WCIRDC 2025 Day #3 Highlights –
Executive Highlights
- The 23rd annual World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease (WCIRDC) conference featured fascinating talks today, ranging from beta cell regeneration and insulin sensitization to treatments for cardiovascular-kidney-metabolic (CKM) comorbidities.
- Several speakers explained pathophysiology of cardiometabolic diseases and proposed therapeutic targets. Dr. Philipp Scherer (UT Southwestern) underscored the central role of adipocyte-derived signals – leptin and endotrophin – in shaping fibro-inflammation and driving cardiometabolic disease. Leptin was found to be a key driver of fibrosis across multiple organs, including the kidney, liver, lung, heart, and vasculature. Endotrophin also contributes to fibroinflammation, with high levels associated with acute kidney injury, HIV-associated adipose fibrosis, coronary artery disease, and heart failure. Leptin and endotrophin neutralization are a promising strategy to mitigate fibroinflammatory disease across the kidney, liver, heart, adipose tissue, and cancer.
- Dr. Ralph DeFronzo (UT Health San Antonio) discussed emerging therapies for beta cell regeneration and insulin sensitization. Explaining the natural disease progression of T2D, he stressed that both should be targeted to ensure beta cell survival and metabolic health. For beta cell proliferation, he detailed inhibition of TXNIP, DYRK1A, and menin as potential treatment targets. For insulin sensitization, he advocated for pioglitazone use, demystifying concerns about weight gain and CV risks.
- Significant emphasis was made on the heart and the liver.
- On the liver, Prof. Michael Roden (Heinrich-Heine University Düsseldorf, Germany) emphasized that the liver plays a crucial pathogenic role in the CKM syndrome. Increasing data have shown that adipose tissue dysregulation may serve as the underlying driver. Prof. Roden elaborated this point by presenting data on the mechanistic pathway of the adipose tissue, subgroup populations affected by diabetes, and emerging treatment options.
- On peripheral artery disease (PAD), Dr. Marc Bonaca (University of Colorado) highlighted the growing burden, affecting one in five adults aged ≥65 years. People with diabetes are at especially high risk of limb amputation driven by infection and microvascular disease. Excitingly, GLP-1 RA semaglutide has shown to improve maximum walking distance in the STRIDE trial and lower the risk of major adverse limb events.
- We were also excited to attend “A Glimpse into the Future.” Dr. Steven Smith (Senior Global Medical Advisor, Zealand) highlighted petrelintide, Dr. Jason Brett (Principal Medical Head, Novo Nordisk) discussed amycretin and ziltivekimab, and Dr. Mikhail Kosiborod (SVP, CVRM late-stage development, AZ) reviewed its incretin-based therapies.
Table of Contents
- 1. Leptin and endotrophin as dual pillars of fibro-inflammation in cardiometabolic disease
- 2. Dr. Ralph DeFronzo on emerging therapies for beta cell regeneration and insulin sensitization
- 3. From the eyes of a cardiologist: Perspectives on healthy diets in cardiometabolic health for obesity management
- 4. Pipeline updates from Zealand: Advancing amylin innovation and diversifying cardiometabolic therapies
- 5. Pipeline updates from Novo Nordisk: Expanding incretin leadership and diversifying into inflammation and beyond
- 6. Pipeline updates from AstraZeneca: Addressing root cause of cardiometabolic disease
- 7. The role of the liver in the cardiovascular-kidney-metabolic syndrome
- 8. Peripheral artery disease in T2D: A modern epidemic of fragmented care
- 9. CVOTs in 2025 for heart failure, lipid management, and hypertension
- 10. Reframing hypercortisolism in T2D: Insights from the CATALYST trial from Dr. John Buse
1. Leptin and endotrophin as dual pillars of fibro-inflammation in cardiometabolic disease
In this morning session, Dr. Philipp Scherer (UT Southwestern) underscored the central role of adipocyte-derived signals in shaping fibro-inflammation and driving residual risk across cardiometabolic disease. He began by contrasting the biology of lean versus obese adipose tissue, drawing on previous observations from metabolically healthy obese mice. This background set the stage for his focus on adipocyte-derived signals as central determinants of cardiometabolic and fibrotic burden.
- Dr. Scherer highlighted leptin as a critical adipocyte-derived signal, with one study confirming its role as a driver of fibrosis across multiple organs. The study found that leptin-neutralizing antibodies revealed their ability to inhibit fibrosis progression in the kidney, liver, lung, heart, and vasculature. These findings reinforce leptin suppression as a therapeutic strategy to mitigate fibroinflammatory disease burden.
- Dr. Scherer highlighted endotrophin as another critical adipocyte-derived signal, with multiple studies confirming its role as a potent driver of fibrosis across organs. One study (n=90) found that in acute kidney injury, urinary endotrophin levels were increased. Another study (n=112) found that in HIV-associated adipose fibrosis, endotrophin and hydroxyproline were both significantly elevated. Cardiometabolic implications were emphasized through genetic and proteomic analyses linking endotrophin to coronary artery disease (CAD). Clinically, elevated endogenous endotrophin levels were associated with a greater risk of heart failure, reinforcing the quantitative link between adipose-derived fibroinflammatory signals and cardiac dysfunction. Together, these findings reinforce endotrophin neutralization as a promising strategy to mitigate fibroinflammatory disease burden across the kidney, liver, heart, adipose tissue, and cancer.
- Dr. Scherer concluded by positioning leptin and endotrophin as dual pillars of the fibroinflammatory microenvironment, connecting metabolic disease and cancer. Their modulation, through weight loss, incretin synergy, or antibody-based therapies, offers a path toward resolving residual disease and achieving broader cardiometabolic resilience.
2. Dr. Ralph DeFronzo on emerging therapies for beta cell regeneration and insulin sensitization
In this fascinating morning session, Dr. Ralph DeFronzo (UT Health San Antonio) discussed the future of menin inhibitors and insulin sensitizes for diabetes treatment. He began by emphasizing that, while seemingly distinct, beta cell proliferation and insulin sensitization are biologically interdependent. Indeed, a 1990 study on the natural history of T2D found that individuals with obesity first develop insulin resistance, causing beta cells to secrete higher amount of insulin. Over time, beta cells become physiologically deteriorated and die, leaving individuals unable to produce enough endogenous insulin. Hence, Dr. DeFronzo emphasized that beta regeneration therapies should be coupled with increasing insulin sensitivity to ensure survival.
- Beta cell proliferation. In humans, beta cell proliferation peaks at 2-3% in the first year after birth and declines with age. Adult beta cells are generally very difficult to stimulate as they do not proliferate in response to high glucose, growth factors, hormones, or drugs. Dr. DeFronzo said that juvenile beta cells are more responsive to glucose stimulation or GLP-1, however, which is why early T1D interventions can help preserve beta cells. Other physiological and pharmacologic conditions associated with beta cell proliferation include: (i) partial pancreatectomy; (ii) pregnancy; (iii) inhibition of thioredoxin-interacting protein (TXNIP); (iv) inhibition of dual-specificity tyrosine-regulated kinase-1a (DYRK1A); and (v) menin inhibitors. Dr. DeFronzo focused on the latter three as potential therapeutic targets.
- TXNIP is a protein strongly induced by glucose in human islets and is overexpressed in both T1D and T2D. It promotes oxidative stress, inflammation, impaired function, and importantly, beta cell death. Hence, the inhibition of TXNIP has been associated with improved beta cell function, survival, and proliferation. Indeed, verapamil, which has a TXNIP-inhibiting effect, preserved C-peptide in both children and adults with new-onset T1D. Another company TIXiMED has recently completed phase 1 trial of TIX100, a small molecule TXNIP inhibitor, for T1D.
- DYRK1A phosphorylates and thereby blocks a transcription factor NFaT (Nuclear Factor activated in T-cells) from entering the nucleus to promote beta cell proliferation. Harmine inhibits DYRK1A and dephosphorylates NFaT, which then activates beta cell replication. Moreover, in an in vivo study, harmine and GLP-1 RA markedly increased beta cell proliferation from 2-3% to 5-7%, suggesting synergistic effects of the combination therapy.
- Menin inhibition plays a crucial role in increasing beta cell mass during pregnancy, when insulin resistance and energy requirements of the fetus increases. Thus, menin levels decrease during the second trimester and increase after delivery. Moreover, menin inhibition promotes beta cell proliferation of human islet cells in vitro. In the phase 2b COVALENT-111 trial, Biomea Fusion’s oral covalent menin inhibitor icovamenib (BMF-219) significantly reduced A1c by 1.23 percentage points in insulin-deficient subgroups (~60% of T2D) and modestly reduced by 0.48 percentage point in insulin-resistant subgroups (~40% of T2D). This finding suggests that menin inhibitors may be effective in people with beta cell depletion, rather than insulin resistance.
- Insulin sensitization. Even when beta cell mass increases, insulin resistance will continue to stress and harm islet cells. Therefore, Dr. DeFronzo reiterated the importance targeting both beta cell-proliferation and insulin sensitization. Insulin sensitizers include: (i) PPAR agonists (thiazolidinedione [TZD], non-TZD, and novel TZD); (ii) imeglimin; (iii) DGAT2 inhibitor; (iv) FGF21 agonist; (v) AMPK activators; (vi) lyn kinase activators; (vii) GPR119 agonists; and (viii) natural alkaloids like berberine.
- Specifically, Dr. DeFronzo advocated for pioglitazone use, demystifying concerns about weight gain and cardiovascular (CV) risks. He said that unlike high calorie-induced weight gain, pioglitazone-associated weight gain is associated with improved metabolic parameters, including A1c, insulin sensitivity, beta cell function, blood pressure, and lipids. Moreover, although pioglitazone has been associated with increased risk of heart failure, several trials found 16% reduced risk of MACE in people with T2D and 24% reduced risk of recurrent stroke or MI in people without diabetes. Further clamp study found that pioglitazone improves insulin sensitivity in muscle, increases coronary blood flow, and enhance left ventricular diastolic function. Interestingly, individuals with more edemas had better outcomes, potentially reflecting higher drug response. Finally, in a real-world observational study, GLP-1 RAs and pioglitazone both reduced all-cause and CV mortality with additive effects when combined, given distinct mechanisms of action.
- Dr. DeFronzo concluded that GLP-1 RAs alone will not be sufficient to address the T2D epidemic. While obesity-driven T2D often responds well to GLP-1 RAs through weight loss, which has become increasingly prevalent, the therapy does not correct obesity-independent insulin resistance, which remains a fundamental driver of hyperglycemia. Thus, GLP-1 RA therapy alone may normalize weight but leave underlying insulin resistance unaddressed. Hence, Dr. DeFronzo advocated for combination strategy that incorporates: (i) beta cell proliferation and preservation through menin inhibitors, DYRK1A inhibitors, TXNIP inhibitors, and GLP-1 RAs; and (ii) insulin sensitization via pioglitazone and next-generation therapies.
3. From the eyes of a cardiologist: Perspectives on healthy diets in cardiometabolic health for obesity management
In an evening session, Dr. Pam Taub (UCSD) addressed healthy diets in cardiometabolic health for obesity management. Dr. Taub sparked laughter from the audience when she said that conference organizer Dr. Yehuda Handelsman must like her a lot, because she was chosen as the last speaker on the second-to-last day of WCIRDC. Her presentation strongly concluded the day, as she provided perspectives from the lens of a cardiologist on evidence-based dietary recommendations, intermittent fasting, and nutrition in people taking GLP-1 RAs.
- Lifestyle modifications as the foundation of obesity management. Dr. Taub said the “beauty” of lifestyle includes its synergies with pharmacotherapies, helping patients experience better outcomes with improved quality of life. She encouraged lifestyle interventions before treatment initiation, particularly in individuals who could benefit from preventive measures. In terms of therapies, Dr. Taub reflected on the multi-billion-dollar supplement industry and expressed disappointment that it’s targeting vulnerable patients to pay for “expensive urine,” as most treatments are not bioavailable. She therefore stressed the need for curating interventions based on evidence and understanding what lifestyle interventions fit each individual patient.
- Dr. Taub clarified that lifestyle intervention is not only about diet but also the quality, quantity, timing, and patient engagement. She reviewed the general dietary recommendations, with an emphasis on prioritizing a lower intake of refined sugar and processed foods, as well as increasing high-quality carbohydrates and fiber. Carbohydrates could be restricted in a beneficial way, but it’s important to do so in a safe manner, avoiding substitution with unhealthy fats.
- Dr. Taub recommended implementing technology to personalize diet recommendations. For example, CGMs can help patients understand how specific foods affect glucose levels and guide their dietary intake. Dr. Taub imagines a future with tailored diets beyond CGMs, including other apps and technological interventions.
- Not all “intermittent fasting” is created equal. One of Dr. Taub’s first studies in 2019 on 10-hour time-restricted eating showed that such an intervention could improve cardiometabolic health in people with metabolic syndromes. Following this study, a randomized trial (n=104) in 2024 assessed whether limiting daily dietary intake to 8-10 hours could provide cardiometabolic benefits. Results showed that compared to the control group, time-restricted eating improved A1c level by 0.1%. While many viewed this result as a modest improvement, Dr. Taub said that a 0.1% A1c improvement in the study population, who were at risk, represents a significant reduction that could help improve metabolic syndrome. Overall, Dr. Taub suggested that intermittent fasting may not be beneficial for everyone, but it could be helpful for specific populations.
- The importance of addressing the side effects of GLP-1 RAs. Dr. Taub shared several cases of her patients on GLP-1 RAs exhibiting vitamin and mineral deficiencies, an increased risk of anemia, and malnutrition. Because patients on GLP-1 RAs lose their appetite, they tend to gravitate toward consuming food they enjoy in limited quantities. These options, however, often fall into unhealthy categories, resulting in a poor overall quality of dietary intake. Dr. Taub highly encouraged HCPs to observe dietary patterns in people on GLP-1 RAs and enforce greater awareness and education among them.
- Dr. Taub noted concerns about sarcopenic obesity, which occurs with aging and results in excess fat and low levels of skeletal muscle. Studies have shown that many patients have sarcopenic obesity at baseline, even before initiating GLP-1 RAs. In this population and many others at risk of sarcopenic obesity, they need adequate protein intake and strength training to conserve and build muscle mass.
- The “cardiometabolic jackpot.” Dr. Taub concluded the session by presenting a slide with an animated jackpot machine labeled “cardiometabolic jackpot.” Dr. Taub stressed the importance of meeting an optimal combination of food content, calories consumed, duration of caloric consumption, meal frequency, and finally, a “WILD” card that includes: (i) genetics; (ii) exercise; and (iii) level of stress. She emphasized that HCPs must prioritize personalized diets and exercises that fit into the daily lifestyles of individual patients. Indeed, as many HCPs stress, one size doesn’t fit all.
4. Pipeline updates from Zealand: Advancing amylin innovation and diversifying cardiometabolic therapies
In this trademark “A Glimpse into the Future” session, Dr. Steven Smith (Senior Global Medical Advisor, Zealand) reviewed Zealand’s cardiometabolic pipeline. For those watching and wondering, type 1 diabetes was not only not a focus of any of three “A Glimpse into the Future” talks, adjunctive therapy (therapy outside insulin) for the T1D population was not mentioned. Perhaps next year, there could be a specific session on it (incretins, SGLTs, other therapeutic classes), and perhaps one day, T1D therapies will show up in the industry-based discussions, following a major FDA approval.
- Dr. Smith began by introducing the company’s pipeline across obesity and comorbidities, which includes: (i) petrelintide (long-acting amylin analog) in phase 2; (ii) combined petrelintide and CT-388 (GLP-1/GIP RA) soon to be in phase 2; (iii) survodutide (glucagon/GLP-1 RA) in phase 3 for obesity and MASH; and (iv) ZP6590 (GIP RA) soon to be in phase 1. Dapiglutide (GLP-1/GLP-2 RA) was discontinued in 3Q25. He then delved into the biology of amylin and therapeutic potential of petrelintide. First discovered in 1987, amylin is a neuroendocrine peptide hormone co-secreted with insulin by beta cells upon food intake. It exerts a multitude of metabolic benefits, such as increase in leptin sensitivity, satiety, energy expenditure, insulin sensitivity, and reduction in weight, insulin and glucagon secretion, and fat accumulation among others. Dr. Smith noted that a key difference from GLP-1 RAs is that amylin increases satiety, rather than reducing appetite, ultimately offering a distinct mechanism of action.
- Excitingly, petrelintide, which is co-developed with Roche, conferred weight loss by up to 8.6% compared to 1.7% in the placebo group in phase 1b results (n=48). The candidate is now evaluated in 42-week ZUPREME-1 trial (n=494) for people with overweight or obesity and in 28-week ZUPREME-2 trial (n=216) for people with overweight or obesity and T2D. Zealand also plans to initiate a phase 2 trial for a fixed-dose combination of petrelintide and Roche’s dual GLP-1/GIP RA, CT-388 in 1H26.
5. Pipeline updates from Novo Nordisk: Expanding incretin leadership and diversifying into inflammation and beyond
In this “A Glimpse into the Future” session, Dr. Jason Brett (Principal Medical Head, Novo Nordisk) spotlighted amycretin and ziltivekimab. Amycretin is a unimolecular GLP-1 and amylin RA evaluated for diabetes and obesity. In the phase 1b/2a trial (n=114) on obesity, subcutaneous amycretin led to ~24% weight loss (vs. 1.1% with placebo) at Week 36 from a baseline weight of 84-99 kg (184-218 lbs). While not mentioned in the talk, Novo Nordisk also recently shared topline results of the phase 2 trial (n=448) for people with T2D, in which subcutaneous and oral amycretin conferred up to 15% and 10% weight loss, respectively, compared to 3% with placebo at Week 36. The company will initiate the phase 3 AMAZE program in 1Q26, which will evaluate benefits across obesity, T2D, obstructive sleep apnea, knee osteoarthritis, and heart health.
- Dr. Brett also discussed ziltivekimab, a fully human monoclonal antibody directed against the IL-6 ligand, which has the potentially to reduce inflammation. In the phase 2 RESCUE trial, ziltivekimab lowered hsCRP by 93% at Week 24 with favorable safety profile. Ziltivekimab is now evaluated in the phase 3 ZEUS, HERMES, ARTEMIS, and ATHENA trials that evaluate the benefits on atherosclerosis and chronic kidney disease, heart failure, acute myocardial infarction, and HF function, respectively.
- Finally, Dr. Brett briefly commented on the evoke/evoke+trial, which evaluated Rybelsus (oral semaglutide) in people with symptomatic Alzheimer’s disease. While the trial did not see benefits on cognition or function, semaglutide improved neuroinflammation and other markers. Dr. Brett is proud that Novo Nordisk led these trials and is hopeful that the rich dataset will help the scientific and medical communities.
6. Pipeline updates from AstraZeneca: Addressing root cause of cardiometabolic disease
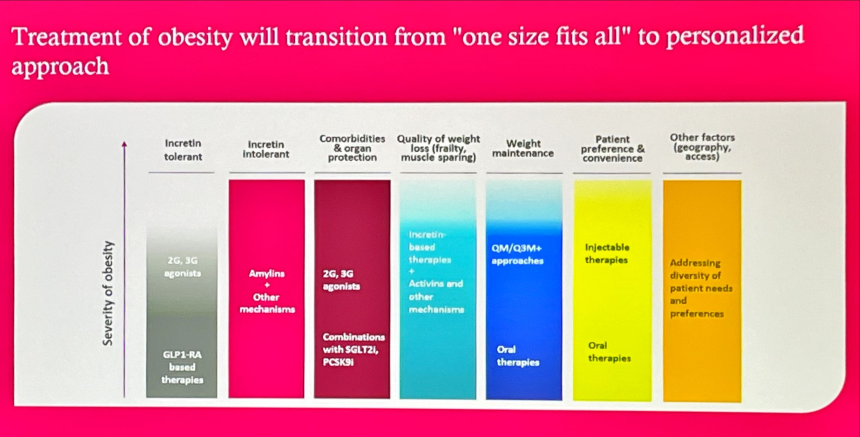
During this “A Glimpse into the Future” session, Dr. Mikhail Kosiborod (SVP, CVRM late-stage development, AZ) began with AZ’s broader vision, which is to address the root causes that underly cardiometabolic diseases: blood pressure, cholesterol, kidney function, adiposity, insulin resistance, and inflammation. He also shared the importance of simple administration methods and early combination therapy to achieve therapeutic goals and influence the standards of care. Among AZ’s comprehensive cardiovascular-renal-metabolic pipeline, Dr. Kosiborod spotlighted aldosterone synthase inhibitor baxtrostat, oral PCSK-9 inhibitor laroprovstat, and obesity therapies. On the latter, he emphasized that obesity treatment will move away from “one size fits all” to a more personalized approach (see figure below for his vision). AZ’s weight management portfolio includes: (i) AZD9550 (dual GLP-1/glucagon RA) currently in the phase 2b ASCEND trial (n=360); (ii) AZD5004 (oral GLP-1 RA) in the phase 2b VISTA and SOLSTICE trials for obesity and T2D, respectively; and (iii) AZD6234 (long-acting amylin analog) in the phase 2b APRICUS trial for obesity. Specifically, AZD5004 aims to serve patients with overweight, while AZD9550 aims to serve those with more severe obesity. AZD6234 aims to serve patients who cannot tolerate incretin-based therapies.
7. The role of the liver in the cardiovascular-kidney-metabolic syndrome
Prof. Michael Roden (Heinrich-Heine University Düsseldorf, Germany) emphasized that the liver plays a crucial pathogenic role in the cardiovascular-kidney-metabolic (CKM) syndrome. In October 2023, the AHA officially termed CKM to characterize the interconnected pathway of the disease. The field previously thought liver dysfunction was directly related to the liver or insulin resistance, but increasing data have shown that adipose tissue dysregulation may serve as the underlying driver. Prof. Roden elaborated this point by presenting data on the mechanistic pathway of the adipose tissue, subgroup populations affected by diabetes, and emerging treatment options.
- What happens in the liver? In people living with obesity and early stages of MASLD, the liver increases its mitochondrial oxidative capacity to accommodate excess fat – a compensatory adaptation by the mitochondria. However, this adaptation has limits, as in MASH and fibrosis, the mitochondria initially respond to the metabolic overload but eventually decline and face decompensation. Unlike the liver, visceral adipose tissue does not have compensatory mitochondrial adaptation. These differences ultimately reflect how visceral adipose tissue serves as a major driver of metabolic disease due to its limited ability to adapt.
- People with severe insulin resistant diabetes (SIRD) show the highest prevalence of MASLD. Referring to data on the prevalence of diabetes subtypes and comorbidities, Prof. Roden explained that those with SIRD show the highest risk of nephropathy, CVD, and endothelial dysfunction, as well as marked increases in peripheral neuropathy. Furthermore, individuals with SIRD demonstrate the highest liver lipid content at baseline, risk of liver fibrosis, and liver triglycerides. Furthermore, they exhibit the highest adipose tissue insulin resistance, in addition to visceral adipose tissue, which is associated with a related polygenic CVD risk and low-grade inflammation. People with SIRD are also significantly affected by metabolic damage at the level of lipotoxicity, mitochondrial stress, inflammation, and tissue fibrosis, leading to a higher risk of complications like MASLD. Therefore, Prof. Roden underscored the importance of understanding the development of complications along the trajectories of prediabetes and diabetes, including various subtypes.
- Emerging treatment options to address unmet needs for the CKM syndrome. Prof. Roden referred to Mark Twain’s quote, “Will power lasts about two weeks and is soluble in alcohol,” to emphasize the difficulty of managing CKM and the need for ongoing efforts to address unmet needs in this space. Some progress he highlighted included blood-restricted exercise training and therapeutics, such as semaglutide, which received FDA approval for MASH in August 2025.
8. Peripheral artery disease in T2D: A modern epidemic of fragmented care
During this engaging session, Dr. Marc Bonaca (University of Colorado) highlighted the growing burden of peripheral artery disease (PAD). Despite one in five of adults aged ≥65 years suffering from this condition, PAD remains a vastly under-diagnosed manifestation of atherosclerosis. Patients rarely volunteer symptoms like pain while walking unless asked directly, leading their clinician to miss early signs of the disease. However, even “mild” PAD is profoundly disabling, and Dr. Bonaca characterized it as “the most malignant form of atherosclerotic disease.” In individuals with T2D, PAD is frequently the first cardiovascular manifestation of atherosclerosis, which significantly increases the risk of further disease progression. Identifying mild functional symptoms early is therefore critical to altering the disease course before chronic limb-threatening ischemia (CLTI) develops.
- Dr. Bonaca cautioned about the epidemic of non-traumatic amputations. More than 450,000 incidences per year are concentrated in regions called the “stroke belt.” People with diabetes (PWD) account for the overwhelming majority of this limb loss, with the dominant driver being infection and microvascular disease, rather than large-artery occlusion. Antiplatelet medication vorapaxar was shown to decrease acute limb ischemia events, informing the VOYAGER trial(n=6,564), which led to the first FDA-approved therapy to reduce major adverse limb events (MALE) after lower-extremity revascularization: Xarelto (rivaroxaban). Dr. Bonaca explained that lowering LDL cholesterol linearly reduces MACE and MALE but does not mitigate the microvascular and infectious drivers that underlie most amputations in PWD.
- On therapies, Dr. Bonaca highlighted evidence for GLP-1 RAs as a potential disease modifier for PAD. Most notably, the STRIDE trial, led by Dr. Bonaca, revealed how functionally impaired even “early” PAD patients are, who can only walk <200 meters before stopping, and often only ~100 meters before feeling pain. Once-weekly semaglutide improved walking distance by ~40 meters, double the threshold typically considered clinically meaningful. Consistent improvement was seen across all functional measures of hemodynamic characteristics of the limb. Furthermore, in a pooled analysis of SOUL (n=9,650), FLOW (n=3,533), and STRIDE (n=1,363), semaglutide conferred a 28% reduction in hospitalization for CLTI, an endpoint typically associated with poor prognosis, as well as reduction in the incidence of limb infection, adverse events, and hospitalization for MALE.
- PAD care remains fragmented across cardiology, vascular surgery, and endocrinology. Dr. Bonaca said that modern care models often fail to care for a disease which spans the three domains. A collaborative, integrated care model could mitigate delayed diagnosis, rapid progression, and persistently high amputation rates. Coordinating care across various specialties is essential to improve outcomes for this large and underserved patient population.
9. CVOTs in 2025 for heart failure, lipid management, and hypertension
In a sweeping afternoon session, Dr. Norman Lepor (National Heart Institute) reflected on major cardiovascular outcomes trial (CVOT) readouts in 2025 that have changed cardiometabolic care. This year was especially marked by breakthroughs in heart failure (HF), lipid management, and hypertension, advancing CV prevention strategies.
- The SUMMIT trial (n=364) of tirzepatide in people with HFpEF and obesity met its primary endpoint, demonstrating a 38% reduction in CV death or a worsening HF event after 136 weeks. Furthermore, tirzepatide conferred significant improvements in HF hospitalizations, urgent HF visits, quality-of-life scores, and 6-minute walk distance.
- In the CORALreef Lipids trial (n=2,912), once-daily oral enlicitide (PCSK9 inhibition) conferred significant lipid lowering effects in adults with prior ASCVD or LDL ≥70 mg/dL, reducing LDL-c by 57%, non-HDL-c by 53%, ApoB by 50%, and Lp(a) by 28% at Week 24.
- The landmark VESALIUS-CV trial (n=12,257) showed that PCSK-9 inhibitor evolocumab reduced 3-point MACE (cardiovascular death, non-fatal MI, and non-fatal stroke) by 25% and, strikingly, lowered all-cause mortality by 20% (p=0.0005) in high-risk patients with subclinical atherosclerosis, including those with T2D, CVD, coronary artery disease, or peripheral artery disease (PAD),.
- In the ALPACA trial (n=320), twice-yearly dosing of lepodisiran (long-duration siRNA targeting Lp(a)) reduced Lp(a) by nearly 90% in individuals with baseline levels ≥175 nmol/L. Dr. Lepor looks forward to the upcoming HORIZON trial that will evaluate whether Lp(a) reduction translates into clinical event reduction.
- Across pooled analyses from BROOKLYN (n=354) and BROADWAY trials (n=2,530), obicetrapib (CETP modulator) demonstrated reductions in coronary events beyond six months of treatment in patients with heterozygous familial hypercholesterolemia (HeFH) and atherosclerotic cardiovascular disease (ASCVD).
- The PISCES trial (n=1,228) showed that daily n-3 fatty acid supplementation reduced rates of serious cardiovascular events in patients receiving maintenance dialysis.
- In Advance-HTN trial (n=285) lorundrostat (aldosterone synthase inhibitor) reduced systolic blood pressure by an average 8 mmHg after 12 weeks in people with uncontrolled hypertension. Notably this was accompanied by a mean 0.4 mEq/L rise in serum potassium.
- The BaxHTN trial (n=796) demonstrated that baxdrostat in patients with uncontrolled and resistant hypertension confers an ~8-10 mmHg reduction in systolic blood pressure after 12 weeks, with moderate hyperkalemia risk similar to mineralocorticoid receptor antagonists (MRAs).
10. Reframing hypercortisolism in T2D: Insights from the CATALYST trial from Dr. John Buse
Dr. John Buse (University of North Carolina) presented data from the CATALYST trial (n=1,113), reframing hypercortisolism as a common, under-recognized contributor to difficult-to-control T2D. He opened by positioning hypercortisolism within the broader pathophysiology of diabetes — alongside insulin resistance, lipolysis, and hepatic glucose production – and argued that excess cortisol should be considered as part of Dr. Ralph Defronzo’s “noxious nine” that drives hyperglycemia. Part 1 of the CATALYST trial (n=1,057), published in April 2025, revealed a 24% prevalence of hypercortisolism, defined by post-DST cortisol >1.8 µg/dL with adequate dexamethasone levels. Importantly, this phenotype was not based on classical Cushingoid appearance but on multimorbidity and medication burden, with predictors including age, ethnicity, lower BMI, and use of SGLT-2 inhibitors, tirzepatide, and high-dose GLP-1 RAs. Specifically, Dr. Buse pointed to the fact that lower BMI was associated with a higher risk.
- Dr. Buse then highlighted results from the Part 2 of the study (n=136), presented at ADA in June 2025. In the trial, mifepristone demonstrated clinically meaningful improvements in glycemic levels and body weight. Among participants with hypercortisolism, mifepristone reduced A1c by 1.5% from a baseline of 8.6%. These improvements occurred despite greater reductions in glucose-lowering medications and were consistent across subgroups with and without adrenal imaging abnormalities. Mifepristone also led to a 5.1 kg (~11.2 lbs) placebo-adjusted reduction in body weight, corresponding to a 3.6% decrease from baseline.
- Safety. Safety findings were consistent with mifepristone’s known profile, with no new safety signals identified. Adverse events were common but mostly mild to moderate. 95% of participants on mifepristone experienced at least one TEAE, and 29% discontinued due to side effects. Hypokalemia was the most frequent event (30%), attributed to mineralocorticoid receptor overstimulation, and was manageable with potassium-sparing diuretics. Serious TEAEs occurred in 32% of mifepristone-treated participants versus 5% on placebo, with hypokalemia and euglycemic ketoacidosis (in SGLT-2 inhibitor users) reported in 3% of participants.
- Clinical implications. Dr. Buse concluded by emphasizing the clinical implications of cortisol-directed therapy in diabetes care. He advocated for routine screening in patients with difficult-to-control T2D, noting that a single 1-mg dexamethasone suppression test with cortisol and dexamethasone levels is sufficient to identify ACTH-independent hypercortisolism. The CATALYST findings offer evidence that targeting cortisol excess can improve glycemia, reduce medication burden, and support weight loss. He urged clinicians to adopt individualized, patient-centered strategies when prescribing mifepristone, including proactive management of hypokalemia and clear communication about steroid withdrawal symptoms.
--by Kayla Mathieu, Elizabeth Rose, Esther Min, Kat Moon, Monica Oxenreiter, and Kelly Close