JPM 2026 Full Report –
Executive Highlights
- The 44th Annual JP Morgan (JPM) Healthcare Conference wrapped earlier this month at the Westin St. Francis Hotel in San Francisco. This year, the meeting convened 525 companies and over 9,000 attendees across the healthcare industry, from large pharmaceutical and device companies to early clinical-stage biotech firms and non-profit organizations. We appreciate JPM for organizing dynamic conversations on innovation, market changes, and health policy.
- Diabetes, obesity, and cardiometabolic disease remained dominant themes throughout the conference,reflecting the continued importance of these conditions in both clinical innovation and commercial focus. Across presentations, speakers discussed therapeutic efficacy alongside maintenance and long-term clinical outcomes. GLP-1 RAs and other next-generation incretin-based therapies were featured prominently, with expanding discussion around combination therapy approaches and differentiation between incretins beyond degree of weight reduction.
- Technology and data infrastructure were discussed as critical factors of scaling, with a strong focus on CGM, AID systems, digital health platforms, and real-world data integration. Speakers highlighted the importance of interoperability and clinician workflow integration as patient adoption expands toward broader populations. Specifically, the opportunity to deeper penetrate US and international markets through coverage expansions and strengthened guidelines for both CGM and AID was a focus of conversation as companies explored how to bring their products to more patients.
- Beyond company updates, the conference hosted several fireside chats with leaders across the ecosystem to explore the present and future of the US’ healthcare ecosystem. JPMorgan CEO Mr. Jamie Dimon led the first of this series, touching on a variety of topics including his perspective on global affairs and the role of corporations and healthcare organizations in this ecosystem. Several administrators from CMS – including Dr. Mehmet Oz (CMS Administrator), Mr. Daniel Brillman (Deputy Administrator and Director), Ms. Stephanie Carlton (Deputy Administrator & Chief of Staff), Mr. Chris Klomp (Deputy Administrator & Director), and Ms. Amy Gleason (Strategic Advisor) – later joined to discuss their approaches to improving long-term US health, and US Commissioner of Food and Drugs Dr. Marty Makary gave a talk on multiple initiatives at the FDA and innovation within the context of population-level health outcomes.
- See our top highlights below across pipeline innovation in diabetes therapy and technology, clinical trial advancements, US public health policy, AI’s role in healthcare, and the economic and geopolitical climate. For a look at our on-the-ground view of the conference, see our Day #1, Day #2, Day #3, and Day #4 coverage, as well as our Resource Hub.
Table of Contents
-
Diabetes Therapy Highlights
- AbbVie: Interest in entering obesity arena by leveraging familiarity with cash-pay channel and compounding market
- Amgen: PCSK-9 inhibitor Repatha highlighted as key to Amgen’s growth through 2030; extensive discussion of long-acting T2D and obesity candidate MariTide
- Amphastar: Dr. Jack Zhang shares updates on glucagon, GLP‑1 RAs, and insulin biosimilars
- Arrowhead Pharmaceuticals: RNA interference treatments for obesity to advance to phase 2b trial
- AstraZeneca: Cardiometabolic focus for 2030 and beyond led by aldosterone synthase inhibitor baxdrostat, PCSK-9 laroprovstat, and GLP-1 RAs in development
- Bayer: Kerendia (finerenone) demonstrates blockbuster potential for CKD and heart failure; pricing pressures with Eylea (aflibercept)
- Biocon: Addressing global non-communicable diseases like diabetes; generics and biosimilar business restructuring
- Biomea Fusion: Phase 2 data for Icovamenib and phase 1 results of GLP-1 RA BMF-650 expected in 2026
- Corcept Therapeutics: Dr. Joseph Belanoff highlights broad implications of cortisol modulation, including hypercortisolism, obesity, and diabetes
- Esperion: Updated US lipid-lowering guidelines to include bempedoic acid offering; international expansions; combination therapy
- Ionis Pharmaceuticals: Tryngolza gains traction in treatment of FCS ahead of broader launch; pelacarsen for Lp(a) risk reduction on track for launch in 2027
- J&J: CEO Mr. Joaquin Duato outlines diversified growth strategy with momentum in cardiovascular portfolio
- Kailera Therapeutics: CEO Mr. Ron Renaud highlights diversified GLP-1 RA pipeline for obesity treatment
- Lexicon Pharmaceuticals: Dr. Mike Exton highlights SGLT-1/2 inhibitor sotagliflozin, pilavapadin for DPN, and non-incretin obesity candidate
- Lilly: Mr. David Ricks shares insights about obesity market, payment channels, and clinical pipeline including orforglipron
- Madrigal: “10% of 10%” of global MASH patients treated; detailed approaches to combination therapy including GLP-1 RAs and DGAT-2 inhibitors
- Merck: “Democratizing” PCSK9 therapy and combinations with Lp(a); MK 3000 as a potential new mechanism of action for diabetic macular edema
- Novartis: De-risked pipeline driving post-Entresto growth; Leqvio as the foundational therapy for the company’s cardiorenal metabolic franchise
- Novo Nordisk: Mr. Mike Doustdar on mastering cash channel, reframing perception of the semaglutide, and clinical pipeline with CagriSema, cagrilintide, and amycretin
- Pfizer: Dr. Albert Bourla shares vision of obesity treatment landscape with Metsera’s assets and reflects on MFN and tariffs
- Regeneron: CEO Dr. Leonard Schleifer and CSO Dr. George Yancopoulos emphasize internal R&D engine, Eylea HD momentum, and obesity strategy
- Roche: Targeting a “top three” role in obesity through petrelintide, pegozafermin, and more; anti-VEGF Vabysmo returns to growth after market challenges
- Sana Biotechnology: Continuing strides for allogeneic islet cell therapy with developed with hypoimmune technology in people with T1D
- SAB Bio: Mr. Samuel Reich on differentiating features of SAB-142 as a disease modifying therapy for T1D
- Sanofi: Strategies and progress across mid- to late-stage development projects; teplizumab receives approval in the EU for stage 2 T1D
- Vertex: Journavx (suzetrigine) shows strong growth in the pain sector with potential indication for diabetic peripheral neuropathy
- Viking: Dr. Brian Lian highlights oral and injectable VK2735 (dual GLP-1/GIP RA) and amylin agonist for obesity
- Zealand Pharma: Dr. Adam Steensberg highlights survodutide and petrelintide; clinical data expected in 2026
-
Diabetes Technology Highlights
- Dexcom: Preliminary full-year 2025 revenue of $4.66 billion (+16%) and 4Q25 revenue of $1.26 billion (+13%); global userbase grows over 25% to 3.5 million
- embecta: GLP-1 RAs offer >$100 million annual opportunity; “market-appropriate” products for China and other geographies
- Insulet: President and CEO Ms. Ashley McEvoy highlights growth opportunity across US T1D, US T2D, and OUS T1D; robust innovation pipeline through 2028
- Medtronic: With Diabetes business spinoff expected by the end of 2026, management highlights four new generational growth platforms
- Omada Health: Preliminary full-year 2025 revenue of ~$257 million (+52%); 2026 will see investment in GLP-1 RA Care Track and AI tools
- Teva Pharmaceuticals: Teva to shift from generics firm to global biopharmaceutical company
- Verily: Progress on Verily Pre for clinical research facilitation and Verily Me for telehealth
- Virta Health: Tailwinds from GLP-1 RAs; combining the platform with pharmacotherapy for sustained weight loss and metabolic benefit
- Ypsomed: CFO Mr. Samuel Künzli reviews product launches and global manufacturing expansion in 2025; one billion unit manufacturing capacity targeted for 2030
- JPM’s Jeremy Meilman welcomes over 9,000 attendees, reflecting on four decades of global health industry
- San Francisco Mayor Mr. Daniel Lurie welcomes business, scientific, and medical leaders to San Francisco
- Fireside Chat Fascinates: JPMorgan Chase CEO Mr. Jamie Dimon in conversation with Ms. Terry-Ann Burrell on geopolitics, the free market, leadership suggestions, and healthcare innovation
- *NEW* Mass General Brigham: Systemwide transformation and strategic expansion
- *NEW* Cleveland Clinic: Applying AI and delivering complex care at a global scale
- *NEW* Mayo Clinic: Embedding AI across care, research, and operations
- *NEW* Intermountain Health: AI and proactive care across the American West
- CMS comes to SF: Dr. Mehmet Oz and CMS leadership discuss GLP-1 RAs, long-term health, MFN, and MAHA
- The FDA’s Dr. Marty Makary on optimized regulation, accelerating the 12-year approval timeline, and additives in our food supply
- From agentic AI to longevity: ARPA-H’s strategy for breakthrough health innovation
- Employer coverage at crossroads: Managing GLP-1 RAs and breakthrough therapies
- Technology and strategy to capture Asia’s growing patient markets
- The growing strength of Chinese biotechnology: Gaining trust and partnership
Diabetes Therapy Highlights
AbbVie: Interest in entering obesity arena by leveraging familiarity with cash-pay channel and compounding market
In this morning session, CEO Mr. Robert Michael shared updates on AbbVie. As background, AbbVie is a global pharmaceutical company with a market cap of $390 billion. Its focus areas span immunology, oncology, neuroscience, ophthalmology, aesthetics, and infectious diseases. Blockbuster drugs include autoimmune disease medications Humira (adalimumab) –which is now facing loss-of-exclusivity – IL-23 inhibitor Skyrizi (risankizumab-rzaa), and JAK inhibitor Rinvoq (upadacitinib). Botox (onabotuliumtoxinA) used for cosmetic purposes is also a multi-billion-dollar product made by AbbVie.
- AbbVie expresses interest in entering the obesity arena. In March 2025, AbbVie entered a partnership with Gubra to develop and commercialize a long-acting amylin analog, GUB014295, for obesity. Mr. Michael said that amylin agonist class is promising due to its favorable tolerability profile. AbbVie will continue to expand its obesity portfolio beyond GUB014295 through business development and licensing strategy and plans to differentiate its portfolio with improved tolerability and durability of weight loss. Moreover, Mr. Michael believes that AbbVie is well-positioned especially given its familiarity with the cash-pay channel and compounding market. Notably, the compounding business had become the second largest segment in the aesthetics market “over a matter of a few quarters.”
- As a reminder, the candidate conferred dose-dependent weight loss up to 3% at six weeks, compared to 1% weight gain with placebo, in a phase 1 SAD trial. The candidate is currently evaluated in a phase 1 multiple ascending dose (MAD) study (n=124), which is recruiting participants and is estimated to complete in April 2026. While early, Mr. Michael said that the candidate has a potential to be “differentiated amylin,” and is eager to see more data.
Amgen: PCSK-9 inhibitor Repatha highlighted as key to Amgen’s growth through 2030; extensive discussion of long-acting T2D and obesity candidate MariTide
Amgen CEO Mr. Robert Bradway discussed Amgen’s approach to general medicine in great detail, including MariTide, Repatha (evolocumab), and olpasiran, which are major cardiovascular therapies for the company. Mr. Bradway first highlighted Amgen’s “broad and deep” portfolio across four therapeutic areas: general medicine, rare disease, oncology, and inflammation. He emphasized consistent execution across financial performance, regulatory progress, and late‑stage pipeline advancement. The company had five successful FDA approvals in 2025, with 10% year-over-year revenue growth and 14 products annualizing at $15 billion. In general medicine, Amgen is focusing on heart attacks, stroke, hypercholesterolemia, osteoporosis, chronic weight management, T2D, and obesity-related conditions. Repatha, a PCSK-9 inhibitor that lowers LDL cholesterol levels to prevent strokes and heart attacks, received high attention throughout the presentation, as did GIP antagonist/GLP-1 RA MariTide and Lp(a)-lowering olpasiran. Looking ahead, Amgen is developing a number of key therapies and is further integrating new technology and AI into its research and commercialization processes. Mr. Bradway also discussed the recent acquisition of Dark Blue Therapeutics and Disco Pharmaceuticals as opportunities for further growth.
- GIP antagonist/GLP-1 RA MariTide was discussed in detail, underscoring its potential as a differentiated long‑acting therapy for both obesity and T2D. Looking back at 2025, Mr. Bradway highlighted the six global phase 3 studies of MariTide that Amgen initiated in 2025. The company sees opportunity for MariTide in chronic weight management, atherosclerotic cardiovascular disease, heart failure, obstructive sleep apnea, and T2D. Phase 2 data showed robust reductions in A1c and weight with monthly dosing, alongside favorable cardiometabolic improvements and a tolerability profile consistent with the GLP‑1 class. In chronic weight management, the majority of participants who achieved ≥15% weight loss maintained the loss for a second year on lower monthly or quarterly dosing, with very low rates of nausea and vomiting. He said that the therapy has garnered high interest with its differentiated approach to obesity and related conditions. He highlighted MariTide’s strong treatment efficacy with monthly or even quarterly dosing in development, and that tolerability at initiation improves with multi-step dose escalation. Mr. Bradway also said that the therapy is very well tolerated at target doses and at maintenance doses. Amgen expects to establish the use of MariTide as a long-term maintenance therapy and as potentially the first monthly therapy for T2D. The company is preparing a phase 3 program to evaluate MariTide in T2D.
- The six phase 3 studies are:
- MARITIME-1, which has completed enrollment in adults living with obesity or overweight but without T2D;
- MARITIME-2, which has completed enrollment in adults with obesity or overweight with T2D;
- MARITIME-CV, which is enrolling adults living with established ASCVD and obesity or overweight;
- MARITIME-HF, which is enrolling adults living with heart failure with preserved or mildly reduced ejection fraction and obesity; and
- MARITIME-OSA-1 and MARITIME-OSA-2, which were both initiated in 3Q25 in adults living with obstructive sleep apnea.
- Recall that full results of the 52-week phase 2 trial of once-monthly MariTide in obesity with and without T2D were presented at ADA 2025. Major takeaways included the high GI adverse event rates despite robust weight and A1c reductions. In the treatment efficacy estimand, MariTide conferred up to 20% weight loss vs. 2.6% with placebo at 52 weeks. For the treatment policy estimand, MariTide conferred up to 16% weight loss compared to 2.5% with placebo.
- GI adverse events. Rates of nausea and vomiting were very high across the MariTide arms. In the non-dose escalation arms, nausea was reported by 77-87% of participants, and vomiting was reported by 68-92% of participants. Dose escalation appeared to lower the rates of adverse events; however, nausea, vomiting, and constipation rates still remained high. During today’s presentation, Mr. Bradway characterized the safety and tolerability profile as consistent with the GLP-1 RA class overall and focused on the therapeutic promise of a once-monthly or once-quarterly drug. He said that real-world experience with incretins has always demonstrated challenges such as high discontinuation rates, high treatment burden, and high required dosing frequency. Amgen believes that MariTide is suited to this challenge and that quarterly dosing can still maintain weight loss. In the second year of MariTide treatment, the therapy was very well tolerated including at quarterly doses, with a very low incidence of nausea and vomiting and no new safety signals observed.
- The six phase 3 studies are:
- PCSK-9 inhibitor Repatha is one of six major growth drivers for Amgen, expected to be a key driver of product sales in 2026 and through the end of the decade. Mr. Bradway highlighted the therapy’s strong commercial performance, up 33% from 4Q24 and annualized at approximately $3 billion, and pointed to the October 2025 VESALIUS‑CV results showing a 36% reduction in first heart attack among patients without prior cardiovascular events and 25% reduction in 3-point MACE. Mr. Bradway emphasized that more than 100 million people worldwide are not at LDL‑C targets, and penetration is still in the single digits. Amgen sees a substantial runway for expansion. He highlighted the strong clinical evidence supporting the use of the therapy and its ability to reduce in risk of first myocardial infarction in people who have never had one. During Q&A, Mr. Bradway said that Repatha was the first therapy with such demonstrable preventative effects and that it provides a new therapeutic option for patients who otherwise have optimized care, including with statins. He said that Amgen hopes to “change heart disease’s status as one of the world’s leading killers.”
- In November 2025, full results of the phase 3 VESALIUS-CV study (n=12,257) were presented at AHA, which evaluated the effects of PCSK-9 inhibitor Repatha (evolocumab) in people with high CV risk without prior atherosclerotic CVD (myocardial infarction [MI] or stroke) – including people with diabetes and/or atherosclerosis. Impressively, evolocumab conferred 20% risk reduction in all cause death, 25% risk reduction in MACE-3, and 19% risk reduction in MACE-4 at five years.
- Olpasiran, first-in-class siRNA molecule targeting Lp(a), was also highlighted for its innovative promise in general medicine. Mr. Bradway highlighted olpasiran as one of Amgen’s most important late‑stage cardiometabolic programs, emphasizing its potential to address what he described as the “residual risk” in cardiovascular disease. He noted that one in five people carries genetically elevated Lp(a), a risk factor that cannot be modified by diet or exercise, and reiterated that phase 2 data showed 95–100% reductions in Lp(a). Amgen expects the phase 3 Ocean(a)-Outcomes trial (n= 7,297) to clarify whether lowering Lp(a) can meaningfully reduce cardiac events, and Mr. Bradway stressed that if the trial confirms this, olpasiran could represent a major advance for patients at high cardiovascular risk. Mr. Bradway noted that results are expected sometime in 2027.
- On biosimilars, Mr. Bradway highlighted that through 3Q25, biosimilars grew 42% from 4Q24, and the portfolio has now generated ~$13 billion in cumulative revenue. He framed the business as a demonstration of Amgen’s ability to “reliably and safely supply” complex biologics at scale, with the slides noting that the second wave of launches (including Eylea biosimilar Pavblu) is driving current growth while a third wave advances through phase 3 development.
Amphastar: Dr. Jack Zhang shares updates on glucagon, GLP‑1 RAs, and insulin biosimilars
CEO Dr. Jack Zhang and CFO Mr. Bill Peters highlighted Amphastar’s dual‑strategy growth model, pairing strategic acquisitions like Baqsimi with internally developed complex generics, biosimilars, and novel peptides (see the webcast and presentation slides). The presentation noted that by 2026, proprietary and biosimilar programs will represent 85% of the pipeline, up from 37% in 2021. This shift is supported by sustained R&D investment and expanding technical capabilities across peptides, intranasal delivery, and recombinant DNA biologics.
- Amphastar’s branded pipeline continues to be led by Baqsimi’s (nasal glucagon) projected $250-275 million peak sales and strong US growth following its June 2023 acquisition from Lilly. Mr. Peters noted that only 12% of insulin users currently fill a glucagon prescription, up from 10% at acquisition, leaving substantial room for greater penetration. Internationally, Mr. Peters stated that Amphastar will withdraw from several unprofitable markets after its three-year contractual commitment ends in June 2026, improving the overall margin profile.
- On pipeline updates, AMP‑018, the company’s generic injectable GLP‑1 RA, is planned for a launch in 2027. He said that Amphastar is beginning third‑party sales of GLP‑1 Active Pharmaceutical Ingredient (APIs) in China, marking a strategic shift from internal‑only API use.
- On insulin, Amphastar’s biosimilar insulin programs – AMP‑004 (Novolog) and AMP‑005 (recombinant human insulin) – continue to advance. For AMP‑004, the FDA accepted the company’s biosimilar application in April 2025, and it is currently under review. Mr. Peters noted that while AMP‑025 (insulin degludec) remains in development, Amphastar may pause the program given current market conditions.
Arrowhead Pharmaceuticals: RNA interference treatments for obesity to advance to phase 2b trial
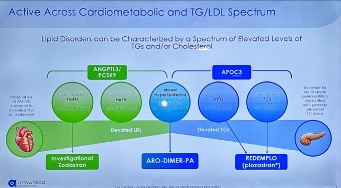
Dr. Chris Anzalone (Arrowhead Pharmaceuticals CEO) highlighted Arrowhead’s RNA interference (RNAi)-based therapy portfolio. Arrowhead is a clinical-stage biopharmaceutical company with a market capitalization of $8.9 billion and cash and investments of $920 million, excluding $200 million each from Sarepta and Novartis and $930 million from recent public offerings. The company is focused on developing RNAi therapies using its targeted RNAi molecule (TRiM) platform for a wide range of diseases. Arrowhead launched its first medicine Redemplo (plozasiran) – an RNAi treatment that targets APOC3 – for familial chylomicronemia syndrome (FCS) in November 2025 and continues to advance 20 early, mid, and late-stage clinical programs across cardiometabolic, pulmonary, liver, and neuromuscular indications. Dr. Anzalone emphasized that the TRiM platform can be applied to seven cell types (i.e., liver, lung, skeletal muscle, central nervous system, adipose tissue, ocular, and cardiomyocyte) with more to come, positioning Arrowhead as a “clear leader” of RNAi therapies.
- Obesity pipeline. Dr. Anzalone established what he envisions as the future of obesity care: (i) recognizing the heterogeneity of obesity; (ii) reducing visceral fat for cardio-kidney-metabolic outcomes; and (iii) combining therapies to further reduce cardiovascular risks. He noted that people with obesity and T2D lose less weight with incretin-based therapies, and therefore, positioned RNAi-based therapies as a potential treatment option to address unmet needs. Arrowhead is advancing ARO-INHBE (n=120) and ARO-ALK7 (n=126) studies in people with obesity with or without diabetes in phase 1/2a trials. ARO-INHBE inhibits Activin E, while ARO-ALK7 reduces the expression of ALK7, both of which are known to regulate energy homeostasis in adipose tissue. According to interim data announced last week, ARO-INHBE significantly reduced serum Activin-E by 85% on average, visceral fat by 9.9% at Week 16, and 16% with two doses at Week 24. In people with obesity and T2D, adding ARO-INHBE to tirzepatide doubled weight loss compared to tirzepatide monotherapy. Meanwhile, ARO-ALK7 decreased ALK7 gene expression by up to 88%, and conferred up to a 13.6% reduction in visceral fat (compared to a 0.5% increase with placebo) at Week 8.
- While remaining cautious about interpreting the early data, Dr. Anzalone expressed excitement about initiating phase 2b studies as soon as possible. Specifically, Arrowhead aims to assess the use of add-on therapies in combination with other GLP-1 RAs or as maintenance therapies following discontinuation of GLP-1 RAs. Beyond these candidates, Arrowhead hopes to expand its obesity pipeline with dimers and new targets for the liver and adipocytes.
- Lipid pipeline. As shown in the slide below, Arrowhead’s portfolio addresses both elevated LDL-C and triglycerides, including homozygous (HoFH) and heterozygous familial hypercholesterolemia (HeFH), severe hypertriglyceridemia (sHTG), FCS, and mixed hyperlipidemia. Redemplo (plozasiran), an RNAi therapy for APOC3, has been approved by the FDA and launched in November 2025. Zodasiran, an RNAi targeting ANGPTL3, has demonstrated a 41% reduction in LDL-C in people with HoFH and a 62% reduction in people taking PCSK9 inhibitors in a phase 2 trial (n=18), suggesting an additive benefit. It is currently being evaluated in a phase 3 trial (n=60). ARO-DIMER-PA is the first dual RNAi therapy targeting APOC3 and PCSK9. Preclinical studies in monkeys showed a significant reduction in non-HDL-C, LDL-C, and triglyceride levels. Arrowhead expects to launch phase 1/2 study for mixed hyperlipidemia in this month, with initial data expected at the end of 3Q26.
AstraZeneca: Cardiometabolic focus for 2030 and beyond led by aldosterone synthase inhibitor baxdrostat, PCSK-9 laroprovstat, and GLP-1 RAs in development
Dr. Aradhana Sarin (CFO) presented AZ’s 2025 broad-scale results and outlook for the decade to come, with a focus on cardiometabolic health second only to oncology. Since the company’s FY 2024 report, AZ has presented 16 positive phase 3 trial readouts with five key focus areas in therapeutics: oncology, cardiovascular, renal & metabolism (CVRM), respiratory & immunology, vaccines & immune therapies, and rare disease. Dr. Sarin discussed the company’s goal to achieve $80 billion in total revenue by 2030 with sustained growth for 2030 and beyond. She said that the Inflation Reduction Act and the loss of exclusivity of Farxiga (dapagliflozin) and other drugs have continued to lower revenue, which reached $54.1 billion in 2024, yet has been offset by growth in the company’s existing portfolio and the upcoming launch of key NMEs. Among other therapies, she highlighted baxdrostat (a selective aldosterone synthase inhibitor for hypertension and primary aldosteronism), Farxiga fixed dose combinations, and laroprovstat (a PCSK-9 inhibitor) as key therapies in development that will propel AZ’s growth in the remainder of this decade. Beyond 2030, she discussed weight management and CV risk factors, cell therapy and T-cell engagers, gene therapy, next-generation IO biospecifics, and antibody-drug conjugates and radioconjugates as areas of focus for the future. AZ hopes to play a role in addressing sustained cardiometabolic disease burden worldwide. Dr. Sarin also touched on the company’s specific approaches to AI, including an AI Development Agent for drug synthesis and quantitative continuous scoring to identify patients most likely to respond to treatment.
- Positive baxdrostat trial results were highlighted as helping drive AZ’s momentum across a diverse pipeline.In September 2025, results from the phase 3 BaxHTN trial for uncontrolled hypertension were announced at ESC 2025 and simultaneously published in NEJM (n=796). At 12 weeks, participants receiving baxdrostat 2 mg achieved a mean reduction of 15.7 mmHg, while those on 1 mg saw a 14.5 mmHg reduction, compared with a 5.7 mmHg reduction in those receiving placebo. These results correspond to a placebo-adjusted reduction of 9.8 mmHg with 2 mg baxdrostat and 8.7 mmHg with baxdrostat 1 mg. Results were consistent across both the uncontrolled and treatment‑resistant hypertension subgroups. Dr. Sarin said that phase 3 trial results from 2025 including BaxHTN and the phase 3 Bax24 trial for resistant hypertension present a $10 billion dollar opportunity for AZ.
- Baxdrostat is currently under FDA Priority Review. As announced in December 2025, the Prescription Drug User Fee Act (PDUFA) date for the therapy is anticipated in 2Q26. If approved, the therapy could address a major need in cardiovascular care in patients with limited treatment options. Dr. Sarin said that, upon approval, AZ expects the therapy’s adoption to proceed from specialists to primary care.
- Addressing weight management and cardiovascular risk factors will form a key part of AZ’s long-term strategy. Dr. Sarin said that AZ hopes to establish a role and eventually lead in a new weight management paradigm and in cardiovascular risk factors. She also said that AZ is uniquely positioned to deliver novel small molecule combinations and committed to “accelerating programs into late-stage development.” Dr. Sarin then highlighted three phase 3 trials ongoing for laprovstat as well as phase 2 trials of:
- Elecoglipron (a small-molecule GLP-1 RA) with readout expected in 1H26;
- AZD6234 (an amylin receptor agonist) with readout expected in 1H26; and
- The combination of AZD9550 (a dual glucagon/GLP-1 RA) and AZD6234, with readout expected in 2H26.
- Phase 3 data for laroprovstat, an oral PCSK-9 inhibitor, are expected in 2027. Dr. Sarin said that laroprovstat holds great potential because it is a once-daily, small molecule therapy with no fasting or food restrictions. In phase 2b trials, the therapy demonstrated an over 50% reduction in LDL cholesterol on top of standard-of-care statins. In 2Q25, AZ initiated three phase 3 clinical trials for AZD0780 (laroprovstat), which are all actively recruiting:
- AZURE-LDL (n=2,800) will evaluate LDL-C reduction in patients with dyslipidemia and a history of clinical ASCVD or who are at risk of a first ASCVD event.
- AZURE-HeFH (n=405) will evaluate LDL-C reduction in patients with heterozygous familial hypercholesterolemia.
- AZURE-Outcomes (n=15,100) will evaluate the time to first event of any component of MACE-Plus, a composite endpoint that includes death, myocardial infarction, stroke, revascularization, heart failure, and thromboembolic events. Patients included will either have dyslipidemia and established ASCVD or will be at high risk of a first ASCVD event.
Bayer: Kerendia (finerenone) demonstrates blockbuster potential for CKD and heart failure; pricing pressures with Eylea (aflibercept)
Mr. Stefan Oelrich (Bayer President of Pharmaceuticals Division) shared updates on Bayer’s therapies, including: (i) non-steroidal MRA Kerendia (finerenone); and (ii) anti-VEGF Eylea (aflibercept). See the webcast and presentation slides here. What a success is Kerendia! We never tire of hearing how many people it is helping.
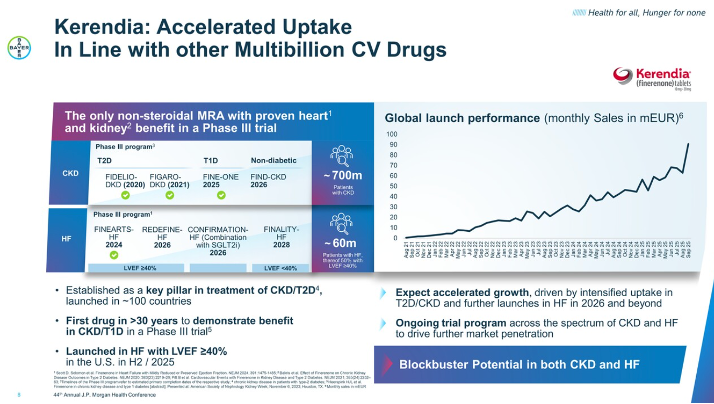
- Kerendia demonstrates blockbuster potential for CKD and heart failure. Mr. Oelrich called Kerendia the next blockbuster drug and included it as one of the key growth drivers of 2025, especially as it has demonstrated accelerated growth in T2D, CKD, and heart failure. Bayer initially pursued Kerendia for the treatment of CKD and T2D, establishing it as a key pillar across ~100 countries. Then, Bayer progressed Kerendia for a heart failure indication to encompass a broader population. At ESC 2024, results of the phase 3 FINEARTS-HF (n=6,001) trial showed that Kerendia demonstrated a 16% relative risk reduction of the primary composite outcome of total heart failure outcomes and cardiovascular death over 32 months among patients with HFmrEF or HFpEF. Following these groundbreaking results, Kerendia received FDA approval for the treatment of heart failure in July 2025. With indications for CKD and heart failure, Mr. Oelrich emphasized Kerendia’s efficacy, expecting accelerated growth driven by increased uptake and further launches in 2026 and beyond.
- Several phase 3 trial results are expected in CKD and heart failure. In 2026 alone, the following trials are expected to complete: (i) FIND-CKD trial (n=1,584) of Kerendia in adults with non-diabetic CKD; (ii) REDEFINE-HF trial (n=5,200) of Kerendia in hospitalized heart failure patients; and (iii) CONFIRMATION-HF trial (n=1,500) of the combination of Kerendia and SGLT-2 inhibitor in hospitalized patients with heart failure. Mr. Oelrich said these ongoing trials across the spectrum of CKD and heart failure are expected to drive further market penetration.
- Kerendia’s potential for T1D. At ASN 2025 in Houston, Bayer announced results from the phase 3 FINE-ONEtrial (n=241) of Kerendia in people with T1D and CKD. Kerendia significantly reduced UACR by 25% compared to placebo at six months. Echoing Mr. Bill Anderson’s (Bayer CEO) remarks during Bayer’s 3Q25 call, Mr. Oelrich emphasized that Kerendia is the first therapy in 30 years to demonstrate positive results in addressing CKD in this population. This is fantastic, particularly given all the risk of kidney disease the longer someone has had T1D. Now this is a therapy indication that we hope gets special treatment!
- Kerendia’s uptake, translated. Bayer has previously predicted a slow uptake of Kerendia, but Mr. Oelrich expressed confidence that the uptake would continue at a fast rate. In fact, we know, of course, Kerendia has shown accelerated uptake in line with “other multibillion-dollar cardiovascular drugs” – look at this curve below Mr. Oelrich said this area has limited options with high unmet needs, and therefore, positioned Kerendia as a promising treatment. He compared Kerendia to statins when they first emerged in the field – statins are used, of course, to lower cholesterol levels, and so many are seeing and experiencing Kerendia reducing risk of kidney disease. It has put UACR on the map, all right!
- Eylea sales remain stable but face increasing pricing pressures. While Mr. Oelrich strongly emphasized Eylea’s leadership in the retinal market and positioned it as the number one anti-VEGF treatment at JPM 2025, he spoke minimally about this product in today’s meeting. As background, Bayer exclusively markets Eylea outside the US, while Regeneron is responsible for US sales. Mr. Oelrich said the conversion from Eylea to Eylea HD (aflibercept 8mg), the only drug for extended treatment intervals (up to five months for nAMD and DME), is “going well.” He also said Eylea sales are “stable for now,” but commented that the company continues facing pricing pressures and expects to see more challenges with emerging biosimilars in the field.
Biocon: Addressing global non-communicable diseases like diabetes; generics and biosimilar business restructuring
Biocon Group CEO Mr. Shreehas Tambe presented the company’s approach to non-communicable diseases and diabetes in particular. Mr. Tambe said that the Biocon Group is a global biopharmaceutical company consisting four arms. Biocon Biologics, which develops biosimilars, represents 62% of revenue and has the goal of expanding access to affordable, lifesaving biotherapeutics. Biocon, the company’s generics business, forms 17% of total revenue. Syngene, the group’s research arm, represents 21% of revenue with a market cap of $2.9 billion. Finally, Bicara develops novel biologics and is NASDAQ-listed with a market cap of $1.1 billion.
Mr. Tambe emphasized Biocon Group’s history of improving access to life-saving therapeutics. In 2004, the company launched India’s first recombined human insulin, and in 2021 commercialized the first interchangeable insulin glargine in the US. In 2024, the company expanded to the ocular complication arena, receiving the first US FDA approval for biosimilar aflibercept for the treatment of eye diseases such as AMD and DME. In 2025, the company received approval and commercialized the first interchangeable insulin aspart in the US and has also offered a number of essential oncology therapies.
- Biocon Group plans to help address a shift in global disease burden from communicable to non-communicable diseases. Mr. Tambe said that Biocon has seen a significant change in global need since the 1990s. Non-communicable disease such as cancer, diabetes, musculoskeletal, and autoimmune diseases now form a very significant portion of global disease burden that Biocon plans to address. He pointed to a number of the company’s current biosimilars and generics, such as the approved therapies glargine U100, liraglutide, aspart, dapagliflozin, and recombinant human insulin for diabetes and obesity as an example of Biocon’s work on this front. In company’s pipeline for diabetes care, Mr. Tambe identified semaglutide, tirzepatide, and glargine U100. When combined with the company’s offerings in oncology and immunology, these therapies will address over 60% of global disease burden, he said. The company hopes to serve one-in-five of all people taking insulin specifically.
- Biocon Group will combine its generics and biosimilar businesses into one entity. Current companies Biocon and Biocon Biologics will become one under “Biocon,” biosimilars, insulins, peptides, and complex generics. Mr. Tambe said that this will help the businesses maximize research & development, manufacturing, and commercialization. The move will also allow Biocon to cross-leverage aspects of its portfolio and commercial infrastructure.
- Mr. Tambe said that Biocon hopes to build upon its strong launch momentum going into 2026. In the US, wave one of the first interchangeable insulin aspart, Kirsty, launched in September 2025, and the therapy has already launched in the rest of the world. In the GLP-1 RA arena, Ladiazyl and Lobezyl (generic liraglutide) have launched in the UK and select EU markets and have been filed in the US. Generic semaglutide has been filed in Canada, Brazil, the US, and in other select markets. With these anticipated approvals and its business restructuring, Biocon Group hopes to begin to address the rise in non-communicable diseases.
Biomea Fusion: Phase 2 data for Icovamenib and phase 1 results of GLP-1 RA BMF-650 expected in 2026
In this afternoon session, Dr. Mick Hitchcock, interim CEO of Biomea Fusion, highlighted key programs: icovamenib and the GLP-1 RA BMF-650. He first began by emphasizing that current treatments for T2D primarily address downstream metabolic symptoms, rather than the disease pathway. Icovamenib is an oral covalent menin inhibitor that promotes beta cell proliferation and function in people with T2D. This candidate was developed based on human physiology: pregnant or lactating women were found to suppress menin, leading to beta cell expansion and insulin secretion. Preclinical studies in rats and human islet cells confirmed that menin inhibition promotes beta cell proliferation.
- In the phase 2b COVALENT-111 trial, icovamenib significantly reduced A1c values by 1.2 percentage points (vs. a 0.3 percentage point increase with placebo) and increased C-peptide level by 29% (vs. 2%) in the severe insulin-deficient subgroup (~60% of T2D) at Week 52. Dr. Hitchcock pointed out that a short 12-week dosing period induced epigenetic changes for beta cell regeneration, resulting in sustained improvement in A1c values for a year. Moreover, a post-hoc analysis found that icovamenib is especially efficacious in people on GLP-1 RA therapy whose baseline A1c was >7.0%. Icovamenib conferred a 1.2 percentage point reduction in A1c in this population compared to a 0.6 percentage point increase with placebo. This finding showed that Icovamenib was generally well-tolerated, with no reports of adverse event-related discontinuations or serious adverse events. Ultimately, Dr. Hitchcock said that icovamenib could offer patients a short-term oral treatment, rather than lifelong insulin use.
- Looking ahead, Biomea Fusion will evaluate icovamenib in the phase 2b COVALENT-211 trial for people with insulin-deficient T2D (~20% of T2D) and the phase 2 COVALENT 212 trial for people with difficult-to-manage T2D already on GLP-1 RAs (70% of people taking GLP-1 RAs). Both trials will begin recruiting in 1Q26, and 26-week results are expected in 4Q26.
- During Q&A, Dr. Hitchcock said that the “win scenario” for icovamenib would be conferring a ≥0.5% A1c reduction at 26 weeks to remain “approvable.” An A1c reduction by 1.8-2.0% would allow icovamenib to be competitive. He also clarified that the phase 3 trials for icovamenib could be smaller programs, given that the drug is administered for 12 weeks and thus is not considered a “chronic agent.”
- BMF-650 is an oral small molecule GLP-1 RA. It is currently evaluated in the phase 1 GLP-131 trial in people with obesity (BMI ≥30 kg/m2) who are otherwise healthy; 28-day weight loss results are expected in 2Q26. Dr. Hitchcock said that BMF-650 is designed for better bioavailability and has the potential to deliver more consistent efficacy than other oral GLP-1 RAs like orforglipron. Moreover, BMF-650 has the same chemotype as orforglipron, as opposed to the chemotype to which the now-discontinued danuglipron, lotiglipron, and TERN-601 belonged. This chemotype, as well as preclinical studies in monkeys, gives Biomea Fusion confidence that BMF-650 will not cause liver-related safety issues.
- During Q&A, Dr. Hitchcock defined success for BMF-650 as involving a competitive weight loss magnitude, favorable tolerability, a faster titration scheme, and durability of weight loss.
Corcept Therapeutics: Dr. Joseph Belanoff highlights broad implications of cortisol modulation, including hypercortisolism, obesity, and diabetes
In this afternoon session, CEO Dr. Joseph Belanoff discussed Corcept Therapeutics’ focus on cortisol modulation.He first explained that cortisol regulates metabolism, immune system, apoptosis, and psychiatric health. Excess cortisol is often an underlying driver of the Cushing syndrome (hypercortisolism); cardiometabolic diseases like hypertension, diabetes, obesity, and metabolic dysfunction-associated steatohepatitis (MASH); cancer; and neurological diseases like Alzheimer’s. Hence, cortisol modulation has a potential for broad therapeutic opportunities.
- Dr. Belanoff reviewed the findings of the CATALYST trial, highlighting the higher-than-expected prevalence of hypercortisolism. To many experts’ surprise, Part 1 (n=1,113) found that nearly a quarter of individuals with difficult-to-manage T2D had underlying hypercortisolism. Moreover, in Part 2 (n=252) of the trial, Korlym (mifepristone), a glucocorticoid receptor antagonist and a treatment for hypercortisolism, significantly lowered mean A1c (1.5 percentage points vs. none with placebo), weight, and visceral fat. Given the high prevalence of hypercortisolism, Dr. Belanoff estimates that the drug has potential to reach $2 billion in annual revenue.
- Corcept Therapeutics is developing relacorilant (a highly selective glucocorticoid receptor agonist) for the treatment of hypercortisolism with hypertension and/or hyperglycemia. Relacorilant aimed to address the limitations of Korylm as a non-selective progesterone and glucocorticoid antagonist (which could also be used to induce abortion). In the phase 3 GRACE program, the candidate significantly lowered systolic blood pressure by 12.6 mmHg and A1c by 0.7 percentage points from a baseline of 7.1%. Despite these results, Corcept Therapeutics received a Complete Response Letter from the FDA in December 2025, noting that more evidence of effectiveness is necessary to show favorable benefit-risk assessment. Dr. Belanoff said that the company plans to meet with the agency soon to discuss its concerns, provide additional analyses, or potentially appeal the decision.
- In MASH, miricorilant, a selective glucocorticoid receptor, is currently evaluated in a phase 2 MONARCH (n=175) study among patients with biopsy-confirmed MASH. The trial has completed enrollment, with results expected by year-end 2026. In phase 1b trial, miricorilant demonstrated 30% reduction in liver fat, as well as improvement in liver health and fibrosis, with favorable tolerability profile.
Esperion: Updated US lipid-lowering guidelines to include bempedoic acid offering; international expansions; combination therapy
Esperion CEO Mr. Sheldon Koenig presented the company’s approach to expansion, profitability, and its bempedoic acid portfolio. He began by saying that Esperion is in a strong financial position, with a strong balance sheet, durable cash flows, and an attractive profit and loss profile. He said that the company will reach sustainable profitability in 2026. Esperion’s current offerings are nexletol (bempedoic acid) and nexlizet (bempedoic acid/ezetimibe). Bempedoic acid is an ATP citrate lyase inhibitor that reduces low-density lipoprotein (LDL) cholesterol levels. It was first approved in the US in February 2020 and offers therapeutic opportunity for patients unwilling or unable to take statins, as well as for use in combination therapy. Mr. Koenig discussed Esperion’s impressive international reach, pipeline, and scientific approach.
- Esperion plans to strengthen and expand the bempedoic acid franchise beyond nexletol and nexlizet. Mr. Koenig identified six major catalysts that will drive growth for Esperion in 2026 and beyond. Most prominently, bempedoic acid is expected to be included in updated US lipid-lowering guidelines by the end of February. This will follow guidelinesreleased by the European Society of Cardiology (ESC) in September 2025, which recommend bempedoic acid in patients who are unable to take statin therapy to achieve their LDL-C goals. Market exclusivity is also expected in 2026, as well as further commercial investment, an oral triple combination therapy, international expansion, and improved gross margins.
- On the updated US lipid-lowering guidelines, Mr. Koenig drew parallels to the treatment of hypertension and of T2D, where combination therapy is now the standard of care after years of having one leading therapy. He said that the management of high cholesterol will now move towards combination therapy including bempedoic acid based on key outcome study data. In a March 2023 study published in NEJM (n= 13,970), bempedoic acid reduced the incidence of myocardial infarction by approximately 14% and incidence of coronary revascularization by 19%.
- Preclinical development continues for Esperion’s triple combination therapies, which include bempedoic acid, ezetimibe, and statin therapy (atorvastatin or rosuvastatin). The company first announced the oral triple combination in 4Q24, positioning it as a next-generation option for LDL-c lowering.
- Mr. Koenig highlighted Esperion’s partner-led international expansion, asking the audience to think of the company as a global franchise. Esperion’s bempedoic acid franchise is currently approved in 41 countries. In Europe, Asia, and South America, Daiichi Sankyo is leading the expansion efforts, with over 600,000 patients treated to date. In Japan, Esperion launched in December 2025 in partnership with Otsuka. The company plans to work with Neopharm Israel to expand to the nation in 1H26, and with CSL Seqirus to seek approvals in Australia and New Zealand, which are expected in 4Q26. In Canada, Esperion has partnered with HLS therapeutics and expects approval in 2026.
- Mr. Koenig also said that the company is also seeking portfolio growth through partnerships, with key areas of focus in cardiometabolic health, kidney disease, diabetes, and rare and orphan diseases. He said that Esperion will not seek any very large acquisitions and will instead pursue strategic acquisitions that are immediately accretive. Mr. Koenig also spoke of “activating” consumers in 2025 with plans to continue this in 2026 – Esperion has launched publicity buttons reading, “Can’t take a Statin? Make NEXLIZET Happen!” as well as non-skippable ads on streaming platforms. Mr. Koenig said that most consumers have not attempted to skip the ads, which he framed as a positive sign for therapeutic awareness.
Ionis Pharmaceuticals: Tryngolza gains traction in treatment of FCS ahead of broader launch; pelacarsen for Lp(a) risk reduction on track for launch in 2027
CEO Dr. Brett Monia highlighted Ionis’s cardiometabolic franchise, emphasizing the commercial momentum of Tryngolza (olezarsen) for the treatment of familial chylomicronemia syndrome (FCS), and the potential of pelacarsen to reshape Lp(a)-driven cardiovascular risk. Tryngolza was approved in December 2024 in the US and September 2025 in the EU for FCS. It generated more than $100 million in US net revenue in its first year, with Dr. Monia describing “overwhelmingly positive” patient feedback and strong physician reauthorization rates. Ionis is preparing a broader launch in severe hypertriglyceridemia (SHTG), for which phase 3 CORE and CORE-2 trial data showed 72% fasting triglyceride reduction, 86% of patients below the pancreatitis risk threshold, and an 85% reduction in acute pancreatitis events. Dr. Monia confirmed that the supplemental NDA was submitted in December and that Ionis has requested priority review. If granted, approval could come as early as July 2026.
- On Lp(a), Dr. Monia reiterated enthusiasm for pelacarsen, developed in partnership with Novartis, and positioned it as a first-in-class siRNA therapy targeting genetically elevated Lp(a). He emphasized that phase 2 data showed >95% reductions in Lp(a) levels. The phase 3 HORIZON outcomes trial (n=8,323) is expected to read out in 1H26, with Dr. Monia Ionis anticipating a 2027 launch pending positive results. Dr. Monia noted that the trial is powered to detect a 20% relative risk reduction overall and 25% in patients with very high Lp(a), but emphasized that given the lack of approved therapies, a 10-15% reduction in cardiovascular events would be considered a meaningful win and may be sufficient for Novartis to pursue approval.
J&J: CEO Mr. Joaquin Duato outlines diversified growth strategy with momentum in cardiovascular portfolio
In this standing-room-only session, CEO Mr. Joaquin Duato discussed J&J’s top priorities in 2026, which include MedTech, cardiovascular business, as well as surgery and ophthalmology sectors. Mr. Duato especially spotlighted J&J’s cardiology franchise, which is approaching $9 billion, anchored by cardiac ablation, heart failure device company Abiomed, and calcified arterial disease with Shockwave Medical. Notably, J&J plans to launch the Shockwave C2 Aero coronary catheter in 2026, reinforcing its leadership in interventional cardiology. While there was no direct mention of diabetes or obesity, we are excited about these advancements given that cardiovascular disease is the leading cause of mortality in this population. Mr. Joaquin also shared insights into how J&J navigates the dynamic business environment with the Trump administration.
- Mr. Duato reiterated the company’s goal to manufacture the majority of its advanced medicines used in the US, with two new plants underway in North Carolina for biologics manufacturing and Pennsylvania for cell therapy manufacturing, part of a $55 billion investment plan. The sites were announced as part of an agreement with the US government that will allow access to medicines at discounted rates for millions of patients. In exchange, the company’s pharmaceutical products are exempt from tariffs. Moreover, as part of the Most Favored Nation deal announced in November 2025, the company will also be participating in the direct-to-consumer platform TrumpRx to offer J&J medicines at discounted rates, joining other companies like Pfizer, Lilly, and Novo Nordisk. Mr. Duato viewed these agreements as a “step in the right direction,” as they expand access to medicines and give companies exception from tariffs, allowing the companies to focus on “what [they] do best” – developing, manufacturing, and commercializing medicines.
Kailera Therapeutics: CEO Mr. Ron Renaud highlights diversified GLP-1 RA pipeline for obesity treatment
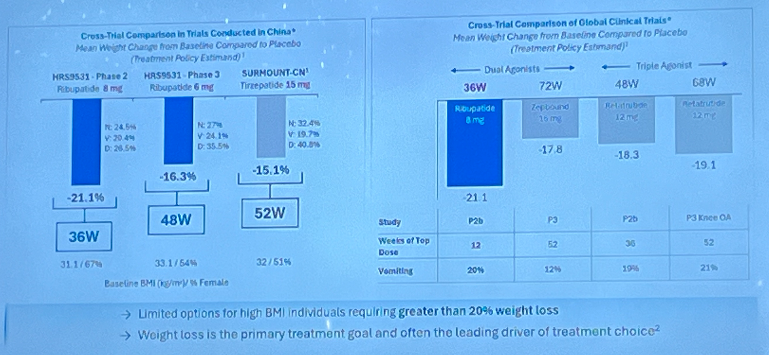
In a morning symposium, CEO Mr. Ron Renaud highlighted Kailera Therapeutics’ obesity pipeline and its broader business strategies. As background, Kailera is a California- and Massachusetts-based clinical-stage company launched in October 2024 with $400 million Series A financing round. It develops an obesity pipeline acquired in May 2024 from Jiangsu Hengrui Pharmaceuticals. Kailera has exclusive global development and commercialization rights outside of Greater China for four metabolic disease assets, as Mr. Renaud detailed in his presentation. He began by highlighting that over half of US adults with obesity are projected to have a BMI ≥35 kg/m2 by 2030. Moreover, 68% of participants in SURMOUNT-1 with baseline BMI ≥35 kg/m2 did not reach BMI <30 kg/m2, indicating significant unmet needs in people with severe obesity.
- Ribupatide (KAI-9531) is an injectable dual GLP-1/GIP RA designed to be more efficacious than tirzepatide, by making GLP-1 agonism three times more potent and GIP agonism half as potent as tirzepatide. KAI-9531 also has a half-life of seven days, compared to five days for tirzepatide. In a phase 2 trial (n=61), ribupatide conferred placebo-adjusted weight loss of 21.1% at Week 36 with a higher dose of 8 mg. In a phase 3 trial (n=567), KAI-9531 6 mg previously achieved up to 17.5% mean weight loss without a plateau at Week 48, with 44% of participants achieving ≥20% weight loss.
- While cautious to make cross-trial comparisons, he noted that ribupatide conferred greater weight loss than tirzepatide and retatrutide at shorter study durations. See figure below.
- Looking forward, ribupatide is evaluated in three ongoing phase 3 KaiNETIC trials (n=1,600, 1,700, and 1,200) for doses up to 10 mg for over 76 weeks. One trial includes participants with T2D, while another includes those with high BMI ≥35 kg/m2. Kailera announced today that the first participants randomized in the phase 3 KaiNETIC program have been dosed.
- Kailera also has other GLP-1 RA-based candidates:
- Oral ribupatide is progressing into phase 2 in 2026. In a phase 1 trial, the candidate conferred 5.4% weight loss at Week 4, and 6.3% experienced vomiting, suggesting potentially favorable tolerability profile.
- Oral KAI-7535, a once-daily oral small molecule GLP-1 RA, will progress to phase 2 in 2026, as well. In primary and post-hoc analyses of a phase 2 trial, KAI-7535 led to 9.5-15% weight loss with low liver risk.
- KAI-4729, a once-weekly GLP-1/GIP/glucagon triple agonist, is intended to deliver strong weight loss and improved liver fat reduction. In preclinical studies, KAI-4729 showed the potential to confer greater weight loss than retatrutide. This candidate will progress to phase 1 in 2026.
- During Q&A, when asked about the impact of semaglutide’s loss of exclusivity in the early 2030s, when these candidates are expected to launch, Mr. Renaud shared confidence that its focus on people with severe obesity (BMI ≥35 kg/m2) and robust clinical data can help Kailera secure reimbursement. To another question about pipeline diversity, Mr. Renaud said that additional mechanisms of action will be needed in parallel or as an add-on to GLP-1 RA-based therapies. However, he believes that GLP-1 RAs will remain backbone treatments, and Kailera’s candidates have a strong potential to be differentiated assets as GLP-1 RA therapies.
Lexicon Pharmaceuticals: Dr. Mike Exton highlights SGLT-1/2 inhibitor sotagliflozin, pilavapadin for DPN, and non-incretin obesity candidate
CEO Dr. Mike Exton discussed Lexicon Pharmaceuticals’s clinical pipeline spanning cardiometabolic diseases and diabetic peripheral neuropathy (DPN). He first explained that Lexicon was founded in 1995 as a genetically informed drug discovery company. From ~5,000 genes identified in the Genome5000 project, the company developed multiple drug candidates, two of which have been approved. Lexicon also continues to advance novel targeted therapies, such as: (i) sotagliflozin for hypertrophic cardiomyopathy (HCM) and T1D; (ii) pilavapadin for DPN; and (iii) LX9851 for obesity and weight management. The company has $125 million in cash and cash equivalents with a runway into 2027.
- Dual SGLT-1/2 inhibitor sotagliflozin is currently approved for heart failure under the brand name Inpefa. In the US, where Lexicon removed all commercial operations as of November 2024, Dr. Exton said that Lexicon’s virtual salesforce team continues to support patients. Outside the US and EU, its partner Viatris secured approval in UAE for worsening heart failure and filed for regulatory approval in Saudi Arabia, Canada, Australia, New Zealand, Mexico, and Malaysia. Dr. Exton also highlighted additional indications that Lexicon is pursuing:
- HCM. Sotagliflozin is currently being evaluated in the phase 3 SONATA-HCM trial (n=500). Lexicon has initiated all trial sites and aims to complete enrollment in 1H26, with topline data expected in 1Q27. Dr. Exton explained that the dual inhibition of SGLT-1 and SGLT-2 allows sotagliflozin to target both obstructive (due to outflow tract obstruction) and non-obstructive HCM (due to altered metabolism) by directly modifying cellular energetics in the heart. Moreover, he believes that the once-daily dosing and safety profile position sotagliflozin to be a potential first-line agent for HCM.
- T1D. Under the brand name Zynquista, sotagliflozin is also being evaluated as an adjunct-to-insulin therapy for glycemic management in people with T1D. Dr. Exton said that a Type D meeting with the FDA confirmed that the STENO1 (n=200) trial is sufficient to support NDA resubmission. Lexicon estimates that resubmission and regulatory decision will occur in 2026.
- The STENO1 trial (n=200) is an open-label study that evaluates the cardiovascular effects of several interventions in adults with T1D. The trial was initiated in July 2024 and is expected to complete in July 2029.
- LX9851 is an oral non-incretin candidate that inhibits Acyl-CoA Synthetase 5 (ACSL5) and is being evaluated for weight management. In March 2025, Novo Nordisk entered an exclusive licensing agreement to develop and commercialize LX9851. Consistent with its 3Q25 update, Lexicon completed all IND-enabling studies and delivered results to Novo Nordisk in 2025, achieving the initial requirements for a $10 million milestone payment. Dr. Exton said that the company has the potential to achieve an additional $20 million in milestone payments in 2026. Preclinical data have shown potential benefits for lipid lowering and MASH.
- Pilavapadin is an oral non-opioid AAK1 inhibitor (LX9211) being evaluated for adults with moderate-to-severe DPN. At EASD 2025, Lexicon announced results of the phase 2b PROGRESS trial, which showed an early separation in pain scores between pilavapadin and placebo. Dr. Exton said that Lexicon is now seeking a partner to conduct phase 3 trials. He also highlighted several legislative initiatives to support non-opioid innovations in chronic pain. These include the Alternatives to PAIN Act, aimed at improving access to non-opioid medications for Medicare Part D beneficiaries, and the FDA’s draft guidance from September 2025 on non-opioid analgesics for chronic pain.
Lilly: Mr. David Ricks shares insights about obesity market, payment channels, and clinical pipeline including orforglipron
In a packed afternoon symposium, CEO Mr. David Ricks shared reflections from 2025 and vision for the coming years for Lilly. He first celebrated that this year marks 150 years of Lilly’s existence and leading innovation since 1876. He then offered reflections about the past couple of years. After a “choppy, unclear year” in 2024 with uncertainty about supply, access, and drug uptake, Lilly delivered strong performance in 2025, stabilizing all three of those factors. There is no longer a shortage of tirzepatide; negotiations with the US government expanded access with lower price burden for patients; and LillyDirect reached more patients through cash channel. Moreover, Lilly continues to advance its clinical pipeline, including tirzepatide (dual GLP-1/GIP RA), orforglipron (oral GLP-1 RA), retatrutide (triple GLP-1/GIP/glucagon RA), eloralintide (long-acting amylin agonist), brenipatide (dual GLP-1/GIP RA), and six additional programs in phase 1. Mr. Ricks said these candidates have the potential to treat one billion people worldwide with obesity, cardio-renal-metabolic diseases, obstructive sleep apnea, and potentially even neurological or inflammatory diseases. Indeed, the indications continue to expand, as a recent phase 3 TOGETHER-PsA trial (n=271) showed significant benefits of tirzepatide when administered together with Taltz (ixekizumab) in people with psoriatic arthritis. In a dialogue with Mr. Chris Schott (Managing Director, JPMorgan), Mr. Ricks shared his insights about the obesity market, payment channels, and the competitive landscape.
- On orforglipron, which delivered key phase 3 results for T2D and obesity last year, Mr. Ricks said that regulatory filing submitted to the FDA under the new priority voucher program. Approval is expected in 2Q26. Mr. Ricks speculated that oral formulation would be helpful for patients with aversion to needles, perception of escalating medicine from lifestyle modifications to injectable medicines, or those already on polypharmacy. Moreover, orforglipron can be a promising option for those who want weight maintenance. In a blinded phase of a clinical trial, orforglipron conferred greater weight loss in people who discontinued semaglutide and gained modest weight in those who took tirzepatide; ultimately, orforglipron stabilized weight loss from either of the two medications. He especially believes that orforglipron would be more dominant than injectable GLP-1 RAs in OUS markets, where launch is expected in 2026 and 2027. Responding to Mr. Mike Doustdar’s (CEO, Novo Nordisk) comment on a clinical trial protocol, in which participants were directed to wait two to four hours after statin administration, Mr. Ricks said that the protocol was largely due to the timing of clinical development – Lilly had simply not conducted drug interaction studies with statins when initiating the trial.
- On different payment channels, Mr. Ricks said that Medicare has better penetration than the commercial market. Because government coverage often becomes the standard, the inclusion criteria for coverage tend to be more based on science. For tirzepatide, the criteria include people with overweight and comorbidities (e.g., CVD, peripheral artery disease, and prediabetes) or obesity – which Mr. Ricks said is significantly better than most commercial coverage. Moreover, with the recent Most Favored Nation negotiation – which Mr. Ricks characterized as a “unique deal” – out-of-pocket cost is “reasonable” at $50. He believes that all states will follow this standard for Medicaid programs and hopes that the coverage will spill over to commercial channels. Mr. Ricks added that incretin-based therapies offer preventive benefits, which is even more beneficial for countries with higher healthcare costs, as the return-on-investment is greater.
- On the commercial channel, he shared that new pharmacy benefit managers (PBMs) are emerging with more price transparency. He advocated for greater transparency is needed in the US, including what the post-rebate cost will be.
- LillyDirect, Lilly’s direct-to-consumer platform, has been very successful. He said that the price transparency with knowing the exact cost before buying, as well as notices for renewal cycle, allows patients to take charge of their own health.
- On the overall obesity market, Mr. Ricks welcomed companies entering the obesity landscape. He emphasized that Lilly will maintain its excellence in R&D and “multiple shots on goal” strategy to develop differentiated candidates. Looking forward, he expects more swings in 2026, especially given the uncertainty about the volume. Hence, the company will likely provide a guidance with a broader range. Finally, he also pointed to its AI initiatives, including its collaboration with NVIDIA, as opportunities for growth.
Madrigal: “10% of 10%” of global MASH patients treated; detailed approaches to combination therapy including GLP-1 RAs and DGAT-2 inhibitors
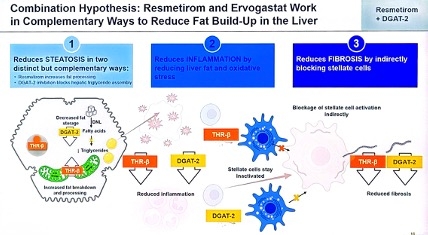
Madrigal CEO Mr. Bill Sibold, CMO Dr. Dave Soergel, and CFO Ms. Mardi Dier discussed the company’s approach to growth in 2026 and beyond, highlighting its recent expansion to a three-product portfolio. Mr. Sibold said that Madrigal has three areas of growth for the future: (i) delivering on the best-in-industry drug launch of Rezdiffra; (ii) progressing towards an indication for stage F4 fibrosis (cirrhosis, F4c); and (iii) extending leadership through pipeline expansion. The company will focus on combination therapy with Rezdiffra and the phase 2 oral DGAT-2 inhibitor ervogastat (which the company licensed from Pfizer just last Friday), combination therapy with SYH2086 (a small molecule oral GLP-1 RA licensed from CSPC Pharmaceutical Group in July 2025), and the F4c indication in 2026. With over 29,500 patients on therapy as of 3Q25, Madrigal still has significant potential for expansion – the market of 315,000 patients with diagnosed F2/F3 fibrosis is about 10% penetrated, which represents only 10% of all patients thought to have MASH. Many patients remain undiagnosed. This “10% of 10%” strategy of addressing a greater patient population fuels Madrigal’s optimism for the future. Mr. Sibold also compared the launch of Rezdiffra to the launch of specialty therapeutics for irritable bowel disease, rheumatoid, and psoriasis over the past thirty years. He explained that therapies for these conditions were all once thought to be very niche markets, yet all three have now grown to over $20 billion markets. Madrigal believes that the liver health market is only at the cusp of its future growth.
- Oral DGAT-2 inhibitor ervogastat offers promise for Madrigal’s pipeline. Three days ago, Madrigal announced that it has entered an exclusive global license agreement with Pfizer for ervogastat, as well as and two early-stage candidates for the treatment of MASH. Pfizer received an upfront payment of $50 million and is eligible for milestone payments and royalties on net sales. Madrigal has rights to develop, manufacture, and commercialize ervogastat globally. Dr. Soergel discussed the mechanism of action of the therapeutic class: DGAT-2 inhibitors block the enzyme called diacylglycerol acyltransferase 2 (DGAT-2), which catalyzes the final step of triglyceride synthesis and storage in the liver, lowering lipotoxic fat and inflammation. The therapy will be delivered orally and is expected to be combined with Rezdiffra, as the therapies work in distinct, complementary ways.
- In 2026, Madrigal will conduct a drug-drug interaction study of the two therapies, with a phase 2 combination study anticipated to start in 2027 following regulatory discussions. In previous studies, ervogastat has demonstrated impressive liver fat reduction, with up to 61% percent of patients considered super responders (a 50% reduction of liver fat from baseline over 48 weeks). This represents significant clinical improvement to liver fibrosis.
- Combination therapy with oral GLP-1 RA MGL-2086 was also a focus of discussion. In July 2025, Madrigal entered an exclusive global license agreement with China-based CSPC Pharmaceutical Group for SYH2086, a preclinical oral small molecule and orforglipron derivative. The therapy, now known as MGL-2086, has the potential to improve Rezdiffra’s efficacy in combination therapy. Dr. Soergel explained that weight loss of ≥5% significantly improves Rezdiffra’s efficacy, emphasizing that the company is therefore targeting such modest weight loss as opposed to greater proportions. He said that a MGL-2086 phase 1 single ascending dose study will begin in 2Q26.
- Madrigal seeks an expanded indication for compensated MASH cirrhosis, also known as stage 4 fibrosis (F4c). A significant unmet need remains in this disease stage, with an estimated addressable patient population of 245,000. There is a high urgency to treat these patients as there is a 42-fold greater risk of liver-related mortality. Management said that F4c outcomes trial data are estimated to be delivered in 2027, and that two-year data from MAESTRO-NASH OUTCOMES provides confidence in the future results. With over 10,000 current or past prescribers of Rezdiffra, Mr. Sibold said that adoption of the therapy for F4c is expected to be rapid upon approval with the therapy’s growing familiarity. As the therapeutic landscape continues to change rapidly, Madrigal says it is tracking to be first to market for this indication and more.
Merck: “Democratizing” PCSK9 therapy and combinations with Lp(a); MK 3000 as a potential new mechanism of action for diabetic macular edema
Merck Chairman and CEO Mr. Robert Davis highlighted a new wave of late-stage assets on Monday afternoon, which extend the company’s reach beyond its historic core of oncology medicines. Enlicitide (oral PCSK9 inhibitor), MK 3000 (tetravalent, tri-specific Wnt antibodies), and the oral Lp(a) small molecule underscore Merck’s expansion into cardiometabolic disease. For a company that developed its Januvia franchise for presumably $1 - $2 billion, that has yielded well over $50 billion in revenue, we are very intrigued by the way that the company discussed Enlicitide – very efficacious, very safe, and very easy to take (our way of describing “tolerable”).
- Overall pipeline and financial portfolio framing. Merck projects over $70 billion in commercial opportunity by mid-2030, representing a $20 billion increase from 2025. Ten key programs, which notably include Enlicitide, account for around 70% of the $70 billion in sales. Nearly all have first-in-class potential with multi-billion peak sales. Four of those ten have already launched or have positive phase 3 data, while the remainder are expected to have major phase 3 readouts in the next 12-18 months. Positively, Mr. Davis shared that half of the $70 billion is expected to be clinically de-risked via phase 3 readouts by the end of 2026, with near-complete de-risking expected by the end of 2027.
- Enlicitide. Mr. Davis characterized Enlicitide as a therapy that was designed to be a potent LDL-lowering pill, with effects that “looked like the antibodies” – functioning as a “biologic in a pill.” In 2025, Enlicitide had three clinical readouts: (i) CORALreef Lipids (n=2,912); (ii) CORALreef HeFH (n=303); and (iii) CORALreef AddOn (n=301). Results demonstrated ~97% adherence and adverse event rates similar to placebo, supporting a broad use profile. Notably, it sounded like Merck hopes to “democratize” PCSK9 with Enlicitide by offering an affordable pill which can be widely accessed in the US and globally – as compared to a more niche, injectable therapy. We were extremely moved by Mr. Davis’ discussion of how good cholesterol scores could look and be. We will be extremely interested in watching how guidelines are discussed in the month and years ahead, particularly given some of the results at AHA.
- MK 3000. Mr. Davis highlighted MK 3000 as a potential new mechanism of action for the treatment of diabetic macular edema (DME). Phase 3 readouts of the BRUNELLO (n=984) and BAROLO (n=1,054) trials are targeted for September 2026. Mr. Davis emphasized that timing is “well ahead” of what was initially expected.
- Lp(a) oral small molecule. Merck acquired the Lp(a) small molecule candidate through a transaction with Longray and hopes to develop it as a combination therapy with Enlicitide – thereby combining a PCKS9-mediated LDL lowering with Lp(a) reduction in patients with a high cardiovascular risk. This combination, notably, was presented as part of a broader cardiometabolic plan which also includes Enlicitide-statin combinations, reflecting a company philosophy of being “first or best” and then planning “what’s next.”
Novartis: De-risked pipeline driving post-Entresto growth; Leqvio as the foundational therapy for the company’s cardiorenal metabolic franchise
CEO Dr. Vas Narasimhan’s presented Novartis as a focused “pure‑play medicines” company entering a “catalyst‑rich” period on Monday morning. He detailed a diversified pipeline that expects to compensate for Entresto’s (an angiotensin receptor-neprilysin inhibitor) loss of exclusivity in July 2025 and sustain ~5% annual growth through 2030.
- Overall pipeline and financial portfolio framing. Dr. Narasimhan shared 14 in‑market blockbusters and nine additional brands with multi‑billion‑dollar sales potential in Novartis’s portfolio. Moreover, the company is hosting six active launches and expects 15 submission‑enabling readouts over the next two years. Dr. Narasimhan shared that the company targets ~5% annual growth through 2030, which is supported by a deep portfolio of patent-protected assets.
- Dr. Narasimhan described Novartis’ cardiovascular risk reduction portfolio as being built “on the back of Leqvio” – a foundational lipid‑lowering medicine. The company intends to extend its cardiovascular risk-reduction portfolio with “siRNAs to more infrequently administered medicines,” signaling interest in its RNA‑based programs that designed to improve durability and reduce patient burden of treatment in chronic cardiovascular disease.
- Dr. Narasimhan also shared excitement on Novartis’ “portfolio of assets in the renal space.” While specific candidates were not specifically named today’s presentation or Q&A, Novartis’ renal assets were considered to be in the company’s late-stage plan for a 2026-2030 catalyst and subsequent launch cycle.
Novo Nordisk: Mr. Mike Doustdar on mastering cash channel, reframing perception of the semaglutide, and clinical pipeline with CagriSema, cagrilintide, and amycretin
In this extremely packed converation, CEO Mr. Maziar Mike Doustdar shared his perspectives on the challenges Novo Nordisk has faced and its vision for 2026 and onward. He began by reiterating Novo Nordisk’s commitment to treating obesity, diabetes, and comorbidities. Given that only 7% of people with diabetes and 2% of those with obesity are prescribed GLP-1 RAs or obesity medications worldwide, there is a significant unmet need that Novo Nordisk can address. That said, Novo Nordisk had a turbulent year in 2025 due to market challenges from continued compounding business, competition, and pricing pressure. Mr. Doustdar characterized these challenges as the “curse of a leader” of having to navigate clinical development and commercialization through trial-and-error. For over a decade, Novo Nordisk often faced doubts for developing medications for obesity, a condition previously considered as a lifestyle choice. Mr. Doustdar said that in 2025, the company had to critically recognize that the landscape had significantly changed, and that Novo Nordisk was no longer alone in the field. He further detailed what Novo Nordisk would have done differently and what key priorities the company will pursue in 2026.
- On the overall strategy for 2026, Mr. Doustdar highlighted three key goals: (i) master direct-to-patient and cash channels; (ii) expand the market through Wegovy pills; and (iii) reframe market perception of injectable semaglutide by launching higher dosage options. On the former, he recognizes that patients in the US – even those with insurance – face significant barriers to accessing medications, like prior authorizations. These obstacles had led to a rise of other entities like compounders. Novo Nordisk will thus continue to focus on cash channels in the US, “meeting the patients where they are.”
- When asked about the Most-Favored-Nation deal, Mr. Doustdar said that Novo Nordisk and the government negotiated carefully to determine the “sweet spot” at which volume increase balances the lower price. While he is confident about the future outlook, he said that there will be “short-term pain” because volume will not double immediately.
- On the Wegovy pill, Mr. Doustdar emphasized that it delivers ~15% weight loss, equivalent to injectable Wegovy, as well as cardiovascular benefits – indicating a promising label. He also believes that the oral formulation will broaden the market to a “large extent.” People who may be needle-aversive, cannot refrigerate Wegovy pens (e.g., due to frequent traveling), or are concerned about “escalating” treatments from lifestyle modification to injectable medication may contribute to the uptake. When asked about the food restriction, Mr. Doustdar said that approximately 2.4 million people have been prescribed with Rybelsus, and there was no evidence in the market that the food restriction hinders the uptake. He also added that we do not know what orforglipron’s label will look like. According to clinical trial protocols, participants taking statins were directed to wait two to four hours before taking orforglipron, for instance. On this comment, Lilly’s CEO Mr. David Ricks said in his symposium that the protocol was largely due to the timing of clinical development – Lilly had simply not conducted drug interaction studies with statins when initiating the clinical trial.
- On injectable GLP-1 RAs, Mr. Doustdar outlined Novo Nordisk’s plan to reframe the injectable obesity market, emphasizing that the company’s priority is to “change the current market perception” by demonstrating that semaglutide can reliably deliver >20% weight loss when appropriately dosed. He noted that the upcoming 7.2 mg semaglutide dose is designed to match or exceed the efficacy of newer competitors and argued that the current narrative – treating Lilly’s higher‑dose agents as inherently “next‑generation” and semaglutide as an older, less potent molecule – is fundamentally imbalanced. Mr. Doustdar stressed that this perception is driven almost entirely by dose, not by underlying biology, and that once the company brings the 7.2 mg dose to market, the comparison will become more balanced as semaglutide demonstrates equivalent 20% weight loss in the phase 3b STEP UP trial (n=1,407), along with its already‑proven cardiovascular, liver, and renal benefits, which competitors have not yet matched in outcomes data or labeling. He framed this as a necessary correction to a market that has overemphasized weight loss percentages while undervaluing semaglutide’s broader clinical profile.
- On the clinical pipeline, Mr. Doustdar highlighted CagriSema (fixed-dose cagrilintide and semaglutide) and amycretin as important late-stage assets. Based on results from the REDEFINE 1 trial, where CagriSema demonstrated 20% weight loss, compared to a reduction of 11.5% with cagrilintide 2.4 mg, 14.9% with semaglutide 2.4 mg, and 3.0% with placebo, the company submitted an NDA to the FDA in December 2025. The company is preparing for late‑stage development and multiple indication expansions. He also emphasized the standalone potential of cagrilintide monotherapy, which is now in phase 3 and aimed at patients who prioritize tolerability over maximal weight loss. Meanwhile, amycretin, a dual GLP‑1/GIP agonist, is advancing toward phase 3 based on positive phase 2 results and represents a key component of Novo Nordisk’s strategy to deliver both higher efficacy and improved GI tolerability.
- On M&A, Novo Nordisk’s acquisition of Akero was framed as a strategic extension of the company’s obesity‑anchored pipeline, given that ~80% of MASLD/MASH patients also have obesity. He emphasized that while semaglutide performs well in F2 and F3 fibrosis, Akero’s FGF21 program could address patients who no longer benefit from GLP‑1 RA therapy and currently face liver transplant as their only option. Mr. Doustdar described the deal as a way to pair Novo Nordisk’s metabolic platform with a complementary mechanism to serve a broader segment of MASLD/ MASH patients.
Pfizer: Dr. Albert Bourla shares vision of obesity treatment landscape with Metsera’s assets and reflects on MFN and tariffs
In this standing room-only symposium, Pfizer Chairman and CEO Dr. Albert Bourla discussed the company’s visions, key milestones, and growth strategies across metabolic health, immunology, cancer, and more. Dr. Bourla began by reflecting on 2024 and 2025, when Pfizer cut operating expenses by $5.6 billion. Noting that the company beat earnings for consecutive quarters, he emphasized Pfizer’s strong performance and business execution. He also highlighted several uncertainties that the company faced in 2025: (i) tariffs, which Pfizer has mitigated effectively via the Most Favored Nation deal; (ii) normalization after significant drop in COVID-19-related revenue; and (iii) acquisition of Metsera to strengthen its obesity pipeline. Entering 2026, Pfizer aims prioritize maximizing the value of recent acquisitions (including Metsera), delivering critical R&D milestones, investing for post-2028 growth, and implementing AI across R&D, manufacturing, and operations. Key catalysts for 2026 include delivering data readouts for phase 2b VESPER trial of ultra-long-acting GLP-1 RA (MET-097i, now named PF’3944) and phase 1/2 trial of the combination of PF’3944 and amylin agonist (MET-233i, now named PF’3945). Impressively, it will also launch ten phase 3 pivotal studies for PF’3944.
- Dr. Bourla placed a significant focus on Pfizer’s “controversial acquisition” of Metsera. As a reminder, in September 2025, Pfizer agreed to acquire Metsera for up to $7.3 billion. However, bidding war set off when Novo Nordisk submitting an unsolicited ~$9 billion acquisition offer on October 30. After several days of public discourse and legal action, Pfizer ultimately acquired Metsera with an amended $10 billion offer. Metsera’s pipeline included: (i) once-monthly GLP-1 RA MET-097i; (ii) once-monthly amylin analog MET-233i; and (iii) oral GLP-1 RAs MET-097o and MET-224o, among other candidates.
- Within five weeks of closing of acquisition, Pfizer and Metsera have efficiently integrated and is advancing the candidates. In fact, Pfizer had launched the first phase 3 trial in December 2025, earlier than when Metsera had originally planned in 2026. Dr. Bourla shared that additional data has further increased Pfizer’s confidence in the candidates. Specifically, he believes that once-monthly candidates have the best-in-class potential with favorable tolerability profile. He also expressed excitement about the benefits of combination therapies, such as amylin agonist with GLP-1 RAs or Metsera’s candidates with an oral small molecule GLP-1 RA licensed from China-based YaoPharma in December 2025.
- Looking forward, Pfizer will launch ten phase 3 obesity trials this year and target commercial launch in 2028 – preferably, management said, in early 2028.
- On the broader obesity market, Dr. Bourla commented that the market size is underestimated, as cash-pay channel constitutes ~30% of the market. He further added that obesity market has similar growth potential to that of Viagra years ago.
- When asked about Most Favored Nation (MFN) pricing deal, Dr. Bourla shared that Pfizer views the negotiations as manageable and positive, albeit a bold move. He further explained that MFN deal only affects eight high-income countries outside the US, while the other hundred countries remain unaffected. One of the countries, the UK, has already signed the deal with the US government to significantly increase its spending on innovative medicines, suggesting that countries are adjusting to the policy changes. Pfizer is now in dialogue with other countries like France and Germany. Dr. Bourla noted that these countries acknowledge that they are behind with innovative medicine compared to China and the US and that, with the new system, “products won’t be launched” unless they are paid for.
Regeneron: CEO Dr. Leonard Schleifer and CSO Dr. George Yancopoulos emphasize internal R&D engine, Eylea HD momentum, and obesity strategy
Regeneron CEO Dr. Leonard Schleifer and CSO Dr. George Yancopoulos described the company’s internally driven innovation model, underscoring the company’s commitment to “following the science” and investing in platforms that deliver long-term value to shareholders (see webcast and presentation slides). The session centered on two areas with significant relevance to diabetes and obesity: cardiometabolic disease and retinal health. Dr. Schleifer and Dr. Yancopoulos gave updates on the company’s GLP‑1/GIP and PCSK9 combination strategy and the accelerating uptake of Eylea HD.
- Dr. Yancopoulos highlighted obesity and cardiometabolic disease as major areas of expansion, focusing on the limitations of current GLP‑1 RA therapies and the opportunity to address obesity alongside hyperlipidemia. He emphasized that approved GLP‑1 RAs lower LDL cholesterol by less than 10%, leaving a substantial unmet need for people with obesity who also have elevated cardiovascular risk. To address this, Regeneron plans to combine its GLP‑1/GIP agonist, olatorepatide, with Praluent (PCSK9 inhibitor), aiming for >50% LDL‑C lowering in addition to weight loss. In China, phase 3 results for olatorepatide in obesity are expected in 1H26, with a global clinical development plan also beginning this year. Presentation slides also emphasized the company’s focus on enhancing the quality of weight loss with GLP-1 RAs, focusing on muscle preservation. The ongoing phase 2 COURAGE trial (n=1,005) showed that trevogrumab (anti‑GDF8/anti‑myostatin), with or without garetosmab (anti‑activin A), significantly preserves 50-80% of lean mass lost with semaglutide alone.
- In ophthalmology, Eylea HD (aflibercept 8 mg) was a major focus. In 4Q25, US net sales reached $506 million, up 66% from 4Q24 and up 18% sequentially. Dr. Schleifer attributed this momentum to a November 2025 label expansion, which added monthly dosing and an indication for macular edema following retinal vein occlusion. Prefilled syringe resubmission is under FDA review, with a decision expected in 2Q26. Dr. Schleifer reiterated the company’s goal of establishing Eylea HD as the preferred anti‑VEGF option across retinal diseases, including diabetic macular edema and diabetic retinopathy.
- During Q&A, Dr. Schleifer emphasized that these three enhancements (monthly dosing, the RVO indication, and the upcoming prefilled syringe) collectively support the rapid shift toward Eylea HD, which has grown from ~30% to ~50% of franchise sales over the past year. They also noted that payer coverage of monthly dosing removes a key barrier to initiating patients on Eylea HD, which they expect will further accelerate adoption.
Roche: Targeting a “top three” role in obesity through petrelintide, pegozafermin, and more; anti-VEGF Vabysmo returns to growth after market challenges
Roche Pharmaceuticals CEO Ms. Teresa Graham characterized Roche’s approach to cardiometabolic care as “delivering the next innovation cycle,” highlighting the company’s obesity portfolio in particular. Ms. Graham said that Roche is entering a new era of innovation in 2026, with early stages of the era taking root in 2025. Key priorities for 2026 include maximizing the current on-market portfolio, which is positioned to deliver growth through 2028, and delivering key launches including vamikibart, an anti-inflammatory antibody for retinal diseases. Roche also plans to prepare for its entry into the Alzheimer’s and obesity markets. Ms. Graham said that 60% of Roche’s R&D pipeline and total pharmaceutical sales involve a partnership, noting its partnership with Zealand on amylin agonist petrelintide and its recent acquisition of 89bio in particular. Roche is on track to achieve full year 2025 guidance, she said. In 2025, the company reported positive phase 3 results for 12 therapies, as well as 10 new molecular entities (NMEs) including pegozafermin, an FGF21 analog. There were no mentions of its diagnostic division, including BGMs and CGMs.
- Ms. Graham reiterated Roche’s commitment to being a top three player in obesity. Data on five NMEs that will enable phase 3 trials for the therapies are expected to be presented in 2026. Roche is focusing on six key areas in the management of obesity designed to address continual gaps in the therapeutic landscape: tolerability, suboptimal responses in up to 20% of patients, lean muscle loss, a ceiling effect on weight loss, weight maintenance challenges, and comorbidities. She named petrelintide, CT-388 (a dual GLP-1/GIP RA), CT-996 (a small molecule GLP-1 RA), pegozafermin, and emugrobart (a monoclonal antibody targeting myostatin) as key therapies in development for obesity. Ms. Graham said that Roche hopes to provide options for patients who prioritize different benefits of GLP-1 RAs, from those seeking moderate weight loss to high weight loss with good tolerability, as well as providing options for combination therapies.
- Roche has up to 19 NMEs with the potential for launch by 2030, including seven candidates in cardiovascular, renal & metabolic disease (CVRM). Ms. Graham said that these candidates provide the greatest potential and greatest level excitement for the company’s future. Roche is developing CT-388 for obesity with or without T2D, CT-868 for T1D with a BMI of 25 kg/m² or greater, petrelintide for obesity with or without T2D, zilbesiran for hypertension, pegozafermin for MASH, and emugrobart for obesity, spinal muscular atrophy, and facioscapulohumeral muscular dystrophy (see figure below). During Q&A, Ms. Graham again said that petrelintide, CT-388, and CT-996 are Roche’s most exciting candidates.
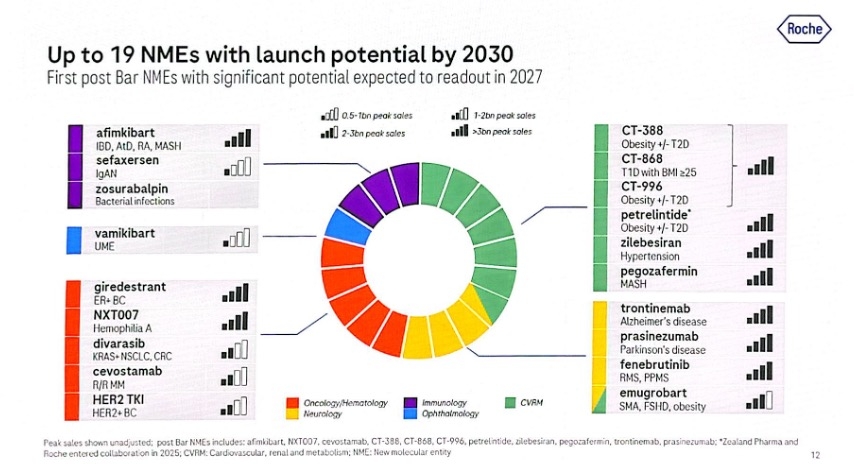
- In ocular health, discussion focused on Vabysmo (faricimab-svoa), the company’s franchise-leading anti-VEGF injection for wet AMD, DME, and RVO. Ms. Graham said that the therapy has had continued strong global growth following challenges in 2025. Recall that in 3Q25, the company revised its global full-year growth guidance for Vabysmo to 15% from 20%, reflecting the approximately 15% contraction of the US branded intravitreal therapy market seen so far in 2025. Roche said that reduced availability of co-pay foundation support has been the primary driver of this decline. Today, Ms. Graham said that the market has leveled and that Vabysmo will now return to accelerating growth.
Sana Biotechnology: Continuing strides for allogeneic islet cell therapy with developed with hypoimmune technology in people with T1D
Dr. Steve Harr (Sana Biotechnology President and CEO) took the stage this morning to present Sana Biotechnology’s vision and progress in the T1D space. Reflecting on 2025, Dr. Harr said the company has made significant strides, including developments across clinical and regulatory conversations for a T1D cure. He emphasized the significant unmet need in people with T1D, who face an immense burden and experience high risks of complications from diabetes. He said, “We can do better.” While islet cell transplantation has been positioned as a promising advancement in the T1D landscape, the procedure requires immunosuppression. To address such challenges, Sana Biotechnology continues advancing UP421, an allogeneic islet cell therapy engineered with the company’s hypoimmune technology. Dr. Harr emphasized that one of the primary distinguishing features of this approach is the elimination of the need for immunosuppression. Throughout the presentation and Q&A, Dr. Harr expressed strong anticipation for the upcoming IND submission for phase 1 trials later this year, as well as insights into the study design.
- Challenges of T1D cure. Dr. Harr said that among the many barriers to developing T1D cures, some of the key challenges include: (i) addressing allogeneic immune rejection without immunosuppression; (ii) developing a “master cell bank” to develop functional beta cells; (iii) manufacturing scale and consistency; and (iv) ensuring purity and potency. Sana Biotechnology has developed UP421 as a single solution that addresses these challenges, and therefore, Dr. Harr affirmed its potential to help the millions of people living with T1D.
- Positive six-month results from the first-in-human study of UP421 transplantation showed efficacy. Building on positive preclinical results, in June 2025, six-month results in one patient showed that UP421 transplantation exhibited a favorable safety profile. Additionally, C-peptide levels and a mixed meal tolerance test showed function and persistence of pancreatic islets. Dr. Harr stated that the patient continues to exhibit detectable C-peptide levels, indicating cell function, one year post-transplantation.
- Dr. Harr affirms Sana Biotechnology’s goal of developing a scalable therapy. While six-month results from the first-in-human study of UP421 represent promising data, Dr. Harr said the company aims to pursue a bigger goal: to develop a scalable treatment. By engineering a universal donor from a single stem cell, the company will apply gene modifications and deliver the therapy as a single treatment.
- Sana Biotechnology’s engagement in several conversations with regulatory bodies. Dr. Harr shared that the company has been in dialogue with multiple regulators worldwide. The FDA has remained “very engaged,” given its understanding of the significant unmet needs in T1D. The regulators have also acknowledged the transformative potential of UP421, especially based on the first-in-human study, and understand the complexity across immunology and stem biology. Across multiple conversations, Dr. Harr said the FDA has been supporting the company in navigating with clear expectations.
- Insights into the phase 1 trial of UP421 transplantation. Dr. Harr said that the phase 1 trial plans to encompass a broad population, starting with adults and later expanding to those at higher risk of comorbidities (e.g., CVD) and younger populations. The trial plans to be conducted in the US and other geographies. Dr. Harr expressed confidence that the phase 1 trial will be straightforward, showing efficacy within just a few weeks of the study.
SAB Bio: Mr. Samuel Reich on differentiating features of SAB-142 as a disease modifying therapy for T1D
In this morning session, CEO Mr. Samuel Reich highlighted updates on SAB-142, a disease-modifying therapy for T1D currently evaluated in a phase 2b SAFEGUARD study (n=159). Mr. Reich began by characterizing T1D as a multi-billion market opportunity, with 64,000 new patients diagnosed with stage 3 T1D each year. Even with insulin treatment, T1D is a serious, chronic burden, underscoring the need for more medications that can address the underlying causes of the disease rather than the symptoms alone.
- SAB-142 is a human anti-thymocyte immunoglobulin (hATG), with potential to be best-in-class disease-modifying therapy for delaying T1D onset and progression. It is produced via SAB Bio’s Tc Bovine platform, in which genetically engineered cows are designed to generate human antibodies upon being immunized with target disease antigens. SAB-142’s mechanism of action is analogous to rabbit ATG (rATG), which targets multiple immune cells like T-lymphocytes involved in destroying pancreatic beta cells. For example, in START, TN-19, and MELD-ATG studies, rATG was associated with beta cell preservation and improved C-peptide and A1c. Moreover, as a fully human molecule, SAB-142 has low or no immunogenicity. This allows SAB-142 to have better safety profile (e.g., no serum sickness) and to be re-dosed safely, which is critical for a chronic disease like T1D.
- Indeed, a phase 1 study (n=68) confirmed that SAB-142 is not immunogenic, leads to sustained T-cell exhaustion, and can be re-dosed twice each year. Notably, Mr. Reich pointed that repeat dosing of SAB-142 led to the same levels of T-cell exhaustion, followed by full recovery, suggesting the efficacy remains consistent.
- Mr. Reich further listed differentiating factors of SAB-142 from other treatments like Sanofi’s Tzield and Thymoglobulin (rATG). See figure below for the full comparison. In addition to the lack of serum sickness, he pointed to regulatory T cell preservation (which reduces autoimmunity). The dosing regimen of two days in outpatient setting is also more manageable than 12-day regimen for Tzield. Finally, the ability to re-dose also allows sustained beta cell preservation over the course of a chronic disease.
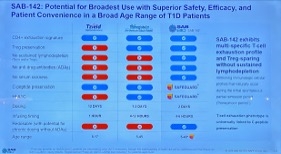
- Currently, SAB-142 is evaluated in a registrational phase 2b SAFEGUARD study (n=159) for pediatric, adolescent, and adult patients (ages 5-40 years) with new onset stage 3 T1D (diagnosed within 100 days, baseline C-peptide ≥200 pmol/L). The primary endpoint will be C-peptide level, and secondary endpoints include A1c, CGM metrics, insulin use, and safety. The trial is currently enrolling participants at multiple centers worldwide, including the US, EU, UK, Australia, and New Zealand – with the first participant dosed in December 2025. Looking forward, SAB Bio aims to complete enrollment of the SAFEGUARD study by the end of 2026 and deliver topline data in 2H27. Currently, the company has cash and cash equivalents of $144 million as of December 31, 2025, with projected runway through 2028. SAB Bio will also evaluate the efficacy of SAB-142 in: (i) stage 3 T1D maintenance; (ii) delaying the onset of stage 3 T1D in people with stage 2 T1D; and (iii) maintenance for those who underwent islet cell transplantation. Beyond T1D, SAB Bio plans to test the drug for other autoimmune diseases, like celiac disease, scleroderma, polymyositis, and dermatomyositis.
Sanofi: Strategies and progress across mid- to late-stage development projects; teplizumab receives approval in the EU for stage 2 T1D
CEO Mr. Paul Hudson, EVP of R&D Dr. Houman Ashrafian, and CFO Mr. François-Xavier Roger discussed Sanofi’s strategic progress throughout 2025, including key mid- and late-stage development projects – see webcast and presentation slides here. With active portfolio management, capital allocation, and the launch of new treatments, Mr. Hudson said 2025 was “an extremely busy” year. Sanofi has generated 8.7% growth in sales through 3Q25, and the company expects double-digit growth continuing into the next decade. Looking forward to the new year, management emphasized confidence in continued profitable growth, with several updates on mid- and late-stage developments across immunology, rare diseases, oncology, neurology, and vaccines.
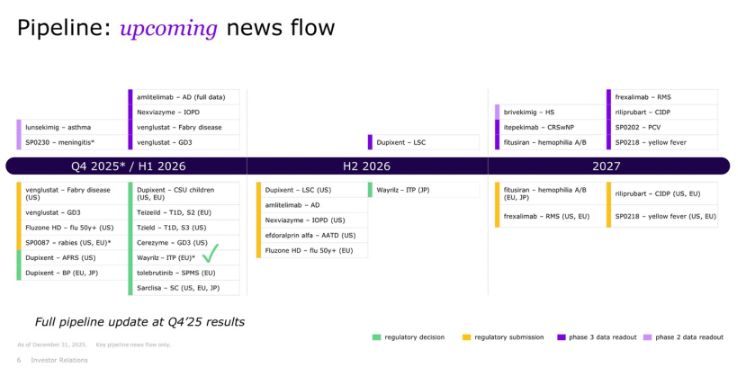
- New indications and breakthrough therapies. While management mentioned several treatments the company focuses on, they didn’t highlight teplizumab during today’s meeting. Nevertheless, teplizumab continues to make strides in the field, with today’s announcement that the treatment has been approved in the EU to delay the onset of stage 3 T1D in adult and pediatric patients eight years and older with stage 2 T1D. This announcement follows the positive opinion granted by the European Medicines Agency’s Committee for Medicinal Products for Human Use in November 2025 under the brand name Teizeild – of note, teplizumab received FDA approval in the US in November 2022 under the brand name Tzield. The press release states that Sanofi has decided not to progress with a second application of teplizumab in recently diagnosed stage 3 T1D in the EU at the moment, with next steps under evaluation. Beyond the US and EU, teplizumab is approved in the UK, China, Canada, Israel, the Kingdom of Saudi Arabia, the United Arab Emirates, and Kuwait.
- Sanofi’s response to tariffs and the administration’s new policies. Mr. Hudson commented on Sanofi’s agreement with the US government, announced in December 2025, to increase the accessibility of treatments by ensuring state Medicaid programs can distribute Sanofi’s treatments at the same prices available to other high-income countries. This decision reduces treatment prices by an average of 61% for select therapies for diabetes, CVD, neurological conditions, and cancer. Sanofi also agreed to offer products through TrumpRx and other direct-to-patient platforms at an average cost reduction of nearly 70%. With this agreement, Sanofi has secured a three-year tariff-free period on products it imports. Mr. Hudson said these decisions will help Sanofi make a further impact in the field and reach greater patient populations – he stated that the 2026 guidance will reflect these outlooks.
- Additionally, regarding policy changes, management responded to a question about the major changes issued this monthregarding the government’s recommendation for vaccinating children. Mr. Hudson explained that more than 50,000 newborns get admitted to the ICU every year, and encouragingly, Sanofi’s vaccines have helped dramatically decrease the numbers by 80-90%. He said it’s clear that the administration has “sensitivity around vaccination policies” and wants to give parents a choice. Yet, Mr. Hudson said there’s a “delicate line” because not everyone is informed about the importance of vaccination, or the consequences of not receiving it, creating significant variability. Therefore, he encouraged the audience that Sanofi will continue “staying objective,” presenting evidence to demonstrate efficacy.
Vertex: Journavx (suzetrigine) shows strong growth in the pain sector with potential indication for diabetic peripheral neuropathy
Dr. Reshma Kewalramani (Vertex CEO) took the stage to present Vertex’s differentiated strategy to continue delivering in three established disease areas (cystic fibrosis, heme, and acute pain), with emerging potential in renal health and more to follow. Dr. Kewalramani emphasized that Vertex only pursues diseases that have high unmet needs and develops targeted treatments. With this focus, the company has seen significant growth from established and emerging diseases, including: (i) cystic fibrosis, which continues to expand market leadership with expectations to sustain such position for many years to come; (ii) Casgevy (exagamglogene autotemcel), which is well positioned to become a “blockbuster medicine”; (iii) povetacicept (dual antagonist of the BAFF and APRIL cytokines), which holds the potential for best in class treatment for renal health; and (iv) Journavx (suzetrigine), which builds on the momentum of its first year launch to grow in prescriptions and revenue. In addition to these key sectors, Dr. Kewalramani stated that the company aims to serve patients across 10+ disease areas, each with a multi-billion-dollar market potential. She reinforced Vertex’s commitment to diversifying geographic presence and revenue base to increase the number of patients the company can support.
- Progress of Journavx. Journavx is a twice-daily, oral, selective non-opioid NaV1.8 inhibitor FDA-approved in January 2025 for moderate-to-severe acute pain. From March 2025, when Journavx became available at pharmacies, to now, Journavx has >200 million covered lives with all three national PBMs contracted and approximately 900 hospitals with treatment access. Additionally, >30,000 prescribers have used Journavx across a broad range of specialties, and >500,000 prescriptions have been distributed to patients.
- Future outlook for Journavx. Looking forward to 2026, Dr. Kewalramani hopes to expand the number of covered lives and hospitals that use the treatment. Furthermore, she expects to double the field team to drive HCPs’ adoption and depth and triple the number of prescriptions from 2025. Dr. Kewalramani affirmed that Vertex is building a durable and long-term franchise in pain treatments, seeking a strong leadership position similar to its significant presence in cystic fibrosis. Some long-term goals of Journavx include: (i) transforming the standard of care and shifting the treatment paradigm away from opioid use; (ii) ensuring patients have an informed and positive journey; and (iii) accompanying patients with access and reimbursement.
- Journavx to penetrate other areas of pain. Dr. Kewalramani reminded Vertex’s pursuit of Journavx for other pain indications, including diabetic peripheral neuropathy (DPN). The first phase 3 trial (n=1,100) of Journavx for DPN was launched in 3Q24, and today, Dr. Kewalramani announced that the second phase 3 DPN trial has also been launched – this timeline aligns with management’s announcement in its 3Q25 call that the study would launch in November 2025. As previously shared, enrollment for both phase 3 trials of suzetrigine is expected by the end of 2026, with results available in 2027.
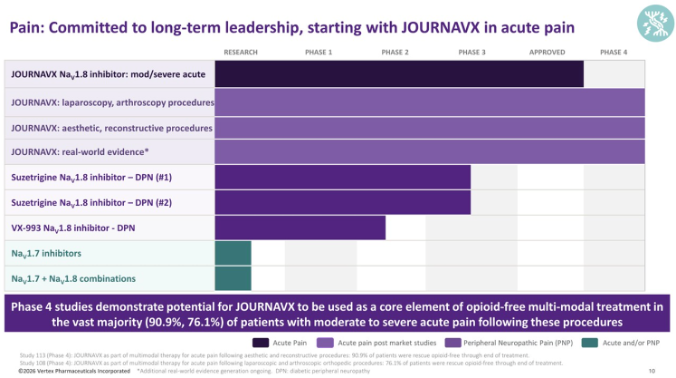
Viking: Dr. Brian Lian highlights oral and injectable VK2735 (dual GLP-1/GIP RA) and amylin agonist for obesity
In an afternoon session, CEO Dr. Brian Lian highlighted multiple clinical programs in development for obesity and other metabolic disease. Viking’s pipeline includes several promising candidates, including injectable and oral VK2375, which are progressing with impressive data.
- Injectable VK2375 (dual GLP-1/GLP RA) for obesity. Dr. Lian described VK2735 as a dual GLP-1/GIP agonist with a pharmacokinetics profile that enables potent, durable weight loss and supports the potential for weekly and monthly dosing. In the phase 2 VENTURE trial (n=4,650) – published today in Obesity – VK2735 conferred up to 14.7% weight loss at 13 weeks with ~90% of treatment effect maintained four weeks after stopping treatment. GI adverse events (AEs) were mostly mild/moderate and concentrated at first exposure and at titration steps. This AE profile inspired Viking’s “start low, go slow” titration mantra that Dr. Lian repeated throughout the session. Two phase 3 VANQUISH trials for stepwise titration up to 17.5 mg and 52-week maintenance are in progress: (i) VANQUISH-1 (n=4,500) for obesity is fully enrolled; and (ii) VANQUISH-2 for obesity and T2D is on track for primary readout in 2027.
- Oral VK2735 (dual GLP-1/GLP RA) for obesity. In phase 1 (n=92), oral VK2735 (the same GLP-1/GIP molecule as the injectable formula) conferred up to 8.2% weight loss and an “excellent” tolerability profile after 28 days of treatment at the highest dose. Treatment effects were largely maintained through Day 57 (roughly 4 weeks after last dose). In the phase 2 VENTURE-Oral trial (n=280), VK2735 demonstrated dose-dependent weight loss up to 12% at the 120 mg dose with no plateau. Durability analyses and a 90 mg titrated to 30 mg “maintenance” arm support most weight loss being maintained after stopped or lowering the dose. Furthermore, continued modest loss was observed at low doses. Dr. Lian shared Viking will focus on the ~20 mg to ~75 mg range, with lower starting doses and slower titration to optimize the GI profile, once again, following the “start low, go slow” approach.
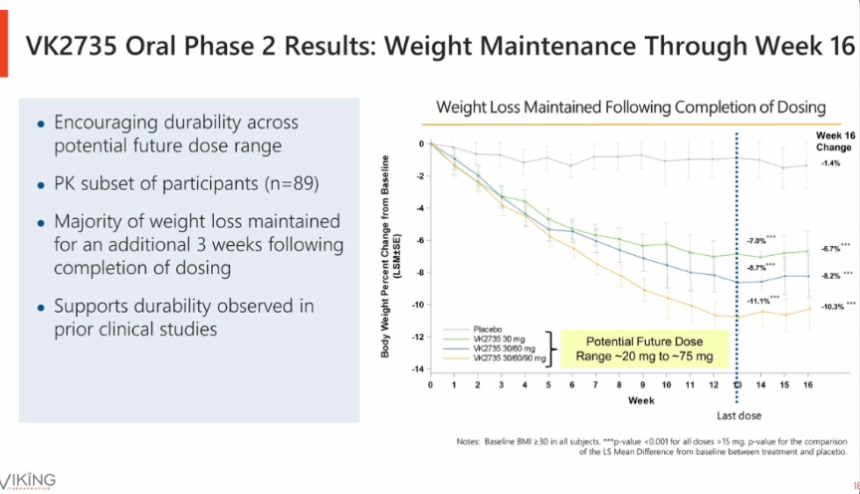
- Injectable and oral VK2735 for weight maintenance. Viking completed enrollment in a dedicated maintenance study for VK2375. The trial will start patients on injectable VK2735. After 19 weekly doses, patients will be randomized to monthly injectable VK2735, every-other-week injectable VK2735, an oral VK2735 regimen (daily or weekly), or a placebo arm. The goal of the trial is to show that after substantial weight loss with injectable VK2735, a lower dose of injectable or oral dosing can maintain weight loss with fewer side effects.
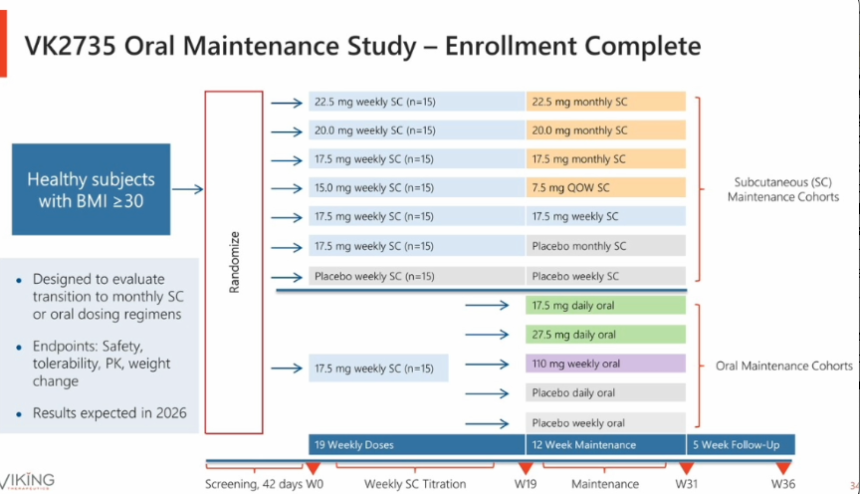
- Amylin agonist for obesity. While not covered in Viking’s prepared presentation, Dr. Lian offered insights into the amylin agonist for obesity during Q&A. Specifically, he noted than an IND filing for a single ascending dose (SAD) trial followed by a 28-day multiple ascending dose (MAD) is planned for 1Q26. Moreover, citing promising preclinical data, Dr. Lian shared that the amylin agonist could act as a standalone therapy, particularly for patients with a lower starting BMI. The company also plans to investigate a combination therapy of amylin analog and a GLP-1-based weight loss therapy like VK2735.
- VK2809 (THR-ß agonist for MASH). While VK2809 delivered a successful phase 2b readout in 2024, Viking does not intend to advance the candidate internally. The therapy is available for out-licensing, and Dr. Lian shared that there is external interest in this candidate.
Zealand Pharma: Dr. Adam Steensberg highlights survodutide and petrelintide; clinical data expected in 2026
In this afternoon session, Zealand CEO Dr. Adam Steensberg presented insights on the obesity market and updates on Zealand’s pipeline of survodutide (dual glucagon/GLP-1 RA) and petrelintide (long-acting amylin analog). He first highlighted Zealand’s capability to compete in the obesity market, including its differentiated pipeline, partnerships with Roche and Boehringer Ingelheim (BI), and robust cash position of $2.5 billion. Moreover, through internal R&D and external partnerships, Zealand plans to bring over 10 clinical programs by 2030. See below for the milestones for 2026:
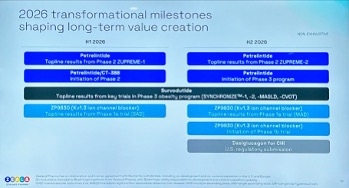
- Dr. Steensberg then delved into the current state of obesity treatments. First, he said that market penetration and maintenance can be expanded, given that 12% of eligible people in the US have been exposed and only ~3% are treated with GLP-1 RAs. Moreover, he pointed to the discrepancy in weight loss efficacy between real world and clinical trials. Although Wegovy and Zepbound conferred 15% and 21% weight loss in STEP-1 and SURMOUNT-1 trials, patients in real-world settings achieved 7.7% and 12.4% weight loss on average, respectively. Dr. Steensberg attributed this difference to: (i) gastrointestinal adverse events intrinsic to GLP-1 RA class; and (ii) different weight loss goals for patients. He emphasized that the field should step back from the “Weight loss Olympics” and understand what the actual medical needs of patients are. According to a survey (n=819) from LifeSci Capital, only about 16% of responders wanted to lose over 20% of their weight. Ultimately, noting that hypertension, dyslipidemia, and T2D each have over eight drug classes, he said that more drug classes are needed for obesity management.
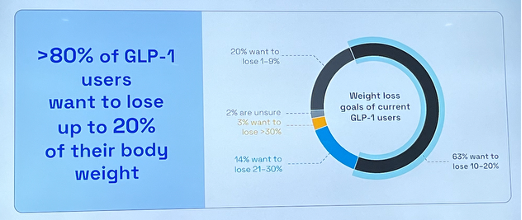
- On petrelintide, he reiterated that the candidate has the best-in-class potential. In a phase 1b trial (n=48), petrelintide conferred weight loss of up to 8.6% (vs. 1.7% with placebo), with only one adverse event-related treatment discontinuation. Results of the ZUPREME-1 trial (n=494) for people with overweight or obesity are expected in 1Q26. Dr. Steensberg said that the ZUPREME-1 trial has a balanced gender distribution (53% vs. 21% female) and higher BMI at baseline (37 vs. 30 kg/m2) compared to the phase 1b trial and is hopeful that the results will be more reflective of the drug’s profile.
- In phase 3 development, Zealand plans to initiate the therapy’s phase 3a program in 2H26. The company will also conduct phase 3b trials to better characterize its effects on cardiovascular (CV) health and other comorbidities. Dr. Steensberg said petrelintide has the potential to confer weight loss of 15-20% and CV risk reduction with less frequent GI events.
- On Zealand’s partnership with Roche, Dr. Steensberg characterized it as an equal collaboration, including 50/50 profit sharing in the US and Europe.
- On survodutide, Dr. Steensberg said that regulatory submissions are expected in 2026 based on the phase 3 SYNCRONIZE program – this was great to hear. While he believes the drug may be beneficial in multiple cardiometabolic indications, survodutide has especially demonstrated a best-in-class potential in MASH. In a phase 2 trial, 65% of participants with MASH (vs. 26% on placebo) experienced an improvement in liver fibrosis without the worsening of MASH at Week 48. The phase 3 LIVERAGE program is advancing at full speed for people with MASH and F2-F3 fibrosis or cirrhosis.
- During Q&A, Dr. Steensberg shared that while oral GLP-1 RAs will expand the market and improve manufacturing, they do not resolve the fundamental challenge of GLP-1 RAs: their tolerability profile. He expects that the market will continue to have residual disappointment until novel agents with improved patient experience enter the market. When asked about potential GLP-1 RA and amylin agonist combination therapy that could achieve weight loss >20%, Dr. Steensberg maintained his position that the greater unmet need is the lack of alternatives rather than higher weight loss efficacy. He believes that amylin monotherapy could be used for a broader population who seek improved adherence and maintenance therapy, while combination therapy could target a smaller segment of patients with morbid obesity and/or advanced T2D who are looking for 25-30% weight loss.
Diabetes Technology Highlights
Dexcom: Preliminary full-year 2025 revenue of $4.66 billion (+16%) and 4Q25 revenue of $1.26 billion (+13%); global userbase grows over 25% to 3.5 million
Ahead of CEO Mr. Jake Leach’s presentation at JPM this morning, Dexcom announced a total preliminary, unaudited full-year 2025 revenue of $4.66 billion, up 16% from 2024. Revenue came in slightly above the high end of Dexcom’s 2025 guidance of $4.63-$4.65 billion (updated in 3Q25). The company also reported preliminary, unaudited 4Q25 revenue of at least $1.26 billion, up 13% from 4Q24 and 4% sequentially. 4Q25 US revenue is expected to be approximately $892 million, up 11% from 4Q24 and 5% sequentially, while international revenue is expected to be $368 million, up 18% from 4Q24 and 3% sequentially. Mr. Leach also announced that Dexcom’s global CGM userbase now exceeds 3.5 million people, up over 20% from 2.8-2.9 million users at the end of 2024.
- Mr. Leach reviewed several key product and platform updates for Dexcom in 2025. He highlighted the FDA clearance and December 2025 launch of the G7 15 Day CGM for adults with diabetes as a major milestone. He described the launch as “extremely successful,” with the product now available across both DME and pharmacy channels. G7 15 Day is already integrated with Insulet’s Omnipod 5 and Beta Bionics’ iLet, and he said Tandem integration “will come very soon.” Among users who have switched, 91% reported the system is as easy or easier to use than their prior CGM.
- Dexcom also received FDA clearance for Smart Basal, designed to help basal-only insulin users reach optimal dosing in about one month and improve adherence – an area Mr. Leach described as one of Dexcom’s fastest-growing segments.
- Dexcom Direct EHR integration continues to progress, with more than 160 healthcare systems live or onboarding.
- Mr. Leach highlighted significant US coverage expansion in 2025, noting that Dexcom announced in 2Q25 that the three largest PBMs now cover CGM for all people with diabetes. The company estimates that more than nine million people currently have CGM reimbursement but are not yet using the technology. He also pointed to potential Medicare coverage expansion for people with T2D not using insulin, saying Dexcom is “on the cusp” of progress driven by strong clinical data. Mr. Leach previewed 12-month real-world data from Dexcom’s T2D non-insulin registry showing sustained improvements in A1c, weight, and BMI, building on previously shared six-month results and demonstrating benefits across age groups and medication regimens. In addition, Dexcom’s randomized controlled trial in T2D non-insulin users is expected to read out in 1H26, supporting broader global coverage expansion.
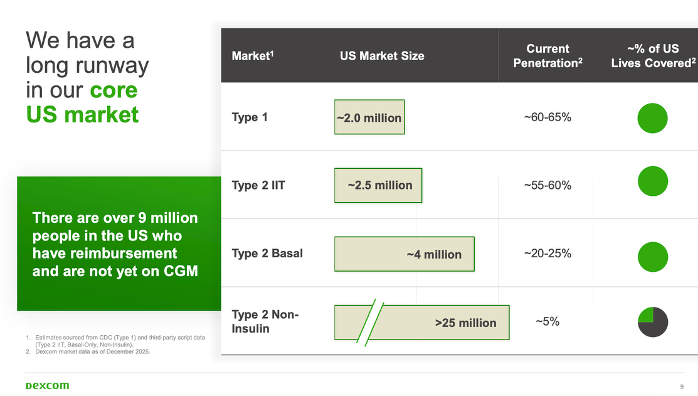
- Gestational diabetes (GDM): Mr. Leach said Dexcom has already established “good coverage” for CGM use in GDM and argued that CGM should be standard of care given strong outcomes, including reductions in C-sections, preterm births, large-for-gestational-age infants, and NICU admissions.
- Inpatient care: He noted that more than 14 million dysglycemic events occur annually in US hospitals, underscoring the need for improved inpatient glucose monitoring.
- Prediabetes: Mr. Leach said CGM can enable earlier diagnosis of prediabetes, prompting behavioral changes that reduce the risk of progression to T2D.
- Dexcom reported record new patient starts in full-year 2025 and described 4Q25 as a “too-close-to-call” race for another record quarter. Mr. Leach said 4Q25 starts were strong, noting that some patients had been delaying initiation while waiting for the G7 15 Day. While he did not provide a regional breakdown, he cited strong sell-through and use patterns in both the US and international markets.
- Mr. Leach expressed confidence in Dexcom’s 2026 financial outlook. The company issued full-year 2026 revenue guidance of $5.16-$5.25 billion, implying 11-13% growth compared to 2025. Mr. Sayer said growth will be driven by increasing CGM adoption across all diabetes populations, the continued rollout of Stelo, and further international coverage expansion. Guidance assumes strong, near-record new patient additions, high patient retention, and a largely unchanged global CGM coverage landscape. Stelo is expected to contribute “nominally.”
- Dexcom also expects a non-GAAP gross margin of 63-64% and a non-GAAP operating margin of 22-23%. Gross margin expansion is projected to be driven in part by momentum from improved manufacturing efficiency in 2H25 and uptake of the G7 15 Day. He also expects operating margin expansion despite incremental investments, including hiring and spending for Dexcom’s new Ireland manufacturing facility (see more below). In response to JP Morgan’s Mr. Robbie Marcus deeming Dexcom’s margin guidance “conservative” in Q&A, Mr. Leach cited flexibility from the G7 15 Day transition and the time required to migrate its current installed base as rationale for Dexcom’s guidance. Dexcom expects to generate more than $1 billion of free cash flow in 2026, with incremental operating expenses allocated to R&D (including software and Dexcom G8), promoting manufacturing efficiency, and expanded global sales and marketing efforts.
- Mr. Leach emphasized international expansion as one of Dexcom’s top growth priorities. He noted that Japan and France now cover CGM for all insulin users, Canada has expanded access for people with T2D, and Dexcom expects additional wins across Western Europe and Australia for insulin-using T2D patients. However, he noted that Dexcom’s guidance does not anticipate major coverage unlocks in 2026, though the company continues to work toward broader global access. Addressing affordability in markets without insurance coverage, Mr. Leach acknowledged varying price sensitivity and said Dexcom aims to keep out-of-pocket costs as low as possible. He added that Dexcom plans to introduce Stelo into international over-the-counter (OTC) markets in 2026, noting that cash-pay access can accelerate eventual reimbursement, as seen previously in Eastern Europe with Dexcom ONE. As international mix increases, he added traditional revenue seasonality may evolve; for example, he said that if Dexcom’s sequential revenue decline from 4Q to 1Q has already evolved from the mid-teens to the low double digits, we could expect to see another one-point improvement to this dynamic in 1Q26.
- Stelo adoption accelerated in 2025 following its late-2024 launch. Dexcom reported $130 million in full-year 2025 Stelo revenue, with more than 500,000 users and a “strong majority share” of the OTC CGM market. Mr. Leach highlighted Stelo’s availability on Amazon and noted that many users have signed up for product subscriptions. Product enhancements continue, including the launch of Dexcom’s AI-based meal-logging feature on Stelo in July 2025 (expanding a previous G7-only feature) that has already seen more than 10 million meals logged to date. Dexcom is also developing more advanced meal-logging tools with macronutrient tracking to better contextualize CGM trends.
- Mr. Leach discussed Dexcom’s hardware pipeline featuring the next-generation Dexcom G8 sensor, which will feature even better accuracy, 50% smaller form factor, and advanced sensing capabilities and error detection. He said Dexcom will also use product as gateway to expand into the additional clinical areas of GDM, inpatient care, and prediabetes. He also announced that Dexcom will introduce new product in its Dexcom ONE+ category.
- Mr. Leach also offered commentary on Dexcom’s pipeline and manufacturing plans. He discussed Dexcom’s next-generation G8 sensor, which is expected to offer improved accuracy, a 50% smaller form factor, and advanced sensing and error-detection capabilities. He said Dexcom will also use product as gateway to expand into GDM, inpatient care, and prediabetes. He also announced that Dexcom will introduce a new product in its international Dexcom ONE+ category in 2026. Finally, Dexcom continues to make progress on its Ireland manufacturing facility, which is expected to come online in 4Q26, alongside broader supply-chain investments to improve resilience and strengthen quality systems.
embecta: GLP-1 RAs offer >$100 million annual opportunity; “market-appropriate” products for China and other geographies
Mr. Dev Kurdikar, CEO of embecta, expressed confidence in the long-term stability of the needle and pen needle market and showcased the company’s durable, recurring revenue base despite potential shifts driven by increased adoption of insulin pumps and GLP-1 RAs in the US. Pen needle revenue has remained stable (approximately +0.6% CAGR) and safety pen needles have grown (+4.9% CAGR). While syringe needle revenue has declined (-4.5% CAGR), it represents a smaller portion of the portfolio (~15%).
- As he shared on prior earnings calls, Mr. Kurdikar reiterated that GLP-1 RAs could represent a more than $100 million annual revenue opportunity for embecta by 2033. Much of this opportunity stems from generic GLP-1 RAs, which are typically delivered in pens co-packaged with pen needles. Generic manufacturers are seeking to replicate the packaging of branded products such as Ozempic, creating a natural B2B opportunity for embecta. More than one-third of embecta’s potential generic partners (over 30 companies) are either in contract negotiations or have executed agreements with it already, with some already having placed purchase orders. These partners anticipate launches in Canada, Brazil, China, and India beginning in 2026, with developed markets in Europe and the US coming as soon as 2031-2032. While branded GLP-1 RAs are not currently co-packaged with pen needles, embecta has developed combination packs and is in active discussions with branded pharmaceutical companies. embecta does not see a role in GLP-1 RA autoinjectors.
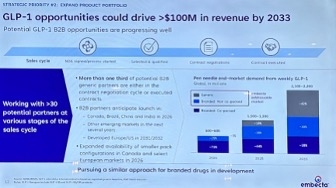
- Mr. Kurdikar also addressed embecta’s operations in China, which (together with Hong Kong and Taiwan) accounts for ~10% of total revenue. embecta distributes through three national distributors in China, but shifting geopolitical dynamics in 2025 drove increased preference for local Chinese brands, along with heightened price competition. In response, embecta introduced products at more competitive price points to better match local market dynamics. While stabilization is expected to take several quarters, management remains confident in China’s long-term importance.
- He also discussed embecta’s strategy to develop additional “market-appropriate” pen needles and syringes for other price-sensitive regions. The company previously exited certain tender-driven markets, such as parts of Latin America, rather than significantly discount its “premium products.” It is now preparing to reenter these markets with cost-optimized offerings better aligned with local needs. embecta has completed design for these products, installed their manufacturing equipment, and is currently validating production lines, with launches expected in the near to medium term in markets where its current share is <5%. These products are intended to drive incremental volume, leveraging embecta’s historical familiarity with these markets.
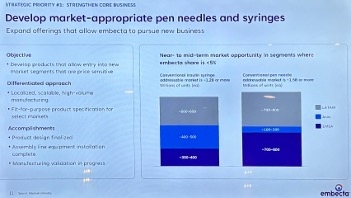
- Looking ahead, Mr. Kurdikar framed 2025-2028 as a period focused on strengthening embecta’s core business, expanding the product portfolio, and building financial flexibility. He cited the discontinuation of the company’s patch pump program last year due to capital allocation priorities and the elimination of nearly $185 million in debt during 2025 as representative of this last point. He also highlighted the completion of embecta’s brand transition in the US and Canada, featuring refreshed packaging and the replacement of the “BD” name with “embecta” to deepen engagement with customers and healthcare providers. This rebranding effort is underway globally and is expected to be completed in most markets by calendar year 2026, with a small number of Asian markets to follow. From 2028 onward, embecta aims to evolve into “a broad-based medical supplies company” serving both chronic care patients and drug delivery partners.
Insulet: President and CEO Ms. Ashley McEvoy highlights growth opportunity across US T1D, US T2D, and OUS T1D; robust innovation pipeline through 2028
Following a successful Investor Day in November 2025, Insulet CEO Ms. Ashley McEvoy emphasized Insulet’s strong business model and three-year innovation plan. She highlighted several advantages that underscore Insulet’s position in the AID competitive landscape that have enabled Insulet to drive ~66% of total AID market growth from 2020-2025, with share expanding from <30% in 2020 to ~50% in 2025. Revenue has grown at a ~25% CAGR since 2021, driven by strong new patient starts, and Insulet became cash-flow positive in 2023 and has accelerated since, reinforcing its ability to fund growth and innovation. While additional entrants to the ecosystem may emerge, Ms. McEvoy said that Omnipod 5 remains “in a class by itself.”
- Ms. McEvoy outlined a coordinated strategy across US T1D, OUS T1D, and US T2D to drive the next leg of growth, highlighting the under-penetration seen across all three populations.
- US T1D ($9B+ total addressable market): AID penetration is ~40%, roughly 30 percentage points below estimated CGM penetration (~70%). Insulet aims to increase penetration to above 50% by 2028 by: (i) driving demand generation in line with evolving clinical guidelines to move more patients from MDI to AID; (ii) strengthening commercial execution to add new prescribers; and (iii) delivering excellent user experience through continued innovation.
- OUS T1D ($10B+ total addressable market): AID penetration remains only ~25% of an estimated four million potential patients, ~40 percentage points below CGM penetration (~65%). Roughly 80% of this opportunity in Insulet’s geographies resides in Europe, with the remainder in Canada, Australia, and the Middle East. Insulet targets 30-35% penetration by 2028 and plans to launch Omnipod 5 in six additional markets in 2026 (Spain and five Middle Eastern countries), bringing the total number of Omnipod 5 markets to 20 by year-end. Ms. McEvoy also reiterated Insulet’s plans to accelerate growth in existing OUS geographies.
- US T2D basal-bolus ($12B+ total addressable market): AID penetration is estimated to be <5%, more than 50 percentage points below CGM penetration (~55%). Insulet aims to more than double penetration to 10-15% by 2028 by positioning Omnipod 5 as standard of care. Specifically, Ms. McEvoy cited the 2026 ADA Standards of Care, which now identify AID as preferred therapy for people with T2D who are currently using MDI, insulin pumps, or sensor-augmented pump therapy. Insulet received FDA clearance for Omnipod 5 use by adults with T2D in August 2024. Prior to the clearance, over half of the company’s direct-to-consumer (DTC) leads had been individuals with T2D, and over 25% of new US user starts in the quarter of the clearance (3Q24) had T2D – this increased to 35% just one year later, in 3Q25. Since then, Omnipod 5 has been joined by Tandem Control-IQ+ and MiniMed 780G with US T2D indications.
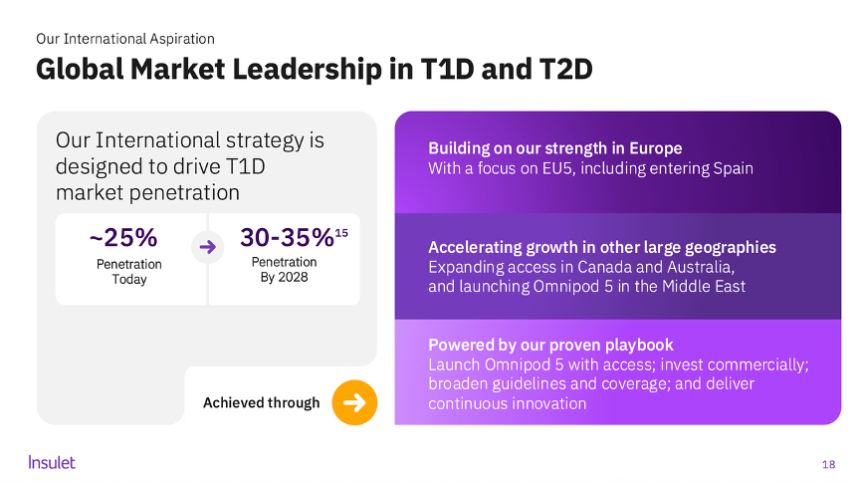
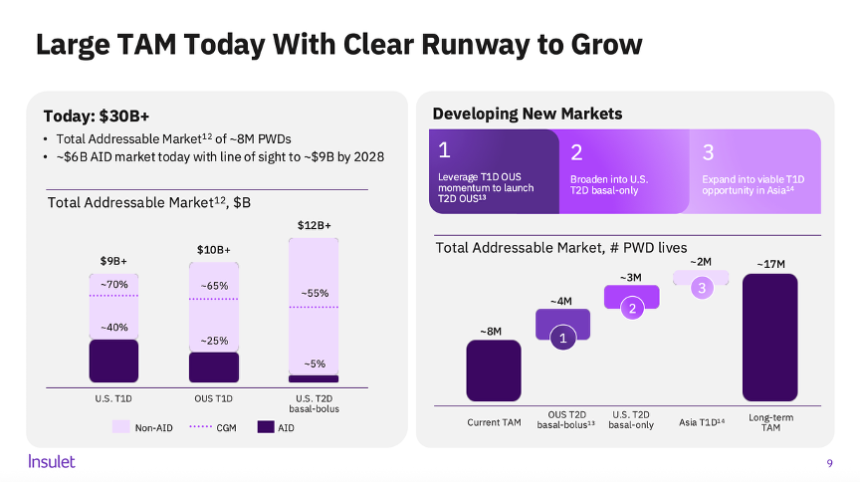
- Ms. McEvoy also highlighted Insulet’s innovation pipeline, with more than $1 billion planned investment in technology over the next three years. This includes the hardware and software innovation noted below, as well as the STRIVE and EVOLUTION clinical studies and development of broader real-world evidence with Omnipod 5. She noted that diabetes distress remains widespread and most insulin users do not currently benefit from AID, underscoring a significant gap in care that Insulet hopes to address through differentiated technologies.
- Insulet plans to launch several highly requested updates in 2026, including: (i) a 100 mg/dL glucose target (in 1H26) alongside increased time in automated mode and improved algorithm responsiveness; (ii) integration with all major CGM sensors; and (iii) the launch of Omnipod Discover to streamline onboarding and office workflows. Insulet expects the algorithm improvements to improve Omnipod 5’s competitive strength among patients and providers seeking even better glycemic management, and the launch of Omnipod Discover to improve action on the insights CGM and AID unlocks, enabling greater optimization of care plans.
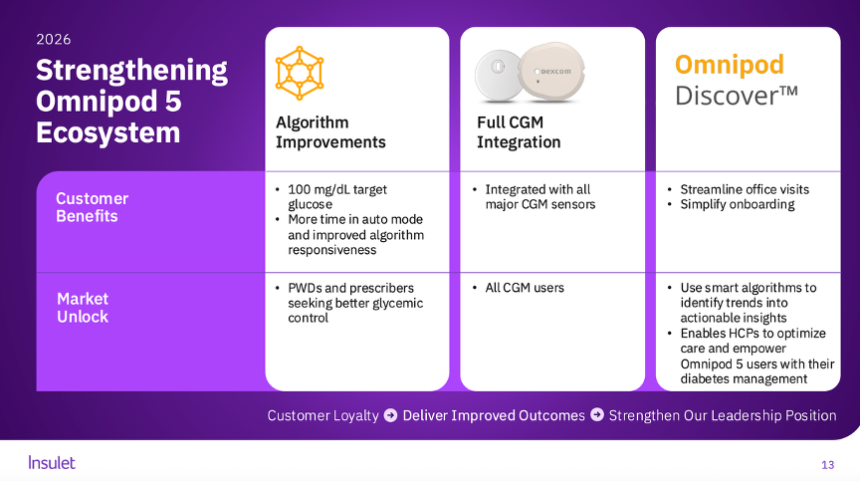
- Insulet plans to launch Omnipod 6 in 2027. Omnipod 6 is Insulet’s next-generation AID system, featuring improved connectivity and more personalized automation. The STRIVE trial is now complete, with results to be presented at ADA 2026. Insulet is also planning for a 510(k) submission of Omnipod 6 in 2026. Ms. McEvoy explained that Omnipod 6 will be an over-the-air-updatable pod, enabling a shift from multiple sensor-specific stock keeping units (SKUs) to one master SKU compatible with all sensors. This will enable direct integration updates to Pods already manufactured, eliminating channel stocking dynamics and will allow users to receive innovations six to nine months faster than they do today, as well as simplifying manufacturing and prescribing practices.
- Insulet plans to launch its fully closed-loop (FCL) AID system for people with T2D in the US in 2028.With ~70% of T2D patients managed in primary care settings and ~75% of insulin-treated patients not meeting recommended glycemic targets, the FCL system is designed to enable broader PCP adoption of AID and, over time, expansion into the larger basal insulin market. Ms. McEvoy emphasized the system as designed for self-start – as it is “ready out-of-the-box” – and for ease of prescription by providers, with no settings to start. She described this as a “game-changing” opportunity to lower the burden of managing T2D.
- Beyond 2028, Insulet plans to bring FCL technology to people with T1D.
- Ms. McEvoy briefly addressed manufacturing and commercial strength, reiterating that Insulet is constructing another manufacturing facility (in Costa Rica, scheduled to come on-line in 2029 – we hope it will have pods that last longer and hold much more insulin in their reservoirs) and continues to produce “tens of millions” of pods annually at scale. Insulet is also working to construct additional lines in Malaysia and improve automation in Acton, Massachusetts.
- She also noted that the company has the highest AID brand awareness among MDI users, and that ~70% of patients who request a specific AID system ask for Omnipod – leading her to characterize Insulet as a “gateway” to the AID ecosystem. Yep, yep it sure is, particularly given how easy it is to use! We loved hearing that Insulet now calls on an even higher number of prescribers, and what now sounds like well over 20,000 (up ~25% in 3Q25). Boy, do we hope those prescribers look at all their patients, particularly those with T1D who aren’t yet on pumps – MDI is so much more challenging to manage than Omnipod 5 or any other continuous insulin delivery.
- Looking ahead, Insulet projects ~20% revenue CAGR in constant currency between 2025-2028, largely driven by increasing penetration of its addressable markets across T1D and T2D, US and international. Insulet also expects approximately 100 basis points annual operating margin expansion between 2025-2028 with “modest” gross margin improvement, driven by its investment in innovation and optimized selling, general, and administrative expenses.
- Finally, brand new CFO Ms. Flavia Pease addressed investor questions following the company’s 3Q25earnings call, saying that Insulet will continue to provide guidance it has a high degree of confidence in achieving and that reflects a balanced outlook. She emphasized that recent concerns about deceleration from peers reflect noise rather than Insulet’s business fundamentals and encouraged investors to focus on the underlying strength and durability of the business.
Medtronic: With Diabetes business spinoff expected by the end of 2026, management highlights four new generational growth platforms
Medtronic CEO Mr. Geoff Martha expressed enthusiasm about the growth trajectory across several of the company’s franchises. Commentary on the diabetes business was limited, as the unit remains on track to separate via IPO by the end of calendar year 2026. As previously disclosed, diabetes revenue totaled $2.8 billion in Medtronic’s fiscal year 2025 (+10%). He reiterated that while diabetes remains a strong business with attractive opportunities, Medtronic believes capital can generate higher returns when redeployed across other areas of the portfolio, supporting the rationale for the separation.
- While unmentioned in prepared remarks, Medtronic also announced today the FDA clearance of MiniMed Go Smart MDI sensor. The system integrates Medtronic’s InPen with the Abbott-partnered Instinct CGM; interoperability with the Simplera Sync CGM is still under review by the FDA.
- Medtronic CFO Mr. Thierry Piéton noted that R&D spending grew to 8.5% of revenue at the end of FY2Q26(3Q25), outpacing revenue growth, and the company has internally set a long-term target of approximately 10%. He added that diabetes currently represents an above-average R&D investment within the portfolio. Medtronic applies a three-tiered prioritization framework for R&D investment:
- Generational growth platforms such as cardiac ablation and Hugo RAS;
- High-growth businesses including neuromodulation and structural heart; and
- Large, established franchises that generate significant profit and sustain Medtronic’s leadership (e.g., next-generation CRM). Funding decisions are “rack-and-stacked” based on expected return on investment.
- Medtronic established two new management committees in 2Q25 to optimize operations and drive growth.Mr. Martha noted that while the Operations Committee is charged with focusing on margin expansion and execution under the Medtronic Performance System – which he called a driver of improved commercial, operational, and financial rigor – the most significant addition has been the Growth Committee, which is tasked with actively pursuing tuck-in M&A opportunities aligned with Medtronic’s core franchises and long-term portfolio strategy. Mr. Piéton also described itself as “on offense” for strategic M&A, with a focus on tuck-in acquisitions that complement internal innovation.
Omada Health: Preliminary full-year 2025 revenue of ~$257 million (+52%); 2026 will see investment in GLP-1 RA Care Track and AI tools
Omada Health announced preliminary, unaudited 4Q25 results on the first day of JPM 2026. The company reported approximately $257 million in 2025 revenue, up 52% from 2024. Preliminary 4Q25 revenue is expected to be $72-$74 million, up 50-54% from 4Q24 and 6-9% sequentially. Omada also reported an adjusted gross margin of 66.4% and today, CEO Mr. Sean Duffy reiterated the company’s commitment to reaching 70%. Notably, Omada shared that nearly half of new deals closed were multi-program rather than single-program sales, a trend the company continues to see in its most recent deals. Omada now serves approximately 2,000 customers across employers, health plans, and integrated health systems, covering 886,000 members, up 55% from 2024. Beyond what Mr. Duffy described as the “two G’s of great growth” reflected in Omada’s 4Q25 performance, he also discussed the company’s focus on an additional “two G’s”: GLP-1s and GPTs.
- Mr. Duffy reiterated Omada’s mission to “bend the curve” of chronic disease. The company began with prevention and weight health and has since expanded into diabetes, hypertension, and musculoskeletal care, reflecting the high prevalence of comorbidities (e.g., 74% of people with diabetes also have hypertension). Omada’s programs integrate connected devices – including cell-connected weight scales, blood pressure monitors, and CGMs – with in-app goal setting, clinical visits, community engagement, and progress tracking. More than 20 million people now have benefits coverage for at least one Omada program. As of December 2024, 55% of members maintained at least monthly engagement one year into the program, declining modestly to 50% at two years. Omada has published more than 30 peer-reviewed studies demonstrating clinical and economic outcomes and continues to focus on securing accreditations, including National Committee for Quality Assurance (NCQA) accreditation for diabetes and hypertension population health.
- Mr. Duffy spoke extensively about Omada’s GLP-1 RA Care Track, describing GLP-1 RAs as “a moment to seize.” He positioned the offering as a “GLP-1 RA maximizer,” designed to enhance weight loss during therapy and minimize weight regain after discontinuation. For example, Omada reported internal data showing 28% greater weight loss among participants using its Enhanced GLP-1 RA Care Track and just 0.8% weight regain one year after stopping therapy, compared with 11-12% weight regain observed in studies such as SURMOUNT-4 (Zepbound) and STEP-1 (Wegovy). He noted that Omada recently began prescribing GLP-1 RAs and expects an increasingly complex landscape with the introduction of oral therapies and additional single- and dual-agonist therapies.
- Addressing the potential impact of oral GLP-1 RAs, Mr. Duffy said that more therapeutic options typically drive greater utilization and emphasized Omada’s ability to help identify which patient profiles are best suited for oral versus injectable therapies. Management also pushed back on the notion that lower-priced oral GLP-1 RAs would diminish Omada’s relevance, emphasizing that employer goals center on the additive benefits of Omada’s tools. Omada Health President Mr. Wei-Li Shao also explained that their entrance into prescribing GLP-1 RAs was driven by employers and health plan customers wishing their members did not experience a gap between therapy initiation and Omada’s digital support system. When asked about future prescribing, he indicated Omada would consider additional medications for other chronic conditions over time.
- On the technology front, Mr. Duffy highlighted its growing use of AI under the OmadaSpark umbrella, including a nutritional intelligence agent that is increasingly being used by members today.
- Looking ahead, Omada plans to expand its addressable market in covered lives, improve enrollment by converting eligible individuals into active members, and drive stronger retention and engagement, supported by continued product innovation.
Teva Pharmaceuticals: Teva to shift from generics firm to global biopharmaceutical company
CEO Mr. Richard Francis highlighted Teva’s “Pivot to Growth” strategy and the company’s long-term vision to open the second day of JPM. Mr. Francis shared that the strategy launched three years ago with an aim to move Teva from a global generics company into a biopharmaceutical company, following years of consecutive revenue declines.
- The “Pivot to Growth” strategy is built on four pillars: (i) delivering on already established pharmaceutical growth engines; (ii) improving innovation and its late-stage pipeline; (iii) creating a sustainable “generics powerhouse”; and (iv) disciplined capital allocation to the highest-return assets. He elaborated that the strategy would take place over three distinct phases:
- A return to growth. Evident in 11 consecutive quarters of growth since early 2023;
- Acceleration of growth. The company’s current strategic phase which focuses on rapidly growing innovative medicines revenue and leveraging its existing pipeline; and
- Maintaining growth. Management shared its ultimate goal of a 20-year plan to sustain a “world-leading” biopharmaceutical company with durable growth and improving returns.
- Mr. Francis emphasized that the company’s financials “prove” its portfolio transformation. Teva has moved from quarters of consistently declining revenue to consistently growing revenue, largely driven by its innovative business. Teva’s innovative business, Mr. Francis continued, has roughly doubled every two years. Moreover, Teva “broadly speaking” aims to keep doubling its innovative revenue in the future – targeting over $10 billion in peak sales from its portfolio.
- Mr. Francis deliberately waited until later in his presentation to discuss Teva’s generics business, framing the delay as evidence of how far Teva has shifted its business towards innovation. Teva currently has 10 biosimilars already on the market, with six additional biosimilar launches expected before 2027. Mr. Francis shared that the company’s goal is to build a portfolio of roughly 20-30 biosimilars globally, using active partnership deals to accelerate entry into separate, key molecules. Notably, biosimilars (highly similar copies of brand-name drugs) were framed by management as a higher-value, more complex segment of the generics (chemically identical copies of brand-name drugs) business that more closely aligns with Teva’s “complex generics” and biopharma capabilities.
- Teva’s generic of Novo Nordisk’s Saxenda (liraglutide) for obesity was not explicitly mentioned during prepared remarks or the Q&A. We found this hugely disappointing and slightly worrying. As background, Teva received FDA approval and subsequently launched its generic version of Saxenda for obesity in August 2025, which followed the company’s 2024 approval of Novo Nordisk’s Victoza (liraglutide) generic for T2D. Teva’s generic GLP-1 Saxenda is now indicated for weight loss in: (i) adults with obesity with at least one weight‑related comorbidity; and (ii) adolescents aged 12–17 years who weigh over 60 kg (~132 lbs). The approval marked Teva’s fifth first-to-market entry of 2025, consistent with its Pivot to Growth strategy. We have purchased the Victoza pen, and without meaning to raise any alarm, for us, it has not worked as well as the traditional OG pen did. In the last pen Kelly used (which she only got very recently), there was a strange ball of wax in the pen that looked quite odd.
Verily: Progress on Verily Pre for clinical research facilitation and Verily Me for telehealth
CEO Mr. Stephen Gillett shared updates on Verily’s recent progress and strategic direction. Verily, an approximately 10-year-old subsidiary of Alphabet, operates with physicians licensed to practice medicine in all 50 states. Although the company that owns it, Alphabet, said it is currently in a quiet period, so they couldn’t say much, we appreciated Mr. Gillett’s updates on the progress the company has made in recent months and focus for 2026. We remember a few years back at JPM, they had a much better time slot and easier-to-find room – this year, although it was rough that they were speaking at the very end of the day, this had its intended effect as many stayed around as as the room was fully jam-packed.
- Mr. Gillett overviewed Verily Me, the company’s consumer-facing telehealth platform that entered a beta launch in October 2025. Verily Me is a mobile app that prompts users to submit a photo of themselves and their driver’s license, after which the platform retrieves their medical records and routes them to a Verily clinician, who then offers personal recommendations on a health plan.
- He also discussed advancements in Verily Pre, the company’s data platform for healthcare research. Verily has established relationships with organizations like the CDC, Vanderbilt Health, and the NIH to host datasets that researchers must access through Verily (the NIH’s All of Us Research Program currently supports approximately 20,000 global researchers). Pre ingests diverse data types – including claims, genomics, and EHRs – and converts them into FHIR-based, health-grade data designed to be “AI-ready” for companies’ specific use cases. Pre enables researchers to significantly increase the speed at which research can be conducted, including 10x faster model training and 30x faster whole-genome analysis. Mr. Gillett cited a partnership with the University of Colorado using Pre to study acute myeloid leukemia, which achieved 95% accuracy and reduced researcher time by 97% – replicating and validating findings in a fraction of the usual time. Furthermore, Verily has entered into a partnership with Nvidia, which Mr. Gillett described as a “powerful ecosystem” for clinical research.
- Mr. Gillett said that Verily will launch “another nice set of updates” in 2026, including plans to publish research that it’s doing on its platforms. In 2026, Verily plans to: (i) expand tools for clinical researchers and for drug development with Verily Pre; (ii) launch new agents on Verily Pre and the Verily Me app; and (iii) drive additional commercial opportunities and partnerships.
Virta Health: Tailwinds from GLP-1 RAs; combining the platform with pharmacotherapy for sustained weight loss and metabolic benefit
Virta Health CEO Mr. Sami Inkinen discussed the company’s outlook for the future, promising clinical data, and its goal of reversing metabolic disease in one billion people. Mr. Inkinen said that metabolic disease is a one-trillion-dollar problem and that modern disease management simply maintains the problem, not solves it. He said that 10+ related conditions including T2D, poor sleep, depression, high blood pressure, inflammation, musculoskeletal pain, obesity, fatty liver disease, cardiovascular disease, and kidney disease are all merely symptoms of an underlying cause: metabolic disease, which affects 93% of Americans. Virta uses individualized nutrition overseen by providers to address this problem, which is delivered by its care platform and tailored use of AI.
- Mr. Inkinen said that Virta’s platform outperforms pharmacotherapies with double the adherence of GLP-1 RAs. He presented a timeline of Virta’s outcomes evaluated in trials. In 2017, he said that Virta demonstrated the potential to reverse diabetes and eliminate the use of medications through the use of its platform. 62% of users had a reversal of T2D with 80% having a reduction to insulin usage. In 2018, Virta also demonstrated positive outcomes for the reversal of hypertension, leading to a 10-year reduction in cardiovascular disease risk of 12%. In 2020, participants in Virta’s clinical trial averaged 13% weight loss which was sustained without the use of pharmacotherapy.
- In 2024, Virta demonstrated is potential to serve as a GLP-1 RA “off-ramp” for sustained weight loss for those who cannot or prefer not to use GLP-1 RAs long term. For background, a 2022 extension of the STEP 1 trial found that participants regained one-third of their body weight one year after discontinuing the use of semaglutide 2.4 mg. Mr. Inkinen said that Virta has submitted a publication that is currently in review and expected to be published this year, if accepted. The work found that Virta’s platform reduced strokes and heart attacks (as assessed by three-point MACE) by 54%, approximately 1-2.5 times better than GLP-1 RAs. When assessing new onset of MACE-3, Virta found that incidence rates were 9.3 events per 1,000 person years in the control group, compared to 4.1 in Virta users. Mr. Inkinen also said that Virta’s platform reduced mortality by 50%. We look forward to further detail on this work including study size and duration.
- Mr. Inkinen devoted significant time to GLP-1 RAs and how they compare to Virta’s platform. He made it clear that Virta does not offer any form of medication through its platform but said that GLP-1 RAs and their popularity still serve as an incremental tail wind for Virta. Virta can help support weight management with GLP-1 RAs before, during, and after use of the therapies for the “best return on investment,” said Mr. Inkinen. When using Virta one year after discontinuing GLP-1 RAs, users maintained 12.1% body weight loss. Using Virta drug-free nutrition alone with no medication demonstrated 13% body weight loss over 12 months. Mr. Inkinen highlighted the cost effectiveness of this option compared to pharmacotherapy in particular. Through Virta’s unique approach to diet, the company copes to solve “the biggest health epidemic of our generation: metabolic disease.”
Ypsomed: CFO Mr. Samuel Künzli reviews product launches and global manufacturing expansion in 2025; one billion unit manufacturing capacity targeted for 2030
Ypsomed CFO Mr. Samuel Künzli helped close out JPM 2026 with a presentation outlining the company’s transition to a pure-play injection device business (spanning autoinjectors, pen injectors, and wearable large-volume injectors) and its outlook through fiscal year 2029/30. Mr. Künzli highlighted four trends underpinning Ypsomed’s growth: (i) therapies continuing to shift from hospital settings to the home; (ii) a broader move from oral to injectable treatments; (iii) expanding access to biosimilars, which is increasing device volumes; and (iv) the strength of the obesity and incretin markets, which predominantly rely on injectable delivery.
- Mr. Künzli also highlighted several notable product launches in 2025. Ypsomed introduced three new platforms – two pen injectors and one autoinjector – each incorporating eco-friendly plastics that reduce CO₂ emissions during production and feature designs that allow disassembly and recycling. Additionally, multiple partners launched therapies that rely on Ypsomed devices, including mazdutide in China using Ypsomed’s autoinjector, an Alzheimer’s therapy using YpsoMate 2.25 mL, and an autoimmune therapy in Japan. He reiterated the breadth and diversity of Ypsomed’s customer base, noting that no single customer (out of more than 130) accounts for more than 15% of sales, and that approximately 30 customers are incretin-focused. Overall, Ypsomed devices support more than 70 approved therapies across multiple therapeutic areas.
- The presentation also covered Ypsomed’s global manufacturing expansion. The company held a topping-out ceremony for its Schwerin 2 facility in October 2025, began production in Changzhou, China, in June 2025, and accelerated plans to expand into the US with a retrofitted facility in Holly Springs, expected to open in 4Q27. Collectively, these investments intend to support capacity of up to one billion devices annually by 2030. Mr. Künzli also reviewed Ypsomed’s CHF 1.5 billion multi-site investment program: the company invested CHF 200 million in fixed assets last fiscal year and expects to invest slightly more than CHF 250 million in the current fiscal year. Given construction timelines and ramp-up periods, full use of a manufacturing facility typically occurs roughly five years after initial investment. Approximately CHF 400 million of the total investment will be co-financed by pharmaceutical partners.
- Finally, Mr. Künzli reviewed Ypsomed’s financial performance and outlook. The company delivered a 24% revenue compound annual growth rate (CAGR) over the past five fiscal years, reaching approximately CHF 500 million, and expects to grow around 20% to roughly CHF 600 million in FY25/26. Diabetes has been a key growth driver, and UnoPen and the YpsoMate 1 mL and 2.25 mL autoinjectors have contributed most significantly. In the last fiscal year, approximately 20% of revenue came from project revenue, with the remainder from commercial sales. Ypsomed typically operates under long-term customer contracts of around 10 years, aligned with the lifecycle of launched drugs.
- While the company expects negative cash flow through FY27/28, Mr. Künzli emphasized that Ypsomed can finance its obligations through its own balance sheet. By FY29/30, commercial sales expected to grow at a ~20% CAGR, while the more “volatile” project business is expected to remain stable or grow modestly. He also reiterated that Ypsomed has exited contract manufacturing for pens and plans to phase out remaining contract manufacturing related to the Diabetes Care business sold to TecMed in 2025 over the next three to five years.
Diabetes Big Picture Highlights
JPM’s Jeremy Meilman welcomes over 9,000 attendees, reflecting on four decades of global health industry
In a crowded Grand Ballroom, Mr. Jeremy Meilman (Global Co-Head of Healthcare Investment Banking, JP Morgan) delivered welcoming remarks. He began by reflecting on the long history of holding JPM Healthcare Conference in San Francisco and how much the health industry has expanded over those decades. In 1983, when JPM first convened at the same Westin St. Francis hotel, only 21 companies, with an aggregated market cap of $4 billion, participated with fewer than 100 attendees. This year, JPM brought together 525 companies, whose collective market cap sums to over $9.9 trillion, for over 9,000 registered attendees. The US market has changed significantly over the years, as well. The Center of Medicare and Medicaid Services’ (CMS) annual spending in the same time period increased from $355 billion to $5.9 trillion, while federal funds rate decreased from 9.9% to 3.6%.
- Mr. Meilman said that strong momentum of growth is carrying through 2026. Since COVID-19, healthcare industry sector has demonstrated robust performance, with the biotech sector becoming the strongest performing sector for the first time in 2025. 2H25 also marked a period with significant increases in M&A (+44% from 2024), with the number of $5 billion+ deals increasing from four in 2024 to 16 in 2025 – which includes Novo Nordisk’s $5.2 billion acquisition of Akero Therapeutics and Pfizer’s $10 billion acquisition of Metsera. This momentum is continuing this year, Mr. Meilman said, as the past week was the busiest first week of January in decades for equity issuance.
- On the key trends for healthcare sectors in 2026, Mr. Meilman highlighted the uncertainty of policy changes like tariffs and Most Favored Nation deals, the increasing role of AI, and robust M&A activity.
- Pharmaceuticals & Biotech sector faces significant uncertainty with regard to tariffs and Most Favored Nation policy, contributing to a slower start to the year. Partnership and M&A activities was robust in 2025, with total value for M&A being $101 billion, up over 3x from $33 billion in 2024. On the other hand, Initial Public Offering (IPO) volume decreased by half from 2024 to 2025, indicating higher standards expected for early-stage companies. He expects 2026 to be a stronger year for IPOs with high-quality biotech companies.
- Healthcare Services sector is focused on integrating AI technology and increasing security. Mr. Meilman predicts 2026 to be active with M&A.
- The MedTech sector has efficiently dealt with tariff challenges in 2025 and continues to mitigate the impact of geopolitics with China and supply chain. M&A activities, portfolio management and restructuring will remain robust.
- The Life Science Tools, Diagnostics, and Pharma Services sector is navigating changes with academic and government funding. The bioprocessing industry is rebounding.
San Francisco Mayor Mr. Daniel Lurie welcomes business, scientific, and medical leaders to San Francisco
For the lunchtime “opening,” San Francisco Mayor Mr. Daniel Lurie returned to welcome leaders to San Francisco and to introduce Mr. Dimon and Ms. Terry-Ann Burrell. We remembered vividly last year Mayor Lurie doing the same and it was terrific to see him again and to see what a difference a year makes! Mr. Lurie reflected on the changes to the city of San Francico that he has overseen in just one year, including improved public safety and economic recovery. He said that 28% of San Francisco residents believed the city was moving in the right direction one year ago, with this figure now standing at 62%! Crime is down 30% in one year and has been reduced by 40% in the city center. Getting specific, he said that car break-ins are at their lowest in 22 years. On a positive note, he said that there were with additional exciting activity in visitors to the city - hotel bookings in San Francisco related to scientific and other conferences have risen a whopping 62% in just one year! Mr. Lurie said he will continue to cultivate a direct line of communication to CEOs and small business owners and he thanked them profusely – as well as the giant group of leaders for continuing to bet on San Francisco!
Fireside Chat Fascinates: JPMorgan Chase CEO Mr. Jamie Dimon in conversation with Ms. Terry-Ann Burrell on geopolitics, the free market, leadership suggestions, and healthcare innovation
In an extremely packed lunchtime fireside chat (even the overflow rooms were very packed!), JPMorgan Chase CEO Mr. Jamie Dimon offered his perspective on global affairs and the role of corporations and healthcare organizations in this ecosystem.
- Mr. Dimon asserted that the US should continue to demonstrate strong military leadership in global affairs yet should not overuse the military. As the war in Ukraine enters its fifth year, with unrest growing in Iran, the broader Middle East, and Venezuela, Mr. Dimon said that the world is not a safe place and never will be. He said that the US’s military should be used to promote US interests overseas and ensure US safety. He lauded President Donald Trump for his military efforts including the deposition of Venezuelan president Nicolas Maduro and his indictment for narcoterrorism, although this operation has been considered illegal under international law, per the University of Cambridge and other sources. Despite promoting the use of the US military to secure key national security outcomes, Mr. Dimon said that approaches should not overuse the military and suggested that the US should not overstep other nations’ sovereignty only in certain cases. He called for the US to be more strategic in global affairs.
- On young voters questioning capitalism and the free market, Mr. Dimon said that corporations must think of national interests with their actions. He criticized corporate America for “fighting every tax policy” and for excessive political lobbying, which he said is part of the “political swamp” with which many voters are frustrated. He said that US K-12 education must be improved to better explain business and economic theory to the youth, so that they may make informed decisions about economic policy and not blame capitalism or socialism as a whole for their economic concerns. He said that things like the housing economy is “crippled” by rules and regulations mostly established by Democrats. Health and safety is widely considered to warrant regulation.
- Providing leadership suggestions, Mr. Dimon urged attendees to be involved, curious, and accept responsibility as leaders. He said that bad leaders continue to operate in the same way once they assume leadership, rather than changing their approach and growing over time. He said that leaders must earn their employees’ trust and respect, be factual and analytical, and must establish key deliverables for every meeting.
- The healthcare industry has exhibited tremendous growth since the first annual JP Morgan Healthcare conference. At this time, in 1983, Mr. Dimon said that both the healthcare industry and the number of investors were significantly smaller. Now, in 2025, 525 companies are in attendance at JPM, with over 10,000 investors. Since 1983, the industry has made incredible progress in cancer treatment, the invention of GLP-1 RAs, and much more, said Mr. Dimon. He believes that AI will further catalyze growth and be a powerful tool for drug discovery. “The US is not the best country in the world by health outcomes, but it is the country with the best medicines,” said Mr. Dimon. He hopes to inspire attendees to begin to change this paradigm through this conference and beyond.
*NEW* Mass General Brigham: Systemwide transformation and strategic expansion
Dr. Anne Klibanski, President and CEO of Mass General Brigham (MGB), provided an overview of the nonprofit health system. MGB is the largest private employer in Massachusetts, with nearly 85,000 employees, over 400,000 Mass General Brigham Health Plan members, and approximately $23 billion in annual system revenue. Its research enterprise totals $2.7 billion. MGB has established three disease-focused institutes, with nearly half of the system’s research investment being dedicated to its Cancer Institute, which includes an AI center focused on lung cancer screening. The Heart and Vascular Institute and the Neuroscience Institute represent additional strategic priorities, with Dr. Klibanski highlighting particularly strong growth opportunities in neuroscience. It is amazing to hear what has been done since the coming together of hospitals only a little over five years ago, in 2019!
- Dr. Klibanski highlighted meaningful clinical and operational improvements following MGB’s transition to being a high-reliability organization. The system estimates that approximately 1,800 additional lives were saved during the transition. The average length of stay declined 10% in 2025, while the number of patients waiting in emergency departments and medical/surgical units for behavioral health services fell 31%. A new single, systemwide transfer entry point now facilitates roughly 2,000 inpatient transfers per month, representing a 9% year-over-year increase.
- MGB launched a digital-first primary care model earlier this year to help address persistent primary care physician shortages. MGB also announced a new collaboration with Tampa General Hospital, beginning with a co-branded radiation oncology center and expected to expand over time. In parallel, the system continues to grow its ambulatory footprint, starting with endoscopy and infusion services, and expand into freestanding sites to improve access and affordability.
- Despite capacity constraints and inflationary pressures during the surge of the Omicron variant of COVID-19 in 2022, MGB reported strong recovery in 2023 and 2024, followed by acceleration in 2025. Performance was driven by expanded patient access and targeted cost reductions in non-patient-facing expenses. Several years ago, MGB launched the SUSTAIN initiative to promote resource stewardship across the system. The organization reported approximately 9% CAGR, significantly outpacing roughly 1% debt growth, and now has more than $10 billion in capital spending capacity over the next five fiscal years to deploy toward new strategic initiatives.
*NEW* Cleveland Clinic: Applying AI and delivering complex care at a global scale
Dr. Tomislav Mihaljevic (Cleveland Clinic CEO) described the organization as a global healthcare system with approximately 83,000 clinical caregivers operating across 280 outpatient locations worldwide. Cleveland Clinic has continued to expand its international footprint through new affiliations, including its most recent expansions in Vietnam and Uzbekistan. He also explained the system’s care model, which centers on delivering high-quality, complex care with a multidisciplinary approach.
- Dr. Mihaljevic highlighted continued investment across Cleveland Clinic’s physical and clinical infrastructure. On its main campus, the organization is advancing several major projects, including a new Neurological Institute building and Global Peak Performance Center for sports medicine. Cleveland Clinic is also planning the construction of a new hospital in West Palm Beach, and Cleveland Clinic London plans to expand into an adjacent building. This will allow the creation of a dedicated cancer center following its designation as the leading private hospital in the UK in 2025.
- Dr. Mihaljevic underscored Cleveland Clinic’s commitment to technology-enabled care delivery using AI and highlighted a collaboration with G42 and Oracle. This partnership is focused on applying AI to “redesign its healthcare delivery.” Current AI deployments include:
- Patient-facing applications: tools such as AI-enabled sepsis detection to improve early intervention and outcomes;
- Caregiver-facing solutions: AI scribes designed to reduce administrative burden and clinician burnout; and
- Organizational operations: use of Palantir software to optimize clinical operations and resource utilization.
- Mr. Dennis Laraway (Cleveland Clinic CFO) described Cleveland Clinic’s operating growth as “deliberate,”with approximately 11% organic growth driven by strong global demand for its services. He noted that many Cleveland Clinic hospitals operate at a capacity of more than 90% daily. Financial performance has now returned to pre-pandemic levels, with a strong recovery in margins. In 2025, the system generated approximately $18 billion in operating revenue, reflecting a very strong compound annual growth rate of nine percent.
*NEW* Mayo Clinic: Embedding AI across care, research, and operations
The Mayo Clinic’s Dr. Richard Gray (CEO, Mayo Clinic Arizona) discussed the health system’s deep commitment to AI as an enabler of more proactive, personal care. The Mayo Clinic currently has 155 AI applications in clinical use, with more than 300 additional applications under development. These tools are designed to improve outcomes, efficiency, and the overall care experience. Dr. Gray highlighted several examples already deployed in practice: (i) an AI model that predicts hospital-acquired infections, providing clinicians with 72-hour advanced warning to enable preventive intervention; (ii) a precision detection model for pancreatic cancer that can identify disease three months to three years earlier than current approaches; and (iii) AI-driven radiation treatment planning for head and neck cancer, which personalizes therapy while reducing clinician work effort by approximately 76%.
- Mayo Clinic is also applying AI to accelerate clinical research with synthetic control arms, which Dr. Gray said preserves scientific rigor while improving trial speed, cost efficiency, and patient access to active treatment.
- Likewise, Mayo Clinic is deploying AI to personalize the pace and sequencing of education and training, with a focus on upskilling its existing workforce. More than 20,000 staff members have completed AI training through the Harper Family Foundation AI Education in Medicine program.
- Dr. Gray described a roadmap for more customized digital patient interactions, including agentic AI systems that can perform tasks on patients’ behalf. Tools such as HealthLocator.org provide information on patient outcomes and safety across more than 5,000 US healthcare organizations, giving patients greater transparency and control over their health. Additional applications include virtual surgeon avatars to answer post-operative questions.
- Mayo Clinic is deploying digital tools to summarize outside medical records, digitally twin patients and care processes, and support real-time learning. Dr. Gray described this evolution as a shift “from a continuously learning organization to an auto-learning organization,” reducing the need for manual data analysis.
- Mayo Clinic also reported strong and sustained financial performance. Operating cash flow is approximately $2 billion annually, supported by strong philanthropy and long-term investment returns. Since the pandemic, the system has delivered consistent results, with a revenue CAGR of 9%, no negative growth quarters, and an operating margin of 6.1%. Mayo continues to invest heavily in technology, including AI, digital pathology, and information security modernization.
*NEW* Intermountain Health: AI and proactive care across the American West
Intermountain Health CEO Mr. Rob Allen highlighted the system’s strong operating performance and quality outcomes. Sixteen of Intermountain Health’s 34 hospitals are ranked as top performers, and the system sits at the 86th percentile nationally on Vizient quality measures.
- Mr. Allen outlined two core areas of focus:
- Simplifying care for caregivers, patients, and members. Intermountain Health continues to standardize operations through expanded Epic deployment across its clinics. While leadership initially expected tens of thousands of support tickets during rollout, the system designed and deployed an AI-enabled support tool that helped process more than 70,000 support tickets. Epic has since cited Intermountain Health’s approach as an example of best practice and plans to use the tool as a model for future implementations.
- Expanding proactive, value-based care. Intermountain Health is strengthening alignment across providers, operations, and its health plan to better manage population health. The system is also placing particular emphasis on rural care, with the goal of keeping patients closer to home whenever possible. Last year, Intermountain Health launched the Mindshare Institute to convene health system leaders to collaboratively solve industry challenges. More recently, in December, it announced the formation of Aeroterra Health, which aims to improve medical transportation nationwide.
- CFO Mr. Clay Ashdown said that Intermountain Health is making targeted infrastructure investmentsby assessing which community needs are growing most rapidly, determining where to expand capacity, and balancing the need for ambulatory versus inpatient growth. Later this year, the nonprofit plans to complete a roughly $1 billion bond offering alongside a restructuring of existing debt.
CMS comes to SF: Dr. Mehmet Oz and CMS leadership discuss GLP-1 RAs, long-term health, MFN, and MAHA
The second “keynote” of JPM 2026 featured an impassioned panel discussion from Centers for Medicare & Medicaid Services (CMS) leaders led by Mr. Dan Mendelson (CEO, Morgan Health). Dr. Mehmet Oz (CMS Administrator), Mr. Daniel Brillman (Deputy Administrator and Director), Ms. Stephanie Carlton (Deputy Administrator & Chief of Staff), Mr. Chris Klomp (Deputy Administrator & Director), and Ms. Amy Gleason (Strategic Advisor) discussed their approaches to improving long-term US health. To no one’s surprise, Mr. Mendelson asked extremely insightful questions on multiple policy fronts including Medicare and Medicaid spending, the specific role of GLP-1 RAs in America’s future, and into the Make America Healthy Again (MAHA) movement. In his opening and closing messages, Dr. Oz even characterized the panel as a “recruiting mission” for healthcare industry leaders to join CMS as it seeks institutional change, saying that the panelists were trying to convince attendees to leave their current roles to help fix a system that “all would agree is broken, but no one would ever leave in favor of care anywhere else.”
- GLP-1 RAs are a “wise investment” into long-term health that should be approached in a responsible way, said the panel leaders. Mr. Klomp said that GLP-1 RAs are the most popular drug class in the US, repeatedly emphasizing the cardiometabolic benefits of the therapies. He said that CMS’ recent decision under Most-Favored-Nation pricing to cover the therapeutic class for obesity, not solely for diabetes, is an effort to capitalize on cardiovascular disease prevention and prediabetes management. He said that CMS is particularly focused on improving overall health in the nation to reduce health system costs. With improved health comes improved productivity, he said, which will further stimulate the US economy.
- Technology and AI may offer opportunities to change healthcare infrastructure and revolutionize rural care. Ms. Gleason humorously described her journey from CES 2026, where she also represented CMS, to San Francisco, which included laundry-folding robots in the CES exhibit hall and self-driving Waymos. She contrasted this to the average experience of healthcare in the US involving clipboards and fax machines instead of digitization and automation. Ms. Gleason said that CMS hopes to empower patients to take better control of their health and to think of this as seeking a better consumer experience in the healthcare industry. In July 2025, CMS launched the Health Technology Ecosystem, which aims to regulate digital health records and make them accessible to patients and providers via a standardized QR code. Dr. Oz said that patients are smart and that the government and healthcare providers should meaningfully engage with them using technological advancements. He urged the audience to think, “What do we need to do together to fix your problem?”
- Mr. Brillman said that now is the time for rural communities to shine. He said that CMS is currently making large investments into rural healthcare with the help of individual states to fill gaps in rural care. He called for a data-first approach to rural medicine and said that seeking advice from industry experts, such as those in the room, will be essential for achieving these goals. As an example, Ms. Carlton discussed a virtual reality headset initiative that has been implemented in Nebraska to help train providers where in-person training is not as accessible.
- Far more will follow on this panel discussion – we’ve just begun to discuss what was most interesting! The passion of the leaders was what was most clear, outdone only by the very clear intelligence of all.
The FDA’s Dr. Marty Makary on optimized regulation, accelerating the 12-year approval timeline, and additives in our food supply
United States Commissioner of Food and Drugs Dr. Marty Makary gave a strong talk discussing the FDA’s balance between regulation and stimulating innovation. He spoke of the privilege that it is to lead the FDA and to address attendees at the conference today, saying that the US healthcare system is amazing. He highlighted proton beam radiotherapy, an advanced cancer treatment, gene therapies, and robotic surgery as just a few examples of the US’s incredible innovation in medicine. However, he said that the system often does incredible work for no credit. When evaluating the success of the system not by its innovation but rather by population health outcomes, Dr. Makary said that the system is at a fifty-year low. Rates of chronic diseases have sharply increased, and new treatments for diseases have not emerged fast enough to keep pace. “Why does it take 12 years for the FDA to bring drugs from invention to market?” he asked. His compelling talk laid out why 12 years is the current state of affairs and his efforts to change this statistic at the FDA.
- In 2026, the FDA will remove onerous requirements that do not result in safer medications, seeking a process that scrutinizes safety, when necessary, yet makes more medications available without prescriptions. He described the roadblocks to availability that many therapeutics face both before and after approval, with extensive trial requirements that do not result in more robust data and prescription requirements for therapies without strong risk factors. Dr. Makary said that the FDA will implement the use of Bayesian statistics to increase the statistical power of studies and streamline them, with one pivotal trial becoming the new standard, as opposed to two. The FDA will also work to eliminate unnecessary animal testing, which comes with animal cruelty concerns and can cause treatment delays. As it stands, each monoclonal antibody that is approved requires 144 chimpanzees to be tested – at a very high logistical and ethical cost.
- In June 2025, the FDA launched the Commissioner's National Priority Voucher (CNPV) Pilot Program, which will reduce drug and biological product application or efficacy supplement approval times for key therapies to 1-2 months from the current 10-12 months. In conjunction with Most-Favored-Nation pricing established by the White House in May 2025 to lower drug costs for Americans, the FDA seeks true therapeutic accessibility in both development and sales. “A 100% effective therapy that only 50% of people can afford is only 50% effective,” Dr. Makary said.
- Dr. Makary said that no patients should visit emergency rooms for prescription refills due to administrative lag and hopes to improve accessibility in all ways. Many patients find themselves unable to schedule timely appointments to receive prescription refills, forcing them to visit emergency rooms seeking medication, which adds further strain to the health system. Safe medications with no abuse potential and no need for continued laboratory work to monitor response should be available over the counter, said Dr. Makary, adding that the FDA must move away from a paternalistic mindset.
- The FDA plans to review over 1,000 chemicals found in the US food supply that have been banned in other nations. In April 2025, the FDA announced that petroleum-based synthetic dyes including Red No. 40 will be phased out of US foods by the end of 2026. Dr. Makary said that this decision had been in discussion for nearly 35 years yet had been thwarted by administrative hurdles. As part of the Make America Healthy Again (MAHA) movement, the FDA will review chemical additives to the US food supply and plans to eliminate the Generally Recognized As Safe (GRAS) loophole in 2026.The policy allows food manufacturers to declare new additives as safe without FDA review, which may lead to unknowingly harmful chemicals in the food supply.
- To achieve these initiatives, the FDA has begun hiring over 1,000 new scientists. Dr. Makary said that 450 of these scientists are currently being onboarded, and that recent layoffs at the FDA did not affect scientists and were focused on streamlining administrative roles. However, Skadden, Arps, Slate, Meagher & Flom LLP and Affiliates previously reported that scientists involved in the regulatory process were affected by these layoffs.
- “The trains are running on time, but the process needs to be reformed,” said Dr. Makary. He seeks deep, systemic change to the FDA’s processes to modernize and support the scientific community. Only then will we be able to deliver more treatments and healthier food for America’s children.
From agentic AI to longevity: ARPA-H’s strategy for breakthrough health innovation
Dr. Alicia Jackson, Director of ARPA-H (the Advanced Research Projects Agency for Health), highlighted several of the agency’s accomplishments in 2025 and outlined priorities for the years ahead. As background, ARPA-H is a federal health innovation agency with approximately $1.5 billion in annual funding dedicated to high-impact advances in human health. Unlike traditional grant-making organizations, ARPA-H operates through milestone-driven contracts. ARPA-H also act as “benevolent dictator,” allowing dissonance within the organization in how to approach a given project rather than seeking consensus, which Dr. Jackson explained as an intentional strategy to accelerate breakthrough innovation. The agency works closely with the FDA to help navigate regulatory risk, creating pathways that others in the ecosystem can follow. Namely, Dr. Jackson said that ARPA-H is willing to take early, high-risk bets in partnership with the FDA to enable later entrants to scale and succeed.
- Dr. Jackson highlighted yesterday’s launch of ADVOCATE (Agentic AI-EnableD CardioVascular CAre TransfOrmation), an agentic AI initiative focused on cardiovascular disease management. Broadly, she described AI as foundational to nearly every ARPA-H program, noting the agency’s unique ability to integrate large, fragmented datasets across the healthcare system. ADVOCATE aims to support both biotech innovation and clinical care, particularly in regions with primary care and specialist shortages. By embedding medical intelligence into AI-powered care delivery and leveraging wearables to monitor patients remotely, these tools could help determine when patients can safely recover at home versus requiring in-person care at a medical center. ARPA-H project manager Mr. Haider Warraich commented that this technology is not yet ready for widespread deployment, but ARPA-H is working to define regulatory pathways, post-approval monitoring frameworks, and strategies to scale it in order to support future adoption.
- Dr. Jackson also highlighted the Biological Data Fabric, an initiative designed to unify fragmented medical data, including EHRs and pathology reports, across health systems to create longitudinal patient histories. Not only does the technology allow families and clinicians to access comprehensive patient histories, but it also allows them to compare their medical journeys to others and learn from comparable cases to inform treatment decisions. The approach has already been successfully implemented in two hospital systems and is now being expanded to across 200 pediatric brain cancer centers – treating the leading cause of disease-related death in children – with $50 million in funding from ARPA-H.
- Speaking on another AI-enabled effort, the CATALYST program, ARPA-H program manager Mr. Andrew Kilianski explained the mission to reduce reliance on animal models by using in silico approaches in drug development. These models have the potential to significantly accelerate clinical trial timelines and reduce development costs.
- Dr. Jackson also discussed ARPA-H’s growing focus on longevity and age reversal. Aging is the greatest risk factor for most chronic and degenerative diseases, and even modest reductions in the biological age of key organ systems like the brain or heart could generate trillions of dollars in system savings. ARPA-H is investing in early-stage research to identify causal biomarkers of aging and link them directly to disease, helping the broader field prioritize the most promising therapeutic pathways. This includes leveraging resources such as the Interventions Testing Program and mouse model data to evaluate potential longevity therapies.
- Finally, Dr. Jackson addressed ARPA-H’s genetic medicines portfolio, citing the high-profile “Baby KJ” case as proof of the technology’s potential. While the science is promising, current approaches are not scalable to all patients who could benefit. Therefore, ARPA-H is focused on reducing manufacturing, delivery, and storage costs through innovations in extracellular vesicles, improved AAV vectors, continuous manufacturing, and better storage options.
Employer coverage at crossroads: Managing GLP-1 RAs and breakthrough therapies
Mr. Brian Heath (Kite Pharma), Dr. Will Shrank (Aradigm), and Dr. Dan Knecht (EmblemHealth) discussed strategies to reduce the cost of employer-sponsored coverage for high-cost therapies. The panel discussed how rising spending on GLP-1 RAs and the complexity of cell and gene therapies can strain this coverage and highlighted gaps in population-level management and payment certainty. They agreed that expanding access will require greater alignment across payers, providers, and manufacturers.
- The panel addressed the GLP-1 RA class that now accounts for ~15% of total spending among employers that offer open access. Dr. Shrank emphasized that GLP-1 RAs are transformative therapies should be available to all patients who need them, but acknowledged that universal access under current pricing would be prohibitively expensive. He commented on unexpected market dynamics, including direct-to-consumer models and compounded versions of GLP-1s RA, that he did not anticipate would gain such traction. Overall, he characterized the space as a “natural experiment” featuring widespread innovation and ongoing price compression as negotiations evolve.
- Dr. Knecht described the healthcare ecosystem as having been “on our heels rather than on our toes” when the latest generation of GLP-1 RAs launched. In hindsight, he said the ecosystem could have moved more quickly to anticipate demand and to counter longstanding narratives that frame obesity as a moral failing rather than a medical condition. Such efforts could have enabled broader coverage and more proactive adoption – though he also acknowledged early limitations with supply constraints.
- Dr. Shrank added that high-cost drugs covered under the medical benefit represent an under-managed category in healthcare, despite them being some of the most clinically impactful medications. He said that carriers have limited tools today but argued that a more proactive approach that “matches the right drug to the right patient” represents a clear opportunity for disruption.
- The panel also spent considerable time discussing access to cell and gene therapies. Mr. Heath explained that challenges in this space extend well beyond cost. Providers face uncertainty around the amount and timing of reimbursement – payment can be negotiated or delayed for months after the fact. Dr. Shrank agreed, noting that this dynamic has made it difficult for manufacturers to recoup R&D investment. Dr. Knecht warned that if these issues persist, more small and mid-sized employers may opt out of covering these therapies altogether.
- Despite these challenges, Mr. Heath emphasized that adoption is meaningful: more than 30,000 patients globally have received cell therapies. Kite Pharma operates in over 40 countries with more than 570 authorized treatment centers and participates in the CAR-T Vision initiative, which brings together stakeholders across the healthcare ecosystem. Mr. Heath identified three barriers hindering access: (i) lack of awareness among patients and providers; (ii) limited access due to insufficient accredited treatment centers; and (iii) the need for improved financing models with faster coverage and reimbursement decisions.
- On the policy front, Dr. Shrank highlighted CMS’s growing engagement in cell and gene therapy reimbursement as an encouraging sign. He pointed to CMS’s value-based contracting approach for sickle cell disease, which aligns incentives among manufacturers, payers, and patients by defining outcomes collaboratively and allowing states to opt in – an option already adopted by roughly two-thirds of states. He suggested this framework could extend to other conditions, noting that approximately 40 cell and gene therapies are currently approved and currently an estimated 3,000-4,000 in development, including drugs for more prevalent diseases like T1D. While an important step forward, he emphasized that this approach alone is not a comprehensive solution.
- The panel also spoke more broadly on improving access to expensive therapies that target smaller patient populations. They came to consensus around the desire to shift away from fee-for-service payment models and toward more outcomes-based arrangements. Dr. Shrank noted that for potentially curative gene therapies, outcomes are often easier to define. Dr. Knecht added that these agreements can be especially impactful when evidence is still emerging, as they help catalyze initial access. However, as the body of evidence grows and the value of the therapies becomes clearer, more traditional fee-for-service pricing models often become more practical.
Technology and strategy to capture Asia’s growing patient markets
Mr. Edward Booty (reach52), Ms. Janet Dorling (Gilead Sciences), Mr. Siddhartha Goyal (Nivi), Ms. Nafisa Jiwani (US International Development Finance Corporation [DFC]), and Ms. Natasha Sunderji (Accenture) discussed strategies to expand US pharmaceutical outreach to the growing Asian patient markets. The panel emphasized several commonalities in developing Asian markets, such as the need for pooled procurement, the importance of digital technology in outreach, and the role of the US government in supporting investments in these developing markets.
- The panel identified pooled procurement as a strategy to make treatment more accessible to developing markets, referencing the increased cost of adapting to national regulations and importing medication from the US or Europe. Ms. Jiwani discussed the strategy’s past success, especially in sub-Saharan Africa during the COVID-19 pandemic, and how the US government is now seeing a similar opportunity in Asia. Mr. Booty said combining multiple smaller markets into one large market through companies like reach52 allows for more affordable bulk pricing for pharmaceuticals and makes individual medications more affordable. Moreover, by navigating different import routes, developing markets – which are typically given a premium – can access cheaper European or American market prices.
- The panel also discussed the importance of digital technologies in international outreach. Mr. Goyal emphasized the value of the direct-to-consumer model in a market without comprehensive insurance systems. He said the best outreach strategy involves engaging consumers through pre-existing messaging platforms like WhatsApp.
- On the role of the US government in investing in Asian markets, panelists identified three main areas for US DFC’s investments: (i) health services and infrastructure; (ii) manufacturing and supply chain; and (iii) health and technology. Ms. Jiwani noted that the government only funds businesses with clear plans, rather than ideas. Therefore, any company seeking US DFC’s investments for its work in Asia must establish a clear plan for profit to be considered favorably.
The growing strength of Chinese biotechnology: Gaining trust and partnership
Dr. Ting Xu (Alphamab Oncology), Dr. Jing Song Wang (Harbour Biotech), Dr. Andrea Wang-Gillam (Jacobio Pharmaceuticals), Mr. Tony Liu (Abelzeta Pharmaceuticals), and Ms. Jane Wu (JP Morgan China) discussed emerging biotechnological development in China. The panel discussed the increasing trust and partnership of Chinese and Western biotechnology, the qualifications of researchers and workers of Chinese biotechnology companies, and the future medical focuses of the Chinese companies represented on the panel.
- Speakers discussed the growing trust and partnership between China and the west around biotechnology. Dr. Wang-Gillam noted that while previously the authenticity and quality of clinical research and data coming from China may have been questioned, there is now very little question of its validity. She commented that the speed and quality of Chinese research is being upheld by the supportive ecosystem of the Chinese FDA-equivalent and its drug-development infrastructure, not by concerns of improper procedures.
- The panel also discussed the numerous biotechnology and pharmaceutical deals and agreements made between Western and Chinese companies. Dr. Wang cited a recent multi-year deal between Harbour and AstraZeneca involving both economic and scientific collaboration. Mr. Liu similarly brought up deals made by Abelzeta with J&J and AstraZeneca as proof of expanding trust in Chinese research and development.
- The panel then fielded a question of where their workers and researchers studied. Multiple panelists, including Dr. Wang and Mr. Liu, revealed a growing trend of locally trained employees, with most chemists training in China, though much international experience is also present in upper management. Dr. Wang-Gillam claimed that the talent of Jacobio, which is US-based, originates from “all over the world,” but that it was fairly US-centric.
- The panel also discussed the future medical initiatives of their represented companies. Dr. Xu mentioned that Alphamab would continue focusing on safer Antibody-Drug Conjugates. Describing it as an “improved version of chemotherapy,” he pledged that they would consider quality of life during treatment development. Dr. Wang-Gillam stated that while her primary interest is oncology, the industry’s interest is also expanding quickly in chronic and metabolic diseases, along with pertinent government investments.
--by Nour Khachemoune, Kat Moon, Jeremy Alkire, Esther Min, Monica Oxenreiter, and Kelly Close