Close Concerns’ Reflections 2025 + 2026 –
Executive Highlights
- Innovation in diabetes technology accelerated in 2025, driven by landmark regulatory approvals and major product launches in continuous glucose monitoring (CGM) and automated insulin delivery (AID). This momentum translated into strong market growth: the insulin pump market reached record revenue of $1.4 billion in 3Q25 (+13% YOY), and the CGM market experienced even greater annual growth (+24% YOY), achieved a record $3.5 billion in 3Q25. Industry efforts are increasingly focused on expanding access — particularly for people with T2D.
- Three AID systems are now cleared for use in adults with T2D in the US. Following the August 2024 clearance of Omnipod 5, Tandem received approval for its updated Control-IQ+ algorithm in February 2025, and Medtronic for MiniMed 780G in September 2025. All three companies are actively driving market adoption. Updates to the ADA 2026 Standards of Care designating AID as the “preferred insulin delivery system” for all people with T1D and for adults and children with T2D using MDI, pumps, or sensor-augmented therapy could further accelerate uptake. Medtronic also received CE-Mark approval for MiniMed 780G in T2D in July 2025.
- CGM innovation progressed meaningfully in 2025. Medtronic expanded its sensor portfolio with two new sensors interoperable with MiniMed 780G in the US: Simplera Sync and Abbott-developed Instinct (Simplera Sync has been available in Europe since 2024; Instinct remains under CE-Mark review). Dexcom launched its G7 15 Day sensor for adults, extending wear time by 50% versus the original G7. Globally, we estimate approximately 11 million people were using CGM by the end of 3Q25, up 10% from late 2024.
- Interoperability significantly expanded with several launches of new CGM integrations. Insulet launched FreeStyle Libre 2 Plus integration across multiple markets, including the UK, Netherlands, US, Italy, Belgium, Switzerland, the Nordic countries, and Australia, and expanded Omnipod 5 integration with Dexcom G7 in at least a half dozen international markets. In the US, Omnipod 5 and Beta Bionics’ iLet integrated with Dexcom G7 15 Day at its December 2025 launch. Tandem also introduced t:slim X2 integration with FreeStyle Libre 3 Plus, while Sequel twiist launched in the US with Libre 3 Plus integration. twiist’s additional integration with Eversense 365 marked the sensor’s first entry into the AID market. Looking ahead, upcoming integrations include Omnipod 5 with FreeStyle Libre 3 Plus (1H26), Tandem Mobi with Libre 3 Plus, and Control-IQ compatibility with Dexcom G7 15 Day.
- In therapy, incretin therapies continued to dominate headlines throughout the year, with new approvals, indications, trial results, and treatment protocols. To name a few, Novo Nordisk’s semaglutide secured new approvals across four major indications: (i) T2D and chronic kidney disease (CKD), (ii) peripheral artery disease (PAD); (iii) MASH; and (iv) oral semaglutide for weight management and cardiovascular (CV) risk reduction. While not approved yet for CV risk reduction, Lilly’s Mounjaro (tirzepatide) demonstrated a nonsignificant 8% reduction in major adverse cardiovascular events (MACE) and significant 16% reduction in all-cause mortality compared to dulaglutide in the landmark phase 3 SURPASS-CVOT (n=13,299). Emerging treatments include dual incretin therapies like CagriSema, oral formulations like orforglipron, and amylin agonists.
- In obesity care, importantly, the ADA Standards of Care 2026 newly added a recommendation that stresses the importance of personal dose titration to balance efficacy, health benefits, and tolerability, as well as a recommendation for GLP-1 RA use in people with T1D.
- In T1D, therapeutic landscape for disease-modifying and cell replacement therapies for T1D continued to evolve,with progress spanning stem cell-derived islets, hypoimmune platforms, immunosuppressants, and disease-modifying therapies. Vertex continues to advance zimislecel program in the phase 1/2/3 trial, while Sana Biotechnology, Adocia, and others developed early clinical- and preclinical-stage candidates. For disease-modifying therapies, teplizumab received the FDA’s new Commissioner’s National Priority Voucher for a potential indication of preserving beta cell function in people with recent onset stage 3 T1D. With the expedited review process, the regulatory decision is now expected in 1H26.
- On complications, significant advancements were made to expand therapeutic options for metabolic dysfunction-associated steatohepatitis (MASH), chronic kidney disease (CKD), and peripheral diseases.
- On screening and monitoring, the field has consistently emphasized the importance of T1D autoantibody screening through efforts like Breakthrough T1D’s submission to the US Preventive Services Task Force (USPSTF) in May 2025, publication of clinical guidelines on screening and monitoring, and education by Sanofi, Beyond Type 1, and more.
- In big picture, significant changes were made on drug pricing, safety of compounded products, and leadership. Continuing last year’s momentum toward lower drug prices in the US, the government reached negotiations with pharmaceutical companies. Under the Medicare Drug Price Negotiation Program (MDPNP), Novo Nordisk’s three semaglutide products – Ozempic, Rybelsus, and Wegovy – will face a 71% cut to their list prices, and will cost $274 per prescription in the US in January 2027, down from ~$950 per month in 2024. We will be very interested to see how this price reduction impacts volume and it’s so interesting that while manufacturing issues were dominant not so long ago, they no longer appear to be a major issue at either Novo Nordisk or Lilly. It will be interesting, of course, to see how Novo Nordisk’s oral Wegovy, approved earlier this week, will be priced, when it comes on the market in early January. Meanwhile, Lilly’s DPP-4 inhibitor Tradjenta will be $78 per month, while Merck’s DPP-4 inhibitor/biguanide Janumet and Janumet XD will cost $80 per month. These are major bargains and we would love to see either company approach FDA with ideas for new indications of pre-T2D prevention.
- Under the Most-Favored-Nation (MFN) policy, some major pharmaceutical companies agreed with the US government to offer GLP-1 RAs at $245 per month through Medicaid and Medicaid. The government will launch TrumpRx, the government’s direct-to-consumer platform, in January 2026, and will sell: (i) Wegovy at $350 per month; (ii) Wegovy pill at $150 per month; and (iii) Zepbound and orforglipron (upon approval) at $346 per month. We look forward to watching execution on this.
- On leadership, there were significant changes to diabetes technology and pharmaceutical companies. In diabetes technology, two major care businesses announced plans to separate from their parent organizations: MiniMed is spinning out from Medtronic, while Ypsomed’s mylife Diabetes Care AG was sold to TecMed. Novo Nordisk underwent sweeping leadership transitions to the CEO and Board of Directors, as well as overall restructuring of the company, after several quarters of underperformance.
- On M&A, the fall of 2025 was a particularly dynamic period in the cardiometabolic field, as companies raced to the next-generation treatments for obesity and MASH. This includes Roche’s acquisition of 89bio (FGF21 analog pegozafermin in phase 3), Novo Nordisk’s of Akero Therapeutics (FGF21 efruxifermin in phase 3), and Pfizer’s purchase of Metsera (several early-stage GLP-1 RAs and amylin candidates).
Table of Contents
-
Diabetes Technology
- Key Questions for 2026
- What’s Coming in 2026?
-
Themes
- 1. CGM reaches ~11 million global users at end of 3Q25, powered by adoption in growing populations; regulatory clearances expand competitive landscape
- 2. AID uptake continues to grow with guidance on initiation at diagnosis and more systems available to the T2D population in the US and Europe
- 3. Closing the loop: Studies evaluating the safety and efficacy of FCL algorithms in T1D and T2D march on; FCL-like use grows in HCL users who don’t bolus
- 4. TITR, Time in Normoglycemia, Time in Happiness? Tighter glycemic management gains traction as debate on its name (and ideal range) emerges
- 5. Diabetes technology in pregnancy: Evolving global guidelines and the search for more data
- 6. Inpatient CGM use demonstrates positive impact on glycemia and re-hospitalization rates as accuracy shows mixed bag
- 7. The many faces of AI: Clinical applications, AI in research
- 8. New ways of continuous monitoring: CKM, range-based feedback, and early disease insight
- 9. Digital health funding stabilizes in 2025 as capital focuses on AI-driven and workflow-focused platforms
- 10. Data interoperability comes into focus as diabetes data continues to be incorporated into routine clinical workflows
- Top Ten Most Read Closer Look Reports in Therapy
- Most Unexpected News/Biggest Surprises
-
Diabetes Therapy
- Key Questions for 2026
- What’s Coming in 2026?
-
Themes
- 1. Incretin-based therapies: New indications and outcomes trial in the heart, kidneys, liver, and limbs
- 2. Expanding competitive landscape for oral GLP-1 RAs and multi-incretins for T2D
- 3. Toward the holy grail: Advances in cell replacement therapies for T1D
- 4. Momentum continues for disease-modifying therapies in T1D
- 5. Meeting the unmet needs in T1D: Finerenone, GLP-1 RAs, and SGLT inhibitors as adjunctive therapies to insulin
- 6. Once‑weekly insulin moves closer to market with robust phase 3 data
- 7. SGLT-2 inhibitors and finerenone as foundational therapies for T2D and comorbidities; new cohorts of interest expanding potential indications
- 8. MASH has a giant year, with semaglutide becoming the second approved option for the treatment in the US; liver health becomes the next frontier for cardiometabolic development
- 9. Beyond opioids and status quo: Emerging therapies for neuropathic pain and limb health
- 10. Regulatory approvals for diabetic macular edema and diabetic retinopathy improve therapeutic access; commercialization efforts of anti-VEGF biosimilars continue
- 11. Obesity treatment has a powerhouse year with lots of excitement for next: New approvals, readouts, and clinical frameworks for incretins, amylin, and beyond
- 12. Reframing T2D care: “Precision” therapies and hypercortisolism
- Top Ten Most Read Closer Look Reports in Therapy
- Most Unexpected News/Biggest Surprises
-
Big Picture
- Key Questions for 2026
-
Themes
- 1. Screening for T1D remains a key priority, with emphasis on education and awareness
- 2. Structural changes in pharmaceutical and tech giants: Spin-off of MiniMed and restructuring of Novo Nordisk indicative of broader industry shifts
- 3. Major M&As for MASH and obesity: The race towards the next-generation therapies
- 4. Inflation Reduction Act and Most-Favored-Nation policy: US government reaches price negotiations with pharmaceutical companies
- 5. Direct-to-consumer market expands amid continued compounding business and pricing pressure
- 6. One trial or two? A key regulatory question emerges at FDA after some riffing
- Top Five Most Read Closer Look Reports in Big Picture
- Most Unexpected News/Biggest Surprises
- Notable Interviews in 2025
- 2025 Resource Hubs for Scientific Conferences Attended by Close Concerns
- Literature Shared in 2025
Diabetes Technology
Key Questions for 2026
Continuous Glucose Monitoring
- What further clinical or real-world evidence is expected next from Abbott and how might upcoming data help define use cases for DGK and CKM?
- How will manufacturers differentiate in an increasingly competitive CGM landscape, as longer-wear sensors and novel form factors expand user choice?
- As CGM is increasing used earlier and earlier in disease progression, will there be formal guidance on using CGM as a diagnostic or risk-stratification tool for prediabetes and early-stage T1D?
- How do uptake trends look after a full year of OTC CGM release for Dexcom’s Stelo and Abbott’s Lingo?
- What other analytes are under consideration for analysis in multi-analyte sensors?
- On CKM and the anticipated DGK sensor from Abbott, what is the current baseline understanding of ketone physiology among people with diabetes and providers, particularly around what constitutes as “normal” or “elevated” ketone levels in daily management?
Insulin Delivery
- With three AID systems now formally indicated for T2D in the US (Tandem’s Control-IQ+, Medtronic’s MiniMed 780G, Insulet’s Omnipod 5) and CE-Mark expansion underway in Europe, how quickly will AID adoption accelerate in T2D now?
- As AID systems expand beyond T1D, which additional safety components will be prioritized for adoption?
- How will reimbursement frameworks evolve as AID systems move toward broader populations?
- What policies will be required to ensure equitable access to AID systems for individuals facing socioeconomic barriers across different health systems?
Digital Health
- What evidence will payers require to reimburse CGM-enabled digital health programs for people without insulin-treated diabetes or without diabetes?
- With Omada Health expanding into GLP-1 RA prescribing and Signos targeting lifestyle-driven alternatives, how will these digital platforms complement provider guidance to support individuals?
- How will the incorporation of AI-generated insights into digital health platforms reshape regulatory pathways and guidance in 2026?
What’s Coming in 2026?
Glucose Monitoring
Abbott
- Expected regulatory application for approval of dual glucose-ketone (DGK) sensor.
- Timeline of integrations of key insulin pump manufacturers with the anticipated DGK sensor.
- Potential impact of CMS policy change on uptake.
- Clinical impact of Libre-Epic integration.
- Expanded commercial launch of Lingo in countries outside of the UK and the US.
- Further incorporation of AI tools to help users understand their data.
Dexcom
- Timeline and details on Dexcom G8 development at undisclosed investor event.
- Real-world traction of Smart Basal and software updates.
- Impact of G7 15 Day on material growth.
- Discontinuation of the G6 and transition to G7 support.
- Continued interoperability with several AID systems.
Medtronic
Roche
- Acceleration of Accu-Chek SmartGuide manufacturing and broader European rollout.
- Expansion of Roche’s Kidney Klinrisk Algorithm.
Senseonics
- Full in-house commercialization of Eversense in the US beginning at the start of 2026.
- European launch of Eversense 365 following CE-Mark approval.
- Regulatory and clinical progression of next-generation implantable CGMs: Gemini system and Freedom.
Insulin Delivery
Abbott
- DGK integration with multiple pump partners.
Beta Bionics
- Continued acceleration of iLet adoption, led by pharmacy-channel expansion.
- Initiation and early readouts from clinical development of the bihormonal iLet system, following the start of human feasibility studies in late 2025.
- Ongoing progress toward the Mint patch program targeting a 2027 commercial launch.
Diabeloop
- European commercial launch of DBLG2 algorithm with ViCentra’s Kaleido patch pump, following CE-Mark approval.
- Potential US commercial launch of DBLG2 algorithm following FDA clearance, though potential pump partners remain unclear.
Insulet
- Omnipod 5 integration with Abbott’s FreeStyle Libre 3 Plus.
- Evidence from STRIVE RCT and EVOLUTION 2 T2D feasibility study.
Medtronic
- Expanded real-world adoption of MiniMed 780G across new indications.
- Continued advancement of next-generation pump hardware: MiniMed Flex and MiniMed Fit FDA submission timelines.
- Launch of Vivera fully closed loop US pivotal trial.
- CE-Mark submission of MiniMed Flex.
- FDA submission of MiniMed Fit.
- Update on FDA application for MiniMed Go.
Roche
- Accu-Chek SmartGuide CGM integration with mySugr app rollout in Europe.
Tandem
- International launch of Mobi OUS.
- Mobi Tubeless final stage testing.
- Launch of pivotal study for Tandem’s fully-closed loop algorithm.
- Tandem Source international expansion.
- Mobi Android FDA clearance.
- Continued broader global rollout of t:slim X2 integration with FreeStyle Libre 3 Plus.
Senseonics
- Eversense 365 integration with Sequel’s twiist.
Sequel
- Continued rollout of twiist throughout territories in the US.
- FDA of twiist for T2D.
Tidepool
- Continued integration of FreeStyle Libre with Tidepool.
- Real-world dataset with Ōura Ring.
Ypsomed
- Launch of new autoinjector line in Solothurn, Switzerland.
Digital Health
endo.digital
- Continued rollout of DreaMed Advisor Pro 2.0 platform for people with T1D and T2D on MDI.
Glytec
- Increasing rollout of Glytec in Ardent Health clinics and hospitals.
- Updates on a US launch of the cobas pulse BGM.
mySugr (Roche)
- Continued growth of mySugr beyond six million users.
- Additional data readouts at conferences.
Omada Health
- Continued integration of digital care and pharmacotherapy as GLP-1 prescribing integrated.
Teladoc
- Further international growth with greater expansion into non-English speaking countries.
- Increasing number of members enrolled in multiple chronic care programs.
Welldoc
- Further expansion of BlueStar digital health platform to the EU.
Themes
1. CGM reaches ~11 million global users at end of 3Q25, powered by adoption in growing populations; regulatory clearances expand competitive landscape
The CGM landscape continued its upward trajectory in 2025, driven by sustained uptake by people with T1D, rapid growth among those with T2D, and the continued emergence of real-world evidence supporting the multidimensional benefits of CGM use. Reflecting on the global market, we now estimate that approximately 11 million people were using CGM by the end of 3Q25, representing a 10% increase from the roughly 10 million users in late 2024 and a 38% increase from the eight million users in late 2023. See the figure below for an expanded time series on the estimated global CGM userbase over the last 15 years. The total CGM market reached ~$3.5 billion at the end of 3Q25, fueled by expanding international reimbursement for insulin-using T2D and national reimbursement for non-insulin T2D, and the first full year of over-the-counter (OTC) CGM availability in the US (Dexcom’s Stelo and Abbott’s Lingo). With nearly one million new users added globally, CGM continues to become entrenched as a foundational tool for glycemic monitoring and as a standard of care.
Estimated CGM Global Userbase (2010-3Q25)
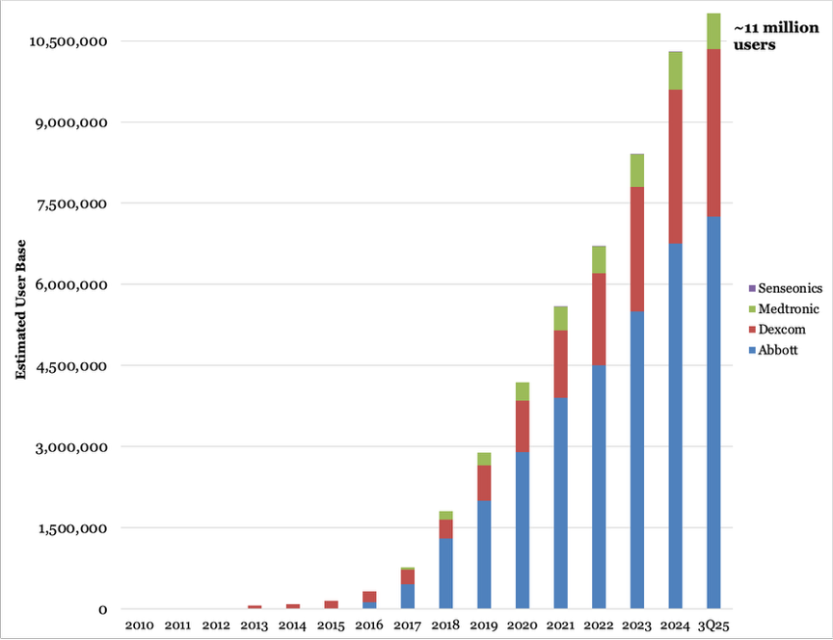
Source: Close Concerns Knowledgebase
- Regulatory momentum was strong in 2025, with several clearances and launches shaping the competitive landscape, including: (i) FDA clearance of Dexcom’s G7 15 Day CGM for adults with diabetes in April; (ii) FDA clearance of Medtronic’s Simplera Sync in April; (iii) FDA De Novo authorization for the Biolinq Shine patch-based CGM in September; and (iv) Medtronic’s rollout of the Abbott-developed Instinct CGM beginning in September. Taken together, these clearances reflect a growing competitive landscape featuring new form-factor designs, ultimately bringing greater choice to people with diabetes.
- Dexcom received FDA clearance for the G7 15 Day sensor in April for adults with T1D, T2D, and gestational diabetes, extending wear to 15.5 days (which includes the 12-hour grace period) and aligning more closely with Abbott’s 15-day Libre Plus sensors. Pivotal data presented at ATTD showed an overall MARD of 8.0%, modestly improving on 10-day G7 performance and meeting iCGM standards. The 15-day sensor officially launched in the US on December 1, with international launches expected in 2026.
- Medtronic made significant regulatory and commercial progress on two new sensors in the US in 2025. Shortly after Medtronic’s SmartGuard algorithm received FDA clearance as an iAGC controller in September and MiniMed 7880G was cleared as an ACE pump (enabling integration with external sensors), the company began its rollout of Instinct, a 15-day iCGM developed by Abbott for exclusive use with MiniMed systems. A full launch was initiated at the beginning of December. Simplera Sync, meanwhile, received FDA clearance in April and has since rolled out.
- Biolinq’s Shine received FDA De Novo Classification in September as the first Glucose Range Monitoring System, targeting adults with T2D not on insulin. The intradermal patch combines glucose, activity, and sleep metrics, with a color-coded LED display providing Time in Range (TIR) feedback visually and detailed insights via the app.
- A growing body of evidence reinforced that CGM meaningfully improves outcomes extending well beyond glycemic metrics, including impacts on renal risk, hypoglycemia prevention, and meaningful behavioral change. At ADA, a large retrospective analysis of adults with insulin-treated diabetes and CKD (n=65,839) showed that CGM initiation was associated with less CKD progression (29% vs. 35%) and a 14% slower decline in eGFR over three years, alongside greater reductions in A1c levels. At EASD, Dr. Hans DeVries reviewed RCTs and real-world evidence showing that CGM significantly reduces recurrent and severe hypoglycemia, particularly among individuals with impaired awareness, and reduces the frequency of emergency room visits. Collectively, these studies strengthen the case for CGM as a multidimensional chronic-disease tool with clinical, behavioral, and cardiometabolic benefits.
- Of course, additional data emerged on its ability to improve A1c and TIR outcomes through diet, activity, and medication habit modifications, helping solidify CGM as a routine tool for people with T2D. Findings from the UNITE study in adults with T2D on non-insulin therapy showed that Dexcom G7 initiation significantly improved TIR in both nutrition-focused and a self-directed arm, while also driving measurable behavioral change such as improved Healthy Eating Index sores and greater confidence in food decisions among participants receiving structured guidance. Regardless, education still helps – CGM-integrated DSMES showed larger glycemic improvements for people with T2D on basal-only insulin. The ROUTE-T1D trial similarly demonstrated that a brief educator-led telehealth intervention improved A1c by 0.7% (from 10.7% to 10.0%) and increased CGM wear-time among socioeconomically diverse youth with historically low technology engagement. At ATTD, Drs. Hirsch, Beck, and Bergenstal also highlighted enhanced outcomes when CGM is paired with GLP-1 RA therapy, and Dr. Bergenstal proposed a “2 × 2” framework that incorporates people with diabetes and healthcare providers in a cross-section of medication and CGM use.
- Initiation of CGM earlier in the disease course was a topic of discussion in 2025, including its potential role in both T1D and T2D diagnosis. At ATTD, Profs. Chantal Mathieu and Tadej Battelino highlighted CGM’s growing diagnostic value, emphasizing that early glucose abnormalities can be detected and addressed long before traditional markers shift. Prof. Mathieu described how CGM-derived patterns that can help stratify progression risk in stage 2 T1D. Prof. Battelino, meanwhile, asserted that CGM should be routinely offered to those with T2D and those with prediabetes, as early glucose abnormalities can be identified and addressed with lifestyle or pharmacologic interventions. He further proposed that CGM could soon become an independent diagnostic marker for dysglycemia, either by establishing specific glucose thresholds for prediabetes and T2D or by incorporating dynamic markers of glycemic variability. Both noted that although formal guidance has yet to catch up, “we have an unwritten consensus already” on the value of initiating CGM as early as possible.
- OTC CGM ended its first full year of availability in the US. While commentary on uptake of these devices has been sparse, Dexcom presented early Stelo real-world engagement data at ADA and Abbott expanded Lingo availability to Walmart, marking the first major brick-and-mortar OTC rollout and an important step for accessibility.
- Continuous ketone monitoring (CKM) platforms signal a shift toward multi-analyte sensing that could redefine metabolic monitoring. At ADA, Dr. Jennifer Sherr presented new pivotal data on Abbott’s dual glucose-ketone (DGK) sensor, demonstrating that ketone levels can rise independently from glucose and highlighting why real-time dual sensing may help identify infusion-set failures among AID users and proactively prompt ketosis management. In its product theater at ADA, Abbott also previewed new data on its multi-analyte sensor, with early clinical evidence suggesting improved pattern recognition and earlier detection of DKA risk compared to glucose-only monitoring. Many have also highlighted the sensor’s potential to safely bring the SGLT-2 inhibitor drug class to people with T1D safely. Momentum is already building across the industry, with five pump partners already confirming it would integrate with the DGK: (i) Sequel’s twiist; (ii) Tandem’s t:slim X2 and Mobi with Control-IQ+; (iii) Beta Bionics’ iLet; (iv) Ypsomed’s mylife Loop; and (v) Insulet’s Omnipod 5.
2. AID uptake continues to grow with guidance on initiation at diagnosis and more systems available to the T2D population in the US and Europe
AID continued its strong growth throughout 2025 with several major regulatory clearances and launches of CGM integrations that will provide more choice for people with diabetes. We estimated that nearly 1.6 million people worldwide use AID systems at the end of 3Q25 (see graph below). Looking ahead, we see no signs of the AID market slowing down, as three AID systems have now received FDA clearance for people with T2D in the US (Omnipod 5, Control-IQ+, and MiniMed 780G), and the EU added MiniMed 780G to its cleared AID in T2D armamentarium (more on this below). While barriers related to access, continued challenges with exercise, prescriber bias, and difficulty with implementation within clinic workflows (particularly in primary care clinics) may impede broader uptake, we are hopeful that expanding interoperability will be able to better meet the unique needs of people with diabetes and enable more people to achieve improved outcomes. Furthermore, we are optimistic that strengthening ADA Standards of Care now designating AID systems as “the preferred insulin delivery system” for all people with T1D, as well as for adults and children with T2D who are currently using MDI, insulin pumps, or sensor-augmented pump therapy.
Estimated Global AID Userbase (3Q17-3Q25)
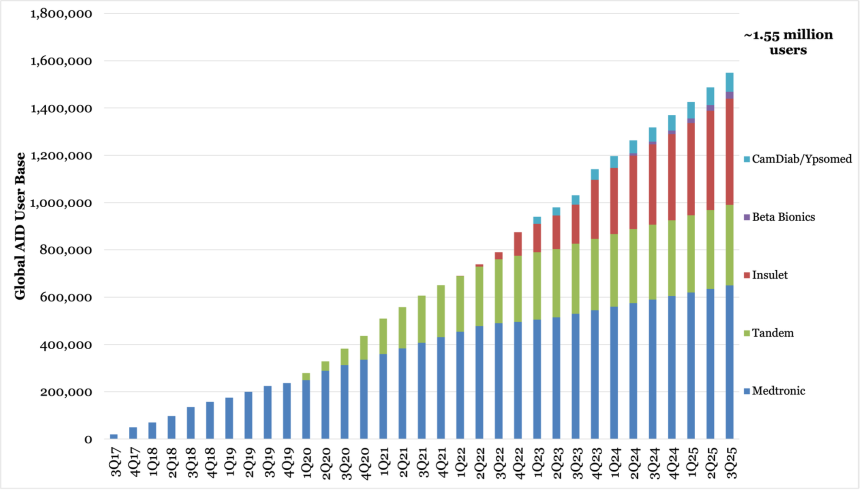
Source: Close Concerns Knowledgebase
- People with T2D in the US and EU were clear winners in the AID landscape in 2025. The first AID system to receive FDA clearance for the population, Omnipod 5 (August 2024), took advantage of its head start in the population and took the US by storm. Since then, up to 35% of new quarterly US starts have come from people with T2D and the company has focused on “taking the science to the street” by educating endocrinologists and PCPs on the latest evidence and treatment standards, and field teams are being equipped for peer-to-peer education and serving as “AID evangelists” to drive adoption in T2D. While Insulet worked on bringing more patients with T2D into the AID fold, two additional AID systems in the US received clearance for use in adults with T2D in 2025: Tandem’s updated Control-IQ+ algorithm in February and Medtronic’s MiniMed 780G in September. MiniMed 780G also received CE-Marking for use in T2D in July. Both companies have plenty of room left to begin taking share – estimates continue to place AID penetration among the US intensive insulin-using population with T2D (~2.5 million people) at only ~5%. Tandem is set to begin expanding its T2D commercial strategy beyond pilot programs. Early commercialization efforts have suggested that T2D users generally prefer t:slim X2 over Mobi, gravitating to the pump’s screen display and 300-unit reservoir size compared to the 200-unit reservoir of the screen-less Tandem Mobi.
- Sequel Med Tech launched its system in 2025: Sequel’s twiist, which is the first FDA-cleared AID system to use an algorithm based on Tidepool Loop, entered a full commercial launch in early fall. The system is also the first FDA-cleared system to offer direct control through the Apple Watch and offers the broadest customizable correction range of any commercial system (87-180 mg/dL).
- Meanwhile, CamDiab’s CamAPS FX, which will be the first FDA-cleared algorithm for pregnancy in T1D, has not yet launched in the US despite the algorithm receiving FDA clearance in 2024. This is due to the lack of an FDA-cleared insulin pump integrated with CamAPS FX in the US offering integration with CGMs Dexcom G6 and FreeStyle Libre 3. Ypsomed submitted its mylife YpsoPump for FDA clearance in the beginning of 2024, but we have not heard any regulatory updates since.
- Interoperability continued to expand in 2025.
- Insulet has launched FreeStyle Libre 2 Plus integration for users in several markets, including the UK, Netherlands, US, Italy, Belgium, Switzerland, the Nordic countries, and Australia. It also integrated Omnipod 5 with Dexcom G7 in at least a half dozen international markets: Sweden, Denmark, Finland, and Italy, the UK, and the Netherlands. In the US, Omnipod 5 integrated with Dexcom G7 15 Day at its launch in December 2025. Looking ahead, the company plans to integrate Omnipod 5 with FreeStyle Libre 3 Plus in 1H26, marking compatibility with every major CGM in the US.
- Tandem launched t:slim X2 integration with FreeStyle Libre 3 Plus in the US in October, with an international launch of the integration and integration with Tandem Mobi expected to come next year – slightly delayed compared to expectations, as an international launch of the compatibility was initially planned for 3Q25. The company continues to work on compatibility with the G7 15 Day.
- Beta Bionics’s iLet integrated with the G7 15 Day at launch.
- Sequel launched in the US with FreeStyle Libre 3 Plus integration and Eversense 365’s integration with twiist is its first entrance into AID systems.
- While Medtronic still does not integrate MiniMed 780G with any non-Medtronic CGMs, it added two new sensors to the MiniMed 780G platform’s repertoire in the US in recent months: Simplera Sync and the Abbott-developed Instinct. Both sensors have already seen strong order rates, and Medtronic is optimistic that their availability will drive MiniMed 780G adoption in the US. Simplera Sync availability expanded across the EU in 2025, now available in approximately 30 countries, and has fueled OUS MiniMed 780G growth.
- We continued to see new data of AID systems in expanded populations, including pregnancy and very young children.
- On AID use during pregnancy, Tandem’s CIRCUIT trial (n=88) for t:slim X2 in pregnant women with T1D was published in JAMA Network in October. Those using t:slim X2 during pregnancy achieved significantly higher mean Time in Pregnancy Range (TIPR, 63-140 mg/dL) than those continuing standard care (CGM; 65% vs. 50%), supporting the efficacy and safety of the system’s use. An immediate improvement to TIPR was seen within a week of initiating Control-IQ, rising from a median of ~55% to nearly 70%. TIPR rose to ~75% in the final few weeks of gestation. Exploratory outcomes from CIRCUIT suggested additional maternal benefits with t:slim X2 use, including: (i) lower A1c levels (0.4 points lower at 34 weeks than standard care); (ii) reduced preeclampsia rates (14% versus 25%); and (iii) lower total insulin requirements (by ~28 units/day).
- On AID in preschoolers, Dr. Klemen Dovč (University of Ljubljana, Slovenia) presented findings from the extension phase of Medtronic’s LENNY trial at ATTD 2025, in which Simplera Sync demonstrated non-inferiority to the Guardian 4 sensor in preschoolers – the A1c difference between groups was not statistically significant (7.3% vs. 7.2%), and there was no clinically significant difference in TIR between treatments (70% vs. 69%). At ATTD 2025, Dr. Jolien De Meulemeester (KU Leuven, Belgium) presented results of a 12-month prospective, observational study of MiniMed 780G in those aged 2-6 years. The study showed median TIR increased 10% (+2.3 hours/day) from 57% at baseline to 66% at 12 months, with equivalent gains to TITR (from 36% to 46%). Median A1c decreased 0.3% from 7.6% at baseline to 7.3% at 12 months, and school and work absenteeism tended to decrease. In July, Medtronic received CE-Mark approval for MiniMed 780G use in those aged 2+ years.
- Also at ATTD 2025, Dr. Torben Biester (Auf Der Bult, Germany) shared findings from a single-center, prospective study (n=27) evaluating the impact of switching preschool-aged children (younger than six years old) with T1D from predictive low glucose management systems to the mylife Loop AID system. TIR increased 2.9 hours/day from 52% to 64% after three months, and A1c decreased significantly from 7.8% at baseline to 6.8% in the same timeframe; reductions remained stable at six months. Another study published in DT&T in November showed that within the first month of CamAPS FX use, TIR rose by ~11%, (from 54% to 64-65%) and A1c levels dropped 0.9% (from 7.8% to ~7.0%).
3. Closing the loop: Studies evaluating the safety and efficacy of FCL algorithms in T1D and T2D march on; FCL-like use grows in HCL users who don’t bolus
In 2025, the push to "close the loop" in automated insulin delivery continued to gather momentum, with several new studies and updates from major diabetes tech companies on upcoming feasibility and pivotal trials.
- Several FCL algorithms made significant strides, with new feasibility data and commitments from the industry to advance their systems.
- CamAPS HX: A randomized crossover study published by DT&T in June compared the FCL CamAPS HX algorithm to sensor-augmented pump (SAP) therapy among adolescents with T1D and above-target A1c (n=24). The results showed that FCL use resulted in a significantly higher TIR compared to SAP (45% vs. 32%), translating to a 3.1-hour daily difference. This improvement was driven by a reduction in Time above 250 mg/dL, which was 7% lower with FCL (29% vs. 40% with SAP). Time below Range (TBR) was similar between groups (2.8% for FCL vs. 3.0% for SAP). However, there was no significant difference in A1c (8.6% with FCL vs. 8.9% with SAP).
- EVOLUTION Study: Insulet announced at its Investor Day in November that it plans to launch its FCL AID system in 2028. Insulet's initial focus will be on the T2D basal-bolus population, with expansion planned for basal-only patients. The EVOLUTION2 feasibility study is expected to begin enrollment in 2026, with a regulatory submission anticipated in 2027.
- FCL@Home Study: At ATTD 2025, Dr. Laya Ekhlaspour (UCSF) presented feasibility results from the FCL neural-net AIDANET algorithm (n=36). Among participants with an A1c <8.0%, FCL was noninferior to usual care (68% vs. 66% TIR). In those with A1c >8.0%, FCL demonstrated significant improvements, with 13% greater TIR (+3.2 hours/day) compared to usual care (62% vs. 49%). Dr. Erin Cobry (University of Colorado) later presented daytime and nighttime results at ADA 2025, where AIDANET use showed non-inferiority to HCL care for daytime (58% vs. 56% TIR), and significantly greater TIR during nighttime use (76% vs. 64%). Also at ATTD 2025, Dr. Boris Kovatchev (University of Virginia) presented promising early results from a study combining AIDANET with a glucose pretrained transformer for automated bolus priming (Bolus GPT). In the first six participants, this combination delivered a 2.2-hour/day improvement in TIR, reaching 76% compared to 67% with AIDANET alone. TITR was also improved, reaching 53% with Bolus GPT and AIDANET versus 46% with AIDANET alone.
- Tandem Freedom: Tandem’s clinical trial for its FCL AID system completed in 2Q25, with a pivotal study expected to start in 2026. Dr. Tom Wilkinson (University of Otago) presented data on the second-generation Tandem Freedom FCL system at ATTD-Asia 2025, which showed strong overnight glycemic outcomes. The median TIR was 61%, an improvement from 56% during the run-in period, with overnight TIR nearly reaching 100% (96%). The system responded quickly to meals, with most postprandial insulin was delivered within two hours for all meals despite the lack of user-initiated announcements.
- Medtronic Vivera: Medtronic announced in 3Q25 that the FDA had authorized the initiation of a US pivotal trial for its third-generation FCL algorithm, "Vivera."
- Inreda AP: DT&T published a qualitative follow-up study in October on the FREE 1 trial, which evaluated Inreda’s bi-hormonal FCL system that delivers both insulin and glucagon. Interviews with participants (n=12) revealed that many found the system transformative, easing the burden of carbohydrate counting. However, some users expressed frustration with the device’s complexity, including daily glucagon changes, two sensors, and frequent alarms. Overall, participants reported feeling less burdened by diabetes, reflecting the strong quantitative outcomes (~80% TIR) from the FREE 1 trial.
- Several companies also demonstrated the effectiveness of their AID systems with simplified meal reporting, further reducing the burden on users.
- Control-IQ: Dr. Laurel Messer (Tandem) highlighted a 12-month single-center study of Control-IQ users at EASD 2025, with the majority relying on AutoBolus (>90%). The study showed a 19% increase in TIR and a 1.6% reduction in A1c from baseline.
- MiniMed 780G: Dr. Jennifer McVean (Medtronic) presented real-world outcomes at ADA 2025 from the MiniMed 780G on days without user-initiated boluses (n=54,553). The system achieved a mean TIR of 71%, with a mean TITR of 44%. Among non-recommended settings users (n=41,830), 37% met the triple composite endpoint: (i) GMI <7.0%; (ii) TIR >70%; and (iii) TBR <4.0%. In comparison, 62% of recommended settings users (n=12,723) met this endpoint.
- At EASD 2025, Dr. Salvatore Scirè Calabrisotto (University of Catania, Italy) compared the response of Medtronic MiniMed 780G and Tandem Control-IQ to unannounced meals in a randomized crossover study (n=20). MiniMed 780G had a lower mean peak (~200 mg/dL) compared to Control-IQ (~220 mg/dL). Both systems performed similarly in terms of TIR and TITR with announced meals, though MiniMed 780G handled unannounced meals slightly better, suggesting that PID-based algorithms may be more effective in such situations.
- Omnipod 5: Dr. Sean Oser (University of Colorado) presented at ADA 2025 data showing that while users who bolused more frequently achieved higher TIR (74% with >4 boluses/day vs. 62% with <1 bolus/day), those relying on simplified carbohydrate counting (using just five main carbohydrate values) achieved comparable outcomes to those using precise carbohydrate counting (69% vs. 73% TIR).
- Open-source AID: A study conducted in China (n=32) with adults with T1D alternated between two weeks of open- and closed-loop use while employing a non-carbohydrate counting meal bolus strategy. After a one-week run-in period, participants achieved ≥70% TIR, with significantly higher TIR (79%) during closed-loop use compared to open-loop (not specified).
- Faster insulins and AID system compatibility. While the FDA cleared fast-acting insulins for use with all insulin pumps in 2021, it required that individual pump manufacturers demonstrate compatibility with AID system algorithms – in 2025, several significant updates on this front were made. In September, Tandem announced FDA clearance to use its t:slim X2 with Control-IQ+ in combination with Lilly’s fast-acting insulin, Lyumjev (insulin lispro-aabc), becoming the first AID system cleared for use with Lyumjev in the US. Meanwhile, Medtronic submitted for FDA clearance of the MiniMed 780G with fast-acting insulins (Lyumjev, Fiasp, Merilog) in 1Q25. Additionally, Sequel entered a co-development agreement with Arecor in September to pair its ultra-rapid insulin AT278 (500 U/mL) with Sequel’s Twiist AID system. This collaboration aims to enable next-generation AID systems with longer wear times and miniaturization potential, especially for individuals with high daily insulin needs.
- Bi-hormonal AID systems. In 3Q25, Beta Bionics reported progress on its bi-hormonal AID system, which delivers both insulin and glucagon. The company completed its first pharmacokinetic-pharmacodynamic (PK-PD) bridging trial for its proprietary glucagon, marking a key milestone. Results met expectations, allowing the company to proceed with a human feasibility study for the dual-hormone system, scheduled for 4Q25. This will precede pivotal trials and regulatory submissions for both glucagon and the integrated device.
4. TITR, Time in Normoglycemia, Time in Happiness? Tighter glycemic management gains traction as debate on its name (and ideal range) emerges
The conversation around Time in Tight Range (TITR; 70-140 mg/dL) moved further into the spotlight in 2025. As part of it, clinicians debated the benefits of tighter management against the clinical and psychosocial challenges of demanding even more precision than with TIR (70-180 mg/dL), and whether TITR should be a primary goal or a secondary metric. This prompted some to suggest a parallel focus with TIR and TITR to balance clinical goals with real-world burden.
- At ADA, Prof. Tadej Battelino (University of Ljubljana, Solvenia) delivered a strong push to replace A1c with CGM-derived metrics, arguing that TIR and TITR outperform A1c in predicting complications and detecting early dysglycemia. He highlighted data linking TITR to reductions in mortality, albuminuria, and retinopathy in T1D and T2D, arguing that it captures early physiologic deterioration that A1c can fail to recognize. Prof. Battelino also introduced the name “TING” – Time in Normoglycemia – explaining that the new name reflects the goal to achieve “normal glycemia.”
- At ATTD, qualitative work from people with diabetes and caregivers revealed enthusiasm for TITR’s potential but concern about burden, burnout, and feasibility, prompting calls for “Time in Happiness” as an alternative goal. Dr. Molly Tanenbaum (Stanford University) shared survey and interview data showing that while about one-third of respondents were open to TITR and many in this group were already informally using 70–140 mg/dL targets with AID systems, roughly two-thirds expressed hesitancy, citing fears of increased hypoglycemia and lack of tools or algorithm performance to realistically sustain tighter ranges. Some parents and athletes worried that TITR-based targets could constrain food choices or safe exercise, while others emphasized that any new goal must be phased in and accompanied by clear evidence of benefit. One respondent’s suggestion to prioritize “Time in Happiness” as an alternative to conventional glycemic metrics captured the emotional impact: tighter numbers alone are not enough if they come at great expense to quality of life.
- A lively debate at ATTD highlighted a key question: should TITR be a core clinical target today or remain a research metric for select groups? Arguing in favor, Dr. Anders Carlson (International Diabetes Center) described TITR as a powerful early-warning signal and complication predictor, citing data linking incremental decreases in TITR with higher risks of retinopathy, microvascular complications, and cardiovascular mortality, and proposing that TITR may detect dysglycemia earlier than TIR can. He outlined patient profiles where TITR might be especially useful, including newly diagnosed individuals aiming for physiologic normoglycemia and those with rising A1c levels driven by high Time in 140-180 mg/dL.
- In contrast, Dr. Jeremy Pettus (UCSD) argued that TIR remains a more patient-friendly target, warning that current technology is not yet capable of consistently delivering this tight management without increased hypoglycemia and burden. He said pushing TITR as a primary goal risks demotivating patients already struggling to achieve TIR. He supported TITR as a valuable research metric but cautioned against premature clinical adoption.
- TITR moved from a niche metric to a practical benchmark in 2025, with multiple studies showing that it can improve meaningfully across AID systems. Namely, we saw large real-world datasets demonstrating that modern algorithms can raise TITR by two to three hours per day while maintaining low hypoglycemia and reduced burden. These findings suggest that when people access advanced AID systems and use optimized settings, tight glycemic profiles are achievable.
- With MiniMed 780G, a cohort of users without user-initiated boluses (n=54,554) showed that mean TITR still reached 44% overall and nearly 50% among users on recommended settings with the system. Elsewhere, Dr. Jennifer McVean (Medtronic) presented three-year real-world evidence (n=1,145) from MiniMed 780G users (≥16 years old) across Europe, the Middle East, and Africa, showing sustained glycemic improvement, with TITR rising from 40% at baseline to 54% and remaining over 50% through 36 months. In yet another MiniMed 780G analysis (n=40,975) stratified by Area Deprivation Index, Dr. McVean found that TITR averaged ~47% across all socioeconomic quartiles, with users on recommended settings reaching ~52% TITR and higher rates of target achievement.
- With Tandem’s Control-IQ, real-world data in children under 11 years showed that both children under six and those six to 10 years old achieved significant and sustained TITR gains by six months, with earlier initiation after diagnosis associated with greater TITR and lower A1c levels. The two-year INRANGE study (n=473) of Tandem’s Control-IQ echoed this durability in adults with T1D, where TITR increased from 37% at baseline to 45-46% at 12 and 24 months. The number of participants achieving TITR over 50% nearly doubled, alongside sustained A1c improved and reduced hypoglycemia.
- The evidence base supporting TITR as a meaningful metric for people with T2D not using insulin continued to expand. In the UNITE RCT of adults with T2D (n=124) on non-insulin therapy initiating Dexcom G7, TITR increased 4.3 hours/day in the nutrition-focused education arm (from 16% to 34%) and 2.9 hours/day in the self-directed arm (from 23% to 35%) over two months, with minimal Time below Range (TBR), significant TIR and A1c improvements, and added dietary quality gains in the nutrition-focused group. Dexcom’s first real-world analysis (n=61,085) of Stelo users expanded this picture into the OTC landscape. There were notable differences to TITR achieved by individuals without diabetes, with prediabetes, and with non-insulin T2D (baseline TIR >70%), at ~93%, ~86%, and ~65%, respectively. These data highlighted TITR’s sensitivity to subtle dysglycemia that standard TIR metrics might fail to recognize. Regardless, in the highest-risk subgroup (people with T2D and baseline TIR ≤70%) TITR still improved from 12% to 20% (+1.9 hours/day) with 30 days of Stelo use, further suggesting that visibility alone can help guide users toward tighter glucose management.
5. Diabetes technology in pregnancy: Evolving global guidelines and the search for more data
Diabetes in pregnancy was defined in 2025 by new global guidelines and regulatory milestones, along with real-world and clinical evidence supporting both CGM and AID use across T1D and GDM. These developments highlighted AID and CGM as powerful tools in the management of T1D pregnancy, while also highlighting the need for pregnancy-specific algorithms, clinician training, and thoughtful implementation.
- 2025 guidelines aligned on expanding technology and structured glycemic management in pregnancy, with the ADA advancing AID use and the World Health Organization (WHO) issuing its first global diabetes in pregnancy care framework. Conferences throughout the year became grounds for clinician education on the evolving guidelines for the population. At ADA, Dr. Sarit Polsky (University of Colorado) outlined extensive updates to the ADA Standards of Care’s pregnancy chapter that recommended (and reiterated in the 2026 iteration published earlier this month) that clinicians consider AID with pregnancy-specific algorithm for individuals with T1D, grounded in evidence from AiDAPT and CRISTAL studies. She emphasized that AID use must occur within experienced provider teams alongside foundational steps of reviewing medications throughout pregnancy and tightly coordinating care. Complementing this, Dr. Rita Kalyani (Chief Scientific and Medical Officer, ADA) promoted Recommendation 7.18 from the ADA 2025 Standards of Care, which formally recommends CGM use for T1D pregnancy. Globally, the WHO published a comprehensive set of guidelines for diabetes care during pregnancy. The guidelines introduced three core practices to guide care for women with diabetes during pregnancy: (i) individualized lifestyle guidance; (ii) education on maternal-fetal health effects; and (iii) access to specialized diabetes-pregnancy teams. Detailed recommendations were issued for glucose monitoring and establishing glycemic targets, including the use of CGM for T1D where available and BGM-based monitoring for T2D and GDM in most settings due to resource constraints. Together, the 2025 ADA and WHO guidelines highlight a growing global consensus that pregnancy care must move forward technology-supported approaches that make sense in the pregnant women’s lives.
- In July, Medtronic received CE-Mark for expanded indications including pregnancy, which launched in the fall. This is the first new AID pregnancy clearance in Europe since CamDiab’s CamAPS FX in 2020. The authorization, supported by data from the CRISTAL trial, positioned MiniMed 780G as a second option for pregnant women with diabetes. Notably, this clearance gives pregnant patients in Europe a choice between two regulated AID systems for the first time, representing meaningful progress in maternal glycemic management. Medtronic has also stated it expects to pursue removal of the pregnancy contraindication in the US, raising the possibility of expanded access beyond Europe in the coming year.
- NHS England launched the first nationwide pregnancy-specific AID initiative, expanding access to the technology in T1D pregnancy. In September, NHS England announced a national rollout of a pregnancy-tailored AID system for women with T1D who are pregnant or planning pregnancy. The program was backed by £3.7M (~$5M) in initial funding as part of a broader £60M (~$81M) initiative. The initiative aims to enable women to reach the tighter pregnancy glucose targets with the AID system and remote monitoring through NHS data infrastructure, aiming to reduce adverse maternal and neonatal outcomes in T1D pregnancy. With more than 600 women enrolled by the beginning of September 2025, this rollout positions the UK as the first country to systemically deploy pregnancy-specific AID use at a national level.
- New trials across T1D and GDM strengthened evidence for CGM to improve maternal and neonatal outcomes. At ADA, Dr. Karen Elkind-Hirsch (Dexcom) shared results from the Steady Sugar RCT (n=120), where early CGM use during pregnancy led to lower unscheduled C-sections (20% vs. 44%), fewer preterm births (7% vs. 18%), and better neonatal outcomes including reductions in LGA births (5% vs. 18%) and NICU admissions (23% vs. 45%). CGM is also received positively by pregnant women – Ms. Rachel Salzman (Weill Cornell) highlighted strong patient satisfaction and high adherence for CGM (76% wore CGM ≥70% of the time) in Weill Cornell’s virtual GDM program. At EASD, Prof. Tina Linder (Medical University of Vienna, Austria) presented results from the international GRACE RCT (n=375), showing that CGM use in GDM significantly reduced LGA rates (2.5% vs. 10.3% with BGM) and improved late-pregnancy glycemia. Prof. Helen Murphy (University of East Anglia, UK) echoed CGM’s role in identifying dysglycemia and GDM earlier in gestation and expressed optimism about forthcoming results from the MAGiC study and its collaboration with GLAM, which she hopes will show that abnormal glucose patterns are already detectable in the first trimester.
- We also saw more real-world data for AID use during T1D pregnancy. At ADA, Dr. Emily Szmuilowicz (Northwestern University) explained that most commercial systems struggle with responding to the rapid progression of insulin resistance during gestation (~250% of pre-pregnancy insulin dose by 35 weeks) and pregnancy-specific fasting targets (70-95 mg/dL). To support optimal outcomes, she outlined trimester-specific adjustments across systems, including: (i) pregnancy-tailored glucose targets (i.e., Time in Pregnancy Range); (ii) aggressive insulin-carbohydrate ratios; (iii) careful pre-bolus timing; and (iv) repeated correction factor updates. At ATTD, Dr. Emma Wilmot described a “watershed moment” for AID adoption in T1D pregnancy, citing 100% uptake in her clinic. At Ypsomed’s sponsored session, Prof. Helen Murphy presented new CamAPS FX pregnancy data demonstrating 1.8% A1c reductions from an undisclosed baseline and 63% of users reaching <6% A1c, alongside healthcare cost reductions and declines in preeclampsia.
6. Inpatient CGM use demonstrates positive impact on glycemia and re-hospitalization rates as accuracy shows mixed bag
Following the less-than-promising results of the TIGHT study in 2024, 2025 was a consequential year for data supporting the technology’s use in the hospital setting. For reference, the highly-anticipated TIGHT study ultimately found no significant difference in mean glucose with CGM use between the intensively managed and standard management groups, though some have since said that this does not mean CGM is ineffective in the inpatient setting – rather, the 90-130 mg/dL target may not be realistic in “real life.” Regardless, support for the use of CGM and decision support systems grew throughout the year.
- Evidence on inpatient CGM accuracy accumulated in 2025:
- At EASD 2025, Prof. Mikkel Olsen (Steno Diabetes Center Copenhagen) presented the DIETEC trial (n=166), which showed that inpatient CGM use increased TIR by 15 percentage points (from 63% to 78%) in patients with T2D. Patients using CGM achieved steady improvements in TIR by discharge, while those using BGM plateaued at 60%. Additionally, CGM use was linked to a 24% reduction in hospital complications, particularly infections. Prof. Olsen acknowledged that accuracy is strongest in non-ICU settings and more variable in ICU patients, reinforcing the need that many in the ICU may need more attention to glycemic health. He called for a consensus framework to define patient selection criteria and glycemic targets, as well as for better integration of CGM data into EHRs.
- Dr. Lyn Hopkinson and colleagues from MedStar Health presented a real-world study at ADCES 2025 showing a clinically significant 79% reduction in hypoglycemic events with CGM use. This study found that CGM provided more accurate readings in patients with blood sugar below 85 mg/dL compared to BGM, supporting its use in detecting and managing hypoglycemia.
- In a study on ICU patients published in DT&T in May, Dr. Jesica Baran (University of Washington) et al. analyzed the accuracy of the Dexcom G7. They found that the MARD in ICU settings was slightly higher (16%) than in outpatient settings, but similar to the MARD observed in non-ICU hospitalized patients (15%). This data underscores the potential for CGM to be useful in critically ill patients, though accuracy remains more variable in such settings. Elsewhere, Dr. Guillermo Umpierrez (Emory University) teased an ongoing RCT comparing Dexcom G7 with POC glucose testing in hospitalized patients with T2D.
- Dr. Magdalena Bogun (Columbia University) presented an observational study (n=163) on the use of CGM in DKA management with IV insulin infusion at EASD 2025. Although CGM sensors showed a MARD of 17.4% during IV insulin treatment — above the typical 10% threshold for outpatient use — the study's Clarke Error Grid analysis indicated that 99% of paired values were within acceptable ranges (Zones A/B) during treatment and 96% post-resolution. The study also found that CGM use resulted in significantly fewer POC tests compared to standard care (five vs. 12 tests, p<0.0001). However, the difference in median hospital stay (120 hours for CGM vs. 99 hours for standard care) was marginally significant, potentially making a noticeable difference to patients.
- Clinicians and guidelines increasingly support the noninferiority of some CGMs to point-of-care (POC) BGM for inpatient glucose management. Prof. Spiros Fourlanos (University of Melbourne, Australia) provided an overview of the growing use of CGM in hospitals, highlighting both its clinical benefits and the challenges posed by real-world implementation. He discussed data from several RCTs, including the DIATEC study presented at EASD 2025. Guidelines from major organizations, including the ADA and recent Australian standards, now endorse CGM use in non-critical care patients, provided it is accompanied by POC monitoring. He emphasized the need for practical rules to ensure safe implementation, including to: (i) remove CGM only if the patient cannot participate (e.g., unconsciousness); (ii) defer but do not necessarily remove during periods of hemodynamic instability; and (iii) otherwise, use CGM as a patient prompt for confirmation POC checks.
- Some clinicians are also looking forward to greater inpatient implementation of other diabetes technologies, including AID and decision support systems. At Diabetes UK 2025, Dr. Hood Thabit (Manchester University NHS Foundation Trust) discussed the potential of decision support software in glycemic management, though he noted the lack of robust RCT evidence. He also highlighted studies showing the benefits of FCL AID systems, which can reduce staff workload and improve glycemic control. Dr. Thabit stressed that successful implementation would require workflow adaptations and training, especially for non-diabetes specialists. Dr. Bruce Bode noted that new CMS mandates in the U.S., effective January 2026, would require hospitals to report severe hypoglycemic and hyperglycemic events, providing additional incentives for hospitals to address these issues proactively.
- In a bid to support the use of inpatient diabetes decision support systems, Glooko announced its acquisition of Monarch Medical Technologies, the maker of the EndoTool Glucose Management System, in September. EndoTool is an FDA-cleared software that provides patient-specific inpatient insulin dosing recommendations aimed at reducing hypoglycemia risk and standardizing outcomes across critical care units. Glooko, which has traditionally focused on outpatient remote monitoring, will expand its platform to integrate more hospital-based features, providing tools for inpatient insulin titration based on individual patient needs, including insulin sensitivity and comorbidities.
- Several companies and clinicians indicated 2026 will see broader uptake of these technologies with the goal of proactively addressing the issue of severe hypoglycemia and hyperglycemic events, as the CMS will begin mandating hospitals report the events beginning January 2026. Financial penalties for failing to report these events have not yet been disclosed, but Dr. Bruce Bode predicted they will drive uptake of tools like Glytec’s Glucommander, which expanded to more hospital systems in 2025.
7. The many faces of AI: Clinical applications, AI in research
AI is increasingly being applied in clinical care, particularly in diabetes management, drug discovery, and disease prediction. Throughout the year, experts emphasized its potential but also advise caution, particularly around issues of accuracy, data privacy, and human oversight.
- AI is transforming the way patients engage with their glycemic and nutritional data, helping contextualize it among other documented lifestyle inputs. Several companies are leading the way with innovative applications:
- Dexcom integrated CGM data with FriskaAi’s health management platform in August, offering real-time alerts, personal care recommendations, and clinician reports. Dexcom also launched AI-powered features like Food Logging (July) and Weekly Insights on its Stelo platform (December 2024), which provides GenAI-powered recommendations on diet, exercise, and sleep for users.
- Roche continued to roll out its AI-powered Accu-Chek SmartGuide Predict app, providing users with AI-powered glucose level predictions, alerts for low glucose risk, and recommendations for preventing hypoglycemia. The company presented a case study on the app’s use and these predictive features at the Swiss Economic Forum in June 2025.
- Omada Health launched Meal Map in October, an AI tool that analyzes the nutrient density of meals and offers personalized dietary recommendations. The new tool builds on Omada’s AI-powered “Nutritional Intelligence” suite, which includes the recently-launched OmadaSpark, and in an internal pilot study (n=1,000) the tool was associated with higher engagement in meal tracking compared to traditional calorie-focused approaches.
- Trinity Biotech unveiled plans in July for CGM+, an AI-powered CGM that is designed to track users’ glucose, heart activity, body temperature, and physical activity continuously. Trinity anticipates a commercial launch in 2026.
- Signos announced the launch of its AI-driven glucose monitoring platform for weight management in August, combining Dexcom Stelo data with a behavioral AI mobile app to deliver real-time, personal lifestyle recommendations. The company is conducting a large clinical trial to study its effects.
- Twin Health saw Cleveland Clinic-led RCT data published in NEJM Catalyst in which the company’s Twin Precision Treatment significantly outperformed standard care for T2D. A1c fell 1.3% after one year, significantly greater than the 0.3% reduction to 6.9% with usual care, and 71% of participants reached A1c <6.5% at one year vs. just 2% of those receiving standard care.
- Additionally, at the MDUFA VI public meeting, FDA Commissioner Dr. Martin Makary highlighted the FDA’s plans to optimize its application processing by digitizing the entire process, including with significant uptake (“thousands” of unique daily users) in the use of ELSA, its AI-powered reviewing tool.
- Yet another application of AI increasingly used by companies is in its role to accelerate drug development. Many have already announced partnerships with several AI-enabled companies to support their innovative pipelines, aiming to reduce timelines and improve the pace of candidate selection:
- Lilly has entered into at least a half dozen AI-based partnerships, including with NVIDIA, TuneLab, Superluminal, Atomwise, Genetic Leap, Isomorphic Labs, and an expanded partnership with Purdue University, to speed up drug discovery.
- Novo Nordisk has similarly appeared to have invested heavily in AI-enabled drug discovery and telehealth collaborations – the company has also partnered with NVIDIA, with Fangzhou on a Smart Healthcare Platform, and with Deep Apple Therapeutics to use AI-powered biological pocket extraction and protein movement modeling to identify and advance novel candidates for a broad range of diseases.
- Roche, expanding on its “Lab-in-the-Loop” approach that was a focus of its 2024 Digitalization Day, shared at its 2025 Pharma Day that its digitalization and AI strategies now includes greater use of generative AI to support R&D by accelerating protocol design, data collection, and study reporting. Roche’s “Lab-in-the-Loop” AI/machine learning model has already cut report generation time by >60%, increased screening yield by >10%, and reduced capital expenditures by making existing facilities more efficient.
- Sanofi reported in November using AI to reduce preclinical discovery timelines by 30-50% and cut costs by 25-50%. AI also helped identify 10 new drug targets within a year. Additionally, AI is being used to prevent supply shortages across 60 sites.
- AI is also being leveraged for chronic disease monitoring and early detection and risk identification for:
- Chronic kidney disease (CKD): Roche received CE-Mark approval for its Kidney Klinrisk Algorithm in October, launching the medical algorithm as part of a new CKD algorithm panel within Roche’s navify Algorithm Suite. The new CKD algorithm panel estimates the risk of kidney function decline in adults with CKD (G1-G4), diabetes, or hypertension, aiming to facilitate earlier risk assessments of patients and coordinated care across clinical teams.
- T1D: The NIH funded in October the Multimodal AI for Type 1 Diabetes (MAI-T1D) project to apply AI to understand the mechanisms driving T1D onset, hopefully uncovering early biomarkers and prevention strategies. Speaking on AI’s applicability in early T1D pathology, Prof. Moshe Phillip (Schneider Children’s Medical Center, Israel) said at Keystone 2025 that while initiating CGM within a year of T1D diagnosis is associated with strong glycemic benefits, the technology will likely require AI-enabled analytical tools to be useful in monitoring pre-T1D staging.
- Diabetic retinopathy (DR): AI tools for DR screening have been evaluated for longer than other conditions. Looking ahead, Ainnova Tech and Avant Technologies will be moving forward with a revised clinical trial protocol assessing the Vision AI platform for the early detection of DR leveraging AI to analyze fundus photos for retinal diseases. In addition to its high accuracy, Dr. Maria Cicinelli (IRCCS San Raffaele Scientific Institute, Italy) emphasized at EASD that AI-assisted screening can positively impact screening uptake by improving patient satisfaction, such as in children.
- Liver fibrosis: AI-powered tools like Altimmune’s Liver Explore have shown promise in analyzing liver fibrosis reduction in clinical trials, demonstrating how AI can streamline disease monitoring and treatment decisions.
- AI in lifestyle interventions and daily management: A phase 3 trial comparing AI-driven vs. human-led diabetes prevention programs (DPP) presented at DTM 2025 showed that AI-driven interventions were equally effective at reducing A1c and weight, suggesting that AI could become a viable alternative to traditional coaching. AI-based forecasting tools have shown potential in predicting hypoglycemia risk, enhancing patient safety, and Dr. Clara Mosquera-Lopez (Oregon Health & Science University) developed an AI algorithm for meal detection and insulin dosing that reduced Time above Range (TAR) by 11%. In a one-week outpatient study she presented at ADA 2025, the AI system showed performance similar to AID with fewer meal boluses, suggesting AI could reduce the burden of diabetes management.
- Clinical trial screening: Dr. AJ Blood (Mass General Brigham) discussed a recently-published trial RAG-Enabled Clinical Trial Infrastructure for Inclusion Exclusion Review (n=4,476) demonstrating that an AI-assisted screening tool can improve both speed and accuracy of trial enrollment compared to manual review.
- AI’s integration into healthcare raises important questions and challenges, particularly in terms of patient-clinician relationships and ethical considerations. Dr. Jeffrey Moon (University of Pennsylvania) discussed at CEU 2025 how AI tools can reduce clinician burden, but warned against information overload. AI solutions like automated message triage and chatbots, if used responsibly, could enhance trust and reduce communication gaps. Dr. Joniqua Ceasar (University of Pennsylvania) discussed at AHA 2025 how AI-enabled prior authorization tools and low-cost telehealth models have the potential to overcome logistical barriers for both clinicians and patients. Meanwhile, Dr. Peter Jacobs discussed at ADA 2025 the potential of AI chatbots in mental health care, emphasizing the risks of overdependence on technology. Specifically, he said that while AI can improve access to mental health services, it may lack the depth and understanding of human therapists, leading to deceptive responses. At ADCES 2025, Ms. Ka Hei Karen Lau (Joslin Diabetes Center) explained that chatbot-generated responses to patient questions have been rated nearly four times higher than physicians for quality (79% versus 22%), and nearly 10 times higher for empathy (45% versus 5%), with over three-quarters of respondents preferring the chatbot’s answer. Challenges remain, however: Dr. Kushner at ATDC 2025 outlined some of these risks of AI in clinical care, particularly the danger of biased algorithms and misinterpreting patient behavior.
8. New ways of continuous monitoring: CKM, range-based feedback, and early disease insight
In 2025, continuous monitoring technologies moved beyond their tradition role in daily glucose management, with growing attention on risk prediction, simplified interpretation, and earlier disease prevention. Across major conferences and regulatory milestones, continuous data was increasingly framed as a tool to detect metabolic dysfunction sooner and extend meaningful insight to broader populations. Three areas stood out this year: (i) continuous ketone monitoring (CKM); (ii) the emergence of glucose range monitoring (GRM); and (iii) the potential use of CGM to support earlier identification and monitoring of presymptomatic, early-stage T1D.
- CKM emerged as a potential tool for DKA prevention and safer therapy use. CKM drew attention throughout 2025, driven by anticipation of Abbott’s dual glucose-ketone (DGK) sensor and growing clinical consensus that elevated ketone levels are often present before severe hyperglycemia. At ADA 2025, CKM was discussed in multiple high-profile sessions, including two powerhouse symposia dedicated to DKA risk and DGK. Dr. Jennifer Sherr (Yale University) presented pivotal and feasibility data on Abbott’s DGK sensor, demonstrating strong alignment with blood beta-hydroxybutyrate reference values across insulin pump suspension studies in adults and children. Notably, Dr. Sherr illustrated multiple cases in which ketone levels rose rapidly well before glucose exceeded 250 mg/dL, underscoring the limitations of glucose-only monitoring. Dr. Lori Laffel (Joslin Diabetes Center) highlighted rising DKA hospitalization rates and reviewed RCT evidence showing that blood ketone testing reduced emergency assessments by nearly 50% compared to urine testing, arguing that CKM could enable even earlier intervention at scale.
- Complementing Abbott’s data, Dr. Ahmad Haider (McGill University) presented accuracy and feasibility results for SiBionics’ SiBio KS1 CKM. In adults with T1D using AID and undergoing ketogenic or intermittent fasting interventions, SiBio demonstrated “acceptable” accuracy versus capillary ketone testing. Results revealed that brief, asymptomatic elevations in ketones were relatively common, but brief. Dr. Haider emphasized that these findings support CKM’s role in acute risk detection and in improving understanding of real-world ketone dynamics during dietary variation.
- More recently at ATTD-Asia 2025, Prof. Thomas Danne (Breakthrough T1D) discussed the importance of CKM adoption, saying that no individual hospitalized with DKA should be discharged without access to dual glucose-ketone monitoring. Dr. Jennifer Ngan (University of Melbourne, Australia) presented early insights from the run-in phase of the Australian PARTNER trial using Abbott’s CKM technology in people with T1D without acute illness. Dr. Ngan reported that most participants maintained normal ketone levels (<0.6 mmol/L) over two weeks of observation, with hyperglycemia being a poor predictor of ketosis and a trend toward lower carbohydrate intake among those with elevated ketone levels. These findings reinforced the concept that glucose and ketone trends frequently intersect in real-world settings, strengthening the case for real-time dual-analyte monitoring capabilities to support proactive DKA prevention and safer adjunctive therapy use.
- Glucose range monitoring became a new regulatory category designed to broaden access to continuous monitoring by prioritizing simplicity for users. In September 2025, the FDA granted its first De Novo authorization for a Glucose Range Monitoring System (GRMS) to Biolinq for Biolinq Shine, formally separating range-based glucose feedback from traditional continuous glucose monitoring. Unlike filament-based CGMs, Biolinq Shine uses a needle-free, intradermal microsensor array placed in the papillary dermis and delivers semi-quantitative, real-time glucose ranges via a color-coded LED display directly on the patch: (i) blue for in Range (70–180 mg/dL); (ii) yellow for above Range; and (iii) red for below Range.
- At DTM 2025, Dr. Courtney Lias (FDA) highlighted Biolinq Shine’s authorization as a signal of FDA’s willingness to support novel device categories that deliver actionable insight without requiring numerical interpretation. Dr. Lias discussed how GRMS represents a regulatory shift toward expanding access and usability, complementing FDA’s momentum this year with expanded AID indications in T2D.
- CGM’s role in staging and monitoring of presymptomatic T1D was discussed. At ATTD-Asia 2025, Prof. Juliana Chan (Chinese University of Hong Kong) reinforced that while OGTT remains the diagnostic gold standard, CGM offers complementary biological insight, even among individuals classified as normoglycemic by fasting glucose or A1c. Prof. Chan emphasized that while CGM is not yet ready to replace OGTT as the standard, it may help refine staging when combined with factors such as biomarkers, genetic risk scores, and AI-driven insights.
- Building on this concept, Dr. Viral Shah (Indiana University) introduced the CGM Dynamic Index (CDI) as a novel metric designed to capture the frequency, amplitude, and velocity of glycemic transitions, which static metrics may miss. Presented in the context of early dysglycemia and stage 2 T1D, CDI is now being validated in a Breakthrough T1D-funded longitudinal study tracking progression from stage 1 and 2 to stage 3 T1D, with the goal of determining whether CGM-derived dynamics can predict progression more accurately than A1c or OGTT alone.
- At the population level, emerging longitudinal data further supported CGM’s potential role in early detection of T1D. A study from the Australian ENDIA cohort, led by Dr. Aveni Haynes (The Kids Research Institute Australia), showed that all children who progressed to clinical T1D had at least one blinded CGM session with time above 140 mg/dL >10% prior to diagnosis. In another perspective, a framework led by Prof. Nicholas Thomas (University of Exeter, UK) offered guidance for adults with islet autoantibody positivity, recommending A1c-led monitoring and selective CGM use in higher-risk or ambiguous cases, while warning that routine CGM may increase anxiety in lower-risk adults without clear clinical benefit. Collectively, these developments suggest that CGM is evolving into a contextual monitoring tool for presymptomatic T1D.
- Reflecting momentum from 2025 evidence and discussions, the 2026 ADA Standards of Care updated Recommendation 3.2 to state that CGM metrics may be considered alongside A1c and OGTT in individuals with presymptomatic T1D, representing a formal recognition of CGM as complementary monitoring tool.
9. Digital health funding stabilizes in 2025 as capital focuses on AI-driven and workflow-focused platforms
In the digital health landscape, 2025 marked a rebound in total capital but reinforced the sector’s shift toward fewer, larger, and more AI-centered deals. Rock Health reported $9.9 billion invested across 351 deals in the first nine months of 2025, up from the $8.4 billion and $8.5 billion by that time in 2024 and 2023, respectively, but still well below record-high investments in 2022 and 2021. Deal volume continued to decline, reflecting investor consolidation around later-stage companies with demonstrated revenue and clinical outcomes. The average deal size increased to $28.1 million, up from $20.4 million in 2024. Nineteen mega-deals of more than $100 million accounted for nearly 40% of all capital. Meanwhile, over one-third of financings were for unlabeled rounds, a sign that startups are increasingly relying on capital to meet challenging benchmarks before progressing to traditional series raises. These trends collectively point to a more selective and outcomes-driven funding environment where AI-enabled workflow automation and value-based care continue to attract the strongest investor demand.
- Workflow and AI-powered tools dominated funding themes, signaling a shift away from disease treatment-focused digital solutions. Clinical and nonclinical workflow tools consisted of a combined 42% of total 2025 funding, with workflow mega-deals alone raising over $2.2 billion. Annual population health management funding rose tenfold to $1 billion by 3Q25, reflecting renewed investor alignment with prevention, risk stratification, and value-based care. AI-enabled products continued to command deal premiums.
- M&A activity increased as startups expand horizontally across the care continuum. More than 160 acquisitions were recorded through 3Q25, already surpassing 2024’s total of 121. This consolidation was driven by tougher performance expectations from investors and a shift toward end-to-end platform strategies. Rock Health noted that many private companies are now pursuing mega-rounds as a precursor to eventual public market entry.
- Across diabetes and metabolic care in 2025, digital health companies secured important regulatory milestones, expanded virtual obesity-care platform, and introduced next-generation sensors.
- Omada Health strengthened its position in obesity and cardiometabolic care following its landmark initial public offering (IPO) in May. The company now reports 831,000 enrolled members (+53% from 3Q24) and $68 million in 3Q25 revenue (+49% from 3Q24). The company announced that its GLP-1 RA Care Track has expanded to include prescribing, an offering built on its “behavioral intelligence” from more than 100,000 GLP-1 RA users. New outcomes shared in 3Q25 showed that members who discontinued GLP-1 RA therapy but remained in Omada’s care platform maintained weight over 12 months, with 63% continuing to lose or maintain weight – much improved discontinuation outcomes compared to the ~11-12% weight regain typically seen in clinical trials.
- Signos received FDA clearance for its AI-driven weight-management platform integrating Dexcom’s over-the-counter (OTC) CGM Stelo with a real-time behavioral AI engine designed to guide lifestyle choices. The company is conducting a five-year clinical trial (NCT05121844) to study weight and glycemic outcomes among platform users, with estimated enrollment of over 30,000 people without diabetes. While reimbursement remains limited, Signos positioned its $129-139/month subscription as a more accessible alternative to GLP-1 RAs. Signos’ FDA clearance highlights the momentum behind CGM as a key tool of lifestyle management, both in consumer wellness and adjunct to therapeutic care for those with diabetes.
10. Data interoperability comes into focus as diabetes data continues to be incorporated into routine clinical workflows
Diabetes data interoperability made progress in 2025 as EHR integrations and clinical workflows began to align more closely, although gaps remain. At DTM and ISPAD, presenters emphasized that data democratization now depends more on public application programming interfaces (APIs) and policy alignment across systems. While initiatives like iCoDE-2 and expanded EHR integrations are building the foundation for more equitable access to diabetes data, experts cautioned that fragmented regulation and lagging consent frameworks continue to cause barriers for clinical impact.
- Data standardization and EHR integration advanced meaningfully, establishing a foundation for more equitable and efficient use of diabetes data in clinical practice.
- At DTM 2025, Dr. Juan Espinoza (Northwestern University) shared progress from the Integration of Connected Diabetes Device Data Into the Electronic Health Care #2 (iCoDE-2) initiative, which builds on iCoDE-1’s work with CGM to define a unified data model for insulin delivery across pumps, pens, and algorithms. The team developed an Insulin Dosing Profile (IDP) that presents 14 days of glucose metrics and insulin delivery data in a clinician-friendly EHR view. Dr. Espinoza plans to release the final iCoDE-2 report and a “public data dictionary” in 1Q26, which he described as a “living record” for insulin data standards that can be referenced by manufacturers and researchers.
- In contrast, Dr. Pietro Randine (UiT The Arctic University of Norway) discussed the technical and ethical constraints of data access within Europe’s fragmented landscape. Device contracts and data infrastructures vary by country and often by region, forcing clinicians to manually transcribe device data into EHRs and creating more room for error. Limited public APIs, reliance on DIY data extraction tools that may violate terms of service, and costly third-party intermediaries further constrain real-time access, particularly for patients with low digital literacy.
- At ISPAD, Mr. John Walsh (SweetSpot) highlighted that milestones such as Substitutable Medical Applications and Reusable Technologies (SMART) on Fast Healthcare Interoperability Resources (FHIR) and the FDA’s integrated CGM (iCGM) and alternate controller enabled (ACE) pump designations have fueled the development of diabetes technologies. However, he stressed that fundamental challenges remain, including the fact that data privacy and consent frameworks lag behind rapid advances in AI-driven decision support. Looking ahead, Mr. Walsh urged multidisciplinary collaboration to ensure interoperability is addressed as a priority as diabetes technology advances.
- Several data integrations were launched into clinical practice in 2025, including EHR-centered workflows. In April, Abbott announced that LibreView accounts can now link directly to Epic, bringing FreeStyle Libre data into the EHR alongside Dexcom G7 and Glooko streams. In parallel, Glooko’s US integration with FreeStyle Libre extended its platform to ~4.5 million Libre users, now serving over 90% of the US CGM market, allowing patients and providers to interpret Libre data in the context of various health factors. Oura, maker of the Oura Ring, saw two notable integrations of its continuous health metrics with diabetes data: it launched app integration with Stelo in May, and partnered with Tidepool in November to build a real-world dataset integrating their wearable and diabetes device data, ultimately aiming to accelerate research on the physiological and behavioral factors that influence glycemic outcomes in diabetes management.
- At DTM 2025, Dr. Juan Espinoza (Northwestern University) shared progress from the Integration of Connected Diabetes Device Data Into the Electronic Health Care #2 (iCoDE-2) initiative, which builds on iCoDE-1’s work with CGM to define a unified data model for insulin delivery across pumps, pens, and algorithms. The team developed an Insulin Dosing Profile (IDP) that presents 14 days of glucose metrics and insulin delivery data in a clinician-friendly EHR view. Dr. Espinoza plans to release the final iCoDE-2 report and a “public data dictionary” in 1Q26, which he described as a “living record” for insulin data standards that can be referenced by manufacturers and researchers.
Top Ten Most Read Closer Look Reports in Therapy
- Interview with Dexcom’s CEO Mr. Kevin Sayer on the launch of Stelo, T2D coverage, upcoming G8, and future of multi-analyte sensors – March 17, 2025 – Dynamic discussion explores product strategy and additional populations who could benefit from CGM
- Interview with Glooko’s leadership team on its acquisition of Monarch Medical and the integration of inpatient insulin dosing algorithm EndoTool – November 11, 2025 – On the Monarch Medical acquisition, CGM integration and care transition, EndoTool’s role in primary care and population health management, raising integration awareness among HCPs, and upcoming eCQM reporting requirements
- Dexcom announces FDA clearance of Dexcom G7 15 Day CGM for adults with diabetes – April 11, 2025 – Expected to launch in US in 2H25; Dexcom seeks to offer AID compatibility upon launch
- Biolinq receives FDA De Novo Classification for Biolinq Shine as Glucose Range Monitoring System: autonomous, needle-free CGM – September 25, 2025 – Patch-based CGM designed to support metabolic health for people with T2D not on insulin
- Interview with Biolinq CEO Mr. Rich Yang on Biolinq Shine, a patch-based CGM, and its FDA De Novo classification – November 14, 2025 – On FDA’s GRM category creation, Biolinq Shine’s indication, intradermal and semiconductor design with LED-screen dual display, access strategy, and multi-analyte platform roadmap
- Medtronic 1Q25 (F4Q25) – May 21, 2025 – Diabetes division will separate as standalone company under Diabetes President and EVP Ms. Que Dallara; worldwide Diabetes revenue of $728 million (+10); MiniMed 780G FDA submissions for T2D and ultra rapid-acting insulins
- Sequel announces US launch of twiist with Abbott’s FreeStyle Libre 3 Plus in 2Q25 – March 18, 2025 – The first FDA-cleared AID system with a Tidepool Loop-based algorithm will launch through the pharmacy channel for people with T1D aged six years and older
- Dexcom to lay off 350 employees as company sharpens R&D focus – August 28, 2025 – Layoffs primarily affect operations and manufacturing at its San Diego headquarters; company reports R&D capital allocation as goal
- Medtronic 4Q24 (F3Q25) – February 18, 2025 – Worldwide Diabetes revenue of $694 million (+8%; +10% operationally); Abbott-partnered CGM on track for FDA submission in 2H25; fifth consecutive quarter of double-digit Diabetes growth
- Abbott 2Q25 – July 17, 2025 – Diabetes Care revenue totals nearly $2 billion (+20%; +19% operationally); discussions on pump integrations with upcoming dual glucose ketone sensor
Most Unexpected News/Biggest Surprises
Glucose Monitoring
- Medtronic launches Instinct with MiniMed 780G in the US and extends rollout of Simplera Sync to additional European countries and the US
- Abbott targets 2026 launch of dual glucose-ketone sensor, with five AID companies (Sequel, Tandem, Beta Bionics, Ypsomed and CamDiab, and Insulet) confirming planned integrations upon launch
- Biolinq receives FDA De Novo Classification for Biolinq Shine as Glucose Range Monitoring System
- Mr. Jake Leach to succeed Mr. Kevin Sayer as CEO effective January 1, 2026, after 21 years at Dexcom
- Dexcom receives FDA clearance of Dexcom G7 15 Day CGM for adults with diabetes and launches the CGM on December 1
- Dexcom to discontinue Dexcom G6 sensor effective July 1, 2026
- Sequel Med Tech and Senseonics announce partnership to integrate Eversense 365 CGM with twiist
- Dexcom receives FDA warning letter for manufacturing and quality control issues
- Senseonics to take over commercialization of Eversense 365 from Ascensia
- OTC CGM expansions: Abbott Lingo goes brick-and-mortar, Lingo and Dexcom Stelo join Amazon
Insulin Delivery
- Medtronic announces MiniMed 780G CE-Mark for expanded use in T2D, pregnancy, and individuals aged 2+ years and FDA clearance for adults with T2D
- FDA clears Tandem’s Control-IQ+ for adults with T2D
- Diabetes division will separate as standalone company, MiniMed, under Diabetes President and EVP Ms. Que Dallara
- Sequel begins full rollout of twiist in the US
- Beta Bionics completes initial public offering
- CMS finalizes competitive bidding rule for diabetes devices in the DME channel, bundling CGMs, insulin pumps, and supplies into a monthly rental payment
- PK-PD glucagon “bridging” trial for Xeris’ glucagon for Beta Bionics’ bi-hormonal iLet validates safety and pharmacologic performance
- More companies enter the patch pump game, with ongoing development work from Medtronic, Beta Bionics, and Tandem
- Ypsomed Diabetes Care AG sold to TecMed as “mylife Diabetes Care AG”
- FDA clears Tandem’s SteadiSet for up to seven days of use, with US launch slated for 2026
- FDA accepts pediatric supplemental Biologics License Application for Afrezza, MannKind shares 52-week INHALE-1 data
Digital Health
- Glooko acquires Monarch Medical, expanding connected diabetes platform with inpatient insulin dosing algorithms
- Virta joins 60 healthcare technology organizations in CMS’s “Health Tech Ecosystem Initiative” aimed at making digital health tools user-friendly to patients and providers
Diabetes Therapy
Key Questions for 2026
Incretins
- Might we see competitive challenges to the Novo Nordisk and Lilly duopoly on incretin therapies in 2026?
- How will generic launches impact the pricing of branded incretin therapies, and will MFN pricing remain the standard globally?
- How will the major GI side effects consistent across the class be addressed to reduce discontinuation rates?
- How might patient segmentation come into play as oral incretins begin to receive approval?
- How might we see increased uptake of incretin therapies in children as more data becomes available?
- Will we see broader indications for these therapies in 2026, such as T1D or other complication reductions?
SGLT Inhibitors
- How might dual-glucose-ketone monitoring affect the use of SGLT-2 inhibitors in people with T1D?
- What additional safety protocols could the FDA require for Lexicon’s resubmission of Zynquista for T1D and CKD?
- How might Medicare Drug Price Negotiation Program’s (MDPNP) negotiated price of Farxiga and Jardiance, which take effect on January 1, 2026, affect the systems cost? How might it affect out-of-pocket costs for patients?
- Will lower costs of SGLT-2 inhibitors in MDPNP encourage the field to move toward earlier use of SGLT-2 inhibitors in a general population with T2D?
T1D
- What lessons from the discontinuation of VX-264 will shape future encapsulation or immune-evasion strategies for stem cell-derived islet programs across the field?
- Could immune invisibility (e.g. Sana Biotechnology’s hypoimmune gene-edited islets) interfere with normal, physiological clearance of dysfunctional β-cells, leading to long-term graft dysfunction?
- How will regulators approach and evaluate risk for gene-edited hypoimmune cells, particularly with respect to longer-term oncogenic risk and the potential for off-target gene editing?
Complications
- What clinical education is required meaningfully shift away from opioids toward newer mechanisms, like NaV1.8 inhibitors?
- What patient subgroups (severity, duration of DPN, and comorbidities) will derive the greatest benefit from Lexicon’s pilavapadin?
- Could limb outcomes become a required endpoint in future CVOTs for therapies in obesity and metabolic disease?
- How will regulators and payers value functional endpoints (e.g. walking distance) versus hard limb events?
Insulin
- With the resubmission of its BLA, will Novo Nordisk’s Awiqli receive approval in the US in 2026?
- How will the approval of Sanofi’s Merilog, as the first rapid‑acting biosimilar to NovoLog, impact Novo Nordisk’s sales?
- How might the cap on insulin at $35/month for all patients in the US, effective January 2026, improve patient compliance, and what metrics might be used to measure this?
- Might we see approval of IcoSema in the EU in 2026?
- How will the increasing uptake of incretin therapy impact insulin use?
What’s Coming in 2026?
Incretins and weight loss
Altimmune
- Phase 3 trial evaluating pemvidutide (dual GLP-1/glucagon RA) for MASH with F2 or F3 fibrosis is expected in 2026, following the phase 2b IMPACT trial (n=212) and an end-of-phase 2 meeting with the FDA in 4Q25.
AZ
- Data for phase 2b VISTA (n=304) and SOLSTICE trials (n=406) evaluating AZD5004 (oral GLP-1 RA) for obesity or overweight are expected in 1H26. The therapy is expected to enter phase 3 trials pending this data.
- Data from phase 2b APRICUS (n=262) and phase 2 ARAY trials (n=64) evaluating AZD6234 (long-acting amylin analog) for obesity are expected in 1H26.
- Results for phase 2b ASCEND trial (n=360) of AZD9550 (dual GLP-1/glucagon RA) in combination with AZD6234 for adults with obesity or overweight with at least one weight-related comorbidity are expected in 2H26.
Lexicon
- IND filing for LX9851 (oral ACSL5 inhibitor) in obesity expected by the end of 2025 under its license agreement with Novo Nordisk.
Lilly
- Filing for the MACE indication of tirzepatide is expected by the end of 2025, based on full results from the SURPASS-CVOT.
- Initiation of global regulatory filings of orforglipron for the obesity indication, upon the completion of the ATTAIN-2 trial, and the launch pending approval is expected in 2026.
- Up to six phase 3 results for retatrutide (triple GLP-1/GIP/glucagon RA) will be available by 2026.
- Lilly has agreed to the Most-Favored-Nation Pricing to offer tirzepatide and orforglipron at discounted prices.
Merck
- Efinopegdutide (GLP-1/glucagon receptor co-agonist MK-6024) continues to be evaluated in phase 2b (n=360) for MASH, with completion expected by the end of 2025.
Novo Nordisk
- Novo Nordisk expects a regulatory decision for semaglutide 7.2 mg in early 2026 and approval of semaglutide 7.2 mg in a single-dose pen in 2H26.
- Novo Nordisk has agreed to the “maximum fair prices” (MFPs) set by the US Inflation Reduction Act for three of its semaglutide medicines – Ozempic, Rybelsus, and Wegovy – which will take effect under Medicare Part D in 2027.
- Novo Nordisk has agreed to the Most-Favored-Nation Pricing to offer semaglutide at discounted prices.
- Novo Nordisk plans to initiate a phase 3 program for once-weekly subcutaneous and once-daily oral amycretin for people with T2D in 2026 to evaluate amycretin in adults with T2D.
- Phase 3 trial evaluating CagriSema in children with obesity or who are overweight is set to begin in January 2026 and is estimated to complete in September 2033.
Regeneron
- Phase 2 study of once-daily oral GIPR antagonist, PF-07976016, expected December 2025.
Roche
- Phase 3 trials of CT-388 (once-weekly dual GLP-1/GIP RA) for obesity with (n=360) or without T2D (n=450) is expected to initiate in 1H26.
- A phase 2 trial (n=340) of CT-996 (once-daily oral GLP-1 RA) is expected to complete in July 2026.
Viking
- IND filing for dual amylin and calcitonin receptor agonist (DARCA) is planned for 1Q26.
- Phase 3 VANQUISH-1 (n=4,500) and VANQUISH-2 (n=1,100) trials for subcutaneous VK2735 (dual GLP-1/GIP RA) in obesity and T2D are expected to be completed in mid 2027.
Zealand
- A phase 2 trial for a fixed-dose combination of petrelintide and Roche’s dual GLP-1/GIP RA, CT-388, is on track to initiate in 1H26.
- Topline results of the phase 3 SYNCRHONIZE-1 (n=727) and SYNCHRONIZE-2 trials (n=756) of BI/Zealand’s survodutide (dual glucagon/GLP-1 RA) for people with overweight or obesity without or with T2D, respectively, are expected in 1H26. The trials are expected to complete in February and April 2026.
- SYNCHRONIZE-CN trial (n=307) evaluating survodutide in people with obesity in China is expected to complete in 1Q26.
SGLT Inhibitors
AstraZeneca
- Farxiga is being investigated as a combination therapy with baxdrostat (highly selective aldosterone synthase inhibitor), balcinrenone (nonsteroidal mineralocorticoid receptor modulator), and zibotentan (endothelin A receptor blocker) in phase 3 trials.
- Medicare Drug Price Negotiation Program’s negotiated price of Farxiga $178.50 for a monthly supply, down 68% from $556 Farxiga, will take effect on January 1, 2026.
BI/Lilly
- Medicare Drug Price Negotiation Program’s negotiated price of Jardiance, down 66% from $573 to $197, will take effect on January 1, 2026.
T1D
Advant Technologies + SGAustria
- Preclinical development of encapsulated stem cell-based therapies for T1D and insulin-dependent T2D is expected to continue in 2026.
Century Therapeutics
- IND-enabling studies for CNTY-813 are expected to complete by year-end (2025), with a regulatory IND submission targeted for 2026.
Sana Biotechnology
- Advancement of the hypoimmune pancreatic islet (HIP) platform into its SC451 program. Clinical follow-up is expected to continue in 2026 following first-in-human proof-of-concept data generated in 2025.
Eldeon Pharmaceuticals
- Ongoing clinical evaluation of tegoprubart in people with T1D undergoing islet transplantation is expected to continue in 2026 following encouraging early insulin-independence data.
Pluristyx
- Pluristyx will continue preclinical development of its immune-cloaked, safety switch-enabled iPSC line for T1D through its collaboration with Breakthrough T1D in 2026.
Vertex
- Regulatory submission for zimislecel (VX-880) is planned for 2026 following completion of enrollment in the phase 1/2/3 FORWARD study (n=52) and ongoing manufacturing analyses.
- Dosing in the phase 3 portion of the study is ongoing.
Sernova
- The last cohort in Sernova’s phase 1/2 trial evaluating the Cell Pouch system in people with T1D is expected to initiate by the end of 2025, with clinical data expected in 2026.
Insulin
Lilly
- With regulatory submission of once-weekly insulin efsitora alfa for T2D in 3Q25, FDA decision may be shared next year.
Novo Nordisk
- FDA decision for Awiqli (once-weekly insulin icodec) in T2D may be shared next year, given that Novo Nordisk resubmitted the application in September 2025.
- Fiasp and NovoLog were selected for the first cycle of the US Medicare Drug Price Negotiation Program (MDPNP), with discounted prices (down 75% to $199/month), which will take effect on January 1, 2026.
Complications
Vertex
- Commercial launch and market expansion of Journavx (suzetrigine) are expected to continue in 2026 following FDA approval in 2025.
Lexicon
- Initiation of phase 3 trials for pilavapadin (LX9211) in diabetic neuropathic pain (DPN) is planned for 2026, following an end-of-phase 2 feedback meeting (expected early next year).
Novo Nordisk
- Additional analyses of SOUL, FLOW, and STRIDE trial data for rybelsus (semaglutide) supporting reduced major adverse limb events with oral semaglutide are expected to continue in 2026.
Bayer
- The phase 3 REDEFINE-HF trial (n=5,200) evaluating finerenone in patients with acute decompensated HF and HFmrEF/HFpEF is expected to complete in April 2026.
- The phase 3 CONFIRMATION-HF trial (n=1,500) assessing finerenone in combination with SGLT-2 inhibitors in hospitalized HF patients is expected to complete in August 2026.
- The phase 3 FIND-CKD trial (n=1584) evaluating finerenone in people with CKD without diabetes is estimated to complete in February 2026.
Lupin
- Lupin holds FDA tentative approvals for generic dapagliflozin and generic canagliflozin, positioning the company to launch these products as patent and exclusivity barriers lift.
Themes
1. Incretin-based therapies: New indications and outcomes trial in the heart, kidneys, liver, and limbs
In 2025, incretin therapies continued to dominate headlines, reshape treatment protocols, and expand into new indications. The year was marked by both regulatory successes and increased accessibility, particularly given expanding indications for a class of medication that has taken the obesity landscape by storm.
- This year, incretin therapies continued to demonstrate benefits beyond glycemic health. Novo Nordisk’s Ozempic (semaglutide) secured new approvals across three major indications. In the US and Canada, semaglutide was approved for risk reduction in kidney disease progression, kidney failure, and cardiovascular death in adults with T2D and CKD. The approval was based on the phase 3 FLOW trial (n=3,533), which showed a 24% reduction in primary kidney disease events. In June 2025, Ozempic was granted an expanded label in the EU based on the phase 3b STRIDE trial (n=792), which demonstrated a 21% improvement in walking distance and a 54% reduction in the composite of rescue therapy, major adverse limb events, or mortality. In August 2025, Novo Nordisk’s Wegovy (semaglutide) was approved in the US for MASH in adults with moderate to advanced fibrosis based on Part 1 of the phase 3 ESSENCE trial (n=1,200), which showed 63% resolution of steatohepatitis without worsening fibrosis and 37% improvement in fibrosis without worsening steatohepatitis, compared to 34% and 23% with placebo, respectively.
- While not approved yet for CV risk reduction, Lilly’s Mounjaro (tirzepatide) delivered compelling results in the landmark phase 3 SURPASS-CVOT (n=13,299). In this head-to-head comparison with dulaglutide, tirzepatide conferred a significant 16% reduction in all-cause mortality, nonsignificant 12% weight loss (vs. 5%), and a significant 1.7 percentage point A1c reduction (vs. 0.9 percentage point). In people with CKD, tirzepatide slowed eGFR decline by 3.54 mL/min/1.73 m² compared to dulaglutide, further supporting its potential as a cardiorenal and metabolic therapy.
- On the access front, the expiration of liraglutide patents in major markets catalyzed a wave of generic launches. Teva, Lupin, Biocon, and Meitheal all entered the market with liraglutide generics, some priced up to 70% lower than branded versions. Moreover, in Canada, semaglutide is set to become generic in January 2026 following a patent lapse due to non-payment. Sandoz and Apotex plan to launch generic semaglutide in 2026. Likewise, Hims&Hers announced plans to enter the Canadian market with discounted generic semaglutide following the termination of its partnership with Novo Nordisk to sell discounted cash-price Wegovy in the US. These developments reflect growing momentum toward lower-cost incretin therapies across geographies and distribution models. We’re watching closely how these generics may impact pricing and access. In addition to generic launches, the US government has reached agreements with Lilly and Novo Nordisk to lower the cost of GLP-1 RAs.Read more about the Most-Favored-Nation (MFN) pricing negotiations and the Centers for Medicare and Medicaid Services’ (CMS) Medicare Drug Price Negotiation Program (MDPNP) in the big picture theme.
2. Expanding competitive landscape for oral GLP-1 RAs and multi-incretins for T2D
2025 marked a dynamic year for oral incretin therapies, with major phase 3 readouts, regulatory approvals, and program discontinuations. We are encouraged by the continued advancement of oral incretins as they can expand access, simplify manufacturing, and reduce treatment burdens.
- For cardiovascular protection, Novo Nordisk’s Rybelsus (oral semaglutide) was approved in both the US and EU for reducing major adverse cardiovascular events (MACE) in adults with T2D and high cardiovascular risk. These approvals were based on the phase 3b SOUL trial (n=9,650), which demonstrated a 14% reduction in MACE compared to placebo.
- Lilly’s orforglipron (oral GLP-1 RA) demonstrated superiority to multiple comparators across three phase 3 trials in people with T2D. In ACHIEVE-2 (n=888), orforglipron (36 mg) reduced A1c by 1.7 percentage points vs. 0.8% with dapagliflozin in people with T2D and inadequate glycemic control on metformin. In ACHIEVE-5 (n=520), orforglipron reduced A1c by up to 2.1 percentage points vs. 0.8 percentage point with placebo in people with inadequately managed T2D on insulin glargine. In ACHIEVE-3 (n=1,698), orforglipron conferred 9.2% weight loss vs. 5.3% with oral semaglutide, and 37.1% of participants on the highest dose achieved A1c <5.7%, compared to 12.5% in the oral semaglutide group. Moreover, in the ATTAIN-2 trial (n=1,500) presented at ObesityWeek 2025, orforglipron conferred up to 11% weight loss vs. 2% with placebo and 1.8 percentage point reduction in A1c vs. 0.1 percentage point with placebo in adults with overweight or obesity and T2D. Notably, 75% of participants on the highest dose achieved an A1c ≤6.5%, reinforcing orforglipron’s potential as a foundational therapy for diabetes.
- While we were excited about the therapeutic potential of Pfizer’s danuglipron (oral GLP-1 RA), the company discontinued development of this program in April 2025. The decision followed a case of potential drug-induced liver injury and high rates of GI-related adverse events in earlier trials. As background, in a phase 2b trial (n=628), twice-daily danuglipron conferred up to 13% weight loss, but discontinuation rates exceeded 50% across all doses. Nonetheless, we are excited for the continued development in oral incretin therapies, including AstraZeneca’s oral GLP-1 RA AZD 5004 and Viking’s oral VK2735 (dual GLP-1/GIP RA) in phase 2.
- Dual incretins continued to gain momentum, with Innovent’s dual GLP-1/glucagon RA mazdutide receiving approval from China’s regulatory agency for glycemic management in T2D based on the phase 3 DREAMS-1 (n=320) and DREAMS-2 (n=731) results. More recently, mazdutide 9 mg conferred a 19% weight loss in the GLORY-2 trial (n=462), with nearly half of participants achieving ≥20% weight loss. Based on the results, China’s National Medical Products Administration (NMPA) accepted Innovent’s supplementary application for the 9 mg dose. Meanwhile, Novo Nordisk’s CagriSema (fixed-dose cagrilintide + semaglutide) conferred a 13.7% weight loss in people with overweight or obesity, compared with 3.4% with placebo, in the phase 3 REDEFINE-2 trial (n=1,206).
3. Toward the holy grail: Advances in cell replacement therapies for T1D
Therapeutic landscape for cell replacement therapies for T1D continued to evolve in 2025, with progress spanning stem cell-derived islets, hypoimmune platforms, and immunosuppressants. Vertex remained a central leader in the cell therapy space with its zimislecel program in the phase 1/2/3 trial, while Sana Biotechnology, Adocia, and others advanced early clinical- and preclinical-stage candidates.
- Vertex offered substantial updates across its T1D cell therapy programs this year. Zimislecel (VX-880), a stem cell-derived islet with standard immunosuppression, continues to be evaluated in the pivotal phase 1/2/3 FORWARD study (n=52), which completed enrollment in 3Q25. Vertex has postponed dosing completion in the phase 3 portion of the study to conduct an “internal manufacturing analysis,” but regulatory submission remains planned for 2026.
- At ADA 2025, Vertex presented one-year follow-up data from the FORWARD phase 1/2 study, following interim data presented at EASD 2024. Of the 12 participants who received full dose therapy, none experienced severe hypoglycemic events between Days 90 and 365, and all achieved an A1c of <7% or a ≥1% reduction from baseline, meeting the primary endpoint. Moreover, 10 of 12 achieved insulin independence. The remaining two had 70% and 36% reductions in daily insulin requirements.
- Separately, in March 2025, Vertex discontinued VX-264, a stem cell-derived islets encapsulated in an immune-evasive device, after Parts A and B of the phase 1/2 study (n=17) failed to demonstrate clinically meaningful increase in C-peptide. Based on the data, Vertex decided not to launch the Part C of the trial.
- Also in cell therapy, at ADA 2025, Sana Biotechnology presented six-month results from the first human transplant of gene-edited hypoimmune pancreatic islet (HIP) cells in a person with longstanding T1D. As background, HIP cells incorporate HLA-I/II knockout and CD47 overexpression to evade immune detection without immunosuppression. The trial demonstrated rapid C-peptide restoration by Week 4 and sustained responses through Week 26. MRI and PET-MRI confirmed viable grafts with no inflammation, and no safety concerns were reported. Sana Biotechnology will incorporate the HIP platform into SC451, a stem cell-derived islet therapy in development as a one-time treatment for T1D without insulin or immunosuppression.
- Beyond Vertex and Sana, early-stage cell therapy efforts are broadening.
- On encapsulation and scaffolding, Adocia reported encouraging in vivo results for AdoShell, its immune-evasive scaffold for stem cell-derived islets, at ADA 2025. In preclinical models, islets encapsulated with AdoShell showed an increase in human C-peptide secretion over three months and a three-fold increase in insulin secretion after explant. In vitro, encapsulated islets retained viability, functionality, and insulin secretion comparable to non-encapsulated islets. Adocia originally announced plans for a first-in-human submission by 2H25, but recent updates have extended this goal to 3Q26.
- Seattle-based Pluristyx and Breakthrough T1D announced a collaboration to develop an “immune-cloaked” and “safety switch-enabled” induced pluripotent stem cell (iPSC) line that would not require chronic immunosuppression.
- Philadelphia-based Century Therapeutics launched CNTY-813, an iPSC-derived ß-cell islet program, using the company’s Allo-Evasion 5.0 technology. Preclinical data conferred rapid, sustained glucose normalization and glucose-responsive insulin secretion with CNTY-813 therapy. IND-enabling studies are planned by year-end with an IND targeted for 2026.
- Las Vegas-based Avant Technologies and Singapore-based SGAustria announced a joint venture to develop encapsulated stem cell-based therapies for T1D and insulin-dependent T2D, combining Avant’s expertise in cell-line engineering and SGAustria’s in encapsulation technology.
- On immunosuppression, Eledon Pharmaceuticals is developing tegoprubart, an anti-CD40L antibody, as a less toxic immunosuppressive therapy for people with T1D who undergo islet transplantation. Early data showed insulin independence in all six subjects three to 12 months post-treatment, with A1c values ranging from 4.7% to 6.0%.
- Finally, funding for T1D programs continued to expand. In October 2025, Breakthrough T1D’s venture arm, the T1D Fund, launched a $150 million fundraising campaign to bolster its investment capacity and accelerate high-potential therapies. The campaign has already secured $60 million toward its goal.
4. Momentum continues for disease-modifying therapies in T1D
In 2025, disease-modifying therapies advanced significantly, led by new updates on Sanofi’s Tzield (teplizumab). Following FDA approval in November 2022 for people with stage 2 T1D, Sanofi secured approvals in other countries, including Canada, China, and the UK. Most recently, in November 2025, Sanofi received a positive CHMP opinion recommending EU approval of teplizumab (Teizeild) for stage 2 T1D. In the US, teplizumab received the FDA’s new Commissioner’s National Priority Voucher for a potential indication of preserving beta cell function in people with recent onset stage 3 T1D. With the expedited review process, the regulatory decision is now expected in 1H26. The application for stage 3 T1D is based on the PROTECT (n=328) trial, in which Tzield demonstrated beta-cell function preservation in children and adolescents with recent onset T1D. A post hoc analysis of this study, presented at ATTD 2025, further found that teplizumab conferred meaningful improvements in TIR (+1.6 hours/day), lowered hyperglycemia incidence, and decreased insulin use compared to placebo.
- In the pipeline, companies continued to invest in novel mechanisms.SAB Biotherapeutics raised $175 million to support the phase 2b SAFEGUARD trial (n=142) of SAB-142, a human anti-thymocyte immunoglobulin (hIgG), following positive phase 1 results. Cambridge, MA-based Zag Bio launched with $80 million in financing to advance ZAG-101, a bifunctional antibody designed to induce central immune tolerance by presenting beta-cell antigens to the thymus. Chicago-based COUR Pharma began dosing in its phase 1b/2a trial of CNP-103 (n=72), a tolerogenic nanoparticle therapy for stages 1, 2, and 3 T1D.
- Existing treatments, like verapamil (for angina pectoris and cardiac arrhythmias) and baricitinib (indicated for autoimmune diseases like rheumatoid arthritis), are also evaluated for potential benefits on C-peptide preservation. As presented at EASD 2025, the phase 2 MELD-ATG trial (n=117) confirmed that low-dose ATG (0.5 mg/kg) significantly preserved C-peptide in young people with new-onset T1D, establishing a minimum effective dose with improved tolerability. The Ver-A-T1D trial (n=136) of verapamil did not meet its primary endpoint, though C-peptide remained higher with treatment. Two-year outcomes from the BANDIT trial (n=91) showed that baricitinib significantly preserved C-peptide during the treatment phase but not beyond, with similar patterns observed for insulin requirements.
5. Meeting the unmet needs in T1D: Finerenone, GLP-1 RAs, and SGLT inhibitors as adjunctive therapies to insulin
In 2025, the field continued to push for adjunctive therapies in T1D to reduce the burden of cardiovascular (CV) and renal complications. As we heard at ADA 2025, people with T1D – including those with well-managed diabetes – face a two- to four-fold increased risk for CV disease compared to those without T1D. Yet, insulin remains the only approved therapy, with adjunctive medications limited to amylin analog Symlin (pramlintide) approved in 2004. To address this therapeutic gap, nonsteroidal mineralocorticoid receptor antagonist (nsMRA) finerenone, GLP-1 RAs, and SGLT inhibitors have been evaluated as add-on therapies to insulin.
- In the landmark phase 3 FINE-ONE trial (n=241), finerenone significantly reduced uACR (urine albumin-to-creatinine ratio) by 25% in people with T1D and chronic kidney disease (CKD) at six months. This benefit was consistent across all prespecified subgroups, including age and sex. On safety, treatment-emergent adverse event rates were comparable between treatment and control groups. Consistent with previous trials, finerenone led to higher rates of hyperkalemia (high blood potassium level; 10%; n=12) than placebo (3%; n=4), but its clinical impact was limited. In Bayer’s 3Q25 call, management commented that finerenone is the first therapy in 30 years to demonstrate positive results in addressing CKD in this population. Given that ~27% of people with T1D have CKD, we are encouraged that an effective and safe medication may soon become available for this population. As background, Kerendia (finerenone) was approved for CKD in people with T2D in 2021 and heart failure with preserved (HFpEF) and mildly reduced ejection fraction (HFmrEF) in July 2025.
- In the phase 2 TIRTLE1 trial (n=24), tirzepatide reduced body weight by 9% and insulin dose by 33% in adults with T1D and obesity (BMI ≥30 kg/m2) at Week 12. Tirzepatide also reduced A1c by 0.5 percentage point from a baseline of 7.3% (vs. 0.2 percentage point with placebo; p=0.05), and numerically improved Time in Range (TIR) and Time below Range (TBR, p=0.17). Notably, tirzepatide led to a 25% reduction in basal insulin dose (p=0.002) and 49% reduction in bolus insulin dose (p=0.008), compared to placebo. Given the positive results, Lilly launched a phase 3 trial (n=905) for people with T1D and obesity, with completion expected May 2027. Separately, Roche also announced in 3Q25 that it will advance CT-868 (once-daily dual GLP-1/GIP RA) to phase 3 for people with T1D and BMI ≥25 kg/m2. The decision is based on the recently completed 16-week phase 2 trial (n=111), the results of which are expected in 2026. The phase 3 trial is expected to launch in 2026. We are encouraged by these advancements, especially given that two-thirds of adults with T1D live with overweight or obesity, and insulin therapy is linked to increased risk of weight gain.
- SGLT inhibitors continue to be considered for use in T1D. Although off-label SGLT-2 inhibitor use in people with T1D has increased from 0.1% in 2010 to 2.4% in 2023 for its known cardiorenal protection, its use is also associated with 3.2x greater diabetic ketoacidosis (DKA) risk in people with T1D. Despite the increased risk, most people with diabetes do not regularly test ketones: urine testing remains common, though less reliable, than blood measurement, and many rely on persistent, CGM-detected hyperglycemia alone to trigger ketone checks. Furthermore, an alarming proportion of patients with diabetes remain unaware of DKA symptoms and are unprepared for emergencies consistent with guidelines. Technological advancements toward dual glucose ketone (DGK) monitoring offer promise for safer SGLT inhibitor use in people with T1D. At EASD 2025, Dr. Richard Bergenstal (International Diabetes Center) said that DGK monitoring has could reduce DKA by providing real-time ketone data, integrating alerts, and supporting early intervention.
- On pharmacologic advancements, Lexicon submitted additional clinical data to the FDA in September 2025, which would support plans to resubmit the New Drug Application (NDA) for Zynquista (sotagliflozin), an oral dual SGLT-1/SGLT-2 inhibitor, for T1D and CKD. New data includes results from three ongoing trials designed to offer more insights into DKA rates, mitigation strategies, and renal outcomes. Lexicon expects feedback from the FDA in 4Q25. As background, in November 2024, Lexicon received a “deficiencies preclude discussion letter” from the FDA regarding the company’s NDA resubmitted in July 2024 for Zynquista. This letter followed an 11:3 vote against Zynquista’s benefit-to-risk profile at the EMDAC meeting in October 2024, which noted insufficient evidence that Zynquista’s benefits of A1c reduction outweighed the risk of DKA.
6. Once‑weekly insulin moves closer to market with robust phase 3 data
This year marked significant progress in insulin therapy with updates in innovation, biosimilars, and affordability. Once‑weekly insulin advanced meaningfully, with Novo Nordisk resubmitting its Biologics License Application (BLA) to the FDA for Awiqli (icodec) in T2D in September 2025, following a Complete Response Letter (CRL) issued in July 2024 that requested additional information on manufacturing processes and T1D indication. Novo Nordisk did not pursue a T1D indication in its resubmission due to increased rates of hypoglycemia. Awiqli has already been approved in the EU, Japan, and China. Across six trials in the phase 3 ONWARDS program, Awiqli demonstrated noninferior A1c reductions compared to insulin glargine or insulin degludec, with favorable safety profile in T2D. Meanwhile, Lilly advanced its once-weekly insulin efsitora alfa through the phase 3 QWINT program, announcing full results of QWINT-1, 3, and 4 at ADA 2025. Efsitora alfa demonstrated non-inferior A1c reduction compared to insulin glargine and insulin degludec in people with T2D on different insulin requirements (initiating basal insulin, already on basal insulin, and basal-bolus insulin, respectively). Results from the QWINT- 2 and 5 trials announced EASD 2024 similarly found non-inferior A1c reduction compared to insulin degludec in people with insulin-naïve T2D and T1D, respectively. However, in people with T1D, insulin efsitora alfa caused higher rates of hypoglycemia. In 3Q25, Lilly submitted for regulatory approval for T2D in the US. These candidates have the potential to reduce injection burden and expand adoption in primary care.
- On combination therapy, IcoSema (once-weekly icodec + semaglutide) demonstrated non‑inferior glycemic control, superior weight loss, and fewer hypoglycemic events compared to basal‑bolus therapy in the phase 3a COMBINE‑3 trial (n=679). Importantly, patient satisfaction scores were higher, compared to those on basal-bolus therapy.
- Ultra‑rapid insulin innovation continued with Adocia and Tonghua Dongbao’s BioChaperone Lispro, which met its primary endpoint of non‑inferiority in A1c reduction when compared with Humalog in a phase 3 trial (n=1,040) in China. The candidate also reduced postprandial glucose excursions and improved daily mean glucose, with comparable safety.
- Alternative forms of insulin, including inhaled and oral insulin, also gained new momentum. MannKind’s Afrezza received FDA acceptance for a pediatric indication. The supplemental Biologics License Application (sBLA) was supported by the phase 3 INHALE‑1 trial (n=230) results, where Afrezza, in combination with basal insulin, showed comparable efficacy and safety to MDI in youth with T1D and T2D. The PDUFA is set for May 2026, and has the potential to expand insulin options for children and adolescents if approved. Meanwhile, in October 2025, Oramed launched a US‑based trial of ORMD‑0801 (oral insulin) in people with T2D, focusing on the high-responder subgroup identified from Oramed’s previous phase 3 trial (n=346).
On the biosimilar and accessibility front, several rapid‑acting biosimilars were approved this year. In February 2025, Sanofi’s Merilog (insulin aspart-szjj) became the first FDA‑approved rapid‑acting biosimilar to NovoLog. In July 2025, Biocon’s Kirsty (insulin aspart-xjhz) was approved as the first and only interchangeable biosimilar to NovoLog. This momentum follows previous years, when Semglee (glargine‑yfgn) and Rezvoglar (glargine‑aglr) were approved as interchangeable biosimilars for Lantus (basal insulin glargine). We are hopeful that these approvals of biosimilar products may promote greater competition in the insulin market and expand access for patients.
- The insulin market also reached several affordability milestones this year. In September 2025, Sanofi expanded its Valyou Savings Program to cap all insulins at $35/month for all patients, regardless of insurance status, starting January 2026. Moreover, in October 2025, Biocon partnered with Utah-based nonprofit Civica Rx and California’s CalRx initiative to launch insulin glargine‑yfgn in the US at $45 for a box of five pens nationwide. Under CalRx, California residents will pay just $11 per pen.
7. SGLT-2 inhibitors and finerenone as foundational therapies for T2D and comorbidities; new cohorts of interest expanding potential indications
Finerenone, a nonsteroidal mineralocorticoid receptor antagonist (nsMRA), formerly approved for CKD in T2D under the brand name Kerendia, had a landmark year with major regulatory and clinical developments. In July 2025, the FDA expanded Kerendia’s indication to include heart failure with mildly reduced (HFmrEF) and preserved ejection fraction (HFpEF), following a Priority Review Designation issued in March. The decision was supported by the phase 3 FINEARTS-HF trial (n=6,001), in which finerenone demonstrated a 16% risk reduction in the composite endpoint of total heart failure (HF) events and cardiovascular death over 2.5 years.
- Momentum for finerenone in heart failure is progressing through Bayer’s MOONRAKER program (n>15,000), which features three ongoing phase 3 trials across the HF spectrum:
- The phase 3 REDEFINE-HF trial (n=5,200) is investigating finerenone for patients with acute decompensated HF and HFmrEF/HFpEF, and is expected to complete in April 2026.
- The phase 3 CONFIRMATION-HF trial (n=1,500) is assessing a combination therapy of finerenone and SGLT-2 inhibitors in patients hospitalized with HF. The trial is expected to complete in August 2026.
- The phase 3 FINALITY-HF trial (n=2,600) is studying finerenone in patients with HFrEF who are unable to tolerate steroidal MRAs. The trial is expected conclude in April 2028.
- Beyond HF, finerenone is evaluated in various understudied populations, including: (i) people using SGLT-2 inhibitors; (ii) children; (iii) people with T1D; and (iv) people without diabetes. In the phase 2 CONFIDENCE trial (n=800), simultaneous initiation of GLP-1 RAs and SGLT-2 inhibitors was associated with ~30% greater reduction in uACR than either therapy in isolation in T2D and CKD. The results demonstrate the early and additive benefits of finerenone in kidney health and support combination therapy for maximal risk reduction, as included in the new ADA Standards of Care 2026.
- Another landmark study was the phase 3 FINE-ONE trial (n=220), which found that finerenone significantly reduced uACR by 25% at six months in people with T1D and CKD. The potential impact of this study is great, as people with T1D and CKD have been limited to intensive glycemic management and RAAS inhibitors for over three decades.
- Other ongoing studies of finerenone include: (i) the phase 3 FIND-CKD trial (n=1,584) investigating finerenone in people with CKD without diabetes; (ii) the phase 3 FIONA trial (n=219) evaluating finerenone and an ACEi/ARB in children with CKD and proteinuria; and (iii) the phase 3 FIONA OLE trial (n=100), which is an 18-month open-label extension study of FIONA.
SGLT-2 inhibitors continue to be central to the management of T2D, CKD, and heart failure. Over the years, ADA and KDIGO guidelines have increasingly positioned SGLT-2 inhibitors as a first-line therapy. For example, the ADA Standards of Care 2026 recommends early SGLT-2 inhibitor use in people with T2D and HF or CKD. In the UK, the NICE draft guidance recommends SGLT-2 inhibitors as a first-line therapy with or without metformin for the general population with T2D; this change would save nearly 22,000 lives if 90% of the patient population takes the dual therapy. Despite abundant evidence and guidelines, real-world uptake of SGLT-2 inhibitor remains low, underscoring the importance of greater access and accessibility.
- SGLT-2 inhibitors will begin to go generic over the next few years. AZ’s Farxiga (dapagliflozin) lost exclusivity for its glycemic management indication in people with T2D in October, although its method-of-use patents related to CKD extend to 2029. Jardiance’s compound patent will expire in 2029 in the US and Europe and 2030 in Japan. Merck’s Steglatro (ertugliflozin) patents will expire in 2030 in the US and 2029 in the EU, China, and Japan. The FDA tentatively approved generic versions of two SGLT-2 inhibitors developed by Mumbai-based Lupin, dapagliflozin and canagliflozin, in November 2023. Lupin is expected to launch both in as patent protections lift.
- In the US, the new Medicaid prices of AstraZeneca’s Farxiga and BI/Lilly’s Jardiance will take effect in January 2026. As background, the Centers for Medicare and Medicaid Services (CMS) had announced in 2024 the negotiated prices – referred to as “Maximum Fair Prices” – for the first 10 drugs included in the Medicare Drug Price Negotiation Program (MDPNP). Farxiga’s negotiated price would be $179, down 68% from the list price of $556, while Jardiance’s negotiated price would be $197, down 66% from $573. While list prices do not reflect out-of-pocket costs for Part D beneficiaries, we imagine the new change will certainly lower the systems cost.
- Cheaper SGLT-2 inhibitor TheracosBio’s Brenzavvy (bexagliflozin) has also become available this year. In June 2025, TheracosBio partnered with Mark Cuban’s Cost Plus Drug Company and Publix pharmacies to offer Brenzavvy at ~$50/month. In October 2025, TheracosBio and Wellgistics Health announced a partnership to offer Brenzavvy at over than 6,500 independent and chain pharmacies nationwide at a lower cost.
8. MASH has a giant year, with semaglutide becoming the second approved option for the treatment in the US; liver health becomes the next frontier for cardiometabolic development
In August 2025, Wegovy (semaglutide 2.4 mg) became the second therapy approved by the US FDA for the treatment of MASH in adults with moderate to advanced liver fibrosis (stages F2 to F3 fibrosis). The approval was based on Part 1 of the phase 3 ESSENCE trial (n=1,200), in which Wegovy conferred a statistically significant and superior improvement in liver fibrosis, as well as resolution of steatohepatitis with no worsening of liver fibrosis compared to placebo. The approval of Wegovy follows the approval of Madrigal’s Rezdiffra (resmetirom), which was the first FDA-approved treatment for this population in March 2024. Beyond these two approved therapies, 2025 brought high interest in liver health as a whole. Mergers and acquisitions became contentious at times as pharmaceutical giants Novo Nordisk, Roche, and Pfizer fought for a stake in the expanding liver health market through candidates such as FGF21 analog efruxifermin.
- Madrigal’s resmetirom expanded its reach in 2025 and addressed the potential competition that Wegovy offers to Rezdiffra.
- In August 2025, the European Commission approved Rezdiffra (resmetirom) for use in MASH with moderate to advanced liver fibrosis. The decision followed Rezdiffra receiving a positive recommendation by the European Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency (EMA) in June 2025. Madrigal plans to begin the European rollout of the therapy in Germany and expand on a country-by-country basis.
- In Madrigal’s 3Q25 earnings call, Rezdiffra’s tolerability and adherence were emphasized, with an estimated 80% patient adherence or higher. In comparison, discontinuation rates for GLP-1 RAs have often approached 70% among patients with obesity. Wegovy also targets a broader range of liver fibrosis for treatment, including F1 fibrosis and the prevention of MASH, while Rezdiffra treats F2 and F3 (moderate-advanced) fibrosis. Madrigal therefore believes that Wegovy is not a direct competitor for Rezdiffra. As prescriptions for the two therapies continue to expand in 2026, we will follow updates on this dynamic.
- Large pharmaceutical companies completed high-value acquisitions related to liver health in 2025, signaling their confidence in the future of this therapeutic class, including Roche’s acquisition of 89bio (FGF21 analog pegozafermin in phase 3), Novo Nordisk’s of Akero Therapeutics (FGF21 efruxifermin in phase 3), and Pfizer’s of Metsera (several early-stage GLP-1 RAs and amylin candidates). Read more on this in this big picture theme on M&A!
- Beyond leading MASH therapies resmetirom and semaglutide, the treatment landscape further expanded in 2025 with non-incretin and incretin-based therapies.
- In June 2025, Rivus Pharmaceuticals announced positive topline results from its phase 2 M-ACCEL trial (n=219) of HU6, a controlled metabolic accelerator (CMA), for MASH. The majority of patients achieved an over 30% reduction in liver fat with no significant change in lean mass at any dose.
- Altimmune also announced positive topline results of the phase 2b IMPACT trial (n=212), which evaluated dual GLP-1/glucagon RA pemvidutide versus placebo for MASH. At Week 24, a significantly higher percentage of participants taking pemvidutide 1.2 mg and 1.8 mg achieved MASH resolution without worsening of fibrosis compared to the placebo group (59% and 52%, respectively, vs. 19% with placebo).
- South Korea-based D&D Pharmatech then announced positive safety and efficacy results from its ongoing 48-week phase 2 trial of DD01, a once-weekly dual GLP-1/glucagon RA. DD01 achieved a mean reduction of liver fat content of 62% versus 8% for placebo. Nearly half of all participants (49%) achieved normalization of liver fat fraction.
- Throughout 2025, survodutide (a dual glucagon/GLP-1 RA), continued to be evaluated in phase 3 trials for MASH and obesity. The LIVERAGE (n=1,800) trial of survodutide in MASH with moderate or advanced fibrosis (stage 2 or 3) is expected to complete at the end of 2031; and the LIVERAGE-Cirrhosis (n=1,590) trial of survodutide in MASH with compensated cirrhosis (stage 4 fibrosis) is expected to complete in 2H29.
- In October 2025, a post-hoc analysis of the SYNERGY-NASH trial evaluating once-weekly tirzepatide in participants with MASH and stage 2/3 fibrosis revealed further liver-directed benefit. 62.4% of people achieved MASH resolution without worsening of liver fibrosis versus 9.8% in placebo. A significantly greater percentage of participants taking tirzepatide (55%) saw an improvement in fibrosis without worsening of MASH versus those taking placebo (30%).
- Responders for MASH resolution and fibrosis reduction showed greater decreases in body weight (p<0.001 and p=0.023, respectively). A1c reductions were also greater among both MASH (p<0.001) and fibrosis responders (p=0.004). Lastly, liver fat reduction and improved adipose insulin sensitivity was notably improved for MASH responders. Normalization of liver fat was a key mediator of both responder outcomes. Collectively, the findings suggest that tirzepatide’s effects on weight loss and metabolism contribute to disease modification in MASH.
- In June 2025, Rivus Pharmaceuticals announced positive topline results from its phase 2 M-ACCEL trial (n=219) of HU6, a controlled metabolic accelerator (CMA), for MASH. The majority of patients achieved an over 30% reduction in liver fat with no significant change in lean mass at any dose.
9. Beyond opioids and status quo: Emerging therapies for neuropathic pain and limb health
This year, the field saw exciting advancements for microvascular complications, including diabetic painful neuropathy (DPN), peripheral artery disease (PAD), and adverse limb events. Therapeutic development for these complications has been stagnant for decades. Among the nine million people in the US with progressive DPN, 60% have tried multiple treatments, as most therapies do not provide sufficient relief, and a third have resorted to opioid treatments for short-term pain relief, which can increase the risk of opioid addiction. Despite these challenges, there has not been a new nonopioid treatment for DPN in the past two decades. Likewise, PAD affects 10-20 million people in the US, lowering quality of life due to pain, difficulty in walking, and amputation. However, the only treatment for claudication (muscle pain due to lack of oxygen) for people with PAD is cilostazol, which was FDA-approved in 1999. Vertex’s oral non-opioid NaV1.8 inhibitors, Lexicon’s pilavapadin (LX9211), and Novo Nordisk’s semaglutide have the potential to address these significant unmet needs.
- On DPN, Vertex is evaluating Journavx (suzetrigine), an oral, twice-daily NaV1.8 inhibitor, in two phase 3 trials, following positive phase 2 data (n=192), in which Journavx demonstrated statistically significant and clinically meaningful reductions in the numeric pain rating scale (NPRS) of over two points (out of a scale of 0-10). Given these results, the FDA granted Fast Track Designation for Journavx in peripheral neuropathic pain (PNP) and Breakthrough Therapy Designation in DPN. Vertex also assesses VX-993, an oral NaV1.8 inhibitor, in the phase 2 DPN trial (n=300). Separately, Journavx was launched for adults with moderate-to-severe acute pain, following FDA approval in January 2025.
- Lexicon’s pilavapadin (LX9211), an oral, non-opioid AAK1 inhibitor for moderate-to-severe DPN, is also advancing to phase 3 trials in 2026. This follows a full readout of the phase 2b PROGRESS trial (n=496) results at EASD 2025, which showed that all pilavapadin doses, including placebo, reduced average daily pain score from baseline through Week 8. While the trial did not meet its primary endpoint (p=0.11), a post-hoc analysis excluding the highest dose (20 mg) arm achieved significance (p<0.04), supporting the 10 mg dose for future phase 3 studies. The company has scheduled an end-of-phase-2 meeting with the FDA for 4Q25, with written feedback expected in early 2026.
- On PAD, semaglutide significantly improved walking function and patient-reported outcomes in people with T2D and early-stage symptomatic PAD in the phase 3b STRIDE trial (n=792). As presented at ACC 2025, at Week 52, participants on semaglutide had 40 meters greater improvement from a baseline of 185 meters in maximum walking distance, compared to placebo. Furthermore, a post-hoc analysis found that increase in functional capacity did not correlate directly with weight or A1c changes, suggesting additional mechanisms driving functional PAD improvements (e.g. enhanced perfusion or vascular function).
- Injectable and oral semaglutide was also associated with reduced major adverse limb events (MALE). A prespecified analysis from the SOUL trial (n=9,650) found that Rybelsus (oral semaglutide) reduced MALE by 30% in people with T2D, with similar benefits observed in participants with and without PAD. In another pooled analysis of the SOUL, FLOW, and STRIDE trials (n=13,975), semaglutide was associated with a ~30% reduction in limb events across patient subgroups. Taken together, findings support semaglutide as the first diabetes therapy to demonstrate significant limb-event reduction, irrespective of patient history of PAD.
10. Regulatory approvals for diabetic macular edema and diabetic retinopathy improve therapeutic access; commercialization efforts of anti-VEGF biosimilars continue
In 2025, treatment options expanded for eye complications, including neovascular (wet) age-related macular degeneration (wAMD), macular edema following retinal vein occlusion (RVO), diabetic macular edema (DME), and diabetic retinopathy (DR). Susvimo (ranibizumab), Vabysmo (faricimab), and Eylea (aflibercept) currently lead the therapeutic landscape, with key biosimilars to reach commercialization in the near future and less-invasive treatment options also continually explored.
This year, Roche’s Susvimo (ranibizumab) 100 mg/dL, a refillable anti-VEGF eye implant, received approval for ocular complications related to diabetes.
- In February 2025, the FDA approved Susvimo (ranibizumab) 100 mg/mL for diabetic macular edema (DME), making it the first and only continuous delivery system available for this condition. The approval was based on one-year results from the phase 3 Pagoda trial (n=634), in which Susvimo sustained vision improvements comparable to monthly 0.5 mg ranibizumab intravitreal injections.
- In May 2025, Roche announced that the FDA approved its effective therapy Susvimo (ranibizumab) 100 mg/dL for diabetic retinopathy (DR) after submission in April 2024. The PAVILION trial (n=174) evaluated the safety and efficacy of Susvimo for DR. At one year, participants who received Susvimo, refilled every nine months, saw reduced severity in eye damage compared to those receiving monthly clinical observation and treatment with anti-VEGF injections as needed
- In September 2025, Roche also received CE-Mark for Contivue, a port delivery platform for refillable anti-VEGF therapy Susvimo (ranibizumab). Contivue is surgically implanted into the eye, continuously delivering Susvimo over six to nine months, after which the medication is refilled by a healthcare professional. The CE-Mark of Contivue was based on the pivotal phase 3 Archway trial (n=415), and two supportive studies, the phase 2 LADDER study (n=225) and the open-label long-term extension phase 3 Portal study (n=1,000).
Vabysmo (faricimab), also manufactured by Roche, also demonstrated long-term safety this year.
- In September 2025, Roche announced new long-term data on Vabysmo (faricimab) at the Euretina Congress, reinforcing its efficacy, safety, and durability in treating neovascular or “wet” age-related macular degeneration (nAMD). The AVONELLE-X and SALWEEN studies demonstrated that the extended dosing of Vabysmo may offer potential to reduced treatment burden for nAMD.
Regeneron’s Eylea (aflibercept) faced both manufacturing setbacks in the US and a key label extension in Europe.
- In April 2025, the FDA issued a complete response letter (CRL) for anti-VEGF Eylea HD (aflibercept 8 mg). The CRL provided a response to the supplemental Biologics License Application (sBLA) of extending the maximum dosing interval (up to every 24 weeks) for Eylea HD across all approved indications: (i) wet age-related macular degeneration (wAMD); (ii) diabetic macular edema (DME); and (iii) diabetic retinopathy (DR). The CRL did not cite any issues with the safety or efficacy of Eylea HD in its current approved indications and dosing regimens and was related to manufacturing issues.
- In June 2025, the European Commission granted a label extension for Eylea HD (aflibercept 8 mg) in the EU with extended treatment intervals of up to every six months. Eylea is an anti-vascular endothelial growth factor (VEGF) treatment injection for neovascular or wet age-related macular degeneration (nAMD) and visual impairment due to diabetic macular edema (DME). With this approval, Eylea HD became the first therapy with a six-month treatment interval for the treatment of nAMD and DME in the EU.
Key anti-VEGF biosimilars Yesafili and Eydenzelt became closer to commercial launch in 2025.
- In April 2025, Biocon Biologics finalized a settlement and license agreement with Regeneron, enabling US commercialization of the vascular endothelial growth factor (VEGF) inhibitor Yesafili (aflibercept-jbvf). Yesafili is indicated for wet age-related macular degeneration (AMD), DME, diabetic retinopathy (DR), and retinal vein occlusion (RVO). The therapy is the first FDA-approved interchangeable biosimilar to Eylea (aflibercept). Under the agreement, Biocon can launch Yesafili in the US in 2H26 or earlier. The FDA approved Yesafili in May 2024 as an interchangeable biosimilar to Eylea following results from the phase 3 INSIGHT study.
- In October 2025, the FDA approved Celltrion’s Eydenzelt (aflibercept-boav), a biosimilar of Regeneron and Bayer’s anti-VEGF therapy Eylea (aflibercept), for neovascular (wet) age-related macular degeneration (wAMD), macular edema following retinal vein occlusion (RVO), diabetic macular edema (DME), and diabetic retinopathy (DR). The FDA’s decision was supported by clinical data from a 52-week, head-to-head phase 3 study (n=348) among patients with DME. Eydenzelt met equivalence criteria in visual acuity improvement and showed comparable safety, pharmacokinetics, and immunogenicity to Eylea. Eydenzelt was also approved by the European Commission in February 2025.
While intravitreal injections remain the standard of care for AMD, diabetic retinopathy, DME, and RVO, work to explore less-invasive alternatives continues.
- In May 2025, UNITY Biotechnology announced full results of the 36-week phase 2b ASPIRE trial (n=52), which evaluated intravitreal injections of small molecule UBX1325 (foselutoclax) in people with diabetic macular edema (DME), compared to anti-VEGF Eylea (aflibercept 2 mg). Results of the ASPIRE trial (n=52) showed that UBX1325 improved visual acuity (VA) by 5.2 letters (vs. 4.8 letters with aflibercept) and 5.5 letters (vs. 5.3 letters) from baseline at Weeks 24 and 36, respectively – this improvement is equivalent to roughly one additional line on an eye chart.
- In July 2025, Boehringer Ingelheim and Re-Vana Therapeutics announced a collaboration and license agreement to develop extended-release therapies for eye diseases. Boehringer Ingelheim plans to combine its eye disease candidates with Re-Vana’s gradual release technology to release treatments slowly over six to 12 months, reducing the frequency of eye injections.
11. Obesity treatment has a powerhouse year with lots of excitement for next: New approvals, readouts, and clinical frameworks for incretins, amylin, and beyond
Obesity and weight management were at the center of clinical development and discussions this year. In the treatment landscape, Wegovy (semaglutide) and Zepbound (tirzepatide) continued to record multi-billion sales each quarter, as they demonstrated benefits beyond weight loss and metabolic health and expanded into cash pay and global markets. In the pipeline, other late-stage candidates, including Lilly’s orforglipron (oral GLP-1 RA) and Novo Nordisk’s CagriSema (fixed dose combination of cagrilintide 2.4 mg and semaglutide 2.4 mg), delivered robust phase 3 results, setting paths for regulatory decisions, while earlier-stage therapies continue to advance in the pipeline, while differentiating themselves from existing therapies. Along with the innovations, the ADA Standards of Care 2026 and conference symposia strengthened important clinical insights, such as the need for personalized titration regime, strategies for lean mass preservation, and underlying causes of heterogeneity in treatment responses.
- Major topline results and trial readouts showed promise in late-stage incretin-based candidates. In December 2025, Lilly announced topline results of the 68-week phase 3 TRIUMPH-4 trial (n=405) of once-weekly retatrutide (triple GLP-1/GIP/glucagon RA), which showed up to 29% weight loss and significant pain reduction in people with obesity and osteoarthritis. In the phase 3 REDEFINE-1 trial (n=3,417), Novo Nordisk’s CagriSema conferred up to 20% weight loss and cardiovascular (CV) benefits in people with obesity without T2D. In the phase 3b STEP UP trial (n=1,407), high-dose semaglutide 7.2 mg conferred 21% weight loss in adults with obesity, leading to FDA submission and positive recommendation by the EMA. Excitingly, Innovent Biologic’s mazdutide (GLP-1/glucagon RA), was approved in China for obesity as the second dual incretin-based therapy based on the phase 3 GLORY-1 trial (n=610), which showed 15% weight loss. Once-monthly MariTide (maridebart cafraglutide; GLP-1 RA and GIP receptor antagonist) demonstrated 20% weight loss in the phase 2 trial (n=592) but with high GI adverse events. Jiangsu Hengrui Pharmaceutical’s HRS9531 (dual GLP-1/GIP RA) conferred 23% weight loss in Chinese adults with overweight or obesity in a phase 2 trial (n=60).
- On oral agents, Novo Nordisk’s Wegovy pill (once-daily oral semaglutide 25 mg) received FDA approval as the first oral incretin-based therapy for weight management. Wegovy pill is indicated for weight loss, long-term weight maintenance, and cardiovascular (CV) risk reduction. The approval is based on the phase 3 OASIS-4 trial (n=307), in which oral semaglutide 25 mg conferred up to 14% weight loss (vs. 2%) at 64 weeks, and SELECT trial (n=17,604), which showed 20% reduction in MACE with injectable semaglutide. As per the Most-Favored Nation pricing, Wegovy pill will be offered at $150 per month on TrumpRx, the government’s direct-to-consumer platform.
- In the pipeline, Lilly’s orforglipron led to 11% weight loss in the phase 3 ATTAIN-1 trial (n=3,127), with a launch expected in 2026 pending approval. Novo Nordisk submitted high-dose oral semaglutide 25 mg for obesity in the US and the EU based on the phase 3 OASIS-4 trial (n=307), which showed 14% weight loss.
- On other emerging therapies, long-acting amylin agonists, like Novo Nordisk’s cagrilintide, Lilly’s eloralintide, and Zealand/Roche’s petrelintide, received spotlights as potentially foundational weight loss therapies that do not cause significant GI side effects. At EASD 2025, a post-hoc analysis of the phase 3 REDEFINE-1 trial (n=3,417) found that cagrilintide achieved an average weight loss of 12%, compared to 2.3% with placebo at Week 68. In a phase 2 trial (n=263), as presented at ObesityWeek 2025, all doses of eloralintide demonstrated statistically significant weight loss, ranging from 9.5% to 20.1%, compared to 0.4% with placebo and favorable tolerability profile. In March, Zealand and Roche entered partnership to co-develop and co-commercialize amylin analog petrelintide for obesity. The candidate is currently evaluated in the phase 2 ZUPREME-1 and ZUPREME-2 trials.
- Clinical discussions included the importance of personalizing titration schemes, challenges of rapid weight loss, and concerns about lean mass preservation. On the former, the ADA Standards of Care 2026 newly added a recommendation that stresses the importance of personal dose titration to balance efficacy, health benefits, and tolerability. This inclusion echoes sentiment from a symposium from ADA 2025 on the new Standards of Care for Obesity, at which speakers unequivocally emphasized that patients have different treatment goals and respond to drugs differently, and that maintenance dosage for obesity pharmacotherapy should be tailored to individuals.
- On the heterogeneity in patients’ treatment responses, a post-hoc analysis of the SURMOUNT-5 trial (n=751) found that rapid responders to tirzepatide and semaglutide were more likely to be female and have lower weight at baseline. Speaker Dr. Louis Aronne (Weill Cornell) challenged the audience that rapid response may not be necessarily “better,” and proposed that the current titration regimen might even be “excessive” in some patients. More recently, at WCIRDC 2025, Dr. Tracey McLaughlin (Stanford University) shared her hypothesis on why the pathophysiology and treatment response for obesity are heterogenous. She said that visceral fat, inflammation, and impaired adipogenesis are key drivers of insulin resistance, which determines whether an individual with overweight or obesity also have metabolic dysfunction.
- On lean mass preservation, clinicians continue to debate its clinical significance. Dr. Sameul Klein (Washington University at St. Louis) argues that muscle mass loss is natural and clinicians should instead focus on whether weight loss improved cardiometabolic health, physical function, and quality of life; meanwhile, Dr. Richard Pratley (AdventHealth) states that muscle mass loss can be critical for older and more vulnerable adults, who are at higher risk of falls. Multiple interventions are in development for muscle mass preservation. In the phase 2b COURAGE trial (n=1,005), trevogrumab (anti-GDF8/anti-myostatin), with or without garetosmab, significantly improved weight loss quality when added to semaglutide. Likewise, in the phase 2 BELIEVE trial (n=507), bimagrumab (monoclonal antibody blocking activin type II receptors) increased muscle mass and decreased fat mass when added to semaglutide, though Lilly discontinued the trial in September 2025.
12. Reframing T2D care: “Precision” therapies and hypercortisolism
2025 brought a renewed attention to the heterogeneity of T2D, and, with it, a push toward more targeted (not to mention, mechanistically-informed) treatment strategies. Two major developments reframed how the field thinks about difficult-to-treat T2D: the emergence of hypercortisolism as a modifiable contributor to challenging glycemic management, and the rise of precision therapies aimed at restoring beta cell function.
- The CATALYST trial (n=1,113) spotlighted hypercortisolism as a clinically relevant and underdiagnosed driver of difficult-to-manage diabetes. In Part 1 of the trial, nearly 25% of participants with difficult-to-treat T2D were found to have hypercortisolism, with prevalence rising to 37% among those on three or more antihypertensives. In Part 2, treatment with mifepristone, a glucocorticoid receptor antagonist, led to a 1.5% A1c reduction over 24 weeks, alongside meaningful reductions in insulin use, body weight, and waist circumference. Notably, one-third of participants with hypercortisolism had adrenal abnormalities seen on imaging, suggesting a structural basis for dysregulation in a subset of patients.
- KOL commentary at ADA 2025 reinforced the clinical implications. Dr. Ralph DeFronzo (UT Health San Antonio) emphasized that hypercortisolism often presents without classic symptoms but instead manifests as some combination of the “big four”: (i) uncontrolled T2D; (ii) hypertension; (iii) obesity; and (iv) osteoporosis, which are commonly seen in endocrine practice. He called for inclusion of hypercortisolism in the “noxious nine” factors driving hyperglycemia. In addition, Dr. John Buse (University of North Carolina) advocated for routine screening in patients who struggle to reach glycemic targets.
- In October 2025, Biomea Fusion announced results of the phase 2 COVALENT-111 (n=163) trial. In the study, icovamenib (BMF-219), a covalent menin inhibitor, conferred sustained A1c reductions in insulin-deficient subgroups of people with T2D, including those on GLP-1 RAs who had not achieved glycemic goals. At Week 52, icovamenib conferred up to 1.5% A1c reduction after just 12 weeks of dosing, with no treatment-related serious adverse events. The agent is designed to promote beta cell proliferation and function, offering a potential disease-modifying approach for patients with severe insulin deficiency. This advancement reflects the field’s transition from broad anti-hyperglycemic approaches to precision strategies that address underlying pathophysiology for specific subgroups.
Top Ten Most Read Closer Look Reports in Therapy
- Obesity Drug Competitive Landscape – December 18, 2025 – see inside for the overview of obesity candidates in preclinical to phase 3 stages
- Type 1 diabetes cures and prevention competitive landscape – September 9, 2025 – read more here for candidates in development for beta cell replacement, immune therapy, or other approaches
- vTv Therapeutics 3Q25 – November 11, 2025 – phase 3 CATT1 trial for cadisegliatin in T1D; $80 million private placement bolsters funding
- GLP-1 Mono, Dual, and Tri-Agonist Competitive Landscape – October 2, 2025 – featuring an ever expanding list of the GLP-1 RAs (injectable and oral), dual agonists, and tri-agonists
- Lilly 4Q24 – February 6, 2025 – diabetes sales total $9.1B in 4Q24 (+59%) and $29.5B in 2024 (+50%), driven by Mounjaro and Zepbound; comments on compounding and patient access program; major focus on oral GLP-1 orforglipron for obesity, T2D, OSA, and hypertension
- Tirzepatide demonstrates noninferiority in MACE reduction compared to dulaglutide in P3 SURPASS-CVOT trial – July 31, 2025 – tirzepatide confers 8% reduction in MACE, though statistically insignificant, and reduces all-cause mortality by 16%
- Novo Nordisk 2Q25 – August 6, 2025 – diabetes/Obesity portfolio totals $11.3B (+17% CER, -2% sequentially); updates on amycretin, CagriSema, MASH; where might legal actions against compounding go?
- Lilly announces positive topline phase 3 ACHIEVE-1 results of oral GLP-1 RA orforglipron in T2D – April 17, 2025 – orforglipron demonstrates up to 1.6% A1c reduction and 8% weight loss
- Semaglutide 7.2 mg confers superior weight loss compared to semaglutide 2.4 mg in phase 3 STEP UP trial – January 2025 – higher-dose semaglutide achieved weight loss of 20.7% at Week 72, compared to 17.5% with semaglutide 2.4 mg and 2.4% with placebo
- Post hoc analysis of SURMOUNT-2 reveals weight reduction with tirzepatide varies by baseline A1c – August 22, 2025 – Reduced glucosuria from improved glycemic management may limit weight loss in patients with high baseline A1c
Most Unexpected News/Biggest Surprises
Incretins
1. Novo Nordisk submits unsolicited ~$9 billion bid to acquire Metsera; offer may trigger “Superior Company Proposal” notice in Pfizer’s existing acquisition agreement
2. Most-Favored-Nation Pricing expands to offer GLP-1 RAs at $245/month through Medicare and Medicaid plus significant discounts through TrumpRx
3. CMS announces negotiated prices for 15 drugs in the second round of Medicare Drug Price Negotiation Program, including semaglutide
Complications Management
1. Vertex announces FDA approval of Journavx (suzetrigine) for moderate-to-severe acute pain; of interest to those with diabetes peripheral neuropathy, this represents first new pain medication class to receive FDA approval in 20+ years
2. Novo Nordisk’s semaglutide did not confer statistically significant reduction in Alzheimer’s disease progression in phase 3 evoke trials
SGLT inhibitor
1. In the UK, the NICE draft guidance recommends SGLT-2 inhibitors as a first-line therapy with or without metformin for the general population with T2D
2. Lexicon submits additional data for Zynquista (sotagliflozin) in continued efforts to address FDA CRL and support NDA resubmission
3. NEJM publishes full results of the phase 2 CONFIDENCE trial of finerenone and an SGLT-2 inhibitor in CKD and T2D
Insulin
1. Novo Nordisk resubmits insulin icodec (Awiqli) to the FDA for T2D; once-weekly insulin already approved in the EU, Japan, and China
T1D
1. Sanofi’s Tzield for the treatment of stage 3 T1D receives first-ever national priority voucher
2. Vertex shares updates on T1D programs; while VX-264 compound discontinued due to lack of efficacy, look for VX-880 regulatory submission in 2026
3. FINE-ONE full results: Finerenone meets primary endpoint, reducing UACR by 25% in people with T1D and CKD
4. ADA publishes 2026 Standards of Care, with recommendations for incretin-based therapies in people with T1D
Obesity
- Lilly discontinues phase 2 trial of bimagrumab and tirzepatide in people with overweight or obesity and T2D
Big Picture
Key Questions for 2026
T1D screening and monitoring
- What initiatives and efforts could be implemented to increase more precise screening and detection of T1D according to subgroups (e.g., genetic risk factors)?
- How will the US Preventive Service Task Force (USPSTF) update its recommendations on screening and preventive care, based on Sanofi’s submission on this importance?
Overall health and comorbidity management
- How could trials integrate more real-world evidence to reflect the ongoing management of overall health outcomes, including comorbidities?
- What risk mitigation strategies could help increase education and awareness about therapies and technologies emerging in the space?
Direct-to-consumer market, compounding, and US drug pricing
- What measures are telehealth companies using to ensure that GLP-1 RAs are prescribed with comprehensive clinical review of patients and without company-employed prescriber bias?
- How has FDA’s “green list” import alert affected the safety and quality of compounded products?
- How will the official launch of TrumpRx affect sales and uptake for diabetes and obesity treatment?
- For companies participating in the Most-Favored-Nation pricing agreement, will price reductions extend to other treatments in their portfolio? What are the inclusion criteria?
- How might the implementation of the discounted prices via the Medicare Drug Price Negotiation Program affect demand for the selected drugs? How will these policy changes impact innovation?
- Will MFN pricing impact global pricing in any material way in 2026?
Regulatory changes
- If the FDA moves toward a single‑trial requirement for approval, where might this happen? Might it only be primarily in areas like oncology? Might it include only very uncontroversial trials in diabetes and obesity? How could, in any therapeutic area, this reshape clinical trial design, evidence expectations, and regulatory strategy? In chronic, heterogeneous diseases such as diabetes and obesity, might there be a different approach, particularly given the historical reliance on multiple parallel trials – for example, the STEP program for Novo Nordisk’s Wegovy and Lilly’s SURMOUNT program for Zepbound to demonstrate consistency across populations, endpoints, and geographies?
- In a single‑trial paradigm, what new expectations might emerge around trial size, statistical powering, confirmatory evidence, real‑world data, and diversity across age, sex, race/ethnicity, and comorbidity profiles to ensure that one study can adequately support a broad, real‑world use?
- Given the FDA’s longstanding requirement for cardiovascular outcomes trials (CVOTs) for diabetes therapies since 2008 and the substantial patient benefit derived from these large safety studies, how might the potential single‑trial approval standard apply to diabetes drugs?
- Could a single‑trial rule apply only to established molecules seeking new indications (e.g., heart failure), while new molecular entities in diabetes and obesity continue to require multi‑trial programs and extensive safety datasets?
Leadership change
- How will Novo Nordisk’s newly reconstituted Board – led by Mr. Lars Rebien Sørensen and shaped by the Foundation’s push for faster and more decisive governance – balance the need for accelerated strategic action in a rapidly shifting US market with the equally critical need for stability and continuity?
- On the private company front, it was interesting to see both a new chairman at Boehringer Ingelheim, Shashank Deshpande, as well as a key competitive hire on the senior management side, Brian Hilberdink from Novo Nordisk?
Themes
1. Screening for T1D remains a key priority, with emphasis on education and awareness
2025 included several highlights on screening to highlight the importance of early intervention and monitoring. The field has consistently emphasized the importance of T1D autoantibody screening through efforts like Breakthrough T1D’s submission to the US Preventive Services Task Force (USPSTF) in May 2025. As background, the application included recommendations for early, population-wide T1D screening, with an emphasis on individuals with an increased genetic risk. Breakthrough T1D believes that a formal recommendation from the USPSTF on this submission would enhance screening and early diagnosis, ultimately improving health outcomes for many patients. In November 2025, Sanofi hosted a webinar to discuss the publishing process, including steps that will lead to clinical treatment recommendations. The webinar also explained the value of education for early screening, particularly for pre-symptomatic populations at high risk of T1D.
- Emerging recommendations for screening, monitoring, and managing. Following last year’s critical publication of “Consensus for monitoring individuals with islet autoantibody-positive pre-stage 3 type 1 diabetes” in Diabetes Care and Diabetologia, several publications have reinforced the importance of autoantibody screening. For example, The Lancet Diabetes & Endocrinology published a pragmatic framework for providing care to adults who have tested positive for one or more islet autoantibodies. This publication addresses the variability, particularly for adults with a lower risk of T1D progression and high prevalence of baseline dysglycemia, and provides a three-year clinical roadmap for adults with positive islet autoantibodies.
- Evidence reinforces the importance of autoantibody screening. Focusing on early intervention, Diabetes Care published a study comparing autoantibody screening and T1D outcomes between adults and children. In the study, progression to stage 3 T1D was lower in adults with single autoantibody positivity or stage 1 T1D in children, resulting in a five-year risk of 8% for adults with single autoantibody positivity versus 22% for children with stage 1 T1D. However, adults with stage 2 T1D from an initial staging OGTT had comparable five-year progression risks to children, which was 78% for both groups. This report provided further evidence that adult relatives with positive autoantibodies have distinct trajectories and progression risks compared to children, suggesting the need for tailored monitoring and intervention strategies for T1D classification.
- Remaining unmet needs in T1D. In honor of World Diabetes Day in November 2025, Breakthrough T1D released its first-ever “State of T1D” report, synthesizing data from epidemiological studies, national surveys, and Breakthrough T1D-supported research projects to provide a comprehensive overview of the global and US burden of T1D. Breakthrough T1D reported that approximately 1.5 million of those living with T1D reside in the US, including nearly 200,000 children under the age of 20. As this number continues to rise, the need for T1D screening programs and a commitment to T1D research becomes increasingly evident.
- Ongoing efforts to increase education and awareness. We continue to reflect on our conversation with notable leaders from Sanofi in May 2025, during which we discussed Sanofi’s efforts to raise awareness among primary care physicians, pediatricians, patients, and their immediate family members with T1D. We particularly appreciated how education remains a key strategy for increasing T1D detection and access to potential interventions. Focusing on education and awareness, Breakthrough T1D has also announced that nearly 82% of its recent $1.2 billion funding has been dedicated to T1D cures. Furthermore, organizations like Beyond Type 1 continue to invest resources in support of breakthroughs and improved patient outcomes. In November 2025, Beyond Type 1 celebrates its 10th anniversary with the Beyond Limits event, which brought together the T1D community, encouraging people with diabetes to grow “beyond their diagnosis, beyond their barriers, and beyond expectations.”
2. Structural changes in pharmaceutical and tech giants: Spin-off of MiniMed and restructuring of Novo Nordisk indicative of broader industry shifts
This year, there were significant changes to diabetes technology and pharmaceutical companies. In diabetes technology, two major care businesses announced plans to separate from their parent organizations: MiniMed is spinning out from Medtronic, while Ypsomed’s mylife Diabetes Care AG was sold to TecMed. In CGM, Dexcom also announced a CEO succession plan, with current President and COO (as well as interim CEO) Mr. Jake Leach set to succeed Mr. Kevin Sayer as CEO effective next year. Novo Nordisk similarly underwent sweeping leadership transitions to the CEO and Board of Directors, as well as overall restructuring of the company. After several quarters of underperformance due to rising competition in the GLP-1 RA market, compounding business, and pricing pressure, the company is focused on redirecting resources to new “growth opportunities” in diabetes and obesity to regain its competitive leadership.
- In May, Medtronic announcedthat it will separate its Diabetes division into a standalone, publicly traded company – MiniMed – by November 2026. Ms. Que Dallara (current Diabetes President and EVP) will serve as its CEO. All steps taken so far have supported its preferred separation pathway, led by an initial public offering (IPO) followed by a split-off. Mr. Geoff Martha implied that the separation is driven by lower margins and the need for future investment across the business and differing business models – the Diabetes business operates mainly as business-to-consumer (B2C), differing from the rest of the company’s portfolio. He said this move will allow Medtronic to streamline its operations, generating proceeds that will support further investment in its higher-growth, higher-margin areas, while simultaneously enabling the new company to devote more resources to developing the diabetes portfolio Medtronic was advancing. Ms. Dallara echoed these sentiments, saying in an interview at ADA that she thinks: “the most exciting thing to us is that we can bring innovations fast for patients. We control our own destiny.” Medtronic filed a registration statement on Form S-1 with the US Securities and Exchange Commission (SEC) for an IPO of its Diabetes business in December, which detailed MiniMed’s financial profile and pipeline supporting independent operation.
- Dexcom announced its CEO succession plan in July, with current President and COO Mr. Leach set to succeed Mr. Sayer as the company’s next CEO effective January 1, 2026. Mr. Leach, who has been with Dexcom for 21 years following experience at MiniMed and Medtronic, has overseen the company’s CGM platforms since their first commercial launch. His promotion follows a series of leadership roles, including EVP & CTO (2018-2022), EVP & COO (2022-2025), and his May 2025 appointment as President & COO with oversight of corporate strategy and development. During Q&A after the announcement, Mr. Leach outlined his vision for the company’s next chapter, highlighting three strategic pillars: (i) global access; (ii) innovation; and (iii) scale and implementation. He pointed to substantial opportunity for Dexcom globally, highlighting both the health and cost benefits that broader adoption could deliver to international healthcare systems. On innovation, Mr. Leach emphasized his excitement in providing real value to Dexcom’s customers – an increasingly divers userbase, including people with T2D not on insulin, prediabetes, and those focused on metabolic health.
- Ypsomed announced in August 2025 that it has successfully completed the sale of its Diabetes Care business (named mylife Diabetes Care AG) to TecMed. The sale, totaling up to CHF 420 million ($514 million), was originally announced in April 2025. TecMed, founded in late 2020 and owned by Mr. Willy Michel (the father of Ypsomed’s CEO Mr. Simon Michel), is an insulin infusion company that will assume control of Ypsomed Diabetes Care’s operations and assets, including the mylife Loop AID system. The sale did not include Ypsomed’s subcutaneous self-injection products, with the company retaining ownership of its pens and auto injectables as it increasingly targets the biologics and biosimilars market.
- Novo Nordisk appointed Mr. Maziar Mike Doustdar, a former EVP of International Operations, as the new President and CEO of the company, effective August 2025. This followed the announcement in May 2025 that Mr. Lars Fruergaard Jørgensen would step down as the CEO due to market challenges, declines in stocks since mid-2024, and a decision by its biggest shareholder, Novo Nordisk Holdings. Indeed, the company had lowered the 2025 guidance four times this past year, with sales growth now expected at 8-11%, down from 16-24% originally projected in January 2025.
- Since becoming the new CEO, Mr. Doustdar led several restructuring efforts to redirect resources to new “growth opportunities” in diabetes and obesity. In September, the company announced its plans to cut ~9,000 jobs globally (~12% of its workforce). In October, the company terminated several stem cell research, including its search for T1D cure. Meanwhile, Novo Nordisk pursued multiple partnerships and acquisitions in the cardiometabolic field, such as its $5.2 billion acquisition of MASH-focused Akero Therapeutics, collaborations for drug development, and an unsuccessful unsolicited $10 billion bid to acquire Metsera.
- In November 2025, Mr. Lars Rebien Sørensen, former CEO and current Chair of the Board of Novo Nordisk Foundation, was elected as the new Chair of the Board of Directors (BOD) in an Extraordinary General Meeting. This leadership transition follows announcement that former BOD Chair Mr. Helge Lund and several board members resigned amid an unresolvable dispute between the BOD and Novo Nordisk Foundation about the future composition of the board and the governance principles of the company. Mr. Sørensen aims to prioritize: (i) supporting Novo Nordisk regain its competitive leadership and (ii) preparing for the future board leadership in the next two-to-three years.
- Also on leadership, Dr. Rita Kalyani (Johns Hopkins) was appointed as the new Chief Scientific & Medical Officer (CSMO) of the American Diabetes Association (ADA) starting in August 2025, following Dr. Bob Gabbay’s resignation in July 2024. At ADA 2025, Dr. Kalyani delivered the ADA’s President of Medicine and Science address, offering a comprehensive look at the past, present, and future of diabetes care and how she envisions the ADA and its members to shape diabetes research, clinical care, and policy.
3. Major M&As for MASH and obesity: The race towards the next-generation therapies
The fall of 2025 was a dynamic period for mergers and acquisitions (M&A) in the cardiometabolic field, as companies raced to the next-generation treatments for obesity and metabolic dysfunction-associated steatohepatitis (MASH). The acquisitions signal the field’s broader focus in liver health alongside glycemic management, weight loss, and cardiovascular health.
- In September 2025, Roche agreed to acquire San Francisco-based 89bio for up to $3.5 billion. 89bio’s lead drug candidate is pegozafermin, an FGF21 analog currently in three phase 3 trials for the treatment of moderate to severe fibrosis (fibrosis score F2-F3)[1] in MASH, cirrhosis (F4) related to MASH, and severe hypertriglyceridemia. The acquisition reflects Roche’s commitment to expanding its cardiometabolic portfolio. Earlier in March 2025, Roche partnered with Zealand to develop and commercialize Zealand’s petrelintide (long-acting amylin analog) and explore combination therapies, such as petrelintide with Roche’s dual GLP-1/GIP RA, CT-388, for the treatment of overweight and obesity.
- In October 2025, Novo Nordisk announced the acquisition of Akero Therapeutics, developer of FGF21 (fibroblast growth factor 21) analog efruxifermin. Akero’s lead therapy is being evaluated in multiple phase 3 trials for compensated cirrhosis (F4) and pre-cirrhosis (F2-F3), respectively, in people with MASH. The definitive agreement has a value of up to $5.2 billion in cash.
- In September 2025, Pfizer agreed to acquire Metsera for up to $7.3 billion. This set off a series of events in a subsequent bidding war, whenon October 30, Novo Nordisk submitted an unsolicited ~$9 billion acquisition offer. However, in November 2025, Metsera entered into an amended merger agreement worth up to $10 billion with Pfizer. Following lawsuits and Federal Trade Commission (FTC) involvement, Pfizer successfully acquired the company and with it: (i) MET-097i, a once-monthly GLP-1 RA; (ii) MET-233i, a once-monthly amylin analog; and (iii) oral GLP-1 RA candidates. The high-cost, highly public acquisition dispute signals the importance of liver health in 2025.
4. Inflation Reduction Act and Most-Favored-Nation policy: US government reaches price negotiations with pharmaceutical companies
Continuing last year’s momentum toward lower drug prices in the US, the government reached negotiations with pharmaceutical companies under the Medicare Drug Price Negotiation Program (MDPNP) and the Most-Favored-Nation (MFN) policy. See the table below for drug price changes from these programs.
- In November 2025, the Centers for Medicare and Medicaid Services (CMS) negotiated prices for the 15 drugs included in the second round of MDPNP, which will become effective on January 1, 2027. The program was established by the Inflation Reduction Act of 2022, which requires that CMS negotiates prices with drug manufacturers for brand-name drugs without generic or biosimilar competition that are covered by Medicare Parts B or D. Only small molecules approved for at least seven years and biologics approved for at least 11 years are eligible for inclusion. Per negotiation, Novo Nordisk’s three semaglutide products – Ozempic, Rybelsus, and Wegovy – will face a 71% cut to their list prices, dropping from ~$950 per month in 2024 to $274 in 2027. Lilly’s DPP-4 inhibitor Tradjenta will be $78 per month, down 84% from $488, while Merck’s DPP-4 inhibitor/biguanide Janumet and Janumet XD will cost $80 per month, down 85% from $526 per month.
- The negotiated prices from the first round of MDPNP will become effective soon on January 1, 2026. This includes: (i) AstraZeneca’s SGLT-2 inhibitor Farxiga; (ii) Merck’s DPP-4 inhibitor Januvia; (iii) BI/Lilly’s SGLT-2 inhibitor Jardiance; and (iv) Novo Nordisk’s rapid-acting insulins NovoLog and Fiasp, which will face a 66-79% cut from the list price. See the table below for specific changes.
- Looking forward, the MDPNP will expand to include 15 additional drugs in 2028 and 20 additional drugs for 2029 and following years. Drugs selected for the MDPNP will continue to be announced in February two years before when the negotiated prices will take effect.
- In November 2025, the White House announced an expansion of the Most-Favored-Nation (MFN) pricing to offer GLP-1 RAs at $245 per month through Medicaid and Medicaid, as well significant discounts through TrumpRx. Medicare will have a direct deal with Novo Nordisk and Lilly to access treatments like Mounjaro (tirzepatide for T2D), Ozempic (semaglutide for T2D), Wegovy (semaglutide for obesity), and Zepbound (tirzepatide for obesity) for $245/month, for which Medicare beneficiaries will have a co-pay of $50 per month. State Medicaid programs will be able to access these medications at the same price. The new price changes are expected to take effect by mid-2026 for Medicare users but vary on a state-by-state basis for Medicaid patients.
- Moreover, the government will launch TrumpRx, the government’s direct-to-consumer platform, in January 2026. As part of the MFN negotiations, drugs will be offered at discounted prices, including: (i) Wegovy at $350 per month; (ii) Wegovy pill at $150 per month; and (iii) Zepbound and orforglipron (upon approval) at $346 per month.
- In December 2025, the government announced additional agreements with nine pharmaceutical companies for similar cost reductions. The drugs included in this agreement ranges from insulin and DPP-4 inhibitors to PCSK-9 inhibitors, as shown in the table below.
- As background, in May 2025, the Trump Administration signed an executive order requiring pharmaceutical companies to align US drug prices with those in other developed nations. The executive order was first issued on a voluntary basis, with reinforcement planned if progress was not made. Since May, federal health agencies have published policy releases referencing the directive, and the administration has continued to meet with manufacturers to evaluate potential MFN options. On July 31, the US government issued a letter regarding the directive to 17 pharmaceutical companies including Amgen, Pfizer, Lilly, Novo Nordisk, AstraZeneca, and Regeneron. In the letter, President Trump reaffirmed the MFN pricing executive order and directed companies to comply within 60 days.
Table 1: Negotiated Prices for Diabetes and Obesity Medications
| Diabetes Medications | Class | Negotiated Monthly List Price | Original List Price for 30-Day Supply | Percent Discount from List Price |
First round of MDPNP (Effective January 1, 2026) | ||||
| Farxiga | SGLT-2 inhibitor | $179 | $556 | 68% |
| Fiasp / NovoLog | Rapid-acting insulin | $119 | $495 | 76% |
| Januvia | DPP-4 inhibitor | $113 | $527 | 79% |
| Jardiance | SGLT-2 inhibitor | $197 | $573 | 66% |
Second round of MDPNP (Effective January 1, 2027) | ||||
| Ozempic, Rybelsus, Wegovy | GLP-1 RA | $274 | $955 | 71% |
| Tradjenta | DPP-4 inhibitor | $78 | $488 | 84% |
| Janumet, Janumet XR | DPP-4 inhibitor / biguanide | $80 | $526 | 85% |
Most-Favored Nation Pricing for Medicaid/Medicare (Effective mid-2026) | ||||
| Ozempic, Wegovy | GLP-1 RA | $245 (co-pay of $50) | $1,000 and $1,350, respectively | 75% and 81%, respectively |
| Mounjaro, Zepbound | GLP-1/GIP RA | $245 (co-pay of $50) | $1,080 and $1,086, respectively | 77% |
| NovoLog | Rapid-acting insulin | $35 | ~$140 | 75% |
| Tresiba | Long-acting insulin | $35 | $508 | 93% |
| Trulicity | GLP-1 RA | $389 | $987 | 61% |
Most-Favored Nation Pricing for TrumpRx (Launch expected in January 2026) | ||||
| Ozempic, Wegovy | GLP-1 RA | $350 | $1,000 and $1,350, respectively | 65% and 74%, respectively |
| Wegovy pill | Oral GLP-1 RA | $150 | N/A | N/A |
| Zepbound | GLP-1/GIP RA | $346 | $1,086 | 68% |
| Orforglipron (upon approval) | Oral GLP-1 RA | $346 | N/A | N/A |
| Repatha | PCSK-9 inhibitor | $239 | $573 | 58% |
| Jentadueto | DPP-4 inhibitor/metformin | $55 | $525 | 90% |
| Januvia | DPP-4 inhibitor | $100 | $330 | 70% |
| Sanofi’s insulins | insulin | $35 | $100-$500 | 65-93% |
5. Direct-to-consumer market expands amid continued compounding business and pricing pressure
This past year, the GLP-1 RA market in the US shifted rapidly with compounding practices, pricing pressure from the government, and direct-to-consumer sales. While the FDA announced that the shortage of semaglutide and tirzepatide were resolved in in February 2025 and December 2024, respectively, mass compounding of “personalized” and more affordable drugs has persisted. For example, Hims & Hers sell compounded semaglutide at $199 per month, while MDEXAM and Curex offer compounded tirzepatide at $258 and $199 per month. Many of these companies add ingredients like vitamins to “personalize” treatments. In a 2Q25 call, Novo Nordisk estimated that approximately one million patients are on compounded GLP-1 RAs in the US and acknowledged that compounding business has negatively impacted its performance.
- To increase access to their drugs, both Novo Nordisk and Lilly launched their direct-to-consumer platforms, NovoCare Pharmacy and LillyDirect, which sell all approved doses of Wegovy, Ozempic, and Zepbound vials at discounted cash prices. After the two companies reached a deal with the government to implement Most-Favored-Nation pricing starting in mid-2026, Novo Nordisk further cut self-pay price of Wegovy to $349 per month in November 2025, while Lilly lowered the price of Zepbound vials to $299-$449 per month in December 2025. These prices reflect up to ~75% reduction from the list prices of $1,349 and $1,086 per month for Wegovy and Zepbound, respectively. Both companies shared the promise of direct-to-consumer marketing, as it offers patients with limited insurance coverage a more affordable option. In 3Q25, Novo Nordisk said that telehealth and retail cash channels account for ~10% of total Wegovy prescriptions (~26,000). Lilly similarly shared that Zepbound vials comprised nearly 30% of TRx and over 45% of new prescriptions in 3Q25.
- Novo Nordisk and Lilly continued to expand partnerships across telehealth companies and retail pharmacies to broaden the reach of their cash channels. Novo Nordisk extended its cash offering to CVS, Costco, and Walmart, as well as several telehealth companies like WeightWatchers, Ro, and LifeMD. In October 2025, Lilly entered its first retail collaboration with Walmart Pharmacy to launch a pick-up option for people with valid prescriptions to single-dose Zepbound vials.
- The FDA introduced more regulations to ensure safety of compounded products. In September 2025, the FDA issued a “green list” import alert to regulate GLP-1 RA active pharmaceutical ingredients (APIs) from foreign facilities. The green list includes APIs from facilities that the FDA has inspected or evaluated to have met the US manufacturing standards. APIs from facilities not on the list would be subject to detention without physical examination (DWPE), for which the facilities are required to provide evidence that manufacturing and distribution of APIs follow the Current Good Manufacturing Practice (CGMP) requirements. This decision follows FDA’s investigation that many compounded GLP-1 RAs are manufactured with bulk APIs sourced from China, India, and Europe and that 21% of foreign API sites (10 of 48 inspected) are non-compliant with CGMP standards.
- To further regulate compounding business, Reps. Rudy Yakym (R-IN) and André Carson (D-IN) introduced a new bill in December 2025, titled “Safeguarding Americans from Fraudulent and Experimental (SAFE) Drugs Act of 2025.” The bill proposes to restrict mass compounding of “essentially cop[ies]” of FDA-approved drugs and increase regulatory oversight on manufacturing and interstate distribution. Multiple lawsuits among the FDA, compounders, and pharmaceutical companies are ongoing, as well.
6. One trial or two? A key regulatory question emerges at FDA after some riffing
In an article with STAT News by Lizzy Lawrence on December 4, “FDA to lower number of trials required for approval of drugs, other medical products,” FDA Commissioner Dr. Marty Makary teased that the FDA would move toward a single-trial requirement for the approval of “most” drugs and certain medical products. He asserted that a single, well-designed trial can provide sufficient statistical power, although two trials may still be required in select cases. FDA expects to finalize the new policy within three to six months. This change would represent a significant deviation from more than six decades of regulatory precedent.
- While there are concerns that this change would weaken the regulatory benchmarks that evaluate drugs’ safety and efficacy, we imagine the new requirement could be applicable for certain oncology drugs, which are already reviewed on an expedited timeline, or more limited specialty drugs for rare diseases.
Within diabetes, we would be surprised to see the one-trial requirement implemented to all new drugs. Since 2008, when observational studies began to find that antihyperglycemic thiazolidinedione Avandia (rosiglitazone) may be associated with increased risk of heart attack and stroke, the FDA has required new diabetes drugs to undergo cardiovascular outcomes trial to demonstrate long-term safety. This regulatory requirement, in fact, led to the discovery that SGLT-2 inhibitors. Moreover, given the chronic and heterogeneous nature of the disease, long-term studies in diverse populations are valuable. For this reason, while trials could get bigger in number of participants tested, we would be very surprised if the double-trial requirement would simply disappear in more complex and chronic illnesses. Nonetheless, we wonder if the one-trial requirement could be applicable for drugs like a sixth-to-market SGLT-2 inhibitors or even classes like incretins that may be submitted in different combinations (GLP-1/GIP/glucagon, etc). We look forward to more detailed guidance from the FDA next year!
Top Five Most Read Closer Look Reports in Big Picture
- ADA publishes 2026 Standards of Care – December 8, 2025 – Read on for the most important changes, ranging from CGM for non-insulin T2D, AID for insulin-using T2D, MASH, and expanded therapeutic options for glycemic targets
- Blue Circle Health announces expansion of virtual T1D program to five additional states, for a total of 16 states with access to the platform – October 24, 2025 – Massachusetts, Connecticut, Pennsylvania, Virginia, and Kentucky will gain access to Blue Circle health, joining 11 states in the eastern US plus Iowa and Missouri
- Most-Favored-Nation Pricing expands to offer GLP-1 RAs at $245/month through Medicare and Medicaid plus significant discounts through TrumpRx – November 6, 2025 – Federal government strikes deal with Novo Nordisk and Lilly to offer discounts for GLP-1 RAs and other therapeutics, highlighting cardiovascular and glycemic benefits
- Novo Nordisk appoints Mr. Maziar Mike Doustdar as new President and CEO; Mr. Marcus Lang as new CSO; lowers 2025 guidance significantly due to ongoing challenges in the US – July 29, 2025 – Sales growth now expected at 8-14%, down from 13-21% due to compounding business, competition, and limited market expansion
- Breakthrough T1D releases inaugural “State of T1D” report showing rising prevalence, widening demographic shifts, and technology access gaps – November 14, 2025 – Report compiles updated prevalence, demographic trends, and research milestones; aims to counter misinformation and elevate public awareness of T1D
Most Unexpected News/Biggest Surprises
- CMS announces negotiated prices for 15 drugs in the second round of Medicare Drug Price Negotiation Program, including semaglutide
- In unresolved dispute between Novo Nordisk BOD and the Novo Nordisk Foundation, Chairman of the Board Mr. Helge Lund exits, along with a majority (seven of 12) of board members
- CMS announces next 15 drugs included in the second phase of Medicare Drug Price Negotiation program, including six diabetes-related medications
- Most-Favored-Nation Pricing expands to nine additional pharmaceutical companies, including those focused on diabetes treatment
- ICER publishes report on “fair” drug pricing, including T2D and obesity treatments
- Novo Nordisk submits unsolicited ~$9 billion bid to acquire Metsera; offer may trigger “Superior Company Proposal” notice in Pfizer’s existing acquisition agreement
- FDA establishes “green list” to regulate imports of GLP-1 RA active pharmaceutical ingredients and ensure safe treatment distribution – ten firms found to be non-compliant
- Novo Nordisk terminates recent partnership with Hims & Hers for Wegovy (semaglutide), citing safety concerns
Notable Interviews in 2025
Diabetes Technology
- Interview with Glooko’s leadership team on its acquisition of Monarch Medical and the integration of inpatient insulin dosing algorithm EndoTool - On the Monarch Medical acquisition, CGM integration and care transition, EndoTool’s role in primary care and population health management, raising integration awareness among HCPs, and upcoming eCQM reporting requirements - (November 11, 2025)
- Interview with Biolinq CEO Mr. Rich Yang on Biolinq Shine, a patch-based CGM, and its FDA De Novo classification - On FDA’s GRM category creation, Biolinq Shine’s indication, intradermal and semiconductor design with LED-screen dual display, access strategy, and multi-analyte platform roadmap - (November 14, 2025)
- Interview with Sequel’s leadership team on twiist’s ongoing US launch, key differentiators, and future expansion into T2D - Discussion touches on phased US rollout for twiist, its key differentiators, and strategy to expand AID access and indications for T2D - (September 11, 2025)
- Interview with Tandem Diabetes Care’s President and CEO Mr. John Sheridan and EVP and Chief Administrative Officer Ms. Susan Morrison - Discussion included extended-wear infusion sets, pharmacy distribution channel, and benefits of AID - (September 11, 2025)
- Interview with Dexcom President & COO Mr. Jake Leach on strategic vision, innovation pipeline, and global expansion - Discussion covered 15-day sensor, adhesive innovation, Oura partnership, and Dexcom’s vision beyond diabetes - (August 11, 2025)
- Interview with Medtronic’s Ms. Que Dallara, Dr. Bob Vigersky, and Ms. Kate Cronin on MiniMed’s spinoff from Medtronic, Abbott partnership, 800-series pump, and InPen use - Discussion identifies touches on the upcoming split of MiniMed from Medtronic Diabetes; potential of 800-series pump and InPen - (August 4, 2025)
- Interview with Medtronic’s Dr. Bob Vigersky and Dr. Jen McVean on expanding MiniMed 780G adoption across diverse populations - Leadership muses on MiniMed 780G in expanded populations, including pregnancy and T2D, and promotes early AID adoption, women’s health - (June 25, 2025)
- Interview with pain specialist Dr. Krishnan Chakravarthy and Medtronic Inceptiv spinal cord stimulator (SCS) user, Mr. Scott Kasoff, explores the role of Inceptiv in managing diabetic painful neuropathy - Pain clinician Dr. Chakravarthy and DPN patient Mr. Kasoff provide insights on Inceptiv, Medtronic’s “closed-loop” SCS therapy for DPN, and the importance of patient and provider education - (July 3, 2025)
- Interview with Abbott’s EVP of Diabetes Mr. Chris Scoggins on Abbott’s initiatives, pipelines, and what’s to come - Discussion touched on upcoming dual glucose-ketone sensor; Above the Bias campaign and lasting impact on stigma; goal of empowering people with diabetes - (June 22, 2025)
- Interview with Insulet’s new CEO Ms. Ashley McEvoy, CMO Dr. Trang Ly, COO Mr. Eric Benjamin, and others on T2D adoption, international expansion, and progress toward fully closed-loop - (June 23, 2025)
- Interview with Abbott’s VP of North America Commercial Operations for Diabetes Care, Dr. Badia Boudaiffa, on the launch of the new Libre app in the US - New universal platform will allow for quicker application updates; ability to customize alarm settings; real-time FreeStyle Libre 2 data streaming launched - (April 15, 2025)
- Interview with Dexcom’s CEO Mr. Kevin Sayer on the launch of Stelo, T2D coverage, upcoming G8, and future of multi-analyte sensors - Dynamic discussion explores product strategy and additional populations who could benefit from CGM - (March 17, 2025)
Diabetes Therapy
- Interview with the T1D Fund’s new CEO Ms. Elizabeth Mily on her appointment and priorities for the Fund’s next chapter – The T1D Fund’s new CEO shares her personal motivations for joining the Fund, her vision for its future, and her goals to expand and strengthen partnerships to accelerate research and development toward finding a T1D cure – (March 4, 2025)
- Interview with Sernova’s CEO Mr. Jonathan Rigby on trial updates for Cell Pouch and visions for T1D cure(s) – Mr. Rigby shares his personal journey with T1D, trial updates for the Cell Pouch Bio-hybrid Organ, and insights on Sernova’s ongoing partnership with Evotec – (March 31, 2025)
- The challenges and opportunities for T1D autoantibody screening: A discussion with top Sanofi leaders, with significant food for thought – Sanofi’s Ms. April Kelly and Mr. John Strayer on raising awareness on T1D screening among PCPs, pediatricians, patients, and immediate family members of those with T1D – (May 20, 2025)
- Interview with Lexicon CMO Dr. Craig Granowitz and Head of External Affairs Dr. Alina Cocuzza on pipeline, FDA engagement, and Inpefa (sotagliflozin) differentiation strategy – How Lexicon is navigating FDA dialogue and positioning sotagliflozin for broader impact – (September 25, 2025)
Big Picture
- Interview with head of Roche and Genentech’s new Boston Innovation Center, Dr. Manu Chakravarthy – Discussion explores how the Cardiovascular, Renal, and Metabolism hub will facilitate further expansion in research on AI/ML innovation and several of Roche’s diabetes and obesity candidates – (May 7, 2025)
- Interview with Team Novo Nordisk CEO Mr. Phil Southerland on the cycling team’s contract renewal with Novo Nordisk – Five-year extension of sponsorship and reducing stigma – (December 1, 2025)
2025 Resource Hubs for Scientific Conferences Attended by Close Concerns
Conference Resource Hubs continued to be our centralized one-stop-shops for all conference happenings in 2025. See below for all our Resource Guides covering conferences and meetings that took place in 2025 in order of occurrence.
- Consumer Electronic Show- January 7-9, 2025
- Changing the Course in T1D – January 13-14, 2025
- JP Morgan Healthcare Conference - January 13-15
- ADA Clinical Update Course- January 31-February 2
- “Above the Bias” Launch – February 4, 2025
- Diabetes UK (DUK)- February 26-28
- nPOD 17th Annual Scientific Meeting - March 2-5
- 18th Annual Conference on Advanced Technologies & Treatments for Diabetes (ATTD)- March 19-22
- Annual American College of Cardiology (ACC) Conference - March 29-31
- International Diabetes Federation (IDF) World Diabetes Congress - April 8-10
- National Minority Quality Forum (NMQF) - April 28-29
- European Association for the Study of the Liver (EASL) Congress 2025 - May 7-10
- European Congress on Obesity (ECO) - May 11-14
- American Association of Clinical Endocrinology (AACE) - May 15-17
- DHNY Obesity+Health – May 20, 2025
- embecta Analyst & Investor Day – May 22, 2025
- Heart in Diabetes- June 6-8
- ADA 85th Scientific Sessions - June 20-23
- Friends For Life- July 9-11, 2025
- ENDO - July 12-15, 2025
- ATDC - July 23-27, 2025
- MDUFA VI Public Meeting – August 4, 2025
- ADCES - August 8-11, 2025
- ESC - August 29-September 1, 2025
- EASD - September 15-19, 2025
- Roche 2025 Pharma Day – September 22, 2025
- HFSA - September 26-29, 2025
- Rock Health Summit- September 30, 2025
- Joslin International Symposium - October 7-9, 2025
- CEU - October 23-25, 2025
- CMHC - October 23-26, 2025
- Breakthrough T1D Mission Summit - October 25-27, 2025
- DTM - October 28-30, 2025
- MTMVI Workshop - November 4, 2025
- ObesityWeek - November 4-7, 2025
- ISPAD - November 5-8, 2025
- AHA - November 7-10, 2025
- The Liver Meeting- November 8-11, 2025
- Rachmiel Levine-Arthur Riggs Symposium - November 14-18, 2025
- Insulet Investor Day – November 20, 2025
- Cardiovascular, Kidney, and Metabolic Outcomes CVOT Summit - November 23, 2025
- WCIRDC - December 3-6, 2025
- ATTD-Asia - December 9-11, 2025
- Zealand Pharma Capital Markets Day – December 11, 2025
- ADCES Diabetes Technology Conference - December 12-13, 2025
Literature Shared in 2025
In 2025, we shared a total of 225 pieces of literature in our Closer Look newsletter. Breaking that number down, we shared 18 in January, 15 in February, 15 in March, 16 in April, 16 in May, 21 in June, 24 in July, 23 in August, 20 in September, 24 in October, 16 in November, and 17 in December. Put another way, that’s 21% in the first quarter, 23.5% in the second quarter, 30% in the third quarter, and 25.5% so far in the fourth quarter.
December 2025
| Title | Author | Journal | Commentary |
| Why childhood obesity endures, grows | Dr. Alvin Powell | Harvard Gazette | He wrote that pediatric obesity in the US has worsened dramatically since Harvard's Dr. Steven Gortmaker first highlighted the issue 40 years ago. Today, approximately 20% of children and adolescents in the US have obesity, with another 16% overweight – alarming statistics given the quicker progression to diabetes-related complications with youth-onset disease. While the “basic” explanations for obesity of kids eating more and moving less remains partly true, he emphasized that the crisis stems from a mix of culture, economics, genetics, and policy failures. While programs like the American Academy of Pediatrics’ Healthy Weight Clinic have shown success by addressing behavior change and social determinants of health, Dr. Powers wrote that treatment alone cannot make up for needed policy reforms. Some initiatives have already shown impact countering these forces driving childhood obesity, yet work is still needed. |
| Continuous Glucose Monitoring in Insulin-Treated Older Adults with Diabetes and Alzheimer Disease and Related Dementias | Dr. Pareeta Kotecha | JAMA Diabetes and Endocrinology | The retrospective study sought to evaluate the impact of CGM versus BGM in older adults with Alzheimer’s disease and related dementias (ADRD) and insulin-treated diabetes. Researchers identified a 1:1 matched cohort of 2,022 insulin-treated older adults (mean age of 76 years) with diabetes ADRD from a random sample of Medicare claims data. Compared to BGM, CGM use was significantly associated with lower risk of all-cause hospitalizations and mortality, conferring hazard ratios (HR) of 0.86 and 0.57, respectively. While not statistically significant, CGM use was also found to have lower point estimates for hypoglycemia hospitalization (HR 0.66) and falls (HR 0.86), alongside higher point estimates for hyperglycemia crisis, (HR 1.38) compared to BGM. In all, Dr. Kotecha’s findings support CGM use as improving long-term outcomes in this vulnerable patient population where cognitive impairment and glycemic management have a bidirectional relationship. |
| Development and recalibration of a multivariable type 1 diabetes prediction model for type 1 diabetes across multiple screening studies | Prof. Richard Oram | Diabetologia | The University of Exeter shared an update on its work to develop a free, globally accessible T1D risk calculator to support earlier identification of individuals who may benefit from disease-modifying therapies like teplizumab. Led by Prof. Richard Oram, the study advances a decade of work on genetic risk scores and screening tools. This included a review of three recent studies demonstrating that predicting T1D risk is now significantly cheaper, faster, and more accessible. In the article published in Diabetologia in May 2025, the authors refined and compared more than 1,900 prediction models to identify low-cost methods that perform as accurately as more complex models. Several months later (July 2025) the team reported in Diabetes Carethat children and adults with the same autoantibody markers progress differently, highlighting the need for age-tailored screening. Simple combinations of metrics, such as A1c, BMI, and C-peptide levels, cut prediction costs by two-thirds and shortened testing time from 2.5 hours in the clinic to ~20 minutes at home, offering a pathway to scalable population-level screening. In the latest BMC Medicine article also published July 2025, the team recalibrated an optimized prediction model using over 4,000 TrialNet participants and more than 7,000 TEDDY participants. The updated model demonstrated improved accuracy across multiple screening settings, and its outputs now power the new online risk calculator designed for clinicians and families. Across all three studies, the University of Exeter team underscored that earlier and more accessible risk prediction is increasingly possible through these tools. |
| Diabetes and sudden cardiac death: a Danish nationwide study | Dr. Tobias Skjelbred | European Heart Journal | Of approximately 5.5 million people and 54,028 deaths in Denmark, the authors identified 6,862 sudden cardiac death cases in 2010. 97 of these individuals were diagnosed with T1D and 1,149 with T2D – while it may be surprising to some that nearly 13% of this population had T1D, we know that northern Europe is a hotbed for T1D. Notably, incidence rates of sudden cardiac death were 3.7 times higher than the general population for T1D and 6.5 times higher for T2D. T1D and T2D were both independently associated with sudden cardiac death, with the greatest risk difference actually observed in younger people with diabetes. On average, patients with T1D lost 14 years of life compared to the broader population, and nearly eight life-years were lost for those with T2D, in line with previous studies based in the UK and Sweden. Of these years, 3.4 years could be attributed to sudden cardiac death for T1D and 2.7 years for sudden cardiac death for T2D. It’s interesting from our view that sudden cardiac death represented nearly 25% and over 33% of the impact for T1D and T2D, respectively. Of note, high rates of hypoglycemia requiring hospitalization were observed among SCD cases with diabetes: 37% of those with T1D and 7.2% of those with T2D had a history of hospitalization for hypoglycemia. The authors identify this as a compelling area for future research to better explain the mechanism beyond the association of SCD and diabetes. As prevalence rates of T2D continue to rise in Denmark and around the globe, and as prevalence rates of T1D continue to rise in some geographies, we will continue searching for mechanistic answers and opportunities. |
| Metabolic Dysfunction-Associated Steatotic Liver Disease in Adults | Prof. Helbert Tilg | JAMA | Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most common chronic liver disease worldwide, encompassing the range between isolated steatosis (excess fat in the liver without inflammation) to metabolic dysfunction-associated steatohepatitis (MASH; excess fat in the liver with inflammation). In all, MASLD affects upwards of 40% of the global adult population, including 60-70% of those with T2D and 70-80% of individuals with obesity. Behavioral modifications stand as first-line treatment for MASLD, including: (i) hypocaloric low-carbohydrate and low-fat diets; (ii) physical exercise; and (iii) reduced alcohol intake alongside management of comorbid conditions (T2D, obesity, hypertension, and hyperlipidemia). These lifestyle changes are complemented by management of comorbid conditions, including T2D, obesity, hypertension, and hyperlipidemia. In therapies, resmetirom (Madrigal’s Rezdiffra) and subcutaneous semaglutide remain the only approved therapies for moderate to advanced fibrosis in MASH. While the disease burden is substantial, the article underscores that MASLD is modifiable—and that targeted interventions, especially physical activity, offer meaningful opportunities to reduce progression and improve outcomes across diverse populations. |
| Potential Benefits of Remission of High Childhood BMI Keep Increasing | Dr. Lise Bjerregaard | Diabetes Care | Dr. Bjerregaard notes that one in five children worldwide are overweight or have obesity, a striking figure with serious consequences across chronic kidney disease, cardiovascular disease, and broader cardio-kidney-metabolic (CKM) syndrome. Previous large-scale studies have demonstrated that high BMI in childhood is associated with increased risk of adult-onset T2D and chronic kidney disease, encouraging research into the potential benefit of remission from childhood obesity. Dr. Bjerregaard discusses recent findings from Wang et al. confirming that increases in BMI from childhood to adulthood increase the risk of cardiovascular and metabolic diseases in adulthood and demonstrating for the first time that the effects of high childhood obesity on long-term health may be reversible. Dr. Bjerregaard calls for health policy changes to focus on the treatment of childhood obesity towards a goal of remission, in addition to the prevention of overweight and obesity in children. She encourages further research into pharmacotherapy and bariatric surgery in youth, particularly into long-term outcomes, in order to explore the full benefit of remission across a life course. |
| Socioeconomic Factors and Initiation of Semaglutide or Tirzepatide Among Medicare Beneficiaries With Type 2 Diabetes | Dr. Sérgio R. Decker | Diabetes Care | This cross-sectional study (n=13,922,387) included Medicare claims from people aged ≥65 years with T2D to identify the social and economic factors associated with the initiation of semaglutide or tirzepatide. Among the study population, 4.8% of the people with T2D initiated treatment with semaglutide or tirzepatide in 2023. One of the major factors associated with lower initiation of treatment included minority racial/ethnic identity, with Hispanic (adjusted odds ratio: 0.75), non-Hispanic Asian (adjusted odds ratio: 0.70), and non-Hispanic Black (adjusted odds ratio: 0.72) individuals all having lower odds of treatment initiation compared to non-Hispanic white individuals, who represented the reference group. Additionally, dual enrollment Medicare status (adjusted odds ratio: 0.90) and residence in the most vs. least socially vulnerable neighborhoods (adjusted odds ratio: 0.93) were associated with lower odds of treatment initiation. We hope these findings will highlight and lead to strategies for expanded treatments in everyone with diabetes. |
| Climate Vulnerability Index and Incident Type 2 Diabetes in a Large Integrated Health Care System | Dr. Jad Ardakani | JAMA | This retrospective study (n=1,003,526) included data from the Houston Methodist Cardiovascular Disease Learning Health System Registry between June 2016 and August 2023 to determine a potential association between residence in communities with higher climate vulnerability index (CVI) and risk of incident T2D. Results showed an overall T2D incidence rate of 1.88 cases per 100 person years. Additionally, the incidence increased across CVI quartiles, from 1.48 cases per 100 person-years in Q1 and 2.66 cases per 100-person years in Q4. These results translate to those in the highest CVI quartile facing a 23% higher risk of developing T2D than those in the lowest quartile, even after adjusting for demographics, insurance status, cardiovascular risk factors, and baseline A1c. As one of the first studies to evaluate the impact CVI has on T2D risk, the study underscores significant implications for public health and clinical decisions aimed at improving environmental contexts. |
| Longitudinal Analysis of Liver Chemistry Trajectories and Risk of Type 2 Diabetes in Children With Metabolic Dysfunction-Associated Steatotic Liver Disease | Dr. Nhat Thai | Diabetes Care | This multicenter cohort study (n=1,035) examined the potential for γ-glutamyl transferase (GGT) aspartate aminotransferase (AST), and alanine aminotransferase (ALT), key liver enzymes, to serve as biomarkers of T2D risk in children with MASLD. For a mean of 3.9 years, a 30-unit increase of GGT, AST, and ALT was associated with a 50%, 31%, and 13% increased risk of T2D, respectively. In addition, there was a 12% cumulative incidence of T2D in the study cohort. Given that MASLD is the most common liver disease in children, affecting about 10% of youth, the study provides crucial parameters for early detection of T2D risk, especially in an era of increased prevalence of childhood obesity and comorbidities like T2D and MASLD. |
| Insurance Coverage and Pricing of Weight-Loss Drugs in the United States | Dr. Stacie Dusetzina | NEJM | This article outlined the impact of expanded Most-Favored-Nation (MFN) pricing, announced in last month, for GLP-1 RAs on patients and companies. The authors said that the price reductions of GLP-1 RAs offered by Lilly (i.e., Mounjaro and Zepbound) and Novo Nordisk (i.e., Ozempic and Wegovy) at $245/month, will lead to broader access to treatment for patients covered by Medicare and Medicaid. Reflecting on these outcomes, they also offered context on recent announcements around GLP-1 RAs and pricing, including price negotiations through the Inflation Reduction Act, tariff reliefs, and regulatory approvals. The authors concluded by saying that this new agreement could improve access for patients with price reductions. However, they also encouraged the need to continue monitoring the health effects on patients and focus on overall healthcare spending for patients, payers, and all stakeholders to ensure equitable access for broader populations. Read more inside. |
| Effect of Low Bolus Frequency on Automated Insulin Delivery System Performance in Youth With Type 1 Diabetes | Dr. Prerana Chatty | Diabetes Care | This study assessed the differences in glycemic outcomes between Omnipod 5 (n=75) and Tandem Control-IQ (n=127) among youth with low bolus frequency (≤3 boluses/day). After propensity score-matching 98 youth, there was no between-group difference in user-initiated boluses (~2.2 boluses/day). However, adjusted TIR was 8% higher in Control-IQ users (55% vs. 47%; p<0.05), though overall glycemic management across both systems remained suboptimal in this population that was not regularly bolusing. The authors posited that higher time in automated mode among Control-IQ users (80% vs. 64% with Omnipod 5) contributed to these stronger glycemic outcomes and concluded that these algorithm-specific effects of bolus frequency should be considered and discussed with families when choosing an AID system. |
| Trajectories of type 2 diabetes and cancer in 330 000 individuals with prediabetes: 20-year observational study in England | Prof. Francesco Zaccardi | The Lancet Diabetes and Endocrinology | This study examined connections between elevated blood glucose levels and increased cancer risk. Using Clinical Practice Research Datalink primary care records, the authors identified over 300,000 individuals with prediabetes between 1998 and 2018 in England. Patients were followed from the time of prediabetes diagnosis until death or the study’s conclusion in November 2018. 10 years after the diagnosis of prediabetes, the probability of remaining in the prediabetes state ranged from 23% (men aged ≥75 years at diagnosis) to 72% (men aged <55 years), the probability of death following prediabetes ranged from 1% (women aged <55 years) to 39% (women aged ≥75 years), the probability of developing T2D and remaining in this state ranged from 8% (men aged ≥75 years) to 24% (women aged <55 years), and the probability of developing cancer and remaining in this state ranged from 2% (men aged <55 years) to 8% (men aged ≥65 to <75 years) in men and women. This indicates that prediabetes disease trajectories vary significantly by age at time of diagnosis, motivating strategies for the prevention and the early detection of prediabetes. These efforts may play a key role in combatting the development of T2D and cancer on a global scale |
| Generic Liraglutide – Overlooked but Not Forgotten | Dr. Shuas Gondi | NEJM | In the article, the authors reflected on the surge of GLP-1 RAs, which now represent a multi-billion-dollar market, with two dominant next-generation treatments: Novo Nordisk’s semaglutide (Ozempic) and Lilly’s tirzepatide (Mounjaro). While liraglutide was once the most prescribed GLP-1 RA, newer generation GLP-1 RAs have overtaken the market – in fact, to date in 2025 according to NEJM, liraglutide only accounted for just 1% of GLP-1 RA prescriptions in the US (we are curious to see NEJM’s quantifications for the newer generation GLP-1 RA prescriptions over the years in relation to liraglutide). The authors attributed the shift away from liraglutide to multiple factors that newer GLP-1 RAs offer |
| Prediabetes remission and cardiovascular morbidity and mortality: post-hoc analyses from the Diabetes Prevention Program Outcome study and the DaQing Diabetes Prevention Outcome study | Dr. Elsa Vazquez Arreola | The Lancet Diabetes and Endocrinology | The authors performed a post-hoc analyses on 2,402 participants with prediabetes from the US Diabetes Prevention Program Outcomes Study (DPPOS) and 540 from the Chinese DaQing Diabetes Prevention Outcomes Study (DaQingDPOS). In the DPPOS study, 12% of participants reached remission after one year of intervention for prediabetes using the standard of care. After a median follow-up of 20 years, the event rate for cardiovascular death or hospitalization for heart failure was 1.74 per 1000 person-years in participants who reached remission versus 4.17 in those without remission (p=0.013). The hazard ratio was 0.41 (p=0.014), meaning that the rate of the cardiovascular outcomes was 59% lower in those who achieved remission. In the DaQingDPOS study, the hazard ratio was 0.49 (p=0.010), confirming the results. These data indicate that achieving remission from prediabetes is linked to decades-long cardiovascular benefits across diverse patient populations. In the future, prediabetes treatment and prevention may represent an important approach to cardiovascular disease |
| An AI-Powered Lifestyle Intervention vs Human Coaching in the Diabetes Prevention Program | Dr. Nestoras Mathioudakis | JAMA | The trial (n=368) aimed to determine whether referral to an exclusively AI-led lifestyle intervention based on the Diabetes Prevention Program (DPP) is noninferior to referral to a human-led DPP in achieving recommended thresholds for weight loss, A1c reduction, and weekly physical activity among adults with prediabetes and overweight or obesity. Participants were randomized 1:1 to receive either a referral to an AI-powered DPP lifestyle intervention delivered via a mobile app and Bluetooth-enabled digital scale or a referral to a human coach-led DPP lifestyle intervention delivered remotely over 12 months. Participants had a mean age of 58 years, 71% were female, and were racially diverse (27% were Black and 6% were Hispanic). Nearly one-third of participants in both the AI-led DPP group and human-led DPP group (32% each) maintained A1c <6.5% throughout the study and achieved: (i) ≥5% weight loss; (ii) ≥4% weight loss and ≥150 minutes of weekly physical activity; or (iii) a reduction in A1c of ≥0.2% at 12 months, meeting noninferiority criterion. |
| SURPASS-CVOT | Dr. Stephen Nicholls | NEJM | The long-awaited, head-to-head cardiovascular outcomes trial compared Lilly’s once-weekly tirzepatide (dual GIP/GLP-1 RA) to Lilly’s dulaglutide (GLP-1 RA) in adults with T2D and established atherosclerotic cardiovascular disease. As background, the study’s topline results were announced in late July, and full results were subsequently presented at EASD 2025. At the time – and still today – we’re very impressed that Lilly would set up a head-to-head trial with two of its own (!) therapies. More typical (and as we've been seeing in the rest of SURPASS)* would be against a competitor therapy, particularly for a therapy as strong as tirzepatide. Tirzepatide met prespecified criteria for noninferiority compared to dulaglutide on the primary endpoint – a composite of CV-related death, MI, or stroke. Beyond the primary endpoint, the publication adds critical clinical details, including that tirzepatide produced significantly greater reductions in A1c and body weight than dulaglutide. Additionally, secondary and exploratory analyses showed favorable trends for tirzepatide use in kidney outcomes and all-cause mortality, supporting the therapy’s use in adults with advanced cardiovascular disease. |
| Time trends in mortality from heart failure and atherosclerotic cardiovascular disease in people with and without diabetes | Dr. Joanna Gong | The Lancet Diabetes & Endocrinolog | Using CV mortality data from Europe, Australia, Canada, and South Korea between 2000 and 2023, investigators estimated mortality rates for coronary heart disease (CHD), cerebrovascular disease, and heart failure by diabetes status. Across geographies and diabetes status, we've been very glad to see CVD mortality rates declined over time. Notably, CHD mortality dropped by 12%-32% in the past five years. HF mortality decreased in most regions, except in Ontario, Canada, but to a smaller degree than that of CHD and cerebrovascular disease. Interestingly, in people with diabetes, CHD mortality rates fell or remained stable across various regions. By contrast, HF mortality in people with diabetes did not drop over time. These findings highlight the importance of addressing excess risks of HF, especially among people with diabetes. We imagine that newer agents, like GLP-1 RAs and finerenone, which have recently demonstrated benefits for HF with preserved (HFpEF) and mildly reduced ejection fraction (HFmrEF), will be associated with drops in mortality rates in the coming years. Ensuring ever expanded access to these therapies and treatment options for HF with reduced EF remains critical, of course. |
November 2025
| Title | Author | Journal | Commentary |
| Development and validation of a type 2 diabetes mellitus prediction tool using a large Japanese regional insurance claims database | Dr. Tatsunori Satoh and Prof. Eiji Nakatani, et al. | Scientific Reports | Predictive models have tremendous potential for population-wide disease management, including identifying individuals at early risk for T2D, allowing timely interventions to reduce the incidence and burden of T2D. However, existing models trained on specific subpopulations are limited in their generalizability to a broader population. This study aimed to address this limitation by developing a predictive model for T2D risk using a large, comprehensive Japanese cohort (n=463,248). The study included patients across the lifespan and of varying degrees of health. The model achieved a Harrell’s c-index of 0.656 – correctly predicting T2D risk profiles 66% of the time (a Harrell’s c-index of 0.5 means the model’s predictions are better than a coin flip) and exhibiting “modest predictive performance,” as described by the authors. |
| Prevalence of Excess Adiposity by Body Mass Index Category Among US Children and Adolescents | Mr. Ashwin Chetty and co-authors from Yale, Drs. James Nugent, Ada Fenick, and Mona Sharifi | JAMA Pediatrics | BMI may underestimate or overestimate adiposity, leading an international commission to recommend confirming excess adiposity when diagnosing obesity. However, in adults, obesity prevalence based on BMI alone changes little with an adiposity confirmation. Therefore, the recommendation’s clinical utility in youth remains uncertain. To address the youth population, authors compared the prevalence of excess adiposity (n=3,194) in US youths aged 8 to 19 years across BMI categories. BMI-defined obesity (BDO) was defined as a BMI in the 95th percentile or greater for age and sex. Commission-defined obesity (CDO) was defined as having excess adiposity based on either 2 elevated anthropometric measures (BMI, waist to height ratio, or waist circumference) or an elevated body fat percentage. Interestingly, the prevalence of BDO was almost identical to the prevalence of BDO with excess adiposity, across age, sex, and race and ethnicity – suggesting that among youth with BDO, there is limited clinical utility in confirming excess adiposity. While the overall prevalence of CDO was more than double BDO, widespread body-fat measurements are currently impractical, and the clinical significance of elevated body fat percentage in youth with overweight or normal BMI is unclear. |
| Glucagon-Like Peptide-1 Receptor Agonists and Pay-Per-Click Direct-to-Consumer Advertising | Dr. Daniel Eisenkraft Klein | JAMA Network | The study analyzed publicly available data from April 2022 to March 2024 on Ozempic (semaglutide) search advertising and revealed that approximately $7.5 million was invested in more than 15,000 keywords that generated 2.4 million paid visits to Ozempic.com. Nearly one-quarter of keywords (23%) did not include the brand name, and many referenced competitors such as Trulicity (dulaglutide) and Mounjaro (tirzepatide) or targeted weight-loss-related search results (e.g., “Ozempic for weight loss”). The authors speculated on whether PPC advertising could prioritize promotional material over unbiased search results and might potentially expose consumers to messaging about non-FDA-approved uses, although they noted that it was hard to generalize with the limited data and relatively modest spending in this case study. |
| Liraglutide in Acute Minor Ischemic Stroke or High-Risk Transient Ischemic Attack With Type 2 Diabetes | Dr. Huili Zhu et al. | JAMA | Conducted across 27 hospitals in China from June 2019 to December 2023, the LAMP trial (n=636) studied the safety and efficacy of liraglutide in people with T2D and minor acute ischemic stroke (AIS) or high-risk transient ischemic attack (TIA). The study randomized participants within 24 hours of symptom onset to either the liraglutide or control group. The liraglutide group received treatment once-daily for 90 days (0.6 mg for the first week, which increased to 1.2 mg in the second and 1.8 mg until Day 90). Within 90 days, 8% of participants in the liraglutide group and 14% in the control group experienced stroke recurrence (hazard ratio: 0.56; p=0.02). Results also showed that a significantly higher proportion of patients in the liraglutide group (87%) met the functional outcomes compared to the control group (78%). Overall, the trial suggests that liraglutide might reduce stroke recurrence and health outcomes in people with T2D and minor AIS or high-risk TIA. |
| Cost-Effectiveness of MASH Diagnosis and Management Approaches Among Those with Type 2 Diabetes | Prof. Jeffrey Lazarus et al. | JAMA Network Open | Using WHO-CHOICE cost-effectiveness framework, the team simulated liver disease progression across 10 fibrosis stages in cohorts from 12 countries, including the US, Germany, Japan, and Brazil. The models assumed a baseline mean A1c levels of 7.2% and MASH prevalence of ~32% in this population. Across modeled regions, it was found that screening followed by intensive lifestyle interventions (ILIs) was cost-effective in all countries, while ILIs plus semaglutide and ILIs plus resmetirom were cost-effective in 11 and seven countries, respectively. Although standard care without systemic screening had the lowest cost-effectiveness ratios in eight settings, the findings strongly support the importance of structured screening and intervention to improve long-term liver and cardiometabolic outcomes. Notably, they found that following systematic screening added ~40-80 quality-adjusted life-years (QALYs) per 100,000 adults at modest incremental cost. The authors called for WHO to formally recognize MASH within pathways of diabetes management, through FIB-4 screening and ILI programs. We’d love to know your thoughts on what are the best ways of doing this. |
| Association of A1c and an updated glucose management indicator (uGMI) with incident diabetic retinopathy in adults with type 1 diabetes: A longitudinal study | Dr. Viral Shah, Dr. Yongjin Xu, and Dr. Timothy Dunn et al. | Diabetologia | The study compared the performance of A1c and uGMI in predicting diabetic retinopathy (DR) risk in adults with T1D. GMI converts mean CGM glucose into an A1c‑like percentage, and uGMI further adjusts that calculation for population red blood cell factors to better reflect glycemia‑related risk. Using up to seven years of CGM data, the investigators found that uGMI showed a stronger association with DR (mutual information score 0.148) than A1c (0.078). Interestingly, combining uGMI and A1c offered only marginal, non-clinically meaningful improvement in prediction accuracy. Researchers also evaluated the performance of other CGM-derived metrics, concluding that uGMI and mean glucose (which also performed better than A1c) were most closely linked to DR, while others (such as TIR, Time in Tight Range, or glucose variability) added little independent value. Furthermore, machine learning (ML) analyses found that while DR risk rose comparably when comparing participants in the lowest and highest quintiles of uGMI and A1c, uGMI predicted a significantly greater jump in DR risk between those in the middle quintiles compared to A1c, suggesting that uGMI can identify sharper changes in DR risk than A1c. The authors concluded that these findings support uGMI’s potential use as a complementary or alternative metric in assessing complication risk in people with T1D. |
| INHALE-1: A Multicenter Randomized Trial of Inhaled Technosphere Insulin in Children With Type 1 Diabetes | Dr. Michael Haller | Diabetes Care | e were glad to see these results published in Diabetes Care after topline findings were announced by MannKind last December. Safety was demonstrated with no significant difference in forced expiration volume between the two groups. The Afrezza group also reported greater patient satisfaction than with standard care. Notably, topline results from the full 52-week INHALE-1 study were shared just last week at ISPAD demonstrating a stable glycemia and safety profile, further supporting MannKind’s supplemental Biologics License Application (sBLA) for a pediatric indication for Afrezza accepted in 3Q25, with a PDUFA date set for this coming May. We were struck by Afrezza growth once again on seeing the latest quarterly results and we love seeing this steady growth. |
| Association of the Age at Type 2 Diabetes Onset With Diabetes Progression | Ms. Seyedeh Forough Sajjadi | Diabetes Care | The study examined the age of T2D diagnosis and rate of disease progression during two prevention trials in the US and India in nearly 1,000 patients. It found that blood glucose, as measured by FPG and A1c, rose faster in younger-onset participants in the US despite being similar at baseline. Furthermore, kidney and heart risk profiles differed by age at onset. Specifically, younger-onset participants in the US and Indian groups had: (i) higher eGFR; (ii) lower systolic blood pressure; and (iii) lower HDL cholesterol (not significant in the Indian group). These findings suggest that T2D diagnosed at a younger age follows a more aggressive course, underscoring the need for greater prevention strategies and earlier, more intensive management. |
| Small things matter: Lack of extraislet beta cells in type 1 diabetes | Dr. Kathryn Maurrall | Science Advances | This article outlines findings from a study that sought to explain whether islet size and composition evolve in people with and without T1D. The study used immunolabeled 2D pancreas sections to characterize endocrine objects (EOs), which were defined as continuous structures containing one or more endocrine cells throughout early development. In total, the study analyzed 458 images from 250 pancreas donors using AI-assisted image analysis. Results confirmed that up to 40-50% of total EOs exist as small clusters of cells, mostly comprised of beta cells. One of the important findings from the study included the observation of an absence of small EOs in the pancreas of donors with T1D – researchers interpreted this as the susceptibility of smaller EOs to autoimmune destruction. Furthermore, the study found lower EO density in people with T1D compared to age-matched donors without diabetes, which may lead to more aggressive immune destruction and compromise the ability to build beta cell mass in young children. Overall, these observations provide insight into the pancreas structure, particularly the density and area of EOs in early development, that could help inform screening and treatment approaches for T1D. |
| Why Early Large-Scale Weight Loss Is the Future of Type 2 Diabetes Care | Prof. Naveed Sattar and Dr. John Buse | Diabetes Care | The authors said that substantial weight loss – through low-calorie diets and incretin-based therapies – soon after a T2D diagnosis can meaningfully alter long-term disease trajectories. They also outlined broader benefits, including reduced ASCVD risk, potential kidney protection, and improved quality of life – to say nothing of perhaps even prompting a pre-T2D diagnosis (i.e., a reversal). Notably, they suggest that incretin-based treatments can help patients adopt healthier behaviors by reducing “food noise.” As shown in the graphic above, their modeled three- to five-year trajectories of weight and A1c values show that early, significant weight loss reduces caloric intake, improves metabolic profiles, and increases the share of patients achieving A1c levels below 6.5%. Incretin therapies appear to sustain these gains longer through both hormonal effects and more durable weight loss. Altogether, the findings support early, intensive weight-loss strategies as a promising paradigm shift in T2D management. As pharmacotherapy evolves to support long-term adherence and guidelines continue to endorse early, aggressive intervention, we hope to see population-level glycemic improvements follow. |
| Efficacy and safety of tirzepatide added to basal insulin in patients with type 2 diabetes in China (SURPASS-CN-INS): a double-blind, multicentre, randomised, placebo-controlled, phase 3 trial | Prof. Lixin Guo et al. | The Lancet Diabetes and Endrocrinology | The authors aimed to evaluate the efficacy and safety of tirzepatide combined with basal insulin in this population based in China, noting that race-dependent effects of GLP-1 RAs have previously been demonstrated. SURPASS-CN-INS (n=257) included adult patients already taking insulin glargine who were randomized to once-weekly tirzepatide 5 mg, 10 mg, or 15 mg, or placebo. Patients receiving tirzepatide had significantly greater reductions in A1c from baseline at Week 40 than those receiving placebo (2.4% in the 10 mg group and 2.4% in the 15 mg group, virtually the same, versus a 0.9% drop [still great!] in the placebo group). The difference versus placebo was -1.48% for the 10 mg group and -1.45% for the 15 mg group - virtually the same. The most common treatment-emergent adverse events among patients receiving tirzepatide were diarrhea (26%, 37%, and 37% of participants in the 5, 10, and 15 mg groups, respectively compared to 8% in placebo), reduced appetite (29%, 25%, and 32%, respectively, compared to none in placebo), and upper respiratory tract infection (20%, 17%, and 18%, respectively, versus 16% in placebo). In all, the authors conclude that the combination of tirzepatide and basal insulin was safe, well-tolerated, and improved glycemic control. |
| SixPeaks CEO talks about $170M sale to AstraZeneca and what comes next in obesity | Mr. Kyle LaHucik | Endpoints News | The deal includes $170 million in upfront payments and up to $130 million in milestone payments. This seems like a great investment. SixPeaks, founded in 2024 with an acquisition option in place, has an “imminent” IND filing, according to CEO Mr. Philip Just Larsen, a longtime and very impressive leader in the field. The article states that the startup is advancing five programs targeting conditions including sarcopenic obesity, T2D, and MASH. Its lead antibody, SPX-001, follows Novartis’s and Lilly’s bimagrumab in blocking activin type II receptors to protect muscle while reducing fat, particularly visceral fat, in older patients with insulin resistance. SixPeaks anticipates combining its activin-targeting platform with other incretins, including GLP-1 RAs. Mr. Larsen is also Board Chair at Antag Therapeutics, which is developing a GIP antagonist similar to Amgen’s MariTide. Antag expects new clinical data “within weeks” as it prepares for a phase 2a study next year. |
| Metabolic Improvement Mediates the Causal Relationship Between GLP-1 Receptor Agonists and Myocardial Infarction | Dr. Jingkai Tong | Diabetes Care | The study aimed to explore the relationship between GLP-1 RAs and reduced risk of myocardial infarction (MI). To do so, researchers completed several statistical analyses, including Mendelian randomization (MR), two-step MR analysis, and a multivariate MR, to determine direct or indirect causality between GLP-1 receptor expression (which served as a proxy for GLP-1 RA use) and MI risk. Ultimately, higher GLP-1 receptor expression (i.e., GLP-1 RA use) was correlated with a lower risk of T2D (OR 0.94) and MI (0.97). However, metabolic improvements mediated the correlation, including: (i) A1c; (ii) BMI; (iii) triglycerides; (iv) HDL-cholesterol; and (v) systolic BP. After adjusting for such metabolic improvements, researchers did not observe a direct effect of GLP-1 receptor expression on MI (p=0.12). Thus, the present study supports the prevailing theory that GLP-1 RA protection against MI occurs primarily through metabolic improvements, with no direct effect independent of these pathways. In all, findings support prioritizing metabolic improvements to a patient’s reduce CV risk in GLP-1 RA usage, and otherwise. |
| Continuous Glucose Monitoring | Dr. Rich Bergenstal, Dr. Thomas Martens, and Dr. Roy Beck | JAMA Insights | The piece highlights how CGM complements A1c and summarizes key randomized trials demonstrating meaningful A1c reductions with CGM vs. BGM, including Dexcom's MOBILE study. The authors also review the ADA’s strong Standards of Care recommendations for CGM use, emphasizing the value of Ambulatory Glucose Profile reports in guiding clinical decision-making, and underscore how CGM empowers day-to-day self-management by allowing patients to understand the real-time impact of food, activity, and medication. While they acknowledged some limitations such as skin reactions and potential medication interferences, the authors conclude that CGM can enhance both safety and efficacy of diabetes management in people with T2D by reducing hyperglycemia, minimizing hypoglycemia, and enabling more informed personal care. |
| The Role of Adaptive and Innovative Trial Designs in Diabetes Research: A Scoping Review | Dr. Ashni Goshrani and Prof. Elif I. Ekinci | Diabetes Care | The study examined the use of various approaches to clinical research for T1D and T2D. Among nearly 400 publications screened, the authors identified six completed trials that employed an adaptive design – most of which were early-phase dose-finding studies. Four of these were under a specific protocol from INNODIA. |
| What’s Keeping the US From Better Population Health? | Dr. Seth A. Berkowitz | Diabetes Care | Using diabetes as a case study, Dr. Berkowitz argues that population health is shaped more by social policies than by healthcare itself, such as inadequate income support systems, adverse commercial drivers of health, and a fragmented, multi-payer healthcare financing system. In 2023, US health care spending reached $4.9 trillion, or 17.6% of GDP, yet life expectancy, maternal mortality, and diabetes rates remain among the worst in peer nations. Dr. Berkowitz calls for stronger social insurance, limiting monopsony purchasing power to curb prices, and a shift from insurance-based to service-based health care models to promote coordinated, longitudinal care. Ultimately, he concluded, “[w]hat’s keeping the US from better population health is us. But we could fix that.” |
October 2025
| Title | Author | Journal | Commentary |
| Prevention of type 2 diabetes through prediabetes remission without weight loss | Dr. Arvid Sandforth | Nature Medicine | In this post‑hoc analysis of PLIS, researchers found that prediabetes remission can occur even without weight loss. Among the 21% of participants who didn’t lose (or gained) weight, 22% still achieved normoglycemia, driven by improvements in insulin sensitivity, beta‑cell function, and GLP‑1-mediated beta‑cell responsiveness. Responders tended to gain subcutaneous fat, while non‑responders accumulated visceral fat. Over up to ten years, responders had a 71% lower risk of developing type 2 diabetes, underscoring that prevention strategies should prioritize glycemic targets, not weight loss alone. Read more here. |
| Lack of Association Between Hemoglobin A1c and Continuous Glucose Monitor Metrics Among Individuals with Prediabetes and Normoglycemia | Dr. Jorge Rodriguez (Brigham and Women’s Hospital) et al. | DT&T | The study cohort was comprised of people with T2D, prediabetes, and normoglycemia. Mean glucose showed the strongest association with A1c in people with T2D, which was significantly attenuated with a moderate association in those with prediabetes. Importantly, mean glucose demonstrating only a weak association with A1c in those with normoglycemia, and Time in Range showed no significant relationship. This stepwise weakening of association likely reflects physiological differences in glucose stability across the glycemic spectrum — particularly the typically high and stable TIR observed in normoglycemic individuals, which limits variability and correlation. |
| Obesity treatment with bariatric surgery vs. GLP-1 receptor agonists | Dr. Tyson Barrett (Highmark Health) and Dr. George Eid (Allegheny Health Network) et al. | JAMA Surgery | Using claims and EHR data, investigators found that two‑year costs were 23% higher for GLP‑1 RAs (~$63,500) than bariatric surgery (~$51,800). Among people with BMI ≥40 kg/m², surgery produced nearly triple the weight loss. Authors noted that chronic drug therapy drives ongoing costs, while surgery is a one‑time intervention with durable benefits. They argued surgery may merit reconsideration beyond a “last resort,” though it’s unclear whether adherence or patient preference was assessed. |
| Medication Use inT1D and the Association with Socioeconomic Disadvantage: Analysis of a National Linked Dataset | Dr. Ella Zomer | DT&T | Across the six-year period of this study, non-insulin-glucose-lowering drugs increased from 12.6% to 16.1%. Within this, SGLT-2 inhibitor use rose from 0.3% to 5.1%, and GLP-1 RA use from 0.5% to 1.8%. Polypharmacy, defined as five or more medications, remained around 55% for the entire population – who had a median age of 39 years and diabetes duration of 17 years. The study’s main conclusion pertained to socioeconomic disparities, where polypharmacy was associated with increased socioeconomic disadvantage. In the most disadvantaged areas (classified by levels of Index of Relative Social Disadvantage), 22% used non-insulin glucose-lowering drugs compared with 12% in the least disadvantaged areas. In the most disadvantaged group, polypharmacy rates stood at 59%, compared to 49% in the least disadvantaged. |
| Health care professional willingness to treat opioid use disorder vs type 2 diabetes in primary care | Drs. Lindsay Dhanani (Rutgers University) and Berkeley Franz (Ohio University Heritage College of Osteopathic Medicine) et al. | JAMA Network | Investigators presented imaginary patient profiles to 375 Ohio primary care clinicians to compare perceptions of T2D and opioid use disorder. Clinicians—average age 47, mostly physicians (51%) and nurse practitioners (≈30%)—expressed less empathy toward T2D (3.0 vs. 3.3) and viewed patients as more responsible for their condition (2.4 vs. 2.0). They rated T2D as more complex to manage but were more willing to treat it themselves (4.4 vs. 3.6), whereas they preferred to refer OUD to specialists (3.3 vs. 4.4). Perceptions did not differ by the race of the patient profiles. The findings underscore persistent provider biases toward people with diabetes. |
| User Experiences of a Bihormonal Fully Closed-Loop System Among Adults with Type 1 Diabetes in a Real-World Setting: A Qualitative Analysis | Dr. Giesje Nefs (Radboud University, the Netherlands), Prof. Frank J. Snoek (Amsterdam University Medical Center, the Netherlands), and Dr. J. Hans DeVries(Amsterdam University Medical Center, the Netherlands) et. al. | DT&T | Following up on the FREE 1 trial, the qualitative study offered a perspective on adults’ day-to-day experiences using Inreda AP, a bi-hormonal, fully closed-loop (FCL) system that automatically delivers both insulin and glucagon. Through interviews with participants, the researchers found that many described the FCL as “transformative,” freeing them from constant carbohydrate counting, while others voiced frustration with the device’s complexity, including: (i) daily glucagon changes; (ii) two sensors; and (iii) frequent alarms. Ultimately, it’s very important to say, participants reported feeling less burdened by diabetes overall – and we bet their Time in Range was better! These findings echo FREE 1’s strong quantitative outcomes (~80% TIR) while adding valuable context about user fatigue and trust. |
| Human pancreatic α-cell heterogeneity and trajectory inference analyses reveal SMOC1 as a β-cell dedifferentiation gene | Dr. Randy Kang (City of Hope) et al. | Nature Communications | Researchers at City of Hope discovered that SMOC1 plays a role in the disease by disrupting how pancreatic cells maintain their identity. Single‑cell RNA sequencing of islet cells from 26 people revealed five distinct cell types and mapped their transitions. In healthy islets, cells could mature into beta or alpha cells, but in T2D that flexibility collapsed: beta cells shifted only toward an alpha‑like state, producing glucagon instead of insulin. The team also identified a new hybrid “AB cell” population that makes both hormones. SMOC1 emerged as a key driver of these identity shifts, positioning it as a potential therapeutic target to preserve or restore beta‑cell function in T2D. |
| GLP-1 Therapeutics and Their Emerging Role in Alcohol and Substance Use Disorders (ASUD): An Endocrinology Primer | Mr. Nirupam Srinivasan (University of Galway, Ireland) and Dr. Lorenzo Leggio (NIH) et al. | The Journal of the Endocrine Society | In this review, authors highlighted that obesity and ASUD share neurological pathways involving reward circuitries, with similar alterations in the dopamine receptor signaling. While developed to treat diabetes and obesity, GLP-1 RAs modulate dopamine signaling and reward circuits in the brain, suggesting therapeutic potential in addiction. In (admittedly preclinical) studies, exendin-4, liraglutide, or semaglutide reduced consumption of alcohol, heroin, fentanyl, nicotine, and cocaine. In humans, cohort and observational studies reported lower rates of alcohol-related and opioid overdose events. In RCTs, exenatide reduced alcohol intake, while semaglutide reduced drinking and smoking in people with alcohol use disorder. Authors concluded that the field needs more RCTs focused on ASUD, as well as studies evaluating the safety and efficacy of co-administering GLP-1 RAs with existing ASUD treatments. We are really hopeful that more investment goes into this area and that GLP-1 RAs may be efficacious in treating addiction. |
| Relationship Between Metabolic and Historical Responses in People with Metabolic Dysfunction-Associated Steatohepatitis With and Without Type 2 Diabetes: | Prof. Cyrielle Caussy and Dr. Mark Hartman | Diabetes Care | The SYNERGY-NASH trial was a 52-week, randomized, placebo-controlled trial evaluating once-weekly tirzepatide (5, 10, or 15 mg) in participants with MASH and stage 2-3 fibrosis. At baseline, 59% of participants had T2D, 57% had stage 3 fibrosis, and the mean BMI was 36 kg/m2. In the present post hoc analysis, responders who demonstrated MASH resolution and fibrosis reduction also showed greater decreases in body weight (p<0.001 and p=0.023, respectively). A1c reductions were also greater among both MASH (p<0.001) and fibrosis responders (p=0.004). Lastly, liver fat reduction and improved adipose insulin sensitivity were notably improved for MASH responders. Normalization of liver fat was a key mediator of both responder outcomes. In all, tirzepatide’s effect on weight loss and metabolism appear to contribute to disease modification in MASH for this SYNERGY-NASHtrial (n=190). |
| Glucagon-Like Peptide-1 Receptor Agonist Order Fills and Out-of-Pocket Costs by Race, Ethnicity, and Indication | Prof. Ameet Sarpatwari, Mr. Mark Soto, and Dr. Ishani Ganguli | JAMA | Using electronic health records and all‑payer claims, investigators analyzed 9,848 GLP‑1 RA orders for 6,094 patients at the University of Colorado Health system between Jan 2018 and Sep 2022. When adjusted for age, six, insurance type, and neighborhood income, the study found that 60% of orders were filled within 90 days. Fill rates were lower for non-Hispanic Black and Hispanic patients compared to non-Hispanic White patients. Those with both diabetes and obesity had higher fill rates than those with diabetes or obesity only — this may be partly due to the significantly higher (2x) out-of-pocket cost and narrower insurance coverage for obesity treatment compared to diabetes. Investigators acknowledged limitations of the study, such as (i) inability to determine reasons for non-fill and (ii) a study period that preceded widespread use of newer, highly effective GLP‑1 RAs for obesity. Nonetheless, the findings emphasize the need for policymakers to consider benefit design changes to improve equitable access to GLP‑1 RAs. |
| Automated Insulin Delivery Is Associated with Reduced Hospital Admissions and Costs for Acute Diabetes Complications in Children with T1D | Dr. Mercedes Burnside, Dr. Elizabeth Davis, and Dr. Craig Taplin, et al. | DT&T | This study assessed hospitalizations and costs among 1,440 children with T1D in Western Australia using different insulin delivery methods. Compared with AID systems, adjusted hospitalization rate ratios were 2.74 for MDI and 1.62 for pump therapy (the latter not significant, reflecting the prevalence of non‑automated pumps at the time). DKA admissions were far more common than hypoglycemia across all groups—5× higher among AID users, nearly 2× among pump users, and ~2.5× among those on MDI. AID use also delivered substantial savings: ~AUD 40,000 per 100 patient‑years vs. MDI and ~AUD 25,000 vs. pump therapy. The findings add to evidence that AID systems reduce acute events and costs, supporting broader adoption in pediatric T1D. |
| Diagnosing Type 1 Diabetes before Symptoms Strike | Ms. Rachel Nuwer (NYU) | Scientific American | This recounts a history of genetic research and studies to uncover a potential genetic indicator(s) for T1D, tests to determine likelihood of T1D development, and a preventative therapy to delay progression into stage 3 T1D. An important launching point for genetic analysis came in 2004 with the Environmental Determinants of Diabetes in the Young (TEDDY) study, which looked at individuals at high genetic risk of developing diabetes. In a similar vein, in 2015 Dr. Richard Oram(University of Exeter, UK) developed a test that compared data across 67 alleles to offer risk analysis for the development of T1D; this test is still the gold standard for screening today. We have seen many initiatives to increase screening in recent years, with a goal of allowing individuals to prepare for diagnosis without DKA at onset as well as for more opportunities for disease-modifying therapies. We appreciated Dr. Nuwer’s fascinating look at the story behind this important therapy that we've covered from the very start. We’ll have more on this series over the next week leading up to World Diabetes Month. |
| Here’s a nuanced look at T1D cases worldwide | Miriam Quick, Jen Christiansen, and Jeanna Bryner | Scientific American | Given the fact that rates of T1D diagnosis are increasing globally (up to half a million people were estimated to be diagnosed this year alone), the authors urge for a more equitable distribution of life-saving technology to manage T1D. Ms. Quick et al. compared the expected lifespan of a child with T1D in UAE (76 years) to that of someone in Niger (20 years). As the authors state, “Where treatment is accessible, a diagnosis no longer amounts to a death sentence” – a compelling case to ensure that advances in T1D care are made accessible to all. We look forward to bringing you more from this series in the coming days. |
| A Cure for Type 1 Diabetes Seems Close, Thanks to New Drugs and Tech | Ms. Tara Haelle | Scientific American | The author highlighted teplizumab as an important first step toward delaying stage 3 T1D, noting that some early trial participants still haven’t progressed. Trial lead Dr. Kevan Herold suggested that better understanding disease pathways could eventually enable combination therapies, with different agents acting at different life stages to approach a true “cure.” But major challenges remain, including diagnostics, access, and cost—the full teplizumab regimen is priced at $200,000, and a single dose is unlikely to deliver the intended benefit, raising the possibility that it functions more like a chronic therapy. Looking ahead, it will be important to see how combination approaches might expand the toolkit for delaying or preventing T1D as research advances. |
| Champions of Caring | Ms. Lauren Young | Scientific American | This piece highlights the work of five remarkable women who have made outstanding contributions. Dr. Sarit Polsky (University of Colorado) and Dr. Florence Brown (Joslin Diabetes Center) have focused on improving diabetes care during pregnancy and reducing risks to infants and mothers through education and expanding access to resources. Dr. Ileana Gill (University of Miami) and her nonprofit organization, Guerreros Azules (“Blue Warriors”) have supported individuals unable to manage this 24/7 condition on their own and have trained 28 pediatric endocrinologists and nurses in Caracas, Venezuela.Dr. Kimberly Driscoll (UVA) and Dr. Danielle Hessler Jones (UCSF) have both led extensive research on the intersection of mental health and diabetes. In the EMBARK study, Dr. Jones found that individuals with T1D who participated in psychologist-led support groups experienced greater reductions in A1c levels and mental health symptoms compared to those in groups led by diabetes educators or with both a psychologist and a diabetes educator. |
| Saving the Vision of People with Diabetic Retinopathy | Ms. Liz Szabo | Scientific American | A staggering 10 million people in the US alone suffer from severe diabetic retinopathy (DR), the leading cause of blindness of working-age Americans. Treatment options for DR include GLP-1 RAs to lower blood glucose levels, anti-VEGF medications like Vabysmo and Eylea to stall early-stage DR, and laser eye surgery, which has long been used to reduce the size of blood vessels in the eyes. Despite this range of treatment options, diagnosis remains the first step, and high costs and low patient education hinder access to care for many. Ms. Szabo illustrated the impact through the story of Sterling Glass, a man from North Carolina who ultimately lost vision in both eyes due to DR. Unwavering support from friends and family allowed him to persevere, however, and find a community of individuals in a similar situation: an all-black, all-blind band known as “The Blind Boys of Alabama,” where he is now both a singer and an advocate of improving access to eye care across the country. |
| Semaglutide and cardiovascular outcomes by baseline and changes in adiposity measurements | Prof. John Deanfield (University College London, UK) et al. | The Lancet | This analysis aimed to assess how baseline and changes in adiposity measures are associated with the risk of MACE at Weeks 20 and 104. Overall, the benefits of semaglutide were consistent across all baseline weights and waist circumference. In the semaglutide arm, lower baseline weight and waist circumference were associated with lower MACE risk, while in the placebo group, lower baseline waist circumference only was linked with reduced risk of MACE. Interestingly, only the reduction in waist circumference was associated with lower MACE risk in the semaglutide group, regardless of weight loss. In the placebo group, weight loss was associated with a higher MACE risk. Ultimately, the investigators found that waist circumference reduction mediated 33% of the benefit on MACE, contributing to the growing thought that semaglutide confers cardiovascular benefits by reducing adiposity and related pathogenic mechanisms. |
| Glucagon-Like Peptide-1 Receptor Agonists and Age-Related Macular Degeneration | Dr. Abhimanyu Ahuja (Oregon Health & Science University) et al. | JAMA Ophthalmology | This retrospective EHR study (2004–2025) examined whether semaglutide or liraglutide reduced age‑related macular degeneration (AMD) risk in people with obesity but without diabetes, compared with other weight‑loss drugs. GLP‑1 RAs were linked to a substantially lower risk of developing dry AMD at five (RR 0.16), seven (RR 0.13), and ten years (RR 0.09), all highly significant. There was no difference in progression to wet AMD, which affects ~10–15% of those with dry AMD and causes rapid vision loss. Overall, the findings suggest GLP‑1 RAs may confer eye‑health benefits even in people without diabetes. |
Why the war on childhood obesity is failing Britain’s strict new curbs on junk-food marketing Could weight-loss drugs eat the world? Scientists are learning why ultra-processed foods are bad for you | Ms. Slavea Chankova | The Economist | For the first time, the prevalence of childhood obesity is now higher than the prevalence of underweight children globally, making obesity the most prevalent form of malnutrition in school-aged children and adolescents. Wealthier nations are also no longer the only “obesity capitals of the world.” Rather, ultra-processed junk foods now overcrowd nutritious alternatives in some of the world’s poorest countries. The article expanded on this evolving landscape of global obesity, which now features higher rates of overweight and obesity in low- and middle-income countries than in many high-income ones. Polynesia and Micronesia now experience the highest obesity rates (>60% of adults), with Tonga and American Samoa having the highest rates of obesity for women (81%) and men (70%), respectively. With weight loss drugs inaccessible for many people around the world, we were keen to see the prestigious publication so clearly spotlight the unrelenting public health crisis. |
| The influence of diabetic retinopathy on the risk of dementia: A nationwide cohort study | Prof. Chaeyeon Lee (Samsung Medical Center, Korea) et al. | Nature Scientific Reports | Using retrospective data from adults over 45 years in the Korean National Health Insurance Service database, researchers examined the association between diabetic retinopathy (DR) and dementia risk, accounting for diabetes severity. At baseline, 62% of participants with DR showed greater metabolic burden, with the same proportion having fasting blood glucose (FBG) ≥126 mg/dL and 46% using insulin. Over an average 11-year follow-up, individuals with DR had a 2.7-fold higher risk of developing dementia than those without DR. The association was most significant among those under 65 years, and risk of both Alzheimer’s disease and vascular dementia were elevated in individuals with DR. The authors hypothesized that shared microvascular and neurodegenerative mechanisms, such as blood-retinal breakdown and tau-related neurotoxicity, may contribute to this correlation. Overall, the findings suggest that DR may serve as an early biomarker for neurodegeneration beyond traditional glycemic markers and underscore the potential role of ophthalmic screening in dementia prevention. |
September 2025
| Title | Author | Journal | Commentary |
| Effect of marked weight loss on adipose tissue biology in people with obesity and type 2 diabetes | Dr. Dmitri Samovski (Washington University School of Medicine in St Louis), Dr. Ronald Kahn (Joslin Diabetes Center), and Dr. Sam Klein (Wash U. in St. Louis) | Diabetes Care | The authors explored adipose tissue-related factors involved in weight loss; specifically, they were interested in answering what alterations at the cell level were responsible for mediating the metabolic benefits of weight loss. Using samples from adults with obesity and T2D (n=10), the hyperinsulinemic-euglycemic clamp procedure was used on tissues before and after 16-20% loss of body weight. Ultimately, the authors concluded that weight loss increases insulin sensitivity by modifying tissue biology! The authors suggested that this was specifically achieved through changes in circulating PAI-1, leptin, HMW adiponectin, and sEV microRNAs |
| Impact of Parental First-Degree Family History of Diabetes on Diabetes Incidence and Progression During Long-term Follow-up in Diabetes Prevention Programs Outcomes Study | Dr. Samuel Dagogo-Jack (University of Tennessee Health Science Center) et al. | Diabetes Care | The study (n=3,072) analyzed the effects of first-degree family history on diabetes incidence in Diabetes Prevention Program (DPP) and Diabetes Prevention Program Study (DPPOS) participants. Results showed that having a first-degree relative with diabetes (n=1,975) significantly increased a participant’s risk of developing diabetes (HR 1.21), and biparental history (n=312) conferred an even greater hazard (HR 1.44) than maternal (n=947; HR 1.22) or paternal (n=716; HR 1.22) histories alone. Interestingly, even when controlling for DPP interventions, parental history still increased T2D risk – which was only partially explained by polygenic risk scores. Thus, Dr. Dagogo-Jack et al. suggest that rare genetic variants and environmental factors may contribute to T2D risk in people with prediabetes. Clinically, such conclusions underscore the importance of gathering detailed family history in risk assessments, which will help to identify those at elevated T2D risk who would most benefit from tailored preventative and monitoring strategies. |
| Are Pediatric Primary Care Providers Ready for Type 1 Diabetes Screening and Monitoring? A Survey From a Large, U.S. Pediatric Network | Dr. Christine March (University of Pittsburgh) et al. | Diabetes Care | Pediatric PCPs were surveyed prior to piloting a T1D screening intervention (n=106). The survey aimed to address understanding, barriers, and attitudes related to T1D screening and was prefaced with information about staging and screening. Only 30% of respondents were familiar with T1D screening, which we interpret as lots of room for upside. One question asked about thresholds for referral to a diabetes specialist/endocrinologist. Answers included: (i) before ordering diabetes-related antibodies; (ii) interpreting diabetes-related antibody results; (iii) monitoring for abnormal blood sugars once diabetes-related antibodies are detected; (iv) when abnormal blood glucoses are identified during monitoring; or (v) only when stage 3 T1D is diagnosed. PCPs tended to agree on the need for a referral to an endocrinologist, but timing was not consistent when deciding to refer before or after antibody testing. While 93% of respondents deemed preventing DKA to be a perceived benefit of early stage T1D screening, just 25% felt comfortable ordering tests. This survey revealed critical gaps in education and clinical workflow for PCPs around T1D screening as well as an ongoing need for integrated care with endocrinologists - as well as lots of opportunity ahead for TZield as education improves. |
| Real-World Clinical Impact of Using Personal Glucose Targets in a Hybrid Closed-Loop System Differs According to Age | Dr. Julia Ware (University of Cambridge, UK) | DT&T | . The study found that very young children and school-aged children were the most frequent users of personal glucose targets (>50% and >40%, respectively), while most other age groups relied on the default target (104 mg/dL; ≥65% of time). Across the cohort, higher glucose targets (>120 mg/dL) were consistently associated with Time in Range (TIR) outcomes below suggested targets, a finding that echoes real-world studies of other systems – both Insulet and Medtronic have reported that use of the lowest glucose target (110 mg/dL) alongside other recommended settings are associated with the best glycemic outcomes. Mean Time below Range remained <4% across most thresholds, except for very young children using default settings and those using the lowest settings (80-89 mg/dL). Overall, older adults achieved strong outcomes, whereas very young children and young adults required lower-than-default targets to reach TIR above 70%. |
| A Tale of Two Diseases | Dr. Maria L. Collazo-Clavell (Mayo Clinic) | NEJM | While the term “diabesity” was coined by Dr. Ethan Sims in the 1970s, therapies addressed the two separately for decades. That changed with the introduction of GLP-1-based incretin therapies, which improved glycemic and weight management simultaneously. Dr. Collazo-Clavell overviewed the evolution from early twice-daily exenatide to weekly semaglutide and dual and triple agonists like tirzepatide and retatrutide. She highlighted a study published by NEJM in June 2025 on maridebart cafraglutide (MariTide), a monthly GLP-1 agonist and GIP antagonist, which promoted weight loss and improved glycemic management. The study showed that gradual dose escalation improved tolerability, while discontinuation was more common in fixed-dose groups. Dr. Collazo-Clavell addressed several key barriers including drug cost, insurance coverage, and access, emphasizing that while incretin-based therapies are a breakthrough for obesity and diabetes, their full potential will rely on affordability and coverage as much as clinical efficacy. |
| Biases in Glucose Metrics Are Directly Related to Low Coverage of Continuous Glucose Monitoring: Insights from Diverse Populations | Prof. Simon Lebech Cichosz (Aalborg University, Denmark) et al. | DT&T | The analysis drew on more than 97,000 participants across both clinical trials and real-world datasets, including people with T1D or T2D managed by MDI, closed-loop systems, or basal insulin only. Leveraging over 35 million days of CGM data, researchers found that even small gaps in coverage (6.4%-10.1% of days) were strongly associated with lower reported TIR, with each 1% increase in daily coverage corresponding to a 0.07%-0.13% within-person rise in TIR (p <0.001). Importantly, the study suggests that missing CGM data are not likely missing “at random.” Low-coverage days likely underrepresent times of poor(er) glycemic control, leading to systematic overestimation of glycemic outcomes and, effectively, bias in TIR reporting. Although we aren’t sure we would’ve worded it the same way, we have always been fans of using CGM and A1c together. CGM, TIR, TAR, and TBR can virtually always help clinicians and patients alike understand the "quality"of A1C. This said, we believe it is much easier to understand challenges for patients if Time above Range (TAR) and Time below Range (TBR) are understood. |
| Potential Impact of Next-Generation Weight Loss Drugs on Cancer Incidence | Dr. Darren Brenner (University of Calgary, Canada) et al. | JAMA Network | Using population-based decision analytical modeling and publicly available data, the authors measured the potential impact of GLP-1 RAs on the incidence of obesity-related cancers (ORCs) in the US. The authors projected that by 2030, 18% of all ORCs among women and 14% among men would be attributable to high BMI. Over the next 25 years, cancer incidence was projected to increase by 27%. With the use of GLP-1 RAs, the model suggested that an average of 10% weight loss could prevent over 1.2 million ORC cases over the next 25 years. The largest prevention potential was projected for breast and endometrial cancers among women and for kidney and liver cancers overall. We hope these strong results will impact further research into the mechanistic impacts of GLP-1 RAs on cancer incidence. |
| Current and Future Medications for Obesity Treatment | Dr. Robert Kushner (Northwestern University), Dr. Ania Jastreboff (Yale University), and Dr. Donna Ryan (Pennington Biomedical Research Center) | JAMA Network | The authors highlight glucagon and amylin as two endogenous hormones with the greatest therapeutic potential. Glucagon has been demonstrated to increase metabolic rate in rodents, and amylin enhances satiety by acting on the brain and stomach. Using these principles, cagrilintide, a long-acting dual amylin and calcitonin receptor agonist, survodutide, a dual GLP-1/glucagon receptor agonist, and MariTide, a monoclonal antibody that inhibits the GIP receptor and is conjugated with two GLP-1 analogue peptides, are currently undergoing investigation for weight loss, alongside oral GLP-1 RAs. Other novel pathways are investigating the activin receptor found in muscle and adipose tissue to enhance muscle mass, improve insulin sensitivity, and reduce body fat. Future therapies show great promise for complementary and additive weight loss effects by targeting multiple pathways. |
| Twenty years of progress in type 1 diabetes mellitus | Prof. Thomas Kay (University of Melbourne at St. Vincent’s Hospital, Australia) and Prof. Jennifer Couper (Adelaide University, Australia) | Nature Reviews Endocrinology | The article highlights landmark trials that have transformed T1D care and management since the DCCT/EDIC studies, including the rise of CGM, AID systems, and islet transplantation. A striking development highlighted in the piece is that of stem cell-derived islets, with Vertex’s early trials showing that 10 out of 12 full-dose recipients became insulin-independent. CGM data showed an average Time in Range (TIR) of ~93%. On the immunotherapy side, teplizumab remains the only therapy proven to delay progression to stage 3 T1D, though other agents like baricitnib and golimumab are being studied. The authors discussed the potential for a future where normal glycemic levels could be achieved through combinations of AID systems, β-cell-preserving immunotherapies, and β-cell replacement, moving the field closer than ever to a functional cure. |
| Exploring the Relationship Between Newly Defined Continuous Glucose Monitoring (CGM) Metrics and the Standard CGM Metrics in 30,000 People with Type 1 Diabetes | Dr. Halis Akturk (University of Colorado) | Diabetes Technology & Therapeutics | Novel CGM-derived metrics included: (i) rebound hyperglycemia (RHyper); (ii) rebound hypoglycemia (RHypo); (iii) extended hyperglycemia (EHyper); and (iv) extended hypoglycemia (EHypo). This retrospective cohort study analyzed Dexcom Clarity data from people with T1D (n=30,000), each with a minimum of 90 days of CGM use. The authors found that rebound and extended events were common: RHyper, RHypo, and EHyper occurred more often during the day, while EHypo predominated at night, as one would expect. RHyper and RHypo were also strongly correlated with glycemic variability, while EHyper showed the strongest negative correlation with Time in Range, confirming the strengths of the new metrics. Notably, RHyper and RHypo had a stronger correlation with standard hypoglycemia metrics than standard TBR, suggesting that these new measures may offer more detailed insight into hypoglycemia risk tied to variability. The authors concluded that the most informative new metric may be the number of rebound or extended events per week, which could potentially complement standard CGM metrics when assessing an individual’s glycemic stability. |
| Adults With Type 2 Diabetes Benefit From Automated Insulin Delivery Irrespective of C-Peptide Level | Dr. Irl Hirsch (University of Washington), Dr. Roy Beck (Jaeb), and Dr. David Ahn (the Mary & Dick Alan Diabetes Center, Hoag Medical Group), et al. | Diabetes Care | The RCT, part of the 2IQP trial that supported FDA clearance of Control-IQ+ for adults with T2D, evaluated t:slim X2 with Control-IQ+ in adults with insulin-treated T2D categorized into high C-peptide (77%) and low C-peptide (23%) groups based on CMS criteria (n=254). Currently, CMS requires low C-peptide levels (or β-cell autoantibody positivity) for insulin pump coverage, excluding many with T2D from access to AID systems. Importantly, mean A1c decreased by 0.8% in both high- and low-C-peptide groups (baseline 8.0% and 8.2%, respectively). These reductions were significantly greater than in the control group (p<0.001 for high C-peptide; p<0.05 for low C-peptide) across all age groups and were consistent in participants ≥65 years old. The findings provide strong evidence that AID systems are effective regardless of baseline C-peptide level and could help inform future changes to CMS reimbursement policy. |
| Improving Time-in-Range in Type 1 Diabetes: Projecting the Clinical and Cost Implications of Automated Insulin Delivery | Dr. Sufyan Hussain (King's College London) et al. | Diabetes Care | The analysis used the IQVIA Core Diabetes Model to project how a 10 percentage-point increase in TIR impacts long-term outcomes for people with T1D. Across baseline TIR levels (50-80%), this improvement reduced the cumulative incidence of complications by: (i) 15-53% for ophthalmic; (ii) 9-48% for renal; (iii) 8-34% for neuropathic; and (iv) 10-18% for cardiovascular events. Gains in TIR also translated to modest increases in life expectancy (0.03-0.05 years) and quality-adjusted life expectancy (0.06-0.14 QALYs), with the greatest benefits seen in those starting from lower TIR. Additionally, fewer complications showed projected cost reductions of 7.5-9.9% from the perspective of England’s NHS. These findings add a valuable health economic lens to ongoing conversations about AID, and for the long-term sustainability of diabetes care. |
| Dementia risk in people with type 1 diabetes and associated risk factors: A nationwide, register-based cohort study | Dr. Milena Jancev(University Medical Center Utrecht, the Netherlands), Dr. Hertzel Gerstein (McMaster University, Canada), Prof. Hans DeVries (Amsterdam University Medical Center, the Netherlands), Prof. Naveed Sattar (University of Glasgow, UK), and Dr. Thomas T. Van Sloten (University Medical Center Utrecht, the Netherlands) et al. | Diabetes Care | Investigators conducted a cohort study (n=2,397) using the Swedish National Diabetes Register and the Swedish Total Population Register to assess the relationship between T1D and dementia risks and types. At baseline, participants were approximately 33 years old and were followed up for a median of 14 years. The study found that individuals with T1D had a two-fold higher risk of all-cause dementia, 38% greater risk of Alzheimer’s disease, ~four-fold risk of vascular dementia, and 87% increased risk of non-Alzheimer-nonvascular dementia. Beyond age, risk factors for dementia in T1D include lower education, being single, higher blood pressure, higher A1c, history of cardiovascular disease, and longer diabetes duration. These findings complement a session from EASD, which showed that dementia is associated with older ages and diabetes. |
| Real-World Effectiveness of the MiniMed 780G Advanced Hybrid Closed-Loop System for People ≥65 Years with Type 1 or Type 2 Diabetes in the United States | Dr. Robert Vigersky (Medtronic) et al. | DT&T | The authors used CareLink data from US adults older than 65 years (n=8,542) and found that mean TIR was 78% with GMI 6.8%. Among the 32% using the recommended optimal settings (100 mg/dL glucose target, two-hour active insulin time), TIR rose to 82% and TITR to 56%, while TBR remained <1%. Results were consistent across T1D and T2D and for those over 75 years. These findings show that MiniMed 780G can help older adults meet consensus glycemic targets without added hypoglycemia risk. The data also strengthens ADA recommendations for AID systems for individuals with T1D while highlighting gaps in CMS clinical coverage criteria for those who are Medicare eligible. |
| The future of type 1 diabetes therapy | Prof. Anette-Gabriele Ziegler (Institute of Diabetes Research at Helmholtz Munich, Germany), Prof. Eda Cengiz (UCSF), and Prof. Thomas W H Kay (University of Melbourne, Australia | The Lancet | The publication outlined multiple significant areas of progress in the T1D landscape, including the approval of Tzield (teplizumab) in late 2022 for delaying the clinical onset of T1D for approximately two years in people aged ≥8 years. Although Tzield is not yet approved for stage 3 T1D (the stage at which clinical diagnosis typically takes place), it has shown promising results in preserving insulin secretion (and is also currently under study to expand its use for children aged ≤8 years). As well, the authors note stem cell therapies as an important breakthrough, especially as an alternative approach for islet transplantation. Some of these developments include Vertex’s VX-880, as well as an autologous induced pluripotent stem cell that demonstrated efficacy in one patient. Finally, the authors elaborated on AID systems and new-generation insulins (e.g., ultrarapid-acting insulin, once-weekly insulin, inhaled insulin) that have helped improve clinical outcomes and quality of life for people living with diabetes. Alongside these advancements, the authors advocated for the need to expand coverage for diagnostics and interventions, and emphasized the importance of social determinants of health to improve treatment access. Additionally, they urged a shift in T1D care toward more personalized immunotherapies, referring to trial analyses that have shown greater efficacy of treatment across specific genes and phenotypes. Ultimately, with existing developments and emerging breakthroughs, they shared enormous hope for improving diabetes management and effective care for people with T1D. |
| Type 2 Diabetes Remission: A Systematic Review and Meta-analysis of Nonsurgical Randomized Controlled Trials | Dr. Diana Sherifali (McMaster University, Canada) et al. | Diabetes Care | There was a 1.75-fold likelihood of achieving T2D remission compared to control for patients using a multimodal pharmacological approach including metformin, SGLT-2 inhibitors, and insulin along with diet and exercise (n=1,488). For patients using a diet-based approach (n=6,433; either total diet replacement, very low-calorie diets, or some combination of diet and exercise), there was also a 5.8-times higher likelihood of achieving remission compared to control. However, the likelihood of maintaining remission over time was lower when using only a lifestyle-based approach. Interestingly, seven pharmacotherapy-based studies did not find a significant change in A1c compared to control, potentially due to attention given to placebo arms during RCTs; five of these studies demonstratedsignificant reductions in body weight compared to control, unsurprisingly to us, given valuable clinician attention. Finally, in an encouraging pricing analysis, one study indicated that participants in the treatment group had a 77% reduction in overall medication costs due to a reduced perceived need for medication compared to a 3% reduction in the control group. We do wonder if cardioprotection and renal protection and liver protection are being assessed optimally for patients in all the cost reduction analyses. In all, the pursuit of T2D remission by various interventions has demonstrated significant physiological and expenditure benefits for patients and certainly is something we like seeing when complications outcomes are considered. |
| Development and Internal Validation of the Multiethnic Type 2 Diabetes Outcomes Model for the US (DOMUS) | Dr. Aaron Winn (University of Illinois Chicago) et al. | Diabetes Care | Investigators developed and validated the DOMUS, a microsimulation model of T2D progression that accounts for the racial, ethnic, and social diversity of the US population. The real-world cohort included newly diagnosed adults with T2D (n=129,000) from Kaiser Permanente Northern California between 2005 and 2016, who were followed for 1-12 years. The mathematical model tracked 17 outcomes spanning microvascular and macrovascular complications, dementia, mortality, and more. Following data calibration, simulated outcomes were found to be closely aligned with observed empirical results across event rates and biomarker trajectories. The authors concluded that DOMUS represents an important step forward by integrating social determinants of health to adequately capture disparities in diabetes management. They underscored the model’s potential for use in long-term comparative and cost-effectiveness analyses, policymaking, and health system planning, as well as to guide interventions in diverse populations. |
| Discontinuation of Semaglutide Among Older Adults with Diabetes in the US and Japan | Drs. Kosuke Inoue (Beth Israel Deaconess Medical Center, Boston, MA), et al. | JAMA Cardiology | Investigators used Medicare claims (2018-2022) and Japan’s DeSC database (2018-2023) to evaluate trends in GLP-1 RA discontinuation among older adults (≥65 years) with diabetes. The study included 327,074 patients (318,543 in the US and 8,531 in Japan) who were 72 years old at baseline, and a little over half female. After one year of Ozempic(injectable semaglutide) initiation, a large proportion – 60% of US patients and 31% of Japanese patients – discontinued all GLP-1 RAs. A smaller percentage – 3% of US patients and 10% of Japanese patients – switched to Rybelsus (oral semaglutide) or other GLP-1 RAs. Clinically, those with hypertension, obesity, or prior use of GLP-1 RA were less likely to discontinue, while, surprisingly to us, those with chronic kidney disease, heart failure, stroke, depression, or dementia were more likely to discontinue. By insurance type, those with dual Medicare and Medicaid enrollment or Medicare Advantage, which generally offer lower out-of-pocket medication costs, were less likely to discontinue. We know that better titration can help so many with better "persistence" ... here's hoping that there can be better strategies ahead to keep more people with T2D looking ahead successfully on GLP-1. |
| Effects of tirzepatide on weight management in patients with and without diabetes | Dr. Eduardo Cerchi (Universidade Evangélica de Goiás, Brazil) et al. | International Journal of Obesity | Investigators analyzed five RCTs in more than 2,000 people with diabetes (n=2,174) and five RCTs in people nearly 4,500 people (n=4,476 to be exact) without diabetes and with obesity or who were overweight that compared tirzepatide to placebo. Tirzepatide conferred a mean weight loss of 12% (vs. 3% with placebo) in people with diabetes and 17% (vs. an increase by 2% with placebo) in people without diabetes. Likewise, tirzepatide significantly increased the proportion of achieving ≥5% (over 70% achieved this level), ≥10% (nearly 50% reached this level), and ≥15% (just under 30% reached this level) weight loss, compared to placebo, especially among those without diabetes. Predictably, and happily, both groups experienced similar reductions in blood pressure and improvements in lipid profiles with similar safety outcomes. And a bit surprisingly, both groups experienced virtually the same A1c change. |
| Prevention of type 2 diabetes through prediabetes remission without weight loss | Dr. Arvid Sandforth (German Center for Diabetes Research, Germany) | Nature Medicine | This post-hoc analysis of the large, multicenter, randomized, controlled Prediabetes Lifestyle Intervention Study (PLIS) demonstrates that prediabetes remission is possible even without weight loss or even with weight gain. Remission also protects against incident T2D. The mechanisms of this effect are improved insulin sensitivity and beta cell function as well as increments in beta-cell-GLP-1 sensitivity. Of the 1,105 individuals originally included in PLIS, 21% did not lose (or even gain) weight during the year of the intervention. Of these, 22% returned to a normal glycemic range, that is, were designated “responders” while 78% were non-responders. While non-responders increased visceral adipose tissue mass, responders increased adipose tissue in subcutaneous depots. Overall, more non-responders than responders developed T2D, leading to a relative risk reduction of 71% in responders over the period of up to ten years. These findings emphasize the need to include glycemic targets in current clinical practice guidelines for T2D prevention, which have more recently focused on weight loss as the primary form of prevention. We are always very intrigued, of course, by combination approaches. |
August 2025
| Title | Author | Journal | Commentary |
| Medicare, Medicaid plan to experiment with covering weight loss drugs | Ms. Paige Cunningham | Washington Post | Ms. Paige Cunningham of the Washington Post reported, “Medicare, Medicaid plan to experiment with covering weight loss drugs,” on a proposed five-year pilot allowing Medicare Part D plans and state Medicaid programs to voluntarily cover GLP-1 RAs — including Ozempic, Wegovy, Mounjaro, Zepbound, and orforglipron (pending 2026 approval) — for “weight management” purposes. The proposal revives a push from the Biden administration to expand obesity treatment coverage under public insurance. The experiment is set to launch in April 2026 for Medicaid and January 2027 for Medicare, coordinated through the Center for Medicare and Medicaid Innovation. |
| Glucagon-Like Peptide-1 Receptor Agonist Eligibility Among US Adolescents and Young Adults | Mr. Ashwin Chetty (Yale University) et al. | JAMA Pediatrics | JAMA Pediatrics published today a study titled, “Glucagon-Like Peptide-1 Receptor Agonist Eligibility Among US Adolescents and Young Adults,” by our very own Close Concerns alumnus Mr. Ashwin Chetty (Yale University) et al. The study included NHANES data on US adolescents aged 12 to 17 years and young adults aged 18 to 25 years who met the FDA eligibility criteria for GLP-1 RA treatment. The study sample found 572 adolescents and 590 young adults eligible for treatment, which translates to nearly 5.8 million adolescents and 11 million young adults. Among adolescents, 99% were eligible for obesity treatment with or without diabetes, and 0.8% for T2D alone. The indication among young adults was 88% for obesity with or without diabetes, and 12% for BMI ≥27 kg/m2 with a weight-related condition with or without diabetes. Additionally, adolescents eligible for GLP-1 RAs included 40% covered by Medicaid, 41% with private insurance, and 7.2% without insurance. Young adults included 21% covered by Medicaid, 49% with private insurance, and 19% without insurance. Furthermore, while 92% of adolescents reported having access to routine healthcare, only 68% of young adults reported having this option – not surprising given the paucity of jobs with strong benefits for young people in the US. Given the prevalence of cardio-kidney-metabolic risk factors in both groups, these findings highlight the importance of expanding coverage of anti-obesity medications like GLP-1 RAs and improving barriers to routine care – as well, of course, as going further upstream and putting in place interventions so that obesity itself declines. |
| Survival of Transplanted Allogenic Beta Cells with No Immunosuppression | Dr. Per-Ola Carlsson (Uppsala University) et al. | NEJM | NEJM published Monday an article titled, “Survival of Transplanted Allogenic Beta Cells with No Immunosuppression,” by Dr. Per-Ola Carlsson (Uppsala University) et al. This article reported results from the 12-week trial of UP421, a human pancreatic islet cell therapy developed from Sana Biotechnology’s hypoimmune technology. The trial studied whether UP421 could be transplanted safely and help insulin production in people with T1D without immunosuppressive therapies. In a 42-year-old male (yes, n=1) who has been living with T1D for over three decades, intramuscular transplantation of UP421 was safe and well-tolerated. Additionally, the cells were shown to evade any immune response, as well as secrete insulin in a glucose-dependent manner. Of note, the participant showed no detectable C-peptide at screening, but at Weeks 4, 8, and 12, C-peptide increased in response to consuming liquids with fats, protein, and carbohydrates. PET-MRI also visually confirmed the functional pancreatic islet grafts at Week 12. These results demonstrate that pancreatic islets modified with hypoimmune technology could help restore insulin production without immunosuppression, marking a significant step for a functional cure for people with T1D. Sana Biotechnology reinforced these results in its press release, sharing plans to file an IND as early as 2026 for SC451, a next-generation pancreatic islet therapy. |
| The Heterogeneity of Type 1 Diabetes: Implications for Pathogenesis, Prevention, and Treatment | Dr. Carmella Evans-Molina (Indiana University) et al. | Diabetes Care | Diabetes Care published an article last week titled, “The Heterogeneity of Type 1 Diabetes: Implications for Pathogenesis, Prevention, and Treatment,” by Dr. Carmella Evans-Molina(Indiana University) et al. The paper summarizes the current understanding of the heterogeneity of T1D, reviewing key factors contributing to the development and progression of the disease, as well as knowledge gaps and opportunities to create personalized treatments. Some of the points include how autoantibodies provide insight into the progression of T1D, but significant variability remains in determining such factors. Additionally, sex plays a significant role – while there’s a roughly equivalent risk of males and females developing T1D at a young age, males face a higher incidence after puberty. Interestingly, this trend differs from many other autoimmune diseases, suggesting the potential involvement of beta-cell function and sensitivity. Heterogeneity also extends to patterns of C-peptide secretion and metabolic trajectories that indicate differences in insulin beta cell mass and insulin sensitivity. Furthermore, variation across pancreatic phenotypes, including pancreatic volume and exocrine dysfunction, remains an area for exploration. The authors emphasize the importance of further understanding the heterogeneity of T1D to study new therapies and develop more tailored treatments. They note that the field is at an “important crossroad,” facing challenges of expanding knowledge and the opportunity to build on emerging research for disease-modifying treatments and beta cell replacement. |
| Continuous Glucose Monitoring Metrics Predict All-Cause Mortality in Diabetes: A Real-world Long-term Study | Dr. Tomoki Okuno (University of California Los Angeles) et al. | Diabetes Care | A study published yesterday in Diabetes Care by Dr. Tomoki Okuno (University of California Los Angeles) et al. called, “Continuous Glucose Monitoring Metrics Predict All-Cause Mortality in Diabetes: A Real-world Long-term Study,” demonstrates the power of CGM metrics for predicting all-cause mortality in diabetes. The authors suggest that CGM may better capture long-term risk of glucose fluctuations and periods of hypo- and hyperglycemia compared to A1c. In this retrospective cohort study of veterans with diabetes (n=2,752; T1D: 35%, T2D: 65%), Dexcom CGM data were taken from the Veterans Affairs Healthcare System. All-cause mortality was assessed over five years from the date of CGM initiation. During the five-year study duration, there were 407 deaths. In each Multivariable Cox model, higher mean glucose, Time above Range, coefficient of variation, and glycemic risk index were all significantly associated with higher mortality. Lower Time in Range was also associated with elevated five-year mortality (p<0.01). Associations remained significant even after adjusting for A1c. In participants with low A1c values, the association between coefficient of variation and mortality was particularly strong. The authors concluded that the ability to capture these glucose fluctuations is a valuable tool to predict long-term complication and mortality risk. As use of CGM expands, evidence such as the work of this study will continue to demonstrate the strength of CGM metrics and help improve long-term outcomes. |
| Diabetes-Related Distress and Glycemic Dysregulation in Everyday Life With Type 1 Diabetes: Which Comes First? | Dr. Jeffrey Gonzalez (Albert Einstein College of Medicine) et al. | Diabetes Care | Diabetes Care published an article right around ADA titled, “Diabetes-Related Distress and Glycemic Dysregulation in Everyday Life With Type 1 Diabetes: Which Comes First?” by Dr. Jeffrey Gonzalez (Albert Einstein College of Medicine) et al. This observational study (n=182) focused on the relationship between glucose levels and “diabetes-related distress,” assessed through surveys, among adults with T1D. Participants wore blinded CGMs for 14 days and completed five to six ecological momentary assessment (EMA) surveys per day. Results showed that the survey ratings were significantly associated with the questionnaire data for diabetes-related distress, well-being, functional and mental health, and quality of life. Additionally, higher mean glucose and less TIR were found to predict greater distress levels. On the other hand, while greater distress levels predicted less Time below Range, they actually didn’t predict any other CGM metrics, at least that could be seen in a trial of this size. Those who have closed look typically get more TbR due to exercise, so we'll be eager in our follow up to hear more on this! |
| The Forces Reshaping America’s Health Landscape for People With Diabetes—This Is Not About DEI, This Is About Whether People Live or DIE | Drs. Cheryl Anderson (University of California San Diego), John Buse (University of North Carolina Chapel Hill), Steven Kahn (University of Washington), and Elizabeth Selvin (Johns Hopkins University) | Diabetes Care | “The Forces Reshaping America’s Health Landscape for People With Diabetes—This Is Not About DEI, This Is About Whether People Live or DIE” was published Friday in Diabetes Care by Drs. Cheryl Anderson (University of California San Diego), John Buse (University of North Carolina Chapel Hill), Steven Kahn (University of Washington), and Elizabeth Selvin (Johns Hopkins University). The editorial warns that recently enacted US policy changes could reverse decades of progress in diabetes care and health inequity. Specifically, the piece examines effects on access to care, research funding, and health outcomes for PWD. Among the developments discussed is the passage of the “One Big Beautiful Bill,” which includes: (i) cuts to Medicaid, SNAP, and other ACA protections; (ii) adjustments to out-of-pocket costs for older adults, low-income families, and those with chronic illnesses; and (iii) tariffs that could affect prescription drug prices. The editorial also notes proposed reductions to NIH and CDC budgets, withdrawal from the WHO, and potential changes to nonprofit advocacy regulations as factors that might influence innovation and access to care in the States. The piece closes with a call for the scientific and clinical community to ensure evidence-based policy remains central to improving outcomes for PWD. |
| The world needs more than drugs to fight obesity | Mr. Lars Fruergaard Jørgensen | The Economist | The Economist published today an opinion piece by former Novo Nordisk CEO Mr. Lars Fruergaard Jørgensen titled, “The world needs more than drugs to fight obesity,” in which he describes the limitations of pharmaceutical solutions in addressing the global obesity crisis. Drawing on his eight years leading Novo Nordisk, Mr. Jørgensen argues that obesity drugs, though promising, cannot reverse this epidemic on their own. With projections published by the Lancet estimating more than half of adults and one in three children are expected to be overweight or obese by 2050, he urged for society-wide prevention efforts. Given that obesity is a disease impacted by socioeconomic, environmental, and biological forces, Mr. Jørgensen advocated for public policies that minimize obesity risk. He also emphasized the need to treat interconnected cardiometabolic diseases in tandem rather than in silos. He concluded with the critical nature of prevention, highlighting the Novo Nordisk’s Childhood Obesity Prevention Initiative, a multi-city study aiming to inform global prevention frameworks. Mr. Jørgensen called for society to seize the moment to redefine how obesity is understood and addressed, shifting focus to coordinated and holistic care. While he acknowledged the immense challenge ahead, he also expressed optimism that, guided by stronger science and smarter policies, future generations can drive lasting change. |
| GLP-1 Receptor Agonists and Sight-Threatening Ophthalmic Complications in Patients With Type 2 Diabetes | Dr. David Ramsey (UMass Chan–Lahey School of Medicine) et al. | JAMA | One large retrospective cohort study (n=185,066) of adults with T2D who were prescribed treatment with GLP-1 RAs found that GLP-1 RA use was associated with a slight increased incidence of diabetic retinopathy (DR) (HR: 1.07; 95% CI: 1.03-1.011). The study also found, in a subgroup analysis (n=32,695) of patients with pre-existing DR, that GLP-1 RA use was associated with a significantly lower risk of sight-threatening complications, such as vitreous hemorrhage (HR: 0.74; 95% CI, 0.68-0.80), neovascular glaucoma (HR: 0.78; 95% CI, 0.68-0.88), and blindness (HR: 0.77; 95% CI: 0.72-0.82). Given that DR is one of the leading causes of blindness in the US and around the globe, regular eye monitoring in patients receiving these therapies remains important. This study found no significant increase in the risk of nonarteritic anterior ischemic optic neuropathy (NAION). |
| Semaglutide or Tirzepatide and Optic Nerve and Visual Pathway Disorders in Type 2 Diabetes | Dr. Lindsey Wang (Case Western Reserve University School of Medicine) et al. | JAMA | Another cohort study (n=159,398) of adults with T2D, treated with either semaglutide or tirzepatide, suggested that GLP-1 RAs were associated with an increased risk of NAION (HR: 1.76; 95% CI, 1.01-3.07) – although only just meeting the 95% confidence interval. Though the absolute risk for NAOIN was low (0.04%) after a two-year follow up, a conservative read of the findings underscores the need for monitoring of optic nerve health in patients prescribed these GLP-1 RAs. |
| Incidence of type 1 diabetes in children before, during, and after the COVID-19 pandemic: 38-year analysis in Southwest Germany | Dr. Julian Ziegler (University Hospital Tübingen, Germany) et al. | Diabetes Care | Diabetes Care published an article yesterday, “Incidence of type 1 diabetes in children before, during, and after the COVID-19 pandemic: 38-year analysis in Southwest Germany,” by Dr. Julian Ziegler (University Hospital Tübingen, Germany) et al. Researchers analyzed T1D incidence trends in children under 15 years between 1987-2024 using data from the Baden-Württemberg Diabetes Registry (DIARY; n=11,797), which sure looks like a very impressive registry. Should we have a diabetes registry here in the US? As shown in the figure below, between 1987-2008, the incidence of T1D increased exponentially from 10 to 23 per 100,000 children, reflecting an annual increase of 4%. Since then, the incidence has remained constant until 2021, consistent with findings from other countries: Finland, Norway, Australia, and Scotland. In 2021 and 2022, the incidence appears to have increased a whopping 32% to 31 per 100,000 children, especially among children between 5-9 years, likely due, the authors say, to the SARS-CoV-2 infection, weight gain, or immune activation. OK. Those are all pretty different. This increase is consistent with previous findings ("JAMA Open Network publication finds COVID-19 infection is associated with a 17% increased risk of incident diabetes") that report a 17% increased risk of incident type 1 and type 2 diabetes, and adds to the ongoing debate on the role of the SARS-CoV-2 virus in the pathogenesis of T1D. Importantly, researchers in yesterday's Diabetes Care piece found the incidence normalized after 2023, suggesting at least a temporary shift - to what this may be attributed, we aren't sure (again, lots of variability) but we are checking with the authors, and the brilliant Ziegler family. |
| Cost Analysis of the FreeStyle Libre Systems in People with Type 2 Diabetes Mellitus on Basal Insulin with Poor Glycemic Control: A Spanish Perspective | Dr. Francisco Javier Ampudia-Blasco (University Clinic Hospital of Valencia) et al. | Diabetes Technology & Therapeutics | Diabetes Technology & Therapeutics published “Cost Analysis of the FreeStyle Libre Systems in People with Type 2 Diabetes Mellitus on Basal Insulin with Poor Glycemic Control: A Spanish Perspective,” by Dr. Francisco Javier Ampudia-Blasco (University Clinic Hospital of Valencia) and colleagues. The study used a model to estimate how switching from self-monitoring of blood glucose (SMBG) to FreeStyle Libre CGM systems might affect healthcare costs for adults in Spain with T2D (n=1,000), A1c >8.0%, and on basal insulin. SMBG was assumed to require 2.5 strips (€0.57/$0.57 each) and 2.5 lancets (€0.14/$0.16 each) per day, with annual rates of 2.5 severe hypoglycemic events (SHEs), 17.0 non-SHEs, and 0.0025 DKA events per patient. FM reduced strip and lancet use by 83%, acute events by 58%, and DKA by 68%. Annual costs per patient were €3,300 ($3,861) with SMBG and €2,320 ($2,714) with GM, with a savings of ~€980,000 (~$1.1 million) across 1,000 patients. Even when strips and lancets were free, FM saved hundreds of thousands annually. The authors concluded the FreeStyle Libre system could lower acute event rates, reduce long-term complications, and meaningfully cut costs for the Spanish health system, especially in high-risk, poorly controlled T2D. |
| Weight-loss weariness and Trump threats wipe $250bn off Novo Nordisk and Eli Lilly | Ms. Hannah Kuchler and Mr. Patrick Temple-West | Financial Times | A striking piece in the Financial Times noted that Novo Nordisk and Lilly have together lost $252 billion in market capitalization so far in 2025, reflecting growing investor caution around obesity drugs. Novo Nordisk is down 49% this year (-$166B) and nearly two-thirds below its June 2024 peak, while Lilly has fallen 11% (-$86B) following trial results for its oral GLP-1 candidate, orforglipron. The authors attributed the declines to intensifying political risks, as both companies recently received letters from President Trump demanding US price cuts under threat of tariffs and pricing policies. Large shareholders are already feeling the impact, with Norway’s $2 trillion oil fund reporting a $1.2B loss on its Novo Nordisk stake in 1H25. Beyond these two companies, the top 10 US and European pharma groups have lost $128B in market value this year, despite solid earnings, as investors shift capital toward sectors like AI. This sell-off highlights that obesity franchises are facing significant impacts from political pressure and competitive trial outcomes. |
| Weighing the risk of GLP-1 treatment in older adults: Should we be concerned about sarcopenic obesity? | Dr. Konstantinos Prokopidis (University of Liverpool, UK) et al. | Journal of Nutrition, Health, and Aging | The Journal of Nutrition, Health, and Aging published last week an article titled, “Weighing the risk of GLP-1 treatment in older adults: Should we be concerned about sarcopenic obesity?” by Dr. Konstantinos Prokopidis (University of Liverpool, UK) et al. The review outlines how GLP-1 RAs have been a key development for weight management, but questions remain about the effect on muscle mass. These points are especially relevant as studies have shown that in adults with or without T2D, 46%-65% of those receiving GLP-1 RAs discontinued treatment within 12 months. Additionally, those discontinuing semaglutide or tirzepatide treatment have been shown to regain approximately 10 kgs (22 lbs) over 48 to 52 weeks. Building on these findings, the study authors suggest that rapid weight regain may promote higher proportion of adipose tissue accumulation compared to lean mass, increasing the risk for sarcopenic obesity risk in adults. They use the phrase “weight cycling” to describe weight loss with GLP-1 RAs and associated muscle loss, coupled with fat regain post-treatment discontinuation. Overall, the authors encourage the need for longitudinal research to develop preventative strategies and mitigate risks of sarcopenic obesity, especially in those with low initial muscle mass. |
| Ultra-processed Foods and Diet Quality in Association with Long-term Weight Change and Progression to Type 2 Diabetes Among Individuals with a History of Gestational Diabetes Mellitus — A Prospective Study | Dr. Cuilin Zhang (National University of Singapore) et al. | Diabetes Care | Diabetes Care just published an article called “Ultra-processed Foods and Diet Quality in Association with Long-term Weight Change and Progression to Type 2 Diabetes Among Individuals with a History of Gestational Diabetes Mellitus — A Prospective Study,” by Dr. Cuilin Zhang (National University of Singapore) et al. In women with prior GDM (n=4,207), food frequency questionnaires every four years and the Alternative Healthy Eating Index-2010 (AHEI) scores were used to assess the impact of ultra-processed food (UPF) consumption and diet quality on long-term weight change and T2D progression. Women in the highest UPF intake group gained 1.7 kg (~3.6 lbs) compared to 0.5 kg (~1.1 lbs) in the lowest group. T2D risk rose most in the third quartile of UPF intake, with a 25% higher risk observed compared to the lowest group. Only those who reduced or stabilized their UPF intake and increased AHEI maintained weight over four years. These findings underscore minimizing UPF consumption as a key strategy for weight management and T2D prevention in this high-risk population. |
| Continuous Glucose Monitoring Metrics and Pregnancy Outcomes in Women With Gestational Diabetes Mellitus: A Secondary Analysis of the DiGest Trial | Dr. Laura Kusinski (University of Leicester, UK) et al. | Diabetes Care | Diabetes Care published a secondary analysis of the DiGest trial earlier this week assessing associations between specific CGM targets and pregnancy outcomes in gestational diabetes (GDM). First author Dr. Laura Kusinski (University of Leicester, UK) et al. set out to optimize metrics, ranges, and targets for the increasing use of CGM in GDM. The authors used logistic regression, receiver operating characteristic curves, and the Youden index to analyze data from the DiGest study (n=425). At 29 weeks of gestation, three metrics were significantly associated with a lower risk of delivering infants large for gestational age: (i) mean glucose <110 mg/dL; (ii) pregnancy-specific Time in Range (TIRp) 63–140 mg/dL ≥90% (yes, ninety percent!); and (iii) pregnancy-specific Time above Range (TARp) <10%. Both TARp <10% and mean nocturnal glucose <110 mg/dL were also associated with reduced odds of preterm birth. The authors conclude that mean glucose <110 mg/dL, ≥90% TIRp, or <10% TARp using a range of 63–140 mg/dL was associated with a low risk of negative outcomes. However, no single statistically robust TIR/TAR target was demonstrated across all outcomes. Future work remains to establish consensus around CGM metrics for GDM to improve infant and maternal outcomes on for widespread public health. We'll be interested to hear recommendations on hypoglycemia and severe hypoglycemia and how much time should be spent there. |
| GLP-1 Receptor Agonists and Cancer Risk in Adults With Obesity | Dr. Hao Dai (Indiana University) et al. | JAMA | JAMA published yesterday an article, “GLP-1 Receptor Agonists and Cancer Risk in Adults With Obesity,” by Dr. Hao Dai (Indiana University) et al. The retrospective cohort study examined whether GLP-1 RAs affect cancer risk in adults (n=86,632), using 2014-2024 electronic health record data from OneFlorida+. The 10-year follow-up data found that GLP-1 RA users had a significantly lower overall incidence of cancer compared with matched non-users (HR=0.83). GLP-1 RA use was particularly associated with reduced risk of endometrial cancer (HR=0.75), ovarian cancer (HR=0.53), and meningioma (HR=0.69). Given the myriad of positive benefits seen by GLP-1 RAs, we are unsurprised to see another example of benefits to users. While the initial purpose of the study was to understand whether the therapy would increase risk of cancer in the long-term, the data shows that the opposite is in fact true. As someone whose parents both passed away from cancer, one well over 20 years ago when he would've benefited enormously from GLP-1 and one nearly 20 years ago when she wouldn't probably have been prescribed GLP-1 but ... well, all I can say is, wellllll. There's a reason we're always writing about this class of therapy. Thank you to Dr. Dai and colleagues for letting us see some more of the power of this class that we all don't always see. |
| The Heavy Cost of Using Weight-Loss Drugs to Get Skinny | Dr. Nicholas Cozzi (Rush University) | Time | Time published Friday an article titled, “The Heavy Cost of Using Weight-Loss Drugs to Get Skinny” by Dr. Nicholas Cozzi (Rush University). As the Director of Emergency Medical Services at the Rush University Medical Center, Dr. Cozzi provides insights on the increasing use of GLP-1 RAs for weight loss and the need to understand important considerations of the treatment class. The 2024 KFF Health Tracking Poll has shown that one in eight Americans has taken GLP-1 RAs, with growing indications from its initial development as a therapy for glycemic management. While it’s encouraging to see GLP-1 RAs support individuals with weight loss, especially after they’ve struggled with diet and exercise alone, Dr. Cozzi raises concerns about the rapid rate of this intervention. Some of his patients in the emergency department have been encouraged by how fast they’re losing weight, yet, they’ve also faced complications like bowel blockages and pancreas inflammation as well as tolerability issues like nausea. In fact, a 2024 study published in JAMAdemonstrated that patients on GLP-1 RAs were nearly four times more likely to develop gastroparesis. Aside from safety issues and side effects, there’s also growing concern with how society is coming to view the idea of weight loss, the piece says, as GLP-1 RAs “give us a lens into how we view body image, class, and identity” ... we'll follow with some additional ideas on this during the week. |
| Proportion of Obesity-Related Conditions Attributable to Obesity and Overweight in US Youth | Mr. Ashwin Chetty (Yale University) et al. | JAMA Network | JAMA Network published today a research letter titled “Proportion of Obesity-Related Conditions Attributable to Obesity and Overweight in US Youth” by Yale Medical School's Mr. Ashwin Chetty et al. The authors conducted a cross-sectional analysis of young adults in the National Health and Nutrition Examination Survey (NHANES) between 2013-2023 to estimate the population attributable fractions of obesity-related conditions due to obesity and overweight in US adolescents and young adults. The study found that all obesity-related conditions except T2D were significantly attributable to obesity in adolescents. Similar findings were seen in young adults, though the PAF with T2D reached significance. The study also uncovered that several obesity-related conditions had significant population attributable fractions due to overweight, though to a smaller degree. The stats were distressing - more specifics ahead! |
| Risk differences and underlying factors of cardiovascular events and mortality in patients with type 2 diabetes versus type 1 diabetes: a longitudinal cohort study of Swedish nationwide register data | Dr. Vagia Patsoukaki (Uppsala University, Sweden) et al. | The Lancet Diabetes & Endocrinology | A study published yesterday in The Lancet Diabetes & Endocrinology by Dr. Vagia Patsoukaki (Uppsala University, Sweden) et al. titled, “Risk differences and underlying factors of cardiovascular events and mortality in patients with type 2 diabetes versus type 1 diabetes: a longitudinal cohort study of Swedish nationwide register data,” demonstrates striking age-dependent differences in cardiovascular risk between the two major diabetes types. Using the Swedish National Diabetes Register, the study followed cohorts of adults with T1D (n=38,351) and T2D (n=365,675) over a five-year period (2016-2020). Notably, adults with T2D under 50 faced higher risks of major cardiovascular disease (HR=1.23) compared to those with T1D. However, after age 60, T1D conferred higher CV-related risks, including myocardial infarction (HR=0.67 for T2D compared to T1D), all-cause mortality (HR=0.89), and overall CVD burden. While younger adults with T2D – who also carry an elevated risk compared to matched controls – should not be overlooked, this study underscores an urgent need to strengthen cardiovascular prevention in people with T1D, especially with regard to modifiable risk factors. |
| Longitudinal Metabolic Trajectories in Diabetes Prevention Program Participants Reveal Subgroups With Varying Micro- and Macrovascular Complication Risks | Dr. Emily Kobayashi (UCSD) et al. | Diabetes Care | This Diabetes Care study found that while most people with pre-type 2 diabetes develop T2D, their complication risk is low. A minority, however, follow high-risk paths. Of the four trajectories, they specified that:
|
| Global Inequities in Diabetes Technology and Insulin Access and Glycemic Outcomes | Dr. Alzbeta Santova (Comenius University, Slovakia) et al. | JAMA Network Open | A cross-sectional study published in JAMA Network Open by Dr. Alzbeta Santova (Comenius University, Slovakia) et al. titled, “Global Inequities in Diabetes Technology and Insulin Access and Glycemic Outcomes,” underscores significant disparities in pediatric T1D care worldwide. Drawing on data from children (n=42,349) across 81 centers in 56 countries within the SWEET registry, the authors found that full reimbursement for CGM, insulin pumps, BGMs, and insulin was associated with markedly lower A1c values (mean baseline of ~7.6%-7.8%) compared to centers with no reimbursement or access (mean baseline of ~9.6%-10.5%). Notably, eight countries reported no reimbursement for insulin or any technologies, while only 19 countries offered full reimbursement across the board. These findings reinforce that access to modern diabetes technology is closely associated with glycemic outcomes and highlight how inequities extend beyond technology to basic insulin availability in some regions. |
| Plant-Based Dietary Patterns Associated With Reduced Risk of All-Cause Mortality in Diabetes Subgroups: A Prospective Cohort Study From the UK Biobank | Dr. Edyta Shaefer (Heinrich Heine University Düsseldorf, Germany) et al. | Diabetes Care | Diabetes Care published a new study, “Plant-Based Dietary Patterns Associated With Reduced Risk of All-Cause Mortality in Diabetes Subgroups: A Prospective Cohort Study From the UK Biobank,” by Dr. Edyta Shaefer (Heinrich Heine University Düsseldorf, Germany) et al. The study analyzed 4,829 UK Biobank participants with T2D over an average follow-up of 11.3 years. Using repeated 24-hour dietary recalls, researchers generated plant-based diet index (PDI) scores, where higher scores indicated greater intake of plant foods and fewer animal foods. They further separated plant foods into “healthy” (whole grains, fruits, vegetables, legumes, nuts) and “unhealthy” (refined grains, sweets, sugary drinks). They found that those in the highest PDI tertile had a 21% lower risk of death than those in the lowest, with each five-point PDI increase translating to about one additional month of survival. While not significant, a higher healthy PDI was also linked to an 18% lower risk of death and about three months longer survival. Meanwhile, higher unhealthy PDI was associated with a 24% greater risk of death. These results reinforce the importance of diet as part of diabetes care. At ADCES earlier this month, several speakers emphasized that the “best diet” is the one that patients will use — a sentiment echoed by the Diabetes Prevention Program, which showed lifestyle interventions reduced diabetes incidence by 58%. |
July 2025
| Title | Author | Journal | Commentary |
| Cardiovascular Outcomes and Efficacy of the PCSK9 Inhibitor Evolocumab in Individuals With Type 1 Diabetes: Insights From the FOURIER Trial | Dr. Yu Mi Kang (Harvard) et al. | Diabetes Care | Diabetes Care just published an article by Dr. Yu Mi Kang (Harvard) et al. on the cardiovascular outcomes in people with T1D taking PCSK-9 inhibitor Repatha (evolocumab). Investigators conducted further analysis of the phase 3 FOURIER trial (n=27,564), in which evolocumab conferred a 59% reduction in LDL cholesterol and 15% reduction in MACE (composite of cardiovascular death, myocardial infarction, stroke, hospitalization for unstable angina, or coronary revascularization) in people with atherosclerotic cardiovascular disease (ASCVD). The study assessed the effects of evolocumab in people with T1D (n=197), which represented 0.7% of the trial participants. In T1D, evolocumab reduced the risk of MACE by 34% and the risk of secondary end points like CV death, MI, or stroke by 42%. Notably, the relative risk reduction with evolocumab in people with T1D was numerically higher than in participants without diabetes (23%) or with T2D (26%), indicating that intensive lowering of LDL-C has the potential to provide significant cardiovascular benefits for people with T1D and ASCVD. While the T1D cohort was small, we are encouraged by the results of this study and hope that this will lead to increased uptake of lipid management in people with T1D and ASCVD. |
| Characterizing Severe and Level 2 Hypoglycemia and Associated Risk Factors in Adults with Type 1 Diabetes Using Hybrid Closed-Loop Insulin Pumps | Dr. Yu Kuei Lin (University of Michigan) et al. | DT&T | DT&T published an article by Dr. Yu Kuei Lin (University of Michigan) et al. evaluating factors associated with severe hypoglycemia (SH) and level 2 hypoglycemia (blood glucose levels <54 mg/dL) in adults with T1D using AID systems (n=601). The cross-sectional survey assessed six-month SH history and found that impaired awareness of hypoglycemia (IAH) and higher glucose coefficient of variation were significantly associated with both SH and more than one instance of level 2 hypoglycemia. Notably, CGM-derived hypoglycemia metrics (i.e., Time below Range) alone were not predictive of SH. Participants with SH also tended to spend more Time above Range and had lower levels of educational attainment. Age and diabetes duration were not associated with SH or level 2 hypoglycemia. Those with both SH and ≥1% of time in level 2 hypoglycemia showed trends toward the most severe IAH. These findings reinforce the importance of IAH screening and glucose variability as key indicators of hypoglycemia risk, specifically in AID users. |
| Cost-Utility Analysis of the MiniMed™ 780G Advanced Hybrid Closed-Loop System Versus Intermittently Scanned Continuous Glucose Monitoring with Multiple Daily Insulin Injections in People with Type 1 Diabetes in France | Prof. Helene Hanaire (CHU Toulouse, France) et al. | DT&T | A new cost-utility analysis published in DT&T by Prof. Helene Hanaire (CHU Toulouse, France) et al. evaluates the long-term value of the MiniMed 780G advanced hybrid closed-loop (AHCL) system compared to intermittently scanned CGM (is-CGM) with MDI in people with T1D in France. Using the CORE Diabetes Model, researchers projected outcomes over 40 years. Baseline cohort characteristics were derived from the ADAPT RCT and included a mean baseline A1c of 9.0%, mean age of 41 years, and mean diabetes duration of 18 years. Results showed the 780G system provided a 2.26 QALY gain over is-CGM + MDI (16.3 versus 14.1 QALYs), with incremental lifetime costs of €78,509 (~$92,000), leading to an incremental cost-utility ratio (ICUR) of €34,732 (~$41,000) per QALY gained. Major A1c and Time in Range gains were made. The study concluded that in France, the MiniMed 780G system offers substantial long-term health benefits, which certainly sounds right on. We know, of course, the incredible value for reimbursement in adults with T1D who are not at their glycemic targets. AID has changed so much, though certainly CGM and all kinds of insulin delivery are easier than using only blood glucose strips, especially for those with high insulin sensitivity. And many, we know, can't even afford strips. None of us is doing well unless we're all doing well and there's so much improvement that awaits us all, with the right focus. |
| NHS app to give patients ‘doctor in your pocket’, vows Keir Starmer | Mr. Chris Smyth, Ms. Poppy Koronka | The Times | We're reading, from today in the UK, The Times' #1 story , on Sir Keir Starmer's hope to reform the NHS through its new app – "a doctor in your pocket." Amidst a broader 10-year plan that includes a focus on "neighborhood" (i.e. local) health services, the app is said to be going to eventually feature the ability for data from "smartwatches, glucose monitors, and intelligent fabrics" to feed into it to fuel care monitoring, a unified medical record, and "Ambient AI" to summarize consultations and reduce the time spent by doctors typing up notes. How fascinating – we look forward to watching to see how this develops. |
| Update on Management of Gestational Diabetes Mellitus and the Role of Continuous Glucose Monitor Technology | Drs. Amber Lachaud and Celeste Durnwald (University of Pennsylvania) | DT&T | Drs. Amber Lachaud and Celeste Durnwald (University of Pennsylvania) just published an insightful update in DT&T on the role of CGM for the management of gestational diabetes (GDM). GDM is the most prevalent metabolic complication of pregnancy, developing in approximately 7% of pregnancies in North America and Europe, 10% in South and Central America, 14% in Africa and the Western Pacific, 21% in Southeast Asia, and an astounding 28% in the Middle East and North Africa. Risk factors include maternal obesity, advanced maternal age, family history of T2D, diagnosis of PCOS, and a prior history of GDM. The condition has implications both for pregnant women and children to be born, with increased risk of adverse pregnancy outcomes as well as increased chance of developing T2D later in life. Drs. Lachaud and Durnwald explore the current first-line treatment of behavioral modification followed by insulin therapy, which normally includes the use of BGM compared to CGM. The authors call for increased use of CGM to improve the management of GDM, including the development of specific glucose targets for GDM, exploration of glycemic profiles for patients early in pregnancy who go on to develop GDM, and the relationship between elevated CGM metrics and adverse pregnancy outcomes. This essential updatehighlights the need for earlier diagnosis of GDM and appropriate intervention, and the essential role of CGM for this key effort. |
| Determining Insulin Pump Candidacy: The Disconnect Between Clinical Care Guidelines and Clinical Practice | Dr. Estelle Everett (UCLA) et al. | Journal of the Endocrine Society | More on AID from ENDO Society: This excellent study that we're reporting on today in our first paragraph spotlight revealed significant variability in provider approaches. Fifty-five percent required carbohydrate counting, 51% required a minimum number of daily glucose checks, and 48% required a minimum number of clinic visits per year for a start. While some of these figures seemed lower than we might have expected, others factors included CGM use (42%), time since diabetes diagnosis (20%), or a specific A1c value (8%). Unbelievably, to us, despite near-universal awareness of insulin pump guidelines (94%), over half of providers (52%) reported rarely referencing them, opting instead to rely on personal judgment in situations that conflict with recommendations. These findings highlight a critical disconnect between evidence-based guidelines and real-world clinical practice, which could well be contributing to insulin pump underutilization. Greater alignment between provider practices and national recommendations may well impact equitable and optimal care for people with diabetes - let us know what you think. |
| Dr. Curtis Triplitt and Dr. Ralph DeFronzo (UT Health San Antonio) | Diabetes Care | Diabetes Care just published results of a phase 4 trial (n=95), which compared exenatide, dapagliflozin, combination therapy, and placebo on beta cell function, insulin sensitivity, and insulin secretion in people with T2D. Investigators, including UT Health San Antonio’s Dr. Curtis Triplitt and Dr. Ralph DeFronzo, hypothesized that combination therapy confers the greatest improvement. Insulin sensitivity increased in all three treatment groups, compared to placebo, after one drug dose, and continued to increase even further in the dapagliflozin and combination therapy groups. Insulin secretion was highest in those taking exenatide and combination therapy, but not dapagliflozin alone or placebo at all time points. Beta cell function was highest in combination therapy (4x vs. placebo), followed by exenatide (3x) and dapagliflozin monotherapies (1.6x) in the acute study; participants taking monotherapies experienced further beta cell function enhancement. Ultimately, these results show that combination therapies are more beneficial. Combination therapy has long been suggested – our coverage goes back to 2008 – and was most recently highlighted at ADA 2025 and HiD 2025. While ADA's current Standards of Care recommend adding therapies to intensify cardiometabolic risk management, we wonder if the new evidence will encourage the ADA to emphasize these benefits even further. |
| Predictors of Diabetes Outcomes at 1 Year After Islet Autotransplantation: Data From a Multicenter Cohort Study | Dr. Piotr Witkowski (University of Chicago) et al. | Diabetes Care | Diabetes Care just published a study, “Predictors of Diabetes Outcomes at 1 Year After Islet Autotransplantation: Data From a Multicenter Cohort Study,” by Dr. Piotr Witkowski (University of Chicago) et al. Patients (n=384) underwent total pancreatectomy with islet autotransplantation (TPIAT) – a procedure used in people with chronic pancreatitis that does not require immunosuppression – and had a mean age of 30 years. 62% of the cohort was female. At one-year post-TPIAT: (i) 83% of patients retained some islet function (C-peptide >0.3 ng/mL); (ii) 20% were off insulin; and (iii) 60% had HbA1c <7.0%. Outcomes were most favorable in those with normoglycemia pre-TPIAT and in children. Children were 2.3 times more likely to be insulin independent at one year, and every 1.0% reduction in pre-transplant A1c was associated with 4x higher likelihood of insulin independence, bolstering the potential use of TPIAT in patients with lower A1c values. |
| Finerenone in Type 1 Diabetes with Chronic Kidney Disease | Dr. Chuping Chen (Guangzhou Red Cross Hospital, China) et al. | DT&T | DT&T just published an article, “Finerenone in Type 1 Diabetes with Chronic Kidney Disease,” by Dr. Chuping Chen (Guangzhou Red Cross Hospital, China) et al., highlighting three cases of Kerendia (finerenone) use in people with T1D and chronic kidney disease (CKD). As a reminder, finerenone is a non-steroidal mineralocorticoid receptor antagonist (nsMRA), currently indicated for CKD in T2D. It is also being investigated for CKD in T1D in the phase 3 FINE-ONE trial, which is expected to complete in September 2025. However, as the authors noted, finerenone use in T1D is not currently well-defined. In two patients (who each had T1D for nearly 15 years), urine albumin-to-creatinine ratio (UACR) fell significantly by 78% from a baseline of 3,534 mg/g (normal range is <30 mg/g) and 64% from a baseline of 1,186 mg/g, respectively. In the third patient, who was diagnosed with latent autoimmune diabetes in adults (LADA) two years previously, UACR decreased by 74% from a baseline of 2,441 mg/g. In all three cases, eGFR decreased by 15-22%, consistent with initial drops seen in other trials, like FIDELIO-DKD. Serum potassium level, a potential mark of side effects of finerenone, remained stable in all three patients. These qualitative cases show promise for finerenone use in T1D. We greatly look forward to the forthcoming results of the FINE-ONE trial, which should elucidate the benefits and risks more definitively. |
| Differential Obesity Trends in Asian and Native Hawaiian or Other Pacific Islander US Adults | Dr. Joan Lo (Kaiser Permanente) et al. As Drs. Nilay Shah and Sadiya Khan (Northwestern) | JAMA Network | JAMA Network just published an article, “Differential Obesity Trends in Asian and Native Hawaiian or Other Pacific Islander US Adults,” by Dr. Joan Lo (Kaiser Permanente) et al. As Drs. Nilay Shah and Sadiya Khan (Northwestern) pointed out in their editorial, “Equity in Obesity Awareness,” this article unveils the heterogeneity of the obesity burdens among Asian American, Hawaiian, and Other Pacific Islanders, who are often considered in the same category. Investigators evaluated trends in high BMI and obesity among racial and ethnic subgroups and compared to non-Hispanic white populations. From 2012-2023, all subgroups increased in obesity and overweight prevalence. Ultimately, authors emphasize the importance of tracking BMI for these groups for early prevention. We note that BMI does not consistently predict cardiometabolic risks in various Asian populations due to differences in fat distribution, warranting the inclusion of additional metrics like the waist-to-circumference ratio. |
| Physical Activity Is Associated With Improved Glycemic Outcomes in Newly Diagnosed Youth With Type 1 Diabetes: 4T Exercise Program | Dr. Dessi Zaharieva (Stanford) et al. | Diabetes Care | Diabetes Care published a study earlier this month titled, “Physical Activity Is Associated With Improved Glycemic Outcomes in Newly Diagnosed Youth With Type 1 Diabetes: 4T Exercise Program,” by Dr. Dessi Zaharieva (Stanford) et al. In this study, the Teamwork, Targets, Technology, and Tight Range (4T) Exercise Program studied physical activity patterns across the first year of T1D diagnosis, determining the association between physical activity and changes in glycemic outcomes through CGM metrics. Days with ≥10 minutes of intense physical activity were associated with an increase in TIR of 2.3%, a decrease in TAR of 3.1%, and an increase in TBR of 0.8% in the 24 hours following physical activity. Additionally, from the first three months to 10-12 months post-diagnosis, the median step count increased by 1,134 steps per day, and daily moderate-to-vigorous physical activity increased by 11 minutes per day. These findings continue to reinforce the large body of evidence that highlights the importance of integrating physical activity into early diabetes management. |
| Minimum Continuous Glucose Monitor Data Required to Assess Glycemic Control in Youth with Type 1 Diabetes | Dr. Sonia Gera (Children’s Hospital of Philadelphia), Dr. Brynn Marks (University of Pennsylvania), et al. | DT&T | A study published Tuesday in DT&T by Dr. Sonia Gera (Children’s Hospital of Philadelphia), Dr. Brynn Marks (University of Pennsylvania), et al. quantifies the minimum amount of CGM data required to assess glycemia in pediatric patients with T1D. Dexcom G6 CGM data were extracted from youth with T1D and ≥70% active CGM time (n=1,316). 77% of participants were non-Hispanic White, average GMI was 7.4%, average Time in Range (TIR) was 61%, and median 14-day CGM active time was 97%. Although 14 days remains the recommendation of consensus guidelines, the authors conclude that assessing approximately 9.6 days of CGM data in youth with T1D provides a reliable assessment of glycemia and note that for youth with higher TIR (≥70%) and lower CV (<36%), seven-day CGM data may prove sufficient. |
| Time to Progression to Proliferative Diabetic Retinopathy in Patients With Type 2 Diabetes | Ms. Iris Kim (University of California San Francisco) et al. | JAMA | A study published this week in JAMA by Ms. Iris Kim (University of California San Francisco), et al. demonstrates the predictive power of survival models on progression to proliferative diabetic retinopathy in patients with T2D. Diabetic retinopathy (DR) is the leading cause of blindness among working-aged adults, but is preventable with timely diagnosis and treatment. Still, recommended routine screening is inconsistently observed. Researchers sought to address this nonfulfillment and found success in three survival models that identified baseline age, ethnicity, diabetic macular edema, non-proliferative DR severity, and mean A1c as possible risk factors. With the potential to facilitate earlier identification of high-risk patients, authors hope survival models will enable targeted interventions and resource allocation for these high-risk patients, which could improve outcomes significantly. While age at diagnosis was excluded from the risk parameters this is of interest given the striking incidence of DR in youth with diabetes, which fell at 50% in 2021’s TODAY2 study. Nevertheless, survival models and AI-powered predictions may well offer promising avenues for personalized care and mitigation of risk factors for patients with T2D and beyond. |
| Gradual Titration of Semaglutide Results in Better Treatment Adherence and Fewer Adverse Events | Dr. Roy Eldor (Tel Aviv Sourasky Medical Center, Israel) | Diabetes Care | Diabetes Care published a study today titled, “Gradual Titration of Semaglutide Results in Better Treatment Adherence and Fewer Adverse Events,” by Dr. Roy Eldor (Tel Aviv Sourasky Medical Center, Israel). This phase 3 open-label pilot study (n=100) compared the effect of a 16-week flexible titration regimen of semaglutide versus the 8-week label-recommended regimen in people with T2D. Study participants were randomized to either a flexible titration (starting at 0.0675 mg, gradually increasing by 0.0675 mg/week and delaying for GI adverse events) or label-recommended titration (0.25 mg, 0.5 mg, 1 mg at four-week intervals). After 26 weeks of titration, the final doses, A1c reduction, and BMI change were similar between the two groups – given the nature of these glycemic benefits, it would have been great to see some TIR and GMI data from participants as well. Only 2% of participants in the flexible regimen group withdrew from the study due to GI adverse events, compared to 19% in the label-recommended group (p=0.005). As well, participants in the flexible group reported less nausea (45% vs. 64%), overall days experiencing nausea (three days vs. six days), and asthenia (10% vs. 25%) than the label group. Given GI that adverse events with semaglutide significantly contribute to treatment adherence and overall patient outcomes, it’s encouraging to see the efficacy of a slower, flexible titration scheme. With these results that demonstrate comparable efficacy, we wonder how HCPs can adopt such treatment plans and deliver individualized care for patients. |
| Sex-based disparities in perceived versus objective glycaemic control in type 1 diabetes: a cross-sectional cohort study | Prof. Coco Snethlage (Amsterdam UMC, the Netherlands) | The Lancet | The Lancet published on Wednesday a cross-sectional cohort analysis by Prof. Coco Snethlage (Amsterdam UMC, the Netherlands), examining sex-based disparities in perceived versus objective glycemic control in adults with T1D. Using CGM and self-reported data from the GUTDM1 cohort (n=496 adults with T1D; 180 men, 316 women), researchers evaluated the differences in how men and women assess their own glycemic control and hypoglycemia risk relative to objective CGM metrics. While women and men had similar Time in Range (67% versus 66%) and A1c levels (~7.3%), men overestimated their glycemic control by 31% and women slightly underestimated theirs. Despite more frequent CGM-recorded hypoglycemia, men also underreported hypoglycemic events more than women. These findings suggest differences in hypoglycemia awareness and risk perception, and researchers highlighted the importance of using CGM metrics instead of relying on general impressions when assessing glycemic control. |
| Real-World Safety and Effectiveness of U200 Insulin Use in Automated Insulin Delivery Systems in Adolescents and Young Adults with Type 1 Diabetes | Dr. Patricia Chu (Children’s Hospital of Philadelphia) et al. | DT&T | In a DT&T study just published last Friday, Dr. Patricia Chu (Children’s Hospital of Philadelphia) et al. investigated the use of concentrated insulin in automated insulin delivery (AID) systems among adolescents and young adults (AYA) with T1D and high insulin needs. Though concentrated insulin is not typically used due to multiple challenges surrounding it, including increased risk of dosing errors as well as some broader clinical skepticism, this study frames U200 (200 units/mL) as a possible practical solution to a limitation of AID system use: small pump cartridge volumes that require frequent pump changes. In this small two-center, retrospective cohort study (n=50), U200 use in AID systems significantly increased both time in range and the number of days between cartridge changes, despite higher total daily insulin use. Notably, Time below Range remained unchanged (it was low, at 45%). Importantly, though it was a small study, we note that no cases of severe hypoglycemia or DKA occurred during follow-up. Dr. Chu et al. findings confer that U200-AID use is a safe and effective option for AYAs with high insulin requirements, offering a promising avenue for overcoming a barrier that often deters the high-insulin need population from AID use. While we imagine that more will have to use this more highly concentrated insulin before it becomes more clinically acceptable, we were very glad to see this study. |
| Tirzepatide Treatment and Associated Changes in β-Cell Function and Insulin Sensitivity in People With Obesity or Overweight With Prediabetes or Normoglycemia: A Post Hoc Analysis From the SURMOUNT-1 Trial | Dr. Andrea Mari (CNR Institute of Neuroscience, Italy) et al. | Diabetes Care | A new post-hoc analysis of the SURMOUNT-1 trial evaluating the effect of tirzepatide treatment on changes in beta cell function and insulin sensitivity was just published in Diabetes Care. Dr. Andrea Mari (CNR Institute of Neuroscience, Italy) et al. assessed the use of tirzepatide for 72 weeks in 2,539 adult participants with obesity or overweight (BMI ≥27 kg/m2) and either prediabetes or normoglycemia at baseline. The authors note that the effect of tirzepatide on beta cell function and insulin sensitivity has yet to be explored in people without diabetes. At Week 72, multivariate regression models demonstrated improvements in insulin sensitivity associated mostly with weight reduction and partly with tirzepatide treatment. Beta cell function was also enhanced overall and was mostly associated with tirzepatide treatment versus primarily weight loss. Improvements increased with higher tirzepatide doses (5, 10, and 15 mg). The authors suggest that tirzepatide treatment may protect against progression of dysglycemia via improvement to insulin sensitivity and beta cell function. This could potentially lead to the normalization of glucose levels in people with prediabetes, possibly preventing beta cell deterioration and the development of diabetes. |
| The Experience of Discrimination Impacts Technology Readiness and Psychosocial States of Minoritized Families Living With Type 1 Diabetes: Findings From the BEAD-T1D Pilot Study | Dr. Ananta Addala (Stanford), Dr. David Maahs (Stanford), and Dr. Korey Hood (Stanford) et al., | Endocrine Practice | Endocrine Practice published findings in early July from the BEAD-T1D Pilot study led by Dr. Ananta Addala (Stanford), Dr. David Maahs (Stanford), and Dr. Korey Hood (Stanford), et al., investigating diabetes technology acceptance among families of children of color with T1D and how perceived discrimination affects this group. The study enrolled parents of children under age 12 with T1D and public insurance in surveys, focus groups, and advisory groups to explore barriers to technology use. In survey data, perceived discrimination was significantly associated with lower diabetes technology acceptance, higher depression, and lower global health scores. Qualitative interviews revealed that parents reported discrimination based on race, ethnicity, and insurance status, driving reluctance to adopt diabetes technologies. While the authors said that perceived discrimination is an overlooked subject, they consider it to be a significant barrier to technology utilization that must be addressed in healthcare and community settings. |
| Contrasting Adult and Pediatric Populations in a Cohort of At-Risk Relatives in The T1D TrialNet Pathway to Prevention Study | Ms. Erin Templeman (University of Exeter, UK) et al. | Diabetes Care | A study published in Diabetes Care called “Contrasting Adult and Pediatric Populations in a Cohort of At-Risk Relatives in The T1D TrialNet Pathway to Prevention Study,” by a prominent and well-known group of authors including first author Ms. Erin Templeman of the University of Exeter in the UK. The study compares autoantibody screening outcomes and T1D outcomes in adults versus children. Here were some things that drew our interest: (i) Over half of incident T1D cases occur in adults, yet research on diseases progression continues to focus “primarily” on at-risk children. Approximately 136,000 children and 100,000 adult relatives of people with T1D screened in the TrialNet Pathway to Prevention study were studied; (ii) Adults were over 30% more likely than children to screen positive for a single autoantibody (4% versus 3%) but, interestingly, nearly 70% less likely for multiple autoantibodies (1% versus 3%); (iii) Progression to stage 3 T1D was lower in adults with single autoantibody positivity or stage 1 T1D (two or more autoantibodies) than in children, which is a five-year risk with single autoantibody of 8% for adults versus 22% for children. There was an even bigger difference with only stage 1 of 17% versus 47%, respectively. However, adults with “full” stage 2 T1D from an initial staging OGTT had comparable five-year progression risks to children, which was 78% for both groups (this struck us as a very specific number!); and (iv) This piece certainly provides further evidence that autoantibody positive adult relatives have distinct trajectories and progression risks compared to children. This suggests the need for tailored monitoring and intervention strategies and could support even further classification of T1D into distinct progression pathways. As evidence builds, we hope that support multiple interventions surrounding T1D will grow. As well, we hope support for earlier use for CGM related to early diagnosis will also grow – this supports, of course, the notion that fewer people will have DKA related to their diagnoses, which certainly would be a win. |
| Non-autoimmune, insulin-deficient diabetes in children and young adults in Africa: evidence from the Young-Onset Diabetes in sub-Saharan Africa (YODA) cross-sectional study | Prof. Jean Claude Katte(University of Exeter, UK), Prof. Jean Claude Mbanya (University of Yaoundé, Cameroon), Prof. Andrew Hattersley (University of Exeter, UK) | The Lancet | A study published in The Lancet: “Non-autoimmune, insulin-deficient diabetes in children and young adults in Africa: evidence from the Young-Onset Diabetes in sub-Saharan Africa (YODA) cross-sectional study,” aimed to determine whether T1D diagnosed in young Black Africans is primarily autoimmune in origin, identifying a potential new subtype of T1D. The work led by Prof. Jean Claude Katte(University of Exeter, UK), Prof. Jean Claude Mbanya (University of Yaoundé, Cameroon), Prof. Andrew Hattersley (University of Exeter, UK), and 29 others was a cross-sectional analysis of insulin-treated participants under age 30 (n=894; mean diabetes duration: five years) from Cameroon, Uganda, and South Africa. Investigators measured islet autoantibodies (GADA, IA-RA, ZnT8A), C-peptide, and a T1D genetic risk score (GRS), and compared these with control populations without diabetes. Only 35% were positive for autoantibodies, suggesting that most (65%) may have a non-autoimmune, insulin-deficient subtype distinct from classic T1D. Autoantibody-negative participants also showed significantly lower genetic risk scores and C-peptide levels inconsistent with T2D. Compared with US SEARCH data, these findings point to a potential ancestry-specific phenotype of T1D and underscore variations in young-onset diabetes. These results build on prior data presented at nPOD 2025, highlighting later age of onset, low absolute insulin requirement, and reduced autoantibody prevalence in African T1D populations. The authors call for further research to identify genetic and environmental factors that drive this subtype of T1D. |
| Time in range—A new gold standard in type 2 diabetes research? | Dr. Ashni Goshrani, Dr. Rose Lin, and Dr. David O'Neal, et al. (Northern Health, Melbourne, Australia) et al. | Diabetes, Obesity, and Metabolism | A review article, “Time in range—A new gold standard in type 2 diabetes research?” by Dr. Ashni Goshrani, Dr. Rose Lin, and Dr. David O'Neal, et al. (Northern Health, Melbourne, Australia) et al. published in Diabetes, Obesity, and Metabolism evaluated the use of Time in Range (TIR) as an outcome measure in T2D trials. The authors note that A1c is the current gold-standard outcome measure for T2D trials, while T1D studies have adopted TIR as a key endpoint metric. In this literature review, the authors identified 247 papers that incorporated TIR as an outcome metric for T2D trials and included 110 of them in their published review – what made them include or not? Dozens of RCTs (n=45) included TIR as an outcome measure in patients with T2D and many papers also validated the use of TIR as a metric. The authors note that unlike A1c, TIR is not affected by ethnicity, hemoglobinopathies, or anemia, which makes it a more reliable outcome measure of glycemia in some populations that are often get excluded in studies that use A1c as a primary outcome measure. Some trials in T2D have also shown differences in outcomes between A1c and TIR – TIR is seen as an increasingly valuable marker for T2D health. The authors encourage the use of TIR as a key metric for T2D as it further contextualizes A1c. |
| Type 2 Diabetes and Financial Outcomes | Dr. Matthew Pesavento (The Ohio State University) et al. | JAMA | JAMA just published "Type 2 Diabetes and Financial Outcomes," an economic evaluation of nearly 170,000 adult patients at a primary care medical center in Ohio between October 2017 to December 2021 (n=166,285) by Dr. Matthew Pesavento (The Ohio State University) et al. Participants were 55% female, 2% Hispanic, 19% Black, and 73% white; 42% were diagnosed with T2D. The study found that the probability of adverse financial outcomes was significantly higher among patients with T2D than without (1.9 vs. 1.2 events). Greater estimated probabilities included: below-prime credit score (60%), medical collections (37%), debt charge-offs (15%), bankruptcy filings (2%), and foreclosures (0.5%). People with T2D also had significantly greater nonmedical debt collections ($1,875 vs. $1,361) and delinquent debt ($11,387 vs. $7,630) than those without T2D. Risk of adverse financial events was higher among those without earned income, Black, Hispanic, Medicaid-enrolled, and young (<65 years old) individuals, as well as in women. The study highlighted the need for providers to consider patients’ financial situation in order tailor strategies that are both effective and feasible, given the double burden of personal and financial health many patients with T2D juggle. |
| Managing Adverse Effects of Incretin-Based Medications for Obesity | Dr. Robert Kushner (Northwestern University) et al. | JAMA | JAMA published a study Tuesday, “Managing Adverse Effects of Incretin-Based Medications for Obesity,” an evaluation of the adverse effects associated with tirzepatide use. The authors, including the renowned former head of TOS Dr. Robert Kushner (Northwestern University), touted Zepbound (tirzepatide) for the treatment of obesity and related comorbidities. As Dr. Kushner described in the article and reinforced on yesterday’s JAMA News Podcast, various adverse side effects often deter individuals from treatment, with little over half (53%) of initiators continuing the therapy beyond one year. GI-related side effects, in particular, remain a most prevalent issue, and very preventable, as characterized by Dr. Kushner and his coauthors. Preventable? We are keen to see what happens. Nausea, diarrhea, vomiting, and constipation, which affect upwards of 44%, 31%, 25%, and 23% of people on incretin-based therapies, respectively, according to this piece, might be mitigated by clinical interventions – namely, dietary consulting, titrating the medications, etc (we loved this quote "titrating on can also mitigate consequences of missed doses ..."). |
| ELAVAY Diabetes Report Exposes Systemic Gaps in Patient Advocacy and Names Top Pharma Leaders in 2025 | Archo Advocacy | Archo Advocacy | In patient advocacy, Archo Advocacy just published its 2025 ELAVAY Diabetes Report, offering a striking snapshot of how patient advocacy organizations perceive leading healthcare companies. Eli Lilly topped the rankings, earning praise for its work in disease education and research collaboration, while Sanofi/Genzyme led in coalition building and patient registry efforts. Abbott and Novo Nordisk were also high scorers. The report identified Dexcom as its biggest surprise, achieving perfect scores in patient-centric insights and education. The report also identified, however, major gaps in industry support for advisory initiatives and public policy transparency. Advocates cited widespread under-education on financial barriers like copay accumulators and non-medical switching, pointing to a disconnect between corporate health equity messaging and on-the-ground impact. Notably, 80% of advocates said programs are irrelevant or invisible to patients, and pointed to a variety of solutions: (i) 71% called for more technology-enabled patient support; (ii) 60% called for greater patient-facing health economics education efforts; and (iii) to reduce out-of-pocket costs, 57% took aim at PBMs and payers. |
June 2025
| Title | Author | Journal | Commentary |
| Fully closed-loop improves glycemic control compared with pump with CGM in adolescents with T1D and HbA1c above target: A two-center, randomized crossover study | Nithya Kadiyala, Rama Lakshman, Janet Allen, Julia Ware, Charlotte Boughton, Malgorzata Wilinska, Ajay Thankamony, Sarar Hartnell, Hood Thabit, Ruben Willemsen, Pratik Shah, Roman Hovorka | DT&T | This article discussed results from a randomized crossover study comparing the efficacy and safety of the fully closed-loop (FCL) CamAPS HX AID algorithm to sensor-augmented pump (SAP) therapy among adolescents with T1D with above-target A1c (n=24). The trial consisted of two, eight-week periods with CamAPS HX with Fiasp or SAP therapy, occurring in random order. No behavioral restrictions were placed on participants. Median A1c at baseline was a high 8.9%. Mean Time in Range was significantly higher during the FCL period than the SAP period (45% vs. 32%, p<0.001), translating to a 3.1 hours/day difference in favor of FCL. This difference was primarily driven by reductions in time in hyperglycemia as Time >250 mg/dL was 7% lower (1.8 hours/day) with FCL than SAP (29% vs. 40%, p<0.001), while Time below Range was similar between groups (2.8% with FCL vs. 3.0% with SAP). Despite the improvements in CGM metrics, there was no statistically significant difference in A1c between groups (8.6% with FCL and 8.9% with SAP, p=0.227), indicating limitations of solely using A1c to monitor glycemic health. We love the idea, of course, of being able to improve multiple factors around one's diabetes experience even as technology improves - for example, thinking around food, exercise, mindset, and sleep! (Thanks, Adam Brown, now therapist extraordinaire and author!) |
| Maternal Glucose and Neonatal Hypoglycemia in Pregnancy with Type 1 Diabetes: A Continuous Glucose Monitoring Cohort | Lukana Preechasuk, Tamara Thompson, Parizad Avari, Ian Godsland, Rebecca Scott, Chukwuma Uduku, Ed Mullins, Nick Oliver, Rochan Agha-Jaffar | DT&T | The analysis examined CGM data from 60 mothers and capillary BGM from their neonates, using two thresholds to define neonatal hypoglycemia: (i) <40 mg/dL and (ii) <47 mg/dL. These are pretty low levels! In the cohort, 25 neonates had hypoglycemia <47 mg/dL, and 19 neonates had hypoglycemia <40 mg/dL. This was worrying to see and read about. Neonates who experienced hypoglycemia <40 mg/dL tended to be born at lower gestational ages (37.0 with hypoglycemia vs. 37.6 without hypoglycemia, p=0.019). Additionally, nearly one-third of neonates with hypoglycemia <40 mg/dL were exposed to antenatal corticosteroids (recommended for pregnant women at risk for preterm delivery) compared to only 7.3% of those without hypoglycemia <40 mg/dL (p=0.014). The worst outcome from our view (beyond the damage to their bodies) was that more neonates with hypoglycemia <40 mg/dL were admitted to the neonatal ICU than those without hypoglycemia <40 mg/dL (42% vs. 12%, p=0.009). This is preventable as are the costs associated with these stays. Similar results were observed with the <47 mg/dL threshold. Maternal Time above Range and Time in Range were both significantly associated with the occurrence of hypoglycemia <40 mg/dL (both p=0.01). The authors suggested that optimizing glycemia earlier in pregnancy could help minimize neonatal hypoglycemia risk. We'd agree, though hypoglycemia is a pretty well known hazard for pregnancy - would that every woman pregnant with T1D (and T2D if needed) could have CGM and AID systems, galore. |
| Income and Severe Hypoglycemia in Type 2 Diabetes | Dr. Misook Kim (The Catholic University of Korea, South Korea) | JAMA Network Open | The study analyzed data from 1.8 million adults with T2D aged 40-70 years in South Korea and ~17,000 in the UK. Participants were stratified by income – into quartiles by household income in Korea and quintiles by individual income in the UK. In the UK, individuals in the lowest quintile had a striking 5.4 times higher risk of severe hypoglycemia compared to those in the highest quintile (HR=5.38; CI: 1.72-16.85). Similarly, in Korea, individuals in the lowest income quartile had a 2.5-fold increased risk (HR=2.50; CI: 2.33-2.57). Notably, Korean participants who moved from the lowest to highest income quartile experienced a 26% reduced risk of severe hypoglycemia (HR=0.74; CI: 0.67-0.81), suggesting interventions aimed at reducing economic disparities could significantly improve diabetes care outcomes. However, the study also found that more than one year of medical aid – issued to those with income below 40% of the median – was associated with a 71% higher risk of severe hypoglycemia (HR=1.71; CI: 1.54-1.89). Given these findings, it raises important questions about the role of patient access programs — such as the Lilly Cares Foundation and Novo Nordisk’s Patient Assistance Program — in addressing income-related disparities in diabetes outcomes. |
| Associations of CGM Metrics With Stimulated C-Peptide Measures in Youth With Recent-Onset Type 1 Diabetes | Drs. Anna Neyman; Linda A. DiMeglio, the study’s corresponding author, Colleen Bauza, Bruce Buckingham, Mark A. Clements; Gregory P. Forlenza, Jennifer L. Sherr, Lauren Kanapka, Roy W. Beck, Craig Kollman, Shannon Beasley, Erin Cobry, Lisa Norlander, Ryan McDonough, Michelle Van Name, and Antoinette Moran | Diabetes Care | In a study of 103 children enrolled in the Closed-Loop/Verapamil study (CLVer), CGM and mixed-meal tolerance test-derived C-peptide measures were observed at time points up to 52 weeks after diagnosis. At Week 52, CGM metrics moderately correlated with C-peptide area under the curve. Time in Range (TIR) had a Spearman correlation of 0.45, indicating a moderately positive correlation, and Time Below Range (TBR) had a moderately negative correlation of 0.33. For predicting peak C-peptide concentrations greater than 0.2 pmol/mL, the combination had a sensitivity of 68% and specificity of 75%. The study’s authors conclude that the sensitivity and specificity are not great enough to replace C-peptide measures in clinical trials at this time – we imagine that further work may provide more detail on this correlation and expand uses of CGM metrics in T1D trials. Of course, we’re very eager to learn more about more reactions to verapamil, rather than just how the strides are measured, and we don’t want to lose the importance of this study by getting lost in which way to measure glycemic health. |
| Glucagon-like peptide-1 receptor agonists and risk of neovascular age-related macular degeneration | Dr. Reut Shor (University of Toronto) | JAMA Ophthalmology | This article examines the association between GLP-1 RA use and the development of neovascular age-related macular degeneration (nAMD) in adults with diabetes aged 66 years and older (n=139,002). The population-based cohort study found that using GLP-1 RAs for at least six months was associated with a more than two-fold greater likelihood of developing new-onset nAMD. Among GLP-1 RA users (n=46,334), 0.2% were newly diagnosed with nAMD between January 2020 and November 2023, compared to 0.1% of those in the non-user group. The risk increased further to an over three-fold greater likelihood of nAMD with longer durations of GLP-1 RA use. |
| Kidney Disease: The Forgotten Legacy of Type 1 Diabetes | Prof. Merlin Thomas (Monash University, Australia) | Diabetes Care | This article calls for attention to early kidney protection in T1D. The authors believe that a different foundational approach to T1D management should be implemented to consider early kidney protection as important as glucose control. A number of new reno-protective strategies have emerged in the last decade, including GLP-1 RAs, aldosterone antagonists, and SGLT-2 inhibitors. Robust data has verified the use of these therapies in T2D, but the risk of serious adverse events in T1D must be carefully considered in clinical trials before use in T1D expands further. The authors explore these therapies and the evidence supporting or discouraging them in T1D, including the limited end-organ benefit of metformin, the curiously small effects of RAS inhibitors in T1D compared to T2D, concerns of diabetic ketoacidosis (DKA) with SGLT-2 inhibitors, and the promise of GLP-1 RAs. Further work to evaluate adjunctive therapies for kidney disease in T1D remains, as the authors emphasize, “Protecting their future means protecting their kidneys today.” We encourage everyone to be proactive with kidney health – stay aware, think long term, and know your numbers! |
| The Association Between Hemoglobin A1c and Complications Among Individuals With Diabetes and Severe Chronic Kidney Disease | Dr. Dea Kofod (Copenhagen University Hospital, Denmark) | Diabetes Care | The Danish registry-based cohort study (n=107,244) evaluated how A1c levels are associated with one-year risk of macro- and microvascular complications, as well as hospitalizations from hypoglycemia among people with severe chronic kidney disease (CKD) and diabetes. The risk of major adverse cardiovascular events (MACE) significantly increased in individuals with A1c ≥7.2% or <5.8%. Similarly, the risk of microvascular complications and hospitalizations from hypoglycemia significantly increased at levels of A1c ≥7.2% or ≥6.7%, respectively. These associations were similar in people with mild-to-moderate CKD or no-to-mild CKD. Ultimately, investigators concluded that A1c between 6.7-7.1% is most optimal for minimizing long-term complications in people with severe CKD and diabetes – which aligns the ADA’s guideline recommending A1c <7%. |
| Changes in weight and glycemic control following obesity treatment with semaglutide or tirzepatide by discontinuation status | Dr. Hamlet Gasoyan (Cleveland Clinic) | Obesity Journal | The study harnessed EHR data from patients in health systems in Ohio and Florida with overweight or obesity without type 2 diabetes (n=7,881) who initiated injectable semaglutide (n=6,109) or tirzepatide (n=1,772). It stratified participants by treatment discontinuation: (i) early (within three months of initiation); (ii) late (three to 12 months of initiation); and (iii) non-discontinuation. Over half of participants (52%) discontinued the therapies by one year. Mean weight reduction at one year was 9% from a baseline of 112 kg (247 lbs). By discontinuation rate, weight loss with early, late, and non-discontinuation was 4%, 7%, and 12%, respectively (p < 0.001). The mean reduction in A1c at one year with early, late, and non-discontinuation was 0.1%, 0.2%, and 0.4%, respectively (p < 0.001). Baseline A1c data was available for just 58% of participants, averaging 5.5%. Participants taking tirzepatide experienced greater weight loss at one year than those on semaglutide (13% vs. 8%, respectively). The authors concluded that the high discontinuation rates likely contributed to the significantly lower weight and A1c reductions observed in this study compared to the results from the phase 3 trials for semaglutide and tirzepatide (15% and 23%, respectively). |
| Titration and discontinuation of semaglutide for weight management in commercially insured US adults | Dr. Yunwen Xu (John Hopkins) | Obesity Journal | The study found that among commercially insured adults in the US (n=15,811), nearly half (46%) discontinued semaglutide by Month 5. The authors attributed part of the high discontinuation rate to cost; participants in the highest monthly copay quintile (≥$161) were 33% more likely to discontinue treatment than those in the lowest (≤$54) quintile (with 51% and 41% discontinuing, respectively). The study also found that real-world dose escalation lagged behind that observed in clinical trials – just 83% to 94% of participants followed the titration schedule and maintained the target dosage up to 68 weeks. In addition to cost, the authors posited that side effects and perceived non-efficacy contributed to the high discontinuation rates and slower-than-expected dose titration. |
| Underrepresentation of older adults in diabetes and kidney disease trials | Prof. Priya Bart (UMC Groningen, the Netherlands) | The Lancet | Prof. Bart discusses the underrepresentation of “older” adults (while this population is defined differently in each trial, it typically refers to people aged ≥65 years) in studies of T2D and chronic kidney disease (CKD) despite the complex management of these conditions in the elderly. Older patients often have multiple comorbidities, take several medications, and are at increased risk of adverse drug reactions. All of these factors necessitate very personalized treatment strategies which should be supported by robust evidence. However, clinical trials in diabetes and CKD often underrepresent older adults, despite these management factors and high prevalence of these diseases in older adults. This can lead to uncertainty among physicians – approximately 30% of physicians have reportedly found it difficult to apply T2D and CKD guidelines to older adults. Instead, they must extrapolate findings in younger adults to their management of the elderly, which may not always apply. Notably, as the global population continues to age, and as people with diabetes stay alive longer, Prof. Bart calls for improved representation of older adults in diabetes and CKD trials and for the evaluation of study selection processes. |
| Diverging mortality trends by educational attainment in the US | Dr. Eugenio Paglino (University of Helsinki) | JAMA Health Forum | The study found that over 525,000 more deaths occurred in 2023 than would have been expected based on pre-2010 trends, with over 480,000 of those among adults without a college degree. While COVID-19 was a leading cause of excess deaths, circulatory diseases and diabetes were primary contributors. The authors attribute the widening mortality gap to both cardiometabolic diseases and external causes, underscoring the growing influence of structural and social inequities on U.S. mortality patterns. |
| Rapid and slow progressors toward beta-cell depletion and their predictors in T1D: Prospective longitudinal study in Japanese T1D (TIDE-J) | Dr. Shinsuke Noso (Kindai University) | Diabetes Care | By monitoring the progression of β-cell dysfunction in a nationwide database, researchers classified genetic markers associated with distinct T1D subtypes that they characterize as -- slowly progressive; -- acute onset; and -- fulminant At five years post-diagnosis, undetectable C-peptide response (CPR) levels were observed in 43% of acute onset, 9% of slowly progressive, and nearly all (93%) of fulminant T1D cases, reinforcing more substantial variation in β-cell loss across subtypes than we might have expected. Interestingly, in cases of acute onset T1D, marked heterogeneity characterized rapid progression (DR4/DR8; DR4/DR9) and slower β-cell decline (DR4/DR4) within the subtype. Clinically predictive markers specific to slowly progressive T1D — low BMI, GAD antibody positivity, and absence of the DR2 haplotype — predicted insulin dependence. Together, these findings underscore the intra-subtype diversity of T1D and support genetic and clinical profiling as a means for disease management that is more personalized. |
| Finerenone in HF with improved ejection fraction | Dr. Akshay S. Desai (Brigham & Women’s Hospital) | The Journal of the American College of Cardiology | This was a prespecified subgroup analysis from the FINEARTS-HF trial (n=6,016) on the efficacy of finerenone in patients with heart failure and preserved or mildly reduced ejection fraction (HFpEF, HFmrEF) following a worsening heart failure (WHF) event. Finerenone significantly reduced the risk of subsequent heart failure hospitalizations or cardiovascular death, with the greatest benefit seen in those treated soonest after the event. Safety was consistent across all groups, with no notable increase in hyperkalemia or renal adverse events. The authors highlight that initiating finerenone soon after a worsening HF episode provides a valuable opportunity to reduce future HF events in this high-risk population. |
| Re-evaluating the concept of remission in T2D: A call for patient-centric approaches | Prof. Kamlesh Khunti(University of Leicester, UK) and Dr. Vanita Aroda (Brigham and Women’s Hospital) | The Lancet | Sustained remission, through the loss of excess weight, can have enormous health and quality of life benefits. However, such remission – defined as normoglycemia without medication – is typically temporary. Many individuals experience weight regain and relapse. Prof. Khunti and his peers suggest that attempting to sustain normoglycemia by weight loss and without medication may not be more beneficial than managing to normoglycemia by adding medication (e.g,. GLP-1 RA), particularly in terms of reducing long-term macrovascular and microvascular complications. This was music to our ears - although none of the organizations that offer GLP-1 receptor agonists or SGLT-2 inhibitors have sought type 2 "delay" labels as far as we know, it seems very possible that this could be achieved, similar to how Sanofi's TZield (approved by the FDA in late 2022) has a type 1 diabetes "delay" label - and, we hope, will one day itself have T1D prevention label. Ultimately, the authors call for a shift in how remission is clinically defined: sustained control of hyperglycemia and a reduction in excess fat, regardless of how it’s achieved (e.g. lifestyle, medication, surgery). Ultimately the authors are advocating for an updated T2D framework that emphasizes the importance of weight reduction and reflects a clinical reality. |
| Efficacy and safety of automated insulin delivery in children aged 2–6 years (LENNY): an open-label, multicentre, randomised, crossover trial | Tadej Battelino, Salla Kuusela, Ambika Shetty, Ivana Rabbone, Valentino Cherubini, Fiona Campbell | Lancet Diabetes & Endocrinology | Medtronic’s LENNY trial evaluated the MiniMed 780G in young children (ages two to six) with T1D (n=98). In this randomized crossover trial (n=98), auto mode significantly improved Time in Range (TIR) and A1c compared to manual mode with suspend before low. TIR increased 10 percentage points (+2.4 hours/day) from 58% at run-in to 68% with auto mode, compared to 58% with manual mode at 26 weeks. A1c decreased 0.5 percentage points from 7.5% after run-in to 7.0% with auto mode (compared to 7.6% in manual mode). No severe hypoglycemia events were reported, and the safety profile was consistent across groups, with nine serious adverse events (including one DKA episode) deemed unrelated to the study device. These findings support the use of AID in very young children and highlight its potential to improve early glycemic outcomes without added safety risk. The results were first presented by Dr. Tadej Battelino at EASD 2024, with additional insights on the extension phase shared by Dr. Klemen Dovč at ATTD 2025. |
| Nonglycemic and glycemic risk factors for painful neuropathic symptoms and for distal symmetrical polyneuropathy (DSPN) in the Diabetes Prevention Program/Diabetes Prevention Program Outcomes Study | Prof. William Herman (University of Michigan) | Diabetes Care | Drawing data from the DPP/DPPOS cohort (n=1,799), the authors compared patients across four mutually exclusive neuropathy types: (i) no symptoms or signs of DSPN; (ii) neuropathic pain without signs; (iii) other neurological symptoms without pain or signs; and (iv) DSPN. Painful symptoms didn’t appear to correlate with glycemia, challenging proposed metabolic causes. People who experienced painful neuropathic symptoms tended to be female, have higher body weight, and lower estimated glomerular filtration rate. And finally, individuals with DSPN (in comparison to those with neuropathic pain and no signs) were typically older, had greater glycemic exposure, and were more often White. Prof. Herman and his team propose that painful neuropathic symptoms and DSPN may have distinct risk profiles. As such, they advocate for clearer diagnostic criteria and stronger clinical recognition of neuropathic symptoms – both critical steps towards better understanding, preventing, and treating these burdensome complications |
| How weight-loss drugs blew out the US trade deficit | Chelsey Dulaney and Jared Hopkins | WSJ | Lilly has invested $800 million into its manufacturing facilities in Ireland, producing $36 billion worth of the drugs that account for half of US imports from Ireland. Irish imports to the US in 1Q25 have grown 400% compared to the same time period in early 2024. The US trade deficit with the small country of 5.4 million people is now second only to the US trade deficit with China. Companies across all sectors have rushed to stockpile imports in the US in advance of tariffs taking effect. While the Trump administration has yet to announce pharmaceutical tariffs, Lilly and other drug manufacturers with Ireland-based operations have increased US imports to minimize shortages in the event of pharmaceutical tariff announcements. Lilly has also announced plans to invest $27 billion into expanding its US-based production, likely in anticipation of further tariffs. As trade evolves, GLP-1 RAs have become a key part of global economies and are worth watching for reasons beyond their key therapeutic benefits. |
| Diagnosis and Treatment of Type 2 Diabetes in Adults | Dr. Rita Kalyani | JAMA | The article examined the latest estimates for T2D prevalence and its related complications. In particular, about one-third of adults with T2D have CVD, while 10% have severe vision limitations or blindness. Moreover, nearly 40% of people with kidney failure have T2D. To target risk factors for complication development, the authors noted that weight management is important for treatment; however, research has been inconsistent in elucidating the most optimal diet to improve outcomes. Beyond diet, physical activity has been associated significant glycemic and cardiometabolic benefits to mitigate risk factors. For individuals with T2D at high risk for cardiovascular or kidney disease (or with existing comorbidities), GLP-1 RAs and SGLT-2 inhibitors are recommended as first-line medications alongside metformin. |
| Continuous glucose monitoring metrics as a predictor of acute complications in youth with T1D | Ms. Julie Sklar (Quinnipiac University) | DT&T | The 24-month study compared CGM metrics with incidence rates of severe hypoglycemia and DKA/severe hyperglycemia, collecting data comprising over 285 person-years of follow-up. In the cohort, there were 75 severe hypoglycemia events and 15 severe hyperglycemia or DKA events. Those who spent less than 45% Time in Range (70-180 mg/dL) experienced twice as much severe hypoglycemia than those who spent more Time in Range (over 45%) – (p=0.003). Additionally, participants with large standard deviations (defined in this study as coefficient of variation (CV) ≥41%) also had twice as much severe hypoglycemia than those with lower standard deviations (defined as CV <41%) – this last had a statistically significant p value (p=0.006). No significant associations were observed between CGM metrics and DKA and severe hyperglycemia – this may be because DKA was so relatively infrequent, which itself may have been because participants were part of a clinical trial. We were very happy to see this article by Ms. Sklar and the renowned Dr. Lori Laffel and we urge those interested in CGM metrics to read the robust discussion that reinforces the importance of Time in Range. Note that although people with diabetes are all urged to have at least 70% Time in Range, benefits accrued in this trial even for those who spent over half their time out of range. |
| Differential Effect of GLP-1 Receptor Agonists and SGLT2 Inhibitors on Lower-Extremity Amputation Outcomes in Type 2 Diabetes: A Nationwide Retrospective Cohort Study | Mr. Alexander Hong (University of Southern California) and Dr. David Armstrong (USC) | Diabetes Care | At three years, the GLP-1 RA cohort was associated with a 23% lower risk of major lower extremity amputations compared to SGLT-2 inhibitor use, even in those with peripheral artery disease (32% reduced risk) and diabetic foot ulcers (30% reduced risk). The risk of minor lower extremity amputations, diabetic foot ulcers, and overall mortality was also lower in the GLP-1 RA cohort, at 27%, 8%, and 34% lower risk, respectively. |
| Thirty-year glycemic trajectories from young adulthood through middle age | Dr. Abigail Arons and Dr. Dean Schillenger | JAMA Network Open | The authors wrote about the paths of young adults (n=4,684) over 30 years, identifying nine unique glycemic trajectories. The work demonstrated surprising heterogeneity in diabetes risk. Many participants with early impaired fasting glucose (IFG) did not progress to diabetes, while most participants who developed diabetes had no prior IFG. These findings challenge the use of IFG-based screening strategies for young adults, which may not be as accurate as previously accepted. The authors called for age-specific risk tools and prevention strategies to better identify diabetes risk in young adulthood. Moving forward, we encourage the use of multiple screening and diagnostic methods to confirm risk of diabetes progression. |
May 2025
| Title | Author | Journal | Commentary |
| Uptake of and Disparities in Semaglutide and Tirzepatide Prescribing for Obesity in the US | Dr. Chungsoo Kim (Yale University) | JAMA Network | Authors in JAMA Network that analyzed EHR data (n=39 million) to explore the disparities in semaglutide and tirzepatide prescriptions for obesity in the US. Between 2020 and 2024, 2.3% of participants received prescriptions for semaglutide or tirzepatide for obesity. The likelihood of receiving a prescription varied by subgroup. Males were less likely to be prescribed than females (1.2% vs 3.0%), and Hispanic, Asian, and Black patients were less likely to be prescribed than white patients (1.8%, 1.7%, 2.3%, and 2.4%, respectively). Similar trends were observed between socially vulnerable and the least socially vulnerable patients (1.9% vs 2.6%), and rural and metropolitan areas (1.5% vs 2.4%). Low adoption of the drugs and prescription disparities likely reflect both system-level access barriers and patient-level demand, including narrow eligibility, limited insurance coverage, financial considerations, and just pure plain education and awareness. The authors encourage strategies that ensure equitable access to these therapies as the evidence, policy, and reimbursement landscape evolves - we better look more closely at these since we know the percentages of all people of every race and geography and income status can be helped by GLP-1 RAs and GLP-1/GIP RAs and so many combos coming up. Even the highest of these percentages is too small, even without considering the disparities for a moment. |
| Has Cheaper Medicare Insulin Made Patients Healthier | Mr. Ike Swetlitz | Bloomberg | In “Has Cheaper Medicare Insulin Made Patients Healthier?” author Mr. Ike Swetlitz discussed the cost of insulin in the US with USC’s Dr. Anne Peters, aiming to answer the question of whether the right insulin is also the most affordable or accessible choice for each person. Questions of access and drug pricing, as well as patient choice, continue to be top of mind throughout much of the field, for insulin and incretins alike. |
| Blood Glucose Prediction Algorithms Require Clinically Relevant Performance Criteria Beyond Accuracy | Dr. Miriam Wolff and Dr. Anders L. Fougner (Norwegian University of Science and Technology, Norway) | DT&T | The article describes the benefits of a newly developed composite glucose prediction metric (CGPM) for evaluating blood glucose prediction models. The standard metric – root mean squared error (RMSE) – misses critical real-world factors like glucose prediction timing and the forecasts’ ability to predict hypo- and hyperglycemic events. The proposed CGPM meshes three metrics: RMSE, temporal gain, and geometric mean, each targeting a different source of potential error. The authors specifically proposed continuing to use RMSE to address baseline errors in predictions, temporal gain for time series forecasting variations, and geometric mean to accommodate glycemic events. We are certainly intrigued by new metrics that take a more holistic view of a patient’s glycemic experience, and look forward to seeing how the authors work to promote their adoption in the research and clinical arenas. |
| Re-Evaluating Inpatient Prandial Insulin Administration Timing: From Data to Clinical Practice | Drs. Hou-Hsien Chiang and Irl Hirsch (University of Washington) | DT&T | They highlighted a growing trend toward postprandial insulin administration, driven by frequent meal interruptions that contribute to inpatient hypoglycemia. This trend has led to increased rates of postprandial hyperglycemia. To address this, they outlined several potential interventions:
Ultimately, they emphasized the importance of targeting pre-meal insulin administration for patients at higher risk of postprandial hyperglycemia, particularly those with T1D and insulin-requiring T2D. In hospitals, this can be more complicated than it sounds. |
| Automated Insulin Pump in Type 2 Diabetes | Dr. Betul Hatipoglu (University Hospitals Cleveland) | NEJM | Dr. Hatipoglu highlighted the results of Tandem’s 2IQP pivotal trial of Control-IQ+ in T2D, which were presented during Day #1 of ATTD and simultaneously published in NEJM in March. Dr. Hatipoglu said the decrease in A1c and increase in Time in Range shown by the AID system may prompt clinicians to consider the use of AID systems in this population to address gaps in care. She also addressed practical barriers to uptake, including insurer mandates for frequent follow-ups and the broader lack of diabetes self-management education in the US. Many clinics lack the infrastructure and staff to deliver high-touch training and support – issues that will only intensify as AID adoption expands across a more heterogeneous T2D population. As a reminder, Control-IQ+ received FDA clearance for adults with T2D in February 2025, and Omnipod became the first AID system approved for people with T2D in August 2024. |
| ATGL links insulin dysregulation to insulin resistance in adolescents with obesity and hepatosteatosis | Dr. Aaron Slusher (Yale University) | The Journal of Clinical Investigation | The study collected biopsies of adipose tissue from 30 adolescents with obesity, including 17 with insulin resistance, before and after insulin infusion. Researchers evaluated glycerol turnover and phosphorylation of adipose triglyceride lipase (ATGL), an insulin-regulated enzyme that breaks down stored fat, as a readout of lipolysis activity (the breakdown of fat). Insulin inhibits ATGL, signaling a “fed state” and preventing fat breakdown. ATGL activation was higher in adolescents with insulin resistance than insulin sensitivity before insulin. Moreover, ATGL activation was reduced in insulin-sensitive adolescents after insulin infusion, but not in insulin-resistant adolescents, suggesting dysregulation of insulin’s inhibition of lipolysis. The research proposes a potential therapeutic target for intervention to prevent type 2 diabetes. See a simplified summary published by the Yale School of Medicine here. |
| Association between Time-in-Range and diabetic retinopathy: Learnings from DCCT to recent times | Dr. Viral Shah (Indiana University) | DT&T | The authors compared two studies: (i) a four-year study (n=163) of adults with T1D with or without DR; and (ii) a “virtual DCCT” (n=1,441) from which CGM data was generated via machine learning from seven BGM measurements every three months. Both studies found strong associations between Time in Range (TIR; 70-180 mg/dL), Time in Tight Range (TITR; 70-140 mg/dL), and DR incidence. |
| Safety and functionality of a novel clinical decision-support algorithm with insulin efsitora alfa in adults with T2D: Early feasibility study | Michelle Katz, Christof Kazda, Jie Xue, Juan Frias, Ronald Brazg, Jit Mitra, Stephanie Gleissner, Eyal Dassau | DT&T | This was a feasibility study examining the efficacy of a clinical decision support (CDS) algorithm for titrating Lilly’s once-weekly basal insulin efsitora alfa. The 16-week study enrolled adults with T2D previously on basal insulin or not on insulin (n=68). The CDS algorithm provided dose recommendations, and investigators could either accept or override the recommendation. Dosing overrides were infrequent in both populations, occurring for ~1% or fewer of total injections - indicating high investigator confidence. Participants experienced significant improvements in A1c from baseline to Week 16 (p<0.05), and the proportion of participants achieving fasting blood glucose targets increased in both populations. The algorithm was also deemed safe, with no level 3 hypoglycemia observed during the trial. |
| Dexcom G7 accuracy and reproducibility in the ICU | Dr. Jesica Baran (University of Washington) and Dr. Irl Hirsch (University of Washington) | DT&T | This was a small and compelling study (n=30) evaluating the accuracy of the Dexcom G7 CGM in an ICU setting by Dr. Jesica Baran (University of Washington) et al. UW’s Dr. Irl Hirsch co-authored the study on behalf of the TIGHT RCT Study Group, which presented its findings at ADA 2024 that CGM alone did not improve glycemic management among patients with type 2 diabetes in the hospital. Dr. Baran’s study analyzed 1,515 sensor-blood glucose pairs and found that the MARD in the ICU was slightly higher relative to outpatient MARD, with a mean difference of 12 mg/dL. However, authors noted that this performance (16%) was comparable to that observed in non-ICU hospitalized patients, which achieved a MARD of 15%. We appreciate the continued focus on demonstrating the need for even greater CGM efficacy in inpatient settings, and look forward to additional data on the use of glucose trends and alarms in this patient population. |
| Long-term health improvements and economic performance among individuals with diabetes | Dr. Jack Chapel (USC) | JAMA Health Forum | This article examined long-term health and economic outcomes among people with diabetes aged 40 to 64 years in the US. The study analyzed self-reported data from the National Health Interview Survey from 1998 to 2018, including nearly 250,000 individuals - about 25,000 had diabetes. From 1998 to 2018, health outcomes significantly improved among people with diabetes, with declines in mortality and lower self-reported health limitations on daily activities. However, economic outcomes did not change significantly over time. From 1998 to 2018, people with diabetes were eight to 11 percentage points less likely to be in the labor force and four to six percentage points more likely to claim disability insurance income than matched peers. The authors acknowledged some limitations with the analysis, including its reliance on self-reported survey data and lack of distinction between T1D and T2D. The authors said more research is needed to explain this paradox. |
| Glucose-lowering medications, glycemia, and cognitive outcomes: GRADE randomized clinical trial | Jose Luchsinger, Samuel Rosin, Erin Kazemi | JAMA Network | This delved into results from the GRADE trial (n=3,721), which compared secondary glucose-lowering drugs and cognitive performance for people with a shorter duration of T2D (<10 years). At baseline, participants had T2D for 4 years, were 57 years old, and 62% were male. They were randomized to receive one of four drugs – long-acting insulin (insulin glargine U-100), sulfonylurea (glimepiride), GLP-1 RA (liraglutide), and DPP-4 inhibitor (sitagliptin) – on top of metformin and were followed for four years. Contrary to the hypothesis that insulin glargine and liraglutide would confer better cognitive outcomes, investigators found no difference in cognitive performance across treatment groups. However, higher A1c was associated with lower cognitive function, as assessed by the Digit Symbol Substitution Test, with scores decreasing by -0.94 per 1 unit increase in A1c (scores range from 0-100, making this change relatively modest). The Spanish English Verbal Learning Test demonstrated a decrease of -0.27 per 1 unit increase in A1c (scores range from 0-15, representing a larger relative decrease using this metric). Severe hypoglycemia, which is associated with cognitive decline, was rare in all four groups (0.9%). The authors note that another study, ACCORD-MIND (n=2,977), found no difference between intensive (A1c goal <6%) and standard glycemic management (A1c goal between 7-7.9%). They believe that hypoglycemia due to a low A1c goal might have countered the cognitive benefits of lower glycemia. |
| Finerenone in heart failure with improved ejection fraction: FINEARTS-HF randomized clinical trial | Dr. Maria Pabon (Brigham and Women’s Hospital) | JAMA Cardiology | An analysis of the FINEARTS-HF RCT demonstrated the safety and efficacy of finerenone in patients with heart failure (HF) with improved ejection fraction (HFimpEF), a high-risk population. Recent advances in the management of HF have led to an increased population of patients with HFimpEF. However, these patients have historically been excluded from major HF trials, which has limited analysis. In this study of 6,001 patients with HF, the treatment effect of finerenone on cardiovascular death and worsening HF events was consistent between patients with HFrEF and HFimpEF. The absolute risk reduction was also greater among those with HFimpEF (9.2 vs 2.5 per 100 patient-years). Patients with HFimpEF tended to develop more hypotension with finerenone treatment, but the safety profile of finerenone was acceptable overall. The treatment benefits of finerenone were consistent among patients with HFimpEF compared to the overall population of patients with HFpEF. These patients remain at heightened risk of adverse outcomes, but finerenone safely and effectively mitigates some of this risk. |
| Early Detection of β-Cell Decline Using Home Dried-Blood-Spot C-Peptide Levels in New-Onset Type 1 Diabetes | Dr. Emile Hendriks (University of Cambridge, UK) | Diabetes Care | Currently, the ability to secrete endogenous insulin is evaluated by the mixed-meal tolerance test (MMTT), which is invasive and cumbersome and, thus, is not conducted in routine clinical care. Hence, the investigators assessed whether dried-blood-spot (DBS) C-peptide levels taken at home predict early decline of beta cell function. Participants with T1D (n=292) collected finger-prick DBS C-peptide data ~6.5 times over the year; at 12 months, they underwent MMTT. Excitingly, investigators found that DBS C-peptide levels from the first six months were associated with peak C-peptide levels at 12 months from MMTT, suggesting the potential of at-home finger-prick testing. |
| Overweight and obesity – capturing the whole picture | Dr. Vanita Aroda (Harvard University) and Dr. Leigh Perreault(University of Colorado Anschutz) | NEJM | Drs. Aroda and Perreault discuss the importance of studying obesity treatments in different ethnic populations. The GLORY-1 study was conducted in China (n=610), and participants had notable demographic differences compared to previous obesity studies like SURMOUNT-1. The mean age in this study was 34 years versus 45 years in SURMOUNT-1, and average BMI was 31 kg/m2 versus 38 kg/m2. Prevalence of prediabetes was also significantly lower, at 11% compared to 41% in SURMOUNT-1. However, nearly 50% of GLORY-1 participants had metabolic dysfunction-associated fatty liver disease (MAFLD) compared to just 7% in SURMOUNT-1, and 62% versus 30% had dyslipidemia. The overall prevalence of weight-related coexisting conditions was high in GLORY-1, at 89%. Projections indicate that over half the global adult population will have overweight or obesity by 2050, with 627 million people in China alone. Notable differences in the prevalence of obesity-related conditions within this population encourage further exploration of ethnic differences in overweight and obesity and in the importance of individual-level risk assessment. In sum, Drs. Aroda and Perreault describe therapeutic agents as key components of an expansive public health toolbox needed to tackle obesity on a global scale. |
| GLP-1R Polymorphisms Modify the Relationship Between Exposure to Gestational Diabetes and Offspring BMI Growth: The EPOCH Study | Dr. Kylie Harrall (University of Florida) | Diabetes Care | This EPOCH study (n=464) evaluated how GLP-1 receptor gene polymorphism, or variations in gene sequence, impacts the association between exposure to gestational diabetes and metabolic markers in children. BMI was measured from 27 months to 18 years of age, and an oral glucose tolerance test (OGTT) was conducted during adolescence. Could that have been CGM? Regardless, researchers found that minor alleles of rs10305420 (genotypes CT or TT) and rs1042044 (CA or AA), as well as the major allele of rs6923761 (GG), were associated with higher BMI when participants were exposed to gestational diabetes before birth. GLP-1 receptor gene polymorphism did not modify the association between gestational diabetes and glucose homeostasis. This is exactly the kind of study we'd hope could continue even longer to assess the associations. |
| CoQ imbalance drives reverse electron transport to disrupt liver metabolism | Dr. Renata Goncalves (Harvard University) | Nature | This piece shows that dysregulation of coenzyme Q in the liver leads to excess reactive oxygen species (ROS) production by mitochondria within the complex I enzyme. Excess ROS has previously been linked to obesity and age-related diseases, but its exact origins have remained unknown. This work may potentially improve the targeting of therapeutics aimed at reducing ROS. In prior studies, eliminating ROS using broad antioxidants had not improved outcomes in conditions like obesity, insulin resistance, and cardiovascular disease, but these new findings may improve site-specific targeted therapeutics for obesity and T2D. Lead author Dr. Renata Goncalves (Harvard University) said that future treatments may consist of “a tailored cocktail of compounds” to treat metabolic diseases, including T2D. In many cases, treatment paradigms begin at the source, and we’re encouraged by the new opportunity to target sources of ROS. |
April 2025
| Title | Author | Journal | Commentary |
| Combination of Glucagon-Like Peptide 1 Receptor Agonist and Thiazolidinedione for Mortality and Cardiovascular Outcomes in Patients With Type 2 Diabetes | Dr. Jing-Xing Li et al. | JAMA Network | The authors explored the potential for GLP-1 RA and thiazolidinedione (TZD) combination therapy to yield cardiovascular benefits in T2D. The authors note that combination therapy has recently emerged as a critical area of interest— we wonder if this contributed to their decision to explore TZD therapies from a new angle even as these treatments have decreased in popularity. In 2010, TZDs reached peak revenue at nearly $5 billion dollars, which was quickly halted by the introduction of the generic form, pioglitazone, in August 2012. Side effects of TZD therapy may include stroke, heart failure, weight gain, which has certainly contributed to their decline in popularity. A total of n=220,822 patients with T2D who received a GLP-1 RA or TZD during the study window, alongside a control group, were enrolled from Taiwan’s National Health Insurance Research Database. Patients receiving GLP-1 RA and TZD combination therapy had five times less risk of all-cause mortality and cardiovascular mortality, and were 15% less likely to experience major adverse cardiovascular events. However, a 61% higher risk of hypoglycemia was seen in patients receiving combination therapy, alongside a 69% higher risk for patients only using TZDs compared to nonuse. This risk may be mitigated with prolonged use. The authors note that GLP-1 RAs seemingly reduce the most severe side effects of TZD therapy when used in combination, which may reopen a current-day therapeutic avenue for TZDs. |
| Reduction of Postprandial Glucose Excursions in Adults, Adolescents, and Children with Type 1 Diabetes Using Ultra-Rapid Lispro Insulin and Control-IQ+ Technology | Dr. Grazia Aleppo and Jaeb's Dr. Roy Beck, et al | DT&T | The study compared the use of Lyumjev (ultra-rapid acting lispro) to insulin lispro in Control-IQ+ users with T1D (n=176). Tandem previously presented results of a prospective study examining t:slim X2 with Control-IQ+ (at the time called Control-IQ 1.5) at ATTD 2024. As a reminder, Tandem launched Control-IQ+ in the US last month, which features several enhancements vs. Control-IQ. In this article, Lyumjev with Control-IQ+ was associated with welcome improvements in postprandial glycemic outcomes. Postprandial glucose most differed 60 minutes post-meal (166 mg/dL with Lyumjev vs. 178 mg/dL with lispro; p<0.001). Greatest improvements were observed after breakfast meals (compared to lunch and dinner) as well as in those with greater insulin resistance (i.e., lower ICR [insulin-to-carb ratio]). |
| Spending on Glucagon-Like Peptide-1 Receptor Agonists Among US Adults | Mr. Stavros Tsipas et al. | JAMA Network | The authors quantified the explosion in GLP-1 RA spending in recent years. The article analyzes total US adult spending on GLP-1 RAs from 2018 to 2023, finding an overall >500% increase during the five-year period. See the key findings here: (i) Spending increased from just under $15 billion to over $70 billion from 2018 to 2023; (ii) a mean of 34% growth per year was observed from 2018 to 2022 and spending grew by 62% from 2022 to 2023 alone; and (iii) spending also differed, of course, according to drug. The study authors acknowledged multiple limitations in the dataset used to generate these estimates, including exclusion of sales at compounding pharmacies and prescription indication without adjustment for rebates, discounts, or price concessions. Given the limitations, they suggested that the study may somewhat overestimate spending – compounding not being counted, of course, would increase the sales estimates, though the estimates covered by commercial insurance should be given a 40 to 60 percent haircut. |
| Association between maternal diabetes and neurodevelopmental outcomes in children: a systematic review and meta-analysis of 202 observational studies comprising 56·1 million pregnancies | Dr. Wenrui Ye et al. | The Lancet Diabetes & Endocrinology | The study included 202 observational studies covering a global dataset of over 56 million pregnancies. 54% (n=110) of the included studies investigated gestational diabetes, while 40% (n=80) focused on pre-gestational diabetes, defined as type 1 diabetes, type 2 diabetes, or pre-gestational diabetes not otherwise specified. 84% (n=169) exclusively focused on children and adolescents aged 18 years or younger. The analysis concluded that maternal diabetes, particularly pre-gestational diabetes, was significantly associated with increased risk of neurodevelopmental disorders in offspring, including autism spectrum disorder (ASD, included in 48% of studies), attention-deficit/hyperactivity disorder (ADHD, included in 25% of studies), and intellectual disability (included in 13% of studies). Moreover, early diagnosis of gestational diabetes (diagnosed at ≤26 weeks) was significantly associated with ASD and ADHD, but this association did not hold for diagnoses after 26 weeks. Given these findings, the authors emphasized the importance of early detection and proactive diabetes management before and during pregnancy to minimize long-term neurodevelopmental risks in children. |
| A Comparative Analysis of Glycemic Metrics Derived From Three Continuous Glucose Monitoring Systems | Dr. Guido Freckmann et al. | Diabetes Care | This single center, prospective, interventional study (n=23) compared glycemic metrics across three next-generation CGMs – FreeStyle Libre 3, Dexcom G7, and Medtronic’s Simplera – used over a 14-day period by people with T1D. CGM-derived metrics were calculated separately for each device, revealing substantial differences in glucose profiles and significant intra-participant discrepancies. Agreement was highest between FreeStyle Libre 3 and G7, while Simplera tended to report lower glucose levels that would have led to varying therapeutic decisions for the same individual. Notably, the study found substantial discrepancies in Time below Range (TBR) among CGM systems: the maximum within-participant TBR difference between FreeStyle Libre 3 and Simplera was 12.9% (185 minutes), and the target of TBR <4.0% was met by 70% of participants using FreeStyle Libre 3, 48% using G7, and only 26% using Simplera. These differences have important clinical implications and could influence therapeutic decisions, target attainment, and self-management. This analysis highlights how much CGM choice matters, even among the most advanced systems, and why alignment across platforms will be key as diabetes tech continues to evolve. |
| Association of Patient Cost Sharing With Adherence to GLP-1RA and Adverse Health Outcomes | Dr. Donglan Zhang et al. | Diabetes Care | The retrospective analysis examined the association between out-of-pocket (OOP) GLP-1 RA costs, non-adherence, and healthcare resource utilization. This analysis of MarketScan Commercial data included adults with T2D aged 18-64 years who initiated GLP-1 RA therapy between 2016 and 2021 (n=61,907). Participants were enrolled in the same private insurance plan for six months before prescription and one year after prescription. Participants were categorized into quartiles according to their average first 30-day OOP costs. Those in the highest OOP quartile were 25% more likely to be non-adherent than the lowest OOP quartile (OR=1.25; CI: 1.19-1.31). Non-adherence was subsequently associated with increased incidence rates (IRR) of diabetes-related hospitalizations or ED visits (IRR=1.86; CI: 1.43-2.42) and all-cause ED visits (IRR=1.38; CI: 1.32-1.45). GLP-1 RA non-adherence was also associated with increased hospitalization duration (IRR=1.56; CI: 1.41-1.72). Consequently, ED-related medical costs were elevated, increasing by $70 on average (CI: $53.54-$86.08), due to non-adherence. |
| M120 Risk Score Improves Identification of Children at High Risk of Developing Clinical Type 1 Diabetes and Reports Short-term Response to Preventive Immunotherapy | Dr. Minh Le et al. | Diabetes Care | The study assessed the metabolic risk score M120, which includes age, BMI, and IA-2A status, as well as A1c, glucose, and C-peptide measurements from a blood sample collected 120 minutes after an OGTT among participants in the TN-01 screening and monitoring trial. Compared to OGTT, M120 stratification increased the pool of high-risk children by at least 26%, including 40% who had stage 1 T1D. The study also assessed whether M120 could serve as a surrogate marker of beta cell function, indicating early treatment effects of Tzield (teplizumab) in the TN-10 trial. M120 scores increased progressively in participants receiving placebo from baseline to six months, while M120 scores decreased in the Tzield group over the same period (p<0.001). Based on these findings, the authors suggest that M120 risk stratification may be more effective compared to OGTT, emphasizing the measurement simplicity of a single blood draw. Furthermore, the authors highlight that this score could potentially improve adherence to monitoring and increase its cost-effectiveness among children at high risk of progressing to T1D. |
| Real-World Performance of Personal Continuous Glucose Monitors During Hospitalization | Dr. Adrian Dumitrașcu et al. | DT&T | The authors evaluated the accuracy of patients’ personal CGMs in an inpatient setting. The study compared CGM to point-of-care (POC) testing and laboratory values across 188 hospitalizations involving 101 adult patients with diabetes. Overall glycemic outcomes showed a mean Time below Range (TBR) of 2%, Time in Range (TIR) of 59%, and Time above Range (TAR) of 40%. Personal CGMs demonstrated adequate accuracy for inpatient glucose monitoring across all ranges except for hypoglycemia. This study echoes key takeaways from Dr. Cecilia Low Wang (University of Colorado), who advocated for CGM use as an adjunct to POC testing in the hospital at ATDC 2024. She emphasized the importance of establishing standardized clinical guidelines, harnessing data like those published here in DT&T, to support the expected growth in CGM use in inpatient care. |
| Engagement in Hypertension and Diabetes Clinical Trials at Federally Qualified Health Centers | Dr. Samual Byiringiro | JAMA | The author analyzed 33 clinical trials conducted from 2013 to 2023 that addressed hypertension or type 2 diabetes in adults at 67 federally qualified health centers (FQHCs) across the US. Most FQHCs were urban (78%) and had EHR capabilities (90%). Engagement was typically limited to participant recruitment and intervention delivery, with FQHCs often sharing EHR data to identify potential participants but not involved in study planning or design. Those higher-engagement FQHCs – involved in planning or leading the study – were found to have more robust staffing (higher physician and patient education specialist ratios), served a greater proportion of Black or African American patients (42% vs. 32% overall, p<0.05), and had fewer patients with private insurance (6% vs. 13% overall, p<0.01). The findings underscore the need for more inclusive trial design processes that engage FQHCs earlier and more meaningfully. |
| Dysglycemic Events after Initiation of Intermittently Scanned Continuous Glucose Monitoring in Patients with Insulin-Treated Type 2 Diabetes | Dr. Lisa Gilliam et al. | DT&T | In this large retrospective cohort study of people with insulin-treated T2D using Freestyle Libre 2 (n=49,387), 14% of participants achieved an A1c <7.0% after using isCGM, up from 9% at baseline. Nearly half (49%) had an A1c <8.0% after using isCGM, up from 29% at baseline. One-quarter had an A1c >9.0% after isCGM, down significantly from 41% at baseline. Among non-initiators, there was no change in the proportion of participants with A1c <7.0% or <8.0%. For acute dysglycemic events, isCGM users demonstrated no improvement in hypoglycemia, with 3% of participants experiencing an event pre- and post-baseline. In the control group, hypoglycemic events increased slightly from 1% to 2%. Hyperglycemic events decreased slightly with the use of isCGM, occurring in 3% of participants pre-intervention compared to 2% post-intervention, compared to no change in the control group (1%). The authors noted that the study population had high average A1c values at baseline, and measured only initiation of isCGM, not its continued use. This study demonstrates the continued glycemic benefit of isCGM, but further supports the use of real-time CGM for patients at risk of hypo- or hyperglycemic events. |
| Impact of Islet Transplantation on Diabetes Complications and Mortality in Patients Living With Type 1 Diabetes | Dr. Quentin Perrier et al. | Diabetes Care | The retrospective, multicenter, cohort study included 61 IT recipients matched to 610 T1D control patients and 45 IT recipients after kidney transplantation matched to 45 T1D control patients over a median follow-up period of over 10 years (n=761). IT recipients with and without kidney transplantation were 39% likely to have composite negative outcomes including death, dialysis, amputation, nonfatal stroke, nonfatal myocardial infarction, and transient ischemic attack, compared to 52% for the control group. The major factors contributing to this were reduced mortality of 22% for IT patients without kidney transplantation and reduced risk of dialysis of 19% for patients receiving kidney transplantation. Both groups showed no significant changes in cancer risk despite the use of immunosuppressive drugs following IT. The improvements to complications and lack of increase to cancer risk highlight the long-term benefits of islet transplantation for T1D. |
| Observations on the Discovery of Glucagon-Like Peptide-1 Action | Prof. Jacques Philippe and Dr. Alvin Powers | JAMA | The authors reflected on Dr. Daniel Drucker’s critical role in the pioneering discovery of glucagon-like peptide-1 (GLP-1). The authors worked as postdoctoral fellows (1984-1988) in Dr. Joel Habener’s laboratory at Massachusetts General Hospital (MGH), which was focused on prohormone processing and peptide action. There they collaborated closely with Dr. Drucker (now at Lunenfeld-Tanenbaum Research Institute and University of Toronto) and Dr. Svetlana Mojsov (now at Rockefeller University). Following the identification of DNA sequences of GLP-1 and GLP-2, Dr. Mojsov developed antibodies and radioimmunoassays to study proglucagon-derived peptides. Both Dr. Drucker and Dr. Mojsov discovered several forms of GLP-1s (1-37 and 7-37) in 1986 in their collaborative studies of the posttranslational processing of proglucagon. During this time, Dr. Drucker, in collaboration with Dr. Philippe and others, found that the shorter, glucose-dependent form (7-37) promoted insulin secretion, upregulated cAMP, and increased insulin gene expression in islets. In the JAMA Viewpoint of key events in the Habener Lab, Prof. Philippe and Dr. Powers noted that Dr. Drucker’s work was the first demonstration of GLP-1 action and laid a foundation for subsequent studies of GLP-1. Prof. Philippe and Dr. Powers also emphasized the importance of basic science research as it can lead to incretin-based therapies like Novo Nordisk’s semaglutide and Lilly’s tirzepatide that are now used in the treatment of millions of patients with obesity, diabetes, cardiovascular, and/or kidney diseases. |
| Childhood Exposure to Air Pollution, Body Mass Index Trajectories, and Insulin Resistance Among Young Adults | Dr. Fangqi Guo et al. | JAMA | The authors investigated the long-term impact of childhood exposure to traffic-related air pollution on insulin resistance in young adults. Dr. Guo et al. followed participants in Southern California (n=282) from gestation through age 24. Researchers found that higher childhood nitrogen oxides (NOx) exposure was associated with increased BMI at age 13, which predicted faster BMI growth and elevated insulin resistance in adulthood. These findings suggest that environmental exposures in early life can have long-lasting effects on metabolic health via weight-related pathways. The study adds compelling evidence to the growing call for integrating environmental risk mitigation into pediatric obesity and diabetes prevention strategies. It’s encouraging to see continued research emerging on environmental determinants of health, underscoring how factors like air quality and residential exposures may play a more significant role in metabolic outcomes than previously recognized. |
| High-Dose Semaglutide (Up to 16 mg) in People With Type 2 Diabetes and Overweight or Obesity: A Randomized, Placebo-Controlled, Phase 2 Trial | Dr. Vanita Aroda et al. | Diabetes Care | The authors characterize the dose-dependent effects of semaglutide in people with T2D and overweight or obesity. In a parallel-group, blinded, phase 2 trial, participants (n=245) on metformin with T2D and BMI ≥27 kg/m2 were randomized to weekly semaglutide (2, 8, or 16 mg) or placebo. The estimated treatment difference between the 16 and 2 mg doses was -0.3% for A1c change and -3.4 kg for weight change for the treatment policy estimand. As expected, notable treatment-emergent adverse events (AEs) and subsequent treatment discontinuations were more frequent in the semaglutide 8 and 16 mg groups than in the 2 mg group. The AEs were primarily gastrointestinal. No severe hypoglycemic episodes were reported. It would be terrific to see if CGM was used to highlight benefits of semaglutide beyond the A1c change noted. The authors conclude that higher semaglutide doses for T2D and overweight or obesity provide modest additional glucose-lowering effect and additional weight loss, which comes at the expense of increased AEs and treatment discontinuations. Additional work evaluating high-dose semaglutide in obesity without T2D is currently underway, as reported by the authors. Notable studies have evaluated semaglutide dosing in recent months, such as the phase 3b STEP UP study where semaglutide 7.2 mg demonstrated a statistically significant and superior weight loss of 20.7% at week 72 compared to semaglutide 2.4 mg and placebo. Note this is a free article - no paywall, lots of changes to learn. |
| Long-term effects and effect heterogeneity of lifestyle and metformin interventions on type 2 diabetes incidence over 21 years in the US Diabetes Prevention Program randomised clinical trial | Dr. William Knowler et al. | The Lancet Diabetes & Endocrinology | As a follow-up to the landmark US Diabetes Prevention Program (DPP), participants in the DPP Outcomes Study (DPPOS; n=3,195) discontinued placebo, continued metformin treatment, and were offered group-based lifestyle interventions four times a year; those in the intensive lifestyle support (ILS) group received booster intervention classes. Compared to placebo, diabetes incidence rate decreased in the original ILS group (hazard ratio: 0.76) and original metformin group (hazard ratio: 0.83); these findings translate to increases in mean duration of diabetes-free survival of 2.0 years and 1.2 years, respectively. The diabetes cumulative incidence curves separated early, especially in the first three years, with ILS and metformin groups demonstrating lower incidences. Overall effects were attributed to early treatment benefits during the DPP. Additionally, intervention effects appeared to be heterogeneous, as they were greater with ILS in participants with higher fasting glucose levels, A1c, and multivariate clinical and physiological risk indices; effects were greater with metformin in younger participants. These findings highlight the sustained effects in reducing diabetes incidence and emphasize the advantage of tailored interventions for T2D. |
| Uptake of and Disparities in Semaglutide and Tirzepatide Prescribing for Obesity in the US | Dr. Chungsoo Kim | JAMA Network | The analyzed EHR data (n=39 million) to explore the disparities in semaglutide and tirzepatide prescriptions for obesity in the US. Between 2020 and 2024, 2.3% of participants received prescriptions for semaglutide or tirzepatide for obesity. The likelihood of receiving a prescription varied by subgroup. Males were less likely to be prescribed than females (1.2% vs 3.0%), and Hispanic, Asian, and Black patients were less likely to be prescribed than white patients (1.8%, 1.7%, 2.3%, and 2.4%, respectively). Similar trends were observed between socially vulnerable and the least socially vulnerable patients (1.9% vs 2.6%), and rural and metropolitan areas (1.5% vs 2.4%). Low adoption of the drugs and prescription disparities likely reflect both system-level access barriers and patient-level demand, including narrow eligibility, limited insurance coverage, financial considerations, and just pure plain education and awareness. The authors encourage strategies that ensure equitable access to these therapies as the evidence, policy, and reimbursement landscape evolves - we better look more closely at these since we know the percentages of all people of every race and geography and income status can be helped by GLP-1 RAs and GLP-1/GIP RAs and so many combos coming up. Even the highest of these percentages is too small, even without considering the disparities for a moment. |
March 2025
| Title | Author | Journal | Commentary |
| One-Hour Oral Glucose Tolerance Test for the Postpartum Reclassification of Women With Hyperglycemia in Pregnancy | Dr. Ravi Retnakaran et al. | Diabetes Care | The authors compared one-hour vs. two-hour glucose measurements from an oral glucose tolerance test (OGTT) at three months postpartum to predict the risk of developing dysglycemia (prediabetes/diabetes) over five years (n=369). Given the standard two-hour OGTT is often skipped due to inconvenience, the study explored whether a one-hour OGTT could serve as a more practical, effective alternative. At three months, the one-hour glucose measurement identified 60 of the 70 women diagnosed with dysglycemia by the two-hour glucose threshold and identified an additional 96 women. Regression analyses revealed that the one-hour glucose value at three months postpartum was a stronger predictor of subsequent dysglycemia over the first five years after pregnancy than the two-hour test. We are excited to see this successful longitudinal study highlight the one-hour OGTT as a more convenient and effective alternative for predicting dysglycemia, though we also wonder how CGM could improve early detection and monitoring of dysglycemia in this population, particularly as a non-invasive, real-time alternative to OGTTs. Though it may be more expensive, we believe it would be far, far more convenient and would enroll far more to take part in testing. |
| Continuous Glucose Monitoring-Based Titration of Once-Weekly Insulin Icodec in Insulin-Naive Individuals with Type 2 Diabetes (ONWARDS 9): A Phase 3b, Multicenter, Single-Arm, Treat-to-Target Clinical Trial | Dr. Richard Bergenstal et al. | DT&T | As a reminder, ONWARDS 9 examined the efficacy of CGM-based titration of Novo Nordisk’s Awiqli (once-weekly insulin icodec) for insulin-naive adults with T2D. In this 26-week trial (n=51), Awiqli doses were titrated weekly, based on pre-breakfast CGM values, targeting a fasting glycemic range of 80-130 mg/dL. Mean A1c decreased 1.2% from 8.2% at baseline to 7.0% at Week 26 (p<0.0001). Moreover, Time in Range increased 22% (+5.3 hours/day) from 54% at baseline to Weeks 22-26, driven by reductions in Time above Range. Time below Range was very low throughout the study period (0.03% at baseline vs. 0.04% at Weeks 22-26), and no severe hypoglycemic events were reported. These positive results support CGM-based titration as an effective strategy for initiating insulin therapy. See our full coverage of the trial readout by Dr. Bergenstal at DTM 2024 for a deeper dive into these results and their implications. |
| GLP-1 receptor agonists in kidney transplant recipients with pre-existing diabetes: a retrospective cohort study | Dr. Babak Orandi et al. | The Lancet Diabetes & Endocrinology | The authors examined the real-world efficacy and safety of GLP-1 RA use in people with diabetes who have received a kidney transplant. The study (n=18,016) included people with T2D who did not use a GLP-1 RA prior to their transplant. GLP-1 RA users were younger and more often female compared to non-users. Most users in the study were non-Hispanic Black (35.7%), followed by Hispanic (28.8%) and non-Hispanic White (28.0%). The study found that GLP-1 RA use was significantly associated with a 49% lower incidence of death-censored graft loss (i.e., loss of the transplanted organ before the recipient’s death) and 31% lower mortality. Of note, safety endpoints were similar between groups, except for an increased risk of diabetic retinopathy associated with GLP-1 RA use, a complication that has been observed in previous studies. We are encouraged by the significant benefit GLP-1 RAs provide in reducing the risk of graft loss and mortality, and we are interested in seeing more research on their effects on eye health. |
| Hematologic Cancers Among Patients With Type 2 Diabetes Prescribed GLP-1 Receptor Agonists | Dr. Omer Ashruf et al. | JAMA | This retrospective study (n=1,601,334) included people with T2D prescribed with GLP-1 RAs (n=51,617), insulin (n=938,602), or metformin (n=611,115) between April 2005 and October 2023. The primary outcome was the first diagnosis of hematologic cancer. Compared to metformin, the use of GLP-1 RA was associated with a statistically significantly lower risk of myelodysplastic syndromes (HR: 0.61) and myeloproliferative neoplasms (HR: 0.67). Compared to insulin, the use of GLP-1 RA was associated with a significantly lower risk of myeloid leukemia (HR: 0.42), lymphoid leukemia (HR: 0.45), non-Hodgkin lymphoma (HR: 0.42), myelodysplastic syndromes (HR: 0.19), myeloproliferative neoplasms (HR: 0.50), monoclonal gammopathy (HR: 0.68), multiple myeloma (HR: 0.49), and amyloidosis (HR: 0.52). Across all hematologic cancer types, the use of GLP-1 RAs was associated with 54% lower risk compared with insulin. The study authors attributed the risk of reduction with GLP-1 RAs to weight reduction, immunomodulatory properties of the drug class, or both. Overall, these findings sure suggest that GLP-1 RAs represent a promising treatment for reducing cancer risk. |
| Why the Obesity Drug Revolution Is a Work in Progress | Ms. Madison Muller, Mr. Robert Langreth, and Mr. Ike Swetlitz | Bloomberg | The authors discussed the recent resolutions of supply issues for Wegovy and Zepbound and the impact that this may have on people with obesity. Notably, the authors reported that only 44% of large employers cover obesity management therapies, and Medicare does not offer coverage. Despite recent price reductions to assist cash-paying patients – such as $50 reductions on 2.5-mg and 5-mg Zepbound vials (now $349 and $499 per month, respectively) and a drop in Wegovy’s self-injector cash price from $1,350 to $499 per month – uncertainty around broad-scale accessibility remains. The authors expressed optimism about the development of Lilly’s retatrutide (“triple G”) and oral orforglipron. The ongoing prominence of the GLP-1 RA revolution in public discourse continues to be striking, and we look forward to seeing the results of these next-generation therapies in the years to come. |
| Quantifying Environmental Waste From Diabetes Devices in the U.S. | Ms. Tiffany Tian et al. | Diabetes Care | The authors quantified medical waste generated by diabetes devices. In 2022, healthcare accounted for 8.5% of US emissions and millions of tons of medical waste. In a small study of 49 adults with diabetes, an average of 2.7 pounds of monthly waste per person was generated by participants using insulin pumps, CGM, and BGM (n=38), while users of MDI, CGM, and BGM (n=11) generated 3.1 pounds of monthly waste per person. This amounts to nearly 2% of average household waste globally, demonstrating a substantial environmental impact from diabetes devices. |
| Continuous Glucose Monitoring Use in Youth with Type 2 Diabetes: A Pilot Randomized Study | Dr. Tejal Patel et al. | DT&T | The authors investigated the feasibility, acceptability, and outcomes of CGM use in individuals with youth-onset T2D who have infrequent BGM regimens (≤twice daily). Participants (n=28) were randomized to 12 weeks of CGM versus fingerstick monitoring. The majority of participants were female (82%) and Black (62%). Mean age was 14.9 years old, and baseline A1c was 7.4%. Study participation in the CGM group was 91%, retention was 100%, and most participants (56%) had ≥60% wear time. Minor sensor adhesion adverse events were frequent causes (75%) of reduced wear time. While there were no significant changes from baseline for glycemia, CGM benefits/burden, and diabetes distress, CGM was feasible and acceptable among this population. We hope to see more research on this front, perhaps in a larger population, especially as the incidence and prevalence of youth-onset T2D is increasing worldwide. |
| A Call-to-Action to Eliminate Barriers to Accessing Automated Insulin Delivery Systems for People with Type 1 Diabetes | Dr. Banshi Saboo et al. | DT&T | The authors issued a call-to-action to the diabetes community – including healthcare providers, individuals with T1D, caregivers, and payers – to eliminate barriers hindering access to automated insulin delivery (AID) systems. While continuous glucose monitoring alone improves glycemic control, the authors emphasize that integrating CGMs with AID systems offers superior outcomes by reducing hyperglycemia without increasing hypoglycemia. Citing extensive pivotal trials and real-world data, they report a 20-30% increase in time in range (TIR) when AID is used with a CGM compared to MDI with CGM. We appreciate the article’s emphasis on collaboration among stakeholders to improve AID access, reduce disease burden, and optimize glycemic management to enhance quality of life for individuals with T1D. |
| Suicide and Self-Harm Events with GLP-1 RAs in Adults with Diabetes or Obesity | Dr. Pouya Ebrahimi and Dr. Juan Carlos Batlle et al. | JAMA Psychiatry | Given that bariatric surgery is associated with a 64% increased risk of suicidality, authors conducted a systemic review and meta-analysis to assess whether GLP-1 RAs are associated with suicide and self-harm events. Among 144 RCTs, 27 studies (n=95141) reported suicide or self-harm; the mean baseline age was 59 years, and 44% were female. Event incidence of suicide, suicide attempts, suicidal ideation, or self-harm was very low for both GLP-1 RA (33 total; 0.044 per 100 person-years) and placebo groups (27 total; 0.040 per 100 person-years), with no statistically significant difference (p=0.24). Subgroup analyses based on diabetes status and GLP-1 RA types did not change the results either. While the study did not show an association between GLP-1 RAs and suicidality, the authors still emphasized the importance of continued monitoring. These results are consistent with previous statements by the FDA and EMA, which concluded that insufficient evidence supports a causal link between GLP-1 RAs and suicidality. As we heard at ADA 2024, even if GLP-1 RAs may not directly cause mental health problems, significant weight loss can often alter social interactions, which can contribute to mental health crises, and we concur with the authors about the importance of psychosocial monitoring in patients on GLP-1 RAs. |
| The Importance of Instigating Automated Insulin Delivery Systems at Onset of Type 1 Diabetes: 1-Year Follow-Up of Children and Adolescents from Two Tertiary Pediatric Diabetes Centers | Dr. Ivana Rabbone et al. | DT&T | The authors evaluated real-world glycemic outcomes in children and adolescents who initiated either AID, predictive low-glucose suspend (PLGS), or MDI in the first month after diabetes onset (n=84). The study found that A1c was significantly lower in the AID group (6.6%) compared to the PLGS group (7.4%) and the MDI group (7.6%; p=0.001). Both the AID and PLGS groups achieved target TIR of 70% after 12 months of treatment; however, the AID group achieved significantly higher TIR than PLGS – 79% vs. 70%, respectively (p=0.001). The AID group also achieved a significantly higher TIR than the MDI group (62%; p=0.001). This difference was driven predominantly by variations in Time above Range (TAR; >250 mg/dL), with the AID, PLGS, and MDI groups seeing TAR of 22%, 27%, and 38%, respectively. Gosh, that is so awful for the MDI group, plus, MDI is so much more challenging than AID or even PLGS. The authors emphasized that these findings reinforce the growing body of evidence supporting the initiation of AID at onset, particularly in children and adolescents diagnosed with T1D, for optimal glycemic management. All we would say is, let's also create a war on hyperglycemia - if we are going to get AID, we'd love to see more focus on reducing hyperglycemia and a bit more attention to what we did in the old days, a little more focus on avoiding hyperglycemia, which, ofc, reduces hypoglycemia also. We love what algorithms enable and we'd love a bit more behavioral work on what to avoid nutritionally. |
| Modeling Cardiovascular Protection With SGLT Inhibition in Type 1 Diabetes: A Risk-Based Approach to Guide Therapy? | Dr. Luxcia Kugathasan et al. | Diabetes Care | Given the benefits of SGLT-2 inhibitors in T2D, a risk prediction model assessed the effects of this drug class on estimated CVD in people with T1D. Wow! The study evaluated the results of SGLT-2 inhibitor empagliflozin in the phase 3 EASE-2 (n=730) and EASE-3 (n=960) trials in people with T1D. The model used the Steno T1 Risk Engine (SRE) and the Scottish Diabetes Research Network (SDRN) to estimate a 10-year cumulative risk of the first fatal or nonfatal CVD event at baseline and Week 26. The mean relative reduction of the 10-year CVD risk was 9.8% in the SRE and 9.6% in the SDRN. These results suggest that SGLT-2 inhibitors could help reduce CVD risk in people with T1D, especially among those with elevated baseline CV risk driven by reductions in A1c, uACR, BMI, and blood pressure. The authors explain that while SGLT-2 inhibitors offer CV benefits, more research is needed to understand whether the benefits outweigh the 2-3% increased risk of DKA in the study population. |
| Albuminuria Responses to Dapagliflozin in Patients With Type 2 Diabetes | Dr. Jelle M. Beernink et al. | JAMA | This crossover trial (n=20) included adults with T2D who had uACR >20 mg/g and eGFR >30 mL/min/1.73 m2. Trial participants were assigned to two one-week treatment periods with dapagliflozin and two one-week treatment periods with placebo in random order, including one-week transition periods in between. The primary outcome was the difference in change in uACR from the start and end of treatment between dapagliflozin and placebo. Dapagliflozin significantly reduced uACR after both exposures (first exposure: 17%; second exposure: 19%), with considerable variability among participants but consistent changes across treatment periods. On the other hand, placebo showed no significant changes (first exposure: 7%; second exposure: 9%), with no consistency across treatment periods. Given these findings, especially on treatment variations, the study authors encourage the need for personalized approaches for the management of diabetes and CKD. |
| Glucose Control in Type 1 Diabetes after Pancreas Transplantation: Does Automated Delivery Offer Comparable Results? | Dr. Martina Zahradnická et al. | DT&T | The study reported results from a prospective study comparing short-term glycemic outcomes among consecutive pancreas-kidney transplant recipients (n=31) to users of either MiniMed 780G (n=200) or t:slim X2 with Control-IQ (n=177). At one month after pancreas transplantation, transplant recipients achieved a significantly lower A1c of 5.6% (wow!) compared to 7.2% with MiniMed 780G and 7.3% with Control-IQ. Transplant recipients also achieved higher Time in Range (90% vs. 72% with MiniMed 780G and 75% with Control-IQ) as well as lower mean glucose (124 mg/dL vs. 153 mg/dL with MiniMed 780G and 148 mg/dL with Control-IQ) at one month post-transplantation. There were no significant differences in Time below Range between groups. |
| Algorithm-Driven Initiation and Adaptation of Hybrid Closed-Loop in Young Children with Type 1 Diabetes: A Pilot Study | Dr. Jacopo Pavan et al. | DT&T | The authors evaluated the safety and efficacy of an algorithm-driven approach to initiating and adjusting hybrid closed-loop (HCL) therapy in children aged two to six years with T1D (n=29). While HCL systems are increasingly used in this population, optimizing pump settings remains a time-intensive task for clinicians. This study tested whether a cloud-based algorithm could safely support pump start and therapy adjustments over an eight-week period at home. The algorithm generated settings for basal rates, insulin-to-carb ratios, correction factors, and sleep schedules. Investigators overrode 15% of recommendations. The algorithm-driven method was found to be noninferior to baseline in Time spent <54 mg/dL and >250 mg/dL (P < 0.001), and significantly improved Time in Range (70–180 mg/dL), Time >250 mg/dL, and mean glucose. There were no significant changes in hypoglycemia measures. Notably, outcomes were similar to a historical cohort managed directly by expert pediatric endocrinologists. These findings suggest that algorithm-supported workflows could help streamline HCL starts in very young children, and authors say a larger trial is warranted to confirm these early results. |
| Drug Reduces Mysterious Particle Involved in Heart Attack Risk | Ms. Gina Kolata | New York Times | We covered the ALPACA results in our ACC Day #2 Highlights, where the Cleveland Clinic’s Dr. Steven Nissen presented extraordinarily compelling data: a single 400 mg dose of lepodisiran reduced Lp(a) by 94% at six months, with durable effects out to 48 weeks. The therapy was well-tolerated, with minimal adverse events. While it remains to be seen whether lowering Lp(a) will lead to reductions in cardiovascular events, phase 3 data from the 12,500-person ACCLAIM-Lp(a) trial are expected in 2029. Lilly is far from alone in this arena – at least four other companies are developing Lp(a)-lowering therapies, including Ionis/Novartis(pelacarsen) and Amgen (olpasiran). The first outcomes data may arrive in 2026, when results from the Lp(a)HORIZON trial of Novartis’ monthly injectable are expected. Lp(a) has long flown under the radar despite being a major genetic risk factor for atherosclerotic cardiovascular disease, myocardial infarction, and stroke. We’re encouraged to see Lp(a) and its implications finally entering mainstream discourse — and hope that this visibility leads to broader screening and better education among clinicians and patients alike. As Dr. Nissen said at ACC, “Patients are waiting.” |
February 2025
| Title | Author | Journal | Commentary |
| Screening for Metabolic Dysfunction–Associated Steatotic Liver Disease–Related Advanced Fibrosis in Diabetology: A Prospective Multicenter Study | Dr. Cyrielle Caussy (Lyon University) et al | Diabetes Care | A study centering on non-invasive screening for advanced fibrosis (AF) related to metabolic dysfunction–associated steatotic liver disease (MASLD) was published in Diabetes Care. The study was motivated by a need to validate the performance of noninvasive tests and compare them to two-step algorithms for detecting patients with a high risk of AF. The prospective multicenter study included participants (n=654) with MASLD, T2D (87%), and obesity (74%). 17.6% of patients had an intermediate/high risk of AF and 9.3% had a high risk of AF. Patients were comprehensively assessed with liver assessment comprising blood-based NITs, vibration-controlled transient elastography (VCTE), and two-dimensional shear-wave elastography (2D-SWE). The authors conclude that the FIB-4 score/VCTE algorithm shows excellent diagnostic performance and applicability for AF screening. Seeing as noninvasive biopsies reduce healthcare costs and improve the likelihood of patient screening, we are encouraged by the exploration of alternatives to traditional screenings. We are all for FIB-4, and yet and still, we think very few patients have heard of it or understand it so … we would praise them for looking at AST/ALT measures, and keep educating about healthy livers |
| Age and Sex Differences in Efficacy of Treatments for Type 2 Diabetes | Dr. Peter Hanlon et al. (University of Glasgow) | JAMA | A meta-analysis examining how age and sex affect the treatment efficacy of SGLT-2 inhibitors and GLP-1 RAs in individuals with type 2 diabetes. The meta-analysis included 103 trials. Results showed that SGLT-2 inhibitors conferred greater cardioprotection in older individuals, with a 24% reduction in major adverse cardiovascular events (MACE) per 30-year age increment (HR 0.76), and less A1c reduction was seen with increasing age. By contrast, GLP-1 RAs were found to be more cardioprotective in younger individuals but demonstrated greater A1c reduction with increasing age. Both drugs were associated with lower risk of MACE. There was also no observed relationship between sex and treatment outcomes. |
| Repeated OGTT Versus Continuous Glucose Monitoring for Predicting Development of Stage 3 Type 1 Diabetes: A Longitudinal Analysis | Prof. Aster Desouter (University of Brussels) et al | Diabetes Care | A study evaluated the oral glucose tolerance test (OGTT), A1c, and intermittent CGM (five-day CGM used twice yearly) for predicting the clinical onset of stage 3 type 1 diabetes (T1D) in individuals with stage 2 T1D (n=34). Over a median 40-month follow-up, 50% progressed to stage 3 T1D. Baseline analyses of standalone metabolic markers found that certain CGM metrics (ROC AUC: 0.77-0.92) predicted progression, as well as elevated OGTT results (ROC AUC: 0.75-0.86). The study’s longitudinal analysis found that A1c, Time ≥120 mg/dL, and Time ≥140 mg/dL increased more in stage 3 T1D progressors, similar to OGTT. However, OGTT-derived AUC glucose (AICc = 71) remained the strongest individual predictor, outperforming CGM Time ≥120 mg/dL (AICc = 75) and A1c (AICc = 80), and was comparable to CGM and A1c metrics combined (AICc = 68). The authors concluded that while OGTT is more effective at predicting risk of progression, repeated CGM and A1c may offer a similarly effective alternative for monitoring those with stage 2 T1D |
| A Cure for Type 1 Diabetes: Are We There Yet? | Mr. Christopher Schaaf and Prof. Lori Sussel (University of Colorado) | DT&T | In the piece, they review the ongoing pursuit of a functional cure for T1D. If you are newer to this field, we recommend it highly; while experienced folks watching T1D cures already will have seen most of this before, it is a most valuable primer. While (non-cure!) insulin therapy has remained the standard of care for over a century, strong research efforts are ongoing in disease-modifying and regenerative therapies. While traditional cure approaches have targeted immune modulation, sustained success has been elusive. Islet transplantation has shown efficacy, yet remains limited by donor shortages and the need for lifelong immunosuppression. More recently, stem cell-based therapies have emerged as a promising avenue, generating an abundant supply of functional beta-like cells for transplantation. Encapsulation technologies offer a potential alternative to immunosuppression by isolating transplanted cells from immune attack, though fibrotic overgrowth and cell death remain key challenges. Ongoing clinical trials and novel immune therapies have demonstrated success in delaying the onset and progression ofT1D, and researchers are actively refining strategies to safeguard transplanted beta cells and achieve long-term insulin independence. While actual cure(s) have long been elusive, tangible progress toward that goal is ongoing and these many developments certainly signal progress. |
| Trump Administration Cuts Put Medical Progress at Risk, Researchers Say | Christina Jewett and Sheryl Gay Stolberg | New York Times | This piece reflects a new policy just put in place in the US to reduce so-called "indirect spending" This news will translate quickly - if there are no changes, as we understand it, "indirect" funding will decline abruptly here in the US, though down to 15% rather than the even lower 10% that was once threatened in a previous US administration. NIH grants are among the most prestigious grants out there to have. While changes in government funding typically move at a much slower pace, this change appears set to be going into place far sooner (read: Monday). No doubt, philanthropic organizations will be asked and will have the opportunity to take on even more in this climate, along with manufacturers, where such funding is allowed and welcomed. Stay tuned for more on this developing story. There will be lots of ways to step up. |
| Short-Term Diabetic Retinopathy Status in People with Type 1 Diabetes Commencing Automated Insulin Delivery | Dr. Matilda Johansson and Prof. Benjamin Wheeler (University of Otago, New Zealand) et al. | DT&T | This study (n=165) examined the risk of early diabetic retinopathy (DR) worsening in people with T1D initiating AID. Prior research has associated rapid A1c improvement with a greater risk of early DR progression. Given AID’s efficacy for rapid glucose lowering, the study sought to examine its effect on short-term DR outcomes. At baseline, nearly all (93%) participants (n=165) used standard pump therapy, and 84% had nil, minimal, or mild DR. After four months on AID, mean A1c dropped from 8.4% to 7.4% (outstanding!). At nine months, DR grading was reassessed: 19% of participants improved, 60% remained stable, and 21% worsened. Most progressors advanced to minimal or mild DR, although 3% progressed to proliferative DR. The study found no increased risk of DR worsening in those with an A1c improvement >1.5 percentage points compared to those with ≤1.5 percentage points. Moreover, initiating AID before the age of 18 years appeared protective (p<0.05). While it’s unclear how much the risk of DR progression influences AID discussions, the authors suggested these findings should alleviate any concerns associated with starting on AID. While we would say that's a small study to form such a conclusive view, we certainly perceive these findings as stirring |
| The Physicians Really Are Healing Themselves, With Ozempic | Ms. Gina Kolata | New York Times | This piece reflects on the growing number of physicians who are using GLP-1 RAs for weight management. The story features personal experiences from physicians, including University of North Carolina’s renowned leader Dr. John Buse, who shared that he started to pay for Wegovy out of pocket after his state stopped covering the drug for state employees. He was then able to get a six-month supply in Europe for a quarter of the price. As Ms. Kolata writes, there are no studies documenting the percentage of physicians using GLP-1 RAs, but physicians have been known to move quickly when adopting highly effective therapies. For instance, when cholesterol-lowering statins were first introduced, cardiologists were among the first to use them in large numbers. Many physicians share similar health concerns as their patients, such as reducing risk factors for heart disease and elevated blood glucose, precipitating GLP-1 RA use. We are encouraged by physicians increasingly recognizing the benefits of these therapies and appreciate hearing their personal experiences, particularly ones as renowned and as committed to our field as Dr. Buse. |
| Cardiovascular Event Prevalence in Type 1 Versus Type 2 Diabetes: Veradigm Metabolic Registry Insights | Dr. Andrew Goldsweig (Baystate Medical Center) et al. | Journal of the Society for Cardiovascular Angiography & Interventions | Researchers found that cardiovascular event risk is significantly lower in T1D than T2D. The study included 5,823 people with T1D and 156,204 people with T2D, aged 46 to 75, from the Veradigm Metabolic Registry. People with T1D were two-thirds as likely (prevalence ratio: 0.66) to have a cardiovascular event compared to people with T2D. By specific event types, T1D was associated with a lower risk for myocardial infarction, percutaneous coronary intervention, stroke, and limb ischemia compared to T2D, while the risk for coronary artery bypass graft surgery, carotid revascularization, and peripheral revascularization did not differ. These findings highlight the different pathophysiologies of T1D and T2D, underscoring the importance of properly diagnosing patients and the need for more research to understand how best to mitigate cardiovascular risk in each population. Ultimately, these results are not surprising. |
| Trends in Obesity-Related Measures Among US Children, Adolescents, and Adults | Dr. Samuel Emmerich (National Center for Health Statistics) et al | JAMA | This study (n=41,449) analyzed the prevalence of obesity-related measures in the US from 2013-2014 to 2021-2023. The study included data from National Health and Nutrition Examination Survey (NHANES), and the prevalence of each obesity-related measure was estimated by overall data, sex, and age group. The study found small increases in the percentage of children and adolescents with obesity, as well as in adults with severe obesity (but not obesity). The study also found no significant changes in obesity-related measures, including waist circumference. The study refers to the Healthy People 2030 goal of reaching an obesity prevalence of 16% in children and adolescents and 36% in adults. With increasing options for weight management techniques and treatments like GLP-1 RAs, we’re curious how such interventions could help address obesity in these populations. |
| Longitudinal Determination of Diabetes Complications and Other Clinical Variables as Risk Factors for Diabetic Ketoacidosis in Type 1 Diabetes | Dr. Priya Bapat (Lunenfeld-Tanenbaum Research Institute, Canada) et al. | Diabetes Care | A longitudinal analysis examines the association between diabetes complications and future diabetic ketoacidosis (DKA) risk using 34 years of data from the Diabetes Control and Complications Trial (DCCT) and the Epidemiology of Diabetes Interventions and Complications (EDIC) study. While poor glycemic outcomes and insulin access have long been recognized as DKA risk factors, this study explored whether macrovascular disease and microvascular complications independently predict DKA occurrence. Among participants with T1D (n=1,441), 297 experienced 488 DKA events during follow-up. Major adverse cardiovascular events (HR 3.16, p=0.001) and late-stage neuropathy, including serious foot ulcer or amputation (HR 1.59, p=0.03), were significantly associated with higher DKA risk. Other independent risk factors included female sex (HR 2.04, p<0.001), higher A1c (HR 1.39 per 1% increase, p<0.001), and current insulin pump use (HR 3.04, p<0.001). These findings suggest that patients with cardiovascular disease (CVD) and advanced neuropathy require targeted interventions to prevent DKA, such as enhanced metabolic (e.g., glycemic and weight) management and DKA education. With increasing focus on DKA education in the field, we are also eager for continuous ketone monitoring (CKM) to be available for people with diabetes. The study highlights the need for a broader approach to DKA prevention beyond traditional glycemic management measures, reinforcing the importance of early identification and proactive management of complications, including pump use, CGM, and the future CKM. |
| Association of Diabetic Ketoacidosis at Onset, Diabetes Technology Uptake, and Clinical Outcomes After 1 and 2 Years of Follow-up: A Collaborative Analysis of Pediatric Registries Involving 9,269 Children With Type 1 Diabetes From Nine Countries | Prof. Tadej Battelino, Dr. Klemen Dovc (University of Ljubljana, Slovenia) | Diabetes Care | This article examined the association between DKA at diabetes onset, diabetes technology uptake, and long-term glycemic outcomes. The study included data from youth diagnosed with T1D in 2019 or 2020 who were followed for two years post-diagnosis (n=9,269), and participants were divided into three subgroups: (i) no DKA; (ii) non-severe DKA; and (iii) severe DKA at diagnosis. About one-third of participants (34%) experienced DKA at diagnosis, with one-eighth of participants (13%) experiencing severe DKA. The findings included: (i) Two years after diagnosis, adjusted mean A1c was higher in the severe DKA group (7.6%) compared to the non-severe DKA (7.4%; p<0.001) and no DKA groups (7.3%; p<0.001); (ii) AID use was associated with lower A1c levels compared to other treatment modalities (i.e., MDI with BGM or CGM and sensor-augmented pump) and mitigated differences between DKA groups after two years (p=0.072). |
| Preoperative SGLT2 Inhibitor Use and Postoperative Diabetic Ketoacidosis | Dr. Anjali Dixit (Stanford University) et al | JAMA Surgery | A study evaluated the risk of postoperative DKA in people using SGLT-2 inhibitors. Hyperglycemic events before surgical procedures have been associated with an increased risk of infection, end-organ injury, longer hospitalizations, and death; FDA guidance recommends that SGLT-2 inhibitors are withheld for at least three days before surgery. This retrospective cohort study included 34,671 people with T2D who underwent emergency surgery (defined as occurring within two days of an ED claim), 7.5% of whom used SGLT-2 inhibitors. The incidence of postoperative DKA was 3.8% among those using SGLT-2 inhibitors compared to 3.5% for those not using this therapy, suggesting preoperative use of SGLT-2 inhibitors in patients undergoing emergency surgery was not associated with increased postoperative DKA risk. The authors suggested these findings could justify relaxing current withholding guidelines. We look forward to future work that may evaluate their effects in scheduled procedures, as well as in patients without diabetes using SGLT-2 inhibitors for the management of heart failure or chronic kidney disease. |
| The Association of Time-in-Range and Time-in-Tight-Range with Retinopathy Progression in the Virtual Diabetes Control and Complications Trial CGM Dataset | Dr. Benjamin Lobo (UVA) et al | DT&T | This study generated virtual CGM traces for all of the 1,441 participants in DCCT, based on the days where PWD in the trial took seven BGM measurements. Dr. Kovatchev presented this at ADA 2024, calculating hazard ratios (HRs) for Time in Range (TIR), Time in Tight Range (TITR), and A1c to predict the development or progression of retinopathy. The study sought to provide more evidence supporting the validation of CGM metrics as predictors for complication risk. It'll only be a matter of time 'til there's cold, hard data on this, but in the meantime, this is very interesting. Each metric demonstrated similar predictive performance. Specifically, for a 1.0 change in standard deviation, the adjusted HR for A1c was 2.37 (CI: 2.13-2.65), TIR was 2.67 (CI: 2.33-3.06), and TITR was 2.74 (CI: 2.36-3.18). Scary - we were very impressed with Dr. Viral Shah of U Indiana when he presented this and of course, with Dr. Boris. We look forward to hearing more at ATTD 2025 from Dr. Kovatchev, who will deliver two presentations: (i) on how digital twin technology can enhance clinical trials and (ii) the role of machine learning in developing a fully closed-loop AID algorithm. The emphasis there is on f-u-l-l-y. As a reminder, he presented preliminary results from a fully closed-loop neural net algorithm with lower computational demands at ATTD 2024. Game on! |
| Impact of bodyweight loss on type 2 diabetes remission: a systematic review and meta-regression analysis of randomised controlled trials | Dr. Sarah Kanbour (Weill Cornell Medicine, Qatar) et al. | The Lancet | This meta-analysis evaluated the relationship between the degree of body weight loss and the likelihood of type 2 diabetes (T2D) remission. The study found that every one percentage point decrease in body weight was associated with a two-percentage point greater likelihood of complete remission, and a three-percentage point greater likelihood of partial remission. Specifically, one year after weight loss intervention, the study found that less than 1% of patients with bodyweight loss of <10% experienced complete remission, compared to 50% in those with bodyweight loss of 20-29% and 79% in those with bodyweight loss of ≥30%. Trends in the effect of body weight loss on partial T2D remission were similar – 5%, 69%, and 90% partial remission was seen in those with body weight loss of <10%, 20-29%, and ≥30%, respectively. There were no significant associations between baseline body weight, A1c, or type of body weight loss with remission. These results show incredible promise in reversing the trend of increasing T2D rates in the US and globally, and we wonder to what degree body weight loss halts or reverses the progression of pre-T2D to T2D. |
| Early Continuous Glucose Monitor Use in Children and Adolescents With Type 1 Diabetes: Rates of Initiation and Impact on Glycemic Outcomes | Dr. Elizabeth Mann (University of Wisconsin) et al | Diabetes Care | This study evaluated the impact of CGM initiation rates on glycemic outcomes in children and adolescents with type 1 diabetes (n=4,164). The study found that 93% (n = 3,877) of participants initiated CGM within three years of diagnosis, with the majority (51%) doing so after 12 months. Comparably, initiation rates were: 21% within three months, 14% at three to six months, and 14% at six to 12 months. Non-CGM users were more likely to be older, male, on public health insurance, from racial and ethnic minority groups, and Spanish-speaking. Earlier CGM initiation was associated with: (i) improved glycemic management – median A1c decreased from a baseline of ~9.9% to 7.9% in the zero-to-three-month group. In the other groups, A1c decreased less with later initiation rates – from a baseline of ~10.1%, the three-to-six-month groups reached an A1c of 7.9%, compared to 8.4% in the six-to-12-month group and 9.5% in the non-CGM group. Moreover, those who initiated CGM within three months had 20% higher odds of achieving A1c <7% compared to those initiating after 12 months, while non-CGM users had 76% higher odds of having A1c >9% compared to early initiators; (ii) reduced diabetes-related complications – with 6.1 DKA events per 100 person-years in the under three-month initiation group compared to 13.1 DKA events per 100-person years in non-CGM users; and (iii) greater subsequent AID adoption – 21% of those initiating CGM within three months were using AID within three years, compared 15% of those initiating after 12 months. |
January 2025
| Title | Author | Journal | Commentary |
| Anti-consumption agents: Tirzepatide and semaglutide for treating obesity-related diseases and addictions, and improving life expectancy | James O’Keefe (University of Missouri-Kansas City) et al. | Progress in Cardiovascular Diseases | Drs. James O’Keefe, Grant Franco, and Evan O’Keefe from the University of Missouri-Kansas City just published a review article. The authors characterize incretin-based therapies semaglutide and tirzepatide as potent “anti-consumption” agents and assert that in addition to the proven benefits of weight loss, glycemic reduction, and cardiovascular and kidney protection, GLP-1 RAs have also been observed to improve substance use disorder or even behavioral (e.g., gambling or shopping) addiction. Notably, they say that GLP-1 RA use has been associated with >50% reduced alcohol consumption, 40% reduction in opioid cravings, and 32% lower risk of tobacco use disorder – possibly due to GLP-1 RA modulation of dopamine signaling in the mesolimbic pathway. |
| Tirzepatide Associated With Reduced Albuminuria in Participants With Type 2 Diabetes: Pooled Post Hoc Analysis From the Randomized Active- and Placebo-Controlled SURPASS-1–5 Clinical Trials | Dr. Ellen Apperloo (University of Groningen, the Netherlands) et al. | Diabetes Care | The post hoc analysis, which pooled the SURPASS 1 through 5 population, examined the change in urine albumin-to-creatinine ratio (UACR) from baseline with tirzepatide relative to active or placebo comparators at Week 40/42. The adjusted mean percent change in UACR from baseline to Week 40/42 was as follows: (i) -19% for tirzepatide 5 mg; (ii) -22% for tirzepatide 10 mg; and (iii) -26% for tirzepatide 15 mg. Wow! Results did not significantly differ across the pooled placebo, active, and insulin comparator studies. Subgroups with UACR ≥30 mg/g experienced more pronounced reductions, as would be expected, and about half of the reduction in albuminuria with tirzepatide appeared to stem from weight loss. This is yet another reason so many patients will benefit from running, now walking to get GLP-1 or GLP-1 combos. Here's to making that more so, in 2025, diabetes world. |
| Effectiveness of Semaglutide and Tirzepatide in Overweight and Obese Adults with Type 1 Diabetes | Janet K. Snell-Bergeon (Barbara Davis Center for Diabetes) et al. | DT&T | A study examined the effectiveness of off-label semaglutide and tirzepatide use in adults with T1D and obesity or overweight. The retrospective chart review included 100 adults prescribed semaglutide (n=50) or tirzepatide (n=50) and 50 controls matched for age, sex, diabetes duration, BMI, and A1c. Over a 12-month period, both drugs demonstrated significant benefits for weight loss and glycemic outcomes. Semaglutide users lost 9.1% of their body weight (−19.2 lbs), while tirzepatide users achieved a remarkable 21.4% reduction (−49.4 lbs). A1c also improved, dropping by 0.5% with semaglutide and 0.7% with tirzepatide. As expected, the control group showed no changes in weight or A1c. With the growing off-label use of semaglutide and tirzepatide in patients with T1D, these findings underscore the urgent need for larger, prospective trials to evaluate their long-term safety and efficacy. |
| Phase 1b Dose Escalation Study of Sozinibercept Inhibition of Vascular Endothelial Growth Factors C and D With Aflibercept for Diabetic Macular Edema | Dr. David Boyer (Retina-Vitreous Associates Medical Group), et al. | Translational Vision Science & Technology | A recent phase 1b trial conducted by Princeton- and Melbourne-based Opthea examined the potential of sozinibercept, a novel VEGF-C/D inhibitor, combined with aflibercept for treating diabetic macular edema (DME). This open-label, dose-escalation study evaluated the safety and preliminary efficacy of the therapy in people who had previously received anti-VEGF-A monotherapy (n=9). Key findings revealed that sozinibercept combination therapy was well-tolerated, with no dose-limiting toxicities. Higher doses demonstrated greater visual improvements, including a mean best-corrected visual acuity (BCVA) gain of +7.7 letters and a central subfield thickness (CST) reduction of −71 µm at 12 weeks. Additionally, 67% of patients achieved a ≥50% reduction in excess foveal thickness. These promising results underscore sozinibercept’s potential as a first-in-class VEGF-C/D trap, complementing anti-VEGF-A therapies to improve DME outcomes. While Opthea plans to advance the clinical development of sozinibercept in DME, the company says its immediate focus is preparing for the anticipated phase 3 topline data readout for sozinibercept in wet AMD with the COAST trial in early 2Q25 and the ShORe trial in mid-2025. |
| The Virtual DCCT: Adding Continuous Glucose Monitoring to a Landmark Clinical Trial for Prediction of Microvascular Complications | Dr. Boris Kovatchev (University of Virginia) et al. | DT&T | This interesting study added CGM metrics to the landmark Diabetes Control and Complications Trial (DCCT; n=1,441) to predict microvascular complications. Previously, the DCCT demonstrated that intensive insulin treatment reduces microvascular complications in T1D and showed that A1c levels predict rates of retinopathy, nephropathy, and neuropathy. The current study used a multistep machine-learning procedure to reproduce virtual CGM traces for the DCCT participants. The machine-learning procedure was trained across self-monitored blood glucose data and then sequentially added with CGM traces that filled in the gaps of the original data for each participant over 10 years of the study duration. The results showed that virtual CGM data computed similar TIR results from the DCCT, which indicated glycemic management differences between intensive and conventional groups. TIR was also associated with the risk of development or progression of retinopathy, nephropathy, and neuropathy (all p<0.0001). With these findings, the study authors encourage CGM metrics as an acceptable endpoint for clinical trials, especially as improvement in TIR and other CGM metrics demonstrates a reduction in chronic vascular complications. Looking ahead, we wonder how new technologies like machine learning could shape research and increase the range of applications, including clinical trials |
| Clinical Decision Support and Cardiometabolic Medication Adherence | Dr. Patrick J. O’Connor (HealthPartners Institute) et al. | JAMA Network | The trial (n=5,421) studied the effectiveness of an intervention using algorithmic identification of low medication adherence, clinical decisions to support HCPs, and pharmacist outreach to patients. At 12 months, participants in the intervention cohort had better adherence to blood pressure treatments (adjusted odds ratio: 1.29) but no improved adherence to statins (adjusted odds ratio: 1.18) or non-insulin diabetes treatments (adjusted odds ratio: 1.03), compared to participants with usual care. The intervention was greatest among those who were eligible for pharmacist outreach, with a 55% decrease in nonadherence to blood pressure treatments and a 43% decrease in statin nonadherence in the group. Results further showed that intervention did not improve A1c, systolic blood pressure, or LDL-cholesterol levels. Given these mixed results, the authors encourage future studies to consider a broader target or more intensive pharmacist outreach to improve treatment adherence. |
| Radon Exposure and Gestational Diabetes | Dr. Yijia Zhang (Columbia University) et al. | JAMA Network | This study explored the association between radon exposure, of all things, and gestational diabetes (GDM) among nulliparous pregnant women in the US - cool, that word refers to women who haven't given birth before! This national cohort study, using data from the nuMoM2b cohort, assessed over 9,100 participants, examining the potential link between county-level radon concentrations and GDM diagnosis. Key findings revealed that individuals residing in counties with higher radon levels (≥2 picocuries per liter) had 37% higher odds of developing GDM compared to those in counties with lower radon levels (<1 pCi/L). The association remained significant even after adjusting for particulate matter (PM2.5) exposure. Additionally, elevated odds of GDM were observed in “ever smokers” and participants in counties with both high radon and PM2.5 levels. Notably, environmental influences, including PM2.5 air pollutants and smoking, have been increasingly recognized alongside biological risk factors in their association with GDM. These findings reinforce the importance of addressing environmental risk factors, such as radon, in maternal health strategies and underscore the need for individual-level radon exposure assessments and further research to elucidate underlying biological mechanisms |
| Subcutaneous weekly semaglutide with automated insulin delivery in type 1 diabetes: a double-blind, randomized, crossover trial | Dr. Melissa-Rosina Pasqua (McGill University, Canada) et al. | Nature Medicine | Nature Medicine published results from a double-blind, randomized, crossover trial (n=28) assessing once-weekly semaglutide as an adjunct therapy to AID in adults with T1D. Participants were titrated up to 1 mg of semaglutide or placebo over 11 weeks, followed by 4 weeks of AID use. Compared to placebo, semaglutide increased participant’s Time in Range by 4.8% (74.2% semaglutide vs. 69.4% placebo, p=0.006) without increasing incidence of hypoglycemia. That is another hour plus per day! Additionally, semaglutide significantly reduced A1c levels, total daily insulin use, and body weight, with an average weight reduction of 5.3 kg compared to placebo (p<0.001), constituting a clinically meaningful 5.1% reduction in body weight from baseline. Those with the greatest weight reduction also tended to achieve the greatest glycemic improvements. Adverse events were generally mild and included gastrointestinal symptoms, though there were two episodes of euglycemic ketosis without acidosis in the semaglutide group. These findings suggest that semaglutide could be an effective adjunct therapy to AID for improving glycemic control and supporting weight loss in adults with type 1 diabetes … careful monitoring is necessary to mitigate risks, as always, especially related to related insulin dose adjustments. |
| Three-Year Follow-up After Antiviral Treatment in New-Onset Type 1 Diabetes: Results From the Diabetes Virus Detection and Intervention Trial | Dr. Ida Mynarek (Oslo University Hospital, Norway) et al. | Diabetes Care | The Diabetes Virus Detection and Intervention trial investigated the long-term effects of antiviral therapy (pleconaril and ribavirin) on preserving endogenous insulin production in children and adolescents newly diagnosed with type 1 diabetes (T1D). Professor Johnny Ludvigsson was among the authors. In this multicenter RCT (n=96), participants aged 6-16 years received either antiviral treatment or placebo for six months and were followed for three years. After one year, a statistically significant difference between groups was observed in C-peptide decline (p<0.05). However, this significance disappeared after two years of follow-up. At two years, the mean C-peptide area under the curve (AUC) was 0.34 ± 0.37 in the antiviral group versus 0.27 ± 0.33 in the placebo group. By three years, both groups experienced a decline in C-peptide AUC, reaching 0.25 ± 0.34 (antiviral) and 0.17 ± 0.23 (placebo). These findings suggest that the initial benefits of antiviral therapy on preserving C-peptide levels diminish over time, which the authors said warrants further research on antiviral strategies for preventing and treating T1D. |
| Financial Incentives, Income Supplementation, Cash Transfer, and Universal Basic Income Interventions in Diabetes: Understanding Differences and Effectiveness: A Scoping Review | Dr. Leonard Egede (University at Buffalo) et al. | Diabetes Care | A review published in Diabetes Care explores how monetary interventions — including financial incentives, income supplementation, and cash transfers — impact diabetes outcomes in adults with T2D. By examining 13 studies across these interventions, the review sheds light on the effectiveness of these approaches in improving key clinical and behavioral outcomes. Interventions showed statistically significant and clinically meaningful A1c improvements, ranging from: (i) 0.2% to 1.7% with financial incentives; (ii) 0.7% to 1.3% with income supplementation; and (iii) 0.2% to 0.7% with cash transfers. Important improvements were also observed in BMI, blood pressure, QoL (quality of life), and self-care behaviors in several studies. The most significant changes often resulted from multicomponent interventions, combining monetary support with education, telemonitoring, or skills training. This is great news - this is action that can be taken on! The review highlights the potential for targeted monetary interventions to enhance diabetes management, while emphasizing the need for future studies to explore the underlying mechanisms of change and to compare different approaches. |
| Genetic Predisposition to Low-Density Lipoprotein Cholesterol and Incident Type 2 Diabetes | Dr. Akshaya Ravi (Broad Institute of MIT and Harvard), et al. | JAMA Cardiology | JAMA Cardiology published a massive (n=361,082) prospective, population-based cohort study from Ms. Akshaya Ravi et al., investigating the relationship between genetic predisposition to LDL cholesterol and incident T2D. The study aimed to assess the relationship between genetic predisposition to elevated LDL levels and the magnitude of incident T2D risk. Study participants were part of the UK Biobank and underwent whole-exome sequencing and genome-wide genotyping. During the follow-up period (median: 13.7 years), 6.3% of participants (n=22,619) developed incident T2D, while 5.0% (n=17,966) developed incident coronary artery disease (CAD). Findings showed that the association between LDL polygenic risk score (PRS) and incident T2D was 0.72 for very high LDL PRS, 0.87 for high LDL PRS, 1.13 for low LDL PRS, and 1.26 for very low LDL PRS. This indicates an inverse relationship between genetic risk of elevated LDL and incident T2D, suggesting a potential metabolic link between the two conditions |
| Mapping the effectiveness and risks of GLP-1 receptor agonists | Dr. Yan Xie (St. Louis Health Care System) et al | Nature Medicine | The study identified comprehensive profile of the effectiveness and risks of GLP-1 RAs. The study used people with diabetes who used GLP-1 RAs (n=215,970) and compared them to those on sulfonylureas (n=159,465), DPP-4 inhibitors (n=117,989), or SGLT-2 inhibitors (n=258,614). The cohort of people with GLP-1 RAs was also compared to a control group of people on sulfonylureas, DPP-4 inhibitors, and SGLT-2 inhibitors (n=536,068), and a control group of people on usual care (i.e., non-GLP-1 RA antihyperglycemic treatments; n=1,203,097). The study mapped the associations of the use of GLP-1 RAs vs. each comparator with 175 health outcomes. Results showed that compared to usual care, the use of GLP-1 RAs was associated with a reduced risk of substance use and psychotic disorders, seizures, neurocognitive disorders (e.g., Alzheimer’s and dementia), coagulation disorders, cardiometabolic disorders, infectious diseases, and several respiratory conditions. The use of GLP-1 RAs was also associated with an increased risk of GI-related disorders, hypotension, syncope, arthritic disorders, nephrolithiasis, interstitial nephritis, and pancreatitis. Overall, these results reinforce the benefits and risks of GLP-1 RAs, which could help inform both patients and HCPs for effective clinical care. With several ongoing trials of GLP-1 RAs, we’re curious about the increasing efficacy of this impressive drug class beyond the management of glycemic levels and obesity. |
| Effectiveness of empagliflozin vs. dapagliflozin for kidney outcomes in type 2 diabetes | Dr. Kasper Bonnesen (Aarhus University Hospital, Denmark) et al | JAMA | Researchers conducted a trial emulation using Danish healthcare data from 2014 to 2020 to compare kidney outcomes in adults with T2D who initiated SGLT-2 inhibitors empagliflozin (n=32,819) vs. dapagliflozin (n=17,464). At baseline, study participants were 63 years old on average, 38% were female, and they had a median eGFR of 88 mL/min/1.73 m2. In a follow-up of up to six years after treatment initiation, empagliflozin and dapagliflozin conferred comparable kidney outcomes, including six-year risks of acute kidney injury (risk ratio (RR)=0.98), chronic kidney diseases (RR=9.97), and progression of CKD (RR=0.94). Ultimately, this study suggests that both empagliflozin and dapagliflozin have similar kidney outcomes and supports the current KDIGO guideline that does not indicate clinical preference for one drug. This is fortunate news for those who may have better access to one or the other therapies. We are also curious how other SGLT-2 inhibitors might compare, such as canagliflozin or generic versions. |
| Dapagliflozin plus calorie restriction for remission of type 2 diabetes: multicentre, double blind, randomised, placebo-controlled trial | Dr. Yuejun Liu (Fudan University, China) et al | BMJ | This randomized controlled trial enrolled 328 participants with T2D aged 20-70 years to assess the effect of calorie restriction with either dapagliflozin or placebo on T2D remission rates. 44% of participants (n=73) in the dapagliflozin group achieved remission compared to 28% (n=46) in the placebo group over 12 months (p=0.002). More substantial reductions in body weight and insulin resistance were observed in the dapagliflozin group alongside greater improvement in body fat, systolic blood pressure, and other metabolic risk factors. No significant differences in adverse events were observed. |
| EValuating Glucose ContrOL Using a Next-GeneraTION Automated Insulin Delivery Algorithm in Patients with Type 1 and Type 2 Diabetes: The EVOLUTION Study | Prof. Tom Wilkinson (University of Otago, New Zealand) et al. | DT&T | The EVOLUTION study evaluated the feasibility of Insulet’s next-generation fully closed-loop AID algorithm. Study results were originally presented at ATTD 2024 by Prof. Martin de Bock (University of Otago). The trial included a 14-day run-in period on usual therapy with Dexcom G6. Individuals with T1D then participated in 48 hours of monitored AID use in a hotel setting, followed by up to six weeks of outpatient use. Individuals with T2D did not participate in the hotel period. During outpatient use, participants were asked to manually bolus for three weeks, followed by a three-week period without manual boluses. Among participants with T1D who completed the outpatient portion of the study (n=9), mean Time in Range (TIR) increased by 4.8 hours/day during the no-bolus portion of the study compared to run-in from 37% to 58%. In the T2D population (n=8), mean TIR increased by three hours/day in fully closed-loop mode, from 52% at run-in to 65%. Improvements were attributed to significant decreases in Time above Range. Among participants with T1D, time in severe hyperglycemia (>250 mg/dL) dropped significantly from 34% at run-in to 9% and 14% with and without manual bolusing, respectively - how excellent. For participants with T2D, Time >250 mg/dL decreased from 21% at run-in to 8% with manual bolusing and 11% without. |
| Automated insulin delivery during the first 6 months postpartum (AiDAPT): a prespecified extension study | Dr. Tara Lee (Norwich Medical School, UK) et al. | Lancet Diabetes and Endocrinology | A prespecified extension to the AiDAPT study – results of which were originally presented at EASD 2023 – showed evidence for the efficacy of AID systems during the postpartum period. As a reminder, AiDAPT reported that participants on the CamAPS FX system spent an additional 2.5 hours/day Time in Range (TIR) compared to the standard care group during T1D pregnancy (68% vs. 56%). This extension followed a subset (n=57) of the individuals originally enrolled in AiDAPT (n=124), who continued either CamAPS FX or standard insulin therapy after delivery. In the first six months postpartum, mean TIR for the AID group was 72% versus 54% for the standard care group. Hyperglycemic metrics favored AID, with those on CamAPS FX achieving 14% less Time above Range. Time below Range was low in both groups over the six-month period: 2.4% and 2.6% for AID and standard care respectively. This extension study provides an excellent discussion of its motivations, noting that sudden postpartum lifestyle changes and the burden of caring for a newborn encourage a continuation of diabetes management used during pregnancy. Additionally, antenatal care typically features multiple weekly appointments, while only two to four appointments per year are standard for postpartum diabetes management in the UK, which this study mimicked. The authors concluded that continuous use of AID postpartum improves outcomes for people with diabetes after delivery and better addresses the postpartum gap in care. |
| Longitudinal Analysis of Obesity Drug Use and Public Awareness | Dr. Philipp Berning (1Johns Hopkins) et al. | JAMA Networks | A study just published in JAMA Network tracks the rapid rise in obesity management drug (OMD) prescriptions and their correlation with public search interest. This is a hyper-obvious “trend” in our view. Analyzing nearly 70 million dispensed prescriptions from 2017 to 2024, researchers found that monthly prescriptions doubled from 0.76 million in 2017 to 1.51 million in 2024, with semaglutide (Wegovy) and tirzepatide (Zepbound) driving the vast majority of this growth. Public awareness closely mirrors prescription trends, with strong correlations between online searches and prescription volumes for semaglutide (r = 0.97) and tirzepatide (r = 0.90). Meanwhile, phentermine (old school obesity therapy) prescriptions declined as newer GLP-1 RAs gained market share. Advanced practice practitioners (APPs) are increasingly prescribing these medications, with their share of prescriptions rising from 25.3% in 2017 to 40.6% in 2024. The findings underscore the real-time association between digital interest and therapy adoption, suggesting online search trends could serve as predictive tools for future supply and demand management in obesity treatment. While we are rather surprised about this piece, we imagine that JAMA Network has its share of GLP-1 inhibitor advertisements – harmless piece, but hardly meaningful. |
| Ophthalmic Complications Associated With the Antidiabetic Drugs Semaglutide and Tirzepatide | Dr. Bradley Katz (University of Utah Health) et al | JAMA Ophthalmology | This article described nine patients using either semaglutide or tirzepatide who were diagnosed with ophthalmic complications: seven with non-arteritic anterior ischemic optic neuropathy (loss of blood flow to optic nerve), one with papillitis (inflammation of optic nerve head), and one with paracentral acute middle maculopathy (an OCT presentation that may indicate vascular abnormalities). Atypical symptoms included progressive vision loss, bilateral disc swelling, and sequential ischemic optic neuropathy. The authors emphasized that a causal relationship between GLP-1 RA use and the observed ophthalmic complications could not be determined. However, they suggested that the rapid glucose-lowering effects induced by therapy, not drug toxicity, could be associated with these complications in some cases. |
--by Riya Chatterjee, Kayla Mathieu, Elizabeth Rose, Jeremy Alkire, Kat Moon, Esther Min, Monica Oxenreiter, and Kelly Close
[1]As background, MASLD is characterized by steatosis, or excessive fat accumulation in the liver, and is common in people with dyslipidemia, insulin resistance, obesity, or T2D. With further inflammation (e.g., lipid peroxidation, mitochondrial dysfunction, oxidative stress, and apoptosis), MASLD advances into MASH, where fibrosis – or scarring – begin to occur. Fibrosis has several stages: (i) F0 refers to no fibrosis; (ii) F1 refers to mild fibrosis; (iii) F2 refers to moderate yet clinically significant fibrosis; (iv) F3 refers to severe fibrosis; and (v) F4 refers to cirrhosis, characterized by advanced cell damage and scarring. Cirrhosis can be compensated or decompensated. People with compensated cirrhosis have minimal or mild symptoms, such as fatigue, nausea, and abdominal pain. In those with decompensated cirrhosis, however, the liver’s functions are heavilyd limited, and patients may experience jaundice and other complications.