Novo Nordisk announces topline results of the phase 3 REIMAGINE 2 trial in adults with T2D –
CagriSema 2.4 mg demonstrates nearly two percentage point reduction in A1c (vs. 1.76 percentage point reduction with semaglutide alone)
Novo Nordisk announced today positive topline results from the phase 3 REIMAGINE 2 trial (n=2,728), which evaluated CagriSema (a fixed-dose combination of semaglutide 2.4 mg and cagrilintide 2.4 mg) in adults with T2D inadequately managed on metformin with or without SGLT-2 inhibitors. We applaud the decision to use three groups of PWD, none of whom are on “only” placebo (no medicine).
At Week 68, CagriSema demonstrated superior A₁c reduction of 1.91 percentage point (vs. 1.76 percentage point with semaglutide 2.4 mg alone) from a mean baseline of 8.2%. Although that may sound like “about the same” A1c drop, the one on CagriSema got a 9% (rounding up) A1c improvement. We’d love to see the difference in Time in Range (TIR). CagriSema also led to 14.2% weight loss vs. 10.2% weight loss with semaglutide alone from a baseline of 101 kg (223 lbs). That improvement is 39% higher with CagriSema – not just 9% better! Notably, no weight loss plateau was observed at Week 68[1]. Though Safety was consistent with incretin and amylin-based therapies, with most adverse events being mild-to-moderate GI events.
Novo Nordisk plans to discuss the regulatory pathway for CagriSema following REIMAGINE 1 (n=189) and REDEFINE 3 (n=7,101). Full REIMAGINE 2 data will be presented at an undisclosed upcoming 2026 scientific conference. We note while the deadline to submit “regular” data to ADA’s Scientific Sessions in New Orleans in early June ended January 5, happily, researchers and others have until March 9 at 5 pm ET to submit late-breaker data to ADA.
Table of Contents
- KOL commentary: REIMAGINE 2 trial shows “strong indirect support” for amylin/GLP-1 combination
- CagriSema demonstrated superior A1c reduction and weight loss compared with semaglutide alone and placebo
- Previously, REDEFINE 1 and REDEFINE 2 trials showed weight loss benefits of CagriSema for obesity with or without T2D
- Ongoing REDEFINE and REIMAGINE trials
- Novo Nordisk envisions CagriSema to serve people with greater weight loss needs
- Close Concerns’ Questions
KOL commentary: REIMAGINE 2 trial shows “strong indirect support” for amylin/GLP-1 combination
Dr. Alan Moses: "The last decade has seen tremendous progress in developing efficacious medications for both T2D and obesity. It seems that the combination of semaglutide and cagrilinotide will be the next iteration on the journey to address both hyperglycemia and overweight. The preliminary results are encouraging and, not surprisingly, while the combination bested semaglutide on both A1c reduction and weight reduction, the difference was greater for weight reduction, an impressive finding for those with both diabetes and obesity. We still need to see more data on safety and on subpopulations, but the availability of multiple effective therapies for T2D is encouraging and allows clinicians to move closer to a truly personalized therapy for each person living with diabetes."
Dr. Dan Drucker (University of Toronto): “Effective medicines that meaningfully reduce HbA1c while producing substantial double digit weight loss represent an unmet need for people with T2D. I look forward to seeing the totality of the data for the Phase 3 program to more fully assess the risk-to-benefit profile of this promising new medicine. However, the clinical trial evidence base supporting the use of semaglutide in people with T2D provides strong indirect support for the amylin-GLP-1 combination.”
Dr. Alice Cheng (University of Toronto): “This is another piece of good news for people living with type 2 diabetes. There is slightly further glucose reduction with the CagriSema compared to Sema 2.4 mg on its own, but what stands out to me is not so much the glycemic effect but rather the additional ~4% body weight reduction – with no sign of plateau at 68 weeks. These results add to what was seen in REDEFINE 2, giving more clinical relevance with the active comparators. I am eager to see the results from the cagrilintide alone arm too, particularly with respect to GI side effects.”
Dr. John Buse (University of North Carolina): “Of course, I want to see more on tolerability and adverse events, but the efficacy looks strong and certainly CagriSema seems to offer additional efficacy to semaglutide alone. What is much harder to tell with the available data is to project how CagriSema will stack up to tirzepatide. Difference in the data that is available and study design features make that challenging at this point. Seems similar in efficacy overall.”
CagriSema demonstrated superior A1c reduction and weight loss compared with semaglutide alone and placebo
In the REIMAGINE 2 trial, a trial with thousands of participants (n=2,734) with a mean baseline A1c of 8.2%, and mean body weight of 101 kg (~223 lbs), the results were striking! Weight loss was far better with CagriSema and A1c was nearly 10% better! Approximately 40% of participants were on SGLT-2 inhibitors at baseline. The study was conducted at 405 locations[2] in the US, Europe, Asia, Africa, and Latin America.
By efficacy estimand (assuming full treatment adherence), CagriSema demonstrated nearly a full 2.0 drop (1.91, specifically) percentage point reduction in A1c, compared with 1.76 percentage point reduction in semaglutide alone and 0.09 percentage point increase with placebo. CagriSema also conferred a 14.2% weight reduction, compared with a 10.1% reduction with semaglutide alone – nearly 40% greater weight loss! and 1.5% weight reduction in placebo. By treatment-regimen estimand (treatment effect regardless of adherence), CagriSema demonstrated a 1.8 percentage point reduction in A1c, compared with a 1.68 percentage point reduction with semaglutide 2.4 mg. In addition, CagriSema demonstrated superior weight loss of 12.9%, compared to 9.2% with semaglutide – a difference of a full 40%. That’s pretty great!
Moreover, 43% of participants treated with CagriSema achieved at least 15% weight loss, and 24% reached 20% or more. As comparison, in the SURMOUNT-2 trial, 40% of participants with obesity or who were overweight and T2D taking tirzepatide achieved ≥15% body weight reduction.
Previously, REDEFINE 1 and REDEFINE 2 trials showed weight loss benefits of CagriSema for obesity with or without T2D
In the REDEFINE 1 trial (n=3,400), which investigated CagriSema in adults with obesity, participants in the treatment group achieved 20.4%, outperforming cagrilintide 2.4 mg (11.5%), semaglutide (14.9%), and placebo (3.0%) at Week 68. In addition, 40.4% of participants achieved ≥25% weight loss, compared to 6.0% with cagrilintide 2.4 mg, 16.2% with semaglutide 2.4 mg, and 0.9% with placebo. Based on this result, Novo Nordisk submitted a New Drug Application to the FDA in December 2025 for CagriSema as an adjunct to lifestyle intervention for the management of long-term weight loss. We assume FDA is working very hard on this submission.
In the phase 3 REDEFINE 2 trial (n=1,206), CagriSema demonstrated statistically significant and superior weight loss compared to placebo in adults with T2D who were overweight or who had obesity. CagriSema conferred a 13.7% weight loss from a baseline body weight of 102 kg (225 lbs), compared to 3.4% with placebo. By trial product estimand (assuming full treatment adherence), CagriSema demonstrated 15.7% weight loss from a baseline body weight of 102 kg (225 lbs), compared to 3.1% with placebo. As a reminder, Lilly’s tirzepatide demonstrated a 15.7% weight loss at Week 72 in the SURMOUNT-2 trial (n=938).
Ongoing REDEFINE and REIMAGINE trials
Novo Nordisk has multiple ongoing trials investigating CagriSema across obesity and T2D. REDEFINE 1,2, 3, 4, and 11 span obesity, CVOT, tirzepatide comparison, and dose escalation strategies. REIMAGINE 1-5 explore CagriSema in T2D populations with varying background therapies, including metformin, SGLT-2 inhibitors, basal insulin, and tirzepatide comparators.
| REDEFINE trials | Description and results | Completion date |
| REDEFINE 1 (n=3,400) | 68-week trial of CagriSema vs. placebo in adults with obesity or overweight with one or more comorbidities and without T2D; topline results announced in December 2024, full results presented at ADA 2025, and subgroup analysis results shared in 4Q24. | October 2026 |
| REDEFINE 2 (n=1,206) | 68-week trial of CagriSema vs. placebo in adults with T2D and either obesity or overweight; topline results announced in March 2025, and full results presented at ADA 2025. | January 2025 |
| REDEFINE 3 (n=7,000) | 235-week CVOT of CagriSema vs. placebo in adults with established CVD with or without T2D. | September 2027 |
| REDEFINE 4 (n=809) | 72-week trial of CagriSema vs. tirzepatide 15 mg in adults with obesity. | October 2027 |
| REDEFINE 11 (n=609) | Trial to assess dose escalation/re-escalation of CagriSema. | October 2028 |
| REIMAGINE trials | Description and results | Completion date |
| REIMAGINE 1 (n=180) | 40-week trial of CagriSema vs. placebo in people with T2D treated with diet and exercise. | December 2025 |
| REIMAGINE 2 (n=2,728) | 68-week trial of CagriSema vs. semaglutide, cagrilintide, and placebo in T2D on metformin and with or without SGLT-2 inhibitor; topline results announced today. | January 2026 |
| REIMAGINE 3 (n=270) | 40-week trial of CagriSema vs. placebo in people with T2D on once-daily basal insulin with or without metformin. | October 2025 |
| REIMAGINE 4 (n=1,000) | 68-week trial of CagriSema vs. tirzepatide in people with T2D on metformin and with or without SGLT-2 inhibitor. | April 2026 |
| REIMAGINE 5 (n=1,023) | 60-week trial of CagriSema vs. tirzepatide 5 mg in people with T2D on metformin, SGLT-2 inhibitor, or both. | July 2026 |
Novo Nordisk envisions CagriSema to serve people with greater weight loss needs
The company emphasized that CagriSema could become the first amylin-based combination therapy for people with T2D who would benefit from greater weight loss. By combining semaglutide and cagrilintide, the company aims to deliver additive benefits in glycemic management and weight loss, surpassing the efficacy of either agent alone. See below for the patient segmentations that Novo Nordisk intends to target for its portfolio: (i) cagrilintide; (ii) semaglutide; (iii) CagriSema; (iv) amycretin; and (v) tri-agonist.
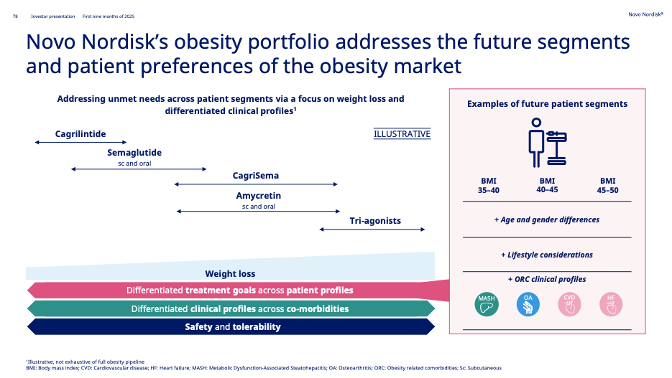
Source: Novo Nordisk 3Q25 slides, page 78
Close Concerns’ Questions
- How might Novo Nordisk advise healthcare providers to choose between CagriSema and Wegovy for obesity or Ozempic for T2D?
- How will payers evaluate the incremental clinical benefit of CagriSema over semaglutide monotherapy?
- Which baseline characteristics (A₁c, prior SGLT‑2 inhibitor use, etc.) were most strongly associated with greater A₁c and weight reduction with CagriSema?
- What additional cardiometabolic benefits did CagriSema confer in people with T2D and overweight or obesity?
- What will the “bar” be for late-breaker data submitted to ADA Sci Sessions in June?
--by Kayla Mathieu, Kat Moon, Monica Oxenreiter, and Kelly Close
[1]We remember similar claims about Amylin’s LAR back in the 00’s … “no plateau”. While this doesn’t always result in significantly more weight loss, we are listening closely.
[2] Trial sites were in the US, Argentina, Australia, Brazil, Bulgaria, Canada, China, Colombia, Croatia, Czechia, Denmark, Finland, Germany, Greece, Hungary, India, Israel, Italy, Japan, Mexico, Poland, Romania, Serbia, Slovakia, Slovenia, South Africa, South Korea, Spain, Sweden, Taiwan, Turkey, and United Kingdom.