Novo Nordisk announces positive topline results of the phase 2 trial of once-weekly subcutaneous and once-daily oral amycretin in people with T2D –
Follows positive topline results from the phase 1b/2a trial of subcutaneous amycretin for obesity or overweight
Novo Nordisk announced today positive topline results from the phase 2 trial (n=448) of once-weekly subcutaneous and once-daily oral amycretin (a unimolecular GLP-1 and amylin RA) in people with T2D.
At Week 36, subcutaneous amycretin conferred up to 15% weight loss and the daily oral formulation conferred up to 10% weight loss, compared with 3% for placebo. Amycretin also improved glycemic management, with mean A1c reductions of 1.8 percentage points achieved with the subcutaneous formulation and 1.5 percentage points with the oral formulation, compared with 0.2 and 0.4 percentage points with placebo, respectively.
Given the positive results, Novo Nordisk plans to initiate a phase 3 program in 2026 to evaluate amycretin in adults with T2D.
Table of Contents
- Study design and baseline characteristics
- Results: Amycretin demonstrated robust glycemic and weight-lowering effects in people with T2D
- Follows full results of phase 1b/2a trial of amycretin in overweight and obesity
- Amylin agonists have the potential to reshape the side effect profile of weight-lowering therapies
- Amycretin to address people with greater weight loss needs, differentiating from semaglutide and cagrilintide
- KOL Commentary
- Figure 1. Novo Nordisk’s vision for obesity market segmentation
- Close Concerns’ Questions
Study design and baseline characteristics
The phase 2 trial (n=448) evaluated both once-weekly subcutaneous and once-daily oral formulations of amycretin in adults with T2D inadequately managed by metformin with or without SGLT-2 inhibitors. The study included nine different treatment arms, including six subcutaneous doses (0.4 mg to 40 mg) and three oral doses (6 mg to 50 mg), administered for up to 36 weeks. The primary endpoint was the change in A1c from baseline to Week 36 and secondary endpoints included percent change in body weight.
At baseline, participants had a mean body weight of 99 kg (~218 lbs) and A1c of 7.8% in the subcutaneous amycretin group, and 101 kg (~222 lbs) and 8.0% in the oral amycretin group. Nearly two-thirds of participants were male across both administration routes.
Results: Amycretin demonstrated robust glycemic and weight-lowering effects in people with T2D
The trial met its primary endpoint, with once-weekly subcutaneous amycretin achieving dose-dependent A1c reductions of up to 1.8 percentage points from a mean baseline of 7.8%, and once-daily oral amycretin achieving up to 1.5 percentage point reduction from a mean baseline of 8.0%. By comparison, placebo groups saw A1c reductions of 0.2 percentage point (subcutaneous) and 0.4 percentage point (oral). Moreover, 89% of participants achieved A1c <7.0% and 76% reached ≤6.5% with subcutaneous amycretin, while 78% and 63% achieved the respective thresholds with oral amycretin.
From a mean baseline body weight of 99 kg (218 lbs), subcutaneous amycretin demonstrated up to 15% weight loss versus 3% with placebo. Oral amycretin demonstrated up to 10% weight loss compared to 3% with placebo from a mean baseline of 101 kg (~222 lbs). Notably, no weight loss plateau was observed at Week 36 for higher doses, and weight loss in participants on the highest subcutaneous dose were maintained for four weeks.
Both formulations were well-tolerated, with safety profiles consistent with other incretin and amylin-based therapies. Gastrointestinal adverse events were common and predominantly mild-to-moderate.
Follows full results of phase 1b/2a trial of amycretin in overweight and obesity
The results follow the phase 1b/2a trial (n=114), which evaluated subcutaneous and oral formulations of amycretin in adults with overweight or obesity but not diabetes. Note that amycretin is not a pure amylin agonist but a unimolecular GLP-1/amylin RA, potentially explaining a side effect profile that was more consistent with GLP-1 RA studies than amylin agonists. We look forward to understanding the full safety and tolerability profile of amycretin in the full results from this phase 2 trial in people with T2D.
As presented at ADA 2025, 60 mg and 20 mg of subcutaneous amycretin led to respective 24% weight loss (vs. 1.1% with placebo) and 22% weight reduction (vs. 1.9% gain) at Week 36 from a baseline weight of 83.6-99.1 kg (184-218 lbs). Most adverse events were mild or moderate in severity, dose-dependent, and GI-related (e.g., nausea, vomiting, diarrhea). Nearly all participants (94%) in the amycretin 5 mg, 20 mg, and 60 mg groups experienced GI-related adverse events, and the majority (63%) of those on amycretin 1.25 mg did as well.
As shared at EASD 2024, once-daily oral amycretin also led to 13% and 10% weight loss with 100 mg and 50 mg doses, respectively, compared to 1.1% with placebo, at Week 12. Results suggested no signs of a weight plateau. Consistent with other incretin-based therapies, the majority of adverse events were mild to moderate in severity and related to GI discomfort (i.e., nausea and vomiting) and decreased appetite.
Amylin agonists have the potential to reshape the side effect profile of weight-lowering therapies
These promising results build on amylin’s known mechanisms of reducing food intake, slowing gastric emptying, and suppressing glucagon, without triggering significant GI side effects. The benefits of amylin have been made clear through previous studies of long-acting amylin analog candidates, including Novo Nordisk’s cagrilintide and Lilly’s eloralintide.
In the post-hoc analysis of the phase 3 REDEFINE-1 trial (n=3,417), cagrilintide conferred 12% weight loss compared to 20% with CagriSema (a fixed combination of cagrilintide 2.4 mg and semaglutide 2.4 mg) and 2% with placebo at Week 68. Notably, only 1% of participants in the cagrilintide group discontinued treatment due to nausea, compared with 0.1% in placebo and 6% with CagriSema. In a phase 2 study (n=263), eloralintide resulted in up to 20% weight loss compared to 0.4% with placebo at Week 48. Moreover, eloralintide demonstrated a similar safety and tolerability profile as amylin analog cagrilintide 2.4 mg.
Amycretin to address people with greater weight loss needs, differentiating from semaglutide and cagrilintide
With multiple companies advancing amylin-based candidates, the field is rapidly evolving toward metabolic therapies with higher tolerability. In 3Q25, Novo Nordisk shared a graphic (see below) illustrating the obesity market segments that Novo Nordisk’s obesity portfolio candidates are targeting. Notably, amycretin is positioned as a treatment for people with greater weight loss needs than the market segment semaglutide will serve.
KOL Commentary
On today's news, Dr. Alice Lee shared: "In my opinion, the amycretin phase 2 results are welcome in the diabetes space and it is good news that the phase 3 program will proceed. The weight loss of the higher doses had not plateaued as of 36 weeks which makes one hopeful that we will see more in a longer phase 3 study. Although they did not provide data for reaching the threshold of ≤5.7% A1c, it is not a clinical goal for everyone living with type 2 diabetes so the 7% and 6.5% data are positive. Further details about the adverse effect profile will be helpful to potentially differentiate amycretin from other nutrient-stimulated hormone therapies being developed."
Figure 1. Novo Nordisk’s vision for obesity market segmentation
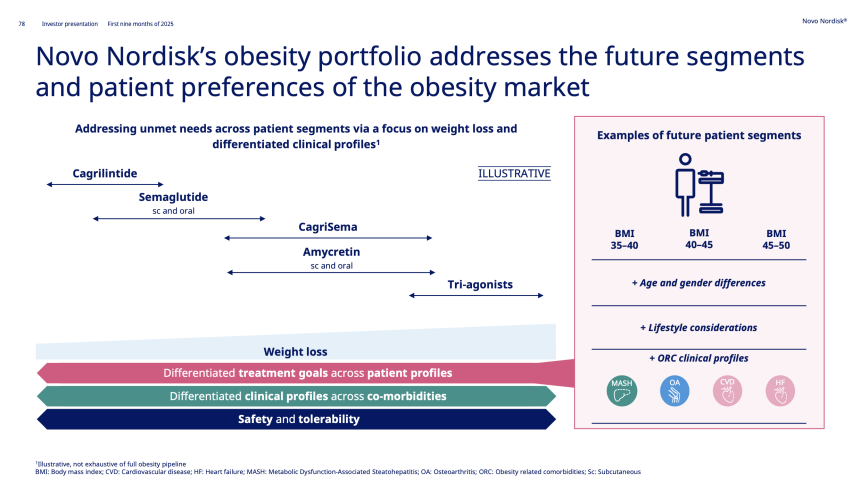
Source: Novo Nordisk’s 3Q25 presentation
Close Concerns’ Questions
- How does the dual GLP-1/amylin receptor agonism of unimolecular amycretin influence its tolerability compared to pure amylin agonists like cagrilintide and eloralintide?
- How does amycretin affect other cardiometabolic markers?
- How might real-world adherence differ between once-weekly injections and daily oral dosing, and what does that mean for outcomes, as well as payer coverage?
- Is Novo Nordisk interested in evaluating amycretin for people with T1D?
--by Kayla Mathieu, Kat Moon, Monica Oxenreiter, and Kelly Close