JPM 2026 Day #2 Highlights –
Executive Highlights
- The second day of the 44th Annual JP Morgan Healthcare Conference continued to highlight lots of movement across and interest in the expansive fields of obesity and diabetes specifically and healthcare more broadly! Building on all the learnings from JPM Day #1, we appreciated the continued focus on the vast landscape across therapies and technology that relate to diseases we watch, namely diabetes and obesity. As we look ahead to additional insightful presentations tomorrow, check out our Resource Hub, and look at what we’re looking forward to in our Preview – seven more companies, effectively, including Amphastar, Biomea, embecta, Omada Health, Sana Biotechnology, Virta Health, and Zealand, as well as several panel discussions on addressing employers’ drug costs, what’s next from ARPA-H, and updates from the FDA Commissioner Dr. Marty Makary.
- In therapy, we heard even more updates on cardio-renal-metabolic health.
- AstraZeneca: Dr. Aradhana Sarin (CFO) presented AZ’s 2025 broad-scale results and outlook for the decade to come, with a focus on cardiometabolic health second only to oncology. Positive baxdrostat – which is currently under FDA Priority Review – trial results were highlighted as helping drive AZ’s momentum across a diverse pipeline. Addressing weight management and cardiovascular risk factors will form a key part of AZ’s long-term strategy, as Dr. Sarin said that AZ is uniquely positioned to deliver novel small molecule combinations and is committed to “accelerating programs into late-stage development.”
- Bayer: Mr. Stefan Oelrich (Bayer President of Pharmaceuticals Division) shared updates on Bayer’s therapies, including: (i) non-steroidal MRA Kerendia (finerenone); and (ii) anti-VEGF Eylea (aflibercept). Mr. Oelrich called Kerendia the next blockbuster drug as it has demonstrated accelerated growth in T2D, CKD, and heart failure. Several phase 3 trial results are expected to complete in 2026: (i) FIND-CKD trial (n=1,584) of Kerendia in adults with non-diabetic CKD; (ii) REDEFINE-HF trial (n=5,200) of Kerendia in hospitalized heart failure patients; and (iii) CONFIRMATION-HF trial (n=1,500) of the combination of Kerendia and SGLT-2 inhibitor in hospitalized patients with heart failure.
- Lilly: CEO Mr. David Ricks shared reflections from 2025 and vision for the coming years for Lilly. On orforglipron, which delivered key phase 3 results for T2D and obesity last year, Mr. Ricks said that regulatory filing submitted to the FDA under the new priority voucher program. Approval is expected in 2Q26. Mr. Ricks speculated that oral formulation would be helpful for patients with aversion to needles, perception of escalating medicine from lifestyle modifications to injectable medicines, or those already on polypharmacy. On the overall obesity market, Mr. Ricks welcomed companies entering the obesity landscape. He emphasized that Lilly will maintain its excellence in R&D and “multiple shots for goals” strategy to develop differentiated candidates. Looking forward, he expects more swings in 2026.
- Novo Nordisk: CEO Mr. Maziar Mike Doustdar shared his perspectives on the challenges Novo Nordisk has faced and its vision for 2026 and onward. The company had a turbulent year in 2025 due to market challenges from continued compounding business, competition, and pricing pressure, and Mr. Doustdar characterized these challenges as the “curse of a leader” of having to navigate clinical development and commercialization through trial-and-error. On the overall strategy for 2026, Mr. Doustdar highlighted three key goals: (i) master direct-to-patient and cash channels; (ii) expand the market through Wegovy pills; and (iii) reframe market perception of injectable semaglutide by launching higher dosage options. Mr. Doustdar highlighted CagriSema (fixed-dose cagrilintide and semaglutide) and amycretin as important late-stage assets in its clinical pipeline.
- In tech, Insulet shared updates on its commercial plans and Alphabet subsidiary Verily reviewed its product offerings.
- Insulet: CEO Ms. Ashley McEvoy highlighted several advantages that underscore Insulet’s position in the AID competitive landscape. She outlined a coordinated strategy across US T1D, OUS T1D, and US T2D to drive the next leg of growth, highlighting the under-penetration seen across all three populations. She also highlighted Insulet’s innovation pipeline, with ~$1 billion planned investment in technology over the next three years.
- Verily: CEO Mr. Stephen Gillett talked about Verily’s recent progress and strategic direction. Presumably, this is in advance of an IPO. He overviewed Verily Me, the company’s consumer-facing personalized health app that entered a beta launch in October 2025, as well as advancements in Verily Pre, the company’s data platform for healthcare research and AI.
- At a lunch symposium, Dr. Mehmet Oz (CMS Administrator), Mr. Daniel Brillman (Deputy Administrator and Director), Ms. Stephanie Carlton (Deputy Administrator & Chief of Staff), Mr. Chris Klomp (Deputy Administrator & Director), and Ms. Amy Gleason (Strategic Advisor) discussed their approaches to improving long-term US health. They said that GLP-1 RAs are a “wise investment” into long-term health that should be approached in a responsible way and that technology and AI may offer opportunities to change healthcare infrastructure and revolutionize rural care.
Table of Contents
-
Diabetes Therapy
- 1. Lilly: Mr. David Ricks shares insights about obesity market, payment channels, and clinical pipeline including orforglipron
- 2. Novo Nordisk: Mr. Mike Doustdar on mastering cash channel, reframing perception of the semaglutide, and clinical pipeline with CagriSema, cagrilintide, and amycretin
- 3. Teva Pharmaceuticals: Teva to shift from generics firm to global biopharmaceutical company
- 4. AstraZeneca: Cardiometabolic focus for 2030 and beyond led by aldosterone synthase inhibitor baxdrostat, PCSK-9 laroprovstat, and GLP-1 RAs in development
- 5. Kailera Therapeutics: CEO Mr. Ron Renaud highlights diversified GLP-1 RA pipeline for obesity treatment
- 6. Bayer: Kerendia (finerenone) demonstrates blockbuster potential for CKD and heart failure; pricing pressures with Eylea (aflibercept)
- 7. Ionis Pharmaceuticals: Tryngolza gains traction in treatment of FCS ahead of broader launch; pelacarsen for Lp(a) risk reduction on track for launch in 2027
- Diabetes Technology
- Diabetes Big Picture
Diabetes Therapy
1. Lilly: Mr. David Ricks shares insights about obesity market, payment channels, and clinical pipeline including orforglipron
In a packed afternoon symposium, CEO Mr. David Ricks shared reflections from 2025 and vision for the coming years for Lilly. He first celebrated that this year marks 150 years of Lilly’s existence and leading innovation since 1876. He then offered reflections about the past couple of years. After a “choppy, unclear year” in 2024 with uncertainty about supply, access, and drug uptake, Lilly delivered strong performance in 2025, stabilizing all three of those factors. There is no longer a shortage of tirzepatide; negotiations with the US government expanded access with lower price burden for patients; and LillyDirect reached more patients through cash channel. Moreover, Lilly continues to advance its clinical pipeline, including tirzepatide (dual GLP-1/GIP RA), orforglipron (oral GLP-1 RA), retatrutide (triple GLP-1/GIP/glucagon RA), eloralintide (long-acting amylin agonist), brenipatide (dual GLP-1/GIP RA), and six additional programs in phase 1. Mr. Ricks said these candidates have the potential to treat one billion people worldwide with obesity, cardio-renal-metabolic diseases, obstructive sleep apnea, and potentially even neurological or inflammatory diseases. Indeed, the indications continue to expand, as a recent phase 3 TOGETHER-PsA trial (n=271) showed significant benefits of tirzepatide when administered together with Taltz (ixekizumab) in people with psoriatic arthritis. In a dialogue with Mr. Chris Schott (Managing Director, JPMorgan), Mr. Ricks shared his insights about the obesity market, payment channels, and the competitive landscape.
- On orforglipron, which delivered key phase 3 results for T2D and obesity last year, Mr. Ricks said that regulatory filing submitted to the FDA under the new priority voucher program. Approval is expected in 2Q26. Mr. Ricks speculated that oral formulation would be helpful for patients with aversion to needles, perception of escalating medicine from lifestyle modifications to injectable medicines, or those already on polypharmacy. Moreover, orforglipron can be a promising option for those who want weight maintenance. In a blinded phase of a clinical trial, orforglipron conferred greater weight loss in people who discontinued semaglutide and gained modest weight in those who took tirzepatide; ultimately, orforglipron stabilized weight loss from either of the two medications. He especially believes that orforglipron would be more dominant than injectable GLP-1 RAs in OUS markets, where launch is expected in 2026 and 2027. Responding to Mr. Mike Doustdar’s (CEO, Novo Nordisk) comment on a clinical trial protocol, in which participants were directed to wait two to four hours after statin administration, Mr. Ricks said that the protocol was largely due to the timing of clinical development – Lilly had simply not conducted drug interaction studies with statins when initiating the trial.
- On different payment channels, Mr. Ricks said that Medicare has better penetration than the commercial market. Because government coverage often becomes the standard, the inclusion criteria for coverage tend to be more based on science. For tirzepatide, the criteria include people with overweight and comorbidities (e.g., CVD, peripheral artery disease, and prediabetes) or obesity – which Mr. Ricks said is significantly better than most commercial coverage. Moreover, with the recent Most Favored Nation negotiation – which Mr. Ricks characterized as a “unique deal” – out-of-pocket cost is “reasonable” at $50. He believes that all states will follow this standard for Medicaid programs and hopes that the coverage will spill over to commercial channels. Mr. Ricks added that incretin-based therapies offer preventive benefits, which is even more beneficial for countries with higher healthcare costs, as the return-on-investment is greater.
- On the commercial channel, he shared that new pharmacy benefit managers (PBMs) are emerging with more price transparency. He advocated for greater transparency is needed in the US, including what the post-rebate cost will be.
- LillyDirect, Lilly’s direct-to-consumer platform, has been very successful. He said that the price transparency with knowing the exact cost before buying, as well as notices for renewal cycle, allows patients to take charge of their own health.
- On the overall obesity market, Mr. Ricks welcomed companies entering the obesity landscape. He emphasized that Lilly will maintain its excellence in R&D and “multiple shots on goal” strategy to develop differentiated candidates. Looking forward, he expects more swings in 2026, especially given the uncertainty about the volume. Hence, the company will likely provide a guidance with a broader range. Finally, he also pointed to its AI initiatives, including its collaboration with NVIDIA, as opportunities for growth.
2. Novo Nordisk: Mr. Mike Doustdar on mastering cash channel, reframing perception of the semaglutide, and clinical pipeline with CagriSema, cagrilintide, and amycretin
In this packed symposium, CEO Mr. Maziar Mike Doustdar shared his perspectives on the challenges Novo Nordisk has faced and its vision for 2026 and onward. He began by reiterating Novo Nordisk’s commitment to treating obesity, diabetes, and comorbidities. Given that only 7% of people with diabetes and 2% of those with obesity are prescribed GLP-1 RAs or obesity medications worldwide, there is a significant unmet need that Novo Nordisk can address. That said, Novo Nordisk had a turbulent year in 2025 due to market challenges from continued compounding business, competition, and pricing pressure. Mr. Doustdar characterized these challenges as the “curse of a leader” of having to navigate clinical development and commercialization through trial-and-error. For over a decade, Novo Nordisk often faced doubts for developing medications for obesity, a condition previously considered as a lifestyle choice. Mr. Doustdar said that in 2025, the company had to critically recognize that the landscape had significantly changed, and that Novo Nordisk was no longer alone in the field. He further detailed what Novo Nordisk would have done differently and what key priorities the company will pursue in 2026.
- On the overall strategy for 2026, Mr. Doustdar highlighted three key goals: (i) master direct-to-patient and cash channels; (ii) expand the market through Wegovy pills; and (iii) reframe market perception of injectable semaglutide by launching higher dosage options. On the former, he recognizes that patients in the US – even those with insurance – face significant barriers to accessing medications, like prior authorizations. These obstacles had led to a rise of other entities like compounders. Novo Nordisk will thus continue to focus on cash channels in the US, “meeting the patients where they are.”
- When asked about the Most-Favored-Nation deal, Mr. Doustdar said that Novo Nordisk and the government negotiated carefully to determine the “sweet spot” at which volume increase balances the lower price. While he is confident about the future outlook, he said that there will be “short-term pain” because volume will not double immediately.
- On the Wegovy pill, Mr. Doustdar emphasized that it delivers ~15% weight loss, equivalent to injectable Wegovy, as well as cardiovascular benefits – indicating a promising label. He also believes that the oral formulation will broaden the market to a “large extent.” People who may be needle-aversive, cannot refrigerate Wegovy pens (e.g., due to frequent traveling), or are concerned about “escalating” treatments from lifestyle modification to injectable medication may contribute to the uptake. When asked about the food restriction, Mr. Doustdar said that approximately 2.4 million people have been prescribed with Rybelsus, and there was no evidence in the market that the food restriction hinders the uptake. He also added that we do not know what orforglipron’s label will look like. According to clinical trial protocols, participants taking statins were directed to wait two to four hours before taking orforglipron, for instance. On this comment, Lilly’s CEO Mr. David Ricks said in his symposium that the protocol was largely due to the timing of clinical development – Lilly had simply not conducted drug interaction studies with statins when initiating the clinical trial.
- On injectable GLP-1 RAs, Mr. Doustdar outlined Novo Nordisk’s plan to reframe the injectable obesity market, emphasizing that the company’s priority is to “change the current market perception” by demonstrating that semaglutide can reliably deliver >20% weight loss when appropriately dosed. He noted that the upcoming 7.2 mg semaglutide dose is designed to match or exceed the efficacy of newer competitors and argued that the current narrative – treating Lilly’s higher‑dose agents as inherently “next‑generation” and semaglutide as an older, less potent molecule – is fundamentally imbalanced. Mr. Doustdar stressed that this perception is driven almost entirely by dose, not by underlying biology, and that once the company brings the 7.2 mg dose to market, the comparison will become more balanced as semaglutide demonstrates equivalent 20% weight loss in the phase 3b STEP UP trial (n=1,407), along with its already‑proven cardiovascular, liver, and renal benefits, which competitors have not yet matched in outcomes data or labeling. He framed this as a necessary correction to a market that has overemphasized weight loss percentages while undervaluing semaglutide’s broader clinical profile.
- On the clinical pipeline, Mr. Doustdar highlighted CagriSema (fixed-dose cagrilintide and semaglutide) and amycretin as important late-stage assets. Based on results from the REDEFINE 1 trial, where CagriSema demonstrated 20% weight loss, compared to a reduction of 11.5% with cagrilintide 2.4 mg, 14.9% with semaglutide 2.4 mg, and 3.0% with placebo, the company submitted an NDA to the FDA in December 2025. The company is preparing for late‑stage development and multiple indication expansions. He also emphasized the standalone potential of cagrilintide monotherapy, which is now in phase 3 and aimed at patients who prioritize tolerability over maximal weight loss. Meanwhile, amycretin, a dual GLP‑1/GIP agonist, is advancing toward phase 3 based on positive phase 2 results and represents a key component of Novo Nordisk’s strategy to deliver both higher efficacy and improved GI tolerability.
- On M&A, Novo Nordisk’s acquisition of Akero was framed as a strategic extension of the company’s obesity‑anchored pipeline, given that ~80% of MASLD/MASH patients also have obesity. He emphasized that while semaglutide performs well in F2 and F3 fibrosis, Akero’s FGF21 program could address patients who no longer benefit from GLP‑1 RA therapy and currently face liver transplant as their only option. Mr. Doustdar described the deal as a way to pair Novo Nordisk’s metabolic platform with a complementary mechanism to serve a broader segment of MASLD/ MASH patients.
3. Teva Pharmaceuticals: Teva to shift from generics firm to global biopharmaceutical company
CEO Mr. Richard Francis highlighted Teva’s “Pivot to Growth” strategy and the company’s long-term vision to open the second day of JPM. Mr. Francis shared that the strategy launched three years ago with an aim to move Teva from a global generics company into a biopharmaceutical company, following years of consecutive revenue declines.
- The “Pivot to Growth” strategy is built on four pillars: (i) delivering on already established pharmaceutical growth engines; (ii) improving innovation and its late-stage pipeline; (iii) creating a sustainable “generics powerhouse”; and (iv) disciplined capital allocation to the highest-return assets. He elaborated that the strategy would take place over three distinct phases:
- A return to growth. Evident in 11 consecutive quarters of growth since early 2023;
- Acceleration of growth. The company’s current strategic phase which focuses on rapidly growing innovative medicines revenue and leveraging its existing pipeline; and
- Maintaining growth. Management shared its ultimate goal of a 20-year plan to sustain a “world-leading” biopharmaceutical company with durable growth and improving returns.
- Mr. Francis emphasized that the company’s financials “prove” its portfolio transformation. Teva has moved from quarters of consistently declining revenue to consistently growing revenue, largely driven by its innovative business. Teva’s innovative business, Mr. Francis continued, has roughly doubled every two years. Moreover, Teva “broadly speaking” aims to keep doubling its innovative revenue in the future – targeting over $10 billion in peak sales from its portfolio.
- Mr. Francis deliberately waited until later in his presentation to discuss Teva’s generics business, framing the delay as evidence of how far Teva has shifted its business towards innovation. Teva currently has 10 biosimilars already on the market, with six additional biosimilar launches expected before 2027. Mr. Francis shared that the company’s goal is to build a portfolio of roughly 20-30 biosimilars globally, using active partnership deals to accelerate entry into separate, key molecules. Notably, biosimilars (highly similar copies of brand-name drugs) were framed by management as a higher-value, more complex segment of the generics (chemically identical copies of brand-name drugs) business that more closely aligns with Teva’s “complex generics” and biopharma capabilities.
- Teva’s generic of Novo Nordisk’s Saxenda (liraglutide) for obesity was not explicitly mentioned during prepared remarks or the Q&A. As background, Teva received FDA approval and subsequently launched its generic version of Saxenda for obesity in August 2025, which followed the company’s 2024 approval of Novo Nordisk’s Victoza (liraglutide) generic for T2D. Teva’s generic GLP-1 Saxenda is now indicated for weight loss in: (i) adults with obesity with at least one weight‑related comorbidity; and (ii) adolescents aged 12–17 years who weigh over 60 kg (~132 lbs). The approval marked Teva’s fifth first-to-market entry of 2025, consistent with its Pivot to Growth strategy.
4. AstraZeneca: Cardiometabolic focus for 2030 and beyond led by aldosterone synthase inhibitor baxdrostat, PCSK-9 laroprovstat, and GLP-1 RAs in development
Dr. Aradhana Sarin (CFO) presented AZ’s 2025 broad-scale results and outlook for the decade to come, with a focus on cardiometabolic health second only to oncology. Since the company’s FY 2024 report, AZ has presented 16 positive phase 3 trial readouts with five key focus areas in therapeutics: oncology, cardiovascular, renal & metabolism (CVRM), respiratory & immunology, vaccines & immune therapies, and rare disease. Dr. Sarin discussed the company’s goal to achieve $80 billion in total revenue by 2030 with sustained growth for 2030 and beyond. She said that the Inflation Reduction Act and the loss of exclusivity of Farxiga (dapagliflozin) and other drugs have continued to lower revenue, which reached $54.1 billion in 2024, yet has been offset by growth in the company’s existing portfolio and the upcoming launch of key NMEs. Among other therapies, she highlighted baxdrostat (a selective aldosterone synthase inhibitor for hypertension and primary aldosteronism), Farxiga fixed dose combinations, and laroprovstat (a PCSK-9 inhibitor) as key therapies in development that will propel AZ’s growth in the remainder of this decade. Beyond 2030, she discussed weight management and CV risk factors, cell therapy and T-cell engagers, gene therapy, next-generation IO biospecifics, and antibody-drug conjugates and radioconjugates as areas of focus for the future. AZ hopes to play a role in addressing sustained cardiometabolic disease burden worldwide. Dr. Sarin also touched on the company’s specific approaches to AI, including an AI Development Agent for drug synthesis and quantitative continuous scoring to identify patients most likely to respond to treatment.
- Positive baxdrostat trial results were highlighted as helping drive AZ’s momentum across a diverse pipeline. In September 2025, results from the phase 3 BaxHTN trial for uncontrolled hypertension were announced at ESC 2025 and simultaneously published in NEJM (n=796). At 12 weeks, participants receiving baxdrostat 2 mg achieved a mean reduction of 15.7 mmHg, while those on 1 mg saw a 14.5 mmHg reduction, compared with a 5.7 mmHg reduction in those receiving placebo. These results correspond to a placebo-adjusted reduction of 9.8 mmHg with 2 mg baxdrostat and 8.7 mmHg with baxdrostat 1 mg. Results were consistent across both the uncontrolled and treatment‑resistant hypertension subgroups. Dr. Sarin said that phase 3 trial results from 2025 including BaxHTN and the phase 3 Bax24 trial for resistant hypertension present a $10 billion dollar opportunity for AZ.
- Baxdrostat is currently under FDA Priority Review. As announced in December 2025, the Prescription Drug User Fee Act (PDUFA) date for the therapy is anticipated in 2Q26. If approved, the therapy could address a major need in cardiovascular care in patients with limited treatment options. Dr. Sarin said that, upon approval, AZ expects the therapy’s adoption to proceed from specialists to primary care.
- Addressing weight management and cardiovascular risk factors will form a key part of AZ’s long-term strategy. Dr. Sarin said that AZ hopes to establish a role and eventually lead in a new weight management paradigm and in cardiovascular risk factors. She also said that AZ is uniquely positioned to deliver novel small molecule combinations and committed to “accelerating programs into late-stage development.” Dr. Sarin then highlighted three phase 3 trials ongoing for laprovstat as well as phase 2 trials of:
- Elecoglipron (a small-molecule GLP-1 RA) with readout expected in 1H26;
- AZD6234 (an amylin receptor agonist) with readout expected in 1H26; and
- The combination of AZD9550 (a dual glucagon/GLP-1 RA) and AZD6234, with readout expected in 2H26.
- Phase 3 data for laroprovstat, an oral PCSK-9 inhibitor, are expected in 2027. Dr. Sarin said that laroprovstat holds great potential because it is a once-daily, small molecule therapy with no fasting or food restrictions. In phase 2b trials, the therapy demonstrated an over 50% reduction in LDL cholesterol on top of standard-of-care statins. In 2Q25, AZ initiated three phase 3 clinical trials for AZD0780 (laroprovstat), which are all actively recruiting:
- AZURE-LDL (n=2,800) will evaluate LDL-C reduction in patients with dyslipidemia and a history of clinical ASCVD or who are at risk of a first ASCVD event.
- AZURE-HeFH (n=405) will evaluate LDL-C reduction in patients with heterozygous familial hypercholesterolemia.
- AZURE-Outcomes (n=15,100) will evaluate the time to first event of any component of MACE-Plus, a composite endpoint that includes death, myocardial infarction, stroke, revascularization, heart failure, and thromboembolic events. Patients included will either have dyslipidemia and established ASCVD or will be at high risk of a first ASCVD event.
5. Kailera Therapeutics: CEO Mr. Ron Renaud highlights diversified GLP-1 RA pipeline for obesity treatment
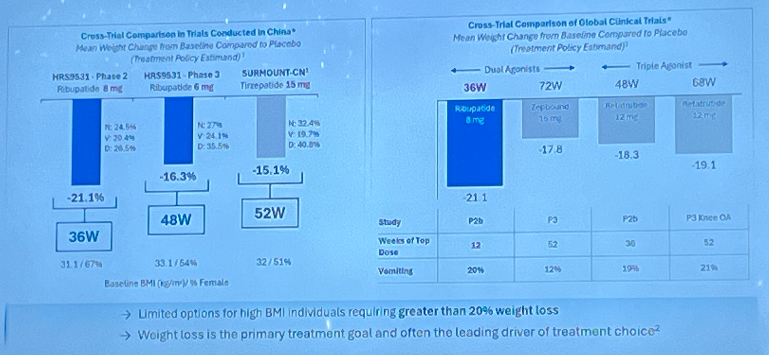
In a morning symposium, CEO Mr. Ron Renaud highlighted Kailera Therapeutics’ obesity pipeline and its broader business strategies.As background, Kailera is a California- and Massachusetts-based clinical-stage company launched in October 2024 with $400 million Series A financing round. It develops an obesity pipeline acquired in May 2024 from Jiangsu Hengrui Pharmaceuticals. Kailera has exclusive global development and commercialization rights outside of Greater China for four metabolic disease assets, as Mr. Renaud detailed in his presentation. He began by highlighting that over half of US adults with obesity are projected to have a BMI ≥35 kg/m2 by 2030. Moreover, 68% of participants in SURMOUNT-1 with baseline BMI ≥35 kg/m2 did not reach BMI <30 kg/m2, indicating significant unmet needs in people with severe obesity.
- Ribupatide (KAI-9531) is an injectable dual GLP-1/GIP RA designed to be more efficacious than tirzepatide, by making GLP-1 agonism three times more potent and GIP agonism half as potent as tirzepatide. KAI-9531 also has a half-life of seven days, compared to five days for tirzepatide. In a phase 2 trial (n=61), ribupatide conferred placebo-adjusted weight loss of 21.1% at Week 36 with a higher dose of 8 mg. In a phase 3 trial (n=567), KAI-9531 6 mg previously achieved up to 17.5% mean weight loss without a plateau at Week 48, with 44% of participants achieving ≥20% weight loss.
- While cautious to make cross-trial comparisons, he noted that ribupatide conferred greater weight loss than tirzepatide and retatrutide at shorter study durations. See figure below.
- Looking forward, ribupatide is evaluated in three ongoing phase 3 KaiNETIC trials (n=1,600, 1,700, and 1,200) for doses up to 10 mg for over 76 weeks. One trial includes participants with T2D, while another includes those with high BMI ≥35 kg/m2. Kailera announced today that the first participants randomized in the phase 3 KaiNETIC program have been dosed.
- Kailera also has other GLP-1 RA-based candidates:
- Oral ribupatide is progressing into phase 2 in 2026. In a phase 1 trial, the candidate conferred 5.4% weight loss at Week 4, and 6.3% experienced vomiting, suggesting potentially favorable tolerability profile.
- Oral KAI-7535, a once-daily oral small molecule GLP-1 RA, will progress to phase 2 in 2026, as well. In primary and post-hoc analyses of a phase 2 trial, KAI-7535 led to 9.5-15% weight loss with low liver risk.
- KAI-4729, a once-weekly GLP-1/GIP/glucagon triple agonist, is intended to deliver strong weight loss and improved liver fat reduction. In preclinical studies, KAI-4729 showed the potential to confer greater weight loss than retatrutide. This candidate will progress to phase 1 in 2026.
- During Q&A, when asked about the impact of semaglutide’s loss of exclusivity in the early 2030s, when these candidates are expected to launch, Mr. Renaud shared confidence that its focus on people with severe obesity (BMI ≥35 kg/m2) and robust clinical data can help Kailera secure reimbursement. To another question about pipeline diversity, Mr. Renaud said that additional mechanisms of action will be needed in parallel or as an add-on to GLP-1 RA-based therapies. However, he believes that GLP-1 RAs will remain backbone treatments, and Kailera’s candidates have a strong potential to be differentiated assets as GLP-1 RA therapies.
6. Bayer: Kerendia (finerenone) demonstrates blockbuster potential for CKD and heart failure; pricing pressures with Eylea (aflibercept)
- Mr. Stefan Oelrich (Bayer President of Pharmaceuticals Division) shared updates on Bayer’s therapies, including: (i) non-steroidal MRA Kerendia (finerenone); and (ii) anti-VEGF Eylea (aflibercept). See the webcast and presentation slides here.
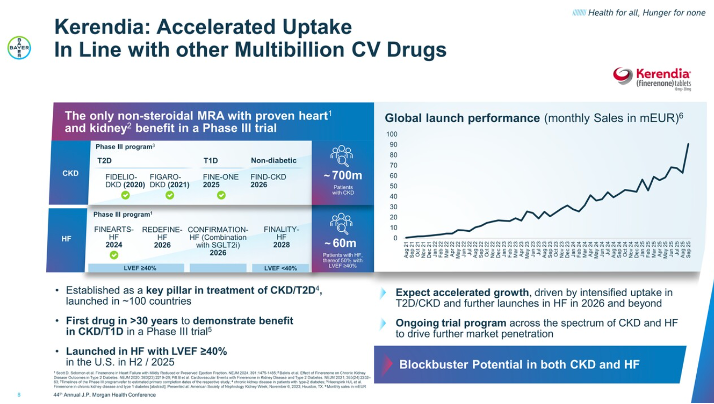
- Kerendia demonstrates blockbuster potential for CKD and heart failure. Mr. Oelrich called Kerendia the next blockbuster drug and included it as one of the key growth drivers of 2025, especially as it has demonstrated accelerated growth in T2D, CKD, and heart failure. Bayer initially pursued Kerendia for the treatment of CKD and T2D, establishing it as a key pillar across ~100 countries. Then, Bayer progressed Kerendia for a heart failure indication to encompass a broader population. At ESC 2024, results of the phase 3 FINEARTS-HF (n=6,001) trial showed that Kerendia demonstrated a 16% relative risk reduction of the primary composite outcome of total heart failure outcomes and cardiovascular death over 32 months among patients with HFmrEF or HFpEF. Following these groundbreaking results, Kerendia received FDA approval for the treatment of heart failure in July 2025. With indications for CKD and heart failure, Mr. Oelrich emphasized Kerendia’s efficacy, expecting accelerated growth driven by increased uptake and further launches in 2026 and beyond.
- Several phase 3 trial results are expected in CKD and heart failure. In 2026 alone, the following trials are expected to complete: (i) FIND-CKD trial (n=1,584) of Kerendia in adults with non-diabetic CKD; (ii) REDEFINE-HF trial (n=5,200) of Kerendia in hospitalized heart failure patients; and (iii) CONFIRMATION-HF trial (n=1,500) of the combination of Kerendia and SGLT-2 inhibitor in hospitalized patients with heart failure. Mr. Oelrich said these ongoing trials across the spectrum of CKD and heart failure are expected to drive further market penetration.
- Kerendia’s potential for T1D. At ASN 2025, Bayer announced results from the phase 3 FINE-ONE trial (n=241) of Kerendia in people with T1D and CKD. Kerendia significantly reduced UACR by 25% compared to placebo at six months. Echoing Mr. Bill Anderson’s (Bayer CEO) remarks during Bayer’s 3Q25 call, Mr. Oelrich emphasized that Kerendia is the first therapy in 30 years to demonstrate positive results in addressing CKD in this population.
- Comments on Kerendia’s slow uptake. Bayer has previously predicted a slow uptake of Kerendia, but Mr. Oelrich expressed confidence that the uptake would increase at a faster rate. In fact, Kerendia has shown accelerated uptake in line with “other multibillion-dollar cardiovascular drugs.” Mr. Oelrich said this area has limited options with high unmet needs, and therefore, positioned Kerendia as a promising treatment. He compared Kerendia to statins when they first emerged in the field to lower cholesterol levels.
- Eylea sales remain stable but face increasing pricing pressures. While Mr. Oelrich strongly emphasized Eylea’s leadership in the retinal market and positioned it as the number one anti-VEGF treatment at JPM 2025, he spoke minimally about this product in today’s meeting. As background, Bayer exclusively markets Eylea outside the US, while Regeneron is responsible for US sales. Mr. Oelrich said the conversion from Eylea to Eylea HD (aflibercept 8mg), the only drug for extended treatment intervals (up to five months for nAMD and DME), is “going well.” He also said Eylea sales are “stable for now,” but commented that the company continues facing pricing pressures and expects to see more challenges with emerging biosimilars in the field.
7. Ionis Pharmaceuticals: Tryngolza gains traction in treatment of FCS ahead of broader launch; pelacarsen for Lp(a) risk reduction on track for launch in 2027
- CEO Dr. Brett Monia highlighted Ionis’s cardiometabolic franchise, emphasizing the commercial momentum of Tryngolza (olezarsen) for the treatment of familial chylomicronemia syndrome (FCS), and the potential of pelacarsen to reshape Lp(a)-driven cardiovascular risk. Tryngolza was approved in December 2024 in the US and September 2025 in the EU for FCS. It generated more than $100 million in US net revenue in its first year, with Dr. Monia describing “overwhelmingly positive” patient feedback and strong physician reauthorization rates. Ionis is preparing a broader launch in severe hypertriglyceridemia (sHTG), for which phase 3 CORE and CORE-2 trial data showed 72% fasting triglyceride reduction, 86% of patients below the pancreatitis risk threshold, and an 85% reduction in acute pancreatitis events. Dr. Monia confirmed that the supplemental NDA was submitted in December and that Ionis has requested priority review. If granted, approval could come as early as July 2026.
- On Lp(a), Dr. Monia reiterated enthusiasm for pelacarsen, developed in partnership with Novartis, and positioned it as a first-in-class RNA-targeted therapy targeting genetically elevated Lp(a). Previously, phase 2 data showed >95% reductions in Lp(a) levels. The phase 3 HORIZON outcomes trial (n=8,323) is expected to read out in 1H26, with Dr. Monia anticipating a 2027 launch pending positive results. Dr. Monia noted that the trial is powered to detect a 20% relative risk reduction overall and 25% in patients with very high Lp(a), but emphasized that given the lack of approved therapies, a 10-15% reduction in cardiovascular events would be considered a meaningful win and may be sufficient for Novartis to pursue approval.
Diabetes Technology
8. Insulet: President and CEO Ms. Ashley McEvoy highlights growth opportunity across US T1D, US T2D, and OUS T1D; robust innovation pipeline through 2028
Following a successful Investor Day in November 2025, Insulet CEO Ms. Ashley McEvoy emphasized Insulet’s strong business model and three-year innovation plan. She highlighted several advantages that underscore Insulet’s position in the AID competitive landscape that have enabled Insulet to drive ~66% of total AID market growth from 2020-2025, with share expanding from <30% in 2020 to ~50% in 2025. Revenue has grown at a ~25% CAGR since 2021, driven by strong new patient starts, and Insulet became cash-flow positive in 2023 and has accelerated since, reinforcing its ability to fund growth and innovation. While additional entrants to the ecosystem may emerge, Ms. McEvoy said that Omnipod 5 remains “in a class by itself.”
- Ms. McEvoy outlined a coordinated strategy across US T1D, OUS T1D, and US T2D to drive the next leg of growth, highlighting the under-penetration seen across all three populations.
- US T1D ($9B+ total addressable market): AID penetration is ~40%, roughly 30 percentage points below estimated CGM penetration (~70%). Insulet aims to increase penetration to above 50% by 2028 by: (i) driving demand generation in line with evolving clinical guidelines to move more patients from MDI to AID; (ii) strengthening commercial execution to add new prescribers; and (iii) delivering excellent user experience through continued innovation.
- OUS T1D ($10B+ total addressable market): AID penetration remains only ~25% of an estimated four million potential patients, ~40 percentage points below CGM penetration (~65%). Roughly 80% of this opportunity in Insulet’s geographies resides in Europe, with the remainder in Canada, Australia, and the Middle East. Insulet targets 30-35% penetration by 2028 and plans to launch Omnipod 5 in six additional markets in 2026 (Spain and five Middle Eastern countries), bringing the total number of Omnipod 5 markets to 20 by year-end. Ms. McEvoy also reiterated Insulet’s plans to accelerate growth in existing OUS geographies.
- US T2D basal-bolus ($12B+ total addressable market): AID penetration is estimated to be <5%, more than 50 percentage points below CGM penetration (~55%). Insulet aims to more than double penetration to 10-15% by 2028 by positioning Omnipod 5 as standard of care. Specifically, Ms. McEvoy cited the 2026 ADA Standards of Care, which now identify AID as preferred therapy for people with T2D who are currently using MDI, insulin pumps, or sensor-augmented pump therapy. Insulet received FDA clearance for Omnipod 5 use by adults with T2D in August 2024. Prior to the clearance, over half of the company’s direct-to-consumer (DTC) leads had been individuals with T2D, and over 25% of new US user starts in the quarter of the clearance (3Q24) had T2D – this increased to 35% just one year later, in 3Q25. Since then, Omnipod 5 has been joined by Tandem Control-IQ+ and MiniMed 780G with US T2D indications.
- Ms. McEvoy also highlighted Insulet’s innovation pipeline, with more than $1 billion planned investment in technology over the next three years. This includes the hardware and software innovation noted below, as well as the STRIVE and EVOLUTION clinical studies and development of broader real-world evidence with Omnipod 5. She noted that diabetes distress remains widespread and most insulin users do not currently benefit from AID, underscoring a significant gap in care that Insulet hopes to address through differentiated technologies.
- Insulet plans to launch several highly requested updates in 2026, including: (i) a 100 mg/dL glucose target (in 1H26) alongside increased time in automated mode and improved algorithm responsiveness; (ii) integration with all major CGM sensors; and (iii) the launch of Omnipod Discover to streamline onboarding and office workflows. Insulet expects the algorithm improvements to improve Omnipod 5’s competitive strength among patients and providers seeking even better glycemic management, and the launch of Omnipod Discover to improve action on the insights CGM and AID unlocks, enabling greater optimization of care plans.
- Insulet plans to launch Omnipod 6 in 2027. Omnipod 6 is Insulet’s next-generation AID system, featuring improved connectivity and more personalized automation. The STRIVE trial is now complete, with results to be presented at ADA 2026. Insulet is also planning for a 510(k) submission of Omnipod 6 in 2026. Ms. McEvoy explained that Omnipod 6 will be an over-the-air-updatable pod, enabling a shift from multiple sensor-specific stock keeping units (SKUs) to one master SKU compatible with all sensors. This will enable direct integration updates to Pods already manufactured, eliminating channel stocking dynamics and will allow users to receive innovations six to nine months faster than they do today, as well as simplifying manufacturing and prescribing practices.
- Insulet plans to launch its fully closed-loop (FCL) AID system for people with T2D in the US in 2028.With ~70% of T2D patients managed in primary care settings and ~75% of insulin-treated patients not meeting recommended glycemic targets, the FCL system is designed to enable broader PCP adoption of AID and, over time, expansion into the larger basal insulin market. Ms. McEvoy emphasized the system as designed for self-start – as it is “ready out-of-the-box” – and for ease of prescription by providers, with no settings to start. She described this as a “game-changing” opportunity to lower the burden of managing T2D.
- Beyond 2028, Insulet plans to bring FCL technology to people with T1D.
- Ms. McEvoy briefly addressed manufacturing and commercial strength, reiterating that Insulet is constructing another manufacturing facility (in Costa Rica, scheduled to come on-line in 2029 – we hope it will have pods that last longer and hold much more insulin in their reservoirs) and continues to produce “tens of millions” of pods annually at scale. Insulet is also working to construct additional lines in Malaysia and improve automation in Acton, Massachusetts.
- She also noted that the company has the highest AID brand awareness among MDI users, and that ~70% of patients who request a specific AID system ask for Omnipod – leading her to characterize Insulet as a “gateway” to the AID ecosystem. Yep, yep it sure is, particularly given how easy it is to use! We loved hearing that Insulet now calls on an even higher number of prescribers, and what now sounds like well over 20,000 (up ~25% in 3Q25). Boy, do we hope those prescribers look at all their patients, particularly those with T1D who aren’t yet on pumps – MDI is so much more challenging to manage than Omnipod 5 or any other continuous insulin delivery.
- Looking ahead, Insulet projects ~20% revenue CAGR in constant currency between 2025-2028, largely driven by increasing penetration of its addressable markets across T1D and T2D, US and international. Insulet also expects approximately 100 basis points annual operating margin expansion between 2025-2028 with “modest” gross margin improvement, driven by its investment in innovation and optimized selling, general, and administrative expenses.
- Finally, brand new CFO Ms. Flavia Pease addressed investor questions following the company’s 3Q25earnings call, saying that Insulet will continue to provide guidance it has a high degree of confidence in achieving and that reflects a balanced outlook. She emphasized that recent concerns about deceleration from peers reflect noise rather than Insulet’s business fundamentals and encouraged investors to focus on the underlying strength and durability of the business.
9. Verily: Progress on Verily Pre for clinical research facilitation and Verily Me for telehealth
- CEO Mr. Stephen Gillett shared updates on Verily’s recent progress and strategic direction. Verily, an approximately 10-year-old subsidiary of Alphabet, operates with physicians licensed to practice medicine in all 50 states. Although the company is currently in a quiet period, we appreciated Mr. Gillett’s updates on the progress the company has made in recent months and focus for 2026.
- Mr. Gillett overviewed Verily Me, the company’s consumer-facing telehealth platform that entered a beta launch in October 2025. Verily Me is a mobile app that prompts users to submit a photo of themselves and their driver’s license, after which the platform retrieves their medical records and routes them to a Verily clinician, who then offers personal recommendations on a health plan.
- He also discussed advancements in Verily Pre, the company’s data platform for healthcare research. Verily has established relationships with organizations like the CDC, Vanderbilt Health, and the NIH to host datasets that researchers must access through Verily (the NIH’s All of Us Research Program currently supports approximately 20,000 global researchers). Pre ingests diverse data types – including claims, genomics, and EHRs – and converts them into FHIR-based, health-grade data designed to be “AI-ready” for companies’ specific use cases. Pre enables researchers to significantly increase the speed at which research can be conducted, including 10x faster model training and 30x faster whole-genome analysis. Mr. Gillett cited a partnership with the University of Colorado using Pre to study acute myeloid leukemia, which achieved 95% accuracy and reduced researcher time by 97% – replicating and validating findings in a fraction of the usual time. Furthermore, Verily has entered into a partnership with Nvidia, which Mr. Gillett described as a “powerful ecosystem” for clinical research.
- Mr. Gillett said that Verily will launch “another nice set of updates” in 2026, including plans to publish research that it’s doing on its platforms. In 2026, Verily plans to: (i) expand tools for clinical researchers and for drug development with Verily Pre; (ii) launch new agents on Verily Pre and the Verily Me app; and (iii) drive additional commercial opportunities and partnerships.
Diabetes Big Picture
10. CMS comes to SF: Dr. Mehmet Oz and CMS leadership discuss GLP-1 RAs, long-term health, MFN, and MAHA
- The second keynote of JPM 2026 featured an impassioned panel discussion from Centers for Medicare & Medicaid Services (CMS) leaders. Dr. Mehmet Oz (CMS Administrator), Mr. Daniel Brillman (Deputy Administrator and Director), Ms. Stephanie Carlton (Deputy Administrator & Chief of Staff), Mr. Chris Klomp (Deputy Administrator & Director), and Ms. Amy Gleason (Strategic Advisor) discussed their approaches to improving long-term US health. Moderator Mr. Dan Mendelson (CEO, Morgan Health) asked insightful questions into the Make America Healthy Again (MAHA) movement, Medicare and Medicaid spending, and the specific role of GLP-1 RAs in America’s future. In his opening and closing messages, Dr. Oz even characterized the panel as a “recruiting mission” for healthcare industry leaders to join CMS as it seeks institutional change, saying that the panelists were trying to convince attendees to leave their current roles to help fix a system that “all would agree is broken, but no one would ever leave in favor of care anywhere else.”
- GLP-1 RAs are a “wise investment” into long-term health that should be approached in a responsible way. Mr. Klomp said that GLP-1 RAs are the most popular drug class in the US, repeatedly emphasizing the cardiometabolic benefits of the therapies. He said that CMS’ recent decision under Most-Favored-Nation pricing to cover the therapeutic class for obesity, not solely for diabetes, is an effort to capitalize on cardiovascular disease prevention and prediabetes management. He said that CMS is particularly focused on improving overall health in the nation to reduce health system costs. With improved health comes improved productivity, he said, which will further stimulate the US economy.
- Technology and AI may offer opportunities to change healthcare infrastructure and revolutionize rural care. Ms. Gleason humorously described her journey from CES 2026, where she also represented CMS, to San Francisco, which included laundry-folding robots in the CES exhibit hall and self-driving Waymos. She contrasted this to the average experience of healthcare in the US involving clipboards and fax machines instead of digitization and automation. Ms. Gleason said that CMS hopes to empower patients to take better control of their health and to think of this as seeking a better consumer experience in the healthcare industry. In July 2025, CMS launched the Health Technology Ecosystem, which aims to regulate digital health records and make them accessible to patients and providers via a standardized QR code. Dr. Oz said that patients are smart and that the government and healthcare providers should meaningfully engage with them using technological advancements. He urged the audience to think, “What do we need to do together to fix your problem?”
- Mr. Brillman said that now is the time for rural communities to shine. He said that CMS is currently making large investments into rural healthcare with the help of individual states to fill gaps in rural care. He called for a data-first approach to rural medicine and said that seeking advice from industry experts, such as those in the room, will be essential for achieving these goals. As an example, Ms. Carlton discussed a virtual reality headset initiative that has been implemented in Nebraska to help train providers where in-person training is not as accessible.
--by Kayla Mathieu, Elizabeth Rose, Jeremy Alkire, Nour Khachemoune, Kat Moon, Esther Min, Monica Oxenreiter, and Kelly Close