ADCES Diabetes Technology Conference 2025 Day #2 Highlights –
Executive Highlights
- The Association of Diabetes Care and Education Specialists’ (ADCES) fifth annual Diabetes Technology Conference (DTC) concluded in the Windy City at the Chicago Marriott Downtown Magnificent Mile. Attendees were eager to trade the brisk cold (the high reached just 13°F) for warm conversation and insightful learning in the halls of the conference. Throughout the day, the conference organizers and speakers remarked on the impressive turnout from first-time attendees – brief show-of-hands made it appear that as many as three-quarters of those at an unopposed afternoon session were attending the conference for the first time. We applaud their commitment to learning more about the latest and greatest in diabetes technology and how to improve patient uptake of the devices back at home. Additionally, many thanks to the outstanding planning committee and the many speakers for yet another outstanding conference bringing the latest on diabetes technology implementation science to a cohort of leaders across the US – we can’t wait for ADCES DTC 2026 to see how the learning at this conference takes root.
- On CGM, Dr. Natalie Bellini (University Hospitals) and Dr. Diana Isaacs (Cleveland Clinic) discussed the role of CGM in T2D care. Dr. Isaacs highlighted CGM’s value at multiple stages of diabetes, including prediabetes, newly diagnosed T2D, and those with longstanding T2D on intensive insulin therapy. This included the growing adoption of over-the-counter CGMs (Abbott Lingo and Dexcom Stelo) in the non-insulin using T2D population, for which Dr. Bellini illustrated how it can still be a key driver of lifestyle-focused care. Dr. Bellini also stressed the importance of simplifying CGM data workflows by standardizing clinic codes and consolidating accounts across health systems.
- On AID, several speakers highlighted strategies to promote its adoption in vulnerable populations. Dr. Brynn Marks (Breakthrough T1D) delivered a comprehensive assessment of the structural, technological, and educational barriers that limit optimal AID use in youth with T1D, calling for change to coverage policies to improve wear time, more research on the use of concentrated insulins with AID, and better tackle inequities in adoption. Dr. Diana Isaacs (Cleveland Clinic) reviewed the current evidence around AID in pregnancy and provided actionable recommendations on the off-label use of systems and on their use with concentrated insulins during pregnancy. She also shared an exciting new initiative sponsored by the Helmsley Charitable Trust, T1DPregnancy&Me. Finally, Drs. Bellini and Isaacs strongly endorsed the broader use of AID in people with T2D, a position bolstered by major updates in the ADA Standards of Care.
- Dr. Anand Iyer (Welldoc) framed AI-enabled diabetes care as the “Google Maps” of chronic disease management, offering precise and adaptive guidance with minimal cognitive burden on patients and physicians. In the near term, AI can help health systems accomplish existing tasks more efficiently, such as identifying which patients are most likely to benefit from expensive therapies, like GLP-1 RAs, compared to those who may respond to lifestyle interventions alone. In the longer term, Dr. Iyer emphasized the opportunity to “swim upstream,” utilizing AI to transform diagnosis and prevention rather than reacting to downstream complications. In his view, “AI-in-the-loop” models will define the future, where CDCESs and clinicians who effectively leverage AI can extend their reach and impact.
- Ms. Teresa McArthur (Cecelia Health) explored strategies for remote device training and monitoring. Several positive trends with telemedicine have evolved from the COVID-19 pandemic, but challenges remain. At Ms. McArthur’s medical facility, clinicians still see 18% no-shows, demonstrating the importance of commitment and participation. Other challenges to the adoption of technology include the digital divide across age groups and socioeconomic factors, as well as stigma and provider comfort.
Table of Contents
-
Top Highlights
- 1. Dr. Brynn Marks overviews key barriers preventing AID use in pediatrics: From coverage to algorithms
- 2. Dr. Natalie Bellini and Dr. Diana Isaacs review the role of CGM across the T2D spectrum
- 3. Automated insulin delivery in T2D: An emerging standard of care
- 4. Dr. Anand Iyer positions AI as the “Google Maps” of diabetes care
- 5. Actionable advice for using AID in pregnancy from Dr. Diana Isaacs
- 6. Strategies for remote device training and monitoring: Ms. Teresa McArthur on helping achieve quality care for patients wherever they are
- 7. Drs. Anders Carlson and Kevin Malloy review clinical evidence and case studies for MannKind’s Afrezza (inhaled insulin)
- 8. Clinical considerations on preparing, administering, and monitoring Sanofi’s Tzield (teplizumab) for T1D
- 9. *NEW* Application of adult learning principles to technology education and training
Top Highlights
1. Dr. Brynn Marks overviews key barriers preventing AID use in pediatrics: From coverage to algorithms
Dr. Brynn Marks (Breakthrough T1D) delivered a comprehensive assessment of the structural, technological, and educational barriers that limit optimal AID use in youth with T1D. Drawing on real-world data and clinical experience, she highlighted how real-world sensor wear time, insurance coverage and supply constraints limit CGM wear time, how cartridge size and insulin concentration limit pump usability for patients with higher insulin needs, and why algorithm design and patient engagement should guide AID system selection. Dr. Marks also emphasized that AID benefits extend across glycemic and socioeconomic strata, underscoring both the promise of rapid technology initiation in underserved populations and the need for greater provider education.
- Dr. Marks argued that CGM wear time will not improve without changes to coverage policies. The current consensus, which defines adequate wear time as >70%, seems insufficient to her, particularly given Czech Registry datashowing a 0.6% A1c difference (6.8% vs. 7.4%) between those with >90% and 70-89% wear time. However, the duration of sensor wear and insurance coverage has important implications for CGM active time. In one real-world study of youth, adolescents, and young adults who used at least three Dexcom 10-day G7 sensors over a 3-month period, only 40% of sensors lasted ≥10 days. On average, children achieved ~8.6 days of wear per sensor, meaning that with current replacement policies, many cannot reach the 90% wear time she believes should be targeted. As coverage efforts advance, she emphasized the importance of working with manufacturers to help ensure access to sufficient supplies.
- Dr. Marks called for more research on the use of concentrated insulins with AID, which remains off-label.Small cartridge sizes are a major limitation for patients with high total daily insulin doses when supplies provided by insurance typically assume that each cartridge lasts three days,. Switching from U100 to U200 insulin can effectively double cartridge capacity. In a retrospective real-world analysis of ~50 adolescents and young adults (primarily Omnipod 5 users, with some t:slim X2 or Mobi users) with a total daily insulin dose of 103 units/day off-label U200 insulin use increased cartridge wear time increased from ~2.2 to 3.0 days per cartridge. TIR improved by 4% to 49%, with no significant increase in TBR. Looking ahead, she highlighted Arecor’s development of a U500 rapid-acting insulin and Sequel’s partnership in this space. Despite ongoing FDA concerns about concentrated insulins in AID systems, Dr. Marks sees promise for expanding patient choice and improving pump accessibility, including through micro-pump applications.
- Dr. Marks also emphasized the importance of selecting the right AID system for the right patient. Reviewing real-world data comparing Omnipod 5 and Control-IQ, Dr. Marks noted no significant differences in TIR during the first 90 days of use. However, there was a trend towards between group differences in those with <40% TIR before AID initiation. A recently published analysis found that among youth with low bolus frequency (~2.2 boluses/day), Control-IQ users spent 16% more time in automation, received approximately six automated boluses per day, and achieved an 8% higher TIR compared to Omnipod 5 users. These differences, she said, are important for families to consider when selecting an AID system, and she expressed interest in whether forthcoming Omnipod 5 algorithm updates may narrow this gap.
- Equity remains an important question with the use of AID in youth with diabetes. Dr. Marks emphasized that AID benefits are evident regardless of baseline glycemia or socioeconomic status. She highlighted a study of Control-IQ initiation in 15 non-Hispanic Black youth with A1c >10% (mean 11.7%) on public insurance, individuals considered “least likely” to access AID. Rapid CGM and AID initiation led to a >30% improvement in TIR (from 12% to 43%), driven largely by reductions in Level 2 hyperglycemia, alongside quality-of-life improvements for both children and caregivers. She also summarized Beta Bionics’ data presented at ATTD 2025, showing a GMI of 7.1–7.5% with iLet use, regardless of baseline HbA1d. However, she raised concerns about pediatric use, including the discontinuation of insulin delivery after 72 hours without CGM data, post-meal hypoglycemia in those not announcing meals and challenges with exercise in those doing sports requiring pump disconnection.
- The future of fully closed-loop systems appears promising. Dr. Marks reviewed findings from an AIDANET hotel and real-world study demonstrating non-inferiority of a fully closed-loop system compared to usual care (predominantly hybrid closed-loop AID), regardless of baseline glycemia.
- Dr. Marks highlighted persistent deficiencies in AID education among pediatric endocrinology fellows. In 2018, 85% of fellows and attendings reported no formal training on AID systems (n=111). By 2024, this had improved only modestly, with ~35% reporting formal training (n=106), despite near-universal agreement on the importance of such knowledge.
- Infusion set failure and ketone management remain significant weaknesses in diabetes technology. Among surveyed clinicians (n=123) at pediatric diabetes centers in the US, ~80% reported having a ketone management protocol, but Dr. Marks underscored wide variation in practice. Glucose thresholds prompting action most commonly exceeded 300 mg/dL (54%) but ranged from >200 to 350 mg/dL, while required duration of hyperglycemia ranged from immediate action to over six hours (most commonly over three hours, 30%). Only 30% reported having an AID-specific protocol for ketone management. With efforts underway in anticipation of continuous ketone monitoring, Dr. Marks referenced newly sharedBreakthrough T1D international expert recommendations on CKM and noted some concerns about pediatric applicability, as ketones can exceed 0.6 mmol/L in very young children even with normoglycemia.
2. Dr. Natalie Bellini and Dr. Diana Isaacs review the role of CGM across the T2D spectrum
Dr. Natalie Bellini (University Hospitals) and Dr. Diana Isaacs (Cleveland Clinic) presented a presentation prepared by Dr. Julia Blanchette (Case Western) on the role of CGM in T2D care. Framing much of the discussion around the 2026 ADA Standards of Care, Dr. Isaacs noted that while the A1c goal of <7.0% remains unchanged, expectations around technology use have evolved. Recommendation 7.15 now supports CGM initiation at diabetes diagnosis or any time, thereafter, including for individuals on non-insulin therapies associated with hypoglycemia (e.g., sulfonylureas) or on any treatment where CGM can aid management. Both speakers emphasized the critical role of CDCESs as “technology champions,” arguing that hands-on support can overcome many persistent barriers, especially in primary care settings.
- CGM benefits across the T2D spectrum. Dr. Isaacs highlighted CGM’s value at multiple stages of diabetes. For newly diagnosed individuals, CGM accelerates early learning and behavior change. For those with longstanding T2D, who by that point are often using insulin, CGM meaningfully reduces the risks of hypoglycemia. She referenced focus groups led by Dr. Blanchette that explored how CGM influenced behavior among people with prediabetes or newly diagnosed T2D. While lack of coverage emerged as the most common barrier, participants consistently described CGM as motivating, enabling better food choices and greater awareness of glucose patterns. Even those experiencing diabetes burnout reported that CGM functioned as a “personal coach,” keeping them accountable and acting almost as a supportive partner in care.
- For individuals on basal-bolus therapy, Dr. Isaacs encouraged the use of CGM data to facilitate more productive clinical conversations, helping to catch patterns such as missed prandial doses that often underlie poor outcomes. Beyond traditional prescription and OTC CGMs, Dr. Isaacs also spotlighted Eversense 365 as an alternative, sharing a case study in which it was particularly beneficial for someone with skin sensitivities to the adhesives in long-wear CGMs.
- CGMs are increasingly being used through OTC channels (with Abbott Lingo or Dexcom Stelo). Dr. Isaacs shared that she has seen patients present to the clinic wearing an OTC sensor. Reviewing a case study of a newly diagnosed woman with T2D who was not on insulin, Dr. Bellini illustrated how OTC CGM can still be a key driver of lifestyle-focused care, rather than therapeutic initiation or titration. She explained that Stelo also offers embedded education modules to support these efforts and features the opportunity to tighten glucose targets to TITR. It can also help inform the need to initiate additional medications when necessary. She suggested that early, assertive intervention directed by CGM may preserve beta-cell function and strengthen long-term engagement.
- Dr. Bellini also highlighted FDA clearance of Biolinq Shine in September, a skin-worn sensor that changes color in response to glucose levels, which generated audible enthusiasm from the audience.
- Reviewing the evidence base supporting CGM use in T2D, Dr. Bellini cited results from the MOBILE study in people with T2D using basal-only insulin, which demonstrated substantial improvements in TIR and reductions in TAR without the need for intensive education or medication optimization. She noted that these findings supported CMS’s decision to expand Medicare coverage for CGM in this population. CGM use has also been associated with reduced hospitalization risk, yet access gaps remain. In Ohio, for example, Dr. Bellini said approximately 50% of Medicaid beneficiaries with diabetes have not received CGM, despite coverage being available for both insulin- and non-insulin-treated individuals.
- Improving data integration and sharing. Dr. Bellini stressed the importance of simplifying CGM data workflows by standardizing clinic codes and consolidating accounts across health systems. At University Hospitals, she noted that CGM-related accounts were consolidated from 97 to a single system-wide account. She also noted the work done by industry on this front, specifically the elimination of a separate app for Dexcom G7, which further reduces friction. She encouraged other clinicians to create dedicated clinic accounts to eliminate the need for dozens of individual ones. Regarding OTC CGMs, she reminded attendees that Stelo integrates with Clarity for clinician review, but Lingo does not yet link to LibreView.
3. Automated insulin delivery in T2D: An emerging standard of care
Drs. Bellini and Isaacs strongly endorsed the broader use of AID in T2D, citing major updates in the ADA Standards of Care. AID is now the preferred insulin delivery method for adults with T2D (Level A), in addition to its established role in T1D. While evidence remains limited in pediatric T2D (Level E), Recommendation 7.25b suggests considering AID for people with T2D on basal insulin, opening the door to earlier initiation. Dr. Bellini challenged the traditional stepwise progression from MDI to pumps, arguing that earlier adoption of AID could reduce treatment burden and simplify the transition to mealtime insulin. She also noted the expansion of pump coverage and recent policy shifts, including the removal of C-peptide and autoimmune testing requirements in the 2026 Standards of Care, although Medicare coverage has yet to fully align.
- Regulatory momentum and clinical trial evidence. Recent FDA clearances of Control-IQ+, MiniMed 780G, and Omnipod 5 for T2D have solidified the benefits of these systems for T2D after long periods of off-label use, which both projected would raise provider confidence, particularly among PCPs. The speakers reviewed the pivotal trials supporting these approvals:
- Tandem 2IQP: Control-IQ+ produced a 0.9% A1c reduction over 13 weeks, with TIR increasing by 24% (40% to 64%).
- Insulet SECURE-T2D: Omnipod 5 led to a 0.8% A1c reduction and a 20% TIR improvement, with notable participant diversity and high engagement in meal estimation and custom foods.
- Medtronic IMPACT T2D: A1c declined by 0.7% to 7.2%, while TIR reached 81% without severe hypoglycemia or DKA. As users increasingly relied on automation, total daily insulin dose rose while carbohydrate intake and user-initiated boluses declined.
- Technologies for T2D beyond AID. Dr. Isaacs reviewed additional options for T2D, including simpler patch pumps (like CeQur Simplicity and V-Go), connected pens, and inhaled insulin. She emphasized that carbohydrate awareness remains essential across all technologies, not solely AID. Several case studies reinforced the importance of iterative AID optimization (with Control-IQ+), consistent pre-bolusing (with Omnipod 5), and use of optimized targets, particularly with MiniMed 780G.
- Dr. Bellini emphasized that CDCESs hold an important responsibility to offer meaningful patient choice. Dr. Isaacs concluded that with 51% of people with diabetes still above A1c targets, the limiting factor is no longer the availability of tools but rather ensuring patients are supported in using them effectively.
4. Dr. Anand Iyer positions AI as the “Google Maps” of diabetes care
Dr. Anand Iyer (Welldoc) framed AI-enabled diabetes care as the “Google Maps” of chronic disease management, offering precise and adaptive guidance with minimal cognitive burden on patients and physicians. Reviewing patient needs, Dr. Iyer emphasized that physicians are no longer just asking for device connectivity, but for tools that offer predictive insight: when a condition may emerge, how severe it could become, and how long it might last. Even better is when this guidance comes in the form of ambient and passive technologies, as Dr. Iyer suggested, “If I don’t have to worry about it right now, let it happen.” He noted growing comfort with AI among both patients and clinicians, particularly when it delivers concrete answers to practical questions, such as what type of exercise to do, for how long, and how often. However, Dr. Iyer also emphasized that clinicians cannot be asked to do more than they already do, pointing to the reality that every hour of telemedicine for a chronic care patient can result in two hours of EMR documentation, concluding that AI must be designed with clinical efficiency in mind as well.
- AI’s value proposition in diabetes relies on efficiency gains today and new capabilities tomorrow. In the near term, AI can help health systems accomplish existing tasks more efficiently, such as identifying which patients are most likely to benefit from expensive therapies, like GLP-1 RAs, compared to those who may respond to lifestyle interventions alone. In the longer term, Dr. Iyer emphasized the opportunity to “swim upstream,” utilizing AI to transform diagnosis and prevention rather than reacting to downstream complications. This is especially important, given that roughly 72% of healthcare costs stem from acute utilization by those he referred to as “frequent flyers.”
- Dr. Iyer outlined how different AI approaches — rules-based systems, machine learning, deep learning, and generative AI — can be combined to create adaptive and trusted clinical tools. While regulators have historically favored rules-based AI for its traceability, he argued that diabetes is a dynamic disease that demands models be able to learn and evolve over time. He believes that hybrid models, which blend these approaches, will demonstrate superior performance. Dr. Iyer also pointed to the FDA’s latest PCCP (Predetermined Change Control Plan) guidance (issued in August 2025) for AI-enabled device software as a positive. The guidance, as expected, requires transparency regarding model training, data cleaning, bias mitigation, and safeguards. However, it also allows for iterative innovation without requiring repeated regulatory submissions.
- Successful AI strategies depend on diverse data streams and strong governance. Dr. Iyer described the hierarchical data structure that is commonly used, which integrates user-generated health data, data interpretation, and other clinical inputs to help uncover “hidden” patient behaviors. For example, early user engagement with Welldoc (making 10+ annotations in the first 30 days) correlates with longer app retention and improved A1c outcomes.
- Ultimately, Dr. Iyer positioned AI as a tool rather than a replacement for diabetes care teams. In his view, “AI-in-the-loop” models will define the future, where CDCESs and clinicians who effectively leverage AI can extend their reach and impact. Drawing an analogy to the Webb Space Telescope, he suggested that AI is a tool that helps clinicians detect patterns that would otherwise remain distant lights, enabling a future in which digital health, CGM, AI, pharma, and providers operate within a shared, scalable infrastructure. This future may be nearer than one believes, he concluded, predicting demonstrated and scalable success of CMS’s “Health Tech Ecosystem Initiative” by July 4, 2026.
5. Actionable advice for using AID in pregnancy from Dr. Diana Isaacs
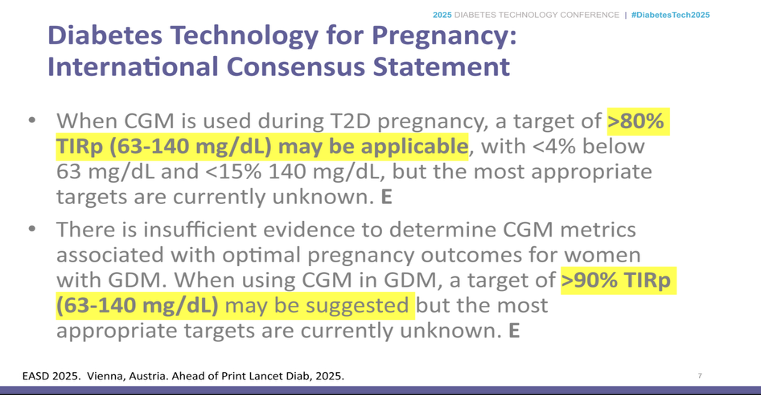
In a Saturday morning session, Dr. Diana Isaacs (Cleveland Clinic) reviewed the current evidence around AID in pregnancy, provided actionable recommendations, and shared an exciting new initiative sponsored by the Helmsley Charitable Trust. Dr. Isaacs highlighted a critical gap in the evidence base, noting that while most studies around AID in pregnancy were for those with prediagnosed T1D, most pregnant people with diabetes actually have gestational diabetes. Additionally, she noted that more people are also presenting with insulin-requiring T2D at the time of pregnancy. Given these gaps, Dr. Isaacs noted that the recent consensus statement from EASD 2025 around glycemic targets in pregnancy, which recommended >80% TIR for pregnant women with T2D and >90% TIR for pregnant women with gestational diabetes, with the explicit disclaimer that “appropriate targets are currently known.”
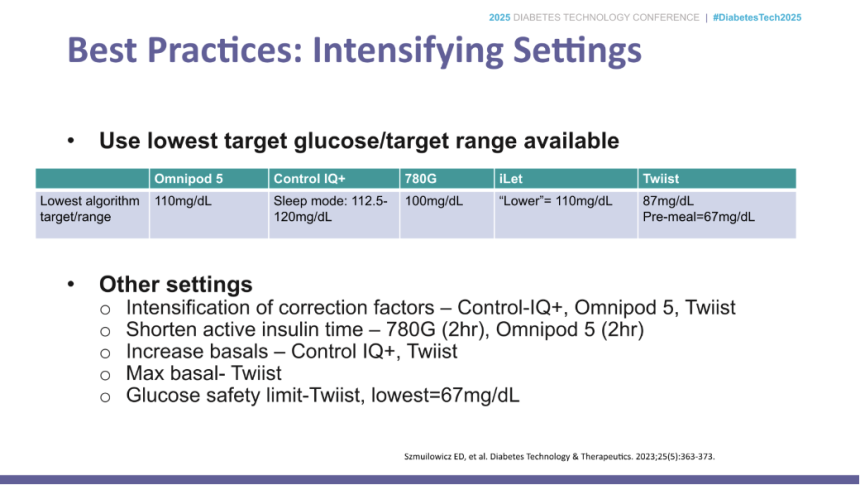
- In the US, CamAPS FX, the only officially cleared system available for pregnancy, is not yet available due to the lack of compatible insulin pumps. As a result, pregnant women often use the available commercial systems off-label. As highlighted during the “AID speed dating” session on Day #1 of DTC, these systems all have slightly different available settings and terminology, which providers and patients have to navigate. For example, the most aggressive setting for Tandem Control-IQ is termed “Sleep Mode,” whereas other systems, such as the MiniMed 780G and Omnipod 5, rely on set glucose targets and active insulin time to tune their aggressiveness.
- Dr. Isaacs also covered recommendations for another off-label use of AID systems in pregnancy, concentrated insulins. As insulin needs increase during pregnancy, Dr. Isaacs noted that many of her patients transition to concentrated insulin to increase the effective capacity of their pumps. With U200, the insulin kinetics are generally similar to U100, and pump settings can be adjusted in a straightforward manner (i.e., doubling I:C ratio and ISF, halving basal rate). However, the kinetics of U500 can be quite different and should often be used with a longer active insulin time.
- While clinical trials for AID in pregnancy show strong advantages to using these systems, Dr. Isaacs noted that none of these achieved the target TIR, demonstrating the difficulty of managing diabetes in pregnancy. In the AiDAPT studywith the CamAPS FX system, mean TIR with AID was 68%; with MiniMed 780G in CRISTAL, mean TIR was 67%; and with Tandem Control-IQ in the CIRCUIT study, mean TIR was 65%. Given the immense challenge of glycemic control during pregnancy, Dr. Isaacs encouraged providers to be patient with both themselves and their patients, and to appreciate the difficulty of diabetes management.
- Finally, Dr. Isaacs highlighted an exciting new initiative sponsored by the Helmsley Charitable Trust, T1DPregnancy&Me. The study is currently enrolling and aims to collect data from over 500 pregnant women with T1D across 10 study centers. Patients will be able to upload glycemic and psychosocial outcomes data remotely with TIR and neonatal and maternal outcomes as endpoints. The study is seeking both subjects and collaborators and is being conducted by the Jaeb Center. Dr. Isaacs encouraged those in the room with an interest to get involved.
6. Strategies for remote device training and monitoring: Ms. Teresa McArthur on helping achieve quality care for patients wherever they are
Reflecting on the post-COVID-19 pandemic era, Ms. Teresa McArthur (Cecelia Health) explored strategies for remote device training and monitoring. Ms. McArthur encouraged the audience to revisit their memories from before the pandemic, when many were unfamiliar with telehealth or virtual training. In fact, only around 10 attendees in a full breakout room raised their hands when asked how many used virtual options before the pandemic broke out. Ms. McArthur shared challenges with transitioning from audio to virtual video training, as it was initially conducted in a one-way approach, with patients only having the option to view demonstrations from clinicians. This policy arose from concerns about liability issues, making it difficult to determine whether patients were administering treatment properly. The field has since made significant advancements in technology.
- While the post-COVID-19 pandemic has opened a new chapter in diabetes technology adoption, challenges remain. Several trends have evolved from COVID-19, including: (i) better understanding of telehealth and the willingness among patients to participate; (ii) improved readiness across internet access and technology literacy; (iii) more options for virtual device training; (iv) improved virtual care infrastructure; (v) considerations for coverage; and (vii) “forced” provider awareness and comfort. Ms. McArthur clarified that she raised the last point not as a negative concept, but to emphasize how COVID-19 prompted clinicians to adopt a new approach to remote teaching, support, and education. It encouraged providers to develop new approaches in healthcare, and there has been more comfort than in previous times.
- However, telehealth and virtual approaches are not perfect even after many years of implementation, with clinicians and patients still navigating barriers. At Ms. McArthur’s medical facility, clinicians still see 18% no-shows, demonstrating the importance of commitment and participation. Other challenges to the adoption of technology include the digital divide across age groups and socioeconomic factors, as well as stigma and provider comfort.
- Important approaches across device training and monitoring. Ms. McArthur distinguished technology training from monitoring, saying they belong to different buckets of diabetes care. When training patients, clinicians should focus on building their confidence and enhancing their experience to promote the adoption of devices. Clinicians should also determine the current regimen and prior experiences, set clear expectations, understand what “training” means for each person, and prepare ahead of time before appointments. A successful outcome might look like one that promotes ongoing confidence for monitoring.
- Ms. McArthur then transitioned to device monitoring, which aims to support long-term use, help interpret data, and, most importantly, impact behavior change. Device monitoring should also include assessment of patients’ comfort in sharing data and their autonomy in device utilization. At times, patients may benefit from phased approaches and family participation to further enhance their comfort.
- Successful use of diabetes devices requires personalization for each patient. Ms. McArthur shared a study that provided virtual support in pediatric diabetes care. The study offered tablets to assist connectivity among families in rural areas lacking access and identified and addressed major barriers to care along the way. Ms. McArthur cited another study that evaluated the remote support model for older adults using insulin and CGM. Individual virtual sessions helped address age-specific barriers (e.g., technology literacy and caregiver needs). With longer, repetitive sessions involving caregivers, patients demonstrated improved adoption and sustained use of technology. Furthermore, the study demonstrated the feasibility of remote training and education on the use of CGM, particularly through the reduction in hypoglycemia risk. Reflecting on both studies, Ms. McArthur emphasized that individualized approaches to addressing barriers help facilitate device training and monitoring across different age groups. She also listed other strategies (see below) to help clinicians adapt to their patients by personalizing care across each life stage.
7. Drs. Anders Carlson and Kevin Malloy review clinical evidence and case studies for MannKind’s Afrezza (inhaled insulin)
MannKind-sponsored presentation kicked things off early on Saturday morning with Dr. Anders Carlson (International Diabetes Center) and Dr. Kevin Malloy (Cleveland Clinic) reviewing some of the history, clinical data, and case studies around MannKind’s Afrezza (inhaled insulin).
- As a pharmacist, Dr. Malloy discussed some details of inhaled insulin, particularly emphasizing its differences from subcutaneous insulin. To start, inhaled insulin has a faster onset time, around 12 minutes, compared to the 16-20 minutes seen in the fastest subcutaneous insulins. Additionally, the peak effect of inhaled insulin occurs about twice as quickly as ultra-rapid subcutaneous insulin, around 45 minutes for inhaled insulin, compared to 90-130 minutes for subcutaneous insulin. Finally, the duration of the effect of inhaled insulin is much shorter than that of subcutaneous insulin, at 180 minutes compared to 300-420 minutes. Due to these faster time frames, Dr. Malloy shared an important educational point for users of inhaled insulin: if glucose levels are high, it is safe to give a follow-up bolus after just an hour of the previous dose, something that would not be appropriate when using subcutaneous insulin.
- Dr. Carlson walked through clinical evidence around inhaled insulin and previewed a few new studies. In particular, Dr. Carlson noted that in the INHALE-3 trial for inhaled insulin, the greatest benefits to A1c and psychosocial outcomes were observed in those with worse baseline values. On the forward-looking side, the INHALE-1 study was presented at ISPAD 2025 to support the use of inhaled insulin in pediatrics, while INHALE-GDM is currently enrolling to support the use of inhaled insulin for people with gestational diabetes.
- Dr. Malloy concluded the session with a case study that highlighted an excellent use case for inhaled insulin.This case study involved a 21-year-old with T1D who played college rugby. The patient had switched to an AID system in 2022, which helped reduce his glycemic levels. However, wearing a pump was not feasible during the rugby season, which lasted from five to six months of the year. As a result, the patient switched over to using Afrezza. The faster onset of Afrezza made it easier to deliver pre-meal boluses, and since the patient was already motivated and engaged in his care, he was comfortable with the more frequent dosing required by Afrezza.
8. Clinical considerations on preparing, administering, and monitoring Sanofi’s Tzield (teplizumab) for T1D
In an afternoon Sanofi-sponsored session, Dr. Natalie Bellini (University Hospital) spoke on clinical considerations for Sanofi’s Tzield (teplizumab), the first and only treatment approved for delaying the onset of stage 3 T1D. Dr. Bellini started the presentation with a sobering statistic that someone is diagnosed with T1D every 10 minutes, saying, “Every 10 minutes is someone’s 10 minutes.” When Dr. Bellini was diagnosed with T1D, people either had a formal diagnosis of T1D or did not. The field evolved in 2015, when the ADA, along with several other diabetes organizations, published an official classification and staging approach for presymptomatic T1D. While this staging process was informative, it wasn’t until the development of Tzield and its approval in November 2022 that screening became markedly more important for detecting T1D prior to the appearance of symptoms external insulin dependency.
- Preparation before Tzield administration. Dr. Bellini explained that before administering Tzield, clinicians should confirm the its appropriateness for patients by documenting T1D-related autoantibodies and identifying dysglycemia. Patient experiences reported across clinical trials have demonstrated difficulties with oral glucose tolerance tests, and therefore, Dr. Bellini recommends avoiding them and using CGMs, unless insurance companies request them. Additionally, clinicians should conduct initial blood work to determine blood count, liver enzymes, and possible infections. Clinicians should also help administer live-attenuated vaccines ≥8 weeks prior to Tzield administration and administer inactivated vaccines ≥2 weeks prior, as these approaches help increase the efficacy of Tzield.
- Administration of Tzield. Dr. Bellini overviewed the 14-day protocol of Tzield, which is infused over a minimum of 30 minutes using dosing based on patients’ body weight. During the infusion process, patients should be closely monitored for liver enzymes (e.g., ALT, AST, bilirubin), vital signs, and side reactions, with the most serious adverse reactions including: (i) cytokine release syndrome; (ii) lymphopenia; (iii) infection; and (iv) hypersensitivity reactions.
- Monitoring with CGMs. Patients administered with Tzield should be continually monitored for progression from stage 2 to stage 3 T1D. In June 2024, an official guidance was published on monitoring for both children and adults, including the recommendation to use CGMs. For individuals under the age of 17 years, the guidance recommends a follow-up frequency of every three months. For adults, it recommends follow-ups every six months until progression occurs, which Dr. Bellini expressed disagreement with, as it represents an excessively long follow-up period. In her clinic, she provides patients with an educator who can touch base and understand the patient’s experience.
- During a period of monitoring, Dr. Bellini strongly encouraged clinicians, “It’s our time to shine.” Clinicians should help educate patients about balanced diets and lifestyles, along with providing them with appropriate services, before their beta cell function declines and glucose levels rise. Dr. Bellini said, “It’s not just one-and-done.”
- Testaments to Tzield’s efficacy. Dr. Bellini was joined by Michelle, a mother whose eight-year-old daughter, Emily, was diagnosed with stage 2 T1D in July 2024. Michelle recounted the confusion she first felt with Emily’s diagnosis, given neither her nor her husband’s family has a history of T1D. When the endocrinologist informed that Emily would be insulin dependent in the next six months but shared the hope Tzield could offer, Michelle said it was a “race against time” to understand more about T1D, the treatment and its side effects, and the next steps. Yet, with the help of caregivers, especially through Sanofi’s mentorship program, Michelle and her husband sought information and support through treatment infusion and monitoring with CGM. Michelle’s enthusiasm spread across the room as she shared that Emily has not progressed to T1D. She acknowledged that, indeed, no two experiences are the same. Still, as Dr. Bellini continually reminded throughout the presentation, screening remains a priority of utmost importance to facilitate early detection and intervention, alleviating the burdens prevalent in T1D.
9. *NEW* Application of adult learning principles to technology education and training
Ms. Becky Sulik (Rocky Mountain Diabetes Center) presented on ways to apply adult learning principles to technology education and training. Specifically, Ms. Sulik first described the differences between adult learners and children and adolescents, and then shared approaches to apply learning principles to diabetes technology training, support, and problem-solving. She ended the session by emphasizing the importance of identifying individual learning styles and sharing tools to help tailor learning and training that accommodates such differences.
- Differences in learning among adults, compared to children and adolescents. Building on Piaget’s long-standing theory, which outlines the four cognitive stages of learning, studies have proposed a potential “post-formal stage” among adults who possess multiple perspectives and develop principles through logic, experiences, emotions, and various contexts. Compared to children and adolescents, adults incorporate life experiences and opinions into their learning and may exhibit greater motivation to learn. Given these traits, Ms. Sulik offered applications in diabetes technology training that aligned with each adult learning principle.
- Relevance. Ms. Sulik emphasized the importance of helping patients understand the “why” for diabetes technology, positioning this interaction as the framework for training. She suggested using stories or cases to allow patients to better understand the applications and significance of such interventions.
- Motivation. Ms. Sulik encouraged clinicians to ask, “What are the appropriate goals?” While case studies that present remarkable improvements in A1c levels and TIR represent promising outcomes, Ms. Sulik said that focusing solely on ideal outcomes may stray from achieving realistic goals. Clinicians should help patients achieve targets that fit into their daily routine and respect the degree of improvement they achieve.
- Self-concept/autonomy. Ms. Sulik mentioned that clinicians should seek to understand patients’ preferred learning styles and match educational resources that are suitable for them. She further elaborated on this point later in her presentation by explaining tools to enhance individual learning approaches.
- Experience. Ms. Sulik highlighted the importance of understanding patients' journeys with diabetes and their use of technology, including past experiences that have been frustrating or others that were considered successes. Training steps should be built around these contexts.
- Readiness. Ms. Sulik said patients may need several visits to understand the purpose and receive resources that will position them for success and confidence.
- Orientation. Ms. Sulik suggested that clinicians structure training around tasks with repetition and critical reminders. In turn, repetition also helps educators evaluate the learning style.
- Variations in learning styles and the use of appropriate tools to accommodate preferences. Matching education resources to learning preferences will enhance engagement, understanding, and confidence among patients using diabetes technology. Ms. Sulik therefore reflected on each learning style and provided examples of applications in diabetes education: (i) colorful diagrams or flow charts for visual learners; (ii) stories, videos, or recordings that discuss steps for auditory learners; (iii) checklists or guidance on notes for reading/writing learners; and (iv) “hands-on” experiences, simulators, or practice sessions (e.g., infusion set, sensor, taping methods) for kinesthetic learners. On the latter point, Ms. Sulik highly encouraged manufacturers to provide clinics with more practice sets and simulators to help patients practice and feel more confident with their diabetes management.
- We were very impressed with this session, and we were grateful that Ms. Sulik could bring graduate school learnings to the diabetes ecosystem. For example, in her master’s program, Ms. Sulik took a course in which she learned a multitude of learning principles and their applications to diabetes management. She expressed gratitude for having the opportunity to receive such training and hopes to share the core principles further to advance technology implementation, as “teaching is as much of an art as it is a science.”
-- by Jeremy Alkire, Esther Min, Albert Cai, and Kelly Close