WCIRDC 2025 Day #4 Highlights –
Executive Highlights
- The 23rd annual World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease (WCIRDC) conference concluded strongly today, featuring pathophysiology of obesity to clinical pearls on diabetes technology use. We are thankful for all the insights from the past four days. If anyone missed it, check out our coverage for Days #1, #2, and #3.
- Dr. Tracey McLaughlin (Stanford) delivered this year’s Gerald Reaven Award Lecture on how excess adipose tissue causes metabolic dysfunction. She explained that not all obesity or overweight manifest the same clinically; insulin resistance is the key driver of metabolic dysfunction, as well as heterogeneity in treatment response to weight loss. In a three-part hypothesis, Dr. McLaughlin proposed that obesity causes adipose tissue remodeling, similar to that of chronic wound healing. Specifically, visceral fat, inflammation, and impaired adipogenesis are key drivers of insulin resistance. This hypothesis explains why how pioglitazone improves metabolic health despite causing weight gain, as the drug acts directly on adipose biology.
- On therapy, Dr. Sunder Mudaliar (UCSD) traversed the “incretin jungle,” reviewing the ever-expanding landscape of mono, dual, triple, and even higher-order agonists. He stressed the importance of better understanding the GIP paradox, in which both agonists and antagonists confer weight loss when combined with GLP-1 RAs. On emerging therapies, he highlighted a renewed interest in amylin, a hormone which slows gastric emptying, suppresses glucagon, and reduces appetite, as well as IGF (insulin-like growth factor), PYY (peptide YY), FGF21 (fibroblast growth factor 21), and GLP-2.
- On technology, Dr. Viral Shah (Indiana University) discussed the use of CGM in prediabetes, spotlighting the diagnostic potential of dynamic glucose changes. Dr. Shah began by presenting data from a multicenter study (n=153) of CGM use in people without diabetes, whose average glucose was 99 mg/dL, Time in Range (TIR; 70-140 mg/dL) of 95%, and Time Above Range (TAR; >140 mg/dL) of 2.9%. Dr. Shah argued that TAR >5% may indicate early dysglycemia, given its high sensitivity for identifying stage 2 T1D. Dr. Shah advocated for personal CGM profiles or “glucotypes” that may better capture metabolic risk than A1c.
Table of Contents
- 1. Gerald Reaven Award Lecture: Dr. Tracey McLaughlin details pathophysiology behind obesity and metabolic dysfunction
- 2. Dr. Sunder Mudaliar explores the “incretin jungle” from GIP paradox to emerging agents
- 3. CGM in prediabetes: Sensor variability and the need for new standards
- 4. Obesity burden and CGM benefits in people with T1D
- 5. Medical management of HFmrEF and HFpEF with rapid sequence or simultaneous initiation of SGLT-2 inhibitors, nsMRAs, and GLP-1 RAs
1. Gerald Reaven Award Lecture: Dr. Tracey McLaughlin details pathophysiology behind obesity and metabolic dysfunction
Dr. Tracey McLaughlin (Stanford) delivered the Gerald Reaven Distinguished Leader in Insulin Resistance 2025 Award Lecture, highlighting the heterogeneity of obesity and its underlying pathophysiology. Not all people with obesity or overweight have the same cardiometabolic risk or treatment response. Dr. McLaughlin argued that this heterogeneity is due to the presence of insulin resistance. In individuals with obesity, insulin resistance is associated with increased risk of hypertension and impaired fasting glucose among other adverse outcomes. Moreover, people with insulin resistance were shown to metabolically benefit the most from dietary changes and weight loss. She presented three hypotheses that explain how excess adiposity drives insulin resistance and why it differs between individuals.
- Adipose tissue is highly dynamic. Composed of adipocytes, macrophages, fibroblasts, endothelial cells, and T cells, adipose tissue plays an important role in fat storage, cytokine signaling, structural support, and angiogenesis. Obesity causes tissue remodeling– similar to that of chronic wound healing – that lead to adipocyte death, inflammation, and fibrosis, and many diseases. Notably, she highlighted visceral fat, inflammation, and abnormal adipogenesis as drivers of metabolic dysfunction.
- Visceral and ectopic fat drains directly into the liver, exposing it to free fatty acids and inflammatory cytokines that drive hepatic insulin resistance, dyslipidemia, fatty liver disease, fibrosis, and reduced insulin clearance. Intrahepatic fat is significantly correlated with insulin resistance. Similarly, individuals with prediabetes and diabetes have greater pancreatic fat. Given the pathogenic role of visceral fat, she said that visceral-to-subcutaneous fat ratio is a more accurate predictor of clinical outcomes than total fat.
- Inflammation in adipose tissue plays a significant role in driving metabolic dysfunction in visceral fat. Normal adipose tissues mainly consist of anti-inflammatory M2 macrophages and regulatory T cells. On the other hand, in enlarged adipose tissue, there is a greater number of pro-inflammatory M1 macrophages, CD8+ T cells, and adipokines, resulting in chronic low-grade inflammation. This may be because macrophages surround necrotic adipocytes to scavenge lipid debris. Inflammation and free fatty acids directly impair insulin-mediated glucose uptake through cellular pathways. Indeed, in individuals with obesity, those with insulin resistance display upregulation of inflammatory genes compared to those without insulin resistance.
- Impaired adipogenesis or fat storage is hypothesized as a pathogenic cause behind inflammation. Healthy fat expansion occurs through hyperplasia – increase in the number of fat cells – which allows lipid storage without metabolic injury. In contrast, unhealthy fat occurs via hypertrophy –increase in the size of fat cells – due to impaired adipocyte differentiation. This can cause hypoxia, ER stress, necrosis, macrophage recruitment, inflammation, and increase in ectopic and visceral fat, all of which leads to insulin resistance and diseases. In humans, those with insulin-resistance are more likely to display impaired adipogenesis.
- Pioglitazone (PPAR-γ agonist), which acts directly on adipose biology, supports these hypotheses. The drug promotes adipocyte differentiation, increases the number of healthy small adipocytes, and shifts fat deposition from visceral to subcutaneous, ultimately improving in insulin sensitivity. This mechanism of action explains why pioglitazone is a potent insulin sensitizer despite its well-known side effect of weight gain. Ultimately, Dr. McLaughlin encouraged clinicians to account for heterogeneity of obesity to identify individuals at risk and offer precision treatments to those who may benefit most.
2. Dr. Sunder Mudaliar explores the “incretin jungle” from GIP paradox to emerging agents
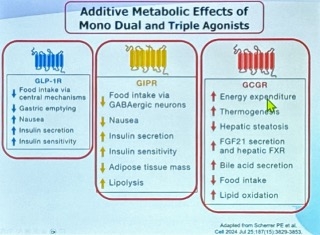
In an exciting afternoon address, Dr. Sunder Mudaliar (UCSD) traversed the “incretin jungle,” reviewing the ever-expanding landscape of mono, dual, triple, and even higher-order agonists. Dr. Mudaliar began by reminding the audience that GLP-1 RAs are approved for T2D, cardiovascular (CV) risk reduction, obesity, and chronic kidney disease (CKD) risk reduction. He remarked that these medicines are so effective that it would be against standard of care if clinicians don't use them when indicated. Newer classes like dual GIP/GLP-1 RA tirzepatide and triple GLP-1/GIP/glucagon RA retatrutide have demonstrated to deliver unprecedented weight loss above 20%.
- One confounding aspect of the “incretin jungle” is the GIP paradox: both agonists and antagonists, in combination with GLP-1 RAs, confer weight loss. From the practical point of view, he acknowledged that clinicians may not necessarily need to resolve mechanistic questions to use the drugs effectively. Yet, he stressed that it is critical to understand both mechanisms for advancing our understanding of physiology and in developing the next generation therapies. For more on this paradox, see previous coverage from ADA.
- Triple agonists appear to “supercharge” metabolic effects of dual agonists with glucagon agonism. Glucagon agonism contributes to increased energy expenditure, enhanced fat oxidation, and reduced liver fat. Furthermore, it may also have synergistic effects on satiety when combined with GLP-1 and GIP. In a phase 2 trial (n=338), retatrutide demonstrated nearly 25% weight loss over 48 weeks of therapy. Still, increased heart rates and GI events at higher doses were noted as potential side effects of the therapy.
- Dr. Mudaliar also highlighted a renewed interest in amylin, a hormone which slows gastric emptying, suppresses glucagon, and reduces appetite. Unsurprisingly, he added amylin analogs as another critical branch of the “incretin jungle,” particularly in combination with GLP-1 RAs. With semaglutide, amylin analogs have been shown to produce large, additive weight-loss effects – often ranging from 15-20%. Long-acting versions of these therapies remain in development, such as eloralintide, cagrilintide, and petrelintide, as well as a once-monthly formulation with promising early results.
- Emerging agents, including IGF (insulin-like growth factor), PYY (peptide YY), FGF21 (fibroblast growth factor 21), and GLP-2, will continue to “thicken” the incretin jungle with novel dual, triple, quadruple agonists, and even a quintuple agonist. As efficacies with new therapies increase, issues related to cost, access to medications, tolerability, side effects, adherence, non-responders, and durability or weight loss remain as primary concerns.

3. CGM in prediabetes: Sensor variability and the need for new standards
In this session, Dr. Viral Shah (Indiana University) discussed the use of CGM in prediabetes, spotlighting the diagnostic potential of dynamic glucose changes. Dr. Shah began by presenting data from a multicenter study (n=153) of CGM use in people without diabetes, whose average glucose was 99 mg/dL, Time in Range (TIR, 70-140 mg/dL) of 95%, and Time Above Range (TAR; >140 mg/dL) of 2.9%. Dr. Shah argued that TAR >5% may indicate early dysglycemia, given its high sensitivity for identifying stage 2 T1D, while a higher diagnostic threshold of TAR >10% may be more sensitive and precise. Dr. Shah suggested that personal CGM profiles or “glucotypes” could better capture metabolic risk than static thresholds like A1c.
- Dr. Shah discussed the limitations of CGMs in people with and without diabetes, noting that the accuracy standards designed for diabetes care may not be relevant for individuals without diabetes. He explained that the commonly accepted “±15/15%” accuracy threshold – i.e., CGM values are considered accurate if they fall within 15 mg/dL or 15% of reference glucose – can be problematic in people without diabetes. For example, a glucose level of 100 mg/dL could be reported anywhere between 85-115 mg/dL, which straddles the diagnostic boundary between normal and prediabetes.
- He illustrated this further using his own CGM data, which would classify him as progressing to diabetes by Dexcom but not by Abbott. This real-life example underscores the variability between sensor platforms. Dexcom reported 6% TAR, while Libre showed only 1% TAR, despite similar average glucose values of 107 mg/dL and 96 mg/dL with Dexcom and Abbott’s CGM, respectively. He explained that this discrepancy reflects differences in algorithm generations and calibration protocols. In a study (n=19,819), there was a regression bias of -0.026x + 9.946 mg/dL between first and third-generation Libre sensors, meaning the newer sensor tended to read about 10 mg/dL higher at lower glucose values and slightly lower at higher glucose values. This finding reinforces that current CGM research is only applicable to the specific sensor used. Dr. Shah concluded with a call to action that CGM accuracy standards must be redefined for people without diabetes, where small deviations can impact diagnostic classification. He further stressed the need for prospective studies to evaluate CGM’s role in diabetes prevention and therapeutic guidance.
4. Obesity burden and CGM benefits in people with T1D
In this morning session, Dr. Peter Reaven (Phoenix VAMC, Arizona College of Medicine) highlighted two studies on the rising burden of obesity and CGM use in people with T1D. He said that while advancements in diabetes technology have offered meaningful benefits on glycemia and health outcomes, the rising prevalence of obesity and its comorbidities may offset these gains. Moreover, the low uptake of anti-obesity medications (AOMs) and the absence of targeted weight management strategies in T1D remain a major gap in current practice. Dr. Reaven concluded that understanding the drivers of weight gain in T1D, developing specific algorithms for use of AOMs for them and integrating these with appropriate diabetes technology will be essential to improving long-term outcomes in this population.
- Dr. Reaven illuminated persistent mortality risks and emerging opportunities for intervention in T1D management. He drew on national Veterans Affairs (VA) data to highlight several of these points. He pointed out that despite advances in diabetes technology, mortality rates in T1D remain high and may be exacerbated by rising rates of overweight and obesity. In a recent study of T1D (n=9,712) he showed that 72% of adults in the VA system had overweight or obesity. Prevalence was highest in the 40-59 age group (78%), but was disturbingly high in the 21-39 age group. Prevalence rates of overweight and obesity also rose rapidly from 2016-2023, and increased by nearly 50% in the youngest age group. Obesity was associated with significantly worse cardiometabolic profiles, including higher systolic blood pressure (132 mmHg vs. 129 mmHg in individuals with normal weight), triglycerides (133 mg/dL vs. 105 mg/dL), lower HDL-c (47 mg/dL vs. 56 mg/dL), and higher LDL-c (98 mg/dL vs. 93 mg/dL). Moreover, 30% of the obesity group appeared to have the metabolic syndrome compared with 1% of the normal weight group. These findings may support the reverse J-shaped mortality curve reported in the FinnDiane study (n=5,836), where both low and high BMI were linked to increased mortality risk, with the lowest hazard observed at BMI of 24-25 kg/m² and higher risk at BMI <18.5 kg/m² (HR=4.26) and ≥30 kg/m² (HR=1.25).
- The second half of the session focused on CGM use and its impact on mortality in T1D. Using a target trial emulation framework of T1D patients (n= 8,423,) he reported that CGM initiation was associated with a 16% lower risk ratio for all-cause mortality over four years. Survival curves for CGM users vs. nonusers began to separate shortly after the 6‑month grace period. Subgroup analyses showed consistent benefit across age, race, A1c levels, and frailty status. CGM use was even more strongly associated with lower all-cause mortality among patients not on insulin pumps at baseline, and in this subgroup, CGM use was associated with reduced hospitalization by 12%, hypoglycemia by 32%, and cardiovascular disease (CVD) events by 18%. These findings build on earlier observational data and suggest that CGM may be a powerful tool for reducing mortality in high-risk T1D populations.
5. Medical management of HFmrEF and HFpEF with rapid sequence or simultaneous initiation of SGLT-2 inhibitors, nsMRAs, and GLP-1 RAs
Reflecting on the evolution of interventions, Dr. Gregg Fonarow (UCLA) emphasized rapid or simultaneous initiation of therapies as the foundational strategy for HFmrEF and HFpEF. Focusing on patients with HFmrEF and HFpEF remains an important strategy, as they contribute to a significant number of heart failure cases, with rising prevalence in the number of hospitalizations and deaths. HFmrEF and HFpEF result from a heterogeneous pathophysiology, including diastolic dysfunction, obesity, diabetes, and CKD. While prior approaches have focused on diuretics and comorbidities, recent trials and guidelines have shifted the focus to disease modification, particularly with the emergence of novel treatments. The three pillars of therapy for HFmrEF and HFpEF now include: (i) SGLT-2 inhibitors; (ii) nsMRAs; and (iii) GLP-1 RAs. Dr. Fonarow strongly encouraged the use of these treatments and, furthermore, emphasized the efficacy of rapid or simultaneous initiation of guideline-directed medical treatments (GDMT) for improved clinical outcomes and patient-reported quality of life.
- Studies demonstrate the efficacy of rapid or simultaneous initiation of GDMT. Similar to a 2021 viewpoint articlefor HFrEF, Dr. Fonarow and his colleagues pushed for a rapid sequence or simultaneous initiation of the three pillars of treatment for HFmrEF and HFpEF in another viewpoint article published earlier this year. The article emphasizes the clinical benefits that appear within days to weeks following GDMT, citing studies such as EMPEROR-PRESERVED of SGLT-2 inhibitors, FINEARTS-HF of nsMRAs, and STEP-HFpEF of GLP-1 RAs. Furthermore, the three pillars of treatment have shown additive benefits, not only for hospitalization due to heart failure but also for MACE and kidney outcomes.
- Addressing the concern about whether starting multiple treatments simultaneously increases the risk of intolerance. Dr. Fonarow acknowledged hesitations among HCPs and patients worrying that polypharmacy alters the safety and efficacy of treatments for HFmrEF and HFpEF. Contrary to many beliefs, he referenced a 2023 and 2024 study to clarify that the efficacy of heart failure treatments does not appear to be diminished among patients taking several medications at baseline.
- Additional strategies to help facilitate GDMT initiation. Dr. Fonarow outlined several considerations to support early and combined GDMT in patients with HFmrEF and HFpEF, including the use of digital health tools, patient activation programs, and interdisciplinary teamwork. He also highlighted the time to diagnosis to optimal GDMT as a key quality metric in heart failure, a focus of his editorial published a couple of months ago. In this article, Dr. Fonarow and his colleagues examined different definitions and scores of GDMT adherence to quantify therapy intensity at discharge and follow-up among patients. Using the scores, they identified differences in GDMT exposure and intensity, with faster and more protocolized GDMT titration resulting in better outcomes for patients with heart failure.
-- by Elizabeth Rose, Kayla Mathieu, Kat Moon, Esther Min, and Kelly Close