ATTD-Asia 2025 Day #1 Highlights –
Executive Highlights
- The second annual ATTD-Asia conference opened in Singapore with more than 750 experts from over 50 countries gathering to explore global and regional advances in diabetes technology and therapy. Following Chinese University of Hong Kong’s Prof. Juliana Chan’s keynote on CGM in prediabetes and diabetes diagnosis, the opening ceremony featured a traditional zapin dance by about a half dozen performers, symbolizing unity, community, and Singapore’s multicultural heritage. The conference organizers also took the chance to preview the third annual ATTD-Asia, which will take place in Kyoto, Japan, in late 2026, generating excitement already for what’s still to come.
- Medtronic and Abbott each hosted pre-conference educational schools featuring insights in glycemic management across CGM and AID.
- Dr. Satish Garg (Barbara Davis Center) helped open Abbott School with cases highlighting the benefits of combining GLP-1 RAs with CGM in people with T2D and, notably, T1D. Profs. Pratik Choudhary (University of Leicester, UK) and Margaret McGill (Royal Prince Alfred Hospital, Australia) discussed using CGM insights to support behavioral health, and later, a panel explored the future of telehealth, AI, and health equity in endocrinology.
- Medtronic School covered a broad range of topics on AID. Prof. Petrovski showed that optimized MiniMed 780G settings are the simplest and most effective way to improve TIR without increasing hypoglycemia. Later, Prof. Ben Wheeler (University of Otago, New Zealand) discussed AID in children and the often-overlooked consequences of hyperglycemia, Dr. Goran Petrovski (Weill Cornell Medicine, Qatar) reviewed evolving glycemic management strategies for adolescents, and Dr. Viral Shah (Indiana University) presented on AID use in older adults.
- Prof. Juliana Chan delivered the opening keynote on whether CGM can aid in diagnosing prediabetes and diabetes. While OGTT remains the diagnostic gold standard, particularly for detecting impaired glucose tolerance, early CGM studies in people without diabetes highlight both potential benefits and key limitations. Ultimately, Prof. Chan emphasized that more evidence is needed before CGM metrics can be used for diagnosis or risk stratification.
- The meeting’s sole debate took place today, featuring Prof. Thomas Danne (Breakthrough T1D) and Prof. David O’Neal (University of Melbourne, Australia) on whether the diabetes ecosystem is ready for continuous ketone monitoring. Prof. Danne argued in favor, citing strong clinical need and emerging evidence. Prof. O’Neal conversely stressed remaining uncertainties as US regulatory review nears. Both referenced the international expert consensus on continuous ketone monitoring, which should be published “at any moment,” as an important early step toward implementation.
- In therapy, Dr. Jothydev Kesavadev (Jothydev’s Diabetes and Research Centre, India) reviewed obesity and liver disease, noting that MASLD can progress to MASH (≈15%), cirrhosis (20–30%), and hepatocellular carcinoma (1–3%), with cardiovascular disease remaining the leading cause of death in this population. He emphasized the need for screening in high-risk groups, those with type 2 diabetes, obesity, or a family history of MASLD/MASH/Cirrhosis using tools such as FIB-4, the ELF test, and FibroScan elastography. While FIB-4 is low-cost and practical for clinic use, he highlighted its reduced accuracy for moderate fibrosis and the need for lower cutoffs in Asian populations. Dr. Kesavadev underscored that weight loss remains the cornerstone of MASLD management, with 10–15% loss potentially reversing steatosis and 5-10% being a realistic target. He discussed the benefits of GLP-1 receptor agonists, especially semaglutide, which improves weight, glycemic control, inflammation, and liver histology, supported by the ESSENCE trial that led to its FDA approval for MASH treatment. He also noted strong evidence for tirzepatide’s metabolic and liver benefits, and highlighted resmetirom as an FDA-approved THR-β agonist for F2–F3 MASH[1], based on the MAESTRO-NASH trial. He concluded by summarizing current management recommendations prioritizing lifestyle modification, GLP-1 therapy, selective use of vitamin E, and bariatric surgery for non-responders.
The second annual ATTD-Asia conference is taking place in Singapore December 9-11. See our Resource Hub and Day-by-Day Preview for the most up-to-date source of conference reporting, as well as a look at what is coming next.
Table of Contents
-
Top Highlights
- 1. Opening session: Prof. Juliana Chan on OGTT and CGM in redefining prediabetes and diabetes
- 2. The case for continuous ketone monitoring: Profs. Thomas Danne and David O’Neal debate the diabetes ecosystem’s preparedness for this technology
- 3. Early gestational diabetes (eGDM) emerges as a distinct entity, prompting work to establish a global consensus
- 4. Medtronic School: How predictive automation, optimal settings, and flexible strategies drive glycemic outcomes
- 5. Medtronic School: AID across all ages: MiniMed 780G for children, adolescents, and the elderly
- 6. Medtronic School: AID for pregnancy and T2D; expanding uses and population-wide health
- 7. Abbott School: Dr. Satish Garg on the dual opportunity with CGM and GLP-1 RAs to optimize T1D and T2D management
- 8. Abbott School: Tips for translating glycemic data into actionable tasks
- 9. Abbott School: Panelists share visions of a future endocrinology clinic including AI, telehealth, precision medicine, and pharmacotherapy
- 10. Key opportunities to reshape the state of AID in Southeast Asia
- 11. Dr. Jothydev Kesavadev on MASLD/MASH pathophysiology, screening, and management
- 12. Real-world AID use in pregnancy demonstrates strong glycemic outcomes during the third trimester and when using pregnancy-specific algorithms
Top Highlights
1. Opening session: Prof. Juliana Chan on OGTT and CGM in redefining prediabetes and diabetes
ATTD-Asia 2025 opened its second annual meeting with a keynote from Prof. Juliana Chan (The Chinese University of Hong Kong), who examined whether CGM can meaningfully support in the diagnosis of prediabetes and diabetes. Prof. Chan said that prediabetes still represents an often-underrecognized state of health and questioned how CGM metrics might complement or refine current classifications. She argued that while CGM has played a critical role in diabetes management and is increasingly being studied in people without diabetes, the oral glucose tolerance test (OGTT) still stands as the diagnostic gold standard. She contrasted it with emerging data on CGM use in people without diabetes. Ultimately, she posed the question of how these tools, and the AI-driven analytics behind them, might reshape early detection, staging, and interventions strategies within diabetes management.
- OGTT remains the gold standard for diagnosing prediabetes and diabetes, especially for identifying impaired glucose tolerance. Prof. Chan reviewed decades of epidemiologic data showing that two-hour OGTT glucose results predict microvascular complications such as retinopathy, supporting the World Health Organization’s (WHO) continued reliance on OGTT for diagnostic criteria. She underscored that the ADA and WHO fully agree on the two-hour threshold of 200 mg/dL and said that the WHO does not formally use the term “prediabetes,” instead preferring “intermediate hyperglycemia.” WHO also does not support A1c metrics alone for prediabetes diagnosis. She also emphasized that OGTT reveals biologically distinct patters, reflecting differences in first- and second-phase insulin secretion and tissue-specific insulin resistance, which may have key therapeutic implications.
- Prof. Chan referenced landmark prevention trials such as the China Da Qing study, the US Diabetes Prevention Program (DPP), and the China DPP, which demonstrate that lifestyle intervention and metformin can delay diabetes onset in people with impaired glucose tolerance (IGT), but also come with risk and demands on resources. This reinforces the need to accurately identify truly high-risk individuals with prediabetes before implementing intensive interventions.
- Early CGM studies in people without diabetes demonstrate both the benefits and challenges of using interstitial glucose data for diagnosis or staging of diabetes. Referencing large CGM datasets, Prof. Chan showed that even individuals classified as normoglycemic by fasting glucose and A1c values spend some amount of time above 140 mg/dL and sometimes even above 180 mg/dL, raising the question of what constitutes “normal” Time in Range (TIR) and Time in Tight Range (TITR) in the general population. She discussed the Pre-D trial, where repeated OGTTs and simultaneous CGM use revealed poor concordance between A1c and OGTT, as well as overlap in high-glucose TIR across normoglycemia, prediabetes, and diabetes cohorts.
- Prof. Chan reviewed research comparing CGM and OGTT, demonstrating a consistent lag of often ~15 minutes or more between venous plasma glucose and interstitial glucose, as well as systematic CGM underestimation of plasma values. Prof. Chan presented Bland-Altman plots showing bias across time points, where only about half of individuals had close agreement between OGTT and CGM values. A study (n=20) comparing venous measurements to Abbott’s FreeStyle Libre 2 and Dexcom G6 in people without diabetes suggested these sensors are capable of excluding diabetes but are not accurate for confirming diagnosis when OGTT is the reference, with ~70% accuracy and notable bias in values at lower glucose levels. Together, these data suggest that CGM is not yet ready to replace OGTT for diagnosis, though it may add biological insight and help define meaningful CGM-derived thresholds in future.
- Prof. Chan closed by underscoring that the use of CGM metrics in people without diabetes still require more evidence before they can inform diagnosis or risk stratification. While CGM clearly captures meaningful biological trends, the prognostic significance of these metrics for progression from prediabetes to diabetes or for long-term complication risk remains unproven. She emphasized that intervention studies are essential to determine whether modifying abnormal CGM-derived patterns can actually change outcomes. Looking ahead, Prof. Chan said that multi-stage strategies combining risk scores, OGTT, biomarkers, and CGM may ultimately help support earlier identification and that cost and equity considerations remain essential.
2. The case for continuous ketone monitoring: Profs. Thomas Danne and David O’Neal debate the diabetes ecosystem’s preparedness for this technology
To help close out a year dominated by buzz around continuous ketone monitoring (CKM), Prof. Thomas Danne (Breakthrough T1D) and Prof. David O’Neal (University of Melbourne) took the stage to debate a central question: Is the diabetes ecosystem ready for this technology? Prof. Danne began with high optimism, pointing to the clear clinical need for CKM and growing bodies of evidence. Prof. O’Neal, in contrast, emphasized the many unknowns that still loom as US regulatory review approaches. A slight majority of the audience initially sided with Prof. Danne, saying they’d likely recommend DGK to about half of patients on intensive insulin therapy.
- Prof. Danne described DGK as deserving of the “breakthrough” label, arguing that international expert consensus on the practical application of continuous ketone monitoring – which he said would be published soon after the session concluded – should precede widespread launch rather than have to respond to it. While there are still open questions, he stressed that this shouldn’t stop the field from offering its best recommendations now with room to revise later.
- There is a clear clinical need for the technology. DKA remains far too common, with some estimates at 30–45% prevalence among children and 5–8% among adults with T1D, with wide variations by region and care setting. Because DKA affects both T1D and T2D, Prof. Danne argued that manufacturers will have no trouble identifying potential users, saying that “no one hospitalized with DKA should be discharged without DGK.” He named those with recurrent DKA as his ideal target cohort, as these individuals account for >20% of all DKA hospitalizations. DGK could meaningfully reduce hospitalizations and reduce system burden given the high cost of DKA admissions. He also highlighted DGK as a long-needed enabling technology of SGLT-2 inhibitor use in T1D, the only diabetes population that remains without access to this cardioprotective drug class. Beyond this, any patient on an insulin pump, those experiencing frequent hyperglycemia, or those with CVD history stand to benefit.
- Prof. Danne reviewed key components of the expert guidance, which includes recommendations for manufacturers and regulators. The consensus document calls for minimum accuracy and performance requirements for CKMs (Level B), including accuracy at different rates of ketone change (Level B). Trend arrows should reflect ketone changes of 0.4 mmol/L/hour (Level E), though Prof. O’Neal underscored that consensus has not yet been reached on what actions to recommend based on those arrows. Threshold-based actions, however, are clearer (>3.0 mmol/L for urgent action; <0.6 mmol/L may not need display). Prof. Danne also emphasized that ketone and glucose trends don’t always align, citing a blinded-sensor case shared by Dr. Bruce Bode (Atlanta Diabetes Association), and called on manufacturers to ensure data access for research (Level E) to help answer these unanswered questions.
- For healthcare professionals (HCPs), the guidance recommends identical CKM interpretation for T1D and T2D, with standardized terminology of: normal (<0.6 mmol/L), elevated (0.6-1.5 mmol/L), high (1.6-2.9 mmol/L), and urgent high (≥3.0 mmol/L) (Level C). Any actions should be guided by thresholds rather than trend arrows (Level E), unless in consultation with an HCP (Level E). Furthermore, all HCPs should receive education on interpreting shifting ketone levels and preventing DKA (Level B).
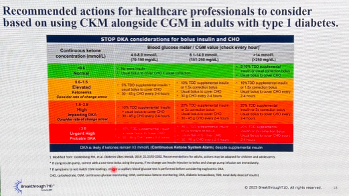
- On supporting daily use among people with diabetes, Prof. Danne acknowledged that alarm fatigue is a real risk with another analyte in the mix, but also that urgent alarms (>3.0 mmol/L) must not be missed. Education for both patients and HCPs will be essential, including reminders to trust clinical symptoms and confirm with blood ketones if sensor readings don’t match. The guidance also outlines recommended clinical responses using CKM values and CGM, building on STOP DKA principles for bolus insulin and carbohydrates (see figure below).
- Prof. O’Neal, meanwhile, approached the discussion much more cautiously, arguing that many foundational questions remain unresolved. Education platforms for HCPs and patients do not yet exist, and even a regulatory pathway for CKM has not been defined. Without established study requirements, he worries that regulators may accept data from non-target populations to validate performance at high ketone levels and questioned whether DGK will be reimbursed broadly for all people with T1D, or rather only for those deemed “high-risk” for DKA.
- To begin, Prof. O’Neal highlighted that sensor accuracy metrics will not be straightforward. He stressed that CGM accuracy standards cannot simply be applied universally to DGK. For example, misreporting 0.2 mmol/L as 0.5 mmol/L likely doesn’t matter clinically, leaving room for ambiguity in what accuracy actually means at low ketone levels. He pointed to early published accuracy data from Abbott and SiBionics reporting MARD values of 14.4% and ~20%, respectively, but without a consensus on acceptable MARD or an established error grid for ketones, these values are hard to interpret. Furthermore, while these MARD values can eventually be reported, there are no Error Grid Zones to support this accuracy data for the device yet. A clinically validated dynamic range for continuous ketone sensors recommending ambulatory care or hospitalization also remains undefined.
- To Prof. O’Neal, open questions about this technology abound. Chief among them: What happens if one analyte (glucose or ketones) fails more often than the other? How will DGK handle rapid changes or dehydration? Should devices display only actionable ketone levels, and what counts as actionable? Is there a clinical difference between 0.2 vs. 0.4 mmol/L rate-of-change arrows? Should alarm tones differ for clinical vs. technical alerts? And critically, where is the clinical evidence to support broad adoption? Some phase 2 studies are underway, but he doubted results would arrive before US launch.
- He also highlighted major deficits in ketosis literacy when it comes to successful technology implementation: only 28% of adults with T1D made “safe” choices in high-risk scenarios in one study; 32% of US adults with T1D do not use urine or blood ketone tests; and nearly half of surveyed Europeans with T1D could not name a single DKA symptom.
- Speaking next on integration challenges, he said that planned DGK systems will not initially integrate with AID, meaning that early adopters on AID may need both DGK and a standard CGM. However, we note several companies – including Sequel, Tandem, Beta Bionics, and Ypsomed and CamDiab’s, and Insulet – committed in the days surrounding ADA 2025 to plans to integrate with Abbott’s DGK upon launch.
- Speaking on a more optimistic note, Prof. O’Neal highlighted the CKM consortium that has been established to study the important question of SGLT-2 inhibitor use in T1D. This includes the study of: (i) ketosis risk with MDI and AID therapy with SGLT-2 doses; (ii) inpatient studies on the time course of ketosis with insulin withdrawal and carbohydrate requirements to reverse ketosis; (iii) ketone threshold that best predicts risk of urgent ketone levels; (iv) CKM accuracy; and (v) the effect of renal disease and dose of SGLT-1/2 inhibitors on ketosis events.
- To begin, Prof. O’Neal highlighted that sensor accuracy metrics will not be straightforward. He stressed that CGM accuracy standards cannot simply be applied universally to DGK. For example, misreporting 0.2 mmol/L as 0.5 mmol/L likely doesn’t matter clinically, leaving room for ambiguity in what accuracy actually means at low ketone levels. He pointed to early published accuracy data from Abbott and SiBionics reporting MARD values of 14.4% and ~20%, respectively, but without a consensus on acceptable MARD or an established error grid for ketones, these values are hard to interpret. Furthermore, while these MARD values can eventually be reported, there are no Error Grid Zones to support this accuracy data for the device yet. A clinically validated dynamic range for continuous ketone sensors recommending ambulatory care or hospitalization also remains undefined.
3. Early gestational diabetes (eGDM) emerges as a distinct entity, prompting work to establish a global consensus
Dr. Viswanathan Mohan (Dr. Mohan’s Diabetes Specialities Centre, India) outlined the growing evidence base identifying early gestational diabetes (eGDM), defined as hyperglycemia detected before 20 weeks of pregnancy that does not meet criteria for overt diabetes. Historically, GDM screening has occurred at 24-28 weeks of gestation, based on the assumption that placental insulin resistance increases before dysglycemia appears. However, Dr. Mohan said growing evidence from India, Australia, Europe, and elsewhere around the world shows that significant numbers of women exhibit abnormal fasting glucose levels not attributable to overt diabetes as early as the first trimester. Dr. Mohan said that this new eGDM state is associated with distinct metabolic features and that treatment is both beneficial and cost-effective.
- eGDM has emerged as a definable condition with distinct metabolic characteristics and high prevalence in South Asian populations. Dr. Mohan outlined the evolution of the diagnostic concept, beginning with the HAPO/IADSPG proposal in 2010. This suggested that first-trimester GDM could be defined by fasting plasma glucose ≥92 mg/dL and <126 mg/dL, although the lower threshold was later criticized as too sensitive. Despite this, global centers continued using similar thresholds, resulting in a large evidence base. The Stratification of Risk of Diabetes in Early pregnancy (STRiDE) study in over 3,000 pregnant women in India provided a clear comparison of eGDM (n=566), late GDM (n=359), and normal glucose tolerance (n=1,556). STRiDE found that women with eGDM had higher fasting glucose of 97 mg/dL, higher BMI and waist circumference, and reduced beta-cell function, even though A1c remained at normal levels of 5.3%. Follow-up analyses showed higher postpartum dysglycemia in those with eGDM compared to late GDM. These findings align with physiological studies demonstrating greater early impairment in insulin secretion, explaining why dysglycemia manifests earlier in pregnancy.
- The Treatment of Booking Gestational Diabetes Mellitus (TOBOGM) RCT (n=802) provided evidence that treating eGDM improves outcomes and is cost-effective. Women with fasting glucose in the range of 92-125 mg/dL were randomized to treatment (n=406) or control groups (n=396) in a fully blinded design. Dr. Mohan highlighted that treatment significantly reduced the composite outcome of preterm birth, respiratory distress, and neonatal complications. Subgroup analyses also found the largest effects in women who were diagnosed before 14 weeks’ gestation and had high fasting glucose ranges of 95-109 mg/dL. Dr. Mohan said an economic evaluation confirmed that early treatment also generated cost savings, driven by reduced neonatal morbidity.
- Global prevalence data show eGDM is particularly common in Asian populations, reinforcing the need for early screening strategies. In the national ICMR-INDIAB survey (a country-level prevalence estimate), nearly one in five pregnant women in India had eGDM, comparable to the 23% with late GDM. Across international populations, Asian subgroups showed the highest prevalence of both early and late GDM. Dr. Mohan highlighted physiological evidence that eGDM reflects severe early beta-cell dysfunction, explaining why metabolic abnormalities appear before 20 weeks.
- Dr. Mohan concluded that first-trimester screening should no longer be limited to ruling out preexisting diabetes but should actively identify eGDM. Multiple countries, such as Belgium and Australia, have already revised national recommendations in line with this conclusion. Dr. Mohan, who chairs the IDF International Consensus Group, including representatives from 20 countries, said that a formal statement with clear diagnostic and treatment recommendations is expected within the next four to five months. Looking ahead, Dr. Mohan stressed a simple message: screen early. With compelling evidence, early detection and treatment of eGDM appears to be both beneficial and cost effective, with the potential to improve pregnancy outcomes and reduce future diabetes burden for both mother and child.
4. Medtronic School: How predictive automation, optimal settings, and flexible strategies drive glycemic outcomes
Prof. Tadej Battelino (University of Medical Center Ljubljana, Slovenia) opened the 2025 Medtronic School with a focus on the growing role of predictive automation in managing the complexity of glucose. This set the stage for a rapid-fire series of presentations from Prof. Ohad Cohen (Medtronic), Prof. Goran Petrovski (Medtronic), Dr. Ben Nash (Medtronic), Prof. David O’Neal (University of Melbourne, Australia), and Dr. Dale Morrison (University of Melbourne) on how MiniMed 780G’s predictive algorithm paired with optimal settings can support strong glycemic outcomes in daily life.
- Prof. Cohen described how the MiniMed 780G algorithm uses real-time simulations that preview the next two to four hours before every insulin action. He reminded attendees that for the MiniMed 780G, the basal profile is recalculated every five minutes based on CGM trends. Key modules within the MiniMed 780G that help manage glycemic excursions from meals, exercise, and stress include the safe correction bolus and the safe meal bolus modules. A safe correction bolus module computes a correction dose, then runs a prediction for the next two hours; if hypoglycemia is predicted, the correction is automatically reduced. Similarly, a safe meal bolus module simulates four hours ahead and reduces the meal bolus if the full user-entered dose would cause glucose levels to fall too low. All these parameters are recalculated nightly.
- Prof.Cohen highlighted the “rule of two” for optimal settings: (i) a glucose target of 100 mg/dL; and (ii) an active insulin time (AIT) of two hours. Real-world data from nearly 400,000 MiniMed 780G users suggest that this combination of settings can raise mean TIR from the mid-70% range to ~80% without increasing hypoglycemia. Across RCTs and large real-world datasets, MiniMed 780G consistently delivers higher mean TIR than MDI, with comparable outcomes across geographies, genders, and ages.
- Prof. Petrovski showed that using optimal settings with the MiniMed 780G is the simplest, highest-yield method to improve TIR across ages without raising hypoglycemia risk. Building on Prof. Cohen’s review of the system’s algorithm, Prof. Petrovski presented data in which MiniMed 780G users saw higher TIR with stable and low Time below Range (TBR). He said that this was unlike outcomes seen with MDI use, where lowering A1c often meant greater time spent in hypoglycemia. Prof. Petrovski also recommended specific glucose targets for different age groups, including: (i) 120 mg/dL for ages 2-6 years; (ii) 110 mg/dL for ages 7-15 years; and (iii) 100 mg/dL for ≥16 years. He recommended an active insulin time (AIT) of two hours regardless of age. Pivotal trial and real-world datasets have demonstrated that a two-hour AIT supports ~80% TIR with ~3% TBR. He further outlined case examples illustrating that switching from non-optimal to optimal settings with MiniMed 780G improves TIR by ~2%, while system features like meal detection and more aggressive auto corrections allow the system to maintain TIR ~80% even with missed or under-estimated meals.
- Dr. Nash demonstrated how MiniMed 780G’s safety modules, meal detection, and auto corrections make meal management more flexible without sacrificing guideline-recommended TIR goals. He reiterated that pre-bolusing ~20 minutes before meals remains the recommendation, but in a study with standardized 60-gram carbohydrate meals, giving 50% of the bolus within 60 minutes after eating still significantly improved four-hour TIR compared to missing a bolus, with comparable hypoglycemia. Adult and pediatric data also show that unannounced snacks of up to 20 grams of carbohydrates can be safely managed by the algorithm with a similar outcome compared to an announced meal of 20 grams, while the “Fix vs. Flex” RCT (n=34) found that a simplified meal scheme achieved TIR of 73.5% – meeting ADA recommendations – suggesting that not everyone needs precise carbohydrate counting to benefit from AID. Relatively similar five-hour glucose profiles were seen among those employing strategies that included: (i) manual mode; (ii) accurate carbohydrate counting in Auto Mode; and (iii) simplified counting for managing complex meals. Finally, Dr. Nash highlighted the safety of MiniMed 780G when fasting during Ramadan, showing CareLink data (n=449) demonstrating stable TIR before, during, and after fasting.
- Prof. O’Neal and Dr. Morrison outlined a practical strategy for using MiniMed 780G during exercise, emphasizing the importance of minimizing insulin on board and tailoring targets. Prof. O’Neal said that hypoglycemia risk is driven by several factors, including starting glucose, glucose rate of change, insulin on board, exercise type, and time of day. Moderate afternoon exercise tends to lower glucose and high-intensity or resistance training may raise glucose due to stronger counter regulatory hormone responses. He noted that morning fasted exercises carry the lowest risk for hypoglycemia. For MiniMed 780G, Prof. O’Neal recommended avoiding full meal boluses within two hours of exercise. If a meal is needed, he recommended reducing the bolus by 25% (by announcing 25% fewer carbohydrates) and starting the temporary target (TT) at the meal to both raise the target and turn off auto corrections. Dr. Morrison then focused on the post-exercise period and prolonged exercise, showing that high-intensity and resistance workouts create a six to 12-hour window of heightened insulin sensitivity in which full meal boluses significantly increase hypoglycemia risk. He reiterated the recommended 25% announced meal bolus reductions in that window and suggested consuming 30-60 grams of carbohydrates per hour for exercise lasting over an hour, citing case studies with ~100% TIR during a 90-minute cycling exercise when TT and structured carbohydrate dosing were used. Both Prof. O’Neal and Dr. Morrison concluded that successful use of MiniMed 780G still depends on education and tailored plans that align strategies with each person’s goals and risk tolerance.
5. Medtronic School: AID across all ages: MiniMed 780G for children, adolescents, and the elderly
Medtronic’s school featured a lively discussion of AID management across a range of patient ages, with an emphasis on family education throughout the session. First, Prof. Ben Wheeler (University of Otago, New Zealand) discussed the use of AID in children, emphasizing the often-overlooked consequences of hyperglycemia. He described how caregivers often prioritize the prevention of hypoglycemia in children due to risk of hospitalization or death, which can inadvertently lead to hyperglycemia and its long-term consequences. As children age, so too do glycemic management strategies, which Dr. Goran Petrovski (Weill Cornell Medicine, Qatar) next described with respect to adolescent patients. He discussed strategies for transitioning to AID from MDI in this population and the ability for adolescents to achieve excellent glycemic outcomes. Finally, Dr. Viral Shah (Indiana University) discussed AID for the elderly, drawing parallels between the role of parents in children’s diabetes care and the role of caregivers in diabetes care for the elderly. Above all, Dr. Shah carefully considers a risk-to-benefit ratio for each patient to tailor glycemic management.
- Dr. Wheeler discussed the sobering consequences of hyperglycemia in young children and the opportunities that AID provides. A 2024 study found that less than half of children under six years old have reached a target A1c value of ≤7.0%, with only 44% of children in Europe, 26% of children in the US, and 28% of children in Australia having achieved this important goal. This persists despite relatively high use of diabetes technology in some regions, with 87% of children in Europe using insulin pumps and 85% using CGM. These metrics suggest that hyperglycemia remains a key concern in young children, although fear of hypoglycemia is often cited as the primary cause of diabetes distress in their parents. Dr. Wheeler cited research showing that hyperglycemia has severe effects on the developing brains with children and is associated with cognitive impairment and brain damage. Acute and chronic hyperglycemia also impairs spatial working memory, in addition to broader effects on cardiovascular health and other related conditions. This leads Dr. Wheeler to seek to minimize hyperglycemia in children while still adequately managing hypoglycemia.
- While the management of T1D in very young children is challenging due to physiological and behavioral reasons, AID systems can adjust to unpredictability and improve outcomes for children. The LENNY study demonstrated an average of 2.4 more hours per day in Range using the MiniMed 780G system, along with a 10% decrease in hyperglycemia. However, Dr. Wheeler acknowledged the challenges of bolusing for children and provided key recommendations: (i) give a bolus 10-20 minutes before meals or snacks containing carbohydrates; (ii) deliver a 50% missed bolus only within 30 minutes of a meal; and (iii) if uncertain if the child will finish the meal, bolus before the meal for a portion of the carbohydrates you expect them to eat and later deliver a correction bolus if recommended by the system. By using these techniques, Dr. Wheeler is confident in the ability of AID to help adjust to the unpredictable lives of young children.
- Prof. Petrovski discussed robust data showing the glycemic benefits of AID for adolescents. A 2022 study demonstrated a 38% increase to TIR in just seven days after transitioning from MDI to AID in adolescents. Acknowledging lifestyle challenges in this population as well, Prof. Petrovski said that even a simplified meal management protocol can result in excellent glycemic results for adolescents. He also noted the ability of MiniMed 780G to adapt to cases ranging from COVID-19 infection and Ramadan fasting, maintaining strong glycemic management.
- Dr.Shah offered a “deep dive” into expanding AID to elderly populations. He began by saying that the number of older adults with diabetes is increasing, particularly with regard to rates of T1D. From 1990 to 2019, the global age standard prevalence of T1D has nearly tripled. Approximately four million people are 65 years of age or older, with the most rapid prevalence increase currently seen in North Africa and the Middle East. He discussed a number of challenges and opportunities in this population that warrant the use of AID, including increased risk of hypoglycemia, hypoglycemia unawareness, complications including reduced vision, risk of falls and fractures, social isolation, cognitive decline, and increased risk of CVD. He encouraged providers to first evaluate frailty in older adults as a marker for long-term health, and to then individualize goals based on frailty. For those with high functioning status, tighter glycemic management is reasonable, while other adults’ quality of life may be improved by lowering glycemic targets. In a 2018 study, Dr. Shah et al. found that severe hypoglycemia is associated with fall risk in older adults, which can have devastating long-term consequences in the elderly.
- With practical considerations, AID can offer key benefits for older adults. Dr. Shah encouraged providers to conduct in-person training with the families of elderly patients, and to understand that it may take a longer time to initiate AID. He also recommended vision, hearing, and tactile sensation assessments before beginning the use of an insulin pump. In all, AID may offer significant reductions to diabetes burden in the elderly and reduce the risk of falls and fractures.
6. Medtronic School: AID for pregnancy and T2D; expanding uses and population-wide health
Medtronic’s school continued to inspire as discussions of AID for T2D and pregnancy expanded the technology’s possibilities. Prof. Sarah Glastras (University of Sydney, Australia) provided compelling evidence on the technology’s benefit for the changing physiology of pregnancy and the importance of balancing glycemia with patient well-being. Building upon this complex use case, Dr. Viswanathan Mohan (Dr. Mohan’s Diabetes Specialities Centre, India) looked to a future of therapeutic possibility for over 100 million patients with T2D in India, exploring the potential benefits of AID.
- Prof. Glastras discussed the rapidly changing requirements of pregnancy and how AID can assist with navigating these changes. Diabetes management changes significantly during pregnancy. Prior to pregnancy, glycemic management has been associated with the risk of fetal malformations, meaning that glycemic planning must begin well in advance of pregnancy. In the first trimester, high glycemic variability and risk of severe hypoglycemia are observed, as well as unpredictable carbohydrate intake due to hyperemesis (severe vomiting). Hyperemesis may lead to hypoglycemia, as well as unstable insulin requirements due to hormonal changes in the first 16 weeks. In the second and third trimesters, insulin needs are higher due to increased insulin resistance after 16 weeks of gestation, as well as altered and delayed absorption of insulin at 16-20 weeks of gestation. Post-meal hyperglycemia has also been observed during this time period. Immediately following delivery, hypoglycemia risk is also high due to a sudden drop in insulin resistance and in insulin requirements after delivery. Lactation can also induce hypoglycemia.
- Several complications are associated with T1D and pregnancy. A 2019 study demonstrated that women with T1D see a 54% prevalence of large-for-gestational-age infants, as well as 25% prevalence of preterm delivery, 17% of preeclampsia, and 5% prevalence of infants with congenital malformations. These complications are associated with elevated A1c values during pregnancy, motivating tight glycemic management during pregnancy.
- Through the use of AID, therapy should be individualized to reach the lowest physiological glucose levels possible without causing severe hypoglycemia. Prof. Glastras recommended optimizing insulin-to-carbohydrate ratio, limiting carbohydrates with a high glycemic index, and increasing awareness that insulin resistance will increase throughout pregnancy, among other recommendations. In the landmark CRISTAL study, hybrid-closed loop AID use was associated with improved glycemic management intrapartum and similar glycemic management in the early postpartum period compared to standard insulin therapy. This was achieved without severe hypoglycemiaor DKA, and reduced TBR compared with standard of care. Echoing the morning’s other speakers, Prof. Glastras viewed MiniMed 780G’s adaptability as a key tool for the complexities of pregnancy.
- Dr. Mohan discussed compelling data on the use of AID in India, one of the world’s largest populations of people with diabetes. As of 2023, 101 million adults have T2D in India. Dr. Mohan quipped, “I dream of all 101 million of these people using the MiniMed 780G,” citing high potential for improvements to glycemic management. Specifically, he believes that AID would be highly beneficial for patients with a long duration of T2D and those already on insulin. In addition to T2D, an estimated 820,000 people have T1D in India. A compelling real-world study (n=25) published in 2023 found an excellent 83% TIR average among patients with T1D using MiniMed 780G in Auto Mode in India, which suggests that broader population health benefits can be achieved with AID. Currently, just 2,040 people are using MiniMed 780G in the country, of which approximately 10% have T2D. Dr. Mohan discussed the similar glycemic parameters observed between these subgroups, with people with T1D 15 years of age or younger having approximately 70% TIR, those 15 or older having 73% TIR, and people with T2D in India achieving 73% TIR on the system.
7. Abbott School: Dr. Satish Garg on the dual opportunity with CGM and GLP-1 RAs to optimize T1D and T2D management
Dr. Satish Garg (Barbara Davis Center) highlighted the critical role of CGM in managing both T1D and T2D, highlighting its ability to provide real-time glucose data, which leads to better decision-making and reduces the risk of dangerous glucose fluctuations. He also cited recently published data on how CGM in T2D not only improves day-to-day glucose management but also contributes to better long-term outcomes: over a two-year period, consistent use of CGM was associated with significant reductions in all-cause mortality, hospitalizations, and severe cardiovascular events. This data underscores the importance of CGM in diabetes management and sets the stage for further advancements in treatment, including adjunctive therapies.
- Dr. Garg largely focused on the use of GLP-1 RAs in T1D, a group that has been severely understudied in terms of adjunctive therapies. Despite over a century of using insulin in T1D and high risk for both cardiovascular disease (CVD) and renal disease in the population, there has been little progress in approving adjunct therapies for T1D. Regardless, Dr. Garg said that the Barbara Davis Center now treats more than 750 T1D patients using GLP-1 RAs, primarily tirzepatide due to its stronger efficacy. He then went on to detail some considerations when initiating GLP-1 RAs in T1D, saying that as the drug class primarily impacts postprandial glucose levels it is essential to adjust prandial and basal insulin doses proactively. When considering GLP-1 RAs for certain patients, Dr. Garg emphasized that some individuals should aim for targets even lower than the <7.0% recommended by the ADA Standards of Care, and the subsequent individual treatment plans could sometimes include the drug class. Achieving personal treatment is only possible with CGM use to guide more precise therapy administration. Presenting a couple case studies, Dr. Garg highlighted the dual benefits of CGM and tactful use of GLP-1 RAs in some of his patients:
- In a patient with T1D who had a starting TIR of 37%, adjustments to basal and bolus insulin after initiating CGM led to significant glycemic improvements – A1c of 7.5% and a TIR of 90% with 85 units/day – but was accompanied by weight gain of 10 lbs, bringing the patient’s weight to 225 lbs. This led Dr. Garg to pose the question: In T1D, is weight gain (leading to insulin resistance) or glycemic management the bigger issue? With many people with T1D living much longer, this is becoming an increasingly important question for individual care. While he did not have an answer to his question at his presentation today, he shared that tirzepatide initiation in his patient improved both outcomes after 1.5 years of use, losing 90 lbs and reducing total daily insulin to just 28 units/day.
- Dr. Garg also discussed the challenge of using BMI as a global metric to guide treatment decisions. For instance, a Chinese patient with a BMI of 22 kg/m² and weight of 118 lbs would be considered "normal" by Western standards (especially when paired with his A1c of 6.8%), yet CGM initiation revealed he had significant post-meal hyperglycemia. After starting semaglutide, the patient lost some weight, and TIR reached 94%.
- Dr. Garg discussed the importance of CGM in T2D management as well. He overviewed findings from his JAMA 2025 publication with Dr. Irl Hirsch, which analyzed data from over six million people with T2D in the Optum EMR database and demonstrated a marked difference in glycemic outcomes between those using CGM and those not using it. Namely, those using CGM saw a mean A1c drop of 0.8% greater than those without CGM (8.9% to 7.4% vs. 8.2%). He also emphasized that CGM and GLP-1 RAs are not an either-or debate in this population. The same cohort showed that GLP-1 RAs alone led to an average A1c reduction of 0.8% after one year, whereas combining CGM with GLP-1 therapy resulted in a 1.9% drop. Drawing on similar case studies in patients with T2D, Dr. Garg illustrated the importance of giving patients the “right medications” for the glycemic and personal issues they face, which can drastically improve their health outcomes, including considering tirzepatide for a greater chance of stronger outcomes and strong glycemic management.
8. Abbott School: Tips for translating glycemic data into actionable tasks
In this informative morning session, Profs. Pratik Choudhary (University of Leicester, UK) and Margaret McGill (Royal Prince Alfred Hospital, Australia) shared tips for using CGM insights to support behavioral health. The ADA Standards of Care states that “behavioral strategies should be used to support diabetes self-management and engagement in health behaviors.” A healthy lifestyle is associated with a 32% lower risk of developing microvascular complications. However, a majority (92%) of people with T2D struggle to adhere to self-management recommendations, including blood glucose monitoring (76%) and adherence to glycemic medications (46%). The speakers argued that CGM is a useful tool for promoting behavioral change, as it: (i) unblinds patients and clinicians to more glycemic data; (ii) allows for micro-experiments; (iii) reinforces positive behaviors; (iv) prompts actions through alarms; and (v) improves communication with healthcare teams. Most of all, Prof. Choudhary emphasized that one cannot change what one does not measure. Speaking to the audience, two-thirds of whom have not prescribed CGM in their practices, the speakers discussed how CGM data offer insights on how food, activity, stress, and medication use impacts glycemic levels in people with diabetes.
- When retrieving CGM data in patient visits, Prof. Choudhary said to first check the date, sensor usage, mean glucose, and glucose variability. For people without diabetes, glucose variability is <25%, while people with strong diabetes management or hybrid closed loop users will have variability of ~25-35%. Variability between 35-50% usually indicates that insulin could be taken at more ideal times for food intake. He said that most low TIR values could be attributed to: (i) missed boluses; (ii) late boluses; (iii) under bolusing; (iv) under-correction of highs; (v) over-correction of lows; or (vi) low rates of CGM use. Notably, if the CGM curve rises at an incline of over 45° after meals, it most likely means that the insulin dose arrived too late to maximize efficacy. He also introduced a common error by patients, “rage bolusing.” Rage bolusing refers to a large impulsive correction after prolonged hyperglycemia, followed by fear of hypoglycemia, eating too much to counter the insulin, and resulting rebound hyperglycemia. This cycle causes not only glycemic fluctuations but also diabetes distress.
- Prof. Choudhary introduced the 1-2-3 rule for interpreting glucose changes after a meal.
- The 1-hour post meal glucose tells patients if they got the timing of insulin right. If they managed to bolus early enough, they should have risen between 3-5 mmol/l (< 70-90 mg/dl), but if they were only able to bolus just as they ate, they would expect a rise of 6-8 mmol/l (140-180 mg/dl).
- The 2-hour post meal glucose tells patients if they took enough insulin. If they are high at two hours, they probably under-bolused and if they are <7 mmol (140mg/dl) and dropping, they probably need to take 4-8 gm carbohydrate to prevent a hypoglycemia.
- The 3-hour post meal glucose tells they about the fat and protein content. If they are still high and rising at three hours, the meal was high in fat with or without protein, and they probably need some extra insulin.
- Prof. Choudhary introduced the 1-2-3 rule for interpreting glucose changes after a meal.
- Ultimately, Prof. Choudhary said that fear of hypoglycemia is a remnant of self-monitoring of blood glucose (SMBG), with which patients used to “walk on a tight rope” while “blindfolded between capillary readings.” CGM takes away the blindfold, and AID makes the path for glycemic management wider.
- Speakers also discussed the weight of diabetes distress on patients, inundated by the number of decisions to be made each day, numerous data points, fear, and guilt. Prof. Choudhary advises patients to follow the “CHIEF” mnemonic: (i) CHeck; (ii) Inject; (iii) Eat; and (iv) Forget. Monitoring a rise in glucose over the first hour will likely induce anxiety in patients although it is an expected physiological process. It is best to scan CGM data before a meal and two hours post-meal. Finally, Prof. McGill said that clinicians only spend three hours on average with each patient each year, while patients spend 8,757 hours annually managing diabetes on their own. It is important for clinicians to acknowledge that diabetes management is challenging and to create an encouraging and nonjudgmental spaces for patients.
9. Abbott School: Panelists share visions of a future endocrinology clinic including AI, telehealth, precision medicine, and pharmacotherapy
The 2025 Abbott School concluded with an insightful panel discussion on what the future holds for endocrinology care. Prof. Ramzi Ajjan (University of Leeds, UK), Dr. Jothydev Kesavadev (Jothydev's Diabetes and Research Centre, India), and Dr. Margaret McGill (Royal Prince Alfred Hospital, Australia) presented clinical considerations for telehealth and hybrid care, while Prof. Pratik Choudhary (University of Leicester, UK) highlighted the importance of data integration amid a wealth of information. Dr. Noriko Kodani (National Center for Global Health and Medicine, Japan) discussed challenges with health equity, and Dr. Satish Garg (University of Colorado) shared how early screening and pharmacotherapy will shape T1D and T2D care. In all, the speakers underscored the importance of listening to the voices of people with diabetes and collaborating with stakeholders to improve accessibility.
- On telehealth and AI integration, Dr. Kesavadev shared his vision for the future by reflecting on the past. He developed the diabetes tele-management system (DTMS) in 1998 after recognizing that diabetes complications could be addressed with proactive care and faster treatment adjustments. DTMS has supported patients through the 24/7 availability of clinicians, nutritionists, and diabetes educators who provided real-time adjustments to medication dosage, diet, and education. Over time, this model lowered rates of complications, hospitalization, emergency visits, and healthcare costs. Dr. Kesavadev also integrated advanced technologies into his clinic, including insulin pumps and CGMs since 2004 and 2005, which has significantly improved diabetes management and remote communication. He is excited that CGM use continues to expand beyond people on insulin, such as those with prediabetes.
- Looking to the future, Dr. Kesavadev aims to integrate electronic health records, CGM, smart insulin, smartwatches, and AID systems data into a single DTMS. Using AI and machine learning (ML) on this abundant dataset can help clinicians detect early trends of complications and prioritize patients who need urgent intervention. He also hopes to conduct digital twin simulations, which can test multiple treatment regimens before applying to real life. While telehealth and technology can improve diabetes management, he still emphasized that physical visits are “mandatory” and critical parts of care.
- Prof. McGill similarly considers hybrid care to be the future of diabetes management. Data. From CGMs, smart pens, and pumps can be directly loaded onto the clinic dashboard, with AI flagging patterns of hypoglycemia and adherence challenges. In-person visits can be used for new diagnoses, technology education, or complication assessment. Prof. McGill cautioned that AI is meant to support, rather than to replace, clinicians. Separately, she believes that the medical field is headed toward personalized medicine using gene markers, microbiome profiling, and digital phenotyping to assess health risks and predict drug responses.
- Prof. Choudhary echoed this vision, especially regarding data integration to derive even better insights on glycemic trends, complications, and health risks. He hopes to see a patient prioritization dashboard that allows clinicians to meet with patients at risk in a timelier manner.
- On diabetes care, Prof. Ajjan and Dr. Garg shared insights on the future of T1D and T2D prevention, delay, and “cures.” For T1D, Prof. Ajjan considers a closed loop system and remote glycemic monitoring to be the immediate future. However, he also underscored the importance of addressing insulin resistance, which is often overlooked in this population. On a longer timescale, he is excited for continued advancements in immunotherapies and more effective beta-cell transplantation strategies. Dr. Garg advocated for antibody screening to identify people in early-stage T1D who may be eligible for Tzield (teplizumab), and accurately diagnose people, as 10-20% of people with “T2D” are misdiagnosed. He also wants to further explore the benefits of GLP-1 RA-based therapies in T1D – which have excitingly been included in the 2026 ADA Standards of Care published earlier this week.
- On T2D, both Prof. Ajjan and Dr. Garg advocated for CGM use, which would allow for early diagnosis, motivate behavioral changes, unveil glycemic abnormalities, and promote safe escalation and de-escalation of therapies. Dr. Garg also believes that people with “true T2D” may not require insulin anymore if they are appropriately treated with GLP-1 RAs early in disease progression.
- On health equity, Dr. Kodani said that clinics in Asia-Pacific should better understand the necessity of CGMs and strive for broader accessibility – especially given that the life expectancy of people with T1D in low-income countries is significantly lower than in high-income countries (13 versus 61 years). To ensure this, people with diabetes, clinicians, researchers, industry, policymakers, and diabetes organizations must collaborate to advocate for changes. Importantly, she emphasized that clinicians should “hear the voices of people with diabetes” and understand their lived experiences without exacerbating stigma and bias. Dr. Garg added that cost is often the barrier to distributing technologies to the masses.
10. Key opportunities to reshape the state of AID in Southeast Asia
Dr. Muhammad Yazid Jalaludin (University Malaya Medical Centre, Malaysia) discussed the need for AID in Southeast Asia and key areas of focus to promote the use of the technology. He began by noting that only 21% of the adult population reaches an A1c target of ≤7.0% with CGM alone, per a 2021 study. As a result, the 2024 International Society for Pediatric and Adolescent Diabetes (ISPAD) Clinical Practice Consensus Guidelines strongly recommend AID systems for youth with diabetes to improve TIR and reduce hyperglycemia. While international recommendations often serve as the first step towards increasing access to technology, Dr. Jalaludin said that real-world implementation continues to lag behind these recommendations, particularly in Southeast Asia. In a rousing call to action, Dr. Jalaludin urged attendees to consider major factors limiting AID adoption in the region.
- Dr. Jalaludin discussed five key factors that limit the implementation of AID in Southeast Asia.
- Economic and financial burdens arise from the high cost of AID technology, a lack of insurance coverage, and out-of-pocket payment burdens;
- Healthcare infrastructure often remains weak in the region, with limited access to endocrinologists and diabetes educators, poor rural healthcare access, and inadequate training of healthcare professionals in the use of advanced diabetes technology;
- Technological and regulatory restrictions may slow access, such as import restrictions or delays in device approval, a lack of local suppliers or device maintenance centers, and interoperability issues with local healthcare systems or EMR;
- Awareness and education around AID remain low among patients and general practitioners in the region, along with digital literacy gaps and cultural skepticism. Many residents of Southeast Asia remain skeptical of automated or foreign-made medical technology; and
- AID policy and government support for the technology have not yet been robustly established. An absence of national diabetes strategies focused on technology remains in the region, along with limited public-private partnerships for healthcare innovation and fragmented health policies across the region.
- Dr. Jalaludin said that reform to diabetes in Southeast Asian diabetes care must address all five of these factors with a stepwise rollout. He discussed government subsidies or tiered pricing models to improve affordability and public health insurance reforms to include diabetes technology. He also said that central procurement at a ministry or wholesale level can reduce costs and ensure uniform supply, and that infrastructure must also be strengthened, including telemedicine expansion, the establishment of diabetes centers in key hospitals, and incentives for specialists to work in underserved areas. Overall, he said that empowering diabetes care teams is essential, calling for hands on simulation and troubleshooting workshops, along with community health campaigns.
11. Dr. Jothydev Kesavadev on MASLD/MASH pathophysiology, screening, and management
In this afternoon session, Dr. Jothydev Kesavadev (Jothydev's Diabetes and Research Centre, India) delivered a comprehensive overview of obesity and liver diseases. Dr. Kesavadev began by positioning obesity as an adiposity-based chronic disease associated with over 229 complications, from T2D and hypertension to various cancers. This includes metabolic dysfunction-associated steatotic liver disease (MASLD), which affects ~30% of the global population, or over two billion people. Similar to other obesity-related complications that develop by systemic inflammation and fibrosis, MASLD is caused by excess caloric intake that increases free fatty acid and triglyceride accumulation in the liver (steatosis). Moreover, systemic increase in insulin resistance further promotes hepatic fat production, causing a vicious cycle. Steatotic liver disease then advances to metabolic dysfunction-associated steatohepatitis (MASH) with various stages of fibrosis (F1-F4), cirrhosis, and eventually critical disease states like hepatocellular carcinoma. While underscoring the need to address this disease, Dr. Kesavadev stressed that non-modifiable risk factors like genes (e.g., PNPLA3) contributes significantly to obesity (>40%) and MASLD (>60%), and that blame should not be directed to patients. In fact, to avoid stigmatizing language, the field introduced a new nomenclature for liver disease in 2023: MASLD and MASH, instead of the previously named non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH).
- Screening for advanced fibrosis is recommended for people with T2D (prevalence of 6-19%), obesity (4-33%), MASLD with moderate alcohol use (17%), or first-degree relative who has cirrhosis from MASLD or MASH (18%). Several non-invasive tests can be used, such as FIB-4 score, enhanced liver fibrosis (ELF), or elastography like FibroScan. Liver biopsies can also be conducted in high-risk populations.
- For Indians, who tend to develop metabolic dysfunction at lower BMI and younger age, a revised definition of obesity should be used for a more accurate risk stratification: BMI ≥23 kg/m2 without (stage 1) or with (stage 2) obesity-associated limitations of daily activities or comorbidities. Moreover, Dr. Kesavadev said that all Indians with T2D should undergo routine screening for MASLD, as prevalence rates reach 70-80%.
- Indians often have moderately elevated or normal liver enzyme levels despite steatosis or fibrosis; hence, FIB-4 score may not reliably predict disease state in this population. Dr. Kesavadev encouraged using lower thresholds for FIB-4 score to assess risk of fibrosis and conducting additional tests, like FibroScan.
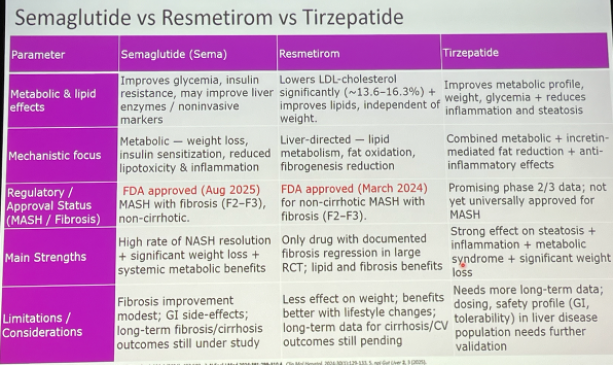
- On management, Dr. Kesavadev highlighted the benefits of weight loss on MASH resolution. In a 52-week study (n=293), 5% weight loss led to MASH resolution in 10% of participants and fibrosis regression in 45% of study participants. Impressively, weight loss by over 10% led to MASH resolution in 90% and fibrosis regression in 81% of participants. Hence, Dr. Kesavadev encouraged GLP-1 RA use (e.g., semaglutide, which is FDA-approved for MASH) to reap weight loss benefits, as well as improvements in cardiorenal and liver health. Rezdiffra (resmetirom), a thyroid hormone receptor-β selective agonist, is also approved for F2-F3 MASH, based on the MAESTRO-NASH trial. Dual GLP-1/GIP RA tirzepatide could also be considered given promising phase 3 SURPASS-3 substudy and phase 2 SYNERGY-NASH. See the table below for the comparison among semaglutide, resmetirom, and tirzepatide.
12. Real-world AID use in pregnancy demonstrates strong glycemic outcomes during the third trimester and when using pregnancy-specific algorithms
Dr. Sarah Price (University of Melbourne, Australia) presented new real-world data on AID use in pregnant women with T1D. These findings offer a practical view of how AID performs throughout pregnancy and how CamAPS FX compares to other systems with its pregnancy-specific Time in Range (TIPR).
- Study design. Dr. Price and her team analyzed women with T1D who attended the Royal Women’s Hospital from 2020-2024. All used CGM, which is subsidized nationally by the Australian government, while insulin pump access depended on private insurance and four-year device “lock-in” warranties, limiting mid-pregnancy device switching. Participants were grouped into standard care (n=92) and AID users (n=41), including 35 women on non-pregnancy-specific systems and six on CamAPS FX, which is the only pregnancy-approved algorithm in Australia. Glycemic outcomes were evaluated across four two-week CGM windows from early pregnancy through 36 weeks, along with obstetric outcomes.
- Baseline characteristics. Women entering pregnancy on AID had significantly better glycemic management, mirroring trends seen in the AiDAPT trial (n=124), CIRCUIT (n=88), and CRISTAL (n=90) trials, which consistently showed improved pre-pregnancy glycemic outcomes among AID system users. Other demographic and clinical characteristics of the women were comparable, supporting the validity of between-group comparisons.
- Results. Although mid-pregnancy glycemia was similar across both groups, a separation emerged late in gestation. The standard care group achieved about 66% of TIPR while AID users exceeded 70%. Within the AID group, CamAPS FX delivered significantly greater performance (82% TIPR versus 62% with other systems). Dr. Price noted that these differences reflect the value of pregnancy-tailored algorithms. No women using AID experienced severe hypoglycemia or required discontinuation of their system on the day of delivery, demonstrating algorithm adaptability during rapid insulin-sensitive shifts.
- Implications. Dr. Price said that many women wish to remain on familiar systems during pregnancy, and the real-world data provide reassurance that these choices do not lead to poorer glycemic outcomes than standard care. However, she also discussed the need for broader access to pregnancy-approved AID systems and future studies assessing (i) glycemic; (ii) obstetric; and (iii) mental-health outcomes. She called for greater advocacy to ensure that AID becomes accessibly for all pregnant women with T1D.
--by Riya Chatterjee, Jeremy Alkire, Nour Khachemoune, Kat Moon, Monica Oxenreiter, and Kelly Close
[1] F2-F3 MASH refers to moderate (F2) to severe (F3) liver fibrosis.