ATTD 2026 Day #1 Highlights –
Executive Highlights
- The 19th edition of ATTD began today in beautiful Barcelona, Spain with a strong opening ceremony and industry symposia. Conference organizers Profs. Tadej Battelino (University Medical Center Ljubljana, Slovenia) and Moshe Phillip (Schneider Children’s Medical Center of Israel) have once again brought the diabetes community together for an excellent four days of programming. 5,300 participants from 105 countries made the trek to Spain this year – up from 95 nations last year. 945 abstracts were submitted, alongside 42 scientific sessions and 21 industry symposia.
- Alongside Profs. Battelino and Philip, Prof. Boris Kovatchev (University of Virginia) gave this year’s opening session lecture, discussing the use of digital twins and artificial intelligence in the human-machine coregulation of diabetes. While there has been an explosion of AI-centric research within the diabetes space, Prof. Kovatchev highlighted that most papers on the topic are not patient facing and are instead focused on AI’s use in diagnostics and clinician-support. In contrast, his work on AI digital twins in diabetes – or cloud-based data entities that enable safe, in silico testing of human responses to treatment – aims to build a human-AI collaboration for diabetes.
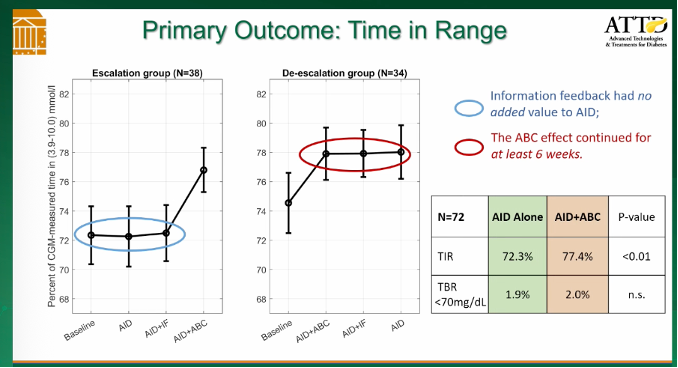
- He specifically highlighted his belief in the future of AI digital twins for diabetes management. In an early six-month study (n=72), TIR increased by 5.1%, from 72.3% to 77.4%. Stratified by baseline A1c, individuals in the highest A1c group (≥7.5%) saw the greatest improvement in TIR. Importantly, the AI digital twin did not “spoil” the control of individuals already with an A1c <6.5% and even improved TIR by 1.2%.
- In tech,
- Dr. Trang Ly (Insulet) and Prof. Martin de Bock (University of Otago, New Zealand) provided new data and real-world evidence to support the benefits of Omnipod 5 use for people with T2D and clearly laid out Insulet’s plan for innovation in the remainder of the decade (!). Prof. de Bock described Insulet’s approach to closing the loop for full automation in T2D. He announced that, in EVOLUTION 2 (n=24), participants aged 16-70 years had a TIR increase to an average of 68%, representing a 24% improvement over MDI without bolusing. This seems particularly extraordinary and we’re imagining how PWD are responding to this. Time below Range (TBR) also remained very low, with a median of 0.14% Time below 70 mg/dL – that’s incredibly low, literally only about two minutes a day (1440 minutes/day times 0.0014).
- Prof. Fernando Gomez-Peralta (Hospital General de Segovia, Spain) and Prof. Ketan Dhatariya (University of East Anglia, UK) discussed growing interest in a dual glucose-ketone (DGK) sensor in development. Speakers emphasized that while the use of CGM has significantly improved glycemic outcomes and reduced the prevalence of acute complications, diabetic ketoacidosis (DKA) remains a major and often preventable emergency. The session focused on the physiology of ketosis, the limitations of relying on glucose alone to detect DKA risk, and how continuous ketone data could enable the earlier identification of metabolic deterioration.
- In therapy,
- Profs. Chantal Mathieu (KU Leuven) and Harpreet Bajaj (LMC Healthcare, Canada) offered their clinical insights on the role of once-weekly insulins in T1D and T2D. Prof. Mathieu highlighted findings from the QWINT (Lilly’s once-weekly insulin efsitora) and ONWARDS (Novo Nordisk’s once-daily insulin degludec) programs to advocate for once-weekly insulin in T2D. In people with T1D, Prof. Bajaj speculated in an “evidence-free zone” that once-weekly basal insulin could have the potential to complement AID use.
- Vertex’s late afternoon session highlighted the next chapter in T1D with islet cell therapy. Dr. Jay Skyler (University of Miami) moderated the session and kicked off the symposium by highlighting the increasing prevalence and incidence of T1D. Dr. Jennifer Sherr (Yale University) then emphasized the remaining T1D burden despite advances in diabetes technology, and Dr. Jason Gaglia (Joslin Diabetes Center) followed with an overview of beta cell replacement with islet cell therapy. Dr. Trevor Reichman (University of Toronto, Canada) concluded the session by focusing on stem cell-derived islet cell therapy for T1D, including promising candidates in the pipeline and ongoing clinical trials.
The 19th annual ATTD meeting continues in Barcelona, Spain from March 11-14, 2026.
Table of Contents
- Big Picture
-
Technology Highlights
- 2. Opening Lecture on human-AI collaboration in diabetes: Prof. Boris Kovatchev on developing AI digital twins
- 3. Insulet: Drs. Trang Ly and Martin de Bock on “Helping diabetes disappear”: Fully closed-loop AID for T2D and beyond
- 4. Abbott: Experts highlight continuous ketone monitoring and its applications to dual glucose-ketone sensing (DGK) for the prevention of DKA
- 5. Roche: Profs. Bogdan Timar and Guido Freckmann on moving from trend-following to proactive intervention with CGM
- 6. Expanding the role of CGM in diabetes detection and early diabetes management
- 7. Tandem: Features, early user data, and glycemic strategies with Tandem Mobi
- 8. Dr. Emma Wilmot addresses evidence and access for CGM in T2D
- 9. Inpatient Diabetes Management: Emerging CGM evidence highlights improvements in glycemic outcomes in the hospital
-
Therapy and T1D Screening Highlights
- 10. Lilly: Profs. Chantal Mathieu and Harpreet Bajaj on the potential for once-weekly insulins, including in combination with GLP-1 RAs, metformin, and AID system
- 11. Vertex: Symposium reflects on the T1D landscape and highlights the next chapter with islet cell therapy
- 12. Dr. Anastasia Albanese-O’Neill on building a global consensus for early-stage T1D screening and monitoring at the general population level
- 13. EDENT1FI screens over 100,000 children in Europe for early stage T1D
- 14. Real-world insights from T1D screening programs in California, Spain, and the Netherlands
- 15. Sanofi’s symposium highlights the future of T1D screening and disease-modifying therapies
Big Picture
1. Opening Ceremony highlights ATTD’s global reach
Profs. Tadej Battelino (University Medical Center Ljubljana, Slovenia) and Moshe Phillip (Schneider Children’s Medical Center of Israel) opened the conference today in Barcelona at 6 pm. This is the 19th ATTD, and it has certainly come a long way from the first ATTD, which was about 300 attendees in Prague, as we were reminded early today by the revered Dr. Neal Kaufman (Canary Health). This 19th ATTD is hopping, with 5,300 participants from 105 countries. Though participant figures are down from last year, we must remember the time of strife this is around the world – many from the Middle East could not even join us and still many others took circuitous routes to reach Barcelona. We thank many researchers for subbing in for those who could not travel. It was truly gratifying to see Prof. Philip and Prof. Battelino together again live – they have created such an entity with ATTD, and many have said how grateful they felt to be among those who are pushing at the field hard and working to make change.
Technology Highlights
2. Opening Lecture on human-AI collaboration in diabetes: Prof. Boris Kovatchev on developing AI digital twins
Prof. Boris Kovatchev (University of Virginia) gave this year’s opening session lecture, discussing the use of digital twins and artificial intelligence in the human-machine coregulation of diabetes. Prof. Kovatchev gave an overview of machine learning and AI before diving into its use in diabetes. While there has been an explosion of AI-centric research within the diabetes space, Prof. Kovatchev highlighted that most papers on the topic are not patient facing and are instead focused on AI’s use in diagnostics and clinician-support. In contrast, his work on AI digital twins in diabetes – or Cloud-based data entities that enable safe, in silico testing of human responses to treatment – aims to build a human-AI collaboration for diabetes.
- Prof. Kovatchev introduced a crash-course on the technological concepts behind AI and its recent presence in the diabetes space. Explaining how AI starts from a base artificial neuron, he summarized how artificial neurons are used to facilitate deep learning, which aggregates to machine learning, which is the foundation behind AI. With a humorous jab at some dystopian projections of AI development, Prof. Kovatchev emphasized his firm prediction that the future of AI will be a collaboration with humans that leads to improvements in biology and healthcare. As emphasis, he highlighted the 5,000 AI-centric diabetes research papers that have been published, mostly within the last five years.
- He specifically highlighted his belief in the future of AI digital twins for diabetes management. By providing an AI digital twin built through data from connected devices, patients and physicians will be able to experimentally adjust parameters are treatments in a digital twin prior to any changes in actual treatment. With his introduction of the concept, he dispelled the idea that this was science-fiction, with research already having shown that in an early six-month study (n=72), TIR increased by 5.1%, from 72% to 77%. Stratified by baseline A1c, individuals in the highest A1c group (≥7.5%) saw the greatest improvement in TIR, as would be expected. Importantly, the AI digital twin did not “spoil” the control of individuals already with an A1c <6.5% and even improved TIR by 1.2% - it may not sound like much, but it’s over 15 minutes!
- Looking ahead, Prof. Kovatchev discussed building a foundation model of glucose-insulin-behavioral interplay in diabetes. Prof. Kovatchev suggested that the next step in advancing digital twin technology is to develop a foundation model for the interaction between glucose, insulin, and human behavior. This is the equivalent to building a diabetes version of what he characterized as well-known AI models such as ChatGPT, Gemini, and Claude. Traditionally, diabetes models have been designed using equations to model human physiology, often drawing on clinical intuition and knowledge. These models are useful when data are limited, but they are restricted in their ability to adapt. AI models, on the other hand, are adaptive and do not require prior knowledge. While they require significant amounts of data, Prof. Kovatchev pointed out that there is plenty of data available, considering are an estimated ~1.4 million AID users globally.
3. Insulet: Drs. Trang Ly and Martin de Bock on “Helping diabetes disappear”: Fully closed-loop AID for T2D and beyond
Insulet’s industry symposium on the opening day of ATTD 2026 drew a crowd that filled the entire large room. Dr. Trang Ly (Insulet) and Prof. Martin de Bock (University of Otago, New Zealand) provided new data and real-world evidence to support the benefits of Omnipod 5 use for people with T2D and clearly laid out Insulet’s plan for innovation in the remainder of the decade.
- Prof. de Bock described Insulet’s approach to closing the loop for full automation in T2D. He reminded the audience that many people with T2D taking multiple daily injections (MDI) continue to not meet glucose targets – 59% of patients have an A1c value of 8.0% or greater, with increased rates of micro- and macrovascular events and a 16% increased likelihood of a cardiovascular event. Patients using Omnipod 5 have demonstrated a 29% reduction in insulin use and, whether or not individuals used a GLP-1 RA, use of Omnipod 5 resulted in a 2.0 percentage point reduction in A1c values for those with the highest baseline values of 9.0% or greater. From a clinical perspective, Prof. de Bock said that these data mitigate certain provider hesitations of weight gain for patients using AID, as total insulin dosing is lowered through the efficiencies created by the use of AID.
- Prof. de Bock also provided an overview of Insulet’s clinical trial process exploring a fully closed-loop system for T2D with new results from the EVOLUTION 2 trial. In 2023-2026, the EVOLUTION 1 and EVOLUTION 2 trials explored the feasibility and fine-tuning of such a system. He announced that, in EVOLUTION 2 (n=24), participants aged 16-70 years had a TIR increase to an average of 68%, representing a 24% improvement over standard insulin therapy (primarily MDI)) without bolusing. Time below Range (TBR) also remained very low, with a median of 0.14% Time below 70 mg/dL. In 2025-2026, the EVOLUTION 3 trial continues to validate these findings, with the EVOLVE pivotal trial to come this year. He emphasized that 91% of participants in EVOLUTION 2 chose to continue in the extension study as patients felt “safer with this system than injections,” and that the system “continues to be life changing.” Prof. de Bock closed by saying that a tubeless, fully closed-loop system for T2D will soon be a reality, and that Insulet hopes the system will be transformative, simple, and effective.
- Dr. Ly described Insulet’s recent innovations to support Omnipod 5’s continued popularity. In 2026, Insulet has already launched Omnipod 5 in five new markets in the Middle East, with four additional launches planned in the near future, beginning with Spain this year. Expansion to additional markets is a key part of Insulet’s innovation to “help diabetes disappear into life,” said Dr. Ly. She said that improving the ease of use for diabetes technology is Insulet’s driving motivation, as the company recognizes the constant burden of diabetes management. In 2026, Insulet will enhance the Omnipod 5 ecosystem, followed by Omnipod 6 in 2027, and a fully closed-loop system for T2D in 2028.
- Changes to glucose targets and the maximum insulin delivery feature have already received highly positive feedback. Insulet has recently introduced a feature enabling patients to set their target glucose level at 110 mg/dL as opposed to 120 mg/dL, the previous lower limit. Upon lowering the target from 120 mg/dL to 100 mg/dL, patients have demonstrated a 4.8% increase in Time in Range (TIR), with a 12% increase in insulin delivered, allowing for tighter glycemic management. This motivates the option for lower targets, which will continue to evolve. Previously, maximum insulin delivery for long periods of time would switch the pump into Limited Mode, but a new feature has allowed the pump to stay in Automated Mode, said Dr. Ly, again improving outcomes.
- Insulet has also explored connectivity through CGM integrations and data visualization. Omnipod 5 is now integrated with the FreeStyle Libre 2 Plus and 3 Plus CGMs, as well as the Dexcom G6 and G7 sensors. Omnipod Discover, a data visualization platform for healthcare providers, has also been launched in select markets in the Middle East and is in a limited US launch with expansion to come. Dr. Ly said that Insulet continues to accelerate into the next steps of innovation for the remainder of this decade. Pointing to more to come, Insulet plans to present results from the STRIVE clinical trial evaluating the SmartAdjust 2.0 algorithm against the current SmartAdjust algorithm at ADA 2026 this June.
4. Abbott: Experts highlight continuous ketone monitoring and its applications to dual glucose-ketone sensing (DGK) for the prevention of DKA
In a standing-room only Abbott-sponsored symposium, Prof. Fernando Gomez-Peralta (Hospital General de Segovia, Spain) and Prof. Ketan Dhatariya (University of East Anglia, UK) discussed growing interest in a dual glucose-ketone (DGK) sensor in development. Speakers emphasized that while the use of CGM has significantly improved glycemic outcomes and reduced the prevalence of acute complications, diabetic ketoacidosis (DKA) remains a major and often preventable emergency. The session focused on the physiology of ketosis, the limitations of relying on glucose alone to detect DKA risk, and how continuous ketone data could enable the earlier identification of metabolic deterioration.
- Prof. Dhatariya reviewed the physiology of ketosis to illustrate why continuous ketone monitoring (CKM) may be clinically important. Ketone production is a normal metabolic response to low insulin levels and reduced carbohydrate availability. It functions as an evolutionary adaption that provides alternative energy substrates for organs such as the brain and heart during starvation. However, when ketones rise rapidly in the presence of insulin deficiency, this physiological process becomes pathological and can lead to DKA. Prof. Dhatariya emphasized that DKA remains the most common hyperglycemic emergency in people with diabetes – mortality rates can still reach up to 30% in regions with limited access to healthcare.
- Importantly, Prof. Dhatariya noted that glucose and ketone trajectories are not always correlated, reinforcing the need for ketone monitoring even with accurate CGM available. Referencing previous work from Dr. Jennifer Sherr (Yale University), he explained that experimental studies interrupting insulin delivery in people with T1D showed that ketone levels and glucose levels often rise independently. This means that clinicians and patients cannot reliably infer ketone status from glucose trends alone. In some participants, glucose levels increased while ketone levels remained low, while in others, ketones rose despite relatively modest glucose elevations. This issue is particularly relevant for euglycemic DKA, where glucose levels may remain below traditional diagnostic levels while ketone levels rise – often the result of adjunctive therapies that can have glucose-lowering impact.
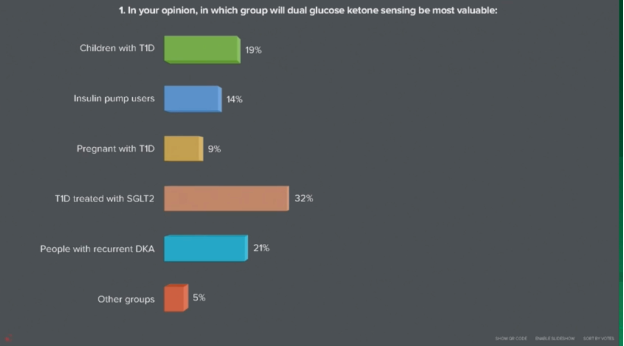
- Audience polling suggests that clinicians see the greatest value in DGK sensing for high-risk populations.Earlier on Wednesday during Abbott School, Prof. Kirsten Nørgaard (Steno Diabetes Center Copenhagen, Denmark) polled attendees on which patient group they believed would benefit most from DGK systems. Notably, 32% of respondents selected people with T1D treated with SGLT-2 inhibitors, a population known to face elevated risk of euglycemic DKA. Prof. Nørgaard referenced these results and highlighted growing clinical interest in technologies that can detect rising ketone levels before symptoms emerge.
- Early expert consensus is beginning to outline potential clinical frameworks for CKM. Proposed thresholdsoutlined by Prof. Dhatariya suggest that ketone levels of <0.6 mmol/L may represent normal physiology, levels 0.6-1.5 mmol/L indicate elevated ketones, 1.5-3 mmol/L represent high risk, and >3 mmol/L should prompt urgent medical attention. These recommendations are preliminary, reflecting the early stage of the technology, but Prof. Dhatariya emphasized that establishing guidance now may help clinicians and patients interpret CKM data once devices become available.
- Looking ahead, speakers collectively suggested that CKM could complement CGM to help prevent DKA and guide earlier interventions. By providing real-time insight into ketone dynamics alongside glucose trends, DGK sensors may help identify infusion set failures, illness-related ketosis, or insulin deficiency earlier than current monitoring approaches. Although challenges around education and the clinical interpretation of ketone trends remain, speakers noted that CKM could follow a trajectory similar to CGM, which initially faced skepticism but is now central to diabetes care.
5. Roche: Profs. Bogdan Timar and Guido Freckmann on moving from trend-following to proactive intervention with CGM
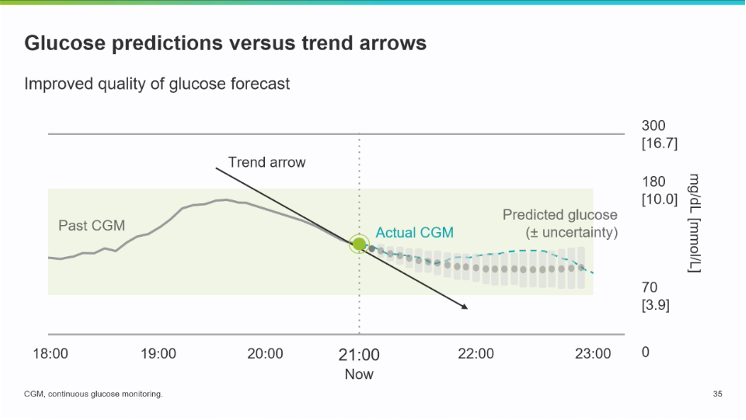
In an engaging afternoon session sponsored by Roche, Prof. Bogdan Timar (Victor Babeş University of Medicine and Pharmacy, Romania) and Dr. Guido Freckmann (Institute for Diabetes Technology Ulm GmbH, Germany) discussed the need for improved glucose predictions based on CGM data. Currently, CGMs use trend arrows that are assumed to be linear, indicating downward or upward trends with varying speeds of change. Patients can use these trend arrows to decide when to bolus or consume carbs to correct trends when appropriate. However, blood glucose does not typically follow a linear trend physiologically.
- Prof. Timar began by discussing the need for proactive clinical intervention that harnesses CGM data. Current limitations of trend arrows can cause patients to over- or underestimate boluses or carbs to consume, leading to unstable blood sugar readings. This inspires the development of advanced glucose forecasting that captures the nuance of blood glucose and has the potential to overcome current unmet needs in diabetes care (see figure below).
- Roche’s Accu-Chek SmartGuide Glucose Predict and Low Glucose Predict features aim to address this gap in glycemic management. The Low Glucose Predict feature alerts patients up to 30 minutes before glucose values fall too low, and the Glucose Predict feature provides a visualization of a two-hour period. This allows patients to analyze the pattern in far greater detail than a trend arrow and adjust accordingly. In the future, Roche also plans to introduce a Night Low Predict feature that will notify users before bedtime of the possibility of having a hypoglycemic event overnight. The features are based on machine learning algorithms and incorporate glucose values, carbohydrates, time of day, and bolus insulin amounts.
- Dr. Freckmann presented first insights from a pilot study of the Accu-Chek SmartGuide Predict Trial (n=20). The study evaluated the effect of the Accu-Chek SmartGuide Glucose Predict and Low Glucose Predict features for diabetes management. Participants were adults with T1D using MDI therapy and the Accu-Chek CGM for 14 days. Baseline A1c values ranged from 5.5-8.2%. In-clinic sessions were standardized with the observation of participant behavior.
- Initial results focused on the technical reliability of glucose predictions and a preliminary look at patient-reported outcomes. Future presentations will discuss impact on glycemic control via metrics like TIR and TBR in the near future. Dr. Freckmann presented a Consensus Error Grid for two-hour glucose predictions and the linear extrapolation of trend arrow errors, demonstrating a strong correlation between predicted glucose values and actual values over a two-hour period. Mean absolute error was higher after about 25 min for extrapolation based on glucose arrows alone compared to the Accu-Chek Glucose Predict feature. This demonstrates the efficacy of this feature and its improvement over existing trend arrows. Further results will quantify these findings in publication and provide additional data on glycemic metrics.
6. Expanding the role of CGM in diabetes detection and early diabetes management
Dr. Valentino Cherubini (Salesi Hospital, Italy) and Dr. Mohammed Almehthel (King Fahad Medical City, Saudi Arabia) opened the ATTD Abbott School by discussing the clinical value of introducing CGM early in the diabetes care pathway, from detection and early disease characterization to guiding early treatment decisions for better long-term outcomes. This is the sixth year of the Abbott School - an ATTD educational event sponsored by Abbott Diabetes. The room was packed with those eager to participate in the conversation around the benefits of CGM, with nearly 90 attendees in person and just as many joining remotely. Both speakers noted that CGM can reveal glycemic patterns not captured by traditional diagnostic tools and supports earlier intervention, more personal care, and improved long-term metabolic trajectories. Moreover, Dr. Almehthel explained that clinicians should use CGM to help guide patients toward better Time in Tight Range (TITR; 70-140 mg/dL), to support prevention or remission efforts in prediabetes and T2D, as well as to minimize complication risk in T1D.
- Dr. Cherubini discussed the evolution of CGM from a management tool to a diagnostic and disease-characterization tool across the diabetes spectrum, particularly in early stage T1D. Traditional diagnostic tests – A1c, fasting glucose, and OGTT – are single-point measures that can miss early dysglycemia and glycemic variability. In presymptomatic T1D (stages 1–3a)[1], CGM can reveal early features such as increased postprandial excursions, prolonged return to baseline after meals, nocturnal hyperglycemia, and small increases in Time above Range (>180 mg/dL).
- CGM may change clinical decision-making in early diabetes by refining the risk stratification,identifying accelerated progression, and enabling the monitoring of disease-modifying therapies. The prime example is teplizumab (Tzield), which has regulatory approval to delay progression to stage 3 T1D in many geographies. Dr. Cherubini noted that CGM can be particularly useful for monitoring glycemia after Tzield treatment to more quickly identify those who may be progressing to stage 3 T1D. In an audience poll, most respondents agreed that the use of CGM would influence their management of patients with presymptomatic T1D. The majority indicated they would use it routinely, and over 85% said they would use it at least in select cases, though nearly one-in-ten reserved judgment and said additional research is needed. During Q&A, Dr. Cherubini clarified that while blinded CGM can be useful for research, unblinded sensors generally provide greater benefit to patients because they enable real-time behavioral feedback.
- Dr. Almehthel then discussed the clinical and behavioral benefits of initiating CGM early in the diabetes journey for people not only with T1D, but also T2D and prediabetes. CGM provides daily insight into the effects of food, insulin, and lifestyle behaviors on glucose levels, helping patients increase TIR with healthier lifestyle behaviors, avoid hypoglycemia and hyperglycemia, and work toward fasting and postprandial glucose targets.
- Dr. Almehthel reviewed evidence suggesting that earlier CGM initiation leads to better outcomes. In one study, type 1 patients who started CGM within one year of diagnosis had lower A1c levels than those who started after three years or those who never used CGM. Early glycemic management also appears important for long-term outcomes, with studies in type 2 diabetes showing that good management soon after diagnosis reduces future risk of complications and mortality (“the legacy effect”), while even a year of elevated A1c early in the disease course is associated with long-term risk. CGM also confers short-term benefits via fewer acute complications, driven largely by reduced incidence of DKA and severe hypoglycemia. This growing body of evidence has led to the ADA Standards of Care recommending CGM initiation early in the disease course, including at diagnosis.
- Dr. Almehthel also highlighted CGM’s potential role in earlier T2D detection and prevention, particularly by prioritizing improvements to TITR. CGM can help identify management issues contributing to the “hidden risk zone” of intermediate hyperglycemia (140–180 mg/dL) and subsequently guide interventions aimed at T2D remission, as well as detect additional cases of prediabetes that standard tests may miss. Specifically, Dr. Almehthel said CGM should be used to establish a baseline glycemic profile and determine if remission is a possible goal in people with newly diagnosed type 2 diabetes. It should also be harnessed for treatment intensification or deintensification for those with established T2D. When pressed in Q&A, he said those aiming for remission should target normoglycemic ranges or >90% TITR. He also mentioned that CGM data may help overcome clinical inertia by providing data to support timely lifestyle changes or medication adjustments.
7. Tandem: Features, early user data, and glycemic strategies with Tandem Mobi
Dr. Laurel Messer (Tandem) and Dr. Viral Shah (Indiana University) led a hands-on presentation focused on Tandem Mobi in this Tandem-sponsored afternoon session. The speakers highlighted the device’s compact design and flexible wear options while also sharing early real-world outcomes and practical guidance for clinicians starting patients on the system. The session combined feature demonstrations and emerging data from early users in the US to confer strategies to optimize glycemic outcomes with the platform ahead of the system’s scaled launch in much of Europe throughout 2026.
- Dr. Messer reviewed many of Mobi’s features. The device is controlled by a cell phone, and Dr. Messer highlighted the small minimum fill requirement of just 30 units, which allows people with low insulin needs to avoid wasting insulin. Mobi also offers the option to deliver a bolus directly from the pump via a quick-bolus button. The system allows flexibility in infusion set use and in addition to insulin delivery adjustments every five minutes, it can deliver up to one AutoBolus per hour, a feature that Dr. Messer described as a “hammer that helps with hyperglycemia.” Clinicians can directly influence how this feature works through the correction factor.
- For clinicians in the room, Dr. Messer also led a hands-on practice session with a demo Mobi and virtual tool, as well as a take-home slider tool that indicates suggested starting doses for new users. While not universally applicable, the tool can ease the start of therapy and can be easily adjusted. It also offers guideline-recommended correction factors for new patients, which can be strengthened to help achieve tighter outcomes.
- Dr. Messer also shared data from the earliest Mobi users in the US. She first reviewed six-week real-world data from adult users (n=1,280), nearly all (97%) with T1D. Across the board, users met or exceeded TIR outcomes within the first six weeks of Mobi use, regardless of the therapy they previously used, and patient satisfaction was high. Tandem also collected real-world data from users who participated in a limited rollout (n=332), showing strong satisfaction across metrics related to freedom, burden, options, ease of use, and effective management. Notably, the data showed that over half (55%) of early users chose to wear the device on the body all the time. The reusable adhesive sleeve was used most of the time and for relatively long periods (with an average wear of 5.5 days). The device was most often worn on the stomach (72%) for discretion, though users reported a wide array of wear locations and styles, with many reporting tucking it into clothing.
- Dr. Shah connected Control-IQ+ to the ability to achieve tight glycemic management. In a paper published in January, he and several co-authors outlined strategies to optimize settings in order to achieve high TIR and Time in Tight Range (TITR) with Control-IQ+. Key recommendations included setting an appropriately aggressive correction factor, establishing a basal rate that accounts for 50-60% of total daily insulin, and turning on Sleep Activity 24/7 for highly engaged users who bolus regularly. With Control-IQ+, using a more intensive correction factor can produce a mean TIR of nearly 80% while maintaining low Time below Range (1.1%). Dr. Shah emphasized that tighter glycemic management with metrics beyond TIR is an important goal – a sentiment a little more than half of the clinicians in the room agreed with, indicating that they discuss TITR with their patients. He noted that tighter targets may be particularly relevant for people early in the course of T1D, during pregnancy, for those with T2D, and for individuals who experience less hypoglycemia.
8. Dr. Emma Wilmot addresses evidence and access for CGM in T2D
Dr. Emma Wilmot (University of Nottingham, UK) discussed how CGM is reshaping T2D care in this Abbott School session. Although evidence shows that CGM consistently improves A1c and reduces hypoglycemia, broader adoption, especially in T2D, often depends on demonstrating cost-effectiveness to payers and updating coverage policies. In the UK, the latestguidance from National Institute for Health and Care Excellence (NICE) still limits CGM access for some people with TYPE 2 DIABEtes, despite growing evidence supporting its use.
- Dr. Wilmot started by reviewing the clinical evidence supporting CGM in people with T2D on insulin therapy. Studies such as the DIAMOND T2 trial and FLASH study showed that CGM use drove meaningful improvements in A1c and reductions in hypoglycemia while on intensive insulin therapy. She added that CGM by itself improves outcomes, but pairing it with structured education (which teaches patients to interpret their CGM data to better adjust their insulin doses and timing), produces even greater A1c reductions.
- Dr. Wilmot also highlighted CGM evidence in people with T2D using basal insulin only, citing the MOBILE trial and PDF study, which demonstrated significant improvements in A1c, TIR, and hypoglycemia with CGM. The MOBILE study was particularly interesting, because total daily insulin dose did not differ between study arms, suggesting that glycemic improvements were largely driven by behavioral changes enabled by CGM insights. Many of these benefits emerged quickly, often within the first two weeks. Dr. Wilmot said that while CGM alone provides powerful feedback, when combined with basic nutrition guidance it can lead to even greater improvements in both A1c and body weight.
- Despite this evidence, access can remain uneven. The current NICE guidance for CGM is largely unchanged since 2015, limiting CGM eligibility for people with T2D on MDI to a subgroup of those with problematic hypoglycemia, impaired hypoglycemia awareness, or those who perform frequent fingerstick testing (at least eight times per day). Dr. Wilmot noted that CGM has clearly changed the “language of the clinic,” enabling more precise discussions about glycemic patterns, but she said that policy must catch up with clinical practice.
- Looking ahead, she teased the presentation of results from the FREEDOM2 trial. This is a 24-site UK-based randomized controlled trial, evaluating whether the FreeStyle Libre 3 CGM improves A1c over 16 weeks compared with BGM in adults with T2D treated with basal insulin and SGLT-2 inhibitors/incretin-based therapies, and with suboptimal glycemia (A1c 7.5–11%). We are certainly eager to show you the results from this study, presented with co-lead Dr. Lalantha Leelarathna tomorrow morning at ATTD, as well as hear their recommendations for future guideline updates and reimbursement decisions for this patient population.
9. Inpatient Diabetes Management: Emerging CGM evidence highlights improvements in glycemic outcomes in the hospital
Prof. Susanne Reger-Tan (Heart and Diabetes Center NRW, Ruhr University of Bochum, Germany) discussed how CGM could reshape inpatient diabetes management. She emphasized the urgency of improving diabetes care in hospitals, noting that remarkably, about 25% of hospitalized patients have diabetes. A diabetes diagnosis is associated with an average of two additional days spent in the hospital per visit, a doubling of complication risk, and ~20% higher treatment costs. Against this backdrop, Prof. Reger-Tan framed CGM as a practical tool for improving glycemic monitoring, workflow efficiency, and outcomes. She envisions a future in which CGM data forms part of a ‘virtual care hub’, enabling scalable and superior glycemic management in the hospital setting.
- Prof. Reger-Tan asserted that CGM could substantially reduce the clinical burden of glucose monitoring in hospitals. She explained that standard care requires nurses to gather multiple devices and consumables, and spend roughly five minutes obtaining a single glucose value via point of care (POC) fingerstick testing. In contrast, CGM allows staff to review glucose trends instantly through an app while leveraging additional features such as trend arrows, real-time alarms, and remote data sharing with diabetes care teams. In her context, confirmatory POC testing is only required for out-of-range values. Prof. Reger-Tan said these capabilities can help clinicians detect overnight hypoglycemia earlier and adjust insulin dosing proactively.
- Building on these operational advantages, Prof. Reger-Tan highlighted early clinical evidence suggesting that CGM-guided insulin management can improve inpatient glycemic outcomes and reduce complications. She cited the DIATEC study (n=166) comparing CGM-guided management to POC glucose monitoring in T2D patients not in the intensive care unit (ICU). In the CGM arm, nurses received real-time glucose values and alarms and could administer additional insulin boluses when glucose remained over 250 mg/dL for more than two hours. Patients using CGM experienced a 15 percentage-point increase in Time in Range (TIR, 70-180 mg/dL) and were twice as likely to achieve ≥70% TIR compared to those receiving standard monitoring. They also lowered time below range, glycemic variability, prolonged hypoglycemic events, insulin usage, and in-hospital complications.
- Prof. Reger-Tan also demonstrated how CGM can reveal hospital-specific glycemic patterns that are often missed with intermittent testing. Using CGM in dermatology patients receiving high-dose glucocorticoids, her team demonstrated how steroid therapy greatly affects glycemia. Nearly all patients with diabetes experienced strongly worsening hyperglycemia and 20-40% of individuals with prediabetes or no diabetes also developed clinically significant hyperglycemia. CGM use showed that the average patient spent 23% of the day (5.5 hours/day) above target glucose levels. Prof. Reger-Tan said that this is just one example of how CGM data can directly inform treatment changes, as visualizing these patterns prompted dermatologists to introduce structured insulin protocols alongside steroid therapy.
- Turning to sensor performance, Prof. Reger-Tan showed that CGM accuracy is acceptable for hospitals and can be further improved with algorithmic adjustments. In a non-ICU evaluation comparing FreeStyle Libre 2 and Libre 3 with POC glucose testing, CGM achieved a MARD of ~10-11%, with most glucose pairs falling within clinically acceptable zones. She noted that accuracy improved after the first day of sensor wear and at higher glucose levels, although, as seen in outpatient use, precision declined in the hypoglycemia range. Applying algorithmic corrections, including time-lag adjustments and linear optimization, reduced MARD to a remarkable ~6%, demonstrating that computational approaches could further improve sensor performance in complex hospital environments.
- Despite the promising data, Prof. Reger-Tan cautioned that infrastructure still limits the widespread use of CGM in the hospital. She noted that in most settings, there is only limited infrastructure for integrating CGM data into electronic records, or paper based systems; which poses a significant barrier to adoption. Additionally, hospitals must also manage device onboarding, cybersecurity, and fragmented data platforms for each CGM system. Prof. Reger Tan said even practical workflow issues, such as patients’ smartphones being stored during surgery, can interrupt data sharing. Looking ahead, she envisioned CGM as the foundation of a “virtual diabetes care hub,” where glucose data could be integrated with information on insulin dosing, nutrition, activity, and additional metabolites, such as ketones. This interoperable platform could allow diabetes specialists to remotely oversee large inpatient populations and move hospital care toward more scalable, data-driven glycemic management.
Therapy and T1D Screening Highlights
10. Lilly: Profs. Chantal Mathieu and Harpreet Bajaj on the potential for once-weekly insulins, including in combination with GLP-1 RAs, metformin, and AID system
In Lilly's industry-sponsored session, Profs. Chantal Mathieu (KU Leuven) and Harpreet Bajaj (LMC Healthcare, Canada) offered their clinical insights on the role of once-weekly insulins in T1D and T2D.
- Prof. Mathieu highlighted findings from the QWINT (Lilly’s once-weekly insulin efsitora) and ONWARDS(Novo Nordisk’s once-daily insulin degludec) programs to advocate for once-weekly insulin in T2D. Specifically, Prof. Mathieu said that once-weekly basal insulin achieved similar A1c reductions and hypoglycemic risk to once-daily doses in both insulin-naïve and insulin-experienced populations. Prof. Mathieu stressed the importance of titration for insulins with a very long half-life (~17.5 days for Lilly’s insulin efsitora), noting that weeks of dosing are required to reach a steady state of basal insulin. Alluding to an imminent guideline update, Prof. Mathieu added that GLP-1 RA therapy and metformin should be maintained while initiating and titrating once-weekly insulin. Importantly, basal insulin use must be individualized, though once-weekly regimens could reduce injection burden and improve adherence and satisfaction for many.
- In people with T1D, Prof. Bajaj speculated in an “evidence-free zone” that once-weekly basal insulin could have the potential to complement AID use. Specifically, he predicted that once-weekly insulin could positively impact PWD who frequently miss insulin injections, those who are newly diagnosed, and persons with relaxed or moderate A1c targets (e.g., patients in palliative care or dependent on a caregiver). Moreover, basal insulin injections could serve as a temporary backup during a pump failure or a supplement in patients with very high insulin needs to reduce frequent pump site changes. Prof. Bajaj ascribed once-weekly insulin the potential to “act as the ‘fixed’ component in AID.” While Prof. Bajaj concluded that substantial evidence is required to determine the real-world impact, once-weekly insulin stands as a potential safety tool to reduce DKA risk in the real world.
11. Vertex: Symposium reflects on the T1D landscape and highlights the next chapter with islet cell therapy
Vertex’s late afternoon session highlighted the next chapter in T1D with islet cell therapy. Dr. Jay Skyler (University of Miami) moderated the session and kicked off the symposium by highlighting the increasing prevalence and incidence of T1D. Dr. Jennifer Sherr (Yale University) then emphasized the remaining T1D burden despite advances in diabetes technology, and Dr. Jason Gaglia (Joslin Diabetes Center) followed with an overview of beta cell replacement with islet cell therapy. Dr. Trevor Reichman (University of Toronto, Canada) concluded the session by focusing on stem cell-derived islet cell therapy for T1D, including promising candidates in the pipeline and ongoing clinical trials.
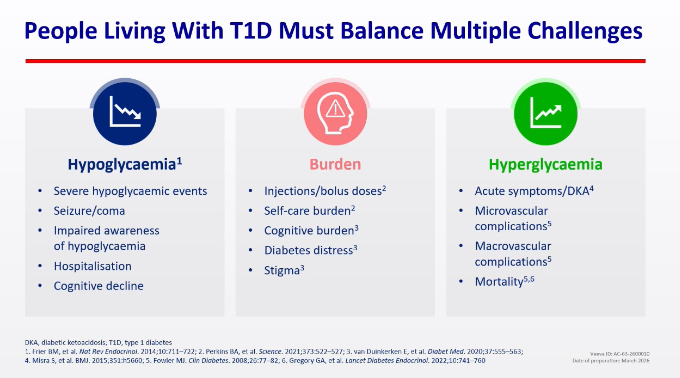
- Dr. Skyler on the prevalence and incidence of T1D. Dr. Skyler shared that in 2025, the estimated global prevalence of T1D was 9.5 million, including 19% aged <20 years, 68% aged 20-59 years, and 12% aged ≥60 years. Also in 2025, there were half a million new diagnoses, including 43% aged <20 years and 57% aged ≥20 years. By 2040, nearly 15 million people are estimated to be living with T1D. Reflecting on the high rates of T1D, Dr. Skyler explained the multiple challenges people living with T1D face on a daily basis, including management of hypoglycemia, hyperglycemia, and burdens with injections, distress, and stigma. Given the increasing prevalence of T1D, ideal therapeutic goals include: (i) prevention of immune destruction; (ii) preservation of beta cell mass or function; (iii) automated insulin delivery; and (iv) replacement or regeneration of beta cells.
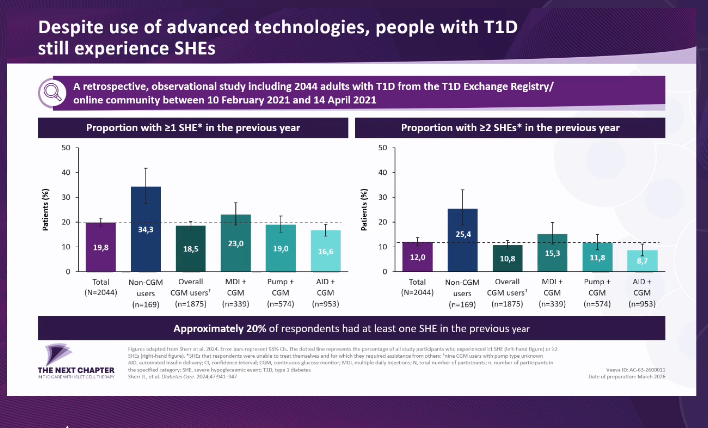
- Dr. Sherr highlighted persisting unmet needs despite advances in diabetes technology. Referring to the well-known results of the DCCT, Dr. Sherr discussed the benefits of intensive insulin treatment compared to conventional diabetes care. Yet, achieving lower glucose targets has also revealed other issues, such as hypoglycemia. Dr. Sherr described this challenge as a “double-edged sword,” given the inverse relationship between A1c levels and rates of rates. Encouragingly, since the DCCT, several new tools have emerged with improved strategies for T1D care – blood glucose meters have transformed into continuous glucose monitors, decision making on paper has been integrated into applications and algorithms that support dose titration, and insulin delivery has transitioned from syringes to pens and ultimately, pumps and AID. However, Dr. Sherr again highlighted the limitations of technology, given the persisting acute complications of diabetes with high rates of hypoglycemia and DKA despite the use of advanced diabetes technology. Dr. Sherr also referred to results from a 2024 retrospective study (n=2,044) that showed persistent rates of severe hypoglycemia despite the use of advanced technologies, as well as a subset of this study of patients who reported CGM data, which also showed that many did not reach glycemic targets despite the use of diabetes technology. Furthermore, Dr. Sherr emphasized that the incidence of diabetes complications, even with achievement of A1c targets, remains a risk to people with T1D. Therefore, Dr. Sherr emphasized, “Technology has improved care, but it is not a cure.”
- Dr. Gaglia on the journey of beta cell replacement with islet cell therapy. Dr. Gaglia presented a comprehensive slide featuring landmarks throughout the history of beta cell replacement, including the most recent advances: (i) the FDA’s approval of Lantidra (donislecel) in June 2023; and (ii) Vertex’s zimislecel demonstrating insulin independence in June 2025. Dr. Gaglia then explained the processes of whole pancreas transplantation and allogeneic cadaveric islet transplantation, highlighting the advantages and disadvantages of each decision. For both procedures, the requirement of immunosuppression still raises concerns about side effects like infection, malignancy, impaired kidney function, anemia, and gastrointestinal-related events. Yet, Dr. Gaglia referred to studies such as the CIT-07 trial, the CITR-T1DX trial, and a 2025 French retrospective study, and he expressed optimism that the downsides of immunosuppression may outweigh the risks. Overall, Dr. Gaglia encouraged that, as the field refines approaches to islet cell treatments, it must consider the appropriate patient population and individual benefits.
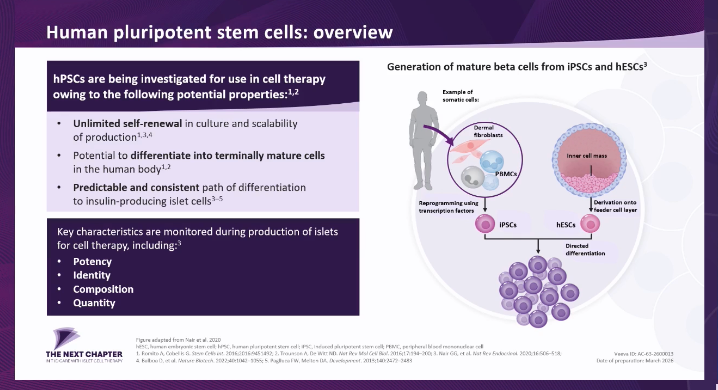
- Dr. Reichman on the potential of stem cell-derived islet therapy in T1D. Dr. Reichman explained that the limitations of cadaveric islet cell transplantation include a limited supply of donor cells with unpredictable quality and the need to protect the cells from the patient’s immune system. Potential solutions for these challenges include islet-like cells developed in vitro at a scalable level, as well as mechanisms to protect cells from the immune system. Current approaches particularly focus on protecting allogeneic stem cells from immune rejection through immunosuppressive treatment, encapsulation, and immune evasion through gene editing. Given the limitations previously explained by Dr. Gaglia, Dr. Reichman elaborated on the latter two emerging potentials, noting that encapsulation provides a highly stable environment for cell transport and that gene editing reduces recognition and enhances inhibition.
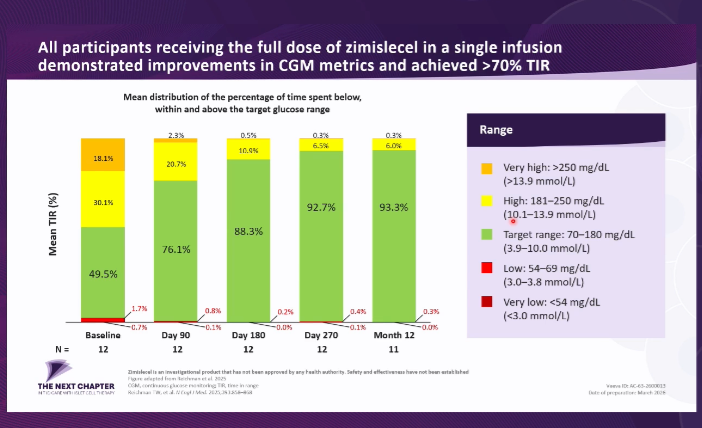
- The pipeline for cell-based therapies includes: (i) phase 1/2 VC-02, which uses perforated microencapsulation and immunosuppression; (ii) phase 1/2 CTX211, which uses gene editing; and (iii) phase 1/2/2 zimislecel, which uses systemic immunosuppression. Dr. Reichman expanded on zimislecel, which demonstrated engraftment of islet cells with endogenous insulin, and eliminated severe hypoglycemia, improved glycemic outcomes (A1c <7.0% and TIR >70%) while reducing exogenous use of insulin.
12. Dr. Anastasia Albanese-O’Neill on building a global consensus for early-stage T1D screening and monitoring at the general population level
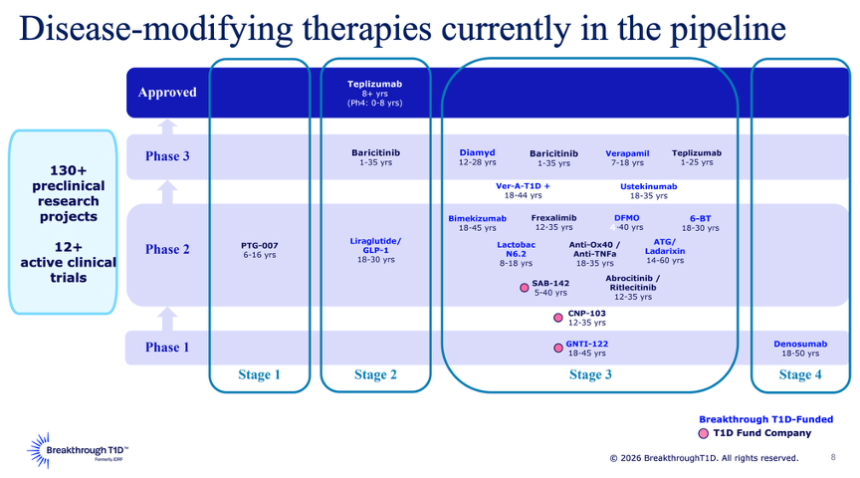
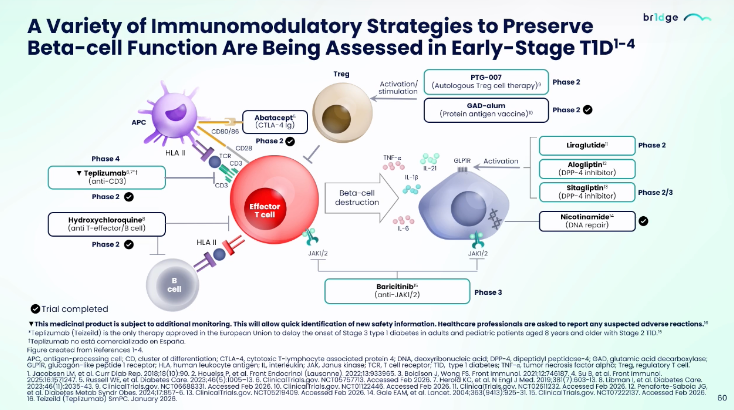
In this standing-room-only symposium, Dr. Anastasia Albanese-O’Neill (Breakthrough T1D) offered insights from an international consensus guidance on T1D screening and monitoring. She began by emphasizing the benefits of screening and identification of early stage T1D, including: (i) an alternative to “unacceptably high” rates of DKA at diagnosis; (ii) time for families and caregivers to educate themselves about diabetes; and (iii) an option to take disease-modifying therapies. She said the field has reached a “pivotal moment,” with Tzield (teplizumab) approved and more candidates emerging to prevent or delay T1D progression (see below). Though her points were met with nods of agreement throughout the packed hall, not one member of the audience raised their hand when Dr. Albanese-O’Neill asked if anyone received education on the importance of screening for T1D during their medical training. She thus stressed an urgent need for consensus screening guidance to raise awareness and clarify screening processes. This builds on the consensus guidance on early-stage T1D monitoring published in June 2024 – this landmark article has been accessed over 85,000 times across Diabetologia and Diabetes Care and cited nearly 100 times, indicating high interest among clinicians, researchers, and the public.
- Breakthrough T1D and collaborating experts created a committee in late 2024 to develop expert-guided consensus on population level screening for T1D. While the consensus itself is currently unpublished, Dr. Albanese-O’Neill provided a high-level overview of the clearly valuable tenets.
- On the implementation of screening programs, Dr. Albanese-O’Neill summarized key elements of the emerging consensus: (i) when adequate policy and follow-up infrastructure are in place, screening for early-stage T1D in the general population is recommended; and (ii) targeted screening of higher-risk groups (family history or coexisting autoimmune disease) is an acceptable starting point in settings that are just beginning to implement programs.
- Clinically, a three-time-point childhood screening strategy is most supported by evidence. The first screening would occur between ages 2-4, another test between ages 6-8, and a final childhood screening between ages 10-15 if earlier tests are negative. For individuals over 15 years old who have never been screened, Dr. Albanese-O’Neill shared that a one-time screen is suggested at some point in adulthood. However, she said that we lack substantial evidence on screening in the adult population. More research needs to be done on the significance of single antibody positivity, optimal screening workflows and follow-up care, screening assays, and T1D staging in individuals of non-European ancestry, as well.
13. EDENT1FI screens over 100,000 children in Europe for early stage T1D
In this jam-packed morning session, Prof. Jurgen Vercauteren (KU Leuven, Belgium) offered the latest updates on EDENT1FI. As background, EDENT1FI is a five-year EU-based research consortium that focuses on early T1D detection in children. Prof. Vercauteren shared that EDENT1FI has already screened over 100,000 children across Europe – halfway to the project’s previously shared goal. EDENT1FI is structured into five “work packages”:
- Screening. Providing a framework to apply and extend early-stage T1D screening to new and existing regions in Europe, as well as expanding a European registry.
- Impact. Evaluating the ethical, psychological, and economic impact of general population screening using a cost‑effectiveness model and questionnaires.
- Monitoring. Developing and implementing a monitoring framework for progression to clinical-stage T1D. Identifying novel biomarkers and CGM approaches to monitor disease progression.
- Roadmap for preventative and intervention studies. Building a unified master protocol and biomarker roadmap for preventive and disease‑modifying therapies.
- Communication. Implementing screening and policy change in Europe through communication campaigns, consensus guidelines, partnerships with advocacy and industry, and engagement with regulators and lawmakers.
As just ~10% of individuals diagnosed with T1D have a first-degree relative with T1D, Prof. Vercauteren and EDENT1FI leaders argued that broader screening is essential to identify individuals with early-stage T1D, reduce DKA incidence, and recruit participants to clinical trials evaluating disease-modifying therapies.
- Prof. Zdeněk Šumník (Motol University Hospital, Czechia) offered insight into EDENT1FI’s efforts in Czechia, where 1% of the national pediatric population has been screened during 22 months of the EDENT1FI protocol. Approximately 0.4% of children tested positive for two or more autoantibodies in the general population, compared to nearly 3% of children with a first-degree relative who has T1D. Of those who tested positive for two or more autoantibodies, 94% provided a confirmatory venous sample. Accordingly, Prof. Šumník stressed that T1D screening at scale is feasible, effective, and well-accepted by parents and physicians – offering a positive foundation for population-wide screening. This conclusion was reiterated by Prof. Parth Narendran (University of Birmingham, UK), who cited newly published findings from the UK-based general population ELISA study to substantiate his argument. The study (n=24,875) identified 75 children (0.3%) with one autoantibody, 160 (0.6%) with two autoantibodies without symptoms, and seven with stage 3 T1D. Among relatives of people with T1D, who were more likely to engage with the program, 3.7% (n=101) of first-degree relatives and 2.2% (n=131) of children with a family history of T1D screened positive.
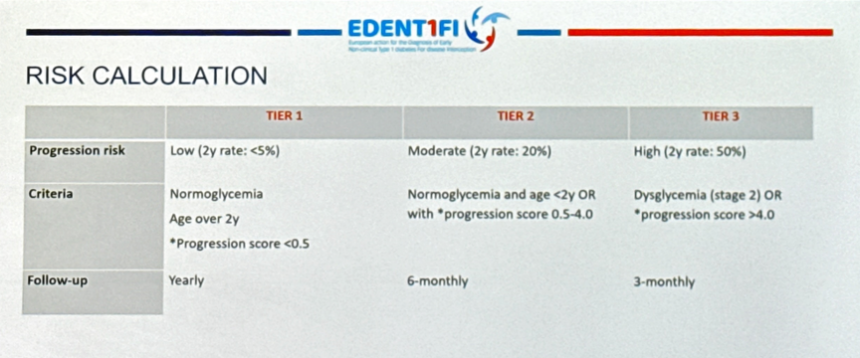
- Prof. Pieter Gillard (KU Leuven) discussed EDENT1FI’s third work program: Monitoring for progression to clinical T1D and biomarker refinement. Prof. Gillard described three risk tiers – Tier 1 (low), Tier 2 (moderate), and Tier 3 (high) – in addition to traditional staging measures (see below). Prof. Gillard advocated for tier- and stage-dependent follow-up timelines in T1D screening initiatives.
- Prof. Gillard also advocated for CGM use after staging OGTTs for risk stratification, citing evidence that Time above Range (TAR; >140 mg/dL) is correlated to T1D progression risk. Furthermore, he shared that a collaboration between MiniMed and EDENT1FI will seek to evaluate if CGM algorithms (e.g., meal detection or sleep patterns) might further improve the prediction of progression to stage 3 T1D beyond traditional biomarkers.
14. Real-world insights from T1D screening programs in California, Spain, and the Netherlands
In a crowded session, Dr. Carla Demeterco-Berggren (UCSD), Ms. Christine Fransman (Diabeter, the Netherlands), and Prof. Luis Castano (Cruces University Hospital, Spain) shared insights from real-world T1D screening initiatives. Beyond the EDENT1FI collaboration, many organizations and clinics have established and led screening programs for early T1D detection.
- UCSD’s Rady Children’s Hospital is part of the T1D Exchange Quality Improvement (T1DX-QI) Collaborative,a network of over 55 centers serving people with T1D. Even the centers of the collaborative, however, demonstrate low readiness to conduct T1D autoantibody screening and administer disease-modifying therapy (e.g., Tzield). In a 2023 survey (n=55 centers), 68% of the clinics did not change their clinical practice after FDA approval of Tzield in November 2022, with screening largely limited to research programs like TrialNet. In response, T1DX-QI Collaborative launched quality improvement pilot programs to integrate screening and monitoring workflows into routine practice. The first pilot (2023-24), funded by Breakthrough T1D, involved Rady Children’s and the University of Florida, and the second pilot (2024-25), funded by Sanofi, involved four additional institutions.
- Across the six pilot centers, 1,396 at-risk children were screened between June 2024 and December 2025, with 153 (11%) testing positive for ≥ two autoantibodies, 76 (5%) diagnosed as stage 2 T1D, and 59 (4%) offered disease-modifying therapy. During follow-up, 33 individuals progressed to stage 3 T1D, but none presented with diabetic ketoacidosis (DKA), highlighting the potential of screening programs to prevent life-threatening emergencies at diagnosis. Dr. Demeterco-Berggren shared key lessons from the pilot program: (i) the importance of early leadership engagement; (ii) patient-centered education; (iii) EHR integration; (iv) readily available screening kits; (v) dedicated T1D at-risk clinics; and (vi) nurse-led screening clinic. Looking forward, Rady Children’s Hospital will focus on developing sustainable reimbursement models, screening networks with primary care providers, and community screening events to expand access. Based on these learnings, T1DX QI Collaborative published a white paper, “Real World Beta Cell Preservation Throughout the Stages of T1D,” in February 2026 to provide a practical implementation guide.
- Independent screening efforts are ongoing in Spain and the Netherlands, as well. Building on Spain’s decades-long history of T1D screening, three Spanish societies established a national consensus to: (i) conduct routine screening for first-degree relatives and people with genetic risk at endocrinology clinics via SCREEND1A-FAM; and (ii) pilot a general population screening program, SCREEND1A, in primary care clinics to evaluate feasibility and cost-effectiveness. Prof. Castano highlighted the use of antibody detection by the agglutination-PCR (ADAP) method, which has offered greater sensitivity and cost-effectiveness, and the expansion of the national T1D registry, REDCap, to include data on early-stage T1D. In the Netherlands, Diabeter, INNODIA, and Sanofi launched a project to pilot T1D screening. It will first begin with INNODIA’s Family & Friends model (n=50-100) and expand to a broader population across the nation (n=7,000). Ms. Fransman hoped that this research initiative will accumulate evidence to show national leaders the value of population-wide screening.
15. Sanofi’s symposium highlights the future of T1D screening and disease-modifying therapies
In a packed lunchtime symposium sponsored by Sanofi, Dr. Alice Cheng (University of Toronto), joined by an expert panel, set the stage for a forward‑looking discussion on the evolving landscape of T1D detection, staging, and management. Dr. Cheng underscored the urgent need to identify individuals with early-stage T1D before they present in the emergency department, shifting from reactive to proactive care. Dr. Cheng framed the conversation around real‑world cases – a 25-year-old male with a history of celiac disease and positive IAb results and a 36-year-old female with a family history of T2D, who was misdiagnosed with T2D – illustrating both the promise of early detection and the challenge of misclassification in adults. Nearly 39% of adults with T1D are initially misclassified as having T2D.
- On early detection and screening, Dr. Sanjoy Dutta (Breakthrough T1D) said that early detection is not merely about identifying risk, but also creating opportunities to slow, stop, or potentially reverse disease progression. Looking ahead, the field is moving toward precision‑medicine approaches that account for the heterogeneity of T1D. He pointed at resources available through Sanofi’s BR1DGE program to help providers navigate screening guidance. Global screening efforts have already begun to improve disease marker identification, reduce misclassification, and support research in stage 1 T1D.
- On interpreting screening results, Dr. Jeremy Pettus (UCSD) focused on how to make islet autoantibody testing a routine part of practice. Barriers to screening include complex test names, lack of familiarity, and inconsistent ordering workflows. Dr. Pettus said that simple system‑level changes, such as embedding autoantibody panels directly into electronic health record order sets, can dramatically increase screening rates. Dr. Pettus also highlighted international guidelines (ISPAD,Breakthrough T1D, ADA, and EDENT1FI), which stress the need to confirm any positive autoantibody result with a second test before making a diagnosis or staging decision. Misclassification persists, reinforcing the need for clinicians to use autoantibodies as a tool not only for staging early T1D but also for distinguishing T1D from T2D in adults. He also highlighted the utility of the AABBCC method, which considers age (<35 years), autoimmunity, body habitus (BMI <25 kg/m2), background of family history, control (glucose management on noninsulin therapies), and comorbidities as common factors of T1D.
- On education, Ms. Jessica Melin (Lund University, Sweden) and Prof. Karen Lange (Hannover Medical School, Germany) shifted the focus to the lived experience of early‑stage T1D, emphasizing that monitoring, education, and psychosocial support are shared responsibilities across the entire healthcare system. Prof. Lange emphasized the emotional turbulence that often follows a positive result, especially in young adults, and encouraged clinicians to normalize reactions, provide clear and focused information, and help individuals maintain a sense of agency amid uncertainty. On the next steps, drawing on experiences from the ELSA study, a UK-based T1D screening program, Dr. Renuka Dias (University of Birmingham, UK) cautioned against offering false reassurance after a negative screen, stressing the importance of education around rescreening, particularly in younger children. She highlighted the importance of monitoring after a positive antibody result to ensure softer landings when starting insulin therapy and differences in our understanding of the natural history in adult and children with positive antibody results. She also said it is crucial to help people understand both the promise and the limits of emerging and existing therapies like Tzield. In that same vein, she emphasized as an exceptionally exciting time to be working in T1D cures, with a rapidly expanding pipeline of disease modifying therapies now moving through clinical development. Specifically, she highlighted therapies across regulatory T cells and effector T cells as well as B cells, being investigated to preserve beta-cell function.
-- by Riya Chatterjee, Kayla Mathieu, Elizabeth Rose, Paul Moon, Jeremy Alkire, Nour Khachemoune, Kat Moon, Esther Min, Elaine Young, Albert Cai, Monica Oxenreiter, and Kelly Close
[1] Dr. Cherubini reviewed the four stages of T1D. Stage 1 T1D is characterized by ≥2 autoantibodies and normoglycemia, stage 2 is characterized by ≥2 autoantibodies and dysglycemia, stage 3a is characterized by patients beginning to experience hyperglycemia, and upon stage 3b and “clinical” T1D patients begin to see symptoms of the disease.