currently living with diabetes globally, projected to rise to ~852 million by 2050, with ~95% of this increase occurring in LMICs. Despite this, healthcare spending remains highly uneven. For instance, Southeast Asia accounts for only ~1% of global diabetes spending. He pointed out that 86% of the global population lives in LMICs, where access to diagnosis and care remains limited, adding that ~73% of diabetes cases in Africa remain undiagnosed as an example.
- Turning to obesity, Dr. Aamir emphasized that over one billion individuals are now living with obesity globally, with prevalence tripling in recent decades and affecting all organ systems. He also stressed the importance of ethnicity-specific risk assessment, noting that individuals of Asian ancestry develop higher metabolic risk at lower BMI thresholds due to greater visceral adiposity. He underscored the importance of global collaboration, through organizations such as the International Diabetes Federation (IDF), to better understand regional trends and expand access to technologies, including CGM, which he helped introduce in Pakistan. Dr. Aamir closed by urging clinicians, particularly in the US, to proactively screen diverse populations using appropriate BMI cutoffs and to address social determinants of health through multidisciplinary care and policy-level interventions.
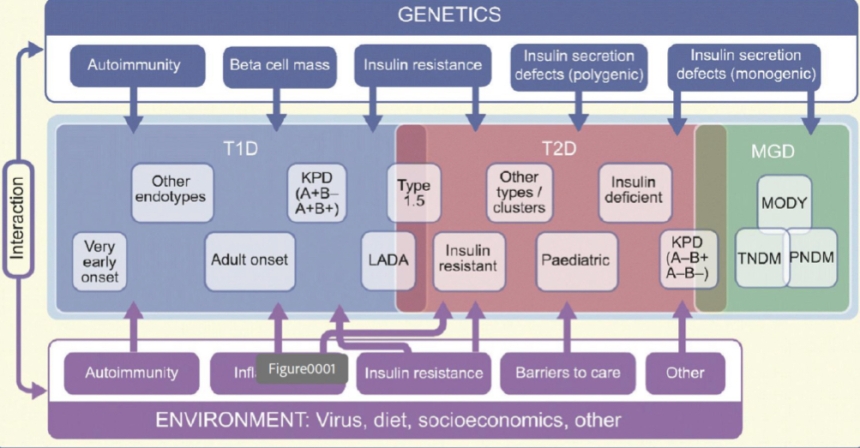
- Prof. Mehta characterized diabetes as a highly heterogeneous disease, with distinct genetic, metabolic, and clinical subtypes across populations that challenge traditional classification. Drawing on advances in molecular biology and population-level data, she proposed a framework of “endotypes” defined by underlying pathophysiology. Within T1D, she described variation in autoimmune activity and beta cell decline, such as rapid early-onset versus slower later-onset forms, noting that these differences influence complications and treatment response. In T2D, she discussed population-specific genetic and metabolic differences, including genetic variants such as SLC16A11 in Mexico and distinct genetic risk loci in sub-Saharan African populations. She also said there is substantial heterogeneity within Asian populations, with South Asians developing insulin resistance earlier and East Asians exhibiting lipodystrophy-like fat distribution.
- Importantly, she underscored the rising burden of young-onset T2D, particularly in Asian, Hispanic, and Indigenous populations, which is associated with significantly higher cardiovascular and renal risk and reduced life expectancy, citing evidence that with each decade earlier diagnosis linked to ~3-4 years shorter lifespan. Dr. Mehta also discussed emerging subtypes such as: (i) ketone-prone diabetes; (ii) fibrocalculous pancreatic diabetes; and (iii) type 5 diabetes (malnutrition-related), further underscoring the need for region-specific research, registries, and phenotyping to enable equitable precision medicine.
- Dr. Chowdhury focused on the dual burden of under- and over-nutrition and the need for context-specific, systems-level approaches to diabetes and obesity care. Using India as a case study, he said that over 100 million individuals live with diabetes, with even larger populations affected by prediabetes and obesity. He argued that global efforts to curb obesity have fallen short, with no country successfully reversing rising prevalence. Dr. Chowdhury attributed this in part to cultural and socioeconomic drivers, including perceptions of obesity as a sign of prosperity and limited access to healthy foods in LMICs. He also questioned the reliance on BMI alone, advocating for additional metrics such as waist circumference or waist-height index (WHI) to better assess metabolic risk.
- On management, Dr. Chowdhury positioned lifestyle interventions as foundational, citing modeling data suggesting that replacing 5% of carbohydrates with protein could reduce T2D risk by ~20% in Indian populations. While newer therapies such as GLP-1 RAs are gaining traction, he acknowledged that sulfonylureas remain widely used, reflecting real-world cost constraints. He concluded by calling for policy-level action to improve affordability and access, while suggesting precision medicine and AI as future priorities requiring global investment.
4. Interdisciplinary strategies to detect and treat “at‑risk MASH”
In this packed session, moderated by Dr. Kenneth Cusi (University of Florida), specialists across hepatology, weight management, and endocrinology talked about the bidirectional relationship between diabetes and metabolic liver disease. They emphasized the urgency of at‑risk MASH, which they described as early-stage MASH which is identified before cirrhosis develops. Dr. Cusi emphasized that the precursor to MASH, MASLD, is now a global epidemic. In endocrine clinics, Dr. Cusi showed that roughly one in five people with T2D also exhibit F2 fibrosis, indicating moderate liver damage, and 14% have F3 or severe fibrosis. He highlighted how diabetes and MASLD/MASH synergize, each amplifying insulin resistance, inflammation, and fibrosis progression. Importantly, he urged clinicians to screen proactively and recognize that cardiometabolic therapies increasingly serve a dual purpose as treatments of the liver as well.
- In hepatology, Dr. Mary Rinella (University of Chicago) traced the field’s evolution from exclusion‑based fatty liver labels to the new MASLD/MASH nomenclature, designed to positively identify disease, reduce stigma, and align with decades of data. She walked through the modern diagnostic framework, including noninvasive tests like FIB‑4 score, Vibration-Controlled Transient Elastography (VCTE) or FibroScan, and Enhanced Liver Fibrosis (ELF) score. She highlighted their strengths, with FIB‑4 as an accessible first‑line tool, VCTE providing quantitative liver stiffness measurement, and ELF capturing fibrosis‑related biomarkers. In terms of limitations, she discussed reduced reliability in high‑risk groups like diabetes and the need for secondary testing or confirmatory imaging when results are discordant. This stepwise approach helps clinicians determine which patients can be managed in primary or endocrine care and which require hepatology referral or further evaluation.
- In weight management, Dr. Holly Lofton (NYU) focused on how obesity clinics can operationalize MASLD screening at scale. She discussed the American Gastroenterological Association Clinical Care Pathway, including embedding FIB‑4 scores into EMR workflows, using VCTE or ELF scores as routine second‑line tools, and stratifying patients by fibrosis stage to determine who can remain in weight‑management care versus who requires hepatology referral. Dr. Lofton emphasized that lifestyle therapy remains foundational, especially given that 7-10% weight loss can drive steatosis, inflammation, and even fibrosis regression, but noted that these approaches are often difficult to sustain and may not achieve the desired metabolic or hepatic improvements. As a result, she integrates medications and, when appropriate, metabolic surgery into her management strategy.
- In endocrinology, Dr. Scott Isaacs (Emory University) discussed the growing evidence base for diabetes medications with liver benefits. He highlighted semaglutide’s strong histologic effects (MASH resolution in 63% vs. 34% with placebo; NNT ~3) and fibrosis improvement in 37% vs. 22% with placebo (NNT ~7). He pointed to SGLT-2 inhibitors, which reduce liver fat independent of weight loss, and to resmetirom, which demonstrated MASH resolution in up to 30% and fibrosis improvement in up to 26% (vs. 10% and 14% with placebo, respectively). He also noted that pioglitazone remains an option for treating MASH in adults with T2D, also demonstrating confirmed benefit on liver enzymes and liver stiffness. He then highlighted next‑generation incretin therapies, including tirzepatide, survodutide, and retatrutide, as well as FGF21 agonists such as efruxifermin and pegozafermin, and pan‑PPAR agonists like lanifibranor. He described these agents as “massive metabolic regulators” poised to reshape the MASH treatment paradigm over the next several years.
5. CKM discussion continues: Dr. Rodolfo Galindo emphasizes metabolic complexity and the need for standardized interpretation
In this packed afternoon session on continuous ketone monitoring (CKM), Dr. Rodolfo Galindo (University of Miami) revisited a familiar theme from recent meetings: while CKM technology is advancing quickly, clinical interpretation remains in early stages. Moving beyond device mechanics, Dr. Galindo centered his talk on what continuous ketone data is already revealing. Specifically, ketone physiology may be more dynamic and not consistently linked to glucose solely. He also highlighted emerging evidence that elevated levels of ketones may or may not precede hyperglycemia, suggesting CKM could eventually help earlier detection of diabetic ketoacidosis (DKA) compared to current approaches.
- CKM technology is progressing, but validation remains limited and lacks standardized benchmarks. Dr. Galindo reviewed early validation work in small cohort studies showing reasonable agreement between sensor-derived and capillary beta-hydroxybutyrate. However, unlike CGM, there are no established accuracy standards or regulatory frameworks for CKM, making it difficult to interpret performance across devices. Multiple systems are already in development globally, including Abbott's DGKM (dual glucose ketone monitoring) and SiBio’s (available in Europe) CKM in the next 12-18 months.
- Continuous data suggest ketones may rise before glucose reaches conventional hyperglycemia thresholds, challenging current DKA paradigms. Echoing prior ATTD discussions, Dr. Galindo highlighted insulin suspension experiments showing a highly variable relationship between glucose and ketones, ranging from tight coupling to near independence of the two measures. These findings challenge the conventional model of hyperglycemia-driven ketogenesis and suggest additional physiologic drivers that CKM may help uncover over time.
- A key barrier is the lack of standardized thresholds and actionable frameworks for CKM data. While traditional cutoffs exist, Dr. Galindo stressed the need to redefine “elevated” and “high-risk” ketone levels in a continuous monitoring context, including appropriate alert thresholds and clinical responses. Early proposals suggest tiered alerts, but consensus is still evolving, particularly for integration into AID systems.
6. Dexcom product theater showcases CGM portfolio, evidence in non-insulin T2D, and Smart Basal titration platform
In Dexcom’s early morning product theater, Drs. Daniel Katselnik (Diabetes and Metabolism Specialists) and Matthew Corcoran (Shore Physicians Group Endocrinology) outlined Dexcom’s growing CGM portfolio and the company’s push into earlier T2D management. The session focused on three themes: (i) AACE-supported momentum for earlier CGM use in T2D; (ii) real-world evidence supporting CGM in adults with non-insulin-using T2D; and (iii) Dexcom Smart Basal, a CGM-guided basal insulin titration program designed to reduce user burden.
- Dr. Katselnik emphasized earlier CGM adoption in T2D, supported by the latest AACE guidance and real-world evidence. He noted that only ~16% of adults with T2D in the US currently use CGM, underscoring significant room for growth. Against this backdrop, he walked through Dexcom’s product lineup, including the standard 10-day G7, the newer G7 15 Day, and the over-the-counter Stelo CGM. The G7 15 Day received particular attention, with a focus on its longer wear time, improved software performance, and strong accuracy profile highlighted as meaningful upgrades for both clinicians and users.
- The speakers also touched on Stelo and Dexcom’s efforts to extend CGM earlier in T2D management algorithms. Dr. Katselnik pointed to recent Stelo updates and growing discussion around prediabetes as more than a “risk state,” suggesting that earlier insights into glycemia could prompt behavioral change and potentially alter disease progression.
- Dr. Katselnik reviewed results from the Dexcom Global Registry study, which includes CGM-naïve adults with T2D (n=318) across 10 US primary care sites. First presented at ATTD last month, results found that CGM use led to a rapid A1c reduction of 0.5 percentage points from a baseline of 7.4%, reaching a ~0.7 percentage point reduction at one year. Benefits were consistent across age groups, with greater improvements observed in those already using GLP-1 RAs, suggesting complementary effects. Real-world adherence was high and participants reported reduced diabetes distress and modest weight loss (~2.4 kg). Together, these findings reinforce CGM’s role as both a behavioral and therapeutic tool primary care settings.
- Dr. Corcoran introduced Dexcom Smart Basal as a CGM-guided solution to delayed insulin initiation and under-titration. Built within Dexcom Clarity and using the G7 15 Day CGM, the program generates personalized daily basal insulin recommendations based on CGM data and logged doses, with patients prompted to take and log doses over 90 days. His overview mirrored ATTD discussions of CGM-enabled titration, where faster optimization of basal insulin was associated with improved glycemic outcomes. The platform is designed to address a persistent barrier in T2D management, of delayed insulin initiation and under-titration once basal insulin is started.
7. Diabetes Year in Review: Treatment algorithm improvements for better care across T1D and T2D
In this morning session, Dr. Priyathama Vellanki (Emory University) and Dr. William Horton (UVA Health) offered a “Year in Review” focused on diabetes. They described the evolving therapeutic landscape in diabetes care, shifting from glucose-centric management toward a more complication-focused and individualized approach.
- Dr. Vellanki focused on contemporary treatment algorithms, which continue to prioritize cardiometabolic risk reduction. Recent CVOTs, including head-to-head comparisons of incretin-based therapies, reinforce the noninferiority of newer dual agonists while suggesting modest benefits in all-cause mortality. She reviewed pivotal trials such as SURPASS-CVOT, which demonstrated that tirzepatide is noninferior to dulaglutide in reducing major adverse cardiovascular events. Her discussion extended to the growing burden of MASLD and the ESSENCE trial, which provided evidence for semaglutide’s role in histologic improvement of steatohepatitis and fibrosis. Dr. Vellanki also highlighted distinctions between peptide- and small-molecule GLP-1 therapies, including differences in bioavailability, administration constraints, and off-target effects. Trials such as ACHIEVE-1 and ACHIEVE-3 illustrated the clinical potential of orforglipron in lowering A1c and promoting sustained weight loss in T2D. She underscored age-related differences in disease progression, noting accelerated beta-cell decline in youth and the promising efficacy of tirzepatide in pediatric populations. Finally, she addressed real-world challenges, including high discontinuation rates of GLP-1 RAs and the associated increase in cardiovascular risk, reinforcing the importance of sustained treatment adherence.
- Dr. Horton focused on advances in T1D, particularly in disease-modifying and potentially curative therapies. He highlighted the growing role of immunotherapy in delaying disease onset, with agents such as Tzield (teplizumab) demonstrating the ability to delay progression from stage 2 to stage 3 T1D by a median of two years. Emerging real-world evidence supports its clinical efficacy and safety beyond randomized controlled trials, while pediatric studies suggest even greater benefit when used earlier in the disease course. Dr. Horton also explored cutting-edge developments in cellular therapies, including stem cell-derived islet cell replacement strategies. Early-phase studies of therapies such as Vertex’s zimislecel (formerly VX-880) show dramatic reductions (93%) in exogenous insulin requirements and restoration of endogenous insulin secretion, albeit with the ongoing challenge of immunosuppression. Novel approaches, including hypoimmune stem cell technologies, aim to overcome these barriers and improve scalability. Collectively, these advances signal a paradigm shift in T1D management, moving beyond glycemic management toward disease modification and potential functional cure.
8. Dr. Michelle Look on exercise and nutrition recommendations during GLP-1 RA/GIP therapy for obesity
Dr. Michelle Look (Knownwell, Boston, MA) delivered clinical insights on managing the risk of sarcopenia for patients using GLP-1 RA and GIPs for obesity. Dr. Look began with a review of GLP-1 RA/GIP therapies, stating that the degree of total body weight loss now achievable with these medications was once seen only with bariatric surgery. While incretin therapies are highly effective for weight loss, she challenged the attendees to move beyond the scale towards treatment goals, patient-centered motivations, functional outcomes, and body composition as decision-making factors. While the clinical objective is to reduce fat mass while preserving lean mass, weight loss observed with incretin-based therapies follows an approximate 3:1 ratio of fat to lean mass loss, leading to challenges in lean mass maintenance. Importantly, she cited data from the SEMALEAN study (n=106), which suggested that incretin-based therapies are associated with improvements in function, despite lean mass decline.
- Dr. Look said that clinicians should screen for sarcopenic obesity and assess body composition before initiating GLP-1RA/GIP therapy. Populations at greatest risk for excessive lean mass include: (i) individuals with a BMI <35 kg/m2; (ii) older individuals with sarcopenic obesity; and (iii) older women. Data from the SELECT trial (n=17,604) identified an increased fracture risk associated with semaglutide use in older patients. She emphasized that baseline assessments should include evaluations for food insecurity and malnutrition risk, as well as body composition and other risk factors for sarcopenia.
- She also highlighted how dietary protein and structured exercise can attenuate the loss of lean mass, making lifestyle modifications an essential complement to therapy. Dr. Look outlined evidence-based nutritional targets to support lean mass preservation during weight loss. Counseling should meet patients at their level of health literacy, and she recommended using visual aids, such as portion guides based on hand size, and emphasized the healthy plate strategy rather than calorie-counting or similarly restrictive frameworks. She also emphasized practical strategies for preventing excessive lean mass loss, including slowing the rate of weight loss via slower titration, incorporating resistance training as an adjunct to treatment, and titrating therapy to each patient’s individual treatment goal rather than a fixed target weight.
- Importantly, Dr. Look emphasized that physical activity guidance should be accessible and framed with habit-forming language. Dr. Look reinforced that any movement is preferable to none, and that the goal of physical activity counseling is to help patients develop habits that no longer require conscious effort. Seated exercises, such as ankle pumps and glute squeezes, and standing exercises, such as the modified plank, can serve as entry points for patients who have been largely sedentary and can help build confidence before progressing to more structured resistance training programs.
9. Cardiometabolic “Year in Review”: Evolving lipid therapy guidelines and cardiometabolic strategies for long‑term risk reduction
In this “Year in Review” session, moderated by Dr. Javier Morales (Hofstra University), Dr. Abhishek Shrivastava (R&R Hormone Clinic and National Hospital, India) delivered an update on cardiometabolic and lipid science. Dr. Shrivastava opened by emphasizing how the field has shifted from glucocentric diabetes care to a broader, adiposity‑centric cardiometabolic framework that integrates obesity biology, insulin resistance, inflammation, lipoprotein pathology, and ASCVD risk. He positioned the updated AACE Integrated Cardiometabolic Model as the clearest expression of this shift, noting that modern care requires treating interconnected metabolic diseases together rather than managing diabetes, lipids, hypertension, fatty liver, and obesity in isolation.
- He reviewed the major changes in AACE’s dyslipidemia guidance, including the move away from rigid LDL‑c targets and toward outcomes‑based decision‑making that prioritizes ApoB, Lp(a), non‑HDL‑c, and global atherometabolic risk. He underscored that residual risk persists even when LDL appears controlled, and that particle number and inflammation often remain unaddressed in traditional approaches.
- Throughout the session, Dr. Shrivastava highlighted the most influential trials shaping current practice. He reviewed the FOURIER trial, which showed a 59% LDL reduction with evolocumab and a 15% reduction in major cardiovascular events, and ODYSSEY OUTCOMES trial, which demonstrated significant event reduction with alirocumab in post‑ACS patients.
- On PCSK9 inhibitors, he emphasized the importance of VESALIUS‑CV, which extended PCSK9 inhibitor benefits into high‑risk primary prevention with roughly a 25% reduction in major events. He also discussed the CORALreef trial of the first oral PCSK9 inhibitor, enlicitide, which achieved LDL reductions of about 55-60% and may broaden access to PCSK9‑based therapy. Inclisiran’s twice‑yearly maintenance dosing and sustained LDL lowering were highlighted through the ORION‑9/10/11 program.
- For statin‑intolerant patients, he reviewed the CLEAR Outcomes trial, which showed that bempedoic acid reduced LDL by about 20% and lowered major cardiovascular events, myocardial infarction, and revascularization. He also summarized supporting evidence from CLEAR Wisdom, Serenity, and Tranquility, including the enhanced LDL reduction seen with the bempedoic acid-ezetimibe combination.
- Dr. Shrivastava emphasized that hypertriglyceridemia is now recognized as a causal contributor to ASCVD rather than a secondary marker, noting that triglyceride‑rich lipoproteins directly participate in atherogenesis. He highlighted evidence showing that triglyceride-rich lipoproteins enter the arterial wall, drive inflammation, and contribute to residual cardiovascular risk even when LDL‑C is controlled. This shift reframes elevated triglycerides as an active disease process tied to insulin resistance, obesity, and metabolic dysfunction. Across the session, he underscored that cardiometabolic conditions share common biological pathways and that effective care requires addressing them together rather than as isolated problems.
10. AACE’s prediabetes algorithm: Case studies to demonstrate efficacy
In this popular morning session, Dr. Scott Isaacs (Emory University) presented prediabetes as a heterogeneous, high-risk metabolic condition that exists along a continuum of dysglycemia rather than as a discrete diagnostic threshold. Using the recently published AACE Diabetes Classification Algorithm, Dr. Isaacs presented three distinct clinical scenarios: (i) classical insulin-resistant prediabetes (e.g., associated with obesity and polycystic ovary syndrome); (ii) early-stage T1D; and (iii) mild autonomous cortisol secretion (MACS) driving dysglycemia. He framed prediabetes as a pathophysiologic state characterized by insulin resistance, impaired glucose uptake in skeletal muscle, compensatory hepatic glucose overproduction, and progressive beta cell dysfunction. Despite its high prevalence in the US, 80% of prediabetes cases remain undiagnosed, underscoring the importance of systematic screening and careful interpretation of diagnostic tools such as A1c.
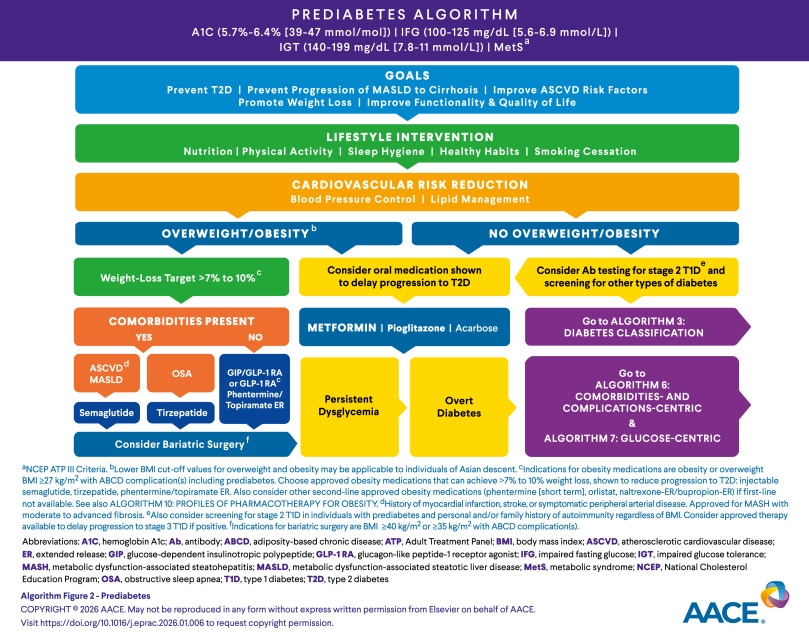
- Evidence from large prevention trials supports lifestyle intervention as the cornerstone of therapy, with a 7-10% reduction in body weight significantly lowering the risk of progression to T2D. However, Dr. Isaacs emphasized that lifestyle modification alone is often insufficient. He used the three case studies to describe how he would intervene in specific situations, with escalation to therapy as dictated by the above guidelines.
11. Nutrition & Obesity Year in Review: Obesity care moves beyond BMI as pharmacologic options accelerate and nutrition remains foundational
In this afternoon session, Dr. Elizabeth Bauer (Naval Medical Center San Diego) delivered a “Year in Review” focused on obesity and nutrition. Her talk spanned the updated AACE 2025 obesity framework, emerging pharmacologic agents, bariatric surgical outcomes, and the latest nutrition evidence, offering a comprehensive view of a field rapidly expanding its treatment options.
- Dr. Bauer discussed the updated AACE Obesity Algorithm, which reframes obesity care. The update incorporates the ABCD framework and redefines obesity as a chronic, progressive disease. A greater emphasis is placed on waist-to-height ratio as a measure of adiposity, along with the integration of lifestyle counseling into care. This signals the field’s movement toward using adiposity distribution and obesity-related complications to guide treatment decisions, rather than BMI alone, which does not capture different metabolic profiles and complication burdens across individuals. Recent literature also suggests that waist-to-height ratio may be a more relevant and accurate measure than BMI in assessing the risk and impact of obesity.
- The second part of the talk focused on trials that have reshaped the obesity landscape. Dr. Bauer reviewed clinical trial data for incretin‑based and multi‑receptor agents, starting with the Chinese phase 3 GLORY-1 trial of mazdutide in people with obesity. In SURMOUNT‑5, tirzepatide produced greater weight reduction than semaglutide with comparable gastrointestinal side‑effect profiles, suggesting improved efficacy without additional adverse effects. She also discussed the REDEFINE‑1 program, which evaluated CagriSema, positioning this emerging adjunct therapy as beneficial for patients who plateau on GLP-1 RA therapy alone. OASIS-4 showed clinically meaningful weight loss with oral semaglutide, supporting its FDA approval. Finally, MariTide, a once-monthly long-acting GLP-1 RA analog, showed substantial weight loss with infrequent dosing capacity.
- On the surgical side, UK comparative and long-term data suggest a fairly clear hierarchy. Gastric banding carries the highest complication burden, while sleeve gastrectomy and Roux-en-Y gastric bypass both provide durable weight loss but differ in their long-term risk profiles, including GERD risk and the need for revisional surgery, as seen in results from the SM-BOSS trial.
- On the nutrition side, Dr. Bauer briefly discussed a consensus statement outlining dietary recommendations for patients on anti-obesity medications, with key themes including: (i) nutrient-dense intake; (ii) smaller, more frequent meals; (iii) adequate protein intake; and (iv) preservation of muscle and bone mass.
12. “Betting on basal”: Casino-themed night focused on how to improve odds for PWDs
In this evening symposium sponsored by Lilly and hosted by PeerView, attendees gathered for an engaging simulation followed by a discussion from leading KOLs on the current management paradigm for T2D. The program began with hands-on activities at gaming kiosks and “Build-a-Case” simulations, where participants were given random clinical scenarios and given the opportunity to apply clinical decision-making skills. The interactive opening experience was designed to help the audience think about persistent gaps in the management of T2D, particularly the underuse and suboptimal implementation of insulin therapy.
- This experiential component transitioned into a formal symposium in which Drs. Harpreet Bajaj (LMC Healthcare, Canada), Carol Wysham (University of Washington), and Athena Philis-Tsimikas (Scripps Health) presented on the evolving role of basal insulin within contemporary treatment paradigms. Dr. Bajaj, Dr. Philis-Tsimikas, and Dr. Wysham discussed the evidence about once-weekly insulins, citing clinical programs like QWINT and ONWARDS. Supported by before and after audience polls, the panel taught the audience of mostly clinicians about how to best incorporate once-weekly basal insulin in the management of T2D. They outlined clear approaches to improve treatment pathways, with a focus on newer therapies that can simplify care, support adherence, and lead to better outcomes for people with T2D. Importantly, more than one-third of patients (nearly 40%) with T2D require insulin over the course of the disease, yet many do not begin treatment at the optimal time. The faculty also highlighted a persistent concern in clinical practice: insulin is too often framed as a last resort or even as a threat, a perception that can delay initiation and undermine effective disease management.
--by Milenka Men, Riya Chatterjee, Kayla Mathieu, Monica Oxenreiter, and Kelly Close